papillary thyroid carcinoma ppt
86
5 1
-
Upload
tariq-maka -
Category
Health & Medicine
-
view
79 -
download
4
Transcript of papillary thyroid carcinoma ppt

5
1
DR TARIQUE AHMED MAKAREGISTRAR ENT
Management of Complicated Papillary Thyroid Carcinoma
2
3
CASE I PRESENTATION
Management of Complicated Papillary Thyroid Carcinoma
Patient Profile
Name XYZ
Age 70 years
Gender Male
Residence Chakwal
Date of admission 15.04.13
4
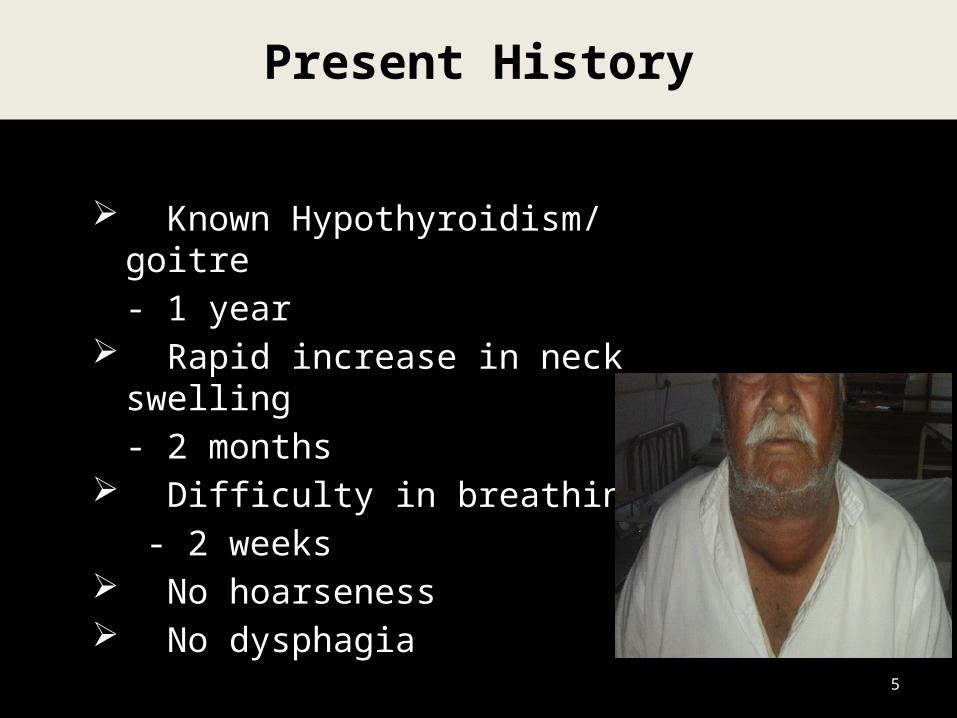
Present History
Known Hypothyroidism/ goitre- 1 year
Rapid increase in neck swelling- 2 months
Difficulty in breathing - 2 weeks
No hoarseness No dysphagia
5
History- cont’d…
Past history Known case of DM, HypertensionHad been op for Fr femur 2 yrs ago
Personal history
Poor socioeconomic class, smoker
Family history
Not positive for thyroid diseases 6

General Physical Examination
Vital signs
Pulse : 84/min
BP : 135/90mmHg
R/ R : 19/min
Temp : 98.4°F
7
General Physical Examination
Pallor Jaundice Negative Cyanosis Lymph nodes Not palpable Clubbing Koilonychia Negative Oedema
8
Systemic Examination
Cardiovascular system
Respiratory system
Gastrointestinal system
Central nervous system
9
NAD

ENT Examination
Neck
Massive multinodular swelling
Inferior extent could not be assessed
Moved on swallowing
Normothermic, non tender
Mobile overlying skin
No bruit10
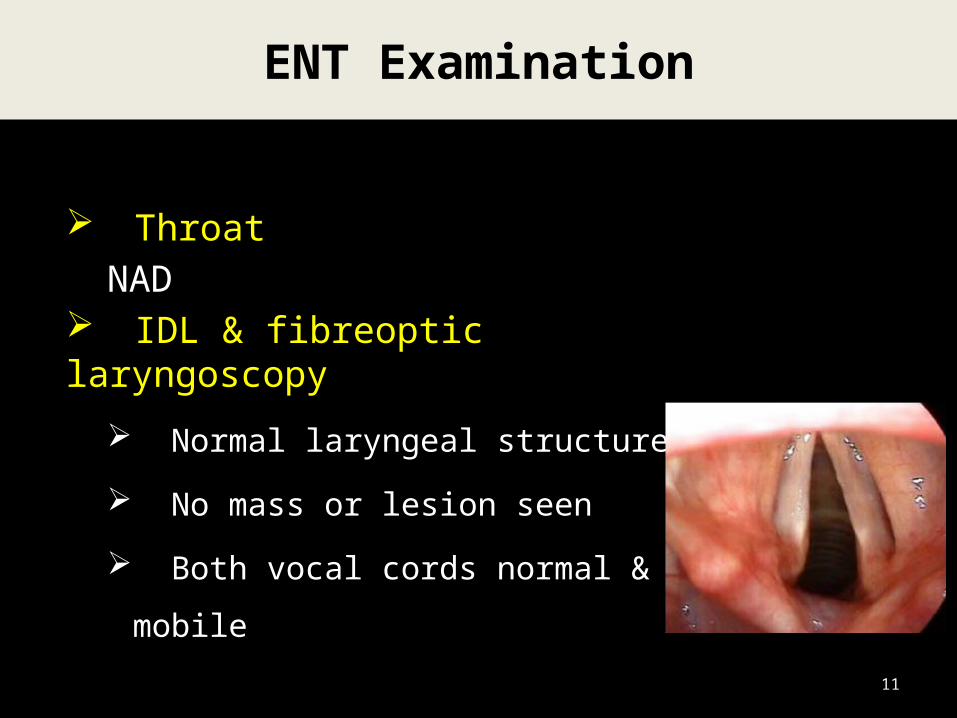
ENT Examination
ThroatNAD
IDL & fibreoptic laryngoscopy
Normal laryngeal structures
No mass or lesion seen
Both vocal cords normal &
mobile11
ENT Examination
Ear
Nose NAD
Oral cavity
12
Provisional Diagnosis
MULTI-NODULAR GOITER
WITH TRACHEAL COMPRESSION
13
Shift to ENT care
Nurse in propped up position
Observation & continuous monitoring
of vitals & SpO2
Immediate management
14
Thyroid profile - WNL
FNAC
Thyroid Scan
CT scan Neck
Carotid Doppler USG
Investigations
15
16
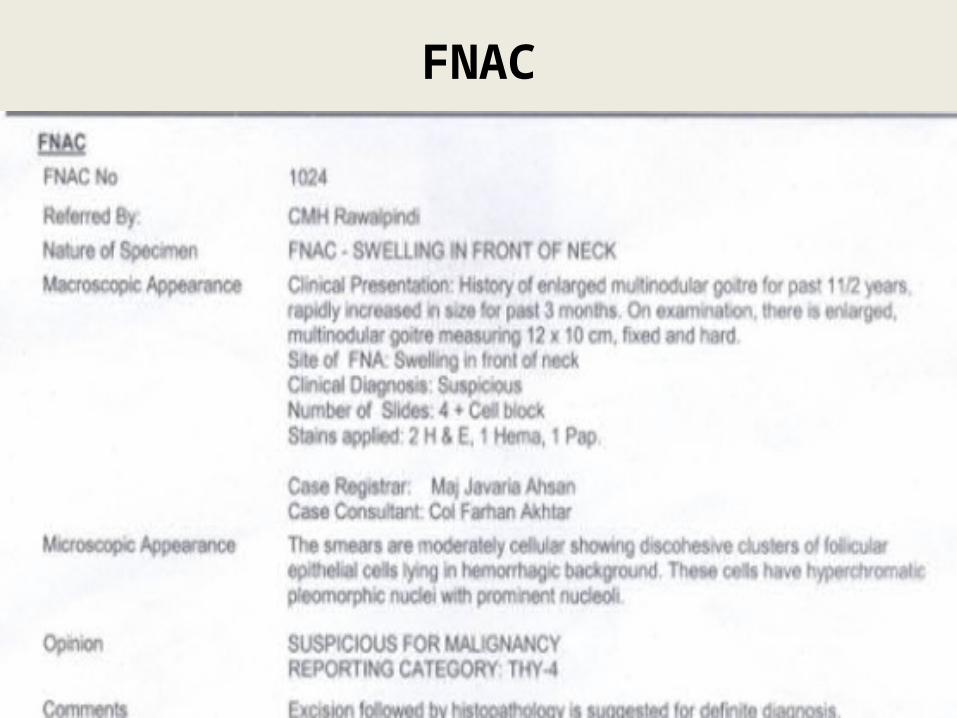
FNAC

17
Thyroid Scan
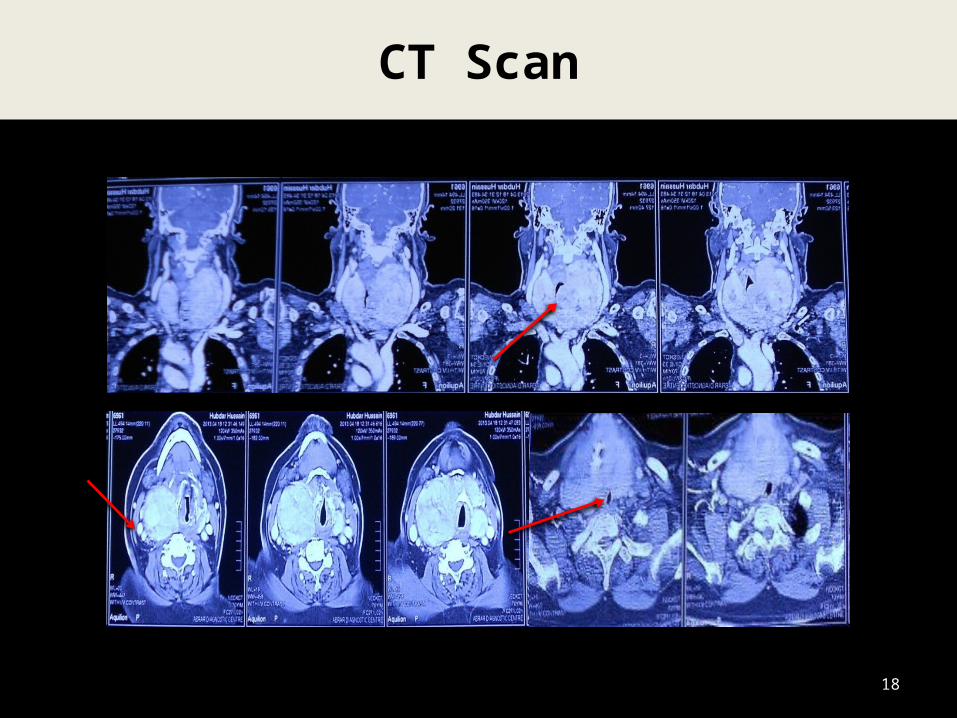
CT Scan
18
Enlarged thyroid gland with multiple nodules displacing the vessels (with normal flow)
Carotid Doppler USG
19
Final Diagnosis
MNG WITH SUSPICION OF MALIGNANCY
20

Management Plan
TOTAL THYROIDECTOMY
21
Pre Op Investigations
Blood complete picture Urine RE Serum urea & electrolytes PT, PTTK LFTs Blood Glucose levels ECG , 2-D echo X-Ray Chest
22
Within normal limits
Pre Op Work Up
Counseling
Informed written consent
Pre-anesthesia assessment ASA-IV
02 Units RCC arranged
NPO over night
23

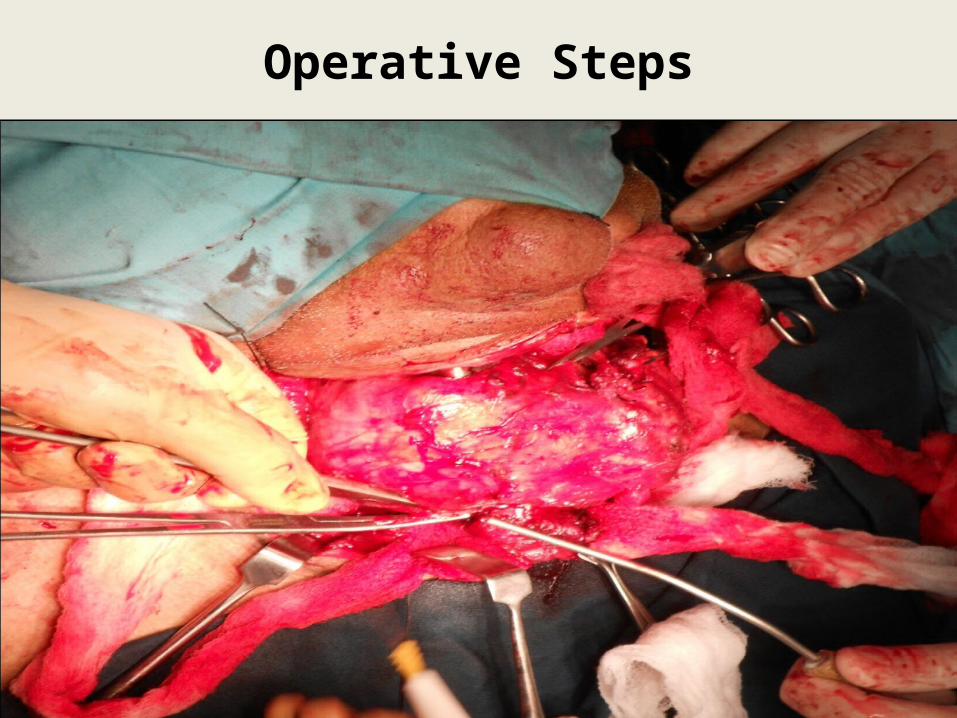
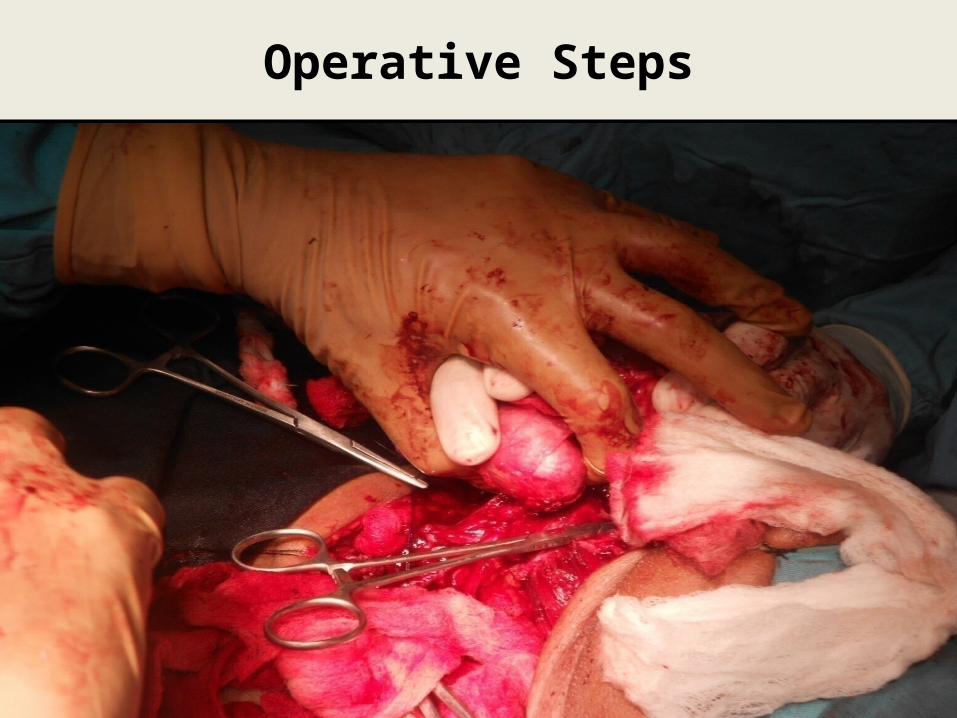
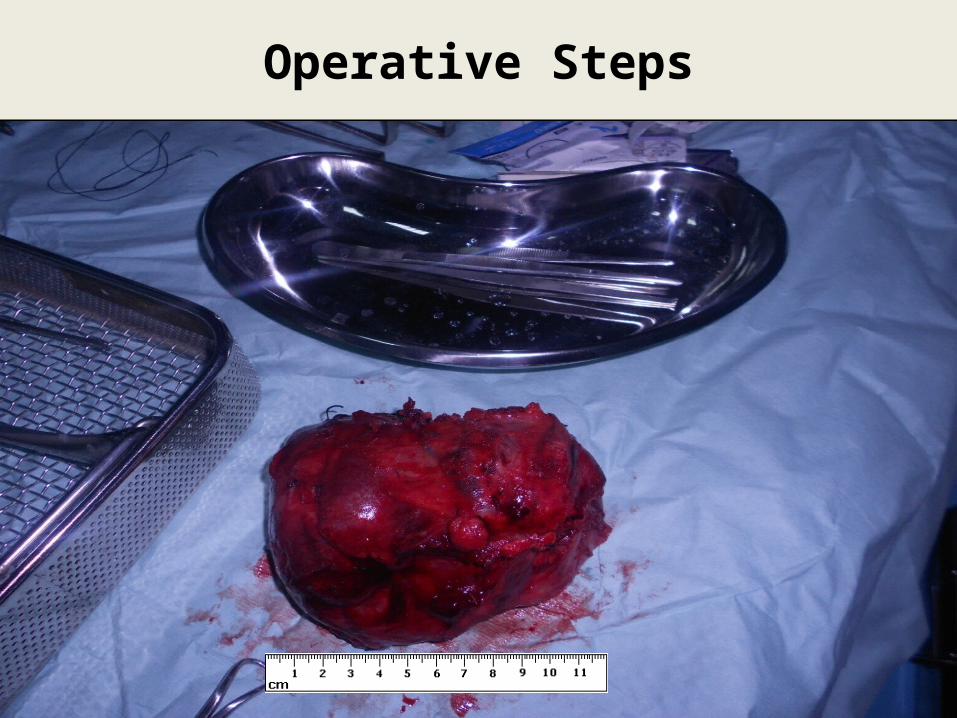
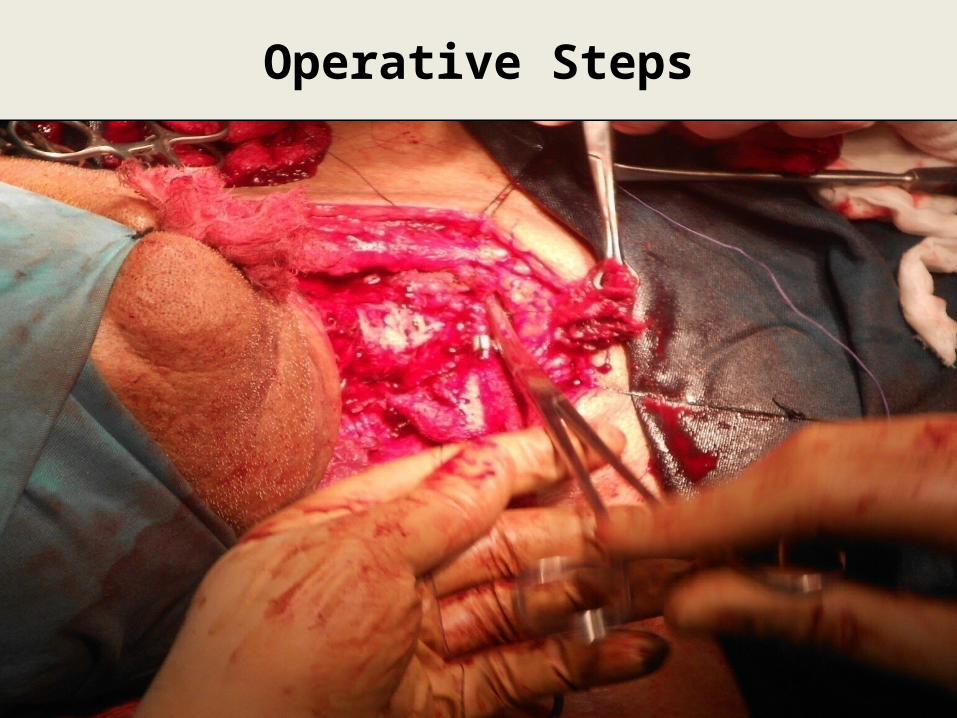
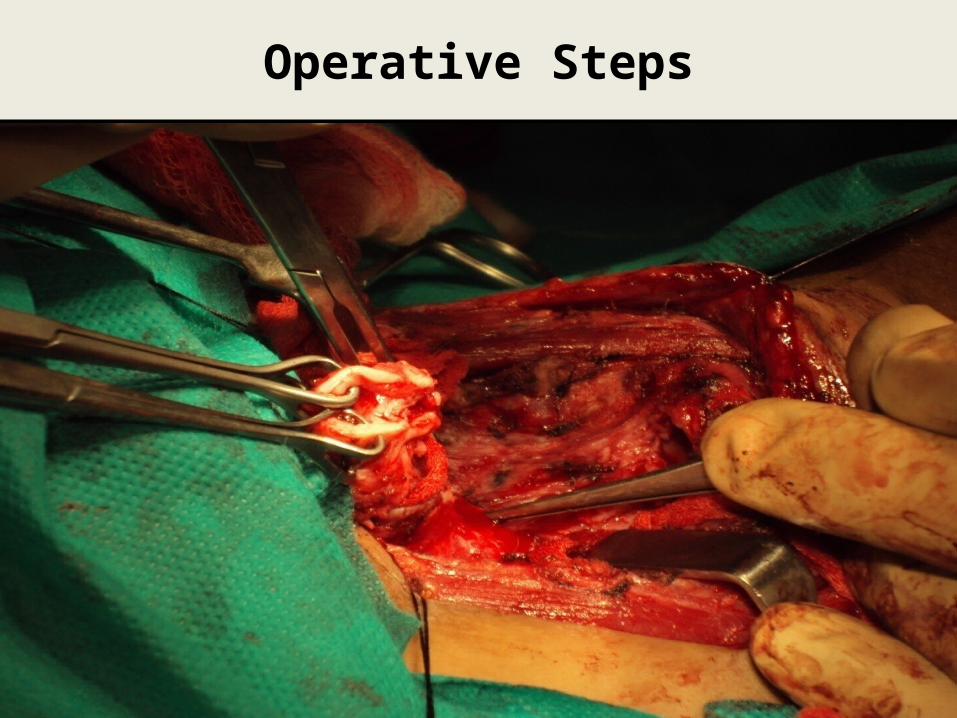
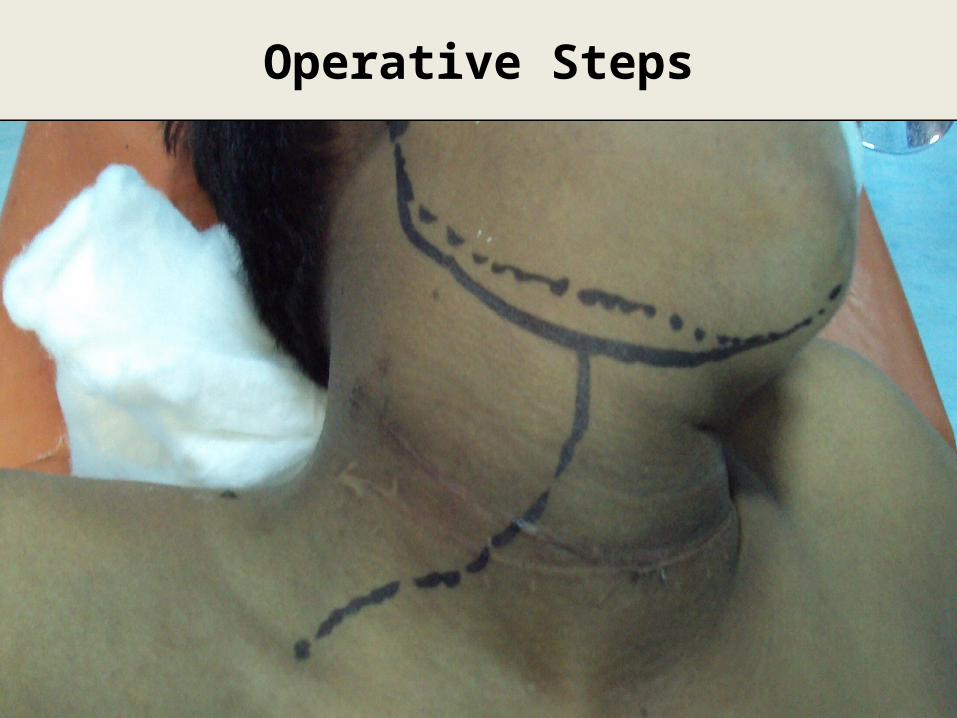
OPERATIVE STEPS
Operative Steps
25 25

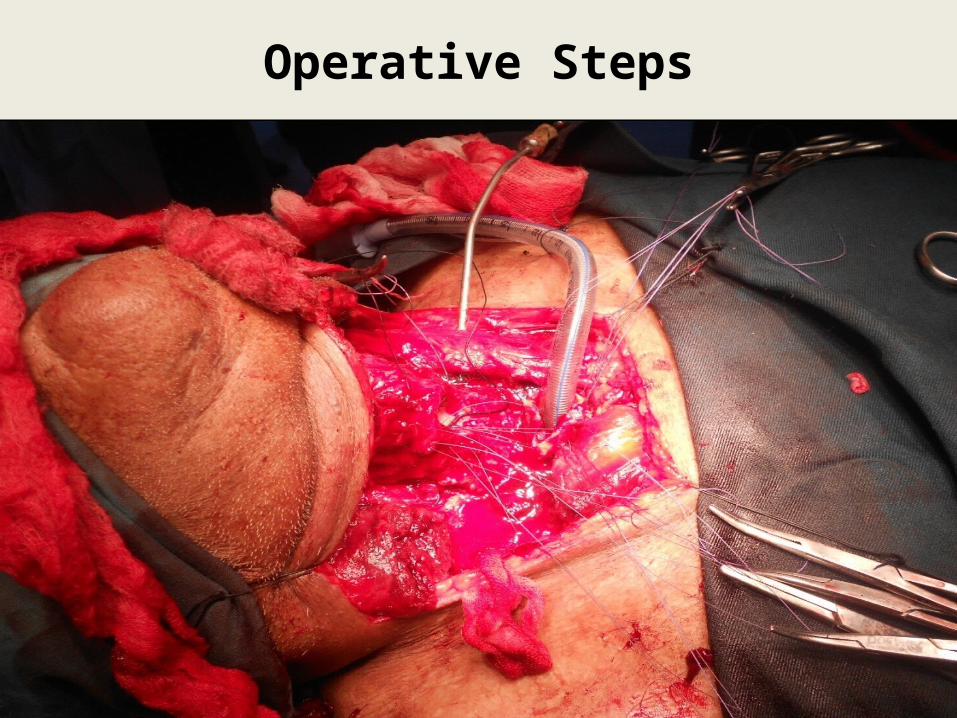
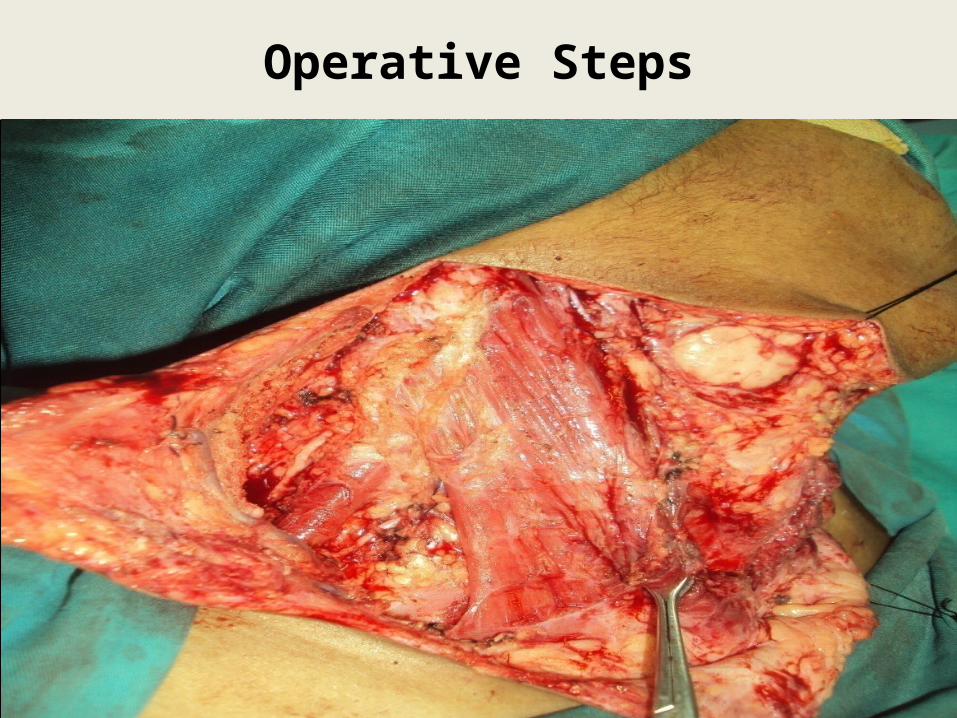
Operative Steps
26
Operative Steps
27
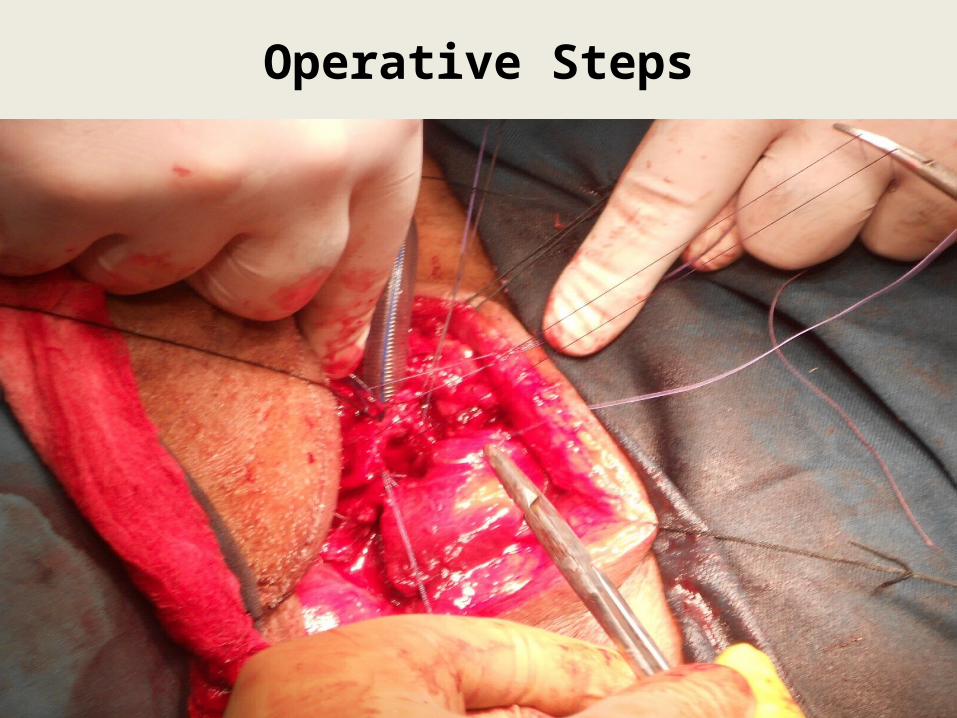
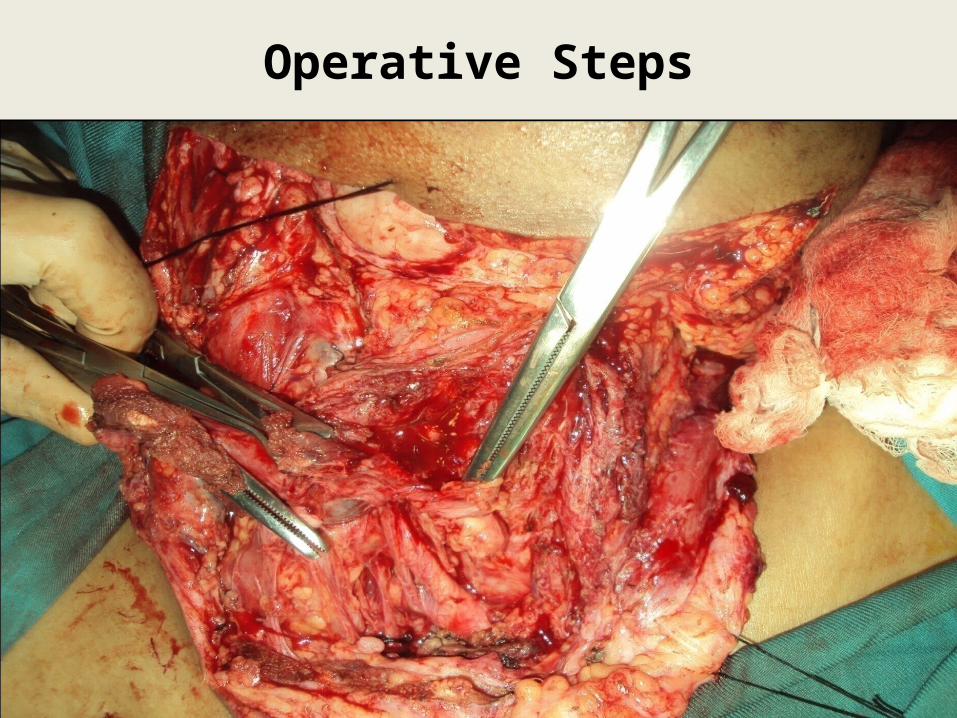
Operative Steps
28

Operative Steps
29 29
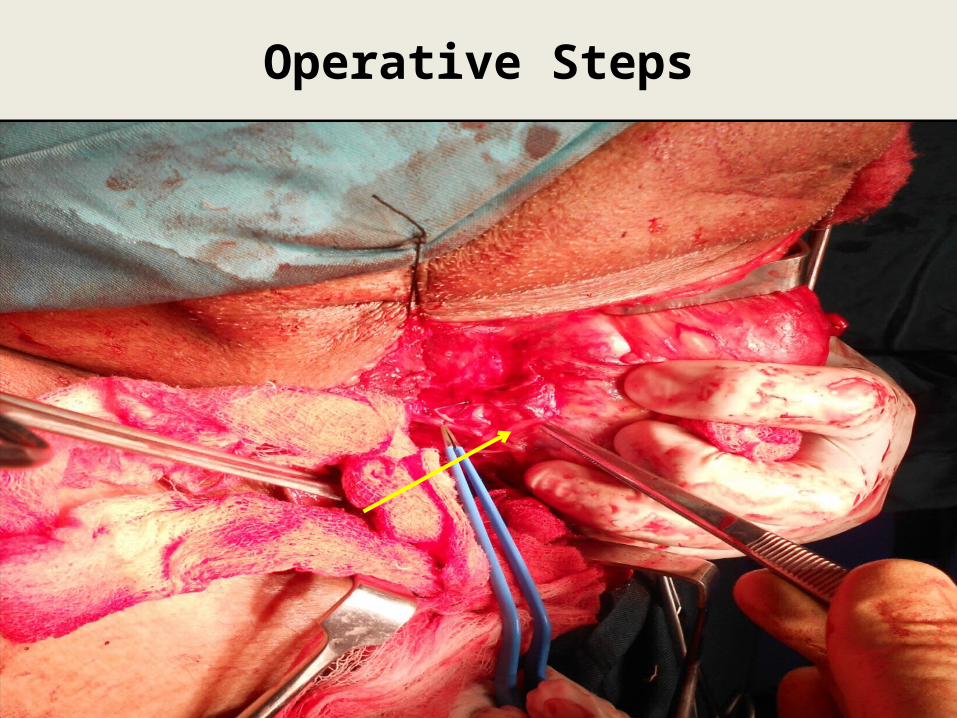
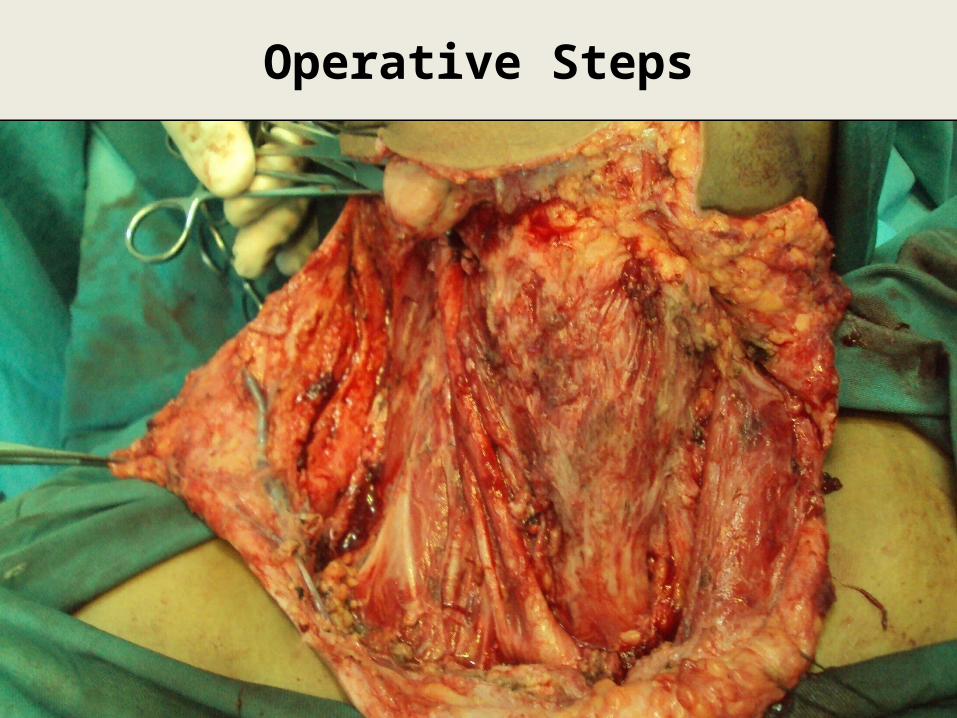
Operative Steps
30 30
Operative Steps
31 31
Operative Steps
32 32
Operative Steps
33 33
Operative Steps
34 34

Operative Steps
35 35
Operative Steps
36

Operative Steps
37
Operative Steps
38 38
Operative Steps
39
Post OP Management
Nursed in ITC
Inj Ceftriaxone 1g I/V 12 hourly (ATD)
Inj Coamoxiclav 1.2g I/V 8 hourly (ATD)
Inj Ketorolac 30mg I/V 08 hourly
Inj Dexamethasone 8 mg I/V 08 hourly
Inj Ca Gluconate 10 mg I/V 08 hourly
40
Post OP Management
41
7th Post op day
- Shifted to ward
10th Post op day
- Fibreoptic laryngoscopy
- Decannulation
14th Post op day
- Grillo’s sutures removed
42
CASE II PRESENTATION
Management of Complicated Papillary Thyroid Carcinoma
Patient Profile
Name XYZ
Age 23 years
Gender Male
Profession Serving
DOA 23.01.2013
43

Case Summary
Painless swelling on Rt side neck
Metastatic Papillary Thyroid Ca on FNAC
Nodule Rt lobe thyroid & Rt Metastatic lymph
nodes Level III, V on CT
Near Total Thyroidectomy with ‘Berry picking’
Cervical Nodes (Rt) 44
45
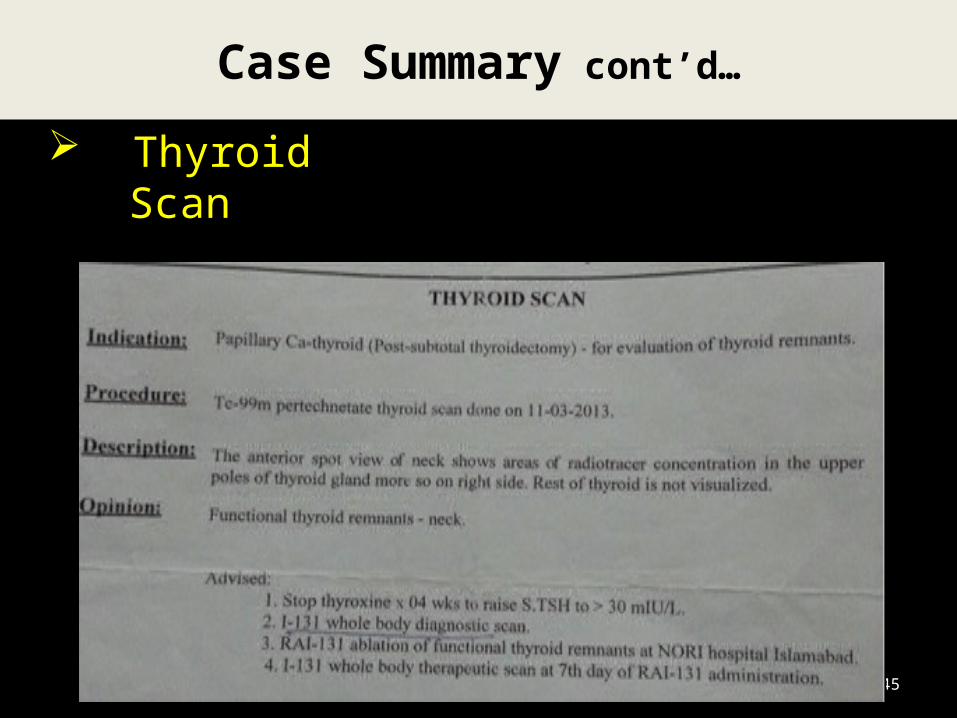
Case Summary cont’d…
Thyroid Scan
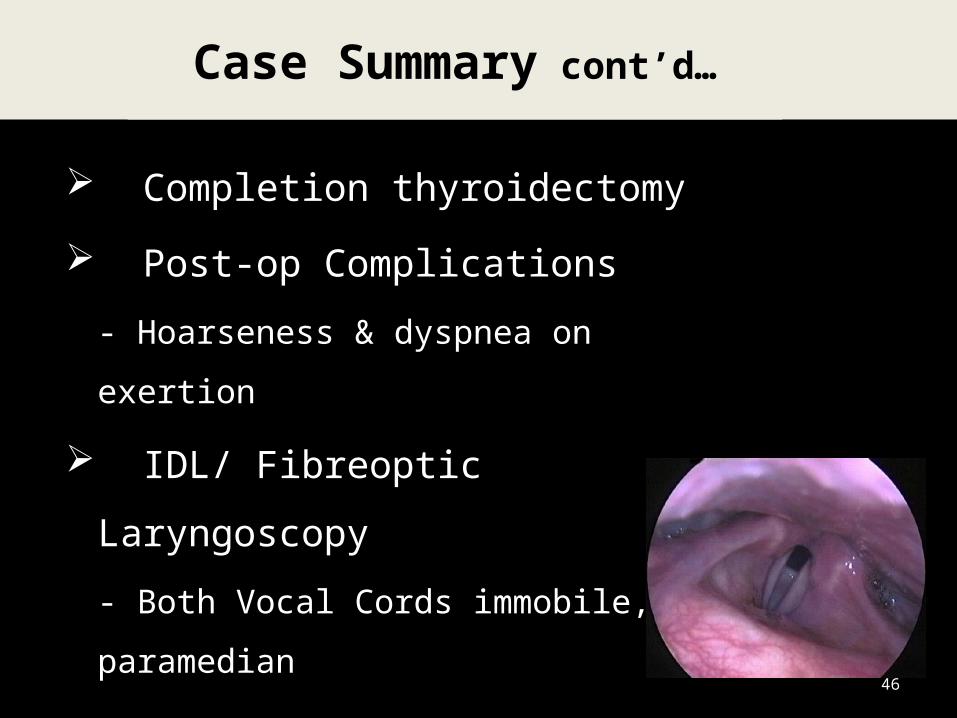
Completion thyroidectomy
Post-op Complications
- Hoarseness & dyspnea on
exertion
IDL/ Fibreoptic Laryngoscopy
- Both Vocal Cords immobile,
paramedian46
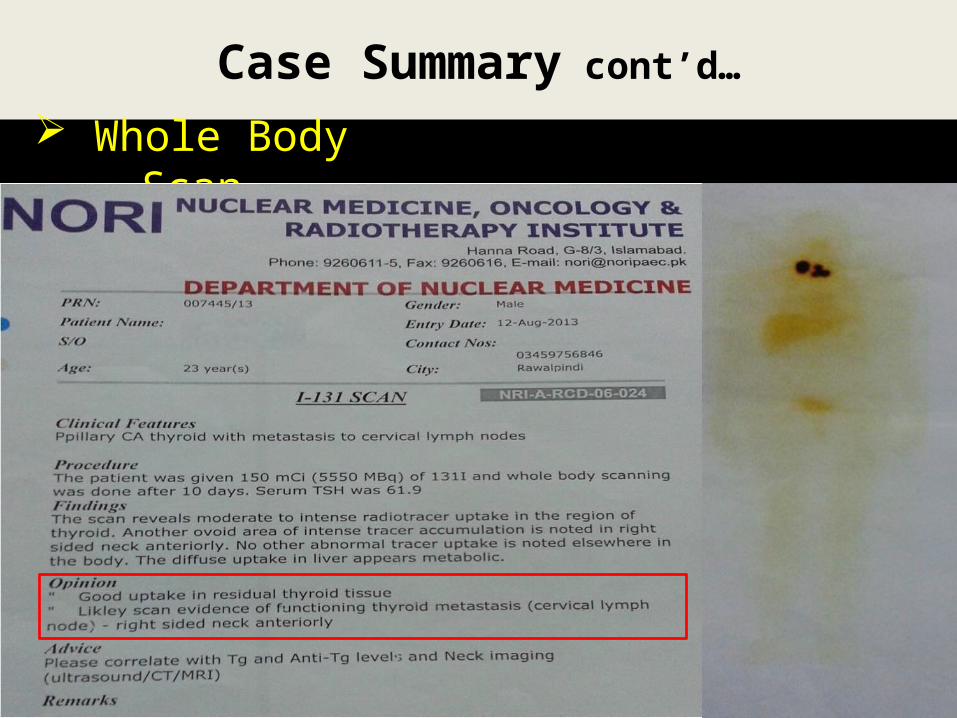
Case Summary cont’d…
47
Case Summary cont’d…
Whole Body Scan
Management Plan
COMPLETION THYROIDECTOMY &RIGHT RADICAL NECK DISSECTION
48
Management
Pre-op work up Counselling
Details of the nature and severity of the disease
Treatment options available Specific risk of surgery and GA
Informed written consent Pre-anesthesia assessment: ASA-I 02 Units RCC arranged
49

OPERATIVE STEPS
Operative Steps
51 51
Operative Steps
52 52
Operative Steps
53 53
Operative Steps
54 54

Operative Steps
55 55
Post OP Management
Nursed in Surgical ITC
Inj Ceftriaxone 1g I/V 12 hourly (ATD)
Inj Coamoxiclav 1.2g I/V 8 hourly (ATD)
Inj Ketorolac 30mg I/V 08 hourly
Inj Dexamethasone 8 mg I/V 08 hourly
Inj Ca Gluconate 10 mg I/V 08 hourly
56
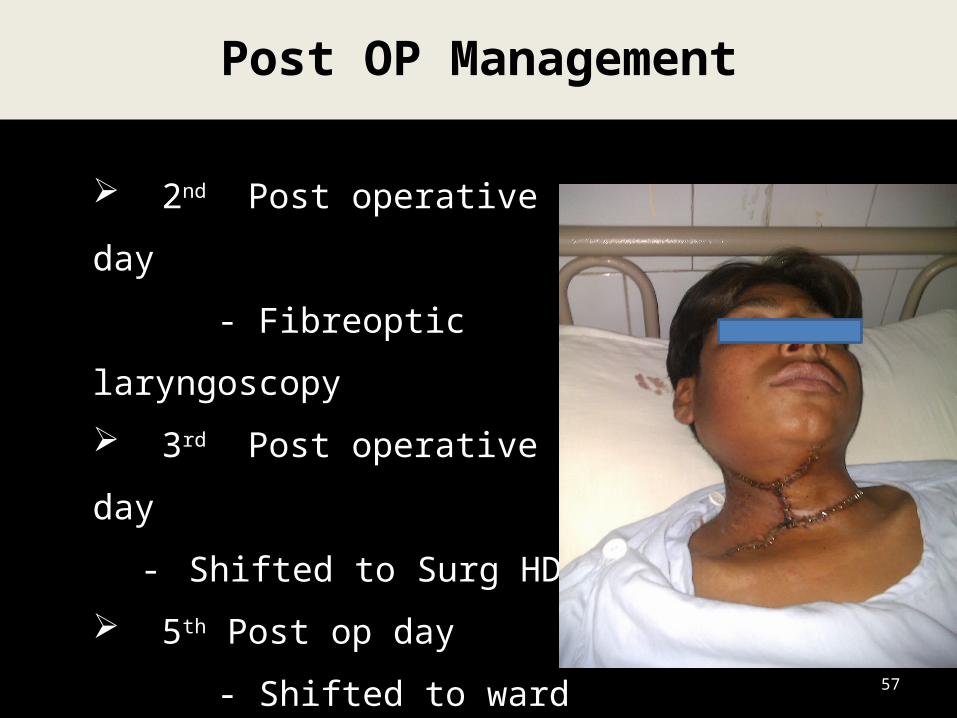
Post OP Management
57
2nd Post operative day
- Fibreoptic laryngoscopy
3rd Post operative day
- Shifted to Surg HDU
5th Post op day
- Shifted to ward
14TH Post op day
- Stitches removed
- Thyroid profile

Follow Up
58
59
LITERATURE REVIEW
Management of Complicated Papillary Thyroid Carcinoma
Case Summary
Commonest thyroid tumour 80%* Age incidence 20-50 years Male : Female 1 : 3 Multifocal 80%† Spread by lymphatics Local invasion 10-20% 10 year survival 93%
* Murray D. The thyroid gland, in: Kovacs L, Asa SL (eds). Functional endocrine pathology. Oxford: Blackwell. Science, 1998: 295-369† Baloch ZW, LivoIsi VA. Pathology of thyroid gland. In: LivoIsi VA, Asa SL (eds). Endocrine pathology. Philadelphia, PA: Churchill Livingstone, 2002: 61-101
Papillary Thyroid Carcinoma
60
Etiology / Risk Factors
61
Prolonged stimulation by TSH*
Persistent solitary thyroid nodule
Radiation exposure
Familial & Genetic factors
- Gardner’s Syndrome
* Williams ED, Abrosimov A, Bogdanova T et al. Thyroid carcinoma after Chernobyl latent period, morphology and aggressiveness. British Journal of Cancer 2004; 90: 2219-24
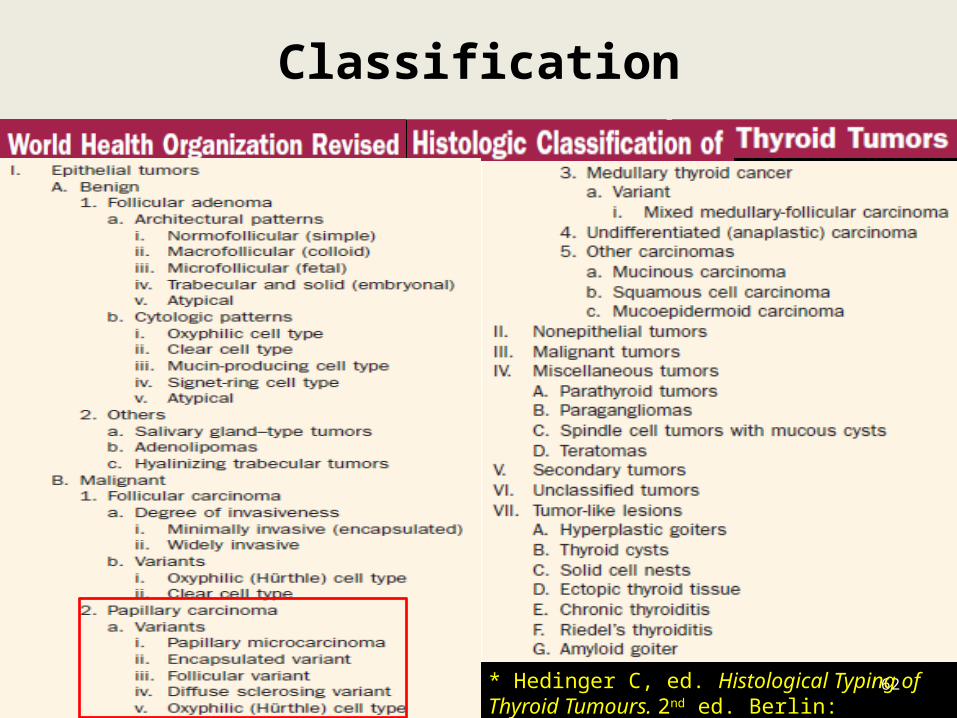
Case SummaryClassification
62* Hedinger C, ed. Histological Typing of Thyroid Tumours. 2nd ed. Berlin: Springer-Verlag; 1988
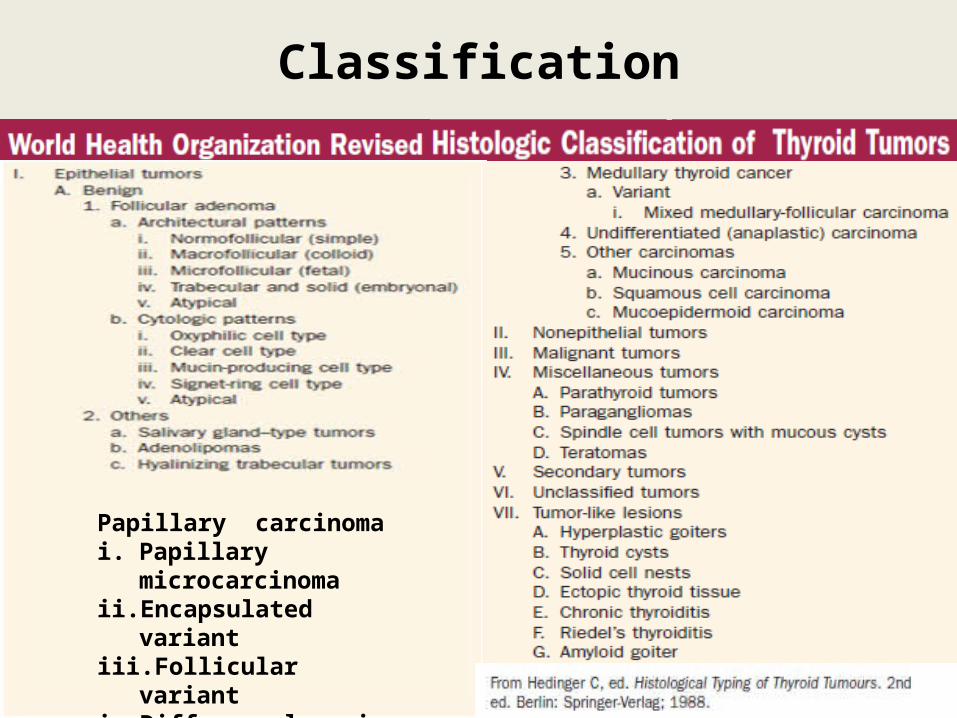
Case SummaryClassification
63
Papillary carcinoma i. Papillary microcarcinomaii. Encapsulated variantiii. Follicular variantiv. Diffuse sclerosing variantv. Oxyphilic(Hurthe) cell type
Case Summary Solitary nodule
Prominent nodule in MNG
Palpable Cervical Lymph Nodes 30% *
Hoarseness
Difficulty in breathing 3-5%
Difficulty in swallowing
*Wang TS, Dubner S, Sznyter LA, Heller KS. Incidence of metastatic well-differentiated thyroid cancer in cervical lymph nodes. Archives of Otolaryngology - Head and Neck Surgery 2004; 130: 110-13
Clinical Presentation
64
Case Summary
Examination of Neck Firm, solitary or dominant nodule in MNG Movement of swelling on swallowing Mobility Consistency Extent Cervical lymph nodes
Examination of Pharynx & Larynx IDL/ Fibreoptic endoscopy
- Vocal cord paralysis/ compression of airway
Physical Examination
65
Case Summary
FNAC
Thy 1 – inadequate for diagnosis
Thy 2 – benign disease
Thy 3 – suspicious for neoplasia
Thy 4 – suspicious for malignancy
Thy 5 – positive for malignancy
Investigations
66
Case Summary
Serum Thyroid Profile
T3, T4 Euthyroid
↑ TSH Malignancy*
↑ Thyroglobulin Recurrence
* Boelaert K, Horacek J, Holder RL et al. Serum thyrotropin concentration as a novel predictor of malignancy in thyroid nodules, investigated by fine-needle aspiration. Journal of Clinical Endocrinology and Metabolism 2006; 91:4295-301
Investigations cont’d…
67

Case Summary USG Neck*
Nodularity, size, consistency, cacifications
Disease in contralateral lobe Cervical lymph nodes US guided FNAC
Colour Flow Doppler Sonography
Type III flow (Intranodular/central)
* Appetecchia M, Solivetti FM. The association of colour flow Doppler sonography and conventional ultrasonography improves the diagnosis of thyroid carcinoma. Hormone Research 2006; 66: 249-56
Investigations cont’d…
68
Case Summary Thyroid Isotope Scan
Iodine-123 or Iodine-131
Technetium-99m
Show nodules greater than 5 mm
Cold nodules may be malignant
Hot or warm nodules are unlikely to be
malignant
Mehahna H, Jain A, Morton RP et al. Investigating the thyroid nodule. British Medical Journal 2009; 338: 733
Investigations cont’d…
69
Case Summary
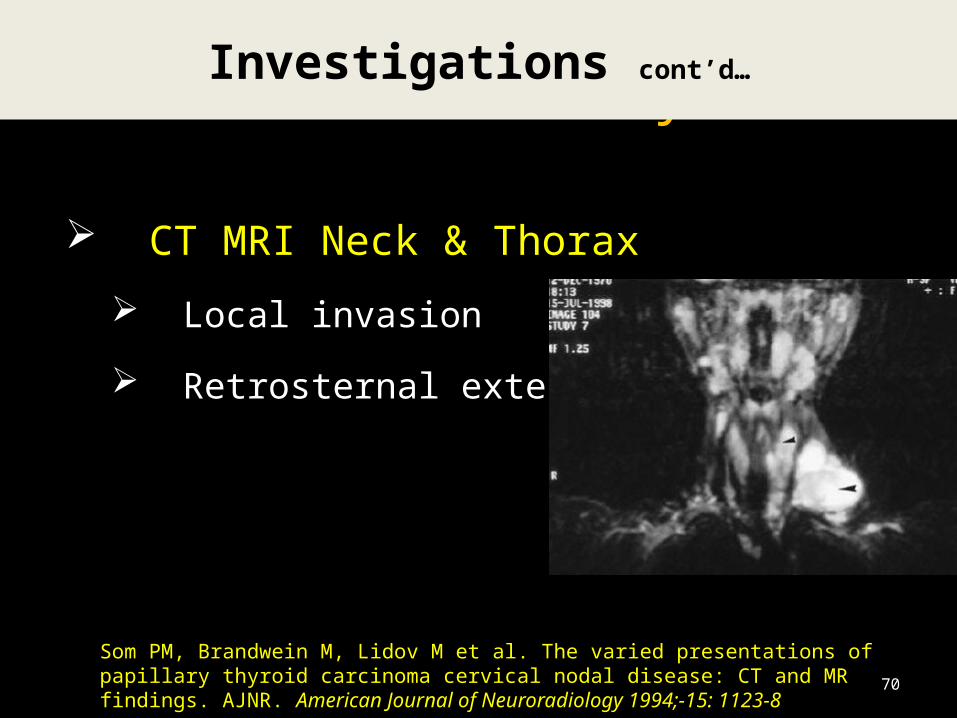
CT MRI Neck & Thorax
Local invasion
Retrosternal extension
Som PM, Brandwein M, Lidov M et al. The varied presentations of papillary thyroid carcinoma cervical nodal disease: CT and MR findings. AJNR. American Journal of Neuroradiology 1994;-15: 1123-8
Investigations cont’d…
70
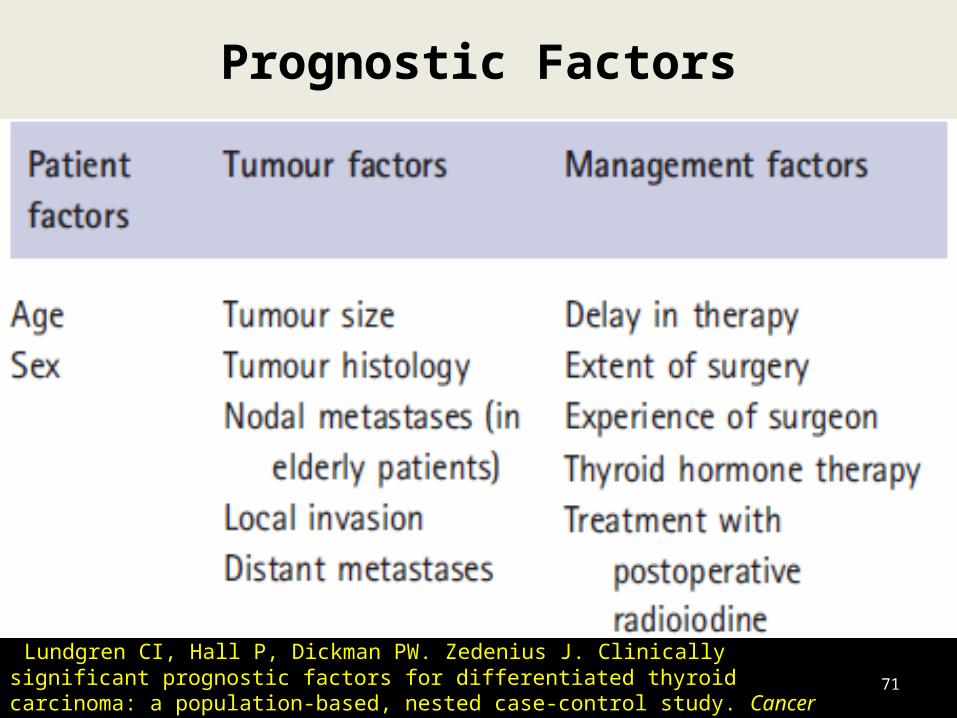
Case SummaryPrognostic Factors
71
Lundgren CI, Hall P, Dickman PW. Zedenius J. Clinically significant prognostic factors for differentiated thyroid carcinoma: a population-based, nested case-control study. Cancer 2006; 106: 524-3
Case Summary
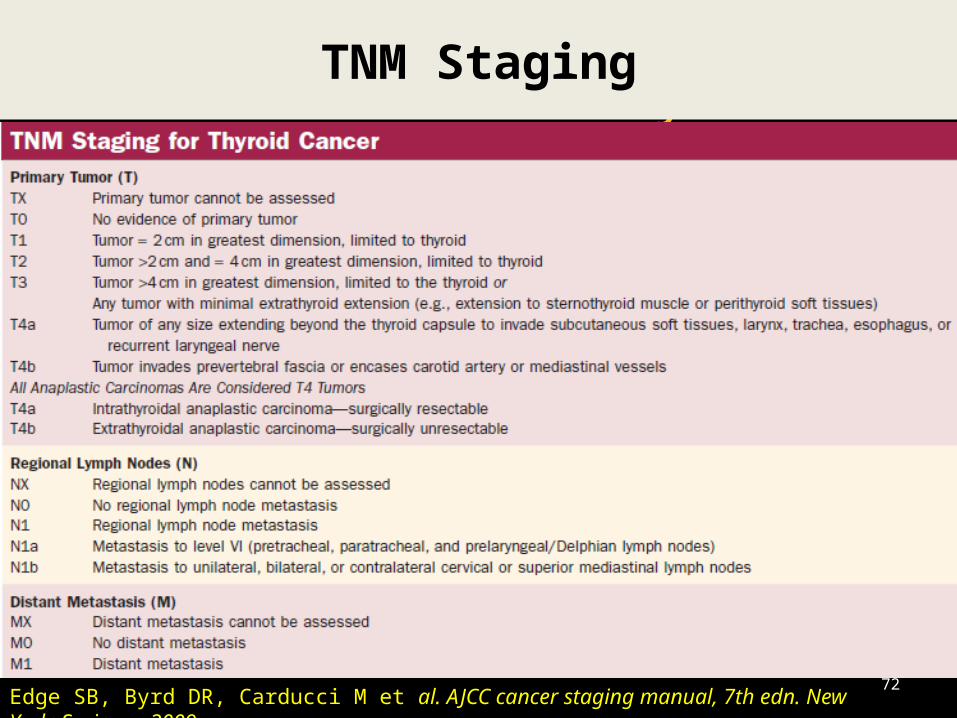
TNM Staging
72Edge SB, Byrd DR, Carducci M et al. AJCC cancer staging manual, 7th edn. New York: Springer, 2009

Case Summary
Staging
73Edge SB, Byrd DR, Carducci M et al. AJCC cancer staging manual, 7th edn. New York: Springer, 2009
Case SummaryClassification
74
Minimal or Micro carcinoma < 1 cm
Intrathyroidal > 1 cm
Extrathyroidal Beyond capsule/ Lymph
node metastasis
Case Summary
Surgery is the mainstay of treatment*
Radio-ablation of thyroid remnant
Thyroxine suppression
External beam radiation
Treatment
75*Mazzaferri EL, Kloos RT. Clinical review 128: Current approaches to primary therapy for papillary and follicular thyroid cancer. Journal of Clinical Endocrinology and Metabolism 2001; 86: 1447-63.
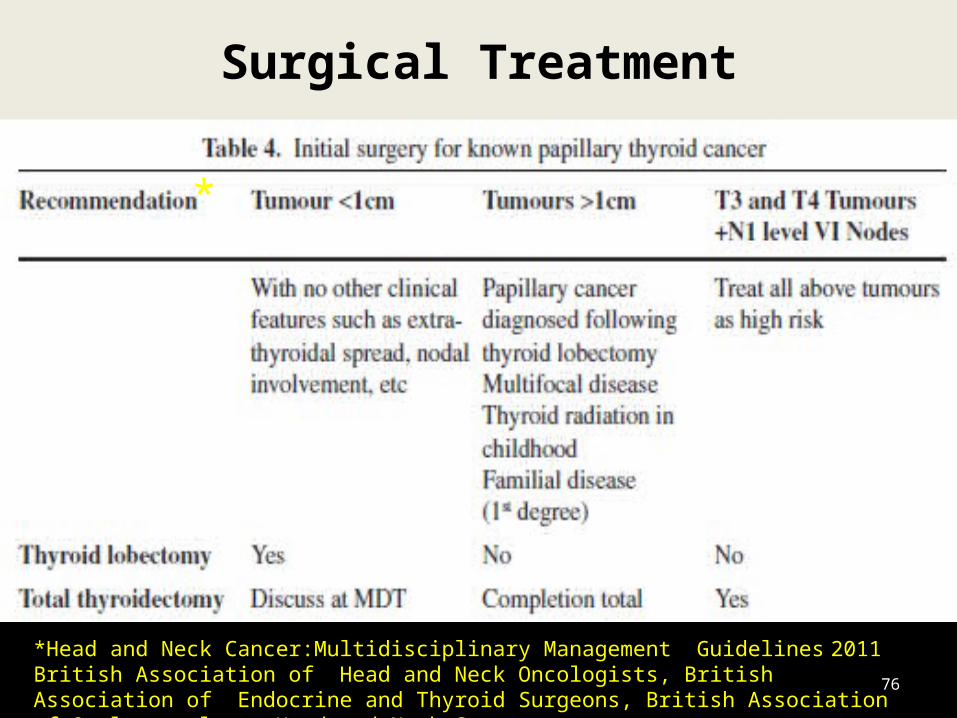
Case SummarySurgical Treatment
76
*Head and Neck Cancer:Multidisciplinary Management Guidelines 2011British Association of Head and Neck Oncologists, British Association of Endocrine and Thyroid Surgeons, British Association of Otolaryngology– Head and Neck Surgery
*
Case Summary Extent of Surgery for cervical lymph nodes
Selective nodal excision (Not recommended)*- Berry/ Cherry picking
Anterior/ Central (Level VI) Neck Dissection
Lateral/ Selective or Modified Radical Neck† Dissection (Level III, II, IV, I, V)
Surgical Treatment
77
*Scheumann GF, Gimm 0, Wegener G ef al. Prognostic significance and surgical management of locoregional lymph node metastases in papillary thyroid cancer. World Journal of Surgery 2009; 18: 559-67†Pingpank JFJr, Sasson AR, Hanlon AL et.al. Tumor above the spinal accessory nerve in papillary thyroid cancer that involves lateral neck nodes: a common occurrence. Archives of Otolaryngology - Head and Neck Surgery 2002; 128: 1275-8.
Case Summary
Post Op TSH suppression by exogenous thyroxine*
TSH levels of < 0.1 mU/L in high risk and between 0.1-0.5mU/L in low risk patients
TSH suppression is discontinued 2-4 weeks before radio ablation
TSH Suppression Therapy
78
*Cooper DS, Specker B, Ho M et al. Thyrotropin suppression and disease progression in patients with differentiated thyroid cancer: results from the National Thyroid Cancer Treatment Cooperative Registry. Thyroid 1998; 8:737-44

Radioiodine is used for ablation of normal thyroid*
tissue & to treat residual thyroid tumour
Pre therapy whole body diagnostic scan
Therapeutic doses of 100-200 mCi
Not recommended in low risk group†
79
Radio Ablation
*Sawka AM, Thephamongkhol K, Brouwers M et al. Clinical review 170: A systematic review and metaanalysis of the effectiveness of radioactive iodine remnant ablation for well-differentiated thyroid cancer. Journal of Clinical Endocrinology and Metabolism 2004; 89: 3668-76†British Thyroid Association and Royal College of Physicians. Guidelines for management of thyroid cancer, 2007. Available from www.british-thyroidassociation.org
EBRT along with Doxirubicin improves local control
80
External Beam RT & Chemotherapy
British Thyroid Association and Royal College of Physicians. Guidelines for management of thyroid cancer, 2007. Available from www.british-thyroidassociation.org
Case Summary 30% recurrence*
Regular TSH levels
Serial Thyroglobulin levels†
Diagnostic Radio iodine scans
US Neck
FDG-PET Scans
Follow up/ Monitoring
81
*Mazzaferri EL, Kloos RT. Clinical review 128: Current approaches to primary therapy for papillary and follicular thyroid cancer. Journal of Clinical Endocrinology and Metabolism 2001; 86: 1447-63† Mazzaferri EL Empirically treating high serum thyroglobulin levels. Journal of Nuclear Medicine 2005; 46: 1079-88.
Case Summary
DATA ANALYSIS
82
Case Summary
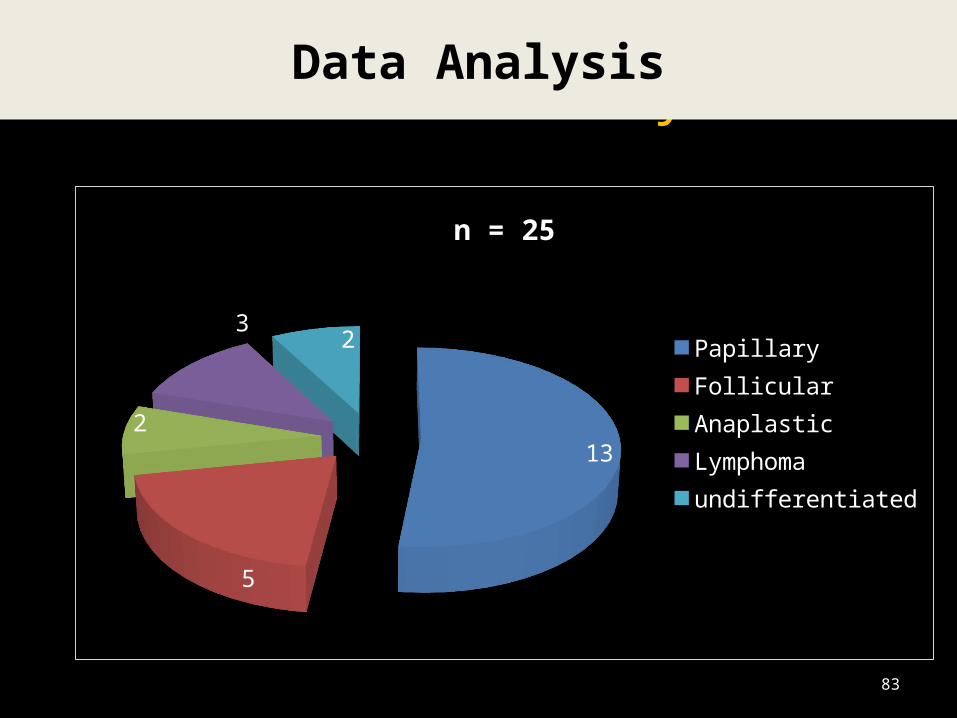
13
5
2
3 2
n = 25
PapillaryFollicularAnaplasticLymphomaundifferentiated
Data Analysis
83
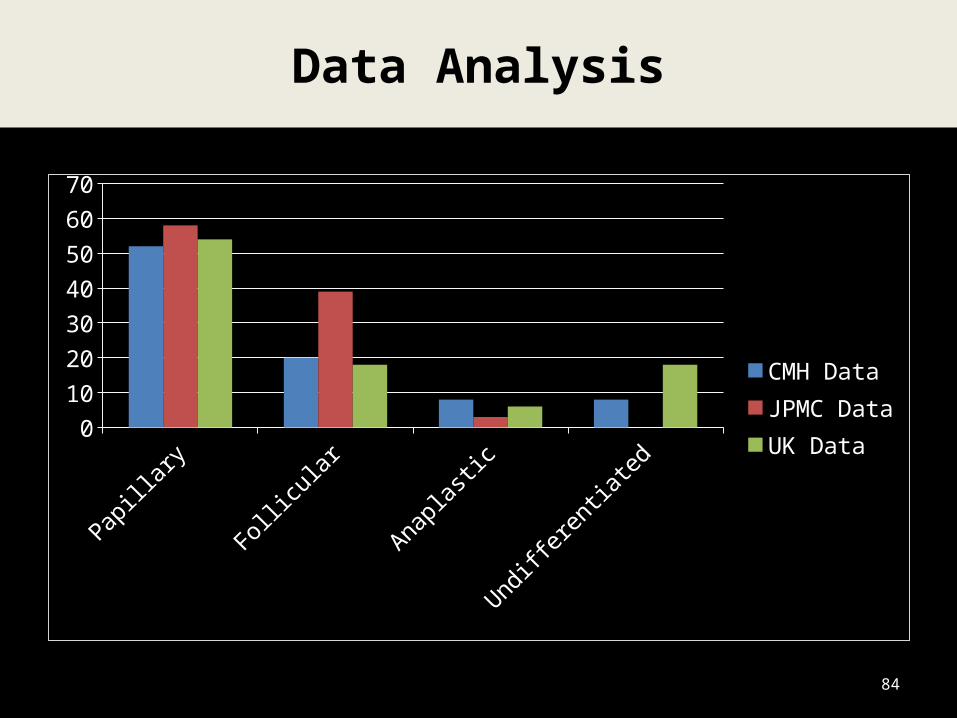
Data Analysis
Papillary Follicular Anaplastic Undifferentiated0
10
20
30
40
50
60
70
CMH DataJPMC DataUK Data
84
Conclusion
85
Thyroid cancer is relatively rare , one of the
most curable cancers
Surgery is the treatment of choice
Complications to be kept minimal
Low recurrences to be ensured
86
DEPARTMENT OF ENT, HEAD AND NECK SURGERY
•