Psychotherapies in Later Life
26
Psychotherapies in Later Life Dr Annette Downey Consultant Psychiatrist, Exeter & cognitive analytic therapist MRCPsych Course, Derriford June 2011
-
Upload
hammett-douglas -
Category
Documents
-
view
30 -
download
1
description
Psychotherapies in Later Life. Dr Annette Downey Consultant Psychiatrist, Exeter & cognitive analytic therapist MRCPsych Course, Derriford June 2011. Therapy is BOTH the Same and Different. Therapy challenges the double pessimism of Old age and mental disorder. How is it Different?. - PowerPoint PPT Presentation
Transcript of Psychotherapies in Later Life

Psychotherapiesin Later Life
Dr Annette DowneyConsultant Psychiatrist, Exeter
& cognitive analytic therapistMRCPsych Course, Derriford
June 2011
Therapy is BOTH the Same and Different
Therapy challenges the double pessimism of Old age and mental
disorder

How is it Different?
• Narcissistic & borderline traits can re-emerge in later life• Self harm• Bereavement & loss• Withdrawal states of pseudo-dementia• Severe disability• Treatment resistant depression• Dementia• Lifelong consequences of early trauma
• These can all adversely affect the thoughts, feelings and behaviour of older people, their families and carers.
Old Dilemmas, Reciprocal roles and idealisations resurface

As can the terror of the threat of illness and the prospect of death
threaten the integrity of self

Cultural and Historical Influences are important
• Adding to the gulf in understanding between the patient and the therapist which is to be bridged through relationship
• With the use of jointly shared language – an example - the state of criticising is understood as ‘chiding’.

Erik Erikson’s Psychosocial developmental tasks of later life
• Emphasized reciprocity across the life course• BOTH young & old need each other if they are to
flourish• The struggle is not just
about life and death but also about all the previous life stages too!
The Seven Ages of WomenHans Baldung GrienMuseum der Bildenden Kunste Leipzig
Ageism
• Psychotherapy for older people challenges negative attitudes and low expectations & prevents collusion.
• The age of ‘decline’• The demographic
timebomb

Therapy Classification
• Specific for older people – usually dementia – Reminiscence therapy, Validation therapy, Reality Orientation
• Generic for all ages – psychodynamic, systemic, cognitive behavioural, interpersonal.

Psychological Treatments used with Older Adults
• Psychoanalytic and psychodynamic – understanding the clinicians reaction
• Systemic – family factors influencing depression• Cognitive behavioural therapy• Interpersonal therapy• Validation therapy• Reminiscence therapy• Cognitive analytic therapy• Problem solving therapy• Dialectical behaviour therapy• Cognitive therapy – aimed at carers improving care skills &
attending to the carers own emotions & reactions• Wilkinson, P: Psychological treatments
• Oxford textbook of Old Age Psychiatry 2008 p241

Common Therapeutic factorsJerome Frank 1961
Persuasion and Healing Baltimore : John Hopkins University Press
• Effect of morale of being attended to by a recognized expert offering a new perspective
• Therapeutic alliance - collaborative• Targeted goals• Guided practice• Specific feedback
• Roth & Fonaghy 1996 reviewed 25 years of psychotherapy research and showed that no one model of therapy works any better than any other.
Roth A & Fonaghy P: 1996 What works for Whom?A critical review of psychotherapy research
NY: Guildford Press

Combination Therapies
• Individual therapy for caregiver and family meetings
• Integrative psychotherapy models• Cognitive analytic therapy – Hepple 2002• Dialectical behaviour therapy – Lynch et al 2007

Indications for psychotherapy
• Patient preference• Augmenting biological treatments• To avoid the useful of harmful medications –
dementia where there is challenging behaviour• Caregiver distress• Psychological problems related to ageing – to
achieve contentment or to resolve family disputes that have happened due to illness of an older family member
• To provide the clinician with a psychological reformulation of the patients problems.
Must take account of Sensory and cognitive changes
• Use technical aids & audiotaping
• Memory aids and other strategies to retain information & skills acquired through therapy
• CBT is being used in the management of patients with established dementia

Unfortunately the provision of psychotherapy for older people is rare and
referral rates are low in the UK – especially in the old older population
Murphy S: (2000)
Provision of psychotherapy services
for older people.
Psychiatric bulletin 24 184-187
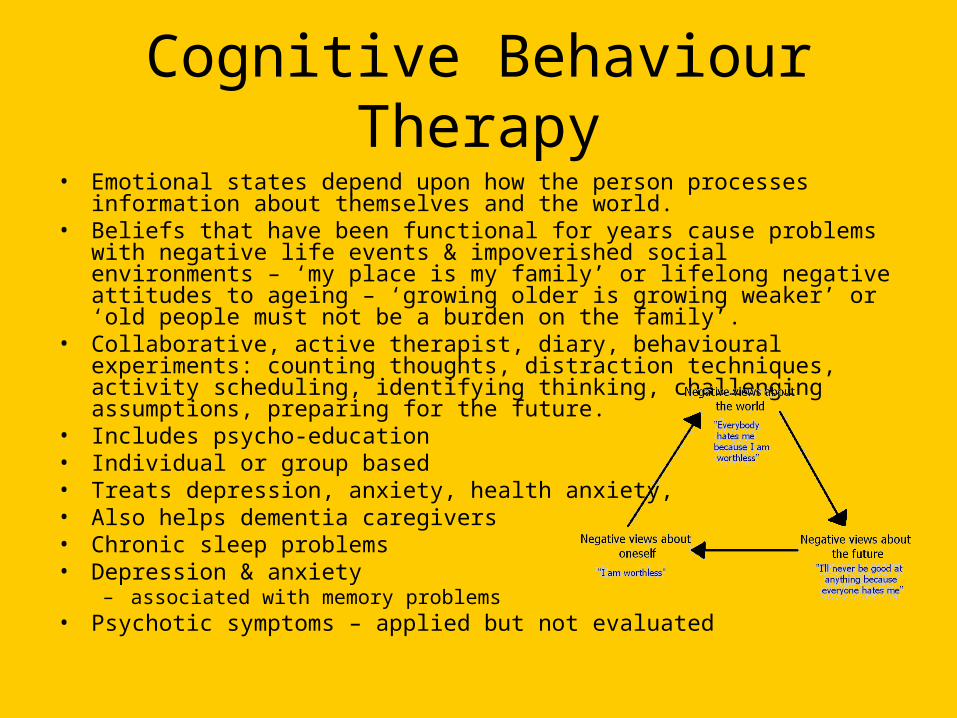
Cognitive Behaviour Therapy• Emotional states depend upon how the person processes information about
themselves and the world.• Beliefs that have been functional for years cause problems with negative life
events & impoverished social environments – ‘my place is my family’ or lifelong negative attitudes to ageing – ‘growing older is growing weaker’ or ‘old people must not be a burden on the family’.
• Collaborative, active therapist, diary, behavioural experiments: counting thoughts, distraction techniques, activity scheduling, identifying thinking, challenging assumptions, preparing for the future.
• Includes psycho-education• Individual or group based• Treats depression, anxiety, health anxiety, • Also helps dementia caregivers• Chronic sleep problems• Depression & anxiety
– associated with memory problems• Psychotic symptoms – applied but not evaluated

Interpersonal Therapy
• Examines the persons distress within an interpersonal context –overlaps with the work of Kitwood (1997) & Stokes (2000)
• Early experiences and unmet attachment needs are seen as important
• Interpersonal inventory of social network & key relationships
• Relevant for late life depression• Distress is conceptualised through:
– Interpersonal disputes (role disputes)– Interpersonal/personality difficulties– Bereavement– Transitions/life events (role transitions)

Systemic Family Therapy
• Aims to foster better relationships between family members within and across generations and to achieve more appropriate support and independence for older family members. Richardson et al 1994
Types of Family Therapy• Structural – Minuchin et al 1967 – the family=the site of the
presenting problems. Families function well with particular structures.
• Strategic Systemic – reframing – the symptom is being maintained by the apparent solution – example: the anxious older man elicits over-protectiveness in the daughter.
• Milan Systemic – Boscolo et al 1987 – multigenerational family patterns; examines the struggles of different family members over several generations; circular questioning
• Contextual – healing of relationships with growth of commitment, trust, & development of loyalty,fairness & reciprocity
• Psycho-educational – especially with carers, reducing expressed emotion, critical comments & hostility

Iveson,C 1990 Whose Life? Community care of Older people & their families
• Three main issues in family therapy with older people – – ‘belongingness’ (being full members of society)– Responsibility for their actions– Capacity to make choices
Therapists need help to empower older adults rather than to over protect them
If we protect older people from themselves we end up making key decisions for them
If we protect older people from their families or neighbours we can be in danger of undermining them.
Yet if we don’t , we may put them at risk

What did Sigmund Freud think of psychotherapy for older people?
Psychodynamic Psychotherapy
– ‘Near or above the age of 50 the elasticity of the mental processes, on which the treatment depends, is as a rule lacking – old people are no longer educable – and on the other hand the mass of material to be dealt with would prolong the duration of the treatment indefinitely’ Freud 1905
– Which he wrote when he was 49!– Offered significantly less often to older people – BUT the
outcomes are often comparable & sometimes better than, for younger patients.
Psycho-dynamically informed mental health services for older people are particular opportunities for containment & reflection

Psychological Interventions in Care homes
• Dementia challenging behaviour – delusions/hallucinations/anxiety/
• depression/apathy/ agitation/aggression/• wandering/ disinhibition• These are common – 60-90% of people with dementia
especially in the later phases of their life.• Psychotropics are associated with stroke, weight gain &
increasing cognitive decline.• The behaviour is often understandable – eg banging the
door because she wants to go home or he calls out frequently in the night – because he wishes to go to the toilet and to get attention of the night nurses.
Non-pharmacological strategies• Reality orientation – rehearsal & physical prompts to improve cognition
related to personal orientation – 6 RCTs, positive cochrane review• Reminiscence therapy – discussion of past experiences – photos, familiar
experiences, sensory items to prompt recall, life story work, increases wellbeing & pleasure - popular-5 RCTs good results but poor quality
• Validation therapy -acceptance of the reality of the person & his/her experience – 3 studies – 2 positive but insufficient evidence for effectiveness – the emotional content of what is being said is important
• Psychomotor therapy – walking/ballgames/dance/ drama 1 trial • Multisensory stimulation – 2 RCTs – insufficent evidence• Cognitive stimulation therapy – 2 cochrane reviews insufficient evidence• Aromatherapy – favourable outcome – 2 RCTs• Music therapy – 5 studies poor quality• Art therapy – self expression, communication,self esteem, new skills• Environment manipulation – cues, signage, building layout, colour, lighting
Animal visitors, dolls, teddy bears, • Behavioural management – functional analysis: antecedants, behaviour,
consequences – 23 studies but poor quality