Financial risk, hospital cost, complications and comorbidities (CCc) in non-CC stratified urology...
5
FINANCIAL RISK, HOSPITAL COST, COMPLICATIONS AND COMORBIDITIES (CCC) IN NON-CC STRATIFIED UROLOGY DIAGNOSTIC RELATED GROUPS ERIC MUNOZ, M.D., M.B.A. HARRIS STERMAN, M.D. RICHARD FRIEDMAN, D.M.D., M.P.H. JONATHAN GOLDSTEIN, M.P.A. THOMAS GEROLD, M.D., M.B.A. LESLIE WISE, M.D. From the Departments of Surgery, Queens Hospital Center and the Long Island Jewish Medical Center, New Hyde Park; SUNY, Stonybrook; and CUNY School of Medicine, New York, New York ABSTRACT-The federal Medicare Diagnosis Related Group payment mechanism is undergoing constant change. Significant interest has been generated at the health policy level regarding reim- bursement for patients with complications and comorbidities. The purpose of this study was to analyze hospital resource consumption for patients in the seventeen urology non-complicating con- dition (CC) stratified Diagnostic Related Groups (DRGs), currently 45 percent of urology DRGs. We analyzed 185 Medicare patients in these non-CC stratified urology DRGs and found that pa- tients with more CCs per patient had higher total hospital costs per patient, financial risk under DRGs, a greater percentage of outliers, and a higher mortality, than patients in these same DRGs with fewer CCs per patient. These findings suggest that the current DRG system is inequitable to some patients and certain hospitals vis-a-vis non-CC stratified urology DRGs. The Health Care Financing Administration has not significantly changed the complicating condition urology DRG classification, as of its recent May, 1988 legislation. Financial disincentives to treat these patients may affect both their access and quality of care in the future. Medicare’s Diagnostic Related Group (DRG) reimbursement scheme is being constantly eval- uated by the U.S. Congress and independent advisory bodies. l Both the Health Care Financ- ing Administration (HCFA) and the Prospective Payment Assessment Commission (ProPAC) are recommending or implementing changes to DRGs. Hospitals face increasing economic un- certainty under new hospital payment schemes such as Medicare’s prospective Diagnostic Re- lated Group system. la Although hospitals have weathered the introduction of DRG payment, the health care environment appears to be be- coming increasingly competitive.2 Some pa- tients (such as emergency admissions or com- plexly ill patients) may be underreimbursed by DRG system. 3-4 Patients are grouped into urology DRGs by the principal diagnosis, operative procedure, presence of complications or comorbidities for some DRGs, and age. Urology DRGs are grouped in an attempt to provide appropriate reimbursement to hospitals based on the type of operative procedure. At the present time 17 of the 38 urology DRGs (44.7 %) are not stratified by the presence or absence of a complicating condition (CC) either a comorbidity (a medical condition present on admission to the hospital) or a complication (a condition acquired in the hospital) .5 The project’s purpose was to analyze resource consumption in non-CC stratified urology DRGs and to test the hypothesis that financial risk would be generated by patients who had a greater number of CCs. 380 UROLOGY ! OCTOBER 1988 / VOLUME XxX11, NUMBER 4
-
Upload
eric-munoz -
Category
Documents
-
view
217 -
download
5
Transcript of Financial risk, hospital cost, complications and comorbidities (CCc) in non-CC stratified urology...

FINANCIAL RISK, HOSPITAL COST, COMPLICATIONS
AND COMORBIDITIES (CCC) IN NON-CC STRATIFIED
UROLOGY DIAGNOSTIC RELATED GROUPS
ERIC MUNOZ, M.D., M.B.A. HARRIS STERMAN, M.D. RICHARD FRIEDMAN, D.M.D., M.P.H. JONATHAN GOLDSTEIN, M.P.A. THOMAS GEROLD, M.D., M.B.A. LESLIE WISE, M.D.
From the Departments of Surgery, Queens Hospital Center and the Long Island Jewish Medical Center, New Hyde Park; SUNY, Stonybrook; and CUNY School of Medicine, New York, New York
ABSTRACT-The federal Medicare Diagnosis Related Group payment mechanism is undergoing constant change. Significant interest has been generated at the health policy level regarding reim- bursement for patients with complications and comorbidities. The purpose of this study was to analyze hospital resource consumption for patients in the seventeen urology non-complicating con- dition (CC) stratified Diagnostic Related Groups (DRGs), currently 45 percent of urology DRGs. We analyzed 185 Medicare patients in these non-CC stratified urology DRGs and found that pa- tients with more CCs per patient had higher total hospital costs per patient, financial risk under DRGs, a greater percentage of outliers, and a higher mortality, than patients in these same DRGs with fewer CCs per patient. These findings suggest that the current DRG system is inequitable to some patients and certain hospitals vis-a-vis non-CC stratified urology DRGs. The Health Care Financing Administration has not significantly changed the complicating condition urology DRG classification, as of its recent May, 1988 legislation. Financial disincentives to treat these patients may affect both their access and quality of care in the future.
Medicare’s Diagnostic Related Group (DRG) reimbursement scheme is being constantly eval- uated by the U.S. Congress and independent advisory bodies. l Both the Health Care Financ- ing Administration (HCFA) and the Prospective Payment Assessment Commission (ProPAC) are recommending or implementing changes to DRGs. Hospitals face increasing economic un- certainty under new hospital payment schemes such as Medicare’s prospective Diagnostic Re- lated Group system. la Although hospitals have weathered the introduction of DRG payment, the health care environment appears to be be- coming increasingly competitive.2 Some pa- tients (such as emergency admissions or com- plexly ill patients) may be underreimbursed by DRG system. 3-4
Patients are grouped into urology DRGs by the principal diagnosis, operative procedure, presence of complications or comorbidities for some DRGs, and age. Urology DRGs are grouped in an attempt to provide appropriate reimbursement to hospitals based on the type of operative procedure. At the present time 17 of the 38 urology DRGs (44.7 %) are not stratified by the presence or absence of a complicating condition (CC) either a comorbidity (a medical condition present on admission to the hospital) or a complication (a condition acquired in the hospital) .5 The project’s purpose was to analyze resource consumption in non-CC stratified urology DRGs and to test the hypothesis that financial risk would be generated by patients who had a greater number of CCs.
380 UROLOGY ! OCTOBER 1988 / VOLUME XxX11, NUMBER 4

Material and Methods
All Medicare urology patients (N = 185) ad- mitted to the Long Island Jewish Medical Cen- ter (an 805 bed teaching hospital in suburban New York City) in any of the seventeen non-CC stratified urology DRGs from January 1, 1985, to December 31, 1986, were studied. Our hos- pital is categorized as an urban teaching hospi- tal by the DRG reimbursement scheme; stand- ard New York State DRG methodology was used for this analysis. Patients were assigned to a CC category based on the number of ICD-9- CM diagnoses codes per patient. Patients were grouped into four CC categories: all patients with no CCs per patient, and all patients with one-two CCs per patient, three-four CCs, and five or more CCs.
Hospital costs for each CC group (exclusive of physician fees) were computed for each pa- tient by hospital service area to include: room and board, laboratory (urinalysis, hematology, coagulation, biochemistry, and microbiology), radiology, blood and blood products, operating room-recovery room, central supply-pharmacy, and other (EKG, pathology, respiratory therapy, etc). A number of characteristics were analyzed for each patient including: mean total hospital cost per patient, mean hospital cost per patient for each hospital service, mean DRG reimbursement per patient, mean profit/loss per patient under DRGs, mean hospital length of stay (LOS) per patient, the mean number of diagnostic codes (ICD-g-CM) per patient, the mean number of procedure codes (ICD-g-CM) per patient, the percent outliers, and mortality. In addition, three clinical characteristics were analyzed for each CC category including: sur- gical intensive care unit (SICU) admission, need for a blood transfusion (i.e., red cells), and the requirement for plasma products (i.e.,
blood products). The analysis of variance (ANOVA) test was used to test for statistical sig- nificance between groups of patients.
Hospital Costing Methodology
Hospital cost per patient was obtained by uti- lizing per patient charge specific data and con- verting these charges to hospital costs. Cost to charge ratios utilized by our hospital account- ing division were used to convert charges to costs. The following ratios were used for each hospital service category:
Room and board 0.75 Laboratory 0.40 Blood (storage, processing,
transfusion, and products) 1.15 Pathology 2.42 Diagnostic radiology 0.94 Therapeutic radiology 1.71 Operating room 1.10 Recovery room 1.15 Respiratory therapy 0.76 Electrocardiology 0.25 Electroencephalography 1.40 Medical supplies 1.00 Pharmacy 1.00 Diagnostic ultrasound 0.46 Computed tomographic scan 0.53 Emergency department 0.91 Pulmonary function 0.08 Thus to obtain the hospital cost for diagnostic
radiology of $100, the following calculation was performed ($100 x 0.94 = $94); medical supplies ($100 x 1.00 = $100); blood ($100 x
1.15 = $115); and so on.
Results The mean total hospital cost per patient for
all patients was $10,691 (Table I). Mean total hospital cost per patient was highest for patients
TABLE I. Urology cost* by hospital service and CC cc Sample Cent-
Category Size R&B Lab Blood X-ray OR-RR Pharm Other Total None 53 $ 2,694 $ 4191 $llf $ 227$ $ 8473 $ 522 $ 2381‘ $ 4,970t One-two 71 5,330 912 21 365 1,246 596 575 9,044 Three-four 27 6,492 1,327
Et 637 1,496 862 875 11,726
Five or more 34 11,950 3,211t 1,286t 1,646$ 1,622t 2,469t 22,266t ALL 185 $ 5,958 $1,253 $31 $ 534 $1,241 $ 802 $ 870 $10,691
KEY: R & B = room and board; laboratory (urinalysis, hematology, coagulation, biochemistry and microbiology); OR-RR = operat- ing room-recovery room; Cent-Pharm = central pharmacy.
*Mean per patient tStatistically different at p < 0.01 from all patients. $Statistically different at p < 0.05 from all patients.
UROLOGY / OCTOBER 1988 / VOLUME XxX11, NUMBER 4 381

TABLE II. Urology resource characteristics * by CC
cc DRG wt
Category Index None 1.4786 One-two 1.6601 Three-four 1.9302 Five or more 2.09171
ALL 1.7240 *Mean per patient. tProfit/loss per patient; ( ) equals loss. $Length of stay (days).
Profit/ Hospital No. of No of Loss f Loss* Diagnoses5 Procedures$
$4,063 5.811 1.0011 1.6411 1,000 11.3 2.4711 3.09 ($279) 13.9 4.4011 4.03
($9,228) II 23.311 7.8811 5.4711
($189) 12.3 3.30 3.25 $(ICD-g-CM) codes per patient. IIStatistically different at p < 0.01 from all patients. fiStatistically different at p < 0.05 from all patients.
with five or more CCs, $22,266. Mean hospital cost by hospital service demonstrated considera- ble variation among the CC categories, how- ever, mean hospital cost rose as CCs per patient increased. The largest component of total hos- pital cost was for room and board, followed by laboratory, operating room-recovery room, other, central supply-pharmacy, radiology, and blood.
The mean DRG weight index per patient for all patients was 1.7240 (Table II). Mean DRG weight index rose as CCs per patient increased; highest was for patients with five or more CCs, 2.0917. Thus one component of the higher total hospital cost for patients with a greater number of CCs was explained by a greater DRG weight index. However, although patients with five or more CCs per patient had a 41 percent greater DRG weight index vs those patients with no CCs, they had a 348 percent greater total hospi- tal cost. The mean financial loss per patient for all patients under DRGs was $189. Financial risk increased as CCs accumulated; greatest risk financially was for patients with five or more CCs, $9,228 loss per patient. The mean hospital length of stay per patient for all patients was 12.3 days. Hospital length of stay rose with CCs; greatest length of stay was for patients with five or more CCs, 23.3 days. The number of diagnoses per patient for all patients was 3.3, and the number of procedures per patient was 3.25. Both diagnoses and procedures per pa- tient rose with CCs.
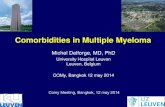
There were no mortalities for patients with no CCs or one-two CCs. However, patients with three-four CCs had a 3.7 percent mortal- ity, and patients with five or more CCs had a 20.6 percent mortality, The percent outliers rose as CCs per patient accumulated; patients with five or more CCs had almost a 25 percent outlier rate (Fig. 1A). SICU utilization in-
creased as CCs per patient rose (Fig. 1B). Blood utilization rose as CCs per patient accumu- lated; almost three fourths of patients with five or more CCs required blood (Fig. 1C).
Comment
The current dynamic world of health care fi- nance requires that urologists analyze health policy issues for their patients. The purpose of this study was to analyze hospital resource con- sumption for patients in the seventeen urology non-CC stratified DRGs. Our findings demon- strated greater resource utilization for patients in these DRGs with more CCs per patient. Thus patients in these DRGs with a greater number of CCs had higher total hospital costs, a much longer hospital length of stay, more procedures per patient, greater financial risk under DRGs, a higher proportion of outliers, and a greater mortality than patients in these same DRGs with fewer CCs. These findings suggest a signif- icant inequity in the current DRG scheme vis-a- vis patients in these non-CC stratified urology DRGs with more CCs per patient.
The Health Care Financing Administration (HCFA) and the Prospective Payment Assess- ment Commission (ProPAC) analyze and rec- ommend changes to the federal Medicare DRG system. There are a number of proposals to modify DRGs to make the payment more equi- table for the urology non-CC stratified DRGs. The Prospective Payment Assessment Commis- sion (ProPAC), an independent advisory body to the Congress regarding DRGs, in its April, 1987, report to the Secretary of Health and Hu- man Services advised several modifications re- garding CCs. Recommendation 21: The Use of Patient Age in Defining DRGs states, “DRGs should not be defined based on the current vari- able of age greater than 69 and/or presence of a
382 UROLOGY i OCTOBER 1988 / VOLUME XxX11, NUMBER 4

FIGURE 1. (A) Outliers rose with CCs, almost one fourth of patients with jive or more CCs were out- Iiers. (B) Surgical intensive care unit (SZCU) utiliza- tion increased as CCs rose; over one third of patients with jive or more CCs were admitted to SZCU. (C) Blood requirements increased as CCs per patient rose; almost three fourths of patients with jive or more CCs used blood.
complication or comorbidity (CC). The Com- mission believes that the resource use for Medi- care patients 70 years or older without a CC is significantly lower than for cases with CCS. DRGs should be defined on the basis of pres- ence or absence of CC, regardless of age. The Secretary should implement this change for DRGs that currently split on age and CC, and should determine whether other DRGs should also be split on CC.‘” Similarly, Recommenda- tion 22: Improving the Use of Complications and Comorbidities in Defining DRGs states, “The Secretary should revise the current list of complications and comorbidities, and its use in defining DRGs, to ensure more appropriate grouping of Medicare cases for payment under PPS. The Secretary should evaluate several pos- sible approaches, including the development of Major Diagnostic Category (MDC)-or DRG specific CCs on the basis of resource intensity, and the specification of levels of complexity among the CCs.?
The Health Care Financing Administration has not adopted these ProPAC recommenda- tions. The most recent HCFA modification to DRGs (May 27, 1988) contains some minor re- finements to the associated diseases categorized as CCS.~ However, no major restructuring of urology DRGs by CCs (as suggested here) has been implemented. Supporters of HCFA con- tend that further payment and stratification of DRGs along the lines of CCs will induce hospi- tals to find more CCs per patient (i.e., “up- code”) and might result in an increase in aggre- gate DRG payments. Thus, it appears that there will not be any immediate change in the current DRG system regarding CCs. This study demonstrates the continued importance of financial analysis of the health care of the urol- ogy patient.
Conclusions
The federal government has not further re- vised the DRG grouping of urology patients into DRGs by associated complications or co-
.&?.I c iv
Il.5 i
1 I 1
w
55-
J-
h-
L- P I5 -
I# -
morbidities, despite some data to do so. This study of 185 Medicare urology patients in the seventeen non-complicating condition (CC) stratified urology DRGs demonstrated that pa- tients in these non-CC stratified DRGs with a greater number of CCs had higher resource consumption, financial risk under DRGs, and a poorer outcome than patients in these same DRGs with fewer CCs per patient. Urologists
UROLOGY / OCTOBER 1988 / VOLUME XxX11, NUMBER 4 383

must analyze health payment changes to assure equitable reimbursement for the patients under their care.
Department of Surgery Long Island Jewish Medical Center
New Hyde Park, New York 11042 (DR. MUNOZ)
ACKNOWLEDGMENT. To James Moyer, Seth Warren, and Gordan Doletto, Divisions of Management Information Systems and the DRG Task Force of the Long Island Jew- ish Medical Center, to Katherine Mulloy for data compu- tation, and to Christina Weiss for assistance in the prepa- ration of this manuscript.
References
1. Medicare Prospective Payment and the American Health Care System, Report to Congress, (Prospective Payment Assess-
ment Commission), Washington, D.C., June, 1988, pp 1-125. la. Igelhart JD: Medicare begins prospective payment for hos-
pitals, N Engl J Med 308: 1428 (1983). 2. Blendon RJ: Policy choices for the 1990s: An uncertain look
into America’s future, in Ginzberg E (Ed): The US Health Care System. A look to the 1900s. Totowa, N.J., Rowman & Allanheld, 1985.
3. Munoz E, Tinker MA, Margolis I, and Wise L: Sur- gonomics. The Cost of Choleycstectomy, Surgery 96: 642 (1984).
4. Horn S, et al: Interhospital differences in severity of illness, N Engl J Med 313: 20 (1985).
5. Healthcare Financing Management Association: Descrip- tion and Analysis of Medicare Prospective Price Setting, Oak Brook, IL, Healthcare Financial Management Association, 1984.
6. Report and Recommendation to the Secretary, U.S. Depart- ment of Health and Human Services, Prospective Payment Assess- ment Commission (April 1, 1987), pp 51-52.
7. Report and Recommendation to the Secretary, U.S. Depart- ment of Health and Human Services, Prospective Payment Assess- ment Commission (April 1, 1987), pp 52-53.
8. Federal Register, United States Government Printing Of- fice, Washington, D.C., 53: 103, 19502-19503 (1988).
384 UROLOGY I OCTOBER 1988 I VOLUME XxX11, NUMBER 4