
Evaluation and Treatment of High Energy Proximal Femur ... · Evaluation and Treatment of High ......
59
6/23/2014 1 Evaluation and Treatment of High Energy Proximal Femur Fractures OVERVIEW • Introduction of Speakers - Objectives (2 minutes) • Injury Patterns, Evaluation - Patient Considerations Mike Gardner -- (10 minutes) • Operative Fixation: Nail - Dave Barei – (10 minutes) • Operative Fixation: Plate - Tim Achor – (10 minutes) • Problems and Complications - David Asprinio – (10 minutes) • Discussion/Cases/Q+A (20 minutes)
Transcript of Evaluation and Treatment of High Energy Proximal Femur ... · Evaluation and Treatment of High ......
6/23/2014
1
Evaluation and Treatment of High Energy Proximal Femur Fractures
OVERVIEW • Introduction of Speakers - Objectives (2 minutes) • Injury Patterns, Evaluation - Patient Considerations Mike Gardner -- (10 minutes) • Operative Fixation: Nail - Dave Barei – (10 minutes) • Operative Fixation: Plate - Tim Achor – (10 minutes) • Problems and Complications - David Asprinio – (10 minutes) • Discussion/Cases/Q+A (20 minutes)
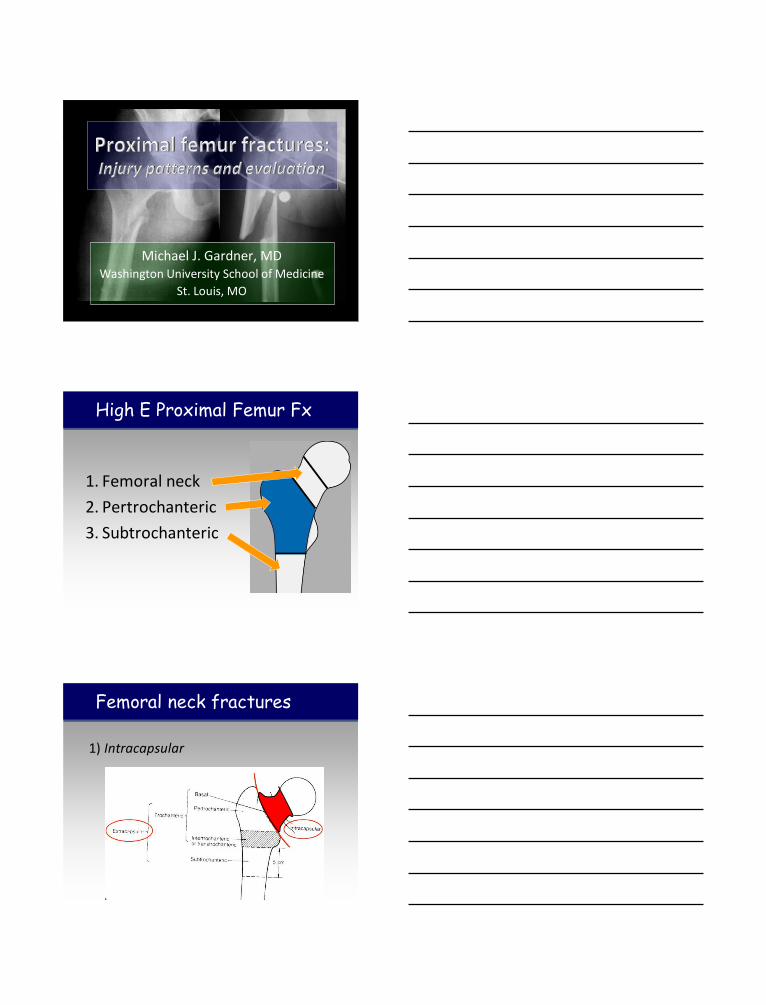
Michael J. Gardner, MD Washington University School of Medicine
St. Louis, MO
1. Femoral neck
2. Pertrochanteric
3. Subtrochanteric
High E Proximal Femur Fx
1) Intracapsular
Femoral neck fractures

1) Intracapsular
Implications:
• Synovial fluid bathed
• Endosteal healing
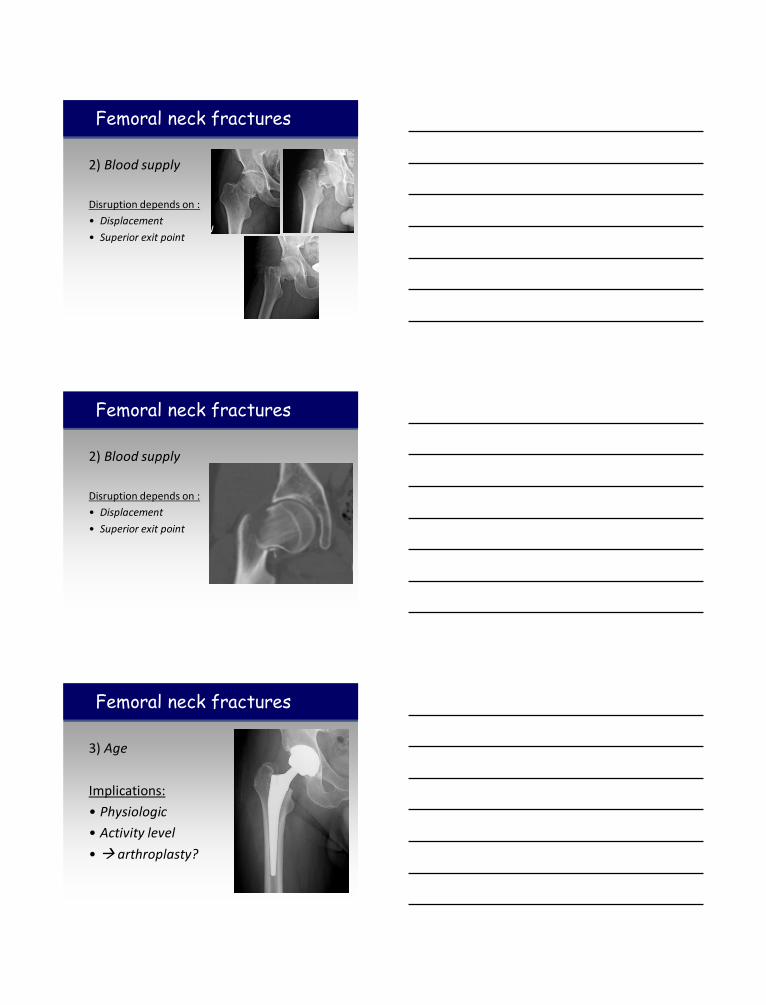
Femoral neck fractures
2) Blood supply
Femoral neck fractures
2) Blood supply
Implications:
• Tenuous
• Frequently disrupted
Femoral neck fractures
2) Blood supply
Disruption depends on :
• Displacement
• Superior exit point
Femoral neck fractures
2) Blood supply
Disruption depends on :
• Displacement
• Superior exit point
Femoral neck fractures
3) Age
Implications:
• Physiologic
• Activity level
• arthroplasty?
Femoral neck fractures

4) Occult in femoral shaft fractures
Femoral neck fractures
Femoral neck fractures
5) Radiography
• Hip frequently externally rotated
• Difficult to visualize fracture
• CT SCAN
• Pauwels’ Classification [1935]
0% non-union 13% AVN
8% non-union 30% AVN
12% non-union 35% AVN
Femoral neck fractures
Verticality Shear forces

Femoral neck fractures
6) Surgical timing
• Priortize REDUCTION and quality of surgery rather than TIME TO OR
Pertrochanteric fx
Pertrochanteric fx
1) “Simple” fx do not behave like geriatric fx
Implications:
• Plan for open reduction
• Avoid fracture table
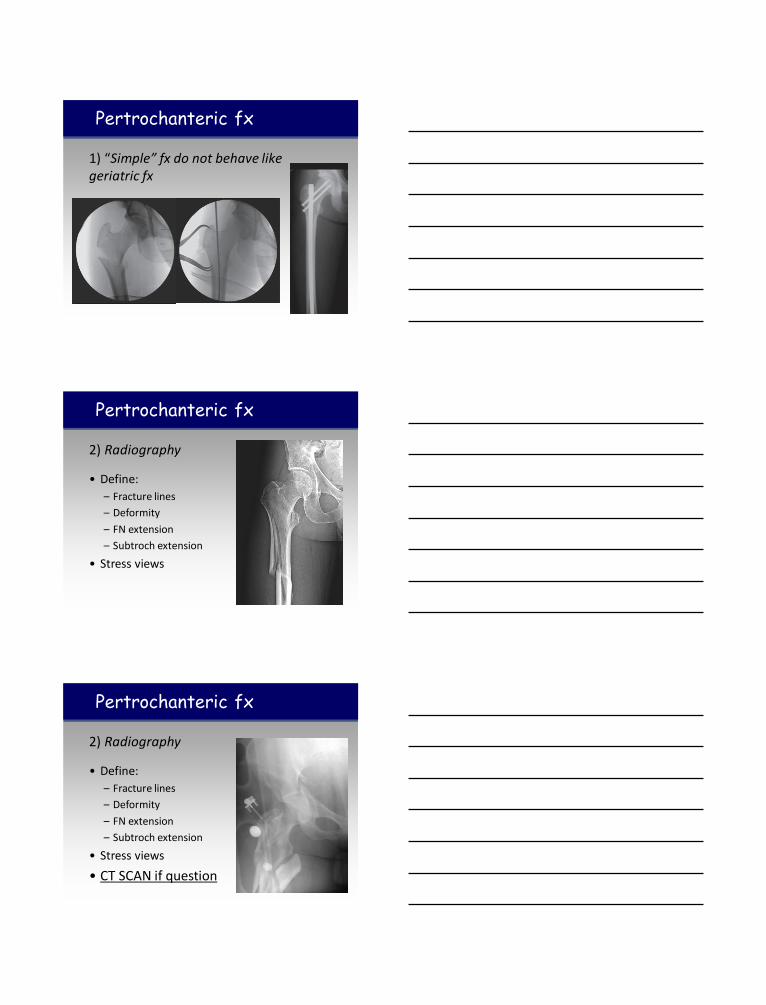
Pertrochanteric fx
1) “Simple” fx do not behave like geriatric fx
Pertrochanteric fx
2) Radiography
• Define:
– Fracture lines
– Deformity
– FN extension
– Subtroch extension
• Stress views
Pertrochanteric fx
2) Radiography
• Define:
– Fracture lines
– Deformity
– FN extension
– Subtroch extension
• Stress views
• CT SCAN if question

Pertrochanteric fx
2) Radiography
Pertrochanteric fx
3) Search for subtrochanteric extensions that are able to be clamped
Pertrochanteric fx
3) Search for subtrochanteric extensions that are able to be clamped

Subtrochanteric fx
vs vs
Wide Spectrum
Subtrochanteric fx
• Classic deforming forces:
• Proximal segment
– Flexion
– Abduction
– ER
• Distal segment
– Adduction
– Shortening
Subtrochanteric fx
1) Radiography
• Quality AP and lateral to understand fracture and deformity

Subtrochanteric fx
1) Radiography
• Quality AP and lateral to understand fracture and deformity
• Proximal femur fractures are highly variable
• Different anatomic regions have different treatment implications
• Accurate understanding of fracture pattern is paramount
Summary
Thank You

6/23/2014
1
Operative Fixation: Nail
David P. Barei MD, FRCSC Associate Professor Harborview Medical Center / University of Washington Seattle, WA [email protected]
Evaluation and Treatment of High Energy Proximal
Femur Fractures
Disclosure
• Teaching Honoraria (AO)
• Synthes Consultant (implant design)
• Journal Reviewer
– JBJS-A, J Orthop Trauma, CORR
• AO Fellowship Committee
Institutional-UW Ortho-Research
• AO Spine North America
• AO-Sti ftung-ASIF Foundation
• Bank of America Foundation
• The Center, Orthopaedics and Neurological Surgeons
• Fidelity Investments
• Helena Orthopaedics Cl inic
• I l linois Orthopaedics & Hand Center
• Inland Orthopaedics of Spokane
• JMS Hand Associates
• Northwest Biomet, Inc.
• Paci fic Rim Orthopaedics
• Prol iance Surgeons, Inc.
• Prol iance Orthopeadics & Sports Medicine
• The Seattle Foundation
• Seattle Christian Foundation
• Si l icon Valley Community Foundation
• Simonian Sports Medicine Cl inic
• SKS Plastic Surgery
• Spectrum Research
• Synthes U.S.A.
• Synthes Spine Co.
• Washington Research Foundation
• Washington State Orthopaedics Association
• Webber Lawn & Yard Care
• National Institutes of Health (NIH)
• National Science Foundation (NSF)
• Veterans Affairs Rehabilitation Research and
• Development Service
• Orthopaedic Research and Education Foundation (OREF)
• A.O. North America
• Amgen, Inc.
• Bayer AG
• BioAxone Therapeutique, Inc.
• CeraPedics, LLC
• Chris topher Reeve Paralysis Foundation
• Depuy (Johnson & Johnson, Inc. )
• Foundation for Orthopedic Trauma
• Integra Lifesciences Corporation
• National Science Foundation
• Ostex International, Inc.
• Orthopaedic Trauma Association
• Paradigm Spine
• Smith & Nephew
• Synthes Spine Co.
• The Boeing Company
• US Army Research Office
• US Department of Education

6/23/2014
2
Definition
• Inferior border of lesser
5 centimeters
8 centimeters
Proximal 1/3 of femur
What are the problems/difficulties
with subtrochanteric fractures?
1. High mechanical stresses
2. Powerful muscular deforming forces on
the proximal segment
3. Complicated patterns
4. Relative avascularity
Maximal Compressive
Forces Medially (2-8 cm below lesser)
(1200 lb/in2)
High Tensile Forces
Laterally
High Mechanical Stresses

6/23/2014
3
Flexion
Abduction
External rotation
Deforming Forces
Infrequently confined to the
subtrochanteric region!
Proximal extensions into the
intertrochanteric region
Complex Fracture Patterns
Implant choices
Plates
Nails
Lateral fixed angle implant
Angled blade plate
Dynamic condylar screw
Lateral locked fixed angle implant (PFLP)
Sliding hip screw (DHS)
Piriformis start antegrade nail
Cephalomedullary nail
Trochanteric versus piriformis starting point
Head fixation (2 small versus 1 large fixation device)
(blade versus screws into head)

6/23/2014
4
Implant choices
Plates
Nails
Lateral fixed angle implant
Angled blade plate
Dynamic condylar screw
Lateral locked fixed angle implant (PFLP)
Sliding hip screw (DHS)
Piriformis start antegrade nail
Cephalomedullary nail
Trochanteric versus piriformis starting point
Head fixation (2 small versus 1 large fixation device)
(blade versus screws into head)
Why Choose A Nail?
Biomechanics
6/23/2014
5
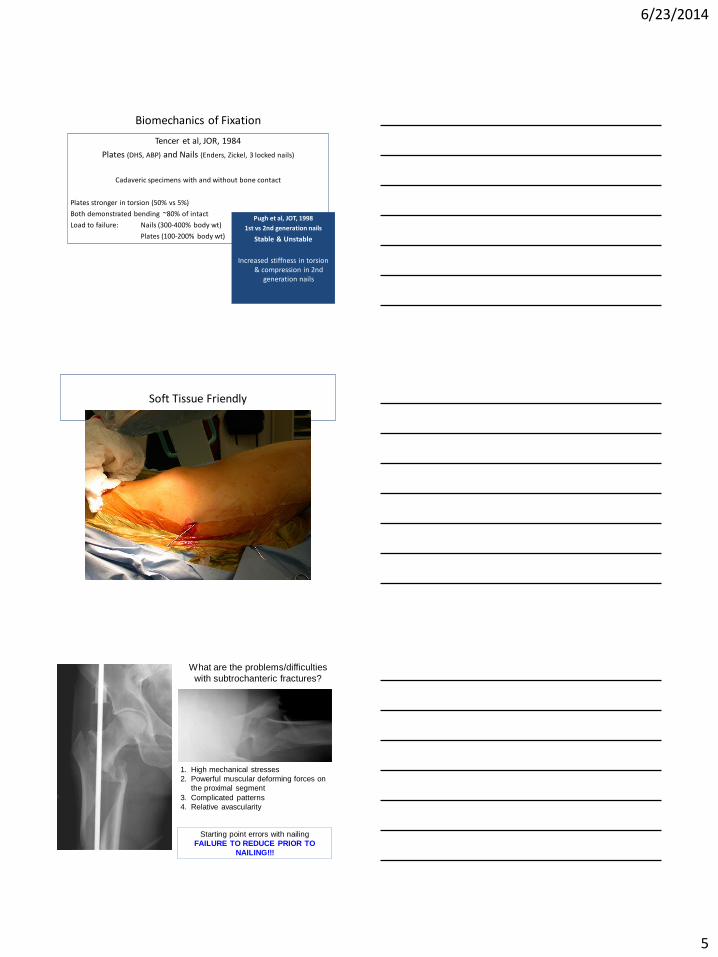
Biomechanics of Fixation
Tencer et al, JOR, 1984
Plates (DHS, ABP) and Nails (Enders, Zickel, 3 locked nails)
Cadaveric specimens with and without bone contact
Plates stronger in torsion (50% vs 5%)
Both demonstrated bending ~80% of intact
Load to failure: Nails (300-400% body wt)
Plates (100-200% body wt)
Pugh et al, JOT, 1998
1st vs 2nd generation nails
Stable & Unstable
Increased stiffness in torsion & compression in 2nd
generation nails
Soft Tissue Friendly
What are the problems/difficulties
with subtrochanteric fractures?
1. High mechanical stresses
2. Powerful muscular deforming forces on
the proximal segment
3. Complicated patterns
4. Relative avascularity
Starting point errors with nailing
FAILURE TO REDUCE PRIOR TO
NAILING!!!

6/23/2014
6
• Allows indirect reduction
• techniques • (Medullary Splint)
• Good biomechanical properties
• Familiar technique
Correct Deformity Before Nailing!!!
Locked Antegrade Nail
Accurate Start Point Accurate Entrance Trajectory
Correct Abduction
Correct Rotation
Correct Flexion
Reduction • Proximal reduction (opposite of
femoral shaft fractures)
• Time limit for closed maneuvers!
• Supine vs. Lateral position
• Tools
• F-tool
• Spike pusher
• Schanz pin(s)
• Large clamp
• Intramedullary reduction
• Open reduction

6/23/2014
7
36 yo female fell while rock climbing
Accurate start point, accurate entrance trajectory, percutaneous and accurate reduction during reaming and nail insertion

6/23/2014
8
Open reduction, limited dissection, pointed reduction clamps and provisional
large diametered K-wires
Scolaro, Injury 2013
Open reduction, limited dissection, pointed reduction clamps and provisional
large diametered K-wires
Scolaro, Injury 2013
3 months postop

6/23/2014
9
Clamp Assisted Reduction of High Subtrochanteric
Fractures of the Femur. Afsari et al, JBJS, 2009
• 43 of 44 fractures united
• Percutaneous technique
• Excellent reduction
• Specific fracture patterns
• Successful technique
Open Reduction and IM Stabilisation of Subtrochanteric
Femur Fractures. Beingessner et al, Injury, 2013
• 56 patients treated with open reduction and IM nailing
• All fractures united
• Open reduction technique with limited dissection
• 98% united within 5° of anatomic in the coronal and sagittal planes
• No wound complications or infections
However…
• If you’re going to open a subtrochanteric fracture…
• Do it nicely!!!

6/23/2014
10
Cephalomedullary Nails….
Piriformis Recon Trochanteric Recon Trochanteric Hip Screw
Cephalomedullary Nails….
• Personally preferred for “lower” subtrochanteric fractures where there remains some diaphyseal shaped canal on the proximal segment – Helps with reduction
– Anatomic axis of the femur
• More commonly used in younger patients with higher quality bone
• Requires a slightly more anterior start point than typical piriformis nailing
Piriformis Recon
Piriformis Centromedullary Nail Start Point

6/23/2014
11
5 mm
Reconstruction =
Cephalomedullary =
Second Generation Nail
Piriformis Cephalomedullary Nail Start Point
Reconstruction =
Cephalomedullary =
Second Generation Nail
Piriformis Cephalomedullary Nail Start Point
Cephalomedullary Nails….
• Personally preferred for the “higher” subtrochanteric femur fracture ± intertrochanteric involvement
• Allows proximal locking to be more collinear with midcoronal plane of the femoral head/neck
• Can use the nail to aid in rotational reduction (built-in nail “version”)
• Requires strict attention to accurate start point to avoid varus malalignments
Trochanteric Recon

6/23/2014
12
Cephalomedullary Nails….
Trochanteric Recon
The tip of the trochanter, or even slightly medial to the tip, should be the entry site of choice for antegrade trochanteric
nailing of subtrochanteric fractures. The lateral starting point, even 2-3mm from the tip of the trochanter, is to be avoided
Recommendation
Trochanteric Cephalomedullary Nail Start Point
Piriformis Recon Trochanteric Recon
Cephalomedullary Nails….
• Single screw cephalomedullary nails – Typically demonstrate large proximal
nail diameters – Large single screw/blade proximal
femoral head/neck interlock
• Consider these as “geriatric”
fracture implants developed for unstable pertrochanteric fractures in that population
• Requires substantial bone removal in younger patients
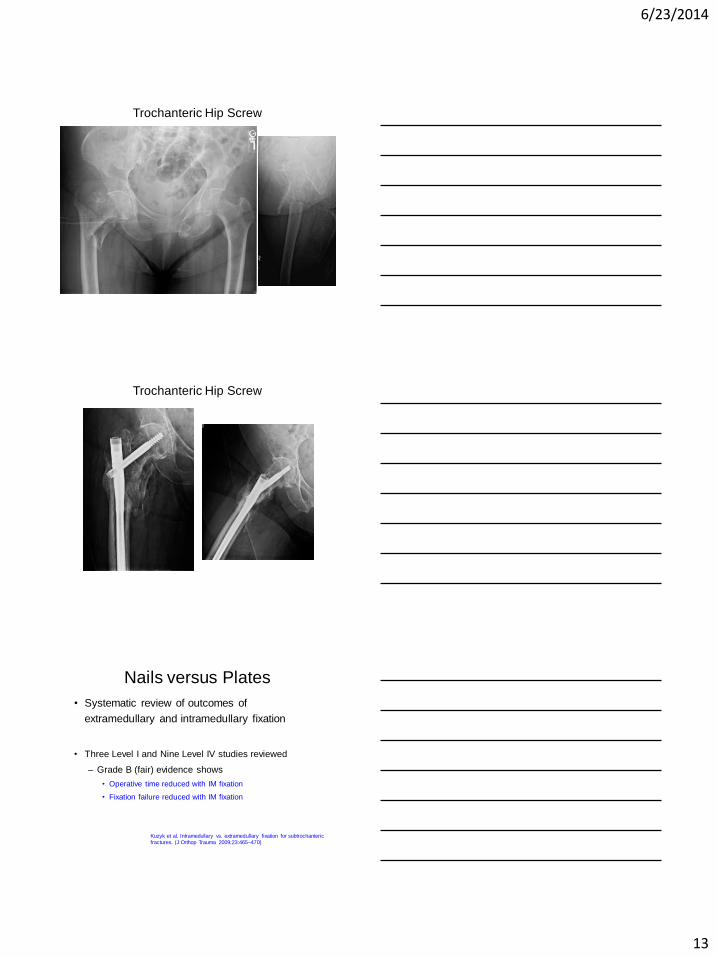
Trochanteric Hip Screw
6/23/2014
13
Trochanteric Hip Screw
Trochanteric Hip Screw
Nails versus Plates
• Systematic review of outcomes of
extramedullary and intramedullary fixation
• Three Level I and Nine Level IV studies reviewed
– Grade B (fair) evidence shows
• Operative time reduced with IM fixation
• Fixation failure reduced with IM fixation
Kuzyk et al. Intramedullary vs. extramedullary fixation for subtrochanteric
fractures. (J Orthop Trauma 2009;23:465–470)
6/23/2014
14
Summary
• High force concentration region
• Notoriously difficult to treat
• Common deformities
– Flexion
– Abduction
– External Rotation
• Complex patterns with proximal extensions
– Trochanteric, piriformis, lesser, comminution
• IM Nails are suitable devices mechanically, but require attention to detail
– Anticipate the predictable deformities
– Reduce BEFORE nailing (using multiple tools and approaches)
– Don’t hesitate to open, but do it nicely
– Piriformis and trochanteric reconstruction nails are very effective but require accurate start points and entrance trajectories!
– Reserve medullary hip screw implants for physiologically older patients and fractures if possible
Summary
Thank You
HMC Trauma Faculty
Barei, Beingessner, Bellabarba, Benirschke, Dunbar, Ferguson, Firoozabadi, Hanel, Hansen, Henley, Kleweno, Sangeorzan, Smith, Taitsman

6/18/2014
1
HIGH ENERGY HIP FRACTURES: PLATING TECHNIQUES
Timothy S. Achor, MD
UT Houston
Memorial Hermann Hospital
OBJECTIVES
• Discuss why high energy proximal femur fractures are different from geriatric hip fractures
• Discuss why plating these fractures is ideal
• Tips, tricks, pitfalls, recommendations
“NOT ALL HIP FRACTURES ARE CREATED EQUAL”

6/18/2014
2
HIGH ENERGY HIP FRACTURES MVC, MCC, FALL FROM HEIGHT
• Flexed
• Abducted
• Externally rotated
• Trend towards intramedullary nails for proximal femur fractures – Advantages:
• Biomechanical advantage
• Percutaneous technique
• Decreased OR time
– Disadvantages • Abductor mechanism
• Reaming
• Easy to introduce varus
NAIL VS PLATE?

6/18/2014
3
SURGERY
REDUCTION
IMPLANT
SURGERY
REDUCTION
IMPLANT
CLOSED
OPEN
PLATE
NAIL

6/18/2014
4
REDUCTION?
• Almost always OPEN
• You already have the incision
• Why disrupt endosteal blood supply and ream a hole in proximal femur?
TREATMENT OPTIONS:
PLATE SLIDING HIP SCREW
DYNAMIC CONDYLAR SCREW
PROXIMAL FEMUR PLATE
ANGLED BLADE PLATE
SLIDING HIP SCREW
• Intertrochanteric fractures • Subtrochanteric fractures* • Basilar neck fractures
• *NOT reverse oblique
FOR USE IN STABLE FRACTURES
CONTROLLED COLLAPSE

6/18/2014
5
OPTIONS
• Barrel length
• CCD angle
• Plate length
LONG
135 degree
2 – 4 hole
Tip-Apex Distance (TAD)

6/18/2014
6
DJ9235A 16
Dynamic Condylar Screw
–Transverse subtroch fractures –Short oblique subtrochanteric fractures –Long oblique subtrochanteric fractures
1. Roy Sanders and P.Regazzoni. “Treatment of Subtrochanteric Femur Fractures Using the Dynamic Condylar Screw.” Journal of Orthopaedic Trauma, vol. 3, no. 3, New York: Raven Press, 1989. 206-213.
Proximal Femur Locking Plates
– Anatomic, precontoured plate
– Multiple fixed angled screws
– MIPO (theoretical?)
– Submuscular
– Locking/cortical screws on shaft
+ / -

6/18/2014
7
ANGLED BLADE PLATE
Excellent historical track record Preferred implant for nonunions Technically challenging Relatively unforgiving 95 degrees – must be righteous

6/18/2014
8
BLADE PLATE?
• Simple fracture patterns • Patterns amenable to lag screws • Patterns amenable to compression • Patterns amenable to loading • Extension into neck • Extension into greater trochanter
• Lateral cortical read/apposition most important

6/18/2014
9
POST-OP PROTOCOL
• PROTECTED WEIGHT-BEARING X 8-12 WEEKS
• Monitor follow-up xrays closely
– May allow weight-bearing as early as 6 weeks
PITFALLS
• Malreduction
• Varus
• Varus
• Varus
• Using a plate when a nail might have been better
– Load-BEARING vs load-SHARING
• NOT TENSIONING THE PLATE!!!

6/18/2014
10
CASE 1
32 M s/p MVC
• Complaining of severe right hip pain
• +EtOH

6/18/2014
11
32 M s/p MVC

6/18/2014
12
• Fracture table?
• Open or closed reduction?
• Nail vs Plate?

6/18/2014
13

6/18/2014
14

6/18/2014
15
ARTICULATED TENSION DEVICE
“LOAD THE FRACTURE” “TENSION THE PLATE”

6/18/2014
16
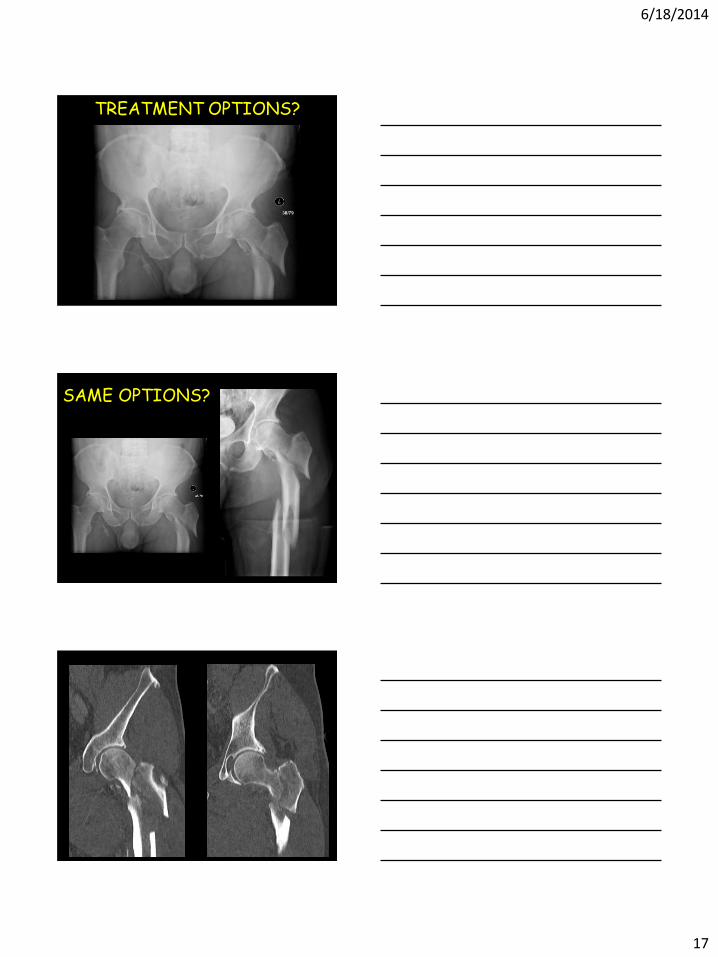
64 M s/p MCC
6/18/2014
17
TREATMENT OPTIONS?
SAME OPTIONS?

6/18/2014
18
TREATMENT?
6 WEEK F/U
6/18/2014
19
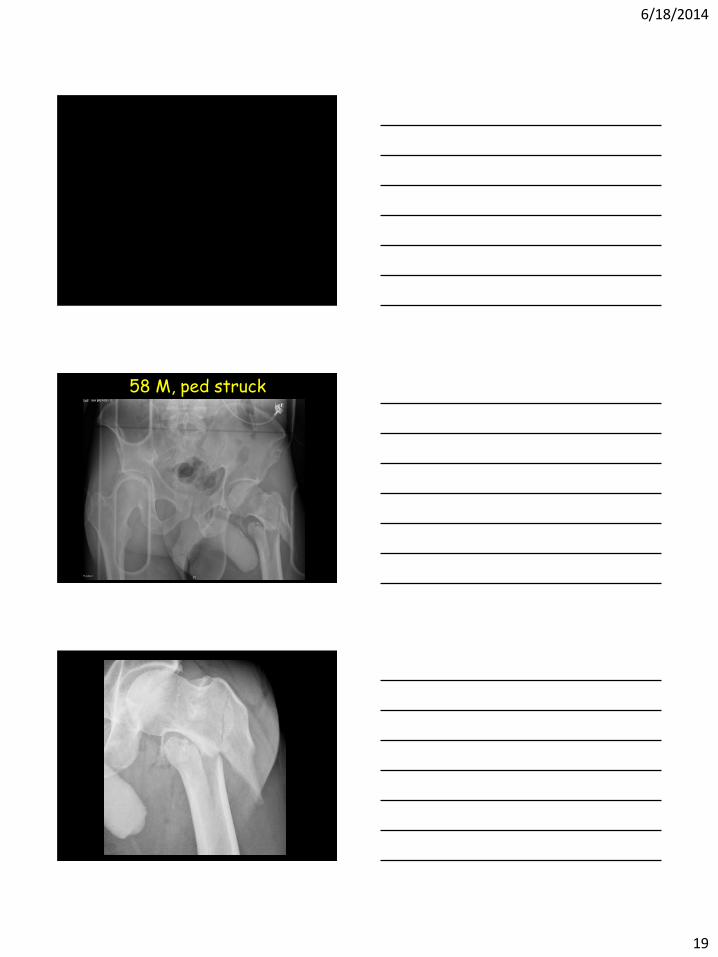
58 M, ped struck
6/18/2014
20
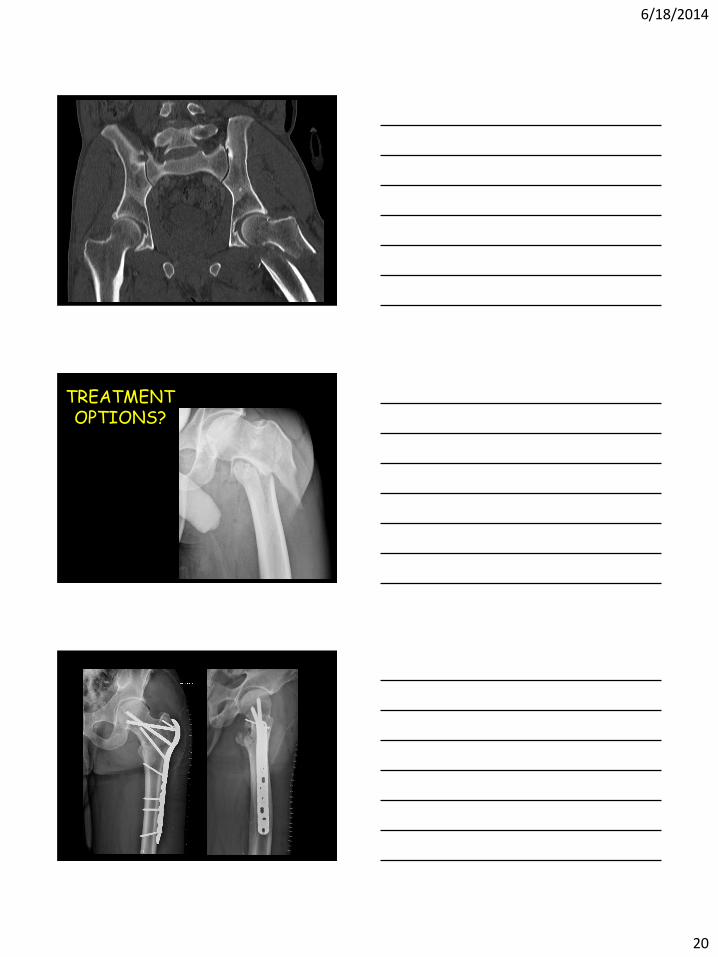
TREATMENT OPTIONS?

6/18/2014
21
2 YEAR FOLLOW UP
22 M s/p MCC

6/18/2014
22
4 month follow-up

6/18/2014
23
IN CONCLUSION…
• Not all proximal femur fractures are equal – Age, Energy, Comminution, “Personality”
• DIFFICULT fractures to treat
• Treat each fracture individually with what
works best in YOUR hands
• Consider the 95 degree angled blade plate WITH the articulated tension device for simple, loadable fracture patterns.
THANK YOU

6/19/2014
1
Evaluation and Treatment of High Energy
Proximal Femur Fractures
David E. Asprinio, M.D.
6/23/2014
Problems and Complications
10 MINUTES
• THESE ARE COMPLEX PROBLEMS
• NO UNIVERSAL SOLUTION
• OPTIONS
– Intramedullary fixation
– Blade plate fixation
– Proximal femur locking plates
– Compression hip screw
– 95 degree dynamic condylar screw
– External fixation
– Replacement arthroplasty
– Skeletal traction
Whatever is done needs to be done well
Many principles apply to prevention and treatment
Avoiding problems and complications • Evaluate the patient and radiographs
– Consider co-morbidities and other injuries
• Need a plan and a backup plan
– Need to be familiar with multiple modalities
– Know what can be done and know your limitations
• Reduction is critical
– Must achieve and maintain
– Intramedullary devices don’t achieve reduction
– Fixed angle devices may achieve reduction
however placement is critical
• Avoid unnecessary soft tissue dissection

6/19/2014
2
RS 1/24/07
INTROPERATIVE TRACTION
RS 1/25/07

6/19/2014
3
VM 76 y/o male 3/9/12
GD 81 y/o male 4/29/14

6/19/2014
4
GD 4/30/14

6/19/2014
5
GD 6 weeks
6/19/2014
6
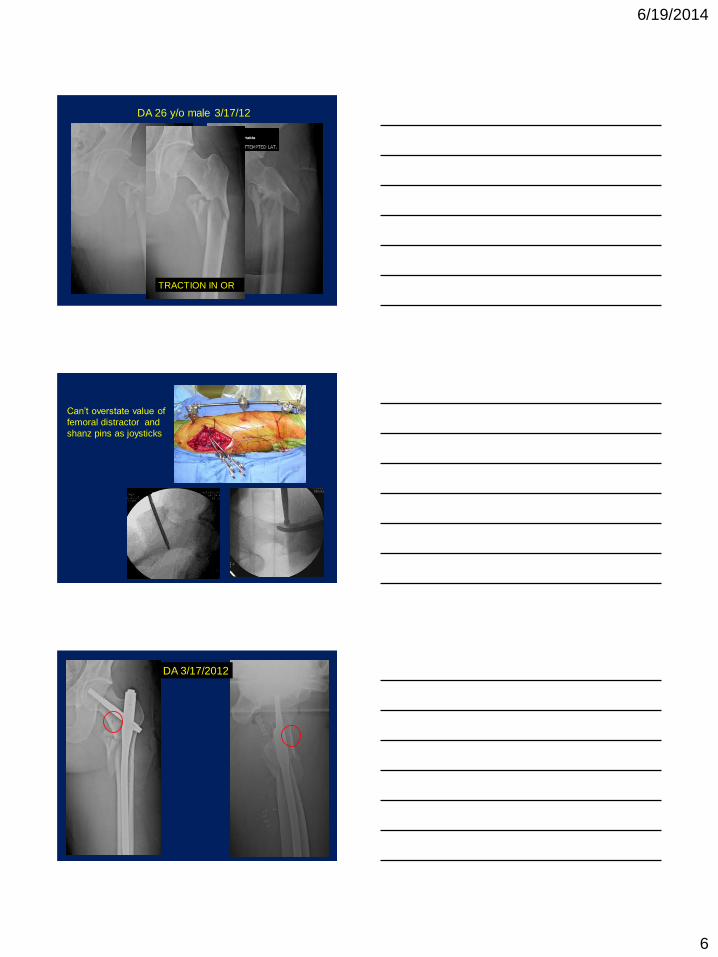
DA 26 y/o male 3/17/12
TRACTION IN OR
Can’t overstate value of
femoral distractor and
shanz pins as joysticks
DA 3/17/2012
6/19/2014
7
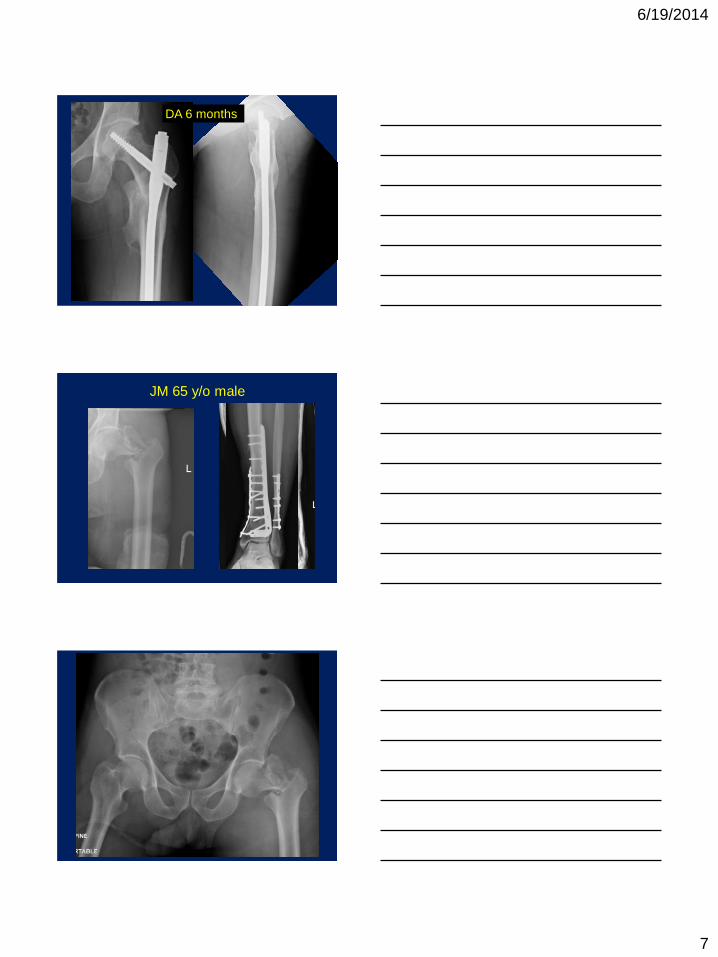
DA 6 months
JM 65 y/o male

6/19/2014
8

6/19/2014
9
When complications occur
• Evaluate the patient and radiographs
– Why did failure occur?
• Mechanical
– Reduction
– Choice of implant
– Placement of implant
• Biological
– Infection
– Osteoporosis
– Metabolic bone disease
• Patient non compliance
Treating complications
• Address prior deficiencies in treatment
• Need plan and backup plan
– Need to be facile with multiple modalities
– Know what can be done and know your
limitations
MUST ACHIEVE REDUCTION
CORRECT VARUS AND FLEXION ABNORMALITIES

6/19/2014
10
WL 51 Y/O MALE
10/2013
8 months
10/24/13
ROH, compression plating with restoration
of alignment, allograft, stem cell autograft
WL 6 months FWB without pain

6/19/2014
11
ES 88 y/o male 12/2013
ES 2/25/14 2months

6/19/2014
12
Summary
• It is better to avoid than treat complications
• Preoperative planning is critical
• Have multiple treatment options available
• Optimizing the mechanical and biological
environment will increase the likelihood of
successful treatment


















