SOS Signs of Suicide ® An Evidence-based Suicide Prevention Program for High Schools.

Evidence-Based Psychotherapies forSuicide Prevention
Future DirectionsGregory K. Brown, PhD, Shari Jager-Hyman, PhD
Psychotherapeutic interventions targeting suicidal thoughts and behaviors are essential for reducingsuicide attempts and deaths by suicide. To determine whether specific psychotherapies areefficacious in preventing suicide and suicide-related behaviors, it is necessary to rigorously evaluatetherapies using RCTs. To date, a number of RCTs have demonstrated efficacy for severalinterventions focused on preventing suicide attempts and reducing suicidal ideation. Althoughthese studies have contributed greatly to the understanding of treatment for suicidal thoughts andbehaviors, the extant literature is hampered by a number of gaps and methodologic limitations.Thus, further research employing increased methodologic rigor is needed to improve psychother-apeutic suicide prevention efforts. The aims of this paper are to briefly review the state of the sciencefor psychotherapeutic interventions for suicide prevention, discuss gaps and methodologiclimitations of the extant literature, and suggest next steps for improving future studies.(Am J Prev Med 2014;47(3S2):S186–S194) & 2014 American Journal of Preventive Medicine
Introduction
The development and implementation of effectiveinterventions are imperative for reducing rates ofsuicide and related behaviors. In response to the
ongoing need for effective treatments aimed at prevent-ing suicide and self-directed violence, the NationalAction Alliance for Suicide Prevention’s (Action Alli-ance) Research Prioritization Task Force (RPTF)1 hasproposed the following Aspirational Goal focused onpsychotherapeutic interventions: “…develop widelyavailable, more effective and efficient psychosocial inter-ventions targeted at individuals, families, and communitylevels.”The current paper has three main aims in discussing
this Aspirational Goal. First, with a focus on RCTs, thestate of the science for evidence-based psychotherapyinterventions for suicidal ideation and behavior isreviewed. Second, limitations of the current researchand suggestions for future research are discussed. Finally,a step-by-step pathway for evaluating psychotherapyinterventions for suicide prevention is proposed.
State of the Science of Evidence-BasedTreatments for Suicide PreventionSeveral RCTs2–5 have demonstrated promising results inreducing suicide attempts and self-directed violence. Acomprehensive review of the literature is beyond thescope of this paper; however, reviews2–5 were used toidentify studies to include in this brief review. A selectionof studies yielding positive effects will be highlighted andpresented in Table 1. Briefly, cognitive therapy for suicideprevention (CT-SP)6; cognitive–behavioral therapy(CBT)7; dialectical behavior therapy (DBT)8; problem-solving therapy (PST)9; mentalization-based treatment(MBT)10; and psychodynamic interpersonal therapy(PIT)11 have all evidenced positive effects for preventingsuicide attempts or self-directed violence in adults.More specifically, recent suicide attempters who
received CT-SP were 50% less likely to reattempt thanparticipants who received enhanced usual care (EUC)with tracking and referrals.6 CBT plus treatment as usual(TAU) also reduced self-harming behaviors relative toTAU alone.7 For individuals with borderline personalitydisorder (BPD), DBT demonstrated a greater reduction insuicide attempts relative to community treatment byexperts.8 However, DBT was not statistically more effec-tive than a manualized general psychiatric managementcondition, consisting of case management, dynamicallyinformed psychotherapy, and medication management.12
Also focused on BPD, MBT, a psychoanalyticallyoriented partial hospitalization program, was more
From the Perelman School of Medicine of the University of Pennsylvania,Philadelphia, Pennsylvania
Address correspondence to: Gregory K. Brown, PhD, Department ofPsychiatry, University of Pennsylvania, 3535 Market Street, Room 2032,Philadelphia PA 19104-3309. E-mail: [email protected].
0749-3797/$36.00http://dx.doi.org/10.1016/j.amepre.2014.06.008
S186 Am J Prev Med 2014;47(3S2):S186–S194 & 2014 American Journal of Preventive Medicine � Published by Elsevier Inc.

Table1.Su
mmaryof
select
RCTs
Autho
rsSa
mple
Stud
yinterven
tion
Con
trol
cond
ition
Outcome
varia
bles
Follow-up
intervals
Mainfind
ings
Batem
anan
dFo
nagy
(1999)10
Adults
with
BPD
referred
topsychiatric
unit
Partial
hospita
lization
(n¼1
9)
Stan
dard
psychiatric
care
(n¼1
9)
Suicide
attempts
3,6
,9,1
2,1
5,
18mon
ths
Patie
ntswho
received
thestud
yinterven
tion
expe
rienced
asign
ificant
redu
ctionin
attempts
from
admission
to18mon
ths(Ken
dall’sW¼0
.59,
χ2(3)¼
33.5,p
o0.001)
Blum
etal.
(2008)13
Adults
with
BPD
STEP
PSplus
TAU(n¼6
5)
TAU(n¼5
9)
Suicide
attempts
1,3
,6,9
,12
mon
ths
Nodifferen
cesin
timeto
firstsuicideattempt
betwee
nST
EPPS
þTA
Uan
dTA
Ugrou
ps;
χ2(1)o
0.1,p
¼0.994
Brownet
al.
(2005)6
Adults
recruited
from
EDfollowing
asuicideattempt
CT(n¼6
0)
EUC(n¼6
0)
Suicidal
idea
tion,
suicide
attempts
1,3
,6,1
2,1
8mon
ths
At6mon
ths,usingtheKap
lan–
Meier
metho
d,estim
ated
reattempt-free
prob
ability:C
Tgrou
p¼0.86(95%
CI¼
074,0
.93);usua
lcare
¼0.68(95%
CI¼
0.54,0
.79)
At18mon
ths,estim
ated
reattempt-free
prob
ability:C
T¼0.76(95%
CI¼
0.62,0
.85);usua
lcare¼0
.58(95%
CI¼
0.44,0
.70)
Patie
ntsin
theCTcond
ition
hadasign
ificantly
lower
reattempt
rate
(Waldχ2¼3
.9,p¼0
.049)a
ndwere50%
less
likelyto
reattempt
than
theusua
lcare
grou
p(hazardratio¼0
.51,95
%CI¼0
.26,0.99
7)Th
erewereno
sign
ificant
grou
pdifferen
cesin
suicidal
idea
tion
Bruce
etal.
(2004)21
Dep
ressed
olde
rad
ults
recruited
from
prim
arycare
Structured
,team
-based
interven
tion
includ
ing
citalopram
þpsycho
therap
y(n¼3
20)
TAU(n¼2
78)
Suicidal
idea
tion
4,8
,12
mon
ths
Rates
ofsuicidal
idea
tionde
clined
faster
forthe
interven
tiongrou
p(12.9%
declinefrom
baseline)
than
theTA
Ugrou
p(3.0%
declinefrom
baseline;
p¼0.01foralld
epressed
patie
nts,p¼
0.006for
patie
ntswith
MDD)
Com
toiset
al.
(2011)17
Adults
evalua
ted
forsuicide
attempt
orim
minen
tris
kbu
tjudg
edsafe
for
discha
rge
CAM
S(n¼1
6)
E-CAU
(n¼1
6)
Suicide
attempts,
suicidal
idea
tion
2,4
,6,1
2mon
ths
Participan
tswho
received
CAM
Smad
efewer
suicideattemptsthan
thosewho
received
E-CAU
at2-,4-,an
d6-m
onth
follow-ups
a
Suicidal
idea
tionim
proved
sign
ificantlyforCAM
Spa
tients,
reaching
89%
redu
ctionat
12mon
ths,
RR¼0
.11,9
5%
CI¼
0.04,0
.30;a
t12mon
ths,
E-CAU
patie
ntsrepo
rted
sign
ificantlyworse
suicidal
idea
tionthan
CAM
Spa
tients(RR¼4
.81,
95%
CI¼
1.61,1
4.33)
(con
tinue
don
next
page
)
Brown and Jager-Hyman / Am J Prev Med 2014;47(3S2):S186–S194 S187
September 2014

Table1.S
ummaryof
select
RCTs
(con
tinue
d)
Autho
rsSa
mple
Stud
yinterven
tion
Con
trol
cond
ition
Outcome
varia
bles
Follow-up
intervals
Mainfind
ings
Davidsonet
al.
(2006)14
Adults
with
BPD
andan
episod
eof
DSH
with
inthe
past
12mon
ths
CBTþ
TAU
(n¼5
3)
TAU(n¼4
9)
Suicidal
acts
6,1
2,1
8,2
4mon
ths
After24mon
ths,therewas
agrea
terredu
ctionin
numbe
rof
suicidal
acts
intheinterven
tiongrou
pcompa
redto
theTA
Ugrou
p(m
eandifferen
ce¼
–0.91,p
¼0.020)
Diamon
det
al.
(2010)19
Adolescents
iden
tified
assuicidal
byscreen
ingdu
ring
prim
arycare
orED
visits
ABFT
(n¼3
5)
EUC(n¼3
1)
Suicidal
idea
tion
6,1
2,2
4wee
ksAt
the12-wee
kassessmen
t,pa
tientsreceiving
ABFT
demon
stratedasign
ificantlygrea
terrate
ofim
provem
entin
suicidal
idea
tionthan
patie
nts
receivingEU
C,F
(1,6
4)¼
12.60,p
¼0.001
ABFT
hadasign
ificant
effect
onclinical
recovery
(SIQ-JRr13)ofsuicida
lide
ationat
alltim
epo
ints;
at6wee
ks,6
9.7%of
ABFT
patie
ntsan
d40.7%of
EUCpa
tientsrepo
rted
suicidal
idea
tionin
the
norm
ativerang
e,OR¼3
.35,9
5%
CI¼
1.15,9
.73,
χ²(1)¼
5.07,p
¼0.02;a
t12wee
ks,8
7.1%of
ABFT
patie
ntsan
d51.7%
ofEU
Cpa
tientsrepo
rted
idea
tionin
theno
rmativerang
e,OR¼6
.30,9
5%
CI¼
1.76,2
2.61,χ²(1
)¼8.93,p
¼0.003;a
t24
wee
ks,7
0%
ofAB
FTpa
tientsan
d34.6%
ofEU
Cpa
tientsrepo
rted
idea
tionin
theno
rmativerang
e,OR¼4
.41,9
5%
CI¼
1.43,1
3.56,χ²(1
)¼7.01,
p¼0.008
Guthrie
etal.
(2001)11
Adults
presen
ting
toED
afterself-
poison
ing
Psycho
dy-
namic
interpersona
ltherap
yde
livered
inho
me(n¼5
8)
TAU(n¼6
1)
Suicidal
idea
tion
1,6
mon
ths
Atthe6-m
onth
follow-upassessmen
t,pa
tients
receivingthestud
yinterven
tionrepo
rted
lower
levelsof
suicidal
idea
tioncompa
redto
those
receivingTA
U(differen
cesbe
twee
nmea
ns¼–4.9,
95%
CI¼
–8.2,–
1.6,p
¼0.005)
Hatcher
etal.
(2011)9
Adults
presen
ting
toaho
spita
lafter
self-ha
rm
PST(n¼5
22)
Usual
care
(n¼5
72)
Self-ha
rm3,1
2mon
ths
Fewer
patie
ntsreceivingPS
Trepo
rted
repe
atep
isod
esof
self-ha
rmat
the12-m
onth
assessmen
tthan
thosereceivingusua
lcare
(RR¼0
.39,9
5%
CI¼
0.07,0
.60,p
¼0.03)
Hue
yet
al.
(2004)16
Youthfollowing
EDvisitfor
suicide
attempt,ide
ation,
orplan
ning
MST
bStan
dard
trea
tmen
tbSu
icidal
idea
tion,
suicide
attempts
4,1
6mon
ths
MST
was
sign
ificantlymoreeffectivethan
stan
dard
trea
tmen
tat
redu
cing
suicideattempts
over
16mon
ths,t(linea
r)¼2
.61,p
o0.01,t
(qua
dratic)¼
3.60,p
o0.001
Therewereno
sign
ificant
grou
pdifferen
cesfor
suicidal
idea
tion
(con
tinue
don
next
page
)
Brown and Jager-Hyman / Am J Prev Med 2014;47(3S2):S186–S194S188
www.ajpmonline.org

Table1.S
ummaryof
select
RCTs
(con
tinue
d)
Autho
rsSa
mple
Stud
yinterven
tion
Con
trol
cond
ition
Outcome
varia
bles
Follow-up
intervals
Mainfind
ings
Line
hanet
al.
(2006)8
Wom
enwith
BPD
with
Z2ep
isod
esof
self-ha
rmin
the
past
5years,
includ
ingZ1
with
inthepa
st8
wee
ks
DBT(n¼5
2)
Com
mun
itytrea
tmen
tby
expe
rts
(n¼4
9)
Suicidal
idea
tion,
suicide
attempts
4,8
,12,1
6,
20,2
4mon
ths
Fewer
patie
ntsreceivingDBTha
dsuicideattempts
than
thosereceivingtrea
tmen
tby
expe
rts(23.1%
vs46%
,hazardratio
¼2.66,p
¼0.005,
NNT¼
4.24,
95%
CI¼
2.40,1
8.07);themea
nprop
ortio
nsof
suicideattempterspe
rtreatmen
tgroup
perp
eriod
were6.2%
(95%
CI¼
3.1%,1
1.7%)a
nd12.2%
(95%
CI¼
7.1%,2
0.3%)for
theDBTan
dcontrol
grou
ps,respe
ctively
Fewer
patie
ntsreceivingDBTthan
commun
itytrea
tmen
tby
expe
rtsha
dno
n-am
bivalent
suicide
attempts(5.8%
vs13.3%,p
¼0.18,F
ishe
r’sexact
test
andNNT¼
13.3,9
5%
CI¼
5.28,2
5.41)
Therewereno
sign
ificant
grou
pdifferen
cesfor
suicidal
idea
tion
McM
ainet
al.
(2009)12
Adults
with
BPD
with
Z2suicidal
orno
n-suicidal
self-injurio
usep
isod
esin
the
past
5years,Z1
episod
ein
the
past
3mon
ths
DBT(n¼9
0)
Gen
eral
psychiatric
man
agem
ent
(n¼9
0)
Freq
uencyan
dseverityof
suicidal
episod
es
4,8
,12
mon
ths
Therewereno
sign
ificant
grou
pdifferen
cesfor
suicidal
episod
es
Slee
etal.
(2008)7
Adults
who
recentlyen
gage
din
deliberateself-
poison
ingor
self-
injury
CBTþ
TAU
(n¼4
0)
TAU(n¼4
2)
Self-ha
rm,
suicidal
cogn
ition
3,6
,9mon
ths
At9mon
ths,pa
tientswho
received
CBTþ
TAU
hadsign
ificantlygrea
terredu
ctions
inself-ha
rmthan
thosewho
received
TAUalon
e(po0.05)
CBTþT
AUpa
tientsha
dsign
ificantlyde
crea
sed
suicidalcogn
ition
sas
compa
redto
TAUpa
tientsat
the3-(po
0.05),6-(po
0.05),an
d9-m
onth
(po0.01)a
ssessm
ents
Stew
artet
al.
(2009)18
Adults
intrea
tmen
tfollowingasuicide
attempt
CBT(n¼1
1),
PST(n¼1
2)
TAU(n¼9
)Su
icidal
idea
tion,
suicide
attempts
4wee
ks(PST
),7wee
ks(CBT),
2mon
ths
(TAU
)
CBTwas
themoste
ffectivetrea
tmen
tfor
redu
cing
suicideattempts;pa
tientsreceivingCBTmad
eno
attemptsdu
ringthestud
y,whe
reas
patie
nts
receivingPS
Tan
dTA
Umad
ean
averag
eof
0.33
attemptsan
d0.22attempts,respectively
Suicidal
idea
tionde
crea
sedwith
both
CBT(z¼
�2.32,p
o0.05,r¼0
.49)a
ndPS
T(z¼�
2.39,
po0.05,r¼0
.49);de
crea
sesin
suicidal
idea
tion
weregrea
terfor
thePS
Tthan
TAUgrou
p(U¼2
6.5,
pr0.05,r¼0
.49)
(con
tinue
don
next
page
)
Brown and Jager-Hyman / Am J Prev Med 2014;47(3S2):S186–S194 S189
September 2014

effective than general psychiatric servicesin reducing suicidal and self-mutilatoryacts.10 Similarly, relative to TAU alone,PST plus usual care resulted in a decreasein repeat hospitalizations for self-harm inindividuals with a history of previous self-harm.9 Finally, four home-based sessionsof interpersonal therapy were more effec-tive than TAU in reducing suicidal idea-tion and repeated self-harm in individualswho self-poisoned.11
Although a number of suicide-prevention interventions have evidencedefficacy, other interventions, includingsystems training for emotional predict-ability and problem solving13 and CBT forCluster B personality disorders,14 havenot been supported empirically. For acomprehensive review of negative find-ings, please see previous reviews.2–5
Fewer studies15,16 have demonstratedefficacy for psychotherapy interventionsin reducing self-directed violence in ado-lescents. Wood and colleagues15 found thatadolescents who received developmentalgroup therapy (consisting of componentsof CBT, DBT, and psychodynamic grouptherapy) plus TAU were less likely toengage in repeated deliberate self-harmon two or more occasions than thosewho received TAU alone. Finally, multi-systemic therapy, an intensive family-based treatment, reduced the frequencyof suicide attempts compared to treatmentreceived during inpatient hospitalization.16
In addition to psychosocial interven-tions designed to prevent suicideattempts, several psychotherapy treat-ments directly target suicidal ideation.Specifically, collaborative assessment andmanagement of suicidality (CAMS),17
CBT,18 PST,18 and PIT11 have resultedin the reduction of suicidal ideation inadults. CAMS, a therapeutic frameworkfocused on identifying causes of suicidalideation and treatment goals for reducingsuicidal ideation, was associated withsignificantly greater and sustained reduc-tion of suicidal ideation at 12 monthspost-treatment compared to TAU.17 Sim-ilarly, both PST and CBT resultedin greater reduction of suicidal ideationthan TAU.16 Attachment-based familyTa
ble1.S
ummaryof
select
RCTs
(con
tinue
d)
Autho
rsSa
mple
Stud
yinterven
tion
Con
trol
cond
ition
Outcome
varia
bles
Follow-up
intervals
Mainfind
ings
Unü
tzer
etal.
(2006)20
Older
adults
with
MDDor
dysthymia
IMPA
CT
interven
tion
(n¼9
06)
Usual
care
(n¼8
95)
Suicidal
idea
tion
6,1
2,1
8,2
4mon
ths
Fewer
patie
ntsreceivingtheIM
PACTinterven
tion
than
usua
lcarerepo
rted
thou
ghts
ofsuicideat
6(OR¼0
.54,9
5%
CI¼
0.37,0
.78,p
¼0.001),12
(OR¼0
.54,9
5%
CI¼
0.40,0
.73,p
o0.001),18
(OR¼0
.52,9
5%
CI¼
0.36,0
.75,p
o0.001),an
d24
(OR¼0
.65,95
%CI¼0
.46,0.91
,po0.01
)mon
ths
Fewer
patie
ntsreceivingtheIM
PACTinterven
tion
repo
rted
thou
ghts
ofde
athor
dyingat
6(OR¼0
.62,9
5%
CI¼
0.49,0
.78,p
o0.001),12
(OR¼0
.44,9
5%
CI¼
0.35,0
.56,p
o0.001),18
(OR¼0
.62,9
5%
CI¼
0.49,0
.79,p
o0.001),an
d24
(OR¼0
.72,95
%CI¼0
.57,0.92
,p¼0
.01)
mon
ths
Woo
det
al.
(2001)15
Adolescents
referred
tomen
tal
health
services
afterde
liberate
self-ha
rm
Group
therap
y(n¼3
2)
Rou
tinecare
(n¼3
1)
Rep
etition
ofself-ha
rm,
suicidal
thinking
6wee
ks,7
mon
ths
Participan
tswho
received
grou
ptherap
ywereless
likelyto
repe
atself-ha
rmthan
thosewho
received
routinecare
(OR¼6
.3,6
5%
CI¼
1.4,2
8.7)
Therewereno
sign
ificant
grou
pdifferen
ces
rega
rdingsuicidal
thinking
Note:
Onlyou
tcom
esrelatedto
suicideidea
tionan
dattemptsarerepo
rted
.aNostatistical
analyses
werepe
rformed
fortheseresults.
bStud
ydidno
tindicate
thenu
mbe
rof
participan
tspe
rcond
ition
.AB
FT,attachm
ent-b
ased
family
therap
y;BPD
,borde
rline
person
ality
disorder;C
AMS,
collabo
rativeassessmen
tand
man
agem
ento
fsuicida
lity;CBT,cogn
itive–be
havioraltherap
y;CT,cogn
itive
therap
y;DBT,
dialectical
beha
vior
therap
y;DSH
,deliberateself-ha
rm;E
-CAU
,enh
ancedcare
asusua
l;ED
,emerge
ncyde
partmen
t;EU
C,e
nhan
cedusua
lcare;
IMPA
CT,
ImprovingMoo
d:Prom
otingAccess
toCollabo
rativeTrea
tmen
t;MDD,m
ajor
depressive
disorder;M
ST,m
ultisystemictherap
y;NNT,
numbe
rne
eded
totrea
t;PS
T,prob
lem-solving
therap
y;RR,riskratio
;SIQ-JR,S
uicide
Idea
tion
Que
stionn
aire–Junior;S
TEPP
S,system
straining
forem
otiona
lpredictab
ility
andprob
lem
solving;
TAU,treatmen
tas
usua
l
Brown and Jager-Hyman / Am J Prev Med 2014;47(3S2):S186–S194S190
www.ajpmonline.org

therapy, which focuses on strengthening the parent–adolescent attachment bond, has also demonstratedpromise in reducing suicidal ideation in suicidal adoles-cents relative to EUC.19
Finally, to our knowledge, two studies have demon-strated efficacy in reducing suicidal ideation in depressedolder adults in primary care settings.20,21 The ImprovingMood: Promoting Access to Collaborative Treatmentstudy determined that a collaborative, team-basedapproach to treating depression resulted in a greaterreduction of suicidal ideation than usual care. ThePrevention of Suicide in Primary Care Elderly: Collabo-rative Trial intervention, consisting of a clinical algo-rithm for treating geriatric depression in primary caresettings and care management, was more effective inreducing suicidal ideation than EUC.
Limitations of the Current State of theScienceAlthough the aforementioned RCTs represent importantfirst steps in gaining a deeper understanding of effectivesuicide prevention strategies, several gaps and methodo-logic concerns limit conclusions that can be drawn fromthese studies. Several significant gaps in the literatureshould be noted. First, given the paucity of RCTs poweredto detect deaths by suicide, it is unknown whether deathby suicide (rather than suicide attempts) can be preventedby psychotherapy. Moreover, it is unclear as to whetherthe reduction of suicide attempts or ideation via psycho-therapy actually reduces deaths by suicide.Second, many studies focused on suicide prevention
exclude patients at imminent risk for suicide, making itimpossible to determine whether interventions that areefficacious for lower-risk patients are also efficacious forthose at highest risk.22 Third, there are limited psycho-therapy RCTs focused on preventing suicide attempts formany at-risk populations, including older adults; Veteransor military service members; lesbian, gay, bisexual, trans-gender, queer, and two-spirit (LGBTQ2) populations;Native Americans and other minority groups; and survi-vors of suicide or suicide attempts. It is unclear whether theresults of existing RCTs generalize to these populations.Additionally, the majority of psychotherapy interven-
tions for suicidal thoughts and behaviors have beenconducted in outpatient settings, and very few RCTs havebeen conducted in acute care settings, such as emergencydepartments, inpatient units, and crisis hotlines. Thedevelopment of interventions for these settings is partic-ularly important given that many high-risk patients onlypresent to acute care services and never receive additionalpsychosocial treatment. The dearth of knowledge abouteffective treatments for inpatient settings is especially
alarming given that the current standard of care is to admithigh-risk patients to inpatient units. This suggests thatpatients who are at high risk for suicide may not receiveappropriate evidence-based treatments to prevent suicide.A final gap in the extant research examining the
efficacy of psychotherapy interventions for suicide pre-vention is the failure to replicate studies in whichtreatments have been found to be efficacious. It isespecially critical that replication trials be conducted byindependent researchers, as in some cases replicationstudies conducted outside of the original research groupshave failed to demonstrate the same beneficial effects.12
A variety of methodologic limitations of the existingresearch hamper the ability to draw firm conclusionsregarding the effectiveness and generalizability of varioussuicide prevention efforts (limitations have been pub-lished elsewhere1–4). First, a lack of consensus regardingterms and operationalized definitions used to describesuicide, attempts, ideation, and other related behaviorslimits the ability to generalize across studies and replicatefindings. Researchers also often neglect to use reliableand validated measures of suicidal ideation and behav-iors, making it difficult to understand the specificbehaviors measured and targeted by the interventionsin question.In addition, many previously published RCTs do not
provide detailed psychotherapy manuals. The absence oftreatment manuals creates significant challenges for dis-semination and implementation efforts in the communityand precludes appropriate replication studies. Furthermore,researchers often neglect to include measures assessing theintegrity of the study intervention. It is important to assessthe extent to which study therapists adhere to the theoryand practice of the intervention of interest.An additional common methodologic problem is that
studies are underpowered to adequately detect treatmenteffects, causing potentially efficacious treatments to yieldnegative results owing to lack of power rather than lack ofefficacy. Moreover, very few studies include descriptions ofpower analyses, making it difficult to determine the reasonsfor failing to find positive effects. Other studies conductpower analyses based on unlikely or biased estimates ofeffects, leading to inadequate estimates of sample sizes.Conservative estimates are necessary to ensure that sam-ples are powered sufficiently to detect effects.Given that RCTs are generally longitudinal, attrition is
common and results in an additional methodologic issueof handling missing data. This is particularly problematicwhen dropout rates differ across treatment conditions,which may result in biased results.7 As recommended inthe CONSORT guidelines for reporting RCT results,intention-to-treat analysis is a helpful statistical approachto handling missing data to minimize bias.23
Brown and Jager-Hyman / Am J Prev Med 2014;47(3S2):S186–S194 S191
September 2014

Other methodologic limitations encountered in theextant literature include potential threats to externalvalidity by choosing highly selective samples11; failureto use blind investigators, assessors, or patients or specifywhether blinding was implemented; potential measure-ment bias (e.g., using differential measurement intervalsand methods for assessing primary outcomes in inter-vention and control groups10); failure to identify, meas-ure, and control for potential non-study co-interventions(e.g., pharmacotherapy); and analyses capitalizing ondifferences in baseline characteristics.16
It is also advised that researchers focus on a priorianalyses and refrain from making firm conclusions onthe basis of unplanned, underpowered subgroup analy-ses. Finally, stratified randomization is an important toolin preventing Type I errors and imbalance betweentreatment groups, particularly for smaller trials in whichknown factors influence treatment responsiveness.
Next Steps and Breakthroughs NeededAlthough the existing RCTs have created an importantjumping-off point for evaluating future psychotherapeuticinterventions for suicide attempts and ideation, muchwork remains. The adoption of the following recommen-dations may lead to increased methodologic rigor withwhich suicide research is conducted, and in turn, thedevelopment and dissemination of treatments that reducesuicidal ideation, suicide attempts, and ultimately, suicide.Given that the current lack of consensus of terms and
definitions leads to difficulty in interpreting results andaggregating findings across studies, an important short-term goal is to adopt an agreed-upon nomenclature forall studies addressing suicide-relevant thoughts andbehaviors, such as the self-directed violence nomencla-ture proposed by the CDC’s National Center for InjuryPrevention and Control.24 It is then essential to employvalid and reliable measures to assess these constructs.The Columbia Suicide Severity Rating Scale (C-SSRS25)
is one such measure endorsed by the U.S. Food and DrugAdministration for use in pharmaceutical trials. It wouldalso be beneficial to use an agreed-upon measure forpsychotherapy trials. Furthermore, to achieve continuityacross studies, it would be helpful for all studies to use thesame endpoints in reporting outcomes, thereby increasingthe ease with which results can be aggregated acrossstudies via meta-analyses.There is also a need for methods to address ambiguous
suicide behavior that may not neatly fit into a specificcategory of suicidal thoughts or behaviors. One potentialsolution to this problem is to form suicide adjudicationboards to review ambiguous behaviors and reach aconsensus regarding appropriate classification.26
An additional short-term goal is to develop interven-tions designed for high-risk populations, including olderadults, Veterans or military service members, LGBTQ2individuals, minority groups, and survivors of suicide orsuicide attempts as indicated by empirical research. Thereis also a need for methods to screen and treat high-riskindividuals in acute care settings, including emergencydepartments, crisis hotlines, and inpatient units.As previously mentioned, many studies assessing the
efficacy of treatments for suicide prevention are under-powered. Although preliminary studies to determineacceptability and feasibility of specific interventions arenecessary, large-scale RCTs that are adequately poweredto detect treatment effects are also imperative. This is truefor studies assessing treatments focused on reducingsuicidal thoughts, suicide attempts, and other self-directed violence, as well as those designed to evaluatetreatments for the prevention of deaths by suicide.Because suicide is a low base rate behavior, very large
samples are required to conduct adequately poweredtrials. Multi-site collaborations allow the collection ofdata from large samples while reducing financial andorganizational burden on any one site. In addition, theuse of standardized outcome measures and data sharingmay facilitate meta-analytic approaches and circum-vent problems associated with inadequately poweredstudies.Further development and dissemination of treatments
specifically targeting suicidal ideation are also necessary,particularly for populations such as older men who havethe highest rates of suicide of any age group.27 Despitetheir increased rate of deaths by suicide, older adults areless likely to make suicide attempts than individuals inany other age group.28 Suicidal ideation may thus serve asthe only warning sign of future suicides in older adults,making it especially important to specifically targetsuicidal ideation in this population. As frequent attemptsare less common in this population, treatments focusedon preventing attempts may be less appropriate.Because suicidal ideation is a dimensional construct
that waxes and wanes over time, RCTs should includeappropriate measures for tracking fluctuations in suicidalideation. The use of ecological momentary assessment,for example, would provide much-needed insight intothe fluctuation of suicidal ideation and inform thedevelopment of timely interventions that specificallytarget changes in suicidal ideation.Very little is known about whether positive effects of
psychotherapies for suicide prevention extend beyondlaboratory settings. In addition to efficacy trials, effec-tiveness trials are also needed to assess whether specifictreatments work in real-world settings. Moreover, inorder to increase external validity of psychotherapy trials,
Brown and Jager-Hyman / Am J Prev Med 2014;47(3S2):S186–S194S192
www.ajpmonline.org

it is important that inclusion and exclusion criteria resultin samples that reflect patients as they present in the realworld (e.g., the exclusion of potential participants who donot misuse substances may result in a biased sample ofsuicide attempters10).There is a need to better develop mechanisms to ensure
that the individuals at risk of suicide have access totreatments that work. In designing interventions,researchers should consider ways to increase the feasi-bility and ease with which treatments can be disseminatedand adapted to various settings. For example, futurepsychotherapies that can be implemented in rural settingsusing telehealth technologies are needed.In addition, researchers are encouraged to clearly
communicate the specific treatment components neces-sary to successfully implement interventions in non-laboratory settings. Another potential approach toincreasing the availability of evidence-based treatmentsis to develop innovative electronic health interven-tions (e.g., smartphone applications, texting, web-basedinterventions, or chat rooms) as either widely availablestand-alone interventions or adjunctive treatments toface-to-face interventions. Finally, further research isneeded to determine the cost-effectiveness and costutility of psychotherapy studies for suicide prevention.As researchers continue to find support for treatments
that reduce suicidal thoughts and behaviors, it is necessaryto identify potential mechanisms of actions that account fortherapeutic change. Thus, in addition to asking whether atreatment works, it is essential to ask why a treatmentworks. This can be achieved by including measures assess-ing constructs underlying treatment effects, such asimprovements in hopelessness or emotion regulation.Identifying mechanisms of action will allow for the
development of more efficient, targeted treatments andmay provide insight into which treatments work bestfor whom.In addition to identifying treatments that are effective in
reducing suicide ideation and behaviors, it is also impor-tant to understand which treatments have not garneredsupport in psychotherapy trials. Systematic trial registra-tion is one method for reducing the “file-drawer effect” inwhich negative findings are not presented to the public.Given the gaps and methodologic flaws in the literature
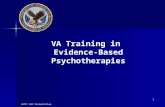
focused on psychotherapy interventions for suicide pre-vention, additional research is needed to determine theefficacy of existing and future treatments. Thus, we proposea general step-by-step research pathway for conductingfuture RCTs with high-risk patients for examining theefficacy of new psychotherapy treatments (Figure 1).The first step of this paradigm is to identify high-risk
subjects by using agreed-upon nomenclature (e.g., CDCnomenclature) as well as validated and reliable assess-ment measures. These high-risk patients can be recruitedfrom a variety of settings including emergency depart-ments, inpatient units, mental health outpatient clinics,and primary care. Following recruitment and initialassessment to determine eligibility, it is recommendedthat patients be randomly assigned to either (1) theco-active intervention condition, which may includemedication, treatment as usual, a comparative therapy,or follow-up services, or (2) the same co-active interven-tion plus a suicide-specific study intervention condition.Alternatively, depending on the question of interest, it
may be more appropriate to omit the co-active inter-vention for participants who are randomized to thesuicide-specific study intervention condition. In orderto gain an understanding of the pathways by which
Figure 1. Proposed step-by-step research pathway for conducting RCTsED, emergency department; MH, mental health; PC, primary care; SDV, self-directed violence; Ss, subjects
Brown and Jager-Hyman / Am J Prev Med 2014;47(3S2):S186–S194 S193
September 2014

treatment affects the outcome of interest (i.e., suicidalideation, suicide attempts, or suicides), it is imperative toexamine moderators of the study treatment and potentialmechanisms of actions. Elucidating the moderators andmechanisms at play will inform the development of moreefficient and targeted future interventions. This paradigmwill also allow for increased understanding of the relationbetween reductions in suicidal ideation and reductions insuicide attempts or deaths by suicide.
ConclusionsDespite important advances in the development andevaluation of psychotherapeutic treatments for suicideprevention, additional research is needed to improve thecurrent state of the science. A focus on filling the gaps inthe literature and increasing methodologic rigor withwhich RCTs of suicide-prevention psychotherapies areconducted will lead to increasingly effective treatmentsfor reducing suicidal ideation, attempts, and deaths.
Publication of this article was supported by the Centers forDisease Control and Prevention, the National Institutes ofHealth Office of Behavioral and Social Sciences, and theNational Institutes of Health Office of Disease Prevention.This support was provided as part of the National Institute ofMental Health-staffed Research Prioritization Task Force ofthe National Action Alliance for Suicide Prevention.
No financial disclosures were reported by the authors ofthis paper.
References1. USDHHS Office of the Surgeon General and National Action Alliance
for Suicide Prevention. 2012 National Strategy for Suicide Prevention:Goals and Objectives for Action. Washington, DC: HHS, September2012. http://www.surgeongeneral.gov/library/reports/national-strategy-suicide-prevention/full-report.pdf.
2. O’Neil M, Peterson K, Low A, et al. Suicide prevention interventionsand referral/follow-up services: a systematic review. Washington, DC:Department of Veterans Affairs, 2012.
3. Mann J, Apter A, Bertolote J, et al. Suicide prevention strategies: asystematic review. JAMA 2005;294(16):2064–74.
4. National Institute for Health andClinical Excellence. Self-harm: longer-termmanagement. (Clinical Guideline CG133). guidance.nice.org.uk/CG133.
5. O’Connor E, Gaynes BN, Burda BU, et al. Screening for and treatmentof suicide risk relevant to primary care: a systematic review for the U.S.Preventive Services Task Force. Ann Intern Med 2013;158(10):741–54.
6. Brown GK, Ten Have T, Henriques GR, et al. Cognitive therapy for theprevention of suicide attempts: a randomized controlled trial. JAMA2005;294(5):563–70.
7. Slee N, Garnefski N, van der Leeden R, et al. Cognitive-behaviouralintervention for self-harm: randomized controlled trial. Br J Psychiatry2008;192(3):202–11.
8. Linehan MM, Comtois KA, Murray AM, et al. Two-year randomizedcontrolled trial and follow-up of dialectical behavior therapy vs therapyby experts for suicidal behaviors and borderline personality disorder.
Arch Gen Psychiatry 2006;63(7):757–66.9. Hatcher S, Sharon C, Parag V, Collins N. Problem-solving therapy for
people who present to hospital with self-harm: Zelen randomisedcontrolled trial. Br J Psychiatry 2011;199(4):310–6.
10. Bateman A, Fonagy P. Effectiveness of partial hospitalization in thetreatment of borderline personality disorder: a randomized controlledtrial. Am J Psychiatry 1999;156(10):1563–9.
11. Guthrie E, Kapur N, Mackway-Jones K, et al. Randomised controlledtrial of brief psychological intervention after deliberate self-poisoning.BMJ 2001;323(7305):135–8.
12. McMain SF, Links PS, Gnam WH, et al. A randomized trialof dialectical behavior therapy versus general psychiatric managementfor borderline personality disorder. Am J Psychiatry 2009;166(12):136–74.
13. Blum N, St John D, Pfohl B, et al. Systems training for emotionalpredictability and problem solving (STEPPS) for outpatients withborderline personality disorder: a randomized controlled trial and1-year follow-up. Am J Psychiatry 2008;165(4):468–78.
14. Davidson K, Norrie J, Tyrer P, et al. The effectiveness of cognitivebehavior therapy for borderline personality disorder: results from theBorderline Personality Disorder Study of Cognitive Therapy(BOSCOT) trial. J Pers Disord 2006;20(5):450–65.
15. Wood A, Trainor G, Rothwell J, et al. Randomized trial of a grouptherapy for repeated deliberate self-harm in adolescents. J Am AcadChild Adolesc Psychiatry 2001;40(11):1246–53.
16. Huey S, Henggeler S, Rowland M, et al. Multisystemic therapy effectson attempted suicide by youths presenting psychiatric emergencies. JAm Acad Child Adolesc Psychiatry 2004;43(2):183–90.
17. Comtois K, Jones D, O’Connor S, et al. Collaborative assessment andmanagement of suicidality (CAMS): feasibility trial for next-dayappointment services. Depress Anxiety 2011;28(11):963–72.
18. Stewart C, Quinn A, Plever S, Emmerson B. Comparing cognitivebehavior therapy, problem solving therapy, and treatment as usual in ahigh-risk population. Suicide Life Threat Behav 2009;39(5):538–47.
19. Diamond G,WintersteenM, Brown GK, et al. Attachment-based familytherapy for adolescents with suicidal ideation: a randomized controlledtrial. J Am Acad Child Adolesc Psychiatry 2010;49(2):122–31.
20. Unützer J, Tang L, Oishi S, et al. Reducing suicidal ideation in depressedolder primary care patients. J Am Geriatr Soc 2006;54(10):1550–6.
21. Bruce M, Ten Have T, Reynolds Cr, et al. Reducing suicidal ideationand depressive symptoms in depressed older primary care patients: arandomized controlled trial. JAMA 2004;291(9):1081–91.
22. Pearson J, Stanley B, King C, Fisher C. Intervention research withpersons at high risk for suicidality: safety and ethical considerations. JClin Psychiatry 2001;62(25S):S17–S26.
23. Moher D, Schulz KF, Altman DG, CONSORT Group. Consoli-dated standards of reporting trials. Ann Intern Med 2001;134(8):657–62.
24. Crosby AE, Ortega L, Melanson C. Self-directed violence surveillance:uniform definitions and recommended data elements, version 1.0.Atlanta GA: CDC, 2011. www.cdc.gov/violenceprevention/pdf/Self-Directed-Violence-a.pdf.
25. Posner K, Brown GK, Stanley B, et al. The Columbia-Suicide SeverityRating Scale: initial validity and internal consistency findings fromthree multisite studies with adolescents and adults. Am J Psychiatry2011;168(12):1266–77.
26. Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment forsuicidality in schizophrenia: International Suicide Prevention Trial(InterSePT). Arch Gen Psychiatry 2003;60(1):82–91.
27. Hoyert S, Smith B, Murphy S, Kochanek M. Deaths: final data for 1999.Natl Vital Stat Rep 2001;49(8):1–113.
28. CDC, National Center for Injury and Prevention Control. Web-BasedInjury Statistics Query and Reporting System (WISQARS). webappa.cdc.gov/sasweb/ncipc/mortrate10_sy.html.
Brown and Jager-Hyman / Am J Prev Med 2014;47(3S2):S186–S194S194
www.ajpmonline.org