ANTICOAGULATION ISSUES In Geriatric Population Ann McBride, M.D. UW Anticoagulation Service.
39
ANTICOAGULATION ISSUES In Geriatric Population Ann McBride, M.D. Ann McBride, M.D. UW Anticoagulation UW Anticoagulation Service Service
-
Upload
mae-dennis -
Category
Documents
-
view
219 -
download
0
Transcript of ANTICOAGULATION ISSUES In Geriatric Population Ann McBride, M.D. UW Anticoagulation Service.
ANTICOAGULATION ISSUESIn Geriatric Population
Ann McBride, M.D.Ann McBride, M.D.
UW Anticoagulation ServiceUW Anticoagulation Service
• No financial disclosuresNo financial disclosures
• Underuse of Anticoagulation for Atrial Underuse of Anticoagulation for Atrial FibrillationFibrillation– Balance of Stroke vs. Bleeding RisksBalance of Stroke vs. Bleeding Risks– AlternativesAlternatives
• Warfarin Initiation and MaintenanceWarfarin Initiation and Maintenance• Bridging TherapyBridging Therapy
Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy:Evidence Based Guidelines
• CHEST Supplement, September 2004CHEST Supplement, September 2004
• Overall CVA Risk for AF 4.5% per yearOverall CVA Risk for AF 4.5% per year
• Risk increases with AgeRisk increases with Age– 1.5% per year 50-59 yo1.5% per year 50-59 yo– 10% per year 80-89 yo10% per year 80-89 yo– 20% per year 90 yo20% per year 90 yo
CHAD
S2
Gage et al, Circulation 2004
CCongestive Heart Failureongestive Heart Failure
HHypertensionypertension
-Treated; untreated >140/90 mmHg-Treated; untreated >140/90 mmHg
AAgege
-Older than 75-Older than 75
DDiabetesiabetes
SStroke - 2troke - 2
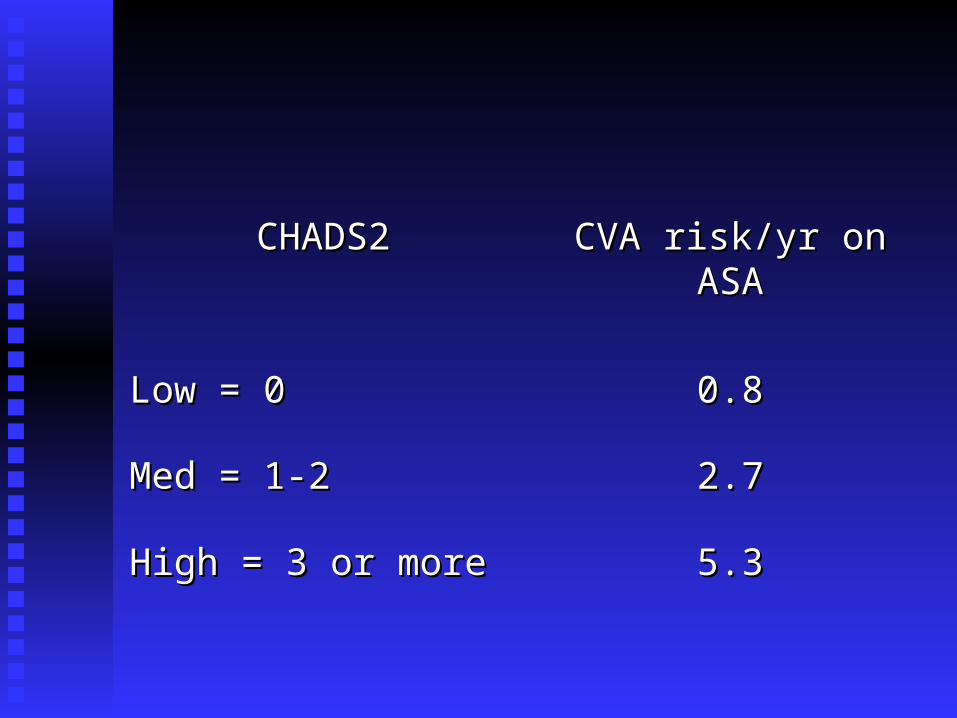
CHADS2CHADS2 CVA risk/yr on ASACVA risk/yr on ASA
Low = 0Low = 0 0.80.8
Med = 1-2Med = 1-2 2.72.7
High = 3 or moreHigh = 3 or more 5.35.3
• Adjusted dose warfarin—Target INR 2.5—Adjusted dose warfarin—Target INR 2.5—reduces CVA risk 60%reduces CVA risk 60%
• ASA reduces CVA risk 20%ASA reduces CVA risk 20%
Warfarin Also Decreases Severity
• INR 2.0-3.0INR 2.0-3.0
• Associated with reduced severity of strokeAssociated with reduced severity of stroke
• Greater likelihood of survivalGreater likelihood of survival
INR Intensity & CVA Severity
• 596 strokes/13,559 pts w/ NVAF596 strokes/13,559 pts w/ NVAF– 32% warfarin32% warfarin– 27% ASA27% ASA– 42% neither42% neither
Hylek, et al, N Engl J Med 2003
1.1. Risk for CVA sharply increased INR < 2Risk for CVA sharply increased INR < 2
2.2. CVA severity & fatality CVA severity & fatality
with INR 1.5 – 1.9 ~ INR < 1.5with INR 1.5 – 1.9 ~ INR < 1.5
3.3. With INR 2-3, CVA more likely to be With INR 2-3, CVA more likely to be “minor”“minor”
Bleeding Risk
• Warfarin increases risk of major Warfarin increases risk of major hemorrhagehemorrhage
1.7 x risk associated with ASA1.7 x risk associated with ASA

Bleeding Risk
• 65 yo and older65 yo and older• Hx of noncardioembolic CVAHx of noncardioembolic CVA• Hx of GI BleedHx of GI Bleed• > 1 Comorbid Conditions> 1 Comorbid Conditions
– Recent MIRecent MI– Hct less than 30Hct less than 30– Creatinine > 1.5Creatinine > 1.5– DiabetesDiabetes
Beyth et al. Am J Med 1998
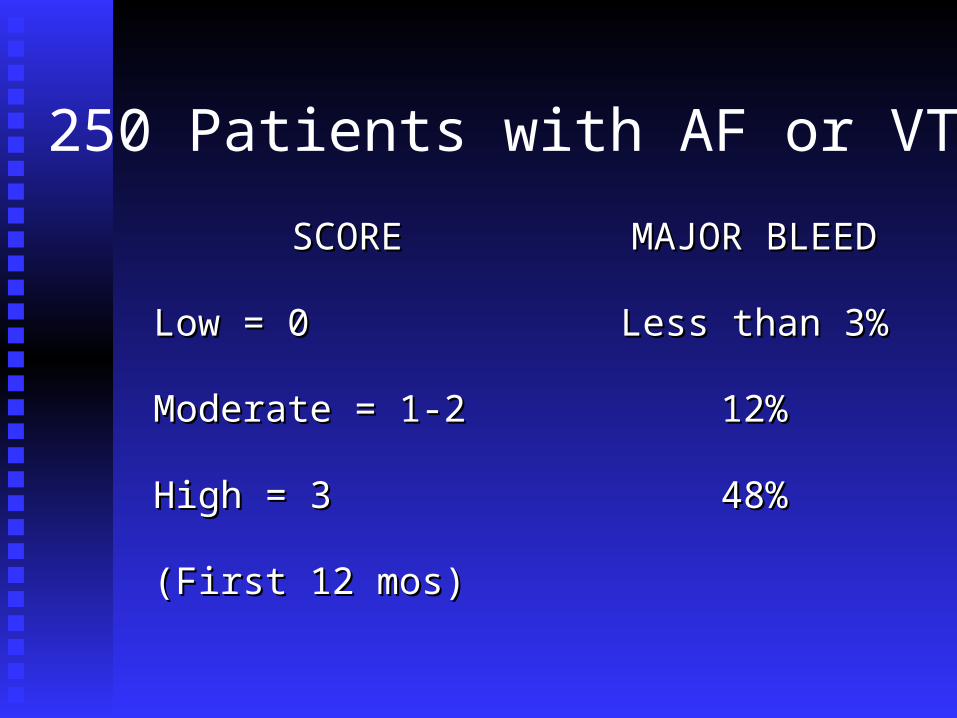
SCORESCORE MAJOR BLEEDMAJOR BLEED
Low = 0Low = 0 Less than 3%Less than 3%
Moderate = 1-2Moderate = 1-2 12%12%
High = 3High = 3 48%48%
(First 12 mos)(First 12 mos)
250 Patients with AF or VTE
• Overall incidence of major bleed 6.5%Overall incidence of major bleed 6.5%
• Greatest risk for bleed first 30 daysGreatest risk for bleed first 30 days
• Most were avoidable maintaining Most were avoidable maintaining therapeutic INR range and avoiding therapeutic INR range and avoiding NSAIDsNSAIDs
Other Risk Factors Excess Warfarin Anticoagulation
• APAP intake 9100 mg/wk or moreAPAP intake 9100 mg/wk or more• New medication known to increase warfarin effectNew medication known to increase warfarin effect• (Note: antibiotic, PPI, amiodarone, SSRI)(Note: antibiotic, PPI, amiodarone, SSRI)• Bleed vs. CVA riskBleed vs. CVA risk• Recent diarrheal illnessRecent diarrheal illness• Decreased oral intakeDecreased oral intake• Incorrectly taking higher dose of warfarin than Incorrectly taking higher dose of warfarin than
prescribedprescribed
Hylek et al. JAMA 1998
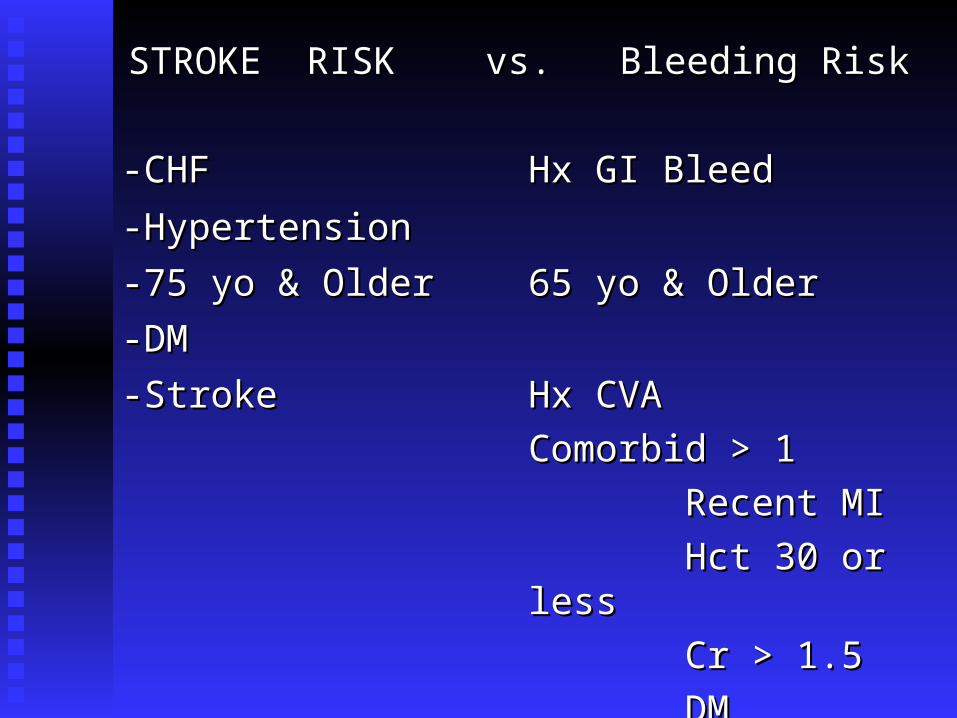
STROKE RISK vs. Bleeding RiskSTROKE RISK vs. Bleeding Risk
-CHF-CHF Hx GI BleedHx GI Bleed
-Hypertension-Hypertension
-75 yo & Older-75 yo & Older 65 yo & Older65 yo & Older
-DM-DM
-Stroke-Stroke Hx CVAHx CVA
Comorbid > 1Comorbid > 1
Recent MIRecent MI
Hct 30 or lessHct 30 or less
Cr > 1.5Cr > 1.5
DMDM
• 145 pts w/ ICH on warfarin145 pts w/ ICH on warfarin
• 870 pts on warfarin w/o ICH870 pts on warfarin w/o ICH
• Increasing Age (especially > 85)Increasing Age (especially > 85)
• Increasing INR (especially > 3.5)Increasing INR (especially > 3.5)
Fang et al. Annals of Internal Medicine 2004
• Risk of ICH was NOT lower in elderly pts Risk of ICH was NOT lower in elderly pts w/ AF when INR < 2.0 compared to INR w/ AF when INR < 2.0 compared to INR 2.0-3.02.0-3.0
• EVEN FOR PTS OLDER THAN 75EVEN FOR PTS OLDER THAN 75
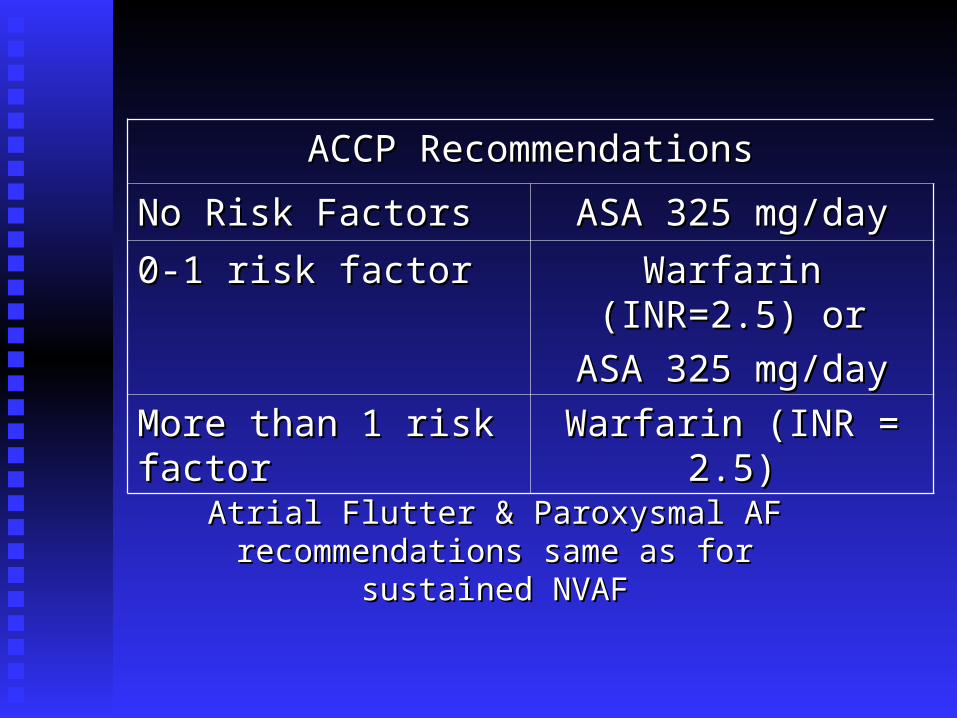
ACCP RecommendationsACCP Recommendations
No Risk FactorsNo Risk Factors ASA 325 mg/dayASA 325 mg/day
0-1 risk factor0-1 risk factor Warfarin (INR=2.5) orWarfarin (INR=2.5) or
ASA 325 mg/dayASA 325 mg/day
More than 1 risk factorMore than 1 risk factor Warfarin (INR = 2.5)Warfarin (INR = 2.5)
Atrial Flutter & Paroxysmal AF recommendations Atrial Flutter & Paroxysmal AF recommendations same as for sustained NVAFsame as for sustained NVAF
Bottom Line
• Stroke RiskStroke Risk• Bleeding RiskBleeding Risk• Patient Functional & Cognitive Status Patient Functional & Cognitive Status • incl. falls riskincl. falls risk
Patient CompliancePatient Compliance• Patient PreferencePatient Preference
Suggest:
1.1. INR 2.5 (2.0 - 3.0)INR 2.5 (2.0 - 3.0)
2.2. Attention to risk factors for bleeding Attention to risk factors for bleeding If bleed occurs, target INR 2.2 (1.8 - 2.5)If bleed occurs, target INR 2.2 (1.8 - 2.5)
3.3. More frequent monitoringMore frequent monitoring
4.4. Attention to Rx med or OTC med changeAttention to Rx med or OTC med change
• Role of Anticoagulation Clinic Role of Anticoagulation Clinic

Patient Sample #1
Initiating Warfarin
ElderlyElderly
FrailFrail
MalnourishedMalnourished
CHFCHF
Liver DiseaseLiver Disease
Concurrent MedicationsConcurrent Medications
(cytochrome P450 isoenzymes mutation)(cytochrome P450 isoenzymes mutation)
Lower Dose In Elderly
• “…“…starting dose of less than 5 mg might be starting dose of less than 5 mg might be appropriate in the elderly…”appropriate in the elderly…”
• Nomograms available, but few geriatric Nomograms available, but few geriatric patients representedpatients represented
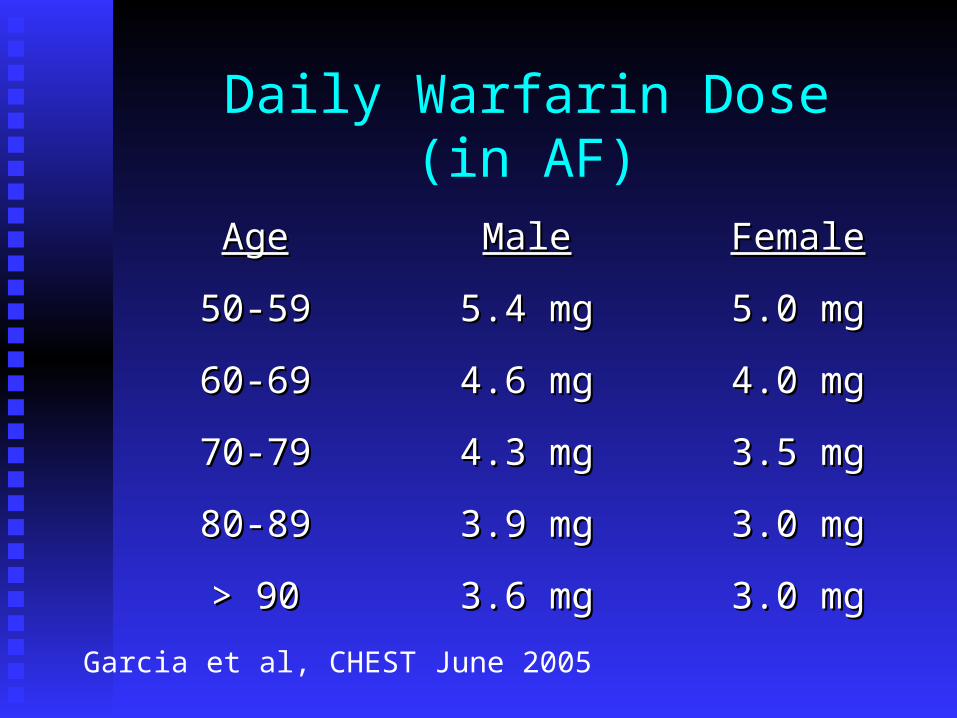
Daily Warfarin Dose(in AF)
AgeAge MaleMale FemaleFemale
50-5950-59 5.4 mg5.4 mg 5.0 mg5.0 mg
60-6960-69 4.6 mg4.6 mg 4.0 mg4.0 mg
70-7970-79 4.3 mg4.3 mg 3.5 mg3.5 mg
80-8980-89 3.9 mg3.9 mg 3.0 mg3.0 mg
> 90> 90 3.6 mg3.6 mg 3.0 mg3.0 mg
Garcia et al, CHEST June 2005
• In each age group, median daily dose for In each age group, median daily dose for afib pts less than for VTE ptsafib pts less than for VTE pts
• Older women require lowest dosesOlder women require lowest doses
• When warfarin initiated, 5 mg/day will When warfarin initiated, 5 mg/day will lead to overanticoagulation for manylead to overanticoagulation for many
geriatric patientsgeriatric patients
• Lower initiation and maintenance doses for Lower initiation and maintenance doses for elderly patientselderly patients
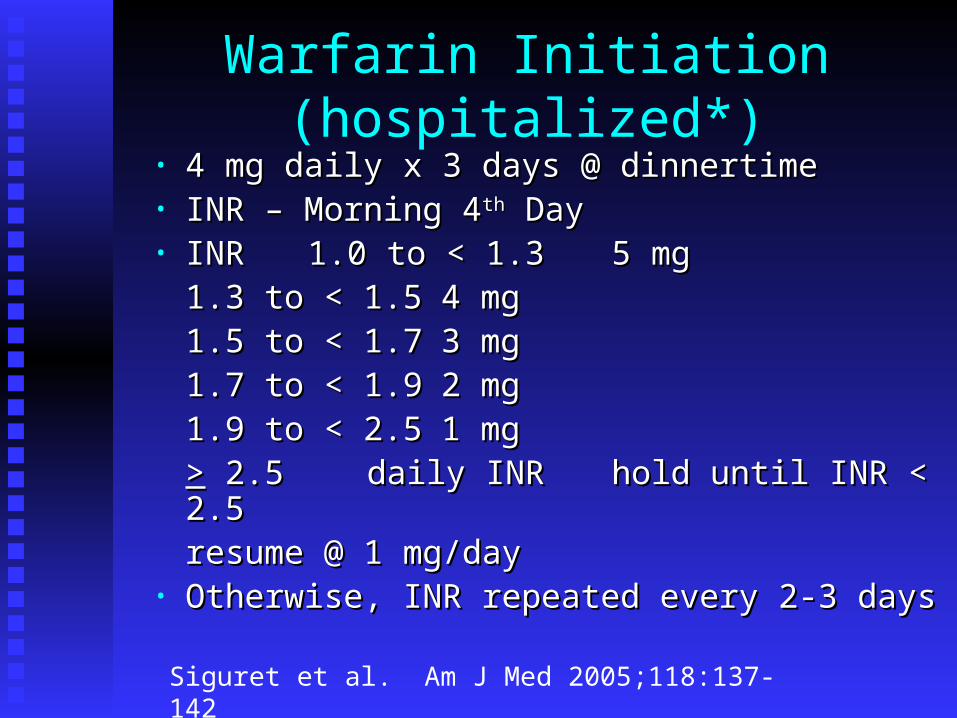
Warfarin Initiation (hospitalized*)• 4 mg daily x 3 days @ dinnertime4 mg daily x 3 days @ dinnertime• INR – Morning 4INR – Morning 4thth Day Day• INRINR 1.0 to < 1.31.0 to < 1.3 5 mg5 mg
1.3 to < 1.51.3 to < 1.5 4 mg4 mg1.5 to < 1.71.5 to < 1.7 3 mg3 mg1.7 to < 1.91.7 to < 1.9 2 mg2 mg1.9 to < 2.51.9 to < 2.5 1 mg1 mg>> 2.5 2.5 daily INR daily INR hold until INR < 2.5hold until INR < 2.5
resume @ 1 mg/dayresume @ 1 mg/day• Otherwise, INR repeated every 2-3 daysOtherwise, INR repeated every 2-3 days
Siguret et al. Am J Med 2005;118:137-142
Other Options ???
• For NVAF pts – ACTIV StudyFor NVAF pts – ACTIV Study– Warfarin vs. ASA/ClopidigrelWarfarin vs. ASA/Clopidigrel
• XimelagatranXimelagatran
Ximelegatran
• Oral Direct Thrombin InhibitorOral Direct Thrombin Inhibitor
• Fixed DoseFixed Dose
• Fast onset and offset activityFast onset and offset activity
• Very few food/drug interactionsVery few food/drug interactions
• No laboratory monitoringNo laboratory monitoring
Ximelegatran, cont.
• Adverse EffectsAdverse Effects
1.1. Liver enzyme elevationLiver enzyme elevation
2.2. Risk for CADRisk for CAD
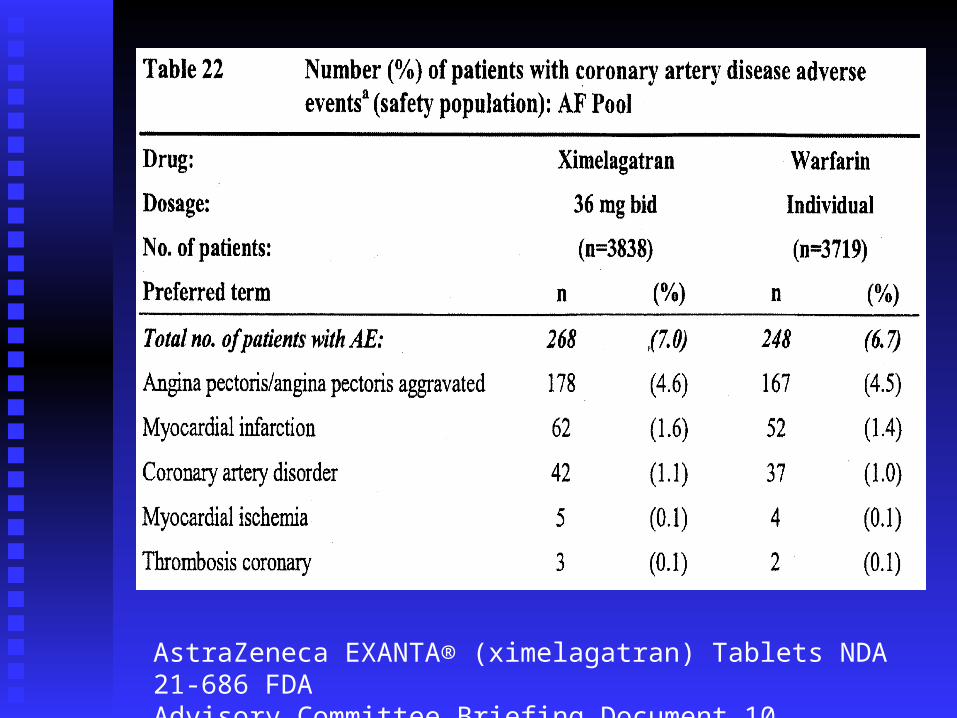
AstraZeneca EXANTA® (ximelagatran) Tablets NDA 21-686 FDA Advisory Committee Briefing Document 10 September 2004 pg. 109

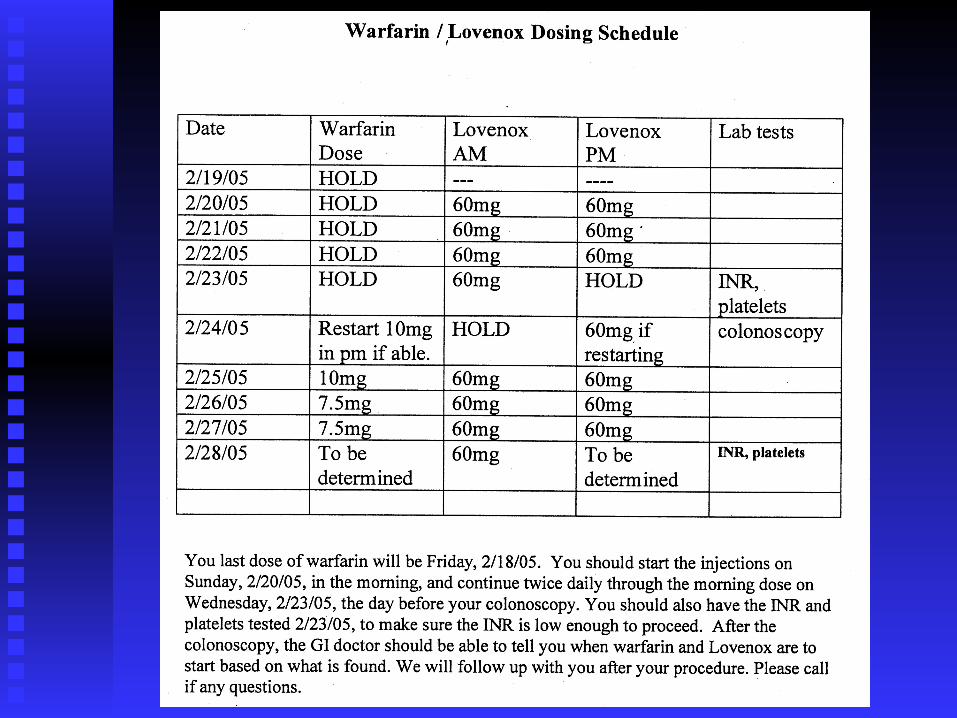
Bridging Therapy
Anticoagulation Perioperative Anticoagulation Perioperative Interruption of WarfarinInterruption of Warfarin
VTE Risk vs. Hemorrhage RiskVTE Risk vs. Hemorrhage Risk
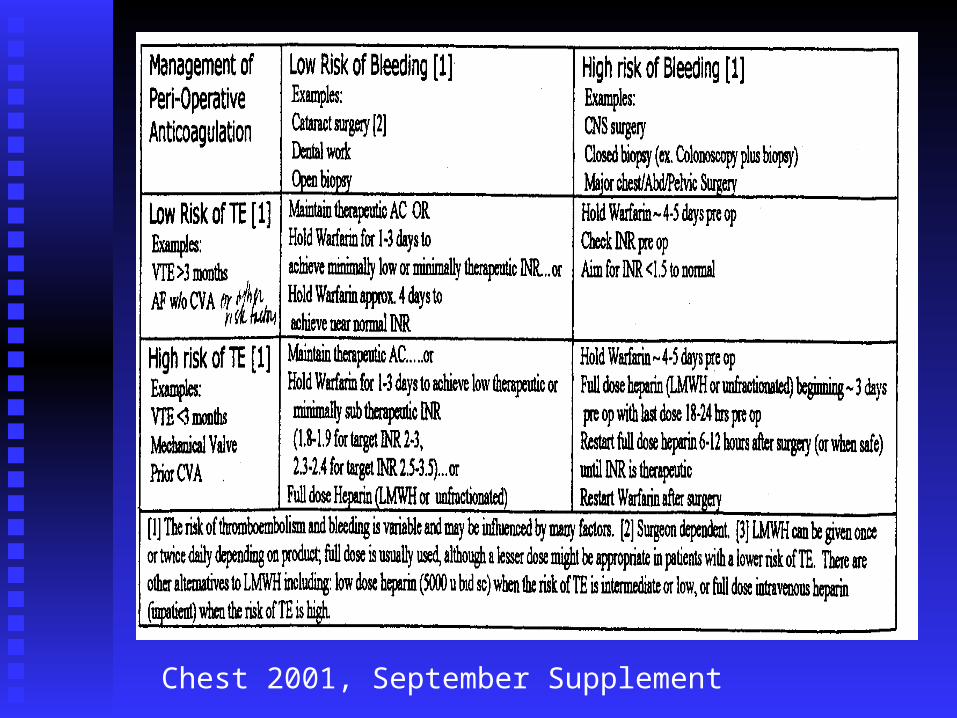
Chest 2001, September Supplement
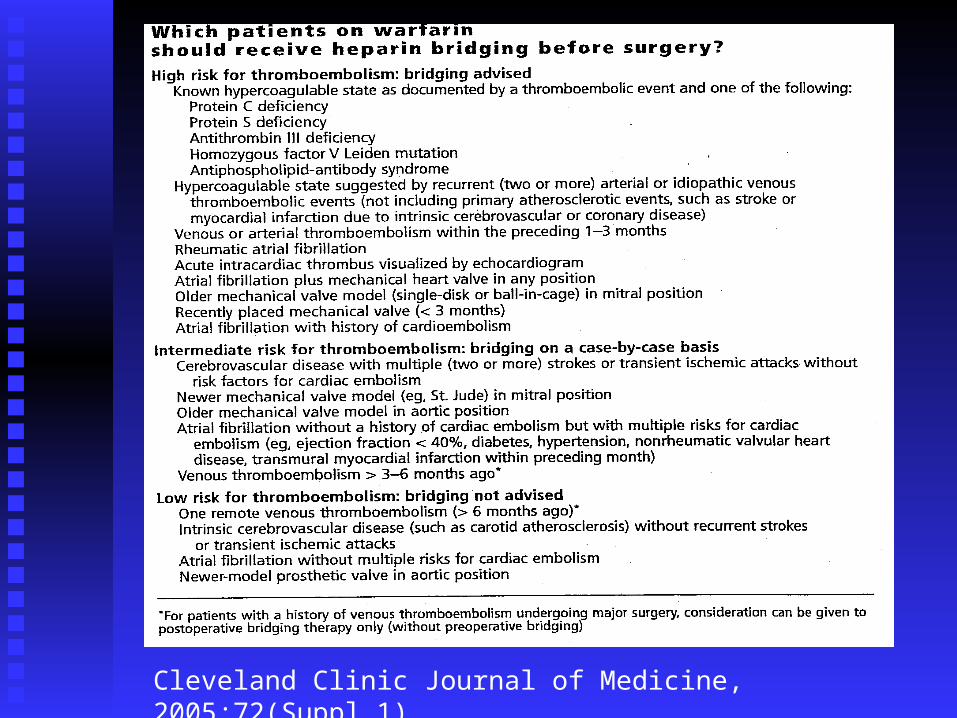
Cleveland Clinic Journal of Medicine, 2005;72(Suppl 1)
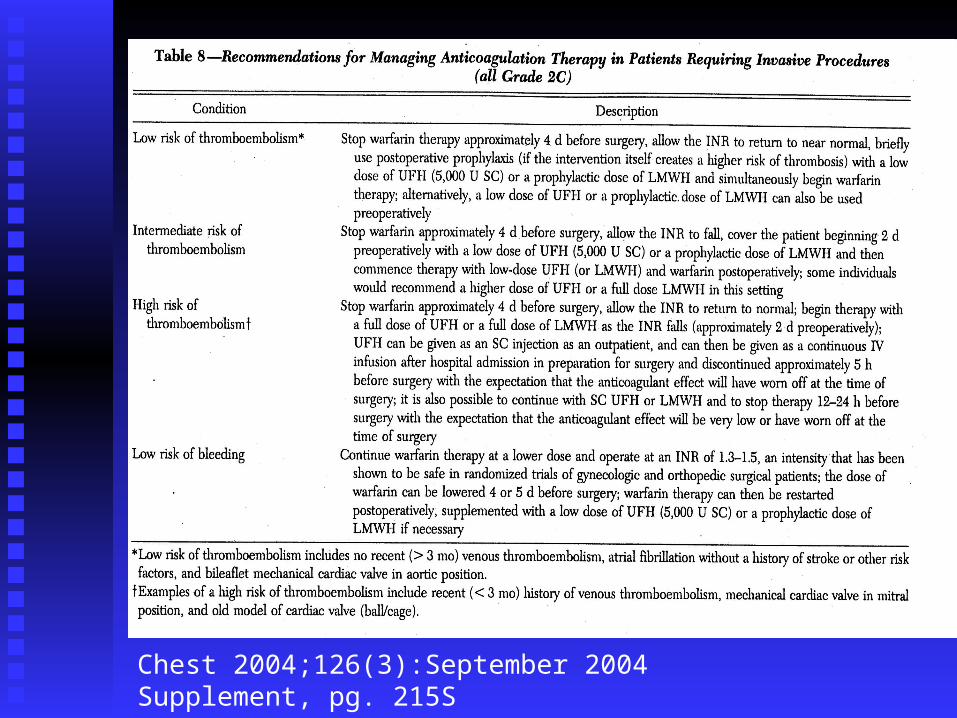
Chest 2004;126(3):September 2004 Supplement, pg. 215S