Evaluation of Pancreatic Lesions that may be interpreted ...papillary formation2 High-grade MCN2 •...
2
In Vivo Microscopy for the Evaluation of Pancreatic Lesions In vivo microscopy (IVM) applies light directly to living tissues to produce images that may be interpreted by a trained pathologist for diagnosis. One important application is imaging of pancreatic lesions via endoscopic procedures. Overview of In-vivo Microscopy Technologies Used for its Evaluation Optical Coherence Topography (OCT) Well- circumscribed dark cystic space with some scattering 1 Mucinous cystic neoplasm 1 Normal pancreatic duct and surrounding parenchyma 3 Normal pancreatic duct with surrounding parenchyma 3 Multiple cysts with highly scattering mucin 1 IPMN 1 Mucinous Cystic Neoplasm Serous cystadenoma Adenocarcinoma Intraductal Papillary Mucinous Neoplasm Honeycomb appearance. Dark cystic spaces divided by white thick septae 1 Serous cystadenoma 1 OCT Images • OCT probes may be passed through the main pancreatic duct and bile duct during endoscopic procedures for the diagnosis of malignant strictures • OCT of a normal main pancreatic duct shows a tri-layer architecture representing the epithelial lining, fibromuscular layer surrounding the epithelium and loose connective tissue / acini surround them 3 • OCT-based IVM provides ultra-sound like cross sectional images at microscopy resolutions (up to a few microns) • OCT provides information about cyst architecture and content for diagnosis of serous and mucinous cysts • Adenocarcinoma involving the main pancreatic duct shows loss of the tri-layered architecture and multiple minute non-reflective areas seen on OCT 3 • OCT can detect main pancreatic duct adenocarcinoma with an accuracy approaching 100% 3 Assessment of Cystic Pancreatic Strictures • Ex-vivo studies show the ability of OCT in differentiating mucinous from serous content of cysts based on the scattering properties of the cyst contents • Cross sectional imaging using OCT allows for assessment of cyst size, wall thickness and extent of septation for differentiation of serous and mucinous cysts Assessment of Malignant Pancreaticobiliary Strictures
Transcript of Evaluation of Pancreatic Lesions that may be interpreted ...papillary formation2 High-grade MCN2 •...

In Vivo Microscopy for the Evaluation of Pancreatic LesionsIn vivo microscopy (IVM) applies light directly to living tissues to produce images that may be interpreted by a trained pathologist for diagnosis. One important application is imaging of pancreatic lesions via endoscopic procedures.
Overview of In-vivo Microscopy Technologies Used for its Evaluation
Optical Coherence Topography (OCT)
In Vivo Microscopy for the Evaluation of Pancreatic Lesions
© 2018 College of American Pathologists. All rights reserved. 26630.0518
cap.org
In vivo microscopy (IVM) applies light directly to living tissues to produce images that may be interpreted by a trained pathologist for diagnosis. One important application is imaging of pancreatic lesions via endoscopic procedures.
Optical Coherence Tomography (OCT)
• OCT-based IVM provides ultra-sound like cross sectional images at microscopic resolutions (up to a few microns).• OCT provides information about cyst architecture and content for diagnosis of serous and mucinous cysts.
Needle-Based Confocal Endomicroscopy (nCLE)
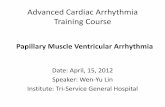
• In needle-based endomicroscopy, an optical probe is passed through a 19-gauge needle during endoscopicultrasound,fineneedle aspiration (EUS-FNA) procedures and produces images in concert with injected Fluorescein contrast. • The probe is placed directly against the cyst wall.•Vascularandepithelialfluorescence and patterns allow for diagnosis of various pancreatic lesions.
Fluorescent Agents Used in CLE
Appearance of tissue using CLE often depends on the contrast agent used.• The widespread use of injectable contrastagentssuchasfluorescein has led to the development of diagnostic criteria based on vascular architecture and hemo-dynamics.• “Leaky vessels” showing leakage of fluorescentagentusually signify malignancy. •Topicalfluorescentagentssuchas acriflavineandproflavinestain nuclei and allow for assessment of nuclear morphology, distribution, and size analogous to classic histopathology.• Research in in-vivo molecular fluorophoresthatarespecificfor pancreatic adenocarcinoma may increasesensitivityandspecificityof in-vivo diagnoses using CLE.1
Overview of In-vivo Microscopy Technologies Used for its Evaluation
“Fern pattern” of vascularity2
Serous cystadenoma2
Horizon-like bands with incomplete papillary
formation2
High-grade MCN2
• Papillarystructuresareeasilyidentifiedusingprobe-basedCLEinintraductalpapillarymucinouscystadenomas• CLEprobesallowthevisualizationofasuperficialvascularnetworkinthecystwallsofserouscystadenomas,asignthatis highlyspecificforthedisease• Ex-vivo studies show the ability of OCT in differentiating mucinous from serous content of cysts based on the scattering properties of the cyst contents. • Cross-sectional imaging using OCT allows for assessment of cyst size, wall thickness, and extent of septation for differentiation of serous and mucinous cysts
Well-circumscribed
dark cystic space with some
scattering1
Mucinous cystic neoplasm1
Normal pancreatic duct and
surrounding parenchyma3
Normal pancreatic duct with
surrounding parenchyma3
Multiple cysts with highly
scattering mucin1
IPMN1
Text References1. Li H, Li Y, Cui L, et al. Monitoring pancreatic carcinogenesis by the molecular imaging of cathepsin E in vivo using confocal laser endomicroscopy. PLoSOne.2014;9(9):e106566.2.MeiningA,ShahR,SlivkaA,etal.Classificationofprobe- basedconfocallaserendomicroscopyfindingsin pancreaticobiliary strictures. Endoscopy. 2012;44(03): 251-257.3. Testoni PA, Mangiavillano B. Optical coherence tomography in detection of dysplasia and cancer of the gastrointestinal tract and bilio-pancreatic ductal system. World Journal of Gastroenterology: WJG. 2008;14(42):6444.4.CaillolF,FilocheB,GaidhaneM,KahalehM.Refined probe-basedconfocallaserendomicroscopyclassificationfor biliarystrictures:theParisClassification.Digestive diseases and sciences. 2013;58(6):1784-1789.Image References1. Nicusor Iftimia, Sevdenur Cizginer, Vikram Deshpande, Martha Pitman, Servet Tatli, Nicolae-Adrian Iftimia, Daniel X Hammer, Mircea Mujat, Teoman Ustun, R. Daniel Ferguson, and William R. Brugge, “Differentiation of pancreatic cysts with optical coherence tomography (OCT) imaging: an ex vivo pilot study,” Biomed. Opt. Express 2, 2372-2382 (2011).*2. Somashekar G Krishna, Rohan M Modi, Amrit K Kamboj, Benjamin J Swanson, Phil A Hart, Mary E Dillhoff, Andrei Manilchuk, Carl R Schmidt, Darwin L Conwell, “In vivo and ex vivo confocal endomicroscopy of pancreatic cystic lesions: A prospective study.” World J Gastroenterol. May 14, 2017; 23(18): 3338-33483. van Manen L. Stegehuis PL, Farina-Sarasqueta A, de Haan LM, Eggermont j, Bonsing BA, et al. (2017) Validation of full- fieldopticalcoherencetomographyindistinguishingmalignant and benign tissue in resected pancreatic cancer specimens. PLoS ONE 12(4): e0175862.
For information about the open access license, please refer to http://journals.plos.org/plosone/s/licenses-and-copyright.
*For the Iftimia images without captions: Biomed. Opt. Express 2, 2372 (2011)
Assessment of Malignant Pancreaticobiliary Strictures
• OCT and CLE probes may be passed through the main pancreatic duct and bile duct during endoscopic procedures for the diagnosis of malignant strictures• With CLE, criteria suggestive of a malignant stricture involving a pancreatic or biliary duct include: – Thick dark bands (>40 microns)2, 3, 4
– Thick, white bands (>20 microns)2, 3, 4
– Dark Clumps2, 3, 4
– Fluorescein leakage2, 3, 4
• CLEpredictsneoplasiainvolvingthepancreatico-biliaryductswithasensitivityandspecificityof83%and75%(comparedto 65%and53%usingcytology)respectively3
• OCTofanormalmainpancreaticductshowsatri-layerarchitecturerepresentingtheepitheliallining,fibromuscularlayer surrounding the epithelium, and loose connective tissue / acini surrounding them3
• Adenocarcinomainvolvingthemainpancreaticductshowslossofthetri-layeredarchitectureandmultipleminutenon-reflective areas seen on OCT3
• OCTcandetectmainpancreaticductadenocarcinomawithanaccuracyapproaching100%3
Serous cystadenoma
Mucinous Cystic Neoplasm
Adenocarcinoma
Intraductal Papillary Mucinous Neoplasm
Complete“finger-like” papillary
projections with vacular cores
(lamina propia)2
IPMN, gastric subtype with high- grade dysplasia2
Assessment of Cystic Pancreatic Structures
Mucinous Cystic Neoplasm
Serous cystadenoma
Adenocarcinoma
Intraductal Papillary Mucinous Neoplasm
Honeycomb appearance. Dark cystic
spaces divided by white thick
septae1
Serous cystadenoma1
CLE Images
OCT Images
• OCT probes may be passed through the main
pancreatic duct and bile duct during endoscopic
procedures for the diagnosis of malignant strictures
• OCT of a normal main pancreatic duct shows a tri-layer architecture representing the epithelial lining, fibromuscular layer surrounding the epithelium and loose connective tissue / acini surround them3
• OCT-based IVM provides ultra-sound like cross sectional images at microscopy resolutions (up to a few microns)
• OCT provides information about cyst architecture and content for diagnosis of serous and mucinous cysts
• Adenocarcinoma involving the main pancreatic duct shows loss of the tri-layered architecture and multiple minute non-reflective areas seen on OCT3
• OCT can detect main pancreatic duct adenocarcinoma with an accuracy approaching 100%3
Assessment of Cystic Pancreatic Strictures
• Ex-vivo studies show the ability of OCT in differentiating mucinous from serous content of cysts based on the scattering properties of the cyst contents• Cross sectional imaging using OCT allows for assessment of cyst size, wall thickness and extent of septation for differentiation of serous and mucinous cysts
Assessment of Malignant Pancreaticobiliary Strictures

In Vivo Microscopy for the Evaluation of Pancreatic Lesions
© 2018 College of American Pathologists. All rights reserved. 26630.0518
cap.org
In vivo microscopy (IVM) applies light directly to living tissues to produce images that may be interpreted by a trained pathologist for diagnosis. One important application is imaging of pancreatic lesions via endoscopic procedures.
Optical Coherence Tomography (OCT)
• OCT-based IVM provides ultra-sound like cross sectional images at microscopic resolutions (up to a few microns).• OCT provides information about cyst architecture and content for diagnosis of serous and mucinous cysts.
Needle-Based Confocal Endomicroscopy (nCLE)
• In needle-based endomicroscopy, an optical probe is passed through a 19-gauge needle during endoscopicultrasound,fineneedle aspiration (EUS-FNA) procedures and produces images in concert with injected Fluorescein contrast. • The probe is placed directly against the cyst wall.•Vascularandepithelialfluorescence and patterns allow for diagnosis of various pancreatic lesions.
Fluorescent Agents Used in CLE
Appearance of tissue using CLE often depends on the contrast agent used.• The widespread use of injectable contrastagentssuchasfluorescein has led to the development of diagnostic criteria based on vascular architecture and hemo-dynamics.• “Leaky vessels” showing leakage of fluorescentagentusually signify malignancy. •Topicalfluorescentagentssuchas acriflavineandproflavinestain nuclei and allow for assessment of nuclear morphology, distribution, and size analogous to classic histopathology.• Research in in-vivo molecular fluorophoresthatarespecificfor pancreatic adenocarcinoma may increasesensitivityandspecificityof in-vivo diagnoses using CLE.1
Overview of In-vivo Microscopy Technologies Used for its Evaluation
“Fern pattern” of vascularity2
Serous cystadenoma2
Horizon-like bands with incomplete
papillary formation2
High-grade MCN2
• Papillarystructuresareeasilyidentifiedusingprobe-basedCLEinintraductalpapillarymucinouscystadenomas• CLEprobesallowthevisualizationofasuperficialvascularnetworkinthecystwallsofserouscystadenomas,asignthatis highlyspecificforthedisease• Ex-vivo studies show the ability of OCT in differentiating mucinous from serous content of cysts based on the scattering properties of the cyst contents. • Cross-sectional imaging using OCT allows for assessment of cyst size, wall thickness, and extent of septation for differentiation of serous and mucinous cysts
Well-circumscribed
dark cystic space with some
scattering1
Mucinous cystic neoplasm1
Normal pancreatic duct and
surrounding parenchyma3
Normal pancreatic duct with
surrounding parenchyma3
Multiple cysts with highly
scattering mucin1
IPMN1
Text References1. Li H, Li Y, Cui L, et al. Monitoring pancreatic carcinogenesis by the molecular imaging of cathepsin E in vivo using confocal laser endomicroscopy. PLoSOne.2014;9(9):e106566.2.MeiningA,ShahR,SlivkaA,etal.Classificationofprobe- basedconfocallaserendomicroscopyfindingsin pancreaticobiliary strictures. Endoscopy. 2012;44(03): 251-257.3. Testoni PA, Mangiavillano B. Optical coherence tomography in detection of dysplasia and cancer of the gastrointestinal tract and bilio-pancreatic ductal system. World Journal of Gastroenterology: WJG. 2008;14(42):6444.4.CaillolF,FilocheB,GaidhaneM,KahalehM.Refined probe-basedconfocallaserendomicroscopyclassificationfor biliarystrictures:theParisClassification.Digestive diseases and sciences. 2013;58(6):1784-1789.Image References1. Nicusor Iftimia, Sevdenur Cizginer, Vikram Deshpande, Martha Pitman, Servet Tatli, Nicolae-Adrian Iftimia, Daniel X Hammer, Mircea Mujat, Teoman Ustun, R. Daniel Ferguson, and William R. Brugge, “Differentiation of pancreatic cysts with optical coherence tomography (OCT) imaging: an ex vivo pilot study,” Biomed. Opt. Express 2, 2372-2382 (2011).*2. Somashekar G Krishna, Rohan M Modi, Amrit K Kamboj, Benjamin J Swanson, Phil A Hart, Mary E Dillhoff, Andrei Manilchuk, Carl R Schmidt, Darwin L Conwell, “In vivo and ex vivo confocal endomicroscopy of pancreatic cystic lesions: A prospective study.” World J Gastroenterol. May 14, 2017; 23(18): 3338-33483. van Manen L. Stegehuis PL, Farina-Sarasqueta A, de Haan LM, Eggermont j, Bonsing BA, et al. (2017) Validation of full- fieldopticalcoherencetomographyindistinguishingmalignant and benign tissue in resected pancreatic cancer specimens. PLoS ONE 12(4): e0175862.
For information about the open access license, please refer to http://journals.plos.org/plosone/s/licenses-and-copyright.
*For the Iftimia images without captions: Biomed. Opt. Express 2, 2372 (2011)
Assessment of Malignant Pancreaticobiliary Strictures
• OCT and CLE probes may be passed through the main pancreatic duct and bile duct during endoscopic procedures for the diagnosis of malignant strictures• With CLE, criteria suggestive of a malignant stricture involving a pancreatic or biliary duct include: – Thick dark bands (>40 microns)2, 3, 4
– Thick, white bands (>20 microns)2, 3, 4
– Dark Clumps2, 3, 4
– Fluorescein leakage2, 3, 4
• CLEpredictsneoplasiainvolvingthepancreatico-biliaryductswithasensitivityandspecificityof83%and75%(comparedto 65%and53%usingcytology)respectively3
• OCTofanormalmainpancreaticductshowsatri-layerarchitecturerepresentingtheepitheliallining,fibromuscularlayer surrounding the epithelium, and loose connective tissue / acini surrounding them3
• Adenocarcinomainvolvingthemainpancreaticductshowslossofthetri-layeredarchitectureandmultipleminutenon-reflective areas seen on OCT3
• OCTcandetectmainpancreaticductadenocarcinomawithanaccuracyapproaching100%3
Serous cystadenoma
Mucinous Cystic Neoplasm
Adenocarcinoma
Intraductal Papillary Mucinous Neoplasm
Complete“finger-like” papillary
projections with vacular cores
(lamina propia)2
IPMN, gastric subtype with high- grade dysplasia2
Assessment of Cystic Pancreatic Structures
Mucinous Cystic Neoplasm
Serous cystadenoma
Adenocarcinoma
Intraductal Papillary Mucinous Neoplasm
Honeycomb appearance. Dark cystic
spaces divided by white thick
septae1
Serous cystadenoma1
CLE Images
OCT Images
Text References1. Li H, Li Y, Cui L, et al. Monitoring pancreatic carcinogenesis by the molecular imaging of cathepsin E in vivo using confocal laser endomicroscopy. PLoS One. 2014;9(9):e106566.2. Meining A, Shah R, Slivka A, et al. Classification of probe-based confocal laser endomicroscopy findings in pancreaticobiliary strictures. Endoscopy. 2012;44(03):251-257.3. Testoni PA, Mangiavillano B. Optical coherence tomography in detection of dysplasia and cancer of the gastrointestinal tract and bilio-pancreatic ductal system. World journal of gastroenterology: WJG. 2008;14(42):6444.4. Caillol F, Filoche B, Gaidhane M, Kahaleh M. Refined probe-based confocal laser endomicroscopy classification for biliary strictures: the Paris Classification. Digestive diseases and sciences. 2013;58(6):1784-1789.Image References1. Nicusor Iftimia, Sevdenur Cizginer, Vikram Deshpande, Martha Pitman, Servet Tatli, Nicolae-Adrian Iftimia, Daniel X Hammer, Mircea Mujat, Teoman Ustun, R. Daniel Ferguson, and William R. Brugge, “Differentiation of pancreatic cysts with optical coherence tomography (OCT) imaging: an ex vivo pilot study,” Biomed. Opt. Express 2, 2372-2382 (2011).*2. Somashekar G Krishna, Rohan M Modi, Amrit K Kamboj, Benjamin J Swanson, Phil A Hart, Mary E Dillhoff, Andrei Manilchuk, Carl R Schmidt, Darwin L Conwell, “In vivo and ex vivo confocal endomicroscopy of pancreatic cystic lesions: A prospective study,” World J Gastroenterol. May 14, 2017; 23(18): 3338-33483. van Manen L. Stegehuis PL, Farina-Sarasqueta A, de Haan LM, Eggermont j, Bonsing BA, et al. (2017) Validation of full-field optical coherence tomography in distinguishing malignant and benign tissue in resected pancreatic cancer specimens. PLoS ONE 12(4): e0175862. For information about the open access license, please refer to http://journals.plos.org/plosone/s/licenses-and-copyright.*For the Iftimia images without captions: Biomed. Opt. Express 2, 2372 (2011)
© 2018 College of American Pathologists. All rights reserved. cap.org
• In needle-based endomicroscopy, an optical probe is passed through a 19-gauge needle during endoscopic ultrasound, fine needle aspiration (EUS-FNA) procedures and produces images in concert with injected Fluorescein contrast.• The probe is placed directly against the cyst wall.• Vascular and epithelial fluorescence and patterns allow for diagnosis of various pancreatic lesions.
Fluorescent Agents Used in CLE
Appearance of tissue using CLE often depends on the contrast agent used.
Assessment of Cystic Pancreatic Structures
• Papillary structures are easily identified using probe-based CLE in intraductal papillary mucinous Neoplas
• CLE probes allow the visualization of a superficial vascular network in the cyst walls of serous cystadenomas, a sign that is highly specific for the disease
Needle-Based Confocal Endomicroscopy (nCLE)
• The widespread use of injectable contrast agents such as fluorescein has led to the development of diagnostic criteria based on vascular architecture and hemo-dynamics.
• “Leaky vessels” showing leakage of fluorescent agents usually signify malignancy.
• Topical fluorescent agents such as acriflavine and proflavine stain nuclei allow for assessment of nuclear morphology, distribution and size analogous to classic histopathology.
• Research in in-vivo molecular fluoroprobes that are specific for pancreatic adenocarcinoma may increase sensitivity and specificity of in-vivo diagnoses using CLE.1
• CLE probes may be passed through the main pancreatic duct and bile duct during endoscopic procedures for the diagnosis of malignant strictures
• Criteria suggestive of a malignant stricture involving a pancreatic or biliary duct include:o Thick dark bands (>40 microns)2, 3, 4
o Thick white bands (>20 microns) 2, 3, 4
o Dark Clumps2, 3, 4
o Fluorescein leakage2, 3, 4
• CLE predicts neoplasia involving the pancreaticobiliary ducts with a sensitivity and specificity of 83% and 75% (compared to 65% and 53% using cytology), respectively3
Assessment of Malignant Pancreaticobiliary Structures