Evoluzione della Chirurgia Radio Guidata del Nodulo...
28
Chirurgia Toracica Dipartimento Cardio - Toracico Azienda Ospedaliera Universitaria Pisana Evoluzione della Chirurgia Radio Guidata del Nodulo Polmonare Solitario: dalla tecnica video-assistita alla robotica F Davini II Congresso Nazionale di Chirurgia Radioguidata Milano 1-2 dicembre 2016
Transcript of Evoluzione della Chirurgia Radio Guidata del Nodulo...

Chirurgia Toracica
Dipartimento Cardio-Toracico
Azienda Ospedaliera Universitaria Pisana
Evoluzione della Chirurgia Radio Guidata del Nodulo Polmonare Solitario: dalla tecnica video-assistita alla robotica
F Davini
II Congresso Nazionale di Chirurgia Radioguidata
Milano 1-2 dicembre 2016

Lesione sferica intraparenchimale, radiologicamente
rilevabile, con diametro uguale o inferiore a 3 cm, non
associata ad atelettasia o linfoadenopatia.
Glossary of terms for thoracic radiology:
recommendations of the Nomenclature committee of the Fleishner society. A J R 1984
Definizione di Nodulo polmonare solitario

L’utilizzo della TAC spirale come screening della neoplasia polmonare ha aumentato di 10 volte l’incidenza del nodulo
polmonare solitario.
Erasmus JJ et al.
Solitary pulmonary nodules: morphologic evaluation for differentiation of benign and malignant lesions. Radiographics, 2000.
Screening del Tumore Polmonare
Tomografia Assiale Computerizzata
European and North American lung cancer screening experience and implications for pulmonary nodule management
The potential for low dose computed tomography (LDCT) to act as an effective tool in screening for lung cancer is currently the
subject of several randomised control trials. It has recently been given prominence by interim results released by the North American
National Lung Screening Trial (NLST). Several other trials assessing LDCT as a screening tool are currently underway in Europe,
and are due to report their final results in the next few years. These include the NELSON, DLSCT, DANTE, ITALUNG, MILD and LUSI
trials. Although slow to instigate a trial of its own, the UK Lung Screen (UKLS) trial will shortly commence. The knowledge gained from
the newer trials has mostly reinforced and refined previous concepts that have formed the basis of existing nodule
management guidelines. This article takes the opportunity to summarise the main aspects and initial results of the trials presently
underway, assess the status of current collaborative efforts and the scope for future collaboration, and analyse observations from these
studies that may usefully inform the management of the indeterminate pulmonary nodule. Key Points • Low dose CT screening for lung
cancer is promising. • The effect of LDCT screening on mortality is still uncertain. • Several European randomised controlled trials
for LDCT are underway. • The trials vary in methodology but most compare LDCT to no screening. • Preliminary results have reinforced
existing nodule management concepts
Eur Radiol. 2011 Dec;21(12):2445-54. doi: 10.1007/s00330-011-2219-y. Epub 2011 Aug 10

Low-dose spiral CT screening and evaluation of the solitary pulmonary nodule
Abstract
Lung cancer screening using helical low-dose computerized tomography (LDCT) increased drastically after publication of a
successful well-designed prospective randomized screening study, the National Lung Screening Trial. This increase in
screening has led to a significant increase in the diagnosis of solitary pulmonary nodules (SPNs). Some of these lesions are
early cancers, and their removal can potentially prevent a lung cancer death. Some have the histologic appearance of a cancer but will
never progress and cause harm. Some are non-neoplastic and are best observed. The number of lesions detected with LDCT is so
great that algorithms are being developed for more efficient evaluation and management of SPNs. This article will discuss current tools,
approaches, and concerns regarding patient care in this setting.
Oncology (Williston Park). 2014 May;28(5):441-6
With a median follow-up of 6.5 years, there were 13% more lung cancers and a 20% reduction in lung cancer mortality (95%
confidence interval [CI], 6.8–26.7; P = .004) in the LDCT arm compared with the chest x-ray arm. The ability of CT imaging to find
suspicious lesions was well demonstrated by the trial. The risk of a false-positive finding in the first screen was 21%. Overall, after three
CTs, 39.1% of participants had at least one positive screening result. Of those who screened positive, the false-positive rate was 96.4%
in the LDCT group.[5]
Oncology (Williston Park). 2014 May;28(5):441-6

Il riscontro occasionale di NPS, in pazienti asintomatici,
Ha una prevalenza stimata del 8-51% secondo i vari studi di screening
ACCP Evidence-based Clinical Practice Guidelines (2° Edition). Chest 2007; 132: 94S-107S
Oltre il 96% dei casi i noduli polmonari incidentali presentano un
diametro < 10 mm, tra questi il 72% ha un diametro < 5 mm
Incidentally detected small pulmonary nodules on CT. Clin Radiol 2009; 64:872-884

Il principale problema è
la gestione dei NP incidentali di piccole dimensioni
ACCP Evidence-based Clinical Practice Guidelines (2° Edition). Chest 2007; 132: 94S-107S
Tasso Malignità
1-12%ACCP Evidence-based Clinical Practice Guidelines (2° Edition). Chest 2007; 132: 94S-107S

Obiettivi
Identificare i pazienti con lesioni Maligne che possono beneficiare
di un trattamento chirurgico potenzialmente curativo
Evitare procedure invasive inutili
Il management dei noduli deve essere
diversificato:
DENSITA’
- Parzialmente solido (probabilità di malignità 63%)
- Non Solido (probabilità di malignità 18%)
- Solido (probabilità di malignità 7%)
Frequency and significance of part-solid and non solid nodules. AJR 2002; 178:1053-1057

NP Parzialmente SolidoPersistente o Transitorio
FUP: LDCT a
3 mesi
Persistente
Margini spiculati
Broncogramma aereo
Retrazione pleurica
Overview and strategic management of subsolid pulmonary nodules.
J thorac Imaging 2012;27:240-248
Transitorio
Margini sfumati
Età giovanile
Lesioni molteplici
Chirurgia

NP non solido (ground glass)le linee guida si basano sulle dimensioni del nodulo
< 5 mm > 5 mm
LDCT annualeLDCT a 3
mesi
Stabile: FUP
con LDCT x 3-
5 anni
Aumento
dimensioni
ChirurgiaOverview and strategic management of subsolid pulmonary nodules.
J thorac Imaging 2012;27:240-248

NP solido
Accurata valutazione della probabilità di malignità
- Fattori di rischio: età, fumo, esposizione asbesto-radon, storia familiare positiva per etp
- Caratteristiche radiologiche: dimensioni, morfologia, sede, margini, enhancement
- Crescita dimensionale: metodo volumetrico tridimensionale, valutato sul tempo di
raddoppiamento o Volume Doubling Time, un VDT tra 20 e 300 giorni è indicativo di etp
- Attività metabolica: PET-TC
La probabilità di malignità cresce in modo proporzionale
alle dimensioni del nodulo:
Noduli < 5mm: 0-1%
Noduli tra 5 e 10 mm: 6-28%
Noduli tra 10 e 20 mm:41-64%
Noduli > 20mm: 67-82%
The incidental small pulmonary nodule and the Fleischner Criteria 5 years later. J Thorac Imaging 2011; 2: 88-89

Nodule size (mm) Basso rischio Alto rischio
≤4 No follow-up Follow-up CT a 12 mesi;
se stabile, no follow-up
>4-6Follow-up CT at 12 mesi;
se stabile, no follow-up
Follow-up CT a 6-12
mesi poi a 18-24 mesi se
stabile
>6-8
Follow-up CT at 6-12
mesi poi a18-24 mesi se
stabile
Follow-up CT a 3-6 mesi
poi a 9-12 mesi e a 24
mesi se stabile
Fleischner Society guideline for
solitary pulmonary nodule management (2005)
Le linee guida indicano la necessità di una caratterizzazione istologica in caso di crescita del
nodulo o di un follow up di 2 anni come limite per ritenerlo stabile

ACCP (2007)American College of Chest Physicians
NP solido (>8< 30mm)
Bassa
probabilità
Intermedia
probabilità
FUTC
3-6-12-24 mesi
Tc con mdc
PET
FNAB
Broncoscopia
Biopsia/VATS
Chirurgia
Alta
probabilità
+-

Metodiche diagnostiche

Kim SK et al.
Accuracy of PET/CT in characterization of solitary pulmonary lesions.
J Nucl Med. 2007 Feb;48(2):214-20.
La TAC PET unisce in maniera sinergica
La sensibilità dell’esame TAC e la specificità
della PET.
TAC/PET
TAC
Sensibilità: 93%
Specificità 31%.
PET
Sensibilità: 97%
Specificità 85%.
PET-TAC
Sensibilità: 97%
Specificità: 85%.
Falsi positivi: infezioni, patologie infiammatorie
Falsi negativi: carcinoide tipico, adenocarcinoma (mucinoso), lesioni < 10 mm

Sensibilità nella diagnosi di lesioni maligne: 64-100%
Weisbrog et al
Transthoracic needle biopsy.
World J Surg 1993; 17: 07-11.
Prelievi trans-toracici nella diagnosi di NPS
Sensibilità nella diagnosi di lesioni benigne: 12-68%
Lacasse et al.
Transthoracic needle aspiration biopsy for the diagnosis of localized
pulmonary lesions: a meta-analisys.
Thorax 1999; 54; 884-893.

Probabilità di fallimento nella localizzazione:
Distanza dalla superficie pleurica, mm
Dimensioni , mm >10 10-5 <5 0
<10 2/2 (100%) 3/6 (50%) 4/12(33%) 1/11 (9%)
>10 4/13 (31%) 3/12 (25%) 1/5 (20%) 5/24 (21%)
Suzuki K et al.
VATS for small Indeterminate Pulmonary Nodules: indication for preoperative marking.
Chest 1999
La localizzazione del NPS
Il nodulo polmonare può risultare di difficile localizzazione in VATS.
Ciò ha reso necessario lo sviluppo e l’utilizzo di metodiche di localizzazione
pre- e intra-operatoria.

PRE-OPERATORIE
Marcatura del nodulo con coloranti vitali (Blu Di Metilene)
Marcatura con aghi uncinati o spirali trans toracici
Marcatura mediante Albumina colloidale marcata con Tecnezio
Radioattivo
Principali tecniche di localizzazione
INTRA-OPERATORIE
Palpazione digitale della lesione
Ecografia endoscopica

Prevede una fase pre-operatoria di Iniezione
del colorante sotto guida TAC
Tecniche di localizzazione pre-operatoria
MARCATURA CON COLORANTI VITALI (Blu di Metilene)
Lenglinger et al.
Localization of pulmonary nodules before thoracoscopic surgery:value of staining with methylene blue dye.
AJR 1994
L’intervento deve essere effettuato
in tempi rapidi (entro tre ore),
data la rapida diffusione del colorante
In caso di antracosi polmonare,
la localizzazione dell’area colorata
può risultare difficoltosa

MARCATURA CON AGHI UNCINATI
Posizionamento di aghi trans-toracici sotto
guida TACche rimangono nella lesione per
mezzo della loro estremità che assume forme
di uncino o di spirale
Tecniche di localizzazione pre-operatoria
Studio N°
Paz.
Posizionamento
TAC guidato
PNX Dislocazione Toraco-
tomia
Motivi della
conversione
Pittet et al.
2007
45 43/2 1/43 0 2/43 Sede del nodulo (2)
Eichfeld et al.
2005
22 22 7/22 2 3/22 Incompleto collasso (1)
Aderenze pleuriche (1)
Dislocazione ago (1)
Ciriaco et al
2004
53 53 4/53 5 4/53 Sede del nodulo (2)
Aderenze pleuriche (1)
Dislocazione ago (1)
Powell et al
2004*
12 12 0 1 0
* Utilizzo di microspirali di platino identificate mediante radioscopia intraoperatoria

CHIRURGIA RADIOGUIDATA



Ogni lesione nodulare di nuova insorgenza dovrebbe essere
considerata maligna fino a prova contraria
Indicazioni all’Exeresi Chirurgica
L’utilizzo di metodiche mini-invasive e la resezione limitata del
parenchima sono il primo approccio chirurgico.
L’utilizzo dell’esame estemporaneo consente, in caso di NSCLC,
l’immediata conversione della procedura in lobectomia con
linfoadenectomia ilo-mediastinica.
Nei pazienti in cui la riserva funzionale è compromessa, resezione
parenchimale limitata è una procedura accettabile.

Totale pazienti NPS (< 3 cm) (2010-2016) 772
Sesso 443 maschi e 329 femmine
Età media 54,7 aa (12-82)
--------------------------------------------------------------------------------------------------
NPS trattati con la metodica Probe 175
Dimensioni medie del nodulo 13 mm (5-20 mm)
Distanza media dalla viscerale 15 mm (6-39 mm)
--------------------------------------------------------------------------------------------------
Chirurgia Toracica
Dipartimento Cardio-Toracico
Azienda Ospedaliera Universitaria Pisana

NSCLC 44 (26%)
Metastasi polmonari 109 (62%)
Lesioni benigne 22 (12%)
Risultati
In 41 pazienti si è proceduto ad eseguire una lobectomia.
29 per via toracotomica, 12 robotica3 pazienti per scarso PS hanno eseguito una wedge resection
I pazienti con sospetto etp primitivo eseguono
l’ intervento in Chirurgia Robotica,
quelli con sospetto di metastasi in Toracoscopia
La Chirurgia Robotica
Consente di mantenere la mini-invasività, eseguendo lobectomie, per i noduli
resecati con l’ausilio della sonda Probe, dopo che all’ esame estemporaneo
sono risultati tumori polmonari primitivi.

Thorac Cardiovasc Surg.2016 Mar 10.
Forty-Two Years' Experience with Pulmonary Resections of
Metastases from Colorectal Cancer.Dudek W, Schreiner W, Hohenberger W, Klein P, Sirbu H
•1Friedrich-Alexander University Erlangen-Nürnberg (FAU), Erlangen,
Germany.
Background Pulmonary metastasectomy is a commonly
performed surgery in patients with controlled metastatic colorectal
cancer (CRC). We reviewed our long-term single institution
experience with lung resections for colorectal metastases to
assess the factors influencing patient survival. Materials and
Methods A cohort of 220 patients (138 men and 82 women;
median age, 59 years) who underwent complete pulmonary
metastasectomy for CRC with curative intent between 1972 and
2014 was retrospectively analyzed. The impact of factors related
to primary tumor, metastases, and associated therapy on patient
survival was assessed. Results Two postoperative inhospital
deaths occurred. The median interoperative interval was 26
months. The overall 5-year survival rate after pulmonary
metastasectomy was 49.4%. In univariable analysis, bilateral
pulmonary metastases (log rank p = 0.02), multiple metastases
(log rank p = 0.005), and stage IV UICC (the International Union
Against Cancer) CRC at the time of initial presentation (log rank
p = 0.008) were significantly associated with poor outcome.
Multivariable Cox analysis demonstrated that stage IV CRC
(p = 0.02) and multiple metastases (p = 0.0019) were statistically
significant predictors of survival after the pulmonary
metastasectomy. There was no significant difference in survival
between patients with high versus low preoperative
carcinoembryonic antigen serum level (p = 0.149), high versus low
preoperative carbohydrate antigen 19-9 serum level (p = 0.291),
and primary tumor location in rectum versus colon (p = 0.845).
Conclusion Patients with unilateral metastasis and stages I to
III primary tumor benefited most from pulmonary metastasectomy
for CRC.
J Thorac Oncol., 2010 Jun;5(6 Suppl 2):S172-8.
Reported outcome factors for pulmonary resection in
metastatic colorectal cancer.
Pfannschmidt J1, Hoffmann H, Dienemann H
Author information
•1Department of Thoracic Surgery, University of Heidelberg,
Thoraxklinik, Heidelberg, Germany.
Abstract
Pulmonary resection of metastatic colorectal cancer is widely
practiced in surgical oncology. However, only a highly selected
subset of patients is eligible for resection, and the average
recurrence rate is still high. We reviewed the recent literature on
pulmonary metastasectomy for colorectal cancer and tried to
address the issue of patient selection based on prognostic
parameters associated with long-term survival. No randomized
phase III trials are available, and data for this review were retrieved
only from retrospective studies. We excluded papers reporting on
patients earlier than 1990. In summary, there is a substantial body
of evidence demonstrating that resection of pulmonary metastases
can be performed safely and with a low mortality rate. For a subset
of highly selected patients, the overall results of a 5-year actuarial
survival rate after complete resection ranged between 40 and 68%.
These outcomes exceed those normally associated with metastatic
colorectal cancer. It is this perception that has encouraged
surgeons and caused the practice to grow.
Metastasi da etp colon
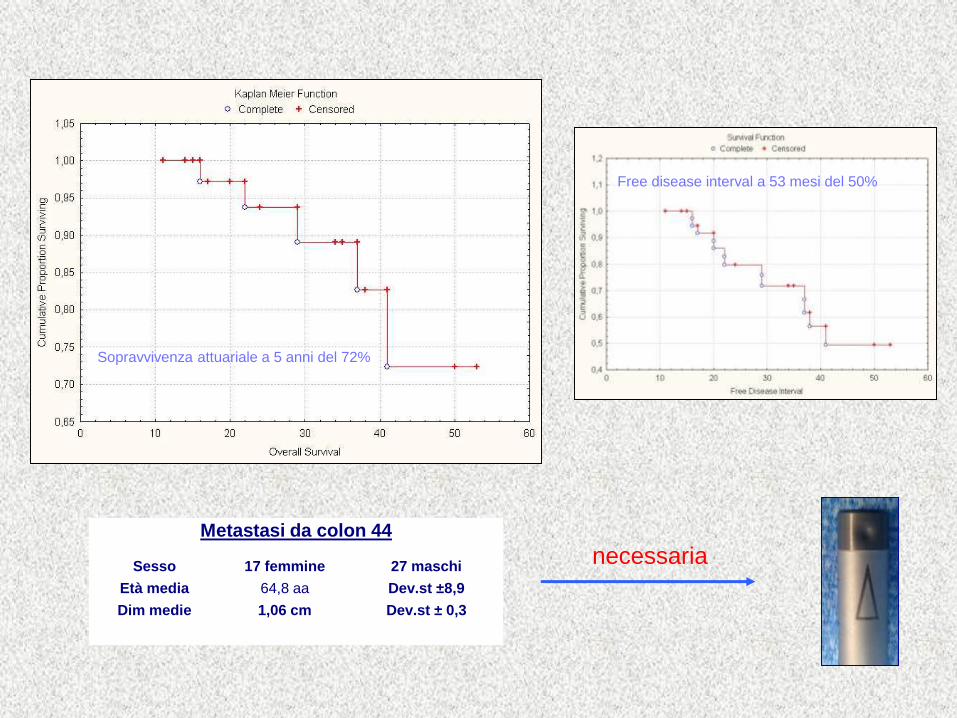
Metastasi da colon 44
Sesso 17 femmine 27 maschi
Età media 64,8 aa Dev.st ±8,9
Dim medie 1,06 cm Dev.st ± 0,3
Sopravvivenza attuariale a 5 anni del 72%
Free disease interval a 53 mesi del 50%
necessaria

Decisions for further management are often based on preference by the
clinician with the majority of physicians not following current guidelines in the
management of pulmonary nodules. Poor adherence to pulmonary nodule
guidelines is multifactorial with a variety of factors coming into play. These
include inappropriate advice given by the radiologist, patient age,
comorbidities, patient preference, and physician's technical skill all influencing
the decision making.J Thorac Dis. 2016 Jul;8(Suppl 6):S494-7. doi: 10.21037/jtd.2016.05.48.
Incidental nodule management-should there be a formal process?
Sethi S
L’utilizzo di metodiche radiologiche sempre più sensibili determinerà un aumento
del rilievo del NPS. Le linee guida dovrebbero essere seguite in linea di massima
La necessità di una diagnosi cito-istologica comporterà un aumento della
applicazione delle metodiche mini-invasive e delle tecniche di localizzazione
Riteniamo la chirurgia radioguidata una metodica sicura ed efficace.
Nuovi “device” possono essere considerati nel trattamento dei noduli polmonari
nell’ottica costo/beneficio
Conclusioni


![[semana14-día2] NODULO TIROIDEO](https://static.fdocuments.net/doc/165x107/557201544979599169a14d8e/semana14-dia2-nodulo-tiroideo.jpg)