Evaluation and Management of Pancreatic Pseudocysts · pancreatic ductal system due to...
9
12 Practical GastroenteroloGy • aPril 2014 FRONTIERS IN ENDOSCOPY, SERIES #10 Douglas G. Adler MD, FACG, AGAF, FASGE, Series Editor Matthew E. Feurer MD, MS Douglas G. Adler MD, FACG, FASGE, AGAF University of Utah School of Medicine, Department of Internal Medicine, Division of Gastroenterology and Hepatology Evaluation and Management of Pancreatic Pseudocysts Douglas G. Adler Matthew E. Feurer INTRODUCTION P ancreatic pseudocysts are commonly encountered in clinical practice. The management of pancreatic pseudocysts is complex and can range from simple observation to aggressive endoscopic and surgical interventions to treat symptomatic lesions. This manuscript will review the current evaluation and treatment of pancreatic pseudocysts. Overview of Pancreatic Pseudocysts A pancreatic pseudocyst is a fluid-filled cavity that occurs within or adjacent to the pancreas that is surrounded by a wall of fibrous and/or granulomatous tissue. Pseudocysts almost always arise as a consequence of acute or chronic pancreatitis. Pseudocysts differ from true pancreatic cysts in that they lack an epithelial lining. Pseudocysts generally contain pancreatic fluids including pancreatic enzymes and zymogens and also often contain debris from degenerated pancreatic tissue. 1 Formation may occur following disruption of the main pancreatic ductal system due to inflammation, fibrosis, calculi or an obstructing protein plug. They may also result from pancreatic necrosis in the setting of severe pancreatitis. Chronic pancreatitis is associated with a higher incidence of pseudocysts than acute pancreatitis (20% to 40% versus 6% to 18.5%). 2,3,4 In patients with alcoholic chronic pancreatitis, incidence rates as high as 70% to 78% have been reported. 5 Chronic pancreatitis is associated with much lower rates of spontaneous regression, especially when compared to those with normal duct anatomy. 6 There have been several proposed classification systems of pancreatic pseudocysts based on morphology or etiology. The revised Atlanta classification characterizes a pseudocyst as a persistent acute peripancreatic fluid collection surrounded by a well-defined wall and contains essentially no solid material that generally arises after 4 weeks. 7 Another classification system proposed by D’Egidio and Schein, is based on the underlying etiology (acute or chronic pancreatitis), and takes the duct anatomy and presence of communication between the pseudocyst and pancreatic duct communication into account. 8 This system suggests that ductal anatomy is more important than pseudocyst
Transcript of Evaluation and Management of Pancreatic Pseudocysts · pancreatic ductal system due to...

Frontiers in endoscopy, series #10
12 Practical GastroenteroloGy • aPril 2014
Frontiers in endoscopy, series #10
Douglas G. Adler MD, FACG, AGAF, FASGE, Series Editor
Matthew E. Feurer MD, MS Douglas G. Adler MD, FACG, FASGE, AGAF University of Utah School of Medicine, Department of Internal Medicine, Division of Gastroenterology and Hepatology
Evaluation and Management of Pancreatic Pseudocysts
Douglas G. AdlerMatthew E. Feurer
introduction
Pancreatic pseudocysts are commonly encountered in clinical practice. The management of pancreatic pseudocysts is complex and can range from
simple observation to aggressive endoscopic and surgical interventions to treat symptomatic lesions. This manuscript will review the current evaluation and treatment of pancreatic pseudocysts.
overview of Pancreatic PseudocystsA pancreatic pseudocyst is a fluid-filled cavity that occurs within or adjacent to the pancreas that is surrounded by a wall of fibrous and/or granulomatous tissue. Pseudocysts almost always arise as a consequence of acute or chronic pancreatitis. Pseudocysts differ from true pancreatic cysts in that they lack an epithelial lining. Pseudocysts generally contain pancreatic fluids including pancreatic enzymes and zymogens and also often contain debris from degenerated pancreatic tissue.1 Formation may occur following disruption of the main pancreatic ductal system due to inflammation, fibrosis, calculi or an obstructing protein plug. They may also
result from pancreatic necrosis in the setting of severe pancreatitis. Chronic pancreatitis is associated with a higher incidence of pseudocysts than acute pancreatitis (20% to 40% versus 6% to 18.5%).2,3,4 In patients with alcoholic chronic pancreatitis, incidence rates as high as 70% to 78% have been reported.5 Chronic pancreatitis is associated with much lower rates of spontaneous regression, especially when compared to those with normal duct anatomy.6
There have been several proposed classification systems of pancreatic pseudocysts based on morphology or etiology. The revised Atlanta classification characterizes a pseudocyst as a persistent acute peripancreatic fluid collection surrounded by a well-defined wall and contains essentially no solid material that generally arises after 4 weeks.7 Another classification system proposed by D’Egidio and Schein, is based on the underlying etiology (acute or chronic pancreatitis), and takes the duct anatomy and presence of communication between the pseudocyst and pancreatic duct communication into account.8 This system suggests that ductal anatomy is more important than pseudocyst
Adler April 14.indd 12 4/1/14 8:51 PM

Frontiers in endoscopy, series #10
Pancreatic Pseudocysts
Practical GastroenteroloGy • aPril 2014 13
Frontiers in endoscopy, series #10
size in predicting spontaneous resolution and that size alone is not an indication for treatment.
Diagnosis Clinical presentation of a pseudocyst can vary from completely asymptomatic to acute or may involve the development of chronic complications. Acute complications include bleeding, infection, rupture or compression of adjacent vessels. Biliary or gastric outlet obstruction can occur from very large cysts, either acutely or over the long term. Given the limited utility of exam findings or serum tests, diagnosis of a pancreatic pseudocyst is generally confirmed by imaging studies.
Transabdominal ultrasound is an inexpensive and non-invasive technique for evaluation of pseudocysts, but has certain limitations. Sensitivity rates for pseudocyst detection are highly operator dependent and can range anywhere from 75% to 100%.9,10 Computerized tomography (CT) is often the imaging modality of choice, demonstrating high sensitivity (82% to 100%) and specificity (98%).11,12 Pseudocysts are demonstrated on CT as rounded, fluid-filled cavities surrounded by a thick wall, often in close proximity to the pancreas in patients with acute or chronic pancreatitis. A primary concern with CT is that up 10% of pseudocysts can have features in imaging that overlap with cystic tumors such as mucinous cystadenomas and intraductal papillary mucinous neoplasm. Differentiation of a pseudocyst from a cystic neoplasm is essential so that the optimal treatment can be devised, although in practice this can sometimes be difficult.13,14
Both magnetic resonance cholangiopancreatography (MRCP) and endoscopic retrograde cholangiopancreatography (ERCP) allow enhanced visualization of the pancreatic and biliary ductal systems. MRCP can also provide improved characterization of fluid collections when compared to CT, and is better at identifying solid tissue or debris within a cyst.15 ERCP allows evaluation of ductal anatomy and direct assessment of communication between a pseudocyst and the pancreatic duct. Rarely, a pseudocyst will communicate with the bile duct as well.16
Endoscopic ultrasound (EUS) is commonly used to further differentiate a pancreatic pseudocyst from other pancreatic cystic lesions, especially in patients without a clear history of pancreatitis.17 (Figure 1) Cyst fluid can be obtained for evaluation via fine needle aspiration at the time of EUS. Amylase levels of
greater than 5000 U/ml in cystic fluid were reported to have a sensitivity of 94% and a specificity of 74% in distinguishing pseudocysts from other cystic lesions.18 Elevated levels of carcinoembryonic antigen (CEA) and a viscosity of greater than 1.6 have also been shown to accurately predict mucinous cystadenoma from pancreatic pseudocyst. Most pseudocysts will have a very low cyst fluid CEA level and will not have extracellular mucin.19
Indications for TreatmentPrevious convention maintained that any pseudocyst that persisted more than six weeks should be intervened upon.20 This recommendation was based on a study by
Figure 1. 7.5MHz EUS image of a symptomatic pancreatic pseudocyst measuring 5.67cm in diameter. Note the thick, irregular walls of the lesion.
Figure 2. Large, symptomatic pancreatic pseudocyst which compressed the stomach and resulted in gastric outlet obstruction. Note the feeding tube in the stomach, as the patient could not tolerate oral feedings. The cyst ultimately underwent endoscopic transgastric drainage.
Adler April 14.indd 13 4/1/14 8:46 PM
14� Practical�GastroenteroloGy� •� aPril�2014
Frontiers in endoscopy, series #10Frontiers in endoscopy, series #10
Pancreatic Pseudocysts
Bradley that showed pseudocysts rarely resolved after seven weeks and were associated with a complication rate up to 50% after this time.21 More recent studies have demonstrated that conservative management with longer periods of observation have led to spontaneous resolution in approximately 60% of patients with serious complication rates of only 3% to 9%.22,23 The size of a pseudocyst has also been used as an indication for drainage. It was formerly recommended that any pseudocyst larger than 6 cm should be drained as these were less likely to resolve and would lead to greater complications.24 Although data regarding pseudocyst size and complication rates are mixed, a size less than 4 cm has been demonstrated to accurately predict spontaneous resolution. In general, however, size alone should not be used as an indicator for intervention.25
Currently, the decision to treat is based primarily on the presence of complications and/or symptoms.26,27,28
Symptoms that warrant intervention typically include infection, jaundice, bleeding (possibly from splenic artery pseudoaneurysm), pain, and gastric outlet obstruction (from gastric or duodenal compression). (Figure 2)
Treatment OptionsHistorically, surgical drainage was the only available option for the treatment of symptomatic pancreatic pseudocysts. More recently, percutaneous and endoscopic drainage techniques have become available. The decision of which method to use is based on local expertise, with the endoscopic approach now considered the first-line approach at many institutions.29 Surgical
drainage is preferred for complex pseudocysts if endoscopy is unavailable, not technically feasible, or in the event of endoscopic failure. Percutaneous drainage can be utilized for pseudocysts that are not adjacent to the GI lumen, do not obviously communicate with the pancreatic duct, or in poor surgical candidates.30
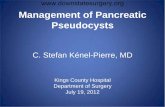
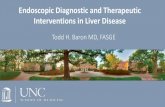
Surgical Treatment Surgical treatment options include open cystgastrostomy or cystenterostomy, partial pancreatic resection (particularly in disconnected pancreatic tail syndrome), and other laparoscopic approaches. Laparoscopic techniques, such as the lesser sac posterior cystgastrostomy, have been associated with lower morbidity and less bleeding compared to open procedures.31,32 Surgical approaches can often resolve symptomatic pancreatic pseudocysts in a single procedure and the surgeon can remove intracyst debris in some cases. (Figure 3)
Percutaneous DrainagePercutaneous catheter drainage of a pseudocyst involves the placement of a drainage catheter under CT or ultrasound guidance. This procedure is usually performed via interventional radiologists but can be done surgically as well. The catheter remains in place until the drainage rate is less than 5 to 10mL per day, at which point a follow-up imaging study, usually a CT scan, is performed to ensure that the catheter tip remains in the pseudocyst cavity. The mean duration of catheter placement in one study was 42 days, however this was also associated with a catheter tract infection rate of
Figure 3a. Laparoscopic creation of a surgical cystgastrostomy. The stomach is at the top of the frame and the pseudocyst cavity is below.
Figure 3b. Laparoscopic removal of large amounts of debris from within the cyst following creation of the cystgastrostomy.
Adler April 14.indd 14 4/1/14 8:47 PM
Frontiers in endoscopy, series #10Frontiers in endoscopy, series #10
Pancreatic Pseudocysts
Practical GastroenteroloGy • aPril 2014 15
48%.33 Percutaneous drainage has been shown to be less effective in resolution of pseudocysts in the presence of ductal communication or loculated pseudocysts.34,
35 For these reasons, surgery or other more aggressive interventions are generally preferred over percutaneous drainage in patients who can tolerate surgery, although this technique is still widely employed in appropriate candidates. Percutaneous drainage is often selected if the cyst is felt to be infected and the patient too acutely ill to undergo surgical or endoscopic drainage.
Endoscopic Treatment Endoscopic drainage of pseudocysts has emerged as a popular treatment approach for symptomatic lesions given its less invasive nature and lack of need for an external drain. A transpapillary approach using ERCP can be used when the cyst communicates with the main pancreatic duct. For pseudocysts adjacent to the gastroduodenal wall, a transmural (transgastric or transduodenal) approach is utilized.
Transpapillary DrainageIf a symptomatic pancreatic pseudocyst appears on imaging (CT, EUS, MRI/MRCP) to communicate with the pancreatic duct, transampullary drainage is often performed. If imaging studies are unclear or indeterminate in this regard, it is sometimes worthwhile to perform an ERCP and see if such a communication does or does not exist. The idea behind transampullary drainage is to create a communication between the cyst and the duodenal lumen using a stent in the pancreatic duct as a conduit.
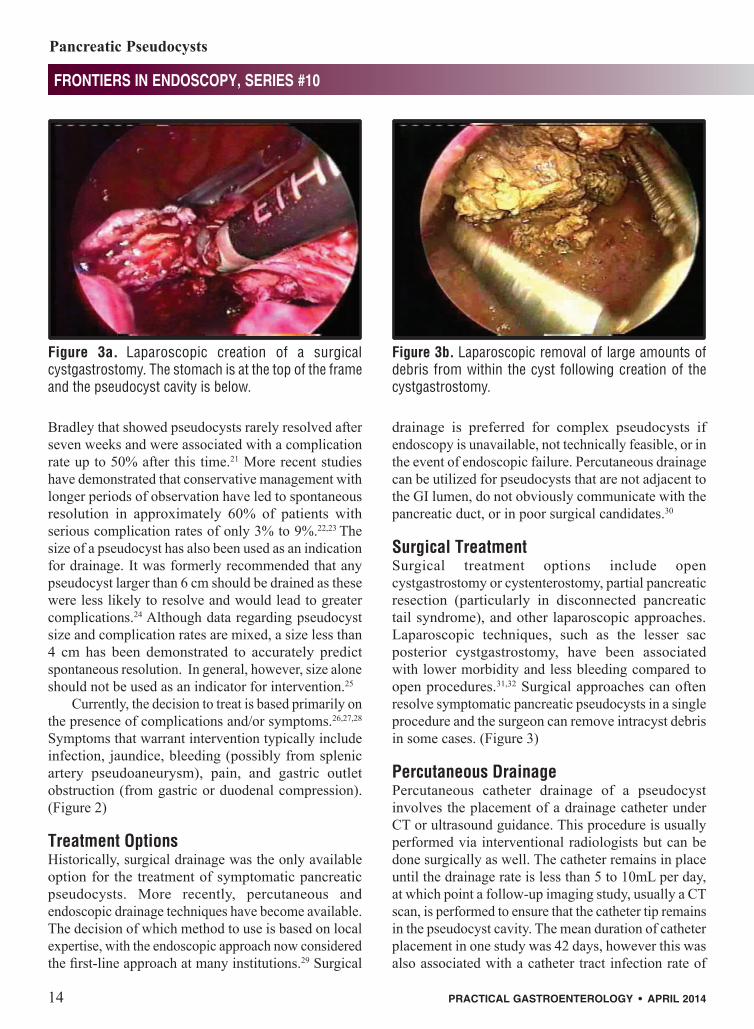
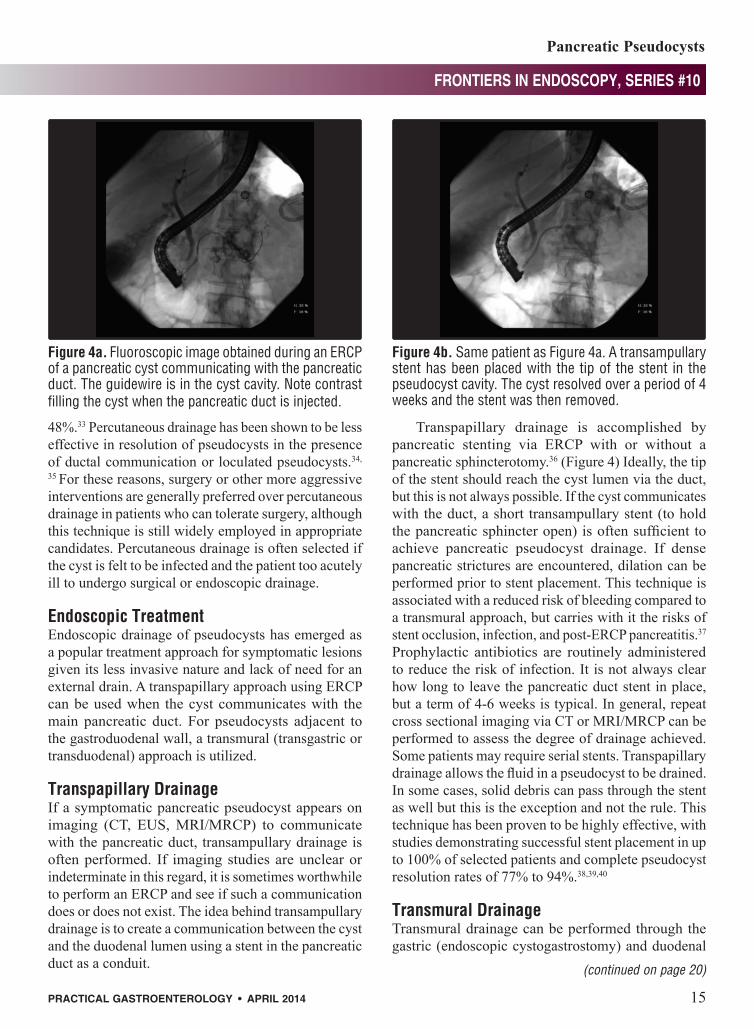
Transpapillary drainage is accomplished by pancreatic stenting via ERCP with or without a pancreatic sphincterotomy.36 (Figure 4) Ideally, the tip of the stent should reach the cyst lumen via the duct, but this is not always possible. If the cyst communicates with the duct, a short transampullary stent (to hold the pancreatic sphincter open) is often sufficient to achieve pancreatic pseudocyst drainage. If dense pancreatic strictures are encountered, dilation can be performed prior to stent placement. This technique is associated with a reduced risk of bleeding compared to a transmural approach, but carries with it the risks of stent occlusion, infection, and post-ERCP pancreatitis.37 Prophylactic antibiotics are routinely administered to reduce the risk of infection. It is not always clear how long to leave the pancreatic duct stent in place, but a term of 4-6 weeks is typical. In general, repeat cross sectional imaging via CT or MRI/MRCP can be performed to assess the degree of drainage achieved. Some patients may require serial stents. Transpapillary drainage allows the fluid in a pseudocyst to be drained. In some cases, solid debris can pass through the stent as well but this is the exception and not the rule. This technique has been proven to be highly effective, with studies demonstrating successful stent placement in up to 100% of selected patients and complete pseudocyst resolution rates of 77% to 94%.38,39,40
Transmural DrainageTransmural drainage can be performed through the gastric (endoscopic cystogastrostomy) and duodenal
(continued on page 20)
Figure 4b. Same patient as Figure 4a. A transampullary stent has been placed with the tip of the stent in the pseudocyst cavity. The cyst resolved over a period of 4 weeks and the stent was then removed.
Figure 4a. Fluoroscopic image obtained during an ERCP of a pancreatic cyst communicating with the pancreatic duct. The guidewire is in the cyst cavity. Note contrast filling the cyst when the pancreatic duct is injected.
Adler April 14.indd 15 4/1/14 8:47 PM

20� Practical�GastroenteroloGy� •� aPril�2014
Frontiers in endoscopy, series #10Frontiers in endoscopy, series #10
Pancreatic Pseudocysts
(endoscopic cystoduodenostomy) walls. This may be accomplished under EUS or non-EUS-guided techniques. Non-EUS guided drainage is a blind procedure and requires an endoscopically visible bulge to gain access. Other than the initial step of accessing the pseudocyst, the technique of EUS and non-EUS guided drainage are similar. It has been reported that from 42% to 48% of pseudocysts are non-bulging, and thus EUS-guided drainage is preferred in centers where it is available.41,42
ERCP-guided Transmural DrainageEndoscopic transmural drainage of pancreatic pseudocysts was developed in the pre-EUS era. The technique was developed as an outgrowth of ERCP and used ERCP accessories (needles, guidewires, stents, etc) in an off label manner. ERCP guided transmural drainage of pancreatic pseudocysts is still performed and is well within the standard of care.
Endoscopic approaches rely upon the creation of a cystenterostomy site, either a cystgastrostomy or a cystduodenostomy. In ERCP guided transmural drainage, endoscopic needle localization (ENL) is performed at the point of maximal endoscopic bulge (either in the stomach or the duodenum). Preprocedure CT or MRI scanning often allows the endoscopist to get a sense of where this location will be in advance and can also give information about the cyst itself, the thickness of the cyst wall, and the presence of any interposed vessels or varices (as can arise in patients with splenic vein thrombosis from pancreatitis). ENL is most commonly performed using a needle knife catheter, but other devices to perform this function are commercially available.43,44
Diathermic puncture utilizes a pre-curved biliary aspiration needle that is mounted in a 7-Fr catheter (HBAN22, Cook Endoscopy Inc. Winston-Salem, NC, USA) or a Cystotome (Cook Endoscopy, Inc. Winston-Salem, NC) or a standard needle knife catheter from any vendor (all of these are acceptable options). The needle is used to find a location with pancreatic cyst fluid return, at which point small amounts of radiocontrast are injected to determine if the pseudocyst has been entered.43 The Seldinger technique uses an 18 or 19 gauge needle (Cook Endoscopy, Inc, Winston-Salem, NC) for initial puncture and threading of a 0.035 or 0.018 inch guidewire into the pseudocyst. When compared to diathermic puncture in a study of 94
patients, successful entry was achieved in 95.3% versus 92.1%, with complications of bleeding and perforation seen in only 4.6% of the Seldinger group versus 15.7% in the diathermic puncture group.44 Following guidewire access, cystenterostomy tract dilation is performed with dilation balloon (often to a diameter of 8 or 10mm) prior to stent placement. Plastic stents, self-expanding metal stents, or a combination thereof can be used for drainage. Risks associated with transmural drainage include perforation and hemorrhage from interposed vessels.45,43
EUS-Guided Transmural DrainageThe first successful drainage of a pancreatic pseudocyst under EUS-guidance was described by Grimm et al. in 1992.46 This technique has gained widespread acceptance since that time. Pseudocyst drainage under EUS-guidance permits visualization of the cyst wall and fluid collection during the entire puncture and drainage procedure, hence identification of an endoscopic bulge is not strictly necessary. EUS can also help to differentiate cystic neoplasms from true pseudocysts prior to drainage and assist in determining management strategies. Very importantly, EUS allows for identification of any interposed vessels (via the use of Doppler) and may reduce the risk of bleeding. If vessels are seen between the stomach or duodenal wall and the pseudocyst, EUS can allow the endoscopist to identify another, safer site for needle puncture and tract dilation.
Studies have shown that information provided by EUS has altered drainage strategies in up to 37% of cases by identifying fluid collection contents, the presence of necrotic debris, interposed vessels, or other contraindications to endoscopic drainage.47,48 Interestingly, when directly compared to non-EUS guided drainage, Kahaleh et al demonstrated in a nonrandomized study that there was no significant difference in the rate of technical success (93% vs. 94%) or complication rate (19% vs. 18%) of EUS and non-EUS guided procedures respectively.49 The outcome of this study indicates that EUS-guided drainage can be carried out in cases without an endoscopically identifiable bulge without additional risk.
Under EUS-guided drainage, color doppler ultrasound is first used to identify an appropriate intraluminal puncture site that is without interposing vessels and within 1 to 2cm of the pseudocyst. Drainage can be performed via the Seldinger or needle knife
(continued from page 15)
Adler April 14.indd 20 4/1/14 8:47 PM

Frontiers in endoscopy, series #10Frontiers in endoscopy, series #10
Pancreatic Pseudocysts
Practical GastroenteroloGy • aPril 2014 21
technique described above, although cyst access is most commonly obtained using a 19gauge aspiration needle (which can accommodate a 0.025” or 0.035” guidewire). Following needle and guidewire insertion, the fistula tract can be dilated or enlarged using either a wire-guided balloon or cystenterotome with cautery.41 The balloon or cystenterstome is then exchanged and one or more stents can then be placed. Choice of stent is based in part on the type of instrumentation used, and again plastic stents, self-expanding metal stents, or a combination thereof can be used. A therapeutic linear echoendoscope with a channel size of 3.7 mm or 3.8 mm allows the placement of a 10 Fr plastic stent or a metal stent.45 The use of a therapeutic echoendoscope
Figure 5: Endoscopic transmural cystgastrostomy with combined EUS and ERCP endoscopes. Figure 5a. CT scan shows a large pseudocyst causing gastric compression and pain.
Figure 5c. Fluoroscopic image of EUS access to the cyst. A guidewire has been passed through a 19 gauge EUS FNA needle and is looped in the cyst.
Figure 5e. Follow up CT scan. The cyst has resolved. Double pigtail stents are visible.
Figure 5b. 7.5MHz EUS image of the cyst, measuring just over 8cm in size. No interposed vessels were identified.duct. The guidewire is in the cyst cavity. Note contrast filling the cyst when the pancreatic duct is injected.
Figure 5d. Final appearance of cystgastrostomy site after two double pigtail stents placed. A 7Fr stent was placed via the EUS scope, and a 10Fr stent was placed via a duodenoscope.
Adler April 14.indd 21 4/1/14 8:47 PM

Pancreatic Pseudocysts
Frontiers in endoscopy, series #10
22� Practical�GastroenteroloGy� •� aPril�2014
is commonly known as the single-step approach, which allows puncture of the pseudocyst under real-time EUS without the need for X-ray guidance or without changing the endoscope.42
Many endoscopists who have dual training in ERCP and EUS will use a combined approach to transmural cyst drainage. Linear EUS echoendoscopes have a relatively “weak” elevator and an oblique viewing angle when compared to duodenoscopes used during ERCP. A combined approach usually involves cyst evaluation, needle entry, tract dilation and the placement of the first stent via the echoendoscope and the placement of any subsequent stents via a duodenoscope to facilitate a more rapid procedure. (Figure 5)
Plastic Versus Self-Expandable Metal Stents for Transmural DrainageOnce a pseudocyst is accessed, drainage has historically been achieved with the placement of multiple plastic double pigtailed stents.49 These stents are designed to prevent migration (either into or out of the cyst) and allow drainage both through and between the stents themselves. Placement of multiple stents can increase procedure times due to the need to access the cyst cavity multiple times and/or increased technical difficulty. Nonetheless, the technique of placing multiple plastic stents has met with wide success. A recent study of 117 patients who underwent transmural drainage utilizing plastic stents resulted in overall treatment success of 98.3% (115/117 patients). Neither the size of plastic stent (7 or 10Fr) nor number of stents placed (1 or more) were found to impact outcomes.50
A growing body of literature has demonstrated the technical feasibility of using self-expandable metal stents (SEMS) for pancreatic pseudocyst drainage. In practice, these are usually covered SEMS to promote easy removability. Talreja et al. originally reported a 95% successful response rate for 18 patients who underwent transmural pseudocyst drainage using SEMSs.51 A later study by Fabbri, et al. achieved clinical success without additional intervention in 17 out of 20 patients who required SEMS placement with a mean follow-up of 610 days.52 Beroza et al. also reported excellent results with technical and clinical success in 7 out 7 patients where SEMSs were used for pseudocyst drainage. 53
These studies have highlighted several advantages of SEMSs over plastic stents, which include: a wider diameter than plastic stents which promotes drainage, elimination of the need for multiple stents or accessing
the pseudocyst multiple times, and reduced risk of stent occlusion.
In addition to the increased cost compared to plastic stents, the main concern with the use SEMS is the potential for stent migration (either into or out of the cyst) due to their coating. Some physicians place a double pigtail plastic stent through the SEMS to reduce the risk of migration, adding to the time and cost of the procedure slightly. Penn et al. reported on their experience placing a single double-pigtailed stent through the SEMS to serve as an anchor. Migration of the SEMS occurred out of the pseudocyst in 3 of 20 patients, however in two of these patients the inner pigtail of the internal plastic stent remained within the pseudocyst cavity, thereby preventing complete migration.54
There have been several reports of novel SEMSs specifically designed create transmural openings and to minimize the risk of migration. The use of a dumbbell-shaped, lumen-apposing covered stent (AXIOS, XLUMENA, Inc., San Francisco, CA, USA) was first reported by Itoi et al in 2012.55 In a study in which the AXIOS stent was successfully placed in 8 out of 9 patients, technical and clinical success rates were similar when compared to plastic double pigtail stents and no migrations of the AXIOS stent were reported.56 One patient in this study developed a tension pneumothorax after transesophageal stent placement, which indicates transesophageal placement of the AXIOS stent may be limited due to its large size. The AXIOS stent has gained FDA approval as of December 2013.
Recently, a single-step exchange free self-expanding metal drainage device (NAVIX, XLUMENA, Inc., San Francisco, CA, USA) has been described in several studies.56,57,58 The NAVIX device integrates a 3.5 mm retractable blade for puncture, an anchoring and dilating balloon, and two guidewire placement ports that allow double wire advancement for sequential stent placement. In cases where the NAVIX system was used, a median procedure time of 22 minutes was reported as opposed to a median time of 40 minutes using echoendoscopes that require device exchanges.56 In a study of 18 patients, Weilert et al. described use of the NAVIX single-step device to successfully place SEMSs in all 18 patients without complications.58 There was one incident of dehiscence following tract dilation in this study that was treated with SEMS placement. Further studies on this and similar devices are expected.
(continued on page 24)
Adler April 14.indd 22 4/1/14 8:47 PM

24� Practical�GastroenteroloGy� •� aPril�2014
Frontiers in endoscopy, series #10Frontiers in endoscopy, series #10
Pancreatic Pseudocysts
ConClusions
In the presence of symptoms or complications, endoscopic management of pancreatic pseudocysts is now considered a first-line approach. Patients without symptoms, complications or evidence of pseudocyst expansion on serial imaging may be observed with expectant management. For pseudocysts that communicate with the pancreatic duct, transpapillary drainage may be performed. For fluid collections amendable to a transmural approach, EUS guided drainage is commonly used given its ability to identify interposed vessels and detect possible malignancy prior to intervention, although ERCP guided approaches without EUS are also a viable option. A combined approach of transmural drainage utilizing both EUS and ERCP is often employed in centers with the appropriate expertise. In the event of endoscopic failure, open cystgastrostomy or cystenterostomy is generally pursued. Percutaneous catheter drainage should be reserved for those with contraindications to endoscopy and who are poor surgical candidates.
Based on the increasing number of studies that have reported on the safety and efficacy of EUS-guided transmural pseudocyst drainage, it has continued to gain in acceptance. The continued development of accessory devices such as the AXIOS SEMS and the NAVIX delivery system will likely contribute to the increased use of endoscopy for the management of pseudocysts in the future. n
References
1. Kloppel G. Pseudocysts and other non-neoplastic cysts of the pancreas. Semin Diagn Pathol 2000;17:7Y15.
2. Imrie CW, Buist LJ, Shearer MG. Importance of cause in the outcome of pancreatic pseudocysts. Am J Surg 1988;156:159–62.
3. Maringhini A, Uomo G, Patti R et al. Pseudocysts in acute nonalcoholic pancreatitis: incidence and natural history. Dig Dis Sci 1999;44:1669–73.
4. Barthet M, Bugallo M, Moreira LS, et al. Management of cysts and pseudocysts complicating chronic pancreatitis. A retrospective study of 143 patients. Gastroenterol Clin Biol1993; 17: 270–6.
5. Ammann RW, Akovbiantz A, Largiader F, Schueler G: Course and outcome of chronic pancreatitis. Longitudinal study of a mixed medical-surgical series of 245 patients. Gastroenterology 1984; 86:820–8.
6. Nealon WH, Bhutani M, Riall TS, et al. A unifying concept: pancreatic ductal anatomy both predicts and determines the major complications resulting from pancreatitis. .J Am Coll Surg. 2009 May;208(5):790-9; discussion 799-801.
7. Banks PA, Bollen TL, Dervenis C, et al. Acute Pancreatitis
(continued from page 22) Classification Working Group. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013 Jan;62(1):102-11.
8. D’Egidio A, Schein M. Pancreatic pseudocysts: A proposed classification and its management implication. Br. J. Surg. 1991; 78: 981–84.
9. Pitchumoni CS, Agarwal N. Pancreatic pseudocysts. When and how should drainage be performed? Gastroenterol Clin North Am 1999; 28: 615-639.
10. Polakow J, Ladny JR, Serwatka W, et al. Percutaneous fine-needle pancreatic pseudocyst puncture guided by three-dimensional sonography. Hepatogastroenterology.2001;48:1308-1311.
11. Balthazar EJ, Freeny PC, vanSonnenberg E. Imaging and intervention in acute pancreatitis. Radiology. 1994; 193: 297–306.
12. Lee JK, Stanley RJ, Melson GL, et al. Pancreatic imaging by ultrasound and computed tomography: a general review. Radiol Clin North Am. 1979;17:105Y117.
13. Brugge WR, Lewandrowski K, Lee-Lewandrowski E, et al. Diagnosis of pancreatic cystic neoplasms: a report of the cooperative pancreatic cyst study. Gastroenterology. 2004;126:1330-1336.
14. Lehman GA. Pseudocysts. Gastrointest Endosc. 1999;49:S81-S84.
15. Sahani D, Prasad S, Saini S, et al. Cystic pancreatic neo-plasms evaluation by CT and magnetic resonance cholan-giopancreatography. Gastrointest Endosc Clin N Am. 2002 Oct;12(4):657-72.
16. Nealon WH, Bhutani M, Riall TS, et al. A unifying concept: pancreatic ductal anatomy both predicts and determines the major complications resulting from pancreatitis. J Am Coll Surg. 2009 May;208(5):790-9.
17. Baron TH. Endoscopic drainage of pancreatic pseudocysts. J Gastrointest Surg 2008;12:369-372.
18. Hammel P, Levy P, Voitot H, et al. Preoperative cyst fluid analysis is useful for the differential diagnosis of cystic lesions of the pancreas. Gastroenterology 1995;108:1230-1235.
19. Linder JD, Geenen JE, Catalano MF. Cyst fluid analysis obtained by EUS-guided FNA in the evaluation of discrete cystic neoplasms of the pancreas: a prospective single-center experience. Gastrointest Endosc 2006; 64: 697-702.
20. Bradley EL. A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Arch Surg 1993; 128: 586–90.
21. Bradley EL, Gonzalez AC, Clements JL, Jr. Acute pancreatic pseudocysts: incidence and implications. Ann Surg 1976; 184: 734–7.
22. Vitas GJ, Sarr MG. Selected management of pancreatic pseu-docysts: operative versus expectant management. Surgery 1992;111:123–30.
23. Yeo CJ, Bastidas JA, Lynch-Nyham A, et al. The natural history of pancreatic pseudocysts documented by computed tomography. Surg Gynecol Obstet 1990;170:411–7.
24. Bergman S, Melvin WS. Operative and nonoperative man-agement of pancreatic pseudocysts. Surg Clin North Am 2007;87:1447–60.
25. Gouyon B, Levy P, Ruszniewski P et al. Predictive factors in the outcome of pseudocysts complicating alcoholic chronic pancreatitis. Gut 1997; 41:821–5.
26. Habashi S, Draganov PV. Pancreatic pseudocyst. World J Gastroenterol 2009;15(1):38-47.
27. Seewald S, Ang TL, Teng KC, et al. EUS-guided drainage of pancreatic pseudocysts, abscesses and infected necrosis. Dig Endosc 2009;21 Suppl 1:S61-5.
28. Lerch MM, Stier A, Wahnschaffe U, et al. Pancreatic pseudo-cysts: observation, endoscopic drainage, or resection? Dtsch Arztebl Int. 2009;106(38):614-21.
Adler April 14.indd 24 4/1/14 8:48 PM

Frontiers in endoscopy, series #10Frontiers in endoscopy, series #10
Pancreatic Pseudocysts
Practical GastroenteroloGy • aPril 2014 25
29. Varadarajulu S, Lopes TL, Wilcox CM, et al. EUS ver-sus surgical cyst-gastrostomy formanagement of pancreatic pseudocysts. Gastrointest Endosc 2008;68:649–55.
30. Nealon WH, Walser E. Main pancreatic ductal anatomy can direct choice of modality for treating pancreatic pseu-docysts (surgery versus percutaneous drainage). Ann Surg 2002;235(6):751-8.
31. Dávila-Cervantes A, Gómez F, Chan C, et al. Laparoscopic drainage of pancreatic pseudocysts. Surg Endosc 2004;18:1420.
32. Park AE, Heniford BT. Therapeutic laparoscopy of the pan-creas. Ann Surg 2002;236:149–58.
33. Adams DB, Anderson MC. Percutaneous catheter drainage compared with internal drainage in the management of pan-creatic pseudocyst. Ann Surg 1992;215(6):571.
34. Heider R, Meyer AA, Galanko JA, et al. Percutaneous drain-age of pancreatic pseudocysts is associated with a higher failure rate than surgical treatment in unselected patients. Ann Surg 1999; 229:781-787.
35. Nealon WH, Walser E. Main pancreatic ductal anatomy can direct choice of modality for treating pancreatic pseu-docysts (surgery versus percutaneous drainage). Ann Surg 2002;235:751–8.
36. Catalano MF, Geenen JE, Schmalz MJ, et al. Treatment of pancreatic pseudocysts with ductal communication by transpapillary pancreatic duct endoprosthesis. Gastrointest Endosc 1995;42:214–8.
37. Varadarajulu S, Noone TC, Tutuian R, et al. Predictors of outcome in pancreatic duct disruption managed by endo-scopic transpapillary stent placement. Gastrointest Endosc 2005;61:568–575.
38. Binmoeller KF, Seifert H, Walter A, et al. Transpapillary and transmural drainage of pancreatic psuedocysts. Gastrointest Endosc 1995;42:219-224.
39. Kozarek RA, Ball TJ, Patterson D, et al. Endoscopic transpap-illary therapy for disrupted pancreatic duct and peripancre-atic fluid collections. Gastroenterology 1991;100:1362-70.
40. Barthet M, Sahel J, Bodiou-Bertei C, et al, Endoscopic trans-papillary drainage of pancreatic pseudocysts. Gastrointest Endosc 1995;42:208-213.
41. Sanchez Cortes E, Maalak A, Le Moine O, et al. Endoscopic cystenterostomy of nonbulging pancreatic fluid collections. Gastrointest Endosc 2002;56:380-386.
42. Antillon MR, Shah RJ, Stiegmann G, et al. Single-step EUS-guided transmural drainage of simple and complicated pan-creatic pseudocysts. Gastrointest Endosc 2006;63:797-803.
43. Howell DA, Holbrook RF, Bosco JJ, et al. Endoscopic nee-dle localization of pancreatic pseudocysts before transmural drainage. Gastrointest Endosc 1993;39:693–8.
44. Mönkemüller KE, Baron TH, Morgan DE. Transmural drainage of pancreatic fluid collections without electrocau-tery using the Seldinger technique. Gastrointest Endosc 1998;48:195–200.
45. Giovannini M. EUS-guided pancreatic pseudocyst drainage. Tech Gastrointest Endosc 2007;9:32-38.
46. Grimm H, Binmoeller KF, Soehendra N. Endosonography guided drainage of a pancreatic pseudocyst. Gastrointest Endosc 1992;38:170.
47. Fockens P, Johnson TG, van Dullemen HM, et al. Endosonographic imaging of pancreatic pseudocysts before endoscopic transmural drainage. Gastrointest Endosc 1997;46:412–6.
48. Varadarajulu S, Wilcox CM, Tamhane A, et al. Role of EUS in drainage of peripancreatic fluid collections not amenable for endoscopic transmural drainage. Gastrointest Endosc 2007;66:1107–19.
49. Kahaleh M, Shami VM, Conaway MR, et al. Endoscopic ultrasound drainage of pancreatic pseudocyst: a prospec-tive comparison with conventional endoscopic drainage. Endoscopy 2006;38:355-359.
50. Bang JY, Wilcox CM, Trevino JM, et al. Relationship
between stent characteristics and treatment outcomes in endoscopic transmural drainage of pancreatic pseudocysts. Gastrointest Endosc 2013;77(5 Suppl):AB382.
51. Talreja JP, Shami VM, Ku J, et al. Transenteric drainage of pancreatic-fluid collections with fully covered self-expanding metallic stents (with video). Gastrointest Endosc 2008;68: 1199-1203.
52. Fabbri C, Luigiano C, Cennamo V, et al. Endoscopic ultra-sound-guided transmural drainage of infected pancreatic fluid collections with placement of covered self-expanding metal stents: a case series. Endoscopy 2012;44:429-433.
53. Berzosa M, Maheshwari S, Patel KK, et al. Single-step endoscopic ultrasonography-guided drainage of peripan-creatic fluid collections with a single self-expandable metal stent and standard linear echoendoscope. Endoscopy 2012;44:543-547.
54. Penn DE, Draganov PV, Wagh MS, et al. Prospective evalu-ation of the use of fully covered self-expanding metal stents for EUS-guided transmural drainage of pancreatic pseudo-cysts. Gastrointest Endosc 2012;76:679-684.
55. Itoi T, Binmoeller KF, Shah J, et al. Clinical evaluation of a novel lumen-apposing metal stent for endosonography-guided pancreatic pseudocyst and gallbladder drainage (with videos). Gastrointest Endosc 2012;75:870-876.
56. Gornals JB, De la Serna-Higuera C, Sánchez-Yague A, et al. Endosonography-guided drainage of pancreatic fluid collections with a novel lumen-apposing stent. Surg Endosc 2013;27:1428-1434.
57. Binmoeller KF, Weilert F, Shah JN, et al. Endosonography-guided transmural drainage of pancreatic pseudocysts using an exchange-free access device: initial clinical experience. Surg Endosc 2013;27:1835-1839.
58. Weilert F, Binmoeller KF, Shah JN, et al. Endoscopic ultra-sound-guided drainage of pancreatic fluid collections with indeterminate adherence using temporary covered metal stents. Endoscopy 2012;44:780-783.
CelebratingOur
38 th Year
PRACTICAL GASTROENTEROLOGY
practicalgastro.com
Adler April 14.indd 25 4/1/14 8:48 PM