ANTICOAGULATION ISSUES In Geriatric Population Ann McBride, M.D. UW Anticoagulation Service.
Upload
judith-mooreCategory
view
218download
0
Evidence Review
Anticoagulation in ACS & PCI
Presented by:Dr Rakesh JainSenior Resident
Dept. of CardiologyGovt. Medical College, Calicut

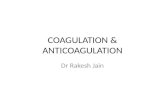
Role of thrombin & Targets for anticoagulants
Tissue factor
Plasma clottingcascade
Prothrombin
Thrombin
Fibrinogen Fibrin
Thrombus
Platelet aggregation
Conformational activation of GPIIb/IIIa
Collagen
Thromboxane A2
ADP
AT
AT
BivalirudinHirudin
Dabigatran
FactorXa
Fondaparinux
LMWHHeparin
Direct Xa inhib
Plaque rupture[Spontaneous/Iatrogenic
(Stenting)]

Selection of anticoagulants
Depends on:1. Type of ACS2. Initial strategy3. In STEMI (1 PCI / TLT)
Non STEMI Initial invasive: UFH, enoxaparin, bivalirudin or fondaparinux Initial conservative: Enoxaparin, fondaparinux or UFH (less
preferred)
STEMI Initial invasive: UFH, bivalirudin Initial conservative (TLT): UFH, enoxaparin or fondaparinux
2012 FOCUSED UPDATE OF THE 2007 ACC/AHA: J Am Coll Cardiol 2011;57:e215–e367: J Am Coll Cardiol 2012; 60:645–681.

Unfractionated heparin (UFH)
Unfractionated heparin: A declining role Bleeding risk HIT Availability of newer anticoagulant

Adding Heparin to Aspirin Reduces the Incidence of Myocardial Infarction and Death in Patients With Unstable Angina:
A Meta-analysis• AIM: To estimate risk of MI & death in unstable angina/non Q- MI pts, treated with
aspirin plus heparin v/s aspirin alone.
• Six randomized trials were included.
• Heparin was given as a continuous infusion for 2 to 7 days (aPTT: 1.5- 2x) and aspirin indefinitely.
• Primary outcome: Incidence of MI or death.
Oler et al. JAMA. 1996;276:811-815

RR: Death/MI
ASA Alone 68/655=10.4%
Heparin + ASA 55/698=7.9%
B
B
B
B
B
B
B
0.1 1 10
Summary Relative Risk
0.67 (0.44-0.1.02)
Theroux
RISC
Cohen 1990
ATACS
Holdright
Gurfinkel
Comparison of Heparin + ASA vs ASA Alone
ASA, acetylsalicylic acid; RISC, Research on InStability in Coronary artery disease; ATACS, Antithrombotic Therapy in Acute Company Syndromes; RR, relative risk; MI, myocardial infarction.Oler A, et al. JAMA. 1996;276:811-815. (with permission)
Conclusion: 33% reduction in risk of MI or death in patients with unstable angina treated with aspirin plus heparin compared with those treated with aspirin alone.

UFH in STEMITrial Design/ Comparisons Comments
Metanalysis of aspirin, UFH & Fibrinolytic therapyNEJM 1997;336:847-60
ISIS-3 and GISSI-2 [only small mort. benefit for s/c heparin] 68000 pts
5 lives saved/1000 pts treated with UFH + STK
GUSTO-I trialNEJM 1993;329:673-82
20 000 pts STK/tPA + [IV vs S/C UFH]
No sign. diff. observed in death, reinfarction, or non h’gic strokes Patency rate (5-7 d)- IV UFH [88% vs 2%] Reinfarction- S/C UFH (3.4% vs 4.0%)5yr follow up demonstrated similar survival rates for STK + UFH cf tPA
SCATI trial Lancet1989;ii:1826
2000-IU bolus UFH followed by 12 500 U s/c BD vs placebo.
Reduction in mortality & stroke. UFH may be given in patients with high risk of embolism
ISIS pilot study.Eur Heart J. 1987 Jun;8(6):634-42.
Post STK ,either intravenous heparin (1000 IU h-1 for 48 hours) or no heparin
Heparin was associated with a decrease in reinfarction (2.2% heparin vs 4.9% no heparin; NS), though not in mortality (in hospital: 8.0% vs 8.5%; NS, and after discharge: 7.0% vs 6.9%; NS),
Hence UFH has been used since years for all types of ACS, mostly because of unavailability of others.

LMWH ESSENCE trial (A COMPARISON OF LMWH WITH UFH FOR UNSTABLE CAD)
• Prospective, double-blind, placebo controlled multicenter study (1994-1996).
• Included 3171 patients with angina at rest or non–Q-wave MI.
• Male: 67%
MARC COHEN et al: N Engl J Med 1997;337:447-52.

ESSENCE: Study Design
Enoxaparin1mg/kg q 12 HSubcutaneous
+ ASA(100 to 325 mg)
Unfr. HeparinIV dose-adjusted
+ ASA
Follow-up VisitDay 14
Follow-up VisitDay 14
Follow-up CallDay 30
Follow-up CallDay 30
Unstable AnginaNon-Q-Wave MI
Treatment Phasemin 48 H, max 8 Days
Follow-up Phase

Inclusion Criteria:• Male or non pregnant female ≥ 18 years
• Recent onset rest angina
• Last episode of angina within 24 hours
• Definite evidence of underlying CAD (1 or more): Ischemic ECG changes on presentation
Previous MI, PTCA or CABG
Previous angiography with > 50% vessel stenosis
Exclusion criteria:• LBBB or pacemaker
• Persistent ST-segment elevation
• Angina with precipitating cause (e.g. heart failure or tachydysrhythmia)
• Contraindications to anticoagulation or
• CrCl ˂ 30 ml/min

NEJM, 337:447-452, August, 1997
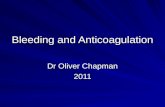
ESSENCE: Primary Results: Death, MI, Recurrent Angina
30%
25%
20%
15%
10%
Time (Days)
HeparinEnoxaparin
5%
0
% D
eath
, M
I o
r R
ecu
rren
t A
ng
ina
1 3 5 7 9 11 13 15 17 19 21 23 25 2729 31
19.8%
16.6%RRR 16.2 %
P=0.019
23.3%
19.8%
RRR 15 % P=0.016

Major Hemorrhagic Events

CONCLUSION
“Antithrombotic therapy with enoxaparin plus aspirin was more effective than UFH plus aspirin in reducing the incidence of ischemic events in patients with UA/Non-Q MI in the early phase. This benefit of enoxaparin was achieved with an increase in minor but not in major bleeding.”

Enoxaparin versus UFH in patients treated with tirofiban, aspirin and an early conservative initial management strategy: results from
the A phase of the A-to-Z trial• Aim: To know relative merits of enoxaparin over UFH in Non-Q MI pts receiving concomitant
glycoprotein IIb/IIIa inhibitors.
• Open label non-inferiority trial included 3987 pts to receive either enoxaparin or UFH in combination with aspirin and tirofiban.
• Early conservative strategy was specified for 1778 patients (45%) [UFH(n = 872) enoxaparin(n = 906)].
• Results: Primary endpoint (death, new MI or documented refractory ischemia within 7 days of randomisation) occurred in 10.6% of patients in UFH and 7.7% in enoxaparin (HR 0.72; 95% CI 0.53–0.99; p = 0.04).
• Combined rate of TIMI major, minor or loss no site bleeding was 1.3% in UFH and 1.8% enoxaparin group (p = ns).
• Conclusion: When a conservative approach to catheterisation and PCI was planned for ACS patients receiving tirofiban and aspirin, enoxaparin was associated with superior efficacy and similar bleeding vs UFH.
De Lemos et al: European Heart Journal (2004) 25, 1688–1694

Primary End point:Composite of Outcome of death, MI or refractory ischemia
10.6%
7.7%
(HR 0.72; 95% CI 0.53–0.99; p = 0.04)

Enoxaparin and Thrombolysis Reperfusion for Acute Myocardial Infarction Treatment (ExTRACT)– Thrombolysis in Myocardial
Infarction (TIMI) 25 Study• Aim: Designed to compare enoxaparin and UFH as adjunctive therapy for
fibrinolysis (streptokinase, tenecteplase, alteplase or reteplase) in STEMI.
• International randomized trial (1:1 ratio) included 20,506 patients (2002-2005).
• Underwent fibrinolysis & receive enoxaparin throughout the index hospitalization or weight based UFH for at least 48 hours.
• Eligibility: ≥ 18 years of age with STEMI within 6 hours before randomization or had new onset LBBB.
• Exclusion: cardiogenic shock, pericarditis, symptoms of aortic dissection, contraindications to fibrinolysis, receipt of a LMWH within 8 hrs, renal insufficiency, life expectancy ˂12 months.
Elliott M. Antman et alk. N Engl J Med 2006;354:1477-88.

A. Primary end point (death or nonfatal MI) at 30 days Significantly lower in the enoxaparin group than in the UFH group (9.9 % vs. 12.0 %, P<0.001)
B. Secondary end point (death, nonfatal MI or urgent revascularization) at 30 days Significantly lower in the enoxaparin group than in the UFH group (11.7 % vs. 14.5 %, P<0.001)

Conclusion: In patients receiving fibrinolysis for STEMI, treatment with enoxaparin throughout the index hospitalization is superior to treatment with UFH for 48 hours but is associated with an increase in major bleeding episodes.
Increase in major bleed in enoxap.

Efficacy and safety of enoxaparin compared with UFH across the acute coronary syndrome spectrum: a meta-analysis
• Aim: To determine whether enoxaparin remains favorable when compared with UFH among patients with ACS.
• Meta-analysis of 12 randomized trials of enoxaparin vs. UFH in STEMI or NSTEMI ACS (n= 49,088). [STEMI n=27,131]
• Female: 34-36%.
• Net clinical endpoint was defined as death, MI or major bleeding by 30 days.
Murphy et al. European Heart Journal (2007) 28, 2077–2086

Results
(favour of enoxaparin)
(favour of enoxaparin in STEMI, not in NSTEMI)
Enoxaparin v/s UFH for the comparison of death or non-fatal MI
Enoxaparin vs. UFH for comparison of death, non-fatal MI or non-fatal major bleed (Net clinical endpoint)
Black square size of reflects the statistical weight of a trial in calculating the OR.

Enoxaparin vs. UFH for the comparison of major bleed
Conclusion: When compared with UFH, enoxaparin was associated with superior efficacy as adjunctive antithrombin therapy across the ACS spectrum. Although bleeding was increased with enoxaparin, this increase was offset by a reduction in death or MI. The net clinical benefit in favour of enoxaparin was evident among the STEMI population and was neutral among the NSTE ACS population.
Bleeding was increased with enoxaparin
Safety outcome:

SYNERGY Trial (Superior Yield of the New Strategy of Enoxaparin,Revascularization and Glycoprotein IIb/IIIa Inhibitors)
• Aim: To compare outcomes of pts treated with enoxaparin vs UFH in NSTEMI-ACS at high risk for ischemic cardiac complications managed with an early invasive approach.
• Prospective, randomized, open-label, multicenter, international trial (2001-2003) n=10027 (Enoxaparin:4993, UFH:4985)
• Primary efficacy outcome: Composite clinical end point of all cause death or nonfatal MI during the first 30 days after randomization.
• Primary safety outcome was major bleeding or stroke.
KennethW et al. JAMA. 2004;292:45-54

Conclusion: Enoxaparin was not superior to UFH but was noninferiorfor the treatment of high-risk patients with NSTEMI- ACS.
Enoxaparin is a safe and effective alternative to UFH and the advantages of convenience should be balanced with the modest excess of major bleeding.
NS
S↑

ATOLL trial (Acute STEMI Treated With Primary PCI and Intravenous Enoxaparin or UFH to Lower Ischemic and Bleeding Events at Short and Long-Term Follow-up)
• Aim: To compared UFH treatment with i/v enoxaparin (0.5 mg/kg) in STEMI pts undergoing primary PCI for STEMI.
• Randomized, open-label, international trial, n=910 (Enoxaparin :450, UFH 460).
Montalescot G et al. Lancet 2011; 378:693-703

STEMIplanned for 1° PCI
ENOXAPARIN IV0.5 mg/kg
(± GP IIb/IIIa inhibitor)
UFH IV 50 – 70 IU/kg if GP IIb/IIIa
70 – 100 IU/kg if no GP IIb/IIIaDose adjusted to ACT
Randomization (N = 850)
1° PCI and stenting
1° EP: Death, complication of MI, procedure failure or non-CABG major bleeding at 30 days
Main 2° EP: Death, MI, refractory ischemia, urgent revasc.
6-month follow-upPatients who have already received UFH or LMWH or any other anticoagulant are excluded.
All concomitant drugs accepted, except lytics; cross-over to other anticoagulant NOT accepted.
ATOLL: Study Design

Results• Primary endpoint occurred in 126 (28%) with enoxaparin versus 155 (34%) on
UFH (relative risk [RR] 0.83, 95% CI 0.68—1.01, p=0.06).
• Incidence of death (enoxaparin, 17 [4%] vs heparin, 29 [6%] patients; p=0.08), complication of MI (20 [4%] vs 29 [6%]; p=0.21), procedure failure (100 [26%] vs 109 [28%]; p=0.61) were decreased but major bleeding (20 [5%] vs 22 [5%]; p=0.79) did not differ between groups.
• Enoxaparin resulted in a significantly reduced rate of the main secondary endpoint (30 [7%] vs 52 [11%] pts; RR 0.59, 95% CI 0.38—0.91, p=0.015).
• Death, complication of MI or major bleeding (46 [10%] vs 69 [15%] pts; p=0.03); death or complication of MI (35 [8%] vs 57 [12%]; p=0.02) and death, recurrent MI or urgent revascularisation (23 [5%] vs 39 [8%]; p=0.04) were all reduced with enoxaparin.
Conclusion: IV enoxaparin compared with UFH significantly reduced clinical ischemic outcomes without differences in bleeding and procedural success. Therefore, enoxaparin provided an improvement in net clinical benefit in patients undergoing primary PCI.

Fondaparinux (Indirect Xa inhibitor) OASIS-5 trial (Fifth Organization to Assess Strategies in Acute Ischemic Syndromes)
Aim: whether fondaparinux would preserve the anti-ischemic benefits of enoxaparin while reducing bleeding.
Yusuf S et al. N Engl J Med 2006;354:1464-76.




(PCI done in 39.5 percent in the fondaparinux group and 39.5 percent in enoxaparin group)
Conclusion: Fondaparinux is similar to enoxaparin in reducing the risk of ischemic events at 9 days, but it substantially reduces major bleeding and improves long term mortality and morbidity.

12,000 Patients with STEMI < 12 h of symptom onsetInclusion: ST 2 mm prec leads or 1 mm limb leads
Exclusion: Contra-ind. for anticoagulant, INR>1.8, pregnancy, ICH<12 mo.
12,000 Patients with STEMI < 12 h of symptom onsetInclusion: ST 2 mm prec leads or 1 mm limb leads
Exclusion: Contra-ind. for anticoagulant, INR>1.8, pregnancy, ICH<12 mo.
UFH not indicatedUFH not indicated
OASIS 6: Randomized, Double Blind (2003-2006)
Lytics (SK, TPA, TNK, RPA), Primary PCI or no reperfusion
StratificationStratification
UFH indicatedUFH indicated
Randomization Randomization
Fondaparinux2.5 mg Placebo
Fondaparinux2.5 mg UFH
Yusuf S et al. JAMA. 2006;295:1519-1530
Aim: To evaluate the effect of fondaparinux in STEMI pts.


Conclusion: In patients with STEMI, particularly those not undergoing PCI, fondaparinux significantly reduces mortality and reinfarction without increasing bleeding and strokes.

APPRAISE-2 (Apixaban for Prevention of Acute Ischemic Events 2 trial)
• Aim: To determine benefit of apixaban (oral direct factor Xa inhibitor) in reducing ischemic events in high risk patients with an ACS.
• Randomized, double-blind, placebo-controlled clinical trial (n=7392).
• Treated with apixaban 5 mg twice daily v/s placebo in addition to standard antiplatelet therapy.
• Inclusion criteria: ACS (MI with or without ST-segment elevation or UA) within the previous 7 days with at least two of following: ≥65 years DM MI ≤5 years CVD PVD Clinical HF or a LVEF ≤40% Creatinine clearance ≤ 60 ml per minute and No revascularization after the index event
Alexander J H et al. N Engl J Med 2011;365:699-708.

Results: Trial was terminated prematurely after recruitment(increase in major bleeding events with apixaban in the absence of a counterbalancing
reduction in recurrent ischemic events)
A greater number of intracranial and fatal bleeding events occurred with apixaban than with placebo.

Conclusions:Addition of apixaban 5 mg 1BD to antiplatelet therapy in high risk pts after ACS increases the number of major bleeding events without a significant reduction in recurrent ischemic events.

ATLAS ACS 2–TIMI 51 (Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Standard Therapy in Subjects with Acute Coronary Syndrome–Thrombolysis in Myocardial Infarction 51)• Aim: to evaluate twice daily rivaroxaban at doses of 2.5 mg and 5 mg as
adjunctive therapy in patients with a recent ACS (within 7 days), with the aim of determining a clinically effective low-dose regimen.
• Double-blind, placebo-controlled trial (n= 15,526)
• Included patients ≥18 years of age with STE/NSTE/UA.
• Divided in 1:1:1 fashion to twice daily administration of either 2.5 mg or 5.0 mg of rivaroxaban or placebo with a maximum follow-up of 31 months.
• Primary efficacy end point: composite of death from cardiovascular causes, MI or stroke (ischemic, hemorrhagic, or stroke of uncertain cause).
Mega JL et al. N Engl J Med 2012;366:9-19

Results: Cumulative Incidence of the Primary Efficacy End Point
Rivaroxaban significantly reduced primary efficacy end point as compared withplacebo, with respective rates of 8.9% and 10.7%

Cumulative Incidence of Efficacy End Points, According to Rivaroxaban Dose
(9.1% vs. 10.7%, P = 0.02) (8.8% vs. 10.7%, P = 0.03)
(2.7% vs. 4.1%, P = 0.002)(Not seen)

Conclusions:In patients with a recent ACS, rivaroxaban reduces the risk of composite end
point of death from cardiovascular causes, MI or
stroke.
Rivaroxaban increases the risk of major bleeding and intracranial hemorrhage but not the risk of fatal
bleeding.

DabigatranRE-DEEM trial (Randomised Dabigatran Etexilate Dose Finding Study In Pts With ACS Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin And Clopidogrel)
• Aim: To evaluate safety & indicators of efficacy of Dabigatran after recent ACS (≤14 days) in pts who remains at risk of recurrent ischemic events, despite contemporary treatment including aspirin and clopidogrel.
• Double-blind, placebo-controlled, dose-escalation trial (n=1861, 161 centres)
• ST-elevation (60%) or non-ST-elevation (40%) MI.
• 99.2% on dual antiplatelet treatment.
Oldgren J et al. European Heart Journal :accepted 22 March 2011

Primary outcome: Composite of major or clinically relevant minor bleeding during the 6-month treatment period

Require atleast one of following:

“Early decrease in coagulation activity after myocardial infarction is associated with lower risk of new ischemic events:” observations from the ESTEEM Trial. Eur Heart J 2007; 28:692–698.
HR 1.77 (95% CI: 0.70-4.50)
HR 2.17 (0.88, 5.31)
HR 4.27 (1.86, 9.81)
3.92 (1.72, 8.95)
37%45%
Conclusion:Dabigatran in addition to dual antiplatelet therapy was associated with a dose-dependent increase in bleeding events (though low overall bleeding rate i.e. < 1% absolute increase in major/severe bleeds with dabigatran 110 - 150 mg b.d. ) and significantly reduced coagulation activity in patients with a recent myocardial infarction.
Primary outcomes differed significantly (P =0.001) for the 110 and 150 mg dabigatran
Lower with higher dose only

BIVALIRUDINBAT [HIRULOG (BIVALIRUDIN) ANGIOPLASTY STUDY]
• Aim: To evaluate whether ischemic or hemorrhagic complications can be decreased with use of bivalirudin v/s UFH during and after coronary angioplasty.
• Double-blind, randomized trial (n=4098)
• Patients undergoing angioplasty for unstable or postinfarction angina.
• Pt received either heparin or bivalirudin immediately before angioplasty.
• Primary end point was death in the hospital, MI, abrupt vessel closure or rapid clinical deterioration of cardiac origin.
JOHN A. BITTL et al N Engl J Med 1995;333:764-9.

• Results: Overall bivalirudin did not significantly reduce incidence of primary end point (11.4%, vs. 12.2 % for heparin) but did result in lower incidence of bleeding (3.8%vs. 9.8 %, P ˂0.001).
• Patients with postinfarction angina, bivalirudin therapy resulted in a lower incidence of primary end point (9.1%vs. 14.2 %, p˂0.04) and a lower incidence of bleeding (3.0 % vs. 11.1 %, P˂0.001).
• Conclusion: Bivalirudin was at least as effective as high-dose heparin in preventing ischemic complications in patients who underwent angioplasty for unstable angina and it carried a lower risk of bleeding. Bivalirudin as compared with heparin, reduced the risk of immediate ischemic complications in patients with postinfarction angina but this difference was no longer apparent after six months.

REPLACE-1 & 2 (Randomized Evaluation of PCI Linking Angiomax to Reduced Clinical Events)
• Aim: To determine whether the efficacy of bivalirudin with that of heparin plus Gp IIb/IIIa blockade undergoing urgent or elective PCI.
• Randomized, double-blind trial conducted among 6010 patients (2001-2002).
Lincoff AM et al:JAMA. 2004 Aug 11;292(6):696-703.

Trial Design
Bivalirudin vs Heparin + GP IIb/IIIa During PCIN = 6010 Patients: Urgent or Elective PCIRandomization: double blind, triple dummy
Heparin65 U/kg initial bolus
Planned GP IIb/IIIa(abciximab or eptifibatide)
Bivalirudin0.75 mg/kg initial bolus,
1.75 mg/kg-hr during PCI
Provisional GP IIb/IIIa(abciximab or eptifibatide)
Abciximab: 0.25 mg/kg bolus, 0.125 mg/kg-min (max 10 mg/min) x 12 hrs
Eptifibatide: 180 mg/kg double bolus, 2.0 mg/kg-min x 18-24 hrs
“Quadruple Endpoint” at 30 Days(Death, MI, urgent revascularisation, major bleeding)
target ACT> 225 sec

Procedural DataHeparin +
Bivalirudin GP IIb/IIIa(N = 2994) (N = 3008)
Indication for PCI (%) unstable angina prior 48 hrs 421 (14.3) 434 (14.7) unstable angina > 48 hrs 599 (20.3) 619 (21.0) MI prior 7 days 248 (8.3) 248 (8.2) stable angina 770 (26.1) 722 (24.4) positive stress test 716 (24.3) 738 (25.0) other 196 (6.6) 192 (6.5)
PCI Type (%) stent 85.1 85.7 PTCA only 7.9 6.9 atherectomy 3.8 3.8
Multi-vessel PCI (%) 16.6 14.9
Bypass graft PCI (%) 5.8 6.2

Results at 30 days
30 days results showed bivalirudin was noninferior to heparin plus planned Gp IIb/IIIa blockade in the prevention of acute ischemic end points and was associated with significantly less bleeding by 30 days after PCI.

Results at 6 months

Results at 12 months
Conclusion: Short & Long-term clinical outcome with bivalirudin and provisional Gp IIb/IIIa blockade is comparable with that of heparin plus planned Gp IIb/IIIa inhibition during contemporary PCI.

ACUITY trial (Bivalirudin in patients with acute coronary syndromes undergoing percutaneous coronary intervention)
• Aim: To determine economic impact of several anticoagulation strategies [heparin (UFH or enoxaparin) + GPI v/s bivalirudin+ GPI v/s bivalirudin monotherapy) for moderate & high risk NSTE-ACS patients managed invasively.
• Prospective, open-label, randomized, multicenter trial.
• 7789 underwent percutaneous coronary intervention after angiography.
• Primary 30-day endpoints of composite ischaemia of death, myocardial infarction or unplanned revascularisation for ischaemia.
Duane S. Pinto et al. Acute Catheterization and Urgent Intervention Triage Strategy J am Coll Cardiol 2008;52:1758–68, The Lancet, Volume 369, Issue 9565, Pages 907 - 919, 17 March 2007.

Study Design – Patient FlowStudy Design – Patient Flow
UFH/Enox+ GP IIb/IIIa
(N=4,603)
Bivalirudin+ GP IIb/IIIa
(N=4,604)
BivalirudinAlone
(N=4,612)
R*
Moderate-high risk unstable angina or NSTEMI undergoing an invasive strategy
Moderate-high risk unstable angina or NSTEMI undergoing an invasive strategy
GPI upstream (N=2294)
GPI CCL for PCI (N=2309)
GPI upstream (N=2311)
GPI CCL for PCI (N=2293)
Aspirin in allClopidogrel
dosing and timingper local practice
Aspirin in allClopidogrel
dosing and timingper local practice
*Stratified by pre-angiography thienopyridine use or administration*Stratified by pre-angiography thienopyridine use or administration
Moderate-high risk
ACS(N=13,819)
This presentation reflects the views of the presenter and does not necessarily reflect the views of the American College of Cardiology. Content Distributed by Cardiosource.

Major Entry CriteriaMajor Entry Criteria
Age ≥18 years Chest pain ≥10’ within 24h At least one of:
New ST depression or transient ST elevation ≥1 mm
Troponin I, T, or CKMB Documented CAD All other 4 TIMI risk criteria- Age ≥65 years- Aspirin within 7 days- ≥2 angina episodes w/i 24h- ≥3 cardiac risk factors
Written informed consent
Age ≥18 years Chest pain ≥10’ within 24h At least one of:
New ST depression or transient ST elevation ≥1 mm
Troponin I, T, or CKMB Documented CAD All other 4 TIMI risk criteria- Age ≥65 years- Aspirin within 7 days- ≥2 angina episodes w/i 24h- ≥3 cardiac risk factors
Written informed consent
Inclusion CriteriaInclusion Criteria Exclusion CriteriaExclusion Criteria No angiography within 72h Acute STEMI or shock Bleeding diathesis or major
bleed within 2 weeks Platelet count ≤100,000/mm3
INR >1.5 control CrCl ≤30 ml/min Abcx or ≥2 prior LMWH doses
Prior UFH, LMWH (1 dose), eptifibatide and tirofiban were allowed
Allergy to drugs, contrast
No angiography within 72h Acute STEMI or shock Bleeding diathesis or major
bleed within 2 weeks Platelet count ≤100,000/mm3
INR >1.5 control CrCl ≤30 ml/min Abcx or ≥2 prior LMWH doses
Prior UFH, LMWH (1 dose), eptifibatide and tirofiban were allowed
Allergy to drugs, contrast
Moderate-high risk unstable angina or NSTEMIModerate-high risk unstable angina or NSTEMI
ACUITY Design. Stone GW et al. AHJ 2004;148:764–75ACUITY Design. Stone GW et al. AHJ 2004;148:764–75This presentation reflects the views of the presenter and does not necessarily reflect the views of the
American College of Cardiology. Content Distributed by Cardiosource.


Clinical ImplicationsClinical Implications
In patients with moderate-high risk ACS undergoing an early invasive strategy with the use of GP IIb/IIIa inhibitors
Bivalirudin is an acceptable substitute for either unfractionated heparin or enoxaparin
However, compared to either UFH/enoxaparin with GP IIb/IIIa inhibition or bivalirudin with GP IIb/IIIa inhibition
A bivalirudin alone strategy results in significantly greater net clinical benefit and enhanced survival free from adverse events at 30 days
In patients with moderate-high risk ACS undergoing an early invasive strategy with the use of GP IIb/IIIa inhibitors
Bivalirudin is an acceptable substitute for either unfractionated heparin or enoxaparin
However, compared to either UFH/enoxaparin with GP IIb/IIIa inhibition or bivalirudin with GP IIb/IIIa inhibition
A bivalirudin alone strategy results in significantly greater net clinical benefit and enhanced survival free from adverse events at 30 days
This presentation reflects the views of the presenter and does not necessarily reflect the views of the American College of Cardiology. Content Distributed by Cardiosource.

ISAR-REACT 3 Trial (Intracoronary Stenting and Antithrombotic Regimen: Rapid Early Action for Coronary Treatment)
• Aim: To know whether bivalirudin is superior to UFH in pts with stable or unstable angina who undergo PCI after pretreatment with clopidogrel 600 mg at least 2 hrs before procedure.
• Double-blind, randomized , n=4570 (bivalirudin:2289, UFH:2281)
• Primary end point: Composite of death, MI, TVR due to myocardial ischemia within 30 days after randomization or major bleeding during the index hospitalization.
• Secondary end point: ischemic end point was the composite of death, MI or urgent TVR.
Kastrati A et al. N Engl J Med 2008;359:688-96.

(P = 0.008)
Conclusion: In patients with stable and unstable angina who underwent PCI after pretreatment with clopidogrel, bivalirudin did not provide a net clinical benefit (i.e. it did not reduce the incidence of the composite end point of death, MI, urgent TVR or major bleeding) as compared with unfractionated heparin, but it did significantly reduce the incidence of major bleeding.

ISAR-REACT 4 Trial (Intracoronary Stenting and AntithromboticRegimen: Rapid Early Action for Coronary Treatment 4)
• Aim: To compare UFH + abciximab with bivalirudin in patients with NSTEMI undergoing PCI (within 24 hours).
• Randomized, double blinded, n= 1721 (861 & 860) age: 19 to 80 yrs.
• All the patients in the trial were given 325 to 500 mg of aspirin and 600 mg of clopidogrel.
• Primary end point: Composite end point of death, large recurrent MI, urgent TVR or major bleeding within 30 days.
• Secondary end point: composite of death, any recurrent MI or urgent TVR (efficacy end point) and major bleeding (safety end point) within 30 days.
Kastrati A et al. N Engl J Med 2011;365:1980-1989

4.6%
2.6%
Conclusion: UFH + Abciximab as compared with bivalirudin, failed to reduce the rate of primary end point and increased the risk of bleeding among patients with NSTEMI who were undergoing PCI.

HORIZONS-AMI Trial (Harmonizing Outcomes with Revascularizationand Stents in Acute Myocardial Infarction)
• Aim: To compare UFH + glycoprotein IIb/IIIa inhibitor with bivalirudin alone in patients with STEMI undergoing PCI (within 12 hrs).
• Randomized, double blinded, n= 3602 (861 & 860) age: ≥18 yrs.
• All the patients in the trial were given 325 to 500 mg of aspirin and 600 mg of clopidogrel.
• Primary end points: Major bleeding and combined adverse clinical events within 30 days
Stone GW et al. N Engl J Med 2008;358:2218-2230

Conclusion:In patients with STEMI who are undergoingprimary PCI, anticoagulation with bivalirudin alone, as compared with heparin plus glycoprotein IIb/IIIa inhibitors results in significantly reduced 30-day rates of major bleeding and net adverse clinical events.
Though, There was an increased risk of acute stent thrombosis within 24 hours in bivalirudin group but no significant increase was present by 30 days
significantly lower significantly lower
significantly lower

Current Guidelines2013 ACCF/AHA Guideline for the Management of
ST-Elevation Myocardial Infarction
Anticoagulant Therapy to Support Primary PCICLASS IFor pts with STEMI undergoing primary PCI, following supportive anticoagulant regimens are recommended:
a. UFH with additional boluses administered as needed to maintain therapeutic activated clotting time levels, taking into account whether a GP IIb/IIIa receptor antagonist has been administered (Level of Evidence: C) or
b. Bivalirudin with or without prior treatment with UFH. (Level of Evidence: B)
CLASS IIaIn pts with STEMI undergoing PCI who are at high risk of bleeding, it is reasonable to use bivalirudin monotherapy in preference to the combination of UFH and a GP IIb/IIIa receptor antagonist. (Level of Evidence: B)
CLASS III: HARMFondaparinux should not be used as the sole anticoagulant to support primary PCI because of the risk of catheter thrombosis. (Level of Evidence: B)
O’Gara PT et al. J Am Coll Cardiol 2013;61:e78 –140.

ADJUNCTIVE ANTICOAGULANT THERAPY WITH FIBRINOLYSIS:
CLASS IPs with STEMI undergoing reperfusion with fibrinolytic therapy should receive anticoagulant therapy for a minimum of 48 hours and preferably for the duration of index hospitalization up to 8 days or until revascularization if performed. (Level of Evidence: A)
Recommended regimens include:a. UFH administered as a weight-adjusted intravenous bolus and infusion to obtain an activated
partial thromboplastin time of 1.5 to 2.0 times control, for 48 hours or until revascularization. (Level of Evidence: C)
b. Enoxaparin administered according to age, weight and creatinine clearance, given as an intravenous bolus, followed in 15 minutes by subcutaneous injection for the duration of the index hospitalization, up to 8 days or until revascularization. (Level of Evidence: A) or
c. Fondaparinux administered with initial intravenous dose, followed in 24 hours by daily subcutaneous injections if the estimated creatinine clearance is greater than 30 mL/min, for the duration of the index hospitalization, up to 8 days or until revascularization.(Level of Evidence: B)
O’Gara PT et al. J Am Coll Cardiol 2013;61:e78 –140.

Current Guidelines2012 ACCF/AHA Focused Update of the Guideline for the Management of Patients With Unstable Angina/
Non–ST-Elevation Myocardial Infarction (Updating the 2007 Guideline and Replacing the 2011 Focused Update)
CLASS I:With initial invasive strategy: Anticoagulation with UFH, enoxaparin, bivalirudin or fondaparinux.
PCI planned: Discontinue anticoagulation after PCI in uncomplicated cases.CABG planned:
1. Continue UFH (Level of Evidence: B)
2. Discontinue enoxaparin 12 to 24 hours before CABG and dose with UFH per institutional practice. (Level of Evidence: B)
3. Discontinue fondaparinux 24 hours before CABG and dose with UFH per institutional practice. (Level of Evidence: B)
4. Discontinue bivalirudin 3 hours before CABG and dose with UFH per institutional practice. (Level of Evidence: B)
Jneid H et al. J Am Coll Cardiol 2012;60:645– 81

Medical therapy planned after established CAD on CAG, anticoagulant therapy should be managed as follows:
1. Continue IV UFH for at least 48 hours or until discharge if given before diagnostic angiography. (Level of Evidence: A)
2. Continue enoxaparin for duration of hospitalization, up to 8 days, if given before diagnostic angiography. (Level of Evidence: A)
3. Continue fondaparinux for duration of hospitalization, up to 8 days, if given before diagnostic angiography. (Level of Evidence: B)
4. Either discontinue bivalirudin or continue at a dose of 0.25 mg/kg per hour for up to 72 hours at the physician’s discretion if given before diagnostic angiography. (Level of Evidence: B)
Initial medical therapy planned:• Continue UFH for 48 hours (Level of Evidence: A) or • Administer enoxaparin (Level of Evidence: A) or• Fondaparinux (Level of Evidence: B) for the duration of hospitalization, up to 8
days and then discontinue anticoagulant therapy.

How to manage antithrombotic treatment during PCI in pts on long term anticoagulation: “to bridge” or “not to bridge”?
• 5% of pts undergoing PCI is on long term OAC (underlying AF, PE, HF, Prosthetic valve).
• Represent substantial challenge to operator to balance the risk of periprocedural hemorrhage, thrombotic complications & thromboembolism.
• Two main options:– Most common is to discontinue OAC few days prior to PCI till INR ˂1.5 and if pt is
considered for higher risk for thromboembolism, give bridging therapy (UFH/LMWH).
– Emerging option is to continue therapeutic OAC throughout periprocedural period with no interruptions or heparin bridging.
Review article, Airaksinrn juhani K.E. et al. Eurointervention 2010;6:520-526


THANKS