EuroTimes Vol. 19 - Issue 3
44
SPECIAL RETINA INDUSTRY NEWS Company Updates EYE ON TRAVEL Come see London VOLUME 19 ISSUE 3 MARCH 2014
description
A European Outlook on the World of Ophthalmology
Transcript of EuroTimes Vol. 19 - Issue 3

Special
RETINA
induStry newScompany updates
EyE oN TRAvElcome see london
VOLUME 19 ISSUE 3 March 2014

Bre
ath
taki
ng
Strong
Any nucleus from soft to hardest, any incision from
1.6 to 3.2 mm, fast, safe and the AC always stable.
That’s easyPhaco®. CortexModeTM for precisely con-
trolled cortical clean-up. HF capsulotomy for difficult
cases. 1200 cuts anterior vitrectomy.
Beautiful
So easy to operate! DirectAccess® to any function
without confusion. Programmable for 20 surgeons.
Bright, easy to read display. A marvel of design,
brings a friendly note in your OR.
Unique
Truly portable, 5 kg, fits in a pilot’s case. HFDS ab
interno glaucoma function, the future of combined
glaucoma surgery. Fantastic toe tip of flow control.
Built-in compressor. Just plug to 90-230 V.
For You
Lets you enjoy most advanced surgery from low to
highest volume in any set-up at controlled costs.
www.oertli-catarhex3.com
Eckn
auer
+Sc
hioc
h A
SW

6
16
32
10
24
39
This issUE...
Special Focus: Retina 3 Following protocols can help to improve
visual outcomes in neovascular AMD patients
4 Guidelines on the way for anti-VEGF agent use in the treatment of neovascular AMD
5 New instruments aid tissue dissection in eyes with proliferative diabetic retinopathy
6 Gene therapy could be way forward in managing some retinal diseases
7 New aids for charting geographic atrophy progression
8 Retinal specialists invited to participate in EsCRs Endophthalmitis Registry
Cataract & Refractive 9 Further study needed in regards to
cataract surgery anaesthesia10 New surgical approaches could reduce
the incidence of PCO after cataract surgery
11 Understanding the mechanisms of accommodating iOLs
12 Combined approach can aid forme fruste keratoconus patients
13 PREMED study hopes to provide guidelines to help manage CME after surgery
14 LAsiK treatments using new planning system showing good preliminary results
16 silicone tip instrument can reduce complications in cataract surgery
17 study shows good results for controlling macular swelling with dual medication
18 A number of techniques can be employed to avoid astigmatism post-keratoplasty
19 Controversy surrounds the desired refractions for pseudophakic monovision
20 Lifestyle factors should be considered when choosing the ideal iOL
Cornea 21 Patients being advised to blink more to
alleviate dry eye symptoms22 DMEK worth the extra effort, says
expert23 OCT could improve corneal disease
screening and diagnosis24 New limbal deficiency treatments based
on understanding corneal epithelium
Glaucoma 25 Can end-of-life visual impairment be
improved in glaucoma patients?26 Measures discussed to insure good
outcomes from trabeculectomy procedure
Ocular 27 Providing eye care services was an
important part of the London Olympic Games
News 28 EsAsO helps develop career paths for
young ophthalmologists29 New technique for glaucoma surgery
has many advantages
Features 30 Resident’s Diary31 Book Review32 Eye on Travel33 JCRs highlights35 Ophthalmologica highlights37 Outlook on industry39 industry News40 Calendar of Events
1
march 2014Volume 19 | Issue 3
EUROTIMESESC
RS ™
With this issue... wSpoS paediatric SUB Specialty day, 5th eUcornea congreSS, 14th eUretina congreSS & xxxii congreSS of the eScrS preliminary programmeS
Cover image shows the left eye of a 34-year-old female patient with Stargardt disease, showing whitish flecks on the fundus picture (FP), which hyperautofluoresce on blue-light autofluorescence images (BAF); fluorescein angiography (FA) shows relative dark choroid consequent upon accumulation of lipofuscin in retinal pigment epithelial cells. Image is courtesy of Bart P Leroy MD, PhD.
Publisher Carol FitzpatrickExecutive Editor Colin KerrEditors sean henahan Paul McGinn
Managing Editor Caroline BrickProduction Editor Angela sweetmanAdvertising Executive Mairin Condon Senior Designer Janice Robb
Designer Lara FitzgibbonCirculation Manager Angela Morrissey Contributing Editors howard Larkin Dermot McGrath Roibeard Ó hÉineacháin Contributors Devon schuyler Eisele stefanie Petrou-Binder Maryalicia Post
Leigh spielberg Pippa Wysong Gearóid Tuohy Priscilla LynchColour and Print W&G Baird PrintersAdvertising Sales EsCRs, Temple house, Temple Road Blackrock, Co. Dublin, ireland Tel: 353 1 209 1100 Fax: 353 1 209 1112 email: [email protected]
Published by the European Society of Cataract and Refractive Surgeons Temple House, Temple Road, Blackrock, Co Dublin, Ireland. No part of this publication may be reproduced without the permission of the managing editor. Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review and acceptance.
ESCRS EuroTimes is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS EuroTimes.ISSN 1393-8983
edito
rial s
taff
EUROTIMESESC
RS ™
Published byThe European Society of Cataract and Refractive Surgeons
As certified by ABC, the EuroTimes average net circulation for the 11 issues distributed between 01 January 2013 and 31 December 2013 is 40,878.

by Francesco Bandello
As president of EURETiNA, it gives me great pleasure to write this editorial for EuroTimes.
These are busy times for the society and we have recently concluded our 4th EURETiNA Winter Meeting
in Rome which was a great success.We are also busy preparing for the 14th EURETiNA Congress
which will take place in London from 11-14 september 2014, and i advise you to visit our website at: www.euretina.org to keep up to date with all the latest news on the meeting.
Our 13th Congress in hamburg last year was a great success with more than 4,000 delegates attending. As my friend and colleague Gisbert Richard pointed out in his presidential address in hamburg, when we held our first congress we had 300 attending guests. The phenomenal growth in the number of delegates attending the meeting is a tribute to the hard work done by Prof Richard and the other founding members in establishing EURETiNA as the world’s leading retina organisation.
so what lies ahead for EURETiNA? We cannot stand still and we must continue to build the society. Our challenge every year as we prepare for a new congress is to make sure we have an excellent scientific Programme with contributions from some of the key opinion leaders from all over the world.
At our Winter Meeting we discussed some of the major issues of interest to retinal specialists including Metabolomics in Diabetes Mellitus, Methods to Evaluate the Retinal Circulatory Disorders and Retinal Metabolism and New Therapy Delivery Methods which generated some excellent debate. We are looking forward to continuing these debates in London.
it is important that we talk to each other about the key areas that are of interest and concern to us but it is also important that we back-up our talk with actions. For that reason, EURETiNA is continuing to build a strong research and educational base. As i discussed last year in an interview with EuroTimes, we need to develop diagnostic techniques that will detect more accurately and consistently the structural changes that correspond with losses and gains in vision. in addition, we need to develop intravitreal agents that will remain effective in the eye for longer than is currently the case.
it should be remembered that EURETiNA is still a comparatively young organisation. Much credit must be given to the pioneers who established and built the society but another major challenge facing us is to make sure that the young ophthalmologists who are the future of retinal medicine will play a major part in the society.
This must be done, not only by encouraging young ophthalmologists to attend our meetings, but also by inviting them to sit on our committees and play an active part in the day-to-day running of EURETiNA.
Let me conclude by thanking the editors of EuroTimes for giving me the opportunity to address the readers. i am delighted to note that the coverage of retina in the magazine is continuing to increase.
14th EURETINA Congress will take place in London from 11-14 September 2014
EUROTIMES | Volume 19 | Issue 3
2
GUEST EDITOrIaL Volume 19 | Issue 3
editorial
CHALLENGING TIMESEURETINA is planning ahead to meet the challenges facing retina specialists
José Güell
Clive Peckar
Emanuel RosenChairman
ESCRS Publications Committee
Ioannis Pallikaris
Paul Rosen
Medical Editors
International Editorial Board
EUROTIMESESC
RS ™
noel alpins australia
Bekir aslan turKEY
Bill aylward uK
peter Barry irElaND
roberto Bellucci italY
Béatrice cochener fraNcE
hiroko Bissen-miyajima JaPaN
John chang cHiNa
alaa el danasoury sauDi araBia
oliver findl austria
i howard fine usa
Jack holladay usa
Vikentia Katsanevaki GrEEcE
thomas Kohnen GErMaNY
anastasios Konstas GrEEcE
dennis lam HONG KONG
Boris malyugin russia marguerite mcdonald usa
cyres mehta iNDia
thomas neuhann GErMaNY
rudy nuijts tHE NEtHErlaNDs
gisbert richard GErMaNY
robert Stegmann sOutH africa
Ulf Stenevi sWEDEN
emrullah tasindi turKEY
marie-Jose tassignon BElGiuM
manfred tetz GErMaNY
carlo enrico traverso italY
roberto Zaldivar arGENtiNa
oliver Zeitz GErMaNY
* Francesco Bandello is president of EURETINA
Francesco Bandello – [email protected]

Closer adherence to published protocols concerning anti-VEGF use, and more aggressive treatment of patients with
neovascular AMD could help to improve visual outcomes in these patients, according to Frank holz MD.
Presenting data from the AURA study, an international retrospective analysis of the real-world utilisation of anti-VEGF therapy in neovascular age-related macular degeneration, Dr holz told delegates attending the 13th EURETiNA Congress in hamburg, that physicians need to consider ways to improve adherence to the published guidelines and recommendations in order to improve the functional benefit of breakthrough anti-VEGF therapy.
“We found overall that the real life utilisation of anti-VEGF therapy was associated with a poorer outcome than might have been expected based on the results from the pivotal prospective randomised clinical trials of ranibizumab. What is clear is that factors such as the monthly visits and the number of injections seem to play a very important role in maximising outcomes, as countries with a higher number of visits and higher number of injections showed better performance in terms of visual outcomes of the patients,” he said.
The objectives of the AURA study were to collect “real life” data on clinical management patterns and resources utilisation in patients with exudative AMD being treated with anti-VEGF therapy in routine clinical practice, said Dr holz.
The clinical endpoints of the study were to evaluate changes in visual acuity and resource utilisation in terms of overall visits, visual acuity and OCT tests and treatment use following anti-VEGF treatment with up to 2.5 years follow-up.
A total of 2,671 patients were enrolled in the study, with 2,227 included in the final effectiveness analysis set. Data was collated from centres in Canada, France, Germany, ireland, italy, Netherlands, UK and Venezuela.
Two years of treatment with ranibizumab resulted in no observed change in visual acuity final score in patients with neovascular AMD in this study, said Dr holz, and the overall number of visits, monitoring visits and number of injections were lower in the second year than in the first year.
Overall, 9.8 visual acuity tests were performed over the study duration. Patients received a mean of five injections in the first year and two injections in the second year.
Patients in the UK fared the best, while results varied in the other countries. There are a number of possible explanations for the disparity in outcomes obtained in participating countries, said Dr holz, some of which might be health-system related or physician- or patient-related.
“When we look at reasons why the United Kingdom performed better than the other countries, we see that the average number of patient visits there was 18.4 over two years, compared to Germany, for example, where it was 10.8. And the number of injections in the United Kingdom was nine while in the other countries it was almost half that. so it seems reasonable to conclude that how closely these patients are monitored, examined and re-injected if necessary seems to be a driving factor in their outcomes,” he said.
Dr holz added that poorer than expected visual outcomes were due to less than monthly monitoring and low numbers of treatments per year.
“Although these results are certainly much better than untreated evolution of neovascular AMD, consideration should be given to closer adherence to published protocols and/or potential barriers to optimal PRN treatment,” he concluded.
3
REALITY CHECKCloser adherence urged to improve AMD outcomesby Dermot McGrath
contact Frank Holz – [email protected]
T. +1 416.398.3306 F. +1 416.631.8272 | www.innovativexcimer.com
Improved Clinical Outcomes of CXL and PRK with Amoils Epithelial Scrubber
Epithelial Removal Has Never Been Easier
Corneal Xlinking, PRK & Advanced Surface
Ablation
• Uniform epithelium removal in only 5 - 7 seconds
• Avoid alcohol damage to surrounding tissue
• Minimize total procedure time
• No need for subsequent scraping
EUROTIMES | Volume 19 | Issue 3
Special focus
rETINa
Although these results are certainly much better than untreated evolution of neovascular AMD, consideration should be given to closer adherence to published protocols and/or potential barriers to optimal PRN treatment
“
Frank Holz MD

EUROTIMES | Volume 19 | Issue 3
EURETiNA has developed a soon-to-be-published set of evidence-based guidelines for the use of anti-VEGF agents in the treatment of neovascular AMD. it will be published in the British Journal
of Ophthalmology, said Ursula schmidt-Erfurth MD, University Eye hospital in Vienna, Austria.
The time is ripe for such guidelines because intravitreal anti-VEGF therapy has proven its potential to reduce the incidence of blindness from AMD, and because data from clinical studies has accrued to a point where it can provide useful insights into the optimal treatment regimens and appropriate diagnostic criteria for the condition, Dr schmidt-Erfurth said at the 13th EURETiNA Congress in hamburg.
As an illustration of the impact the advent of anti-VEGF agents have had on society, she cited a study conducted in Denmark showing that the incidence of AMD-associated legal blindness in that country per 100,000 people aged 50 years or over fell from 52.2 in 2001 to 25.7 in 2010. The bulk of the reduction occurred in the years after 2006 when anti-VEGF agents first became available (S Bloch et al, Am J Opth,153:2: 209-213I).
since the condition requires treatment for the lifetime of the patient, retinal specialists can expect an increasing caseload of neovascular AMD patients in years to come. Evidence-based guidelines are therefore crucial to insuring that the available resources are directed towards those patients who are actually likely to benefit and to also insure that those patients receive the optimal regimen.
“The management of AMD has to be practical and economic in terms of diagnosis and therapy for the entire population in all subgroups at all times in all patients,” she said.
Dosing and regimen One of the main controversies regarding anti-VEGF agents in the treatment of neovascular AMD is the question of whether patients should receive the agent on a fixed regimen or PRN basis.
The results from the hARBOR study showed that a 0.5 dosage of ranibizumab (Lucentis®, Novartis) was no more effective than a 0.2mg dosage in terms of visual acuity and that a monthly regimen and a PRN regimen achieved similar results with about one third of patients in each group gaining 15 or more letters of BCVA during the first year (Busbee et al Ophthalmology2013; doi: 10.1016/j.ophtha.2012.10.014).
she noted that the decision to treat in the PRN group was based on monthly monitoring with spectral domain OCT and the trial results may therefore represent the best that can be achieved with a PRN regimen.
The findings of the hARBOR study may also add to the emerging evidence that long-term anti-VEGF therapy for neovascular AMD can cause geographic atrophy. The study showed that although patients’ central foveal thickness continued to decrease throughout 24 months of treatment, some of the vision gained during the first year was lost during the second year in all of the treatment groups.
“The fact that the retina becomes flatter over time may not be a good thing over the years. There is over-treatment and there is under-treatment. We have to find out how to keep patients between these two extreme poles,” she said.
Ranibizumab vs. bevacizumab Dr schmidt-Erfurth noted that the results of the CATT study showed that both ranibizumab and bevacizumab (Avastin®, Genentech) provide results that are highly satisfactory and roughly equivalent, when administered on a fixed monthly regimen. however, the study failed to prove the non-inferiority of bevacizumab to ranibizumab when administered on an as-needed basis (Martin et al, Ophthalmology 2012;119: 1388-1398).
in addition, patients receiving a fixed monthly regimen of ranibizumab had a significantly greater reduction in central retinal thickness than those receiving the PRN ranibizumab regimen and both of the bevacizumab regimens. The study also showed less favourable results for bevacizumab in terms of adverse events. At one year’s follow-up, the proportion of patients with one or more systemic serious adverse events was significantly higher with bevacizumab than ranibizumab (39.9 per cent vs. 31.7 per cent, P = 0.009). The relevance of the finding has been debated on the basis that most were events not of the sort typically associated with VEGF inhibition.
Aflibercept Aflibercept (EYLEA ®, Regeneron), formerly known as VEGF-trap, is the latest addition to the anti-VEGF agent armamentarium and results from the View 1 and View 2 trials indicate that a two-monthly regimen of 0.5mg aflibercept produced results equal to those achieved with monthly injections of 0.2mg ranibizumab. in all treatment arms of the two studies, patients first received three monthly intravitreal injections of the anti-VEGF agent.
“Our recommendation regarding currently available anti-VEGF agents is that ranibizumab, bevacizumab and aflibercept are all effective in neovascular AMD. Aflibercept seems to work slightly better than ranibizumab and ranibizumab is a little bit better than bevacizumab. With the monthly strategy or even a bimonthly strategy these differences are irrelevant, however, when you switch over to a PRN regiment then the differences become more evident,” Dr schmidt-Erfurth said.
EURETINA GUIDELINESResearch providing a clearer picture of optimal anti-VEGF treatment for neovascular AMDby Roibeard O’hEineachain
4
Avoiding astigmatic surprisesWhat is the best approach to dealing with astigmatism before and after cataract surgery? Dr Oliver Findl talks to Dr Noel Alpins about current and innovative methods of pre-op visual assessment and IOL calculation.
EYE CHAT
Exclusive interviewsUp to date informationProblem solving
Scan this QR code to gain access to EuroTimes podcasts
podcastwww.eurotimes.org
Also available on iTunes
Ursula Schmidt-Erfurth – [email protected]
contact
Special focus
rETINa
The fact that the retina becomes flatter over time may not be a good thing over the years. There is over-treatment and there is under-treatment
“Ursula Schmidt-Erfurth MD

EUROTIMES | Volume 19 | Issue 3
Newer small-gauge vitrectomy instruments can facilitate the dissection of all types of proliferative tissue in eyes with
proliferative diabetic retinopathy, said Borja Corcóstegui MD at the 13th EURETiNA Congress in hamburg.
“Good results can be achieved with any size of instrument, and it is up to the surgeon's preference which gauge to use. however, 23-gauge or new 25-gauge with a variable duty cycle seems to be the more acceptable size of instrument to use today, said Dr Corcóstegui, institut de Microcirurgia Ocular (iMO) Barcelona, spain.
The advantages of small-gauge instruments include a small port that is closer to the distal end of the probe, and a better duty cycle than the older cutters. Furthermore, the shape of the port of vitreous cutters enables a more efficient removal of proliferative tissue from the macula, Dr Corcóstegui noted.
“25-gauge or 27-gauge instruments can be very useful in removing proliferative tissue over the retina especially over the main veins. it is also a good idea to use valved micro-cannulas to avoid having a low pressure during the operation and bleeding inside of the eye,” he added.
he noted that, prior to surgery, it is essential to perform fundus examination in order to determine the extent and location of the vitreoretinal attachments and the amount of proliferative tissue present. in many cases a B scan will be necessary because of an opaque vitreous.
The goal of surgery in eyes with proliferative diabetic retinopathy is to remove the maximum amount of proliferations while avoiding damage to the main retinal vessels and the creation of retinal breaks and controlling retinal bleeding during the operation, Dr Corcóstegui said.
Surgical strategies Dr Corcóstegui noted that he uses three different surgical strategies depending on the place of the proliferation and the extent of the proliferation.
in the simpler cases he will simply remove the proliferative tissue over the
retina using only the new 23-gauge and 25-gauge vitreous cutters with a one-handed technique.
in the more complex cases with much more proliferative tissue and where the space between the proliferation and the retina cannot be visualised, he uses a bimanual method with a forceps and a 23-gauge or 25-gauge vitreous cutter.
Using a light irrigation system and infusion, he teases the proliferative tissue to one side with a forceps to find the attachments points, which he then slowly removes with controlled pressure. At the end of the operation he removes all the proliferation over the macula.
Avoid surgical bleeding he also uses a bimanual approach in eyes with proliferative diabetic retinopathy that have retinal detachment, using a forceps with one hand and the slightly curved scissors to remove the proliferative tissue.
“For me, using only three good sclerotomies with a light irrigation system makes it possible to remove every type of proliferative tissue. You can avoid surgical bleeding by working fast and maintaining high-pressure during the dissection. scleral buckle is still useful in some cases with retinal detachment, but silicone oil is rarely needed,” Dr Corcóstegui said.
5
GooD RESULTSSmall-gauge vitrectomy has advantages in all levels of proliferative diabetic retinopathyby Roibeard O’hEineachain
Borja Corcóstegui – [email protected]
contact
EYEFILL® A CARING DECISION
… DEVELOPED TO MEET THE DEMANDSOF ALL SURGICAL EVENTUALITIES
EYEFILL® S.C.S U P R E M E C O H E S I V E
SUPREME COHESIVE
HIGHLY COHESIVEVISCOELASTIC
COHESIVE
THE NEW STANDARDVISCOELASTIC
EYEFILL® D.C.
D I S P E R S I V E C O H E S I V E
DISPERSIVE COHESIVE
THE VISCOADAPTIVEVISCOELASTIC
HIGH DISPERSIVE
DISPERSIVE HPMCVISCOELASTIC
CROMA GmbH • www.croma.atAEY001Aa | 0123
ad EYEFILL 1-2hoch ENG 131003v1 cho.indd 1 03.10.13 13:20
Special focus
rETINa
For me, using only three good sclerotomies with a light irrigation system makes it possible to remove every type of proliferative tissue
“
Borja Corcóstegui MD
don’t miss Eye on Technology, see page 29

EUROTIMES | Volume 19 | Issue 3
Gene therapy strategies have the potential to revolutionise management of a number of inherited retinal diseases in the
future, according to Bart P Leroy MD, PhD.Addressing delegates at the 13th
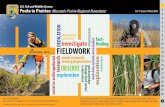
EURETiNA congress in hamburg, Germany, Dr Leroy, Ghent University hospital & Ghent University, Ghent, Belgium and The Children's hospital of Philadelphia, PA, Us, said that a number of clinical trials have started, or are scheduled to get under way in the near future, for diseases such as Leber congenital amaurosis (LCA), stargardt disease, Usher syndrome, choroideraemia and achromatopsia.
“The eye has a lot of advantages from a geneticist’s point of view. We are capable of easily accessing the eye, it is a pretty straightforward procedure to implant the replacement gene and we can look and observe what is happening in relative safety because of the immune-privileged status of the eye,” he said.
For patients with incurable retinal disease, gene therapy represents a real hope that their visual function can be preserved or even improved, and that one day the disease
progression might be slowed or even halted, said Dr Leroy.
“Clearly we want to improve vision for patients first and foremost, which means an improved quality of life for them, but we can also reduce the cost of blindness to society which is extensive,” he said.
Dr Leroy said that much of the pioneering work was initially performed in LCA patients. At present, at least 19 different genes, mutations in which lead to different forms of LCA, have been identified, including the RPE65 gene, which accounts for 5-10 per cent of all LCA cases, he said.
After successful proof-of-principle trials in the Briard dog model by Jean Bennett et al. over a decade ago, the first human gene therapy replacement trials for LCA began in 2008 when three groups, two in the Us and one in the UK, reported success in RPE65-associated LCA using the adeno-associated viral (AAV2) vector (Bainbridge et al, 2008; Cideciyan et al, 2008; Maguire et al, 2008).
“The results of these three independent trials showed that the treatment was safe and successful. There was some improvement of vision but that was not the primary outcome of the trials. There are now at least six clinical
trials for LCA with a total of between 40 and 50 patients currently, and apparently so far there have been no vector-related issues, so it seems safe to do,” he said.
Dr Leroy noted that the phase i trial of 12 patients carried out at the Children’s hospital of Philadelphia, as well as a follow-up trial of 11 of these patients, showed that the results were sustainable over a six-year follow-up period. “We see increased light sensitivity and improved pupillary responses in most of the patients, as well as improvement of the visual acuity. While we are not making these patients see normally, we are vastly improving their quality of life,” he said.
After initial treatment of the first eye, visual improvement was also noted in the untreated other eye. “We think there are potentially two or more mechanisms at work here to explain this. First, the fact that the nystagmus has decreased probably also helps the visual acuity for the untreated better eye. Cerebral plasticity in the cerebral cortex may also account for some of the improvements prior to the treatment that we saw,” he said.
Other conditions Dr Leroy said that there is a lot of excitement surrounding the trials for stargardt macular dystrophy currently under way at Casey eye institute at the Oregon health and science University in Portland, Oregon, Us, and the Centre hospitalier Nationale D’Opthalmologie des Quinze-Vingts in Paris, France.
“There are a lot more patients with
stargardt disease than LCA. Most of them appear in our clinics at their best ages for treatment, between 10 and 30 years of age, and so they are economically active and they could be seriously helped by gene replacement therapy,” he said.
The same company behind the stargardt trial, Oxford BioMedica, is also recruiting for trials of Ushstat, its gene therapy targeted for the treatment of retinitis pigmentosa associated with Usher syndrome type 1B, said Dr Leroy.
Positive news has also been emerging from the first clinical trial in humans of a gene therapy for choroideraemia, an inherited retinal degenerative disease caused by a defective Rab escort protein-1 (REP1) gene.
starting in October 2011, a team at John Radcliffe hospital in Oxford led by Prof Robert E MacLaren of Oxford University began treatment of the first of six patients using a modified AAV vector to deliver the replacement gene. “We are awaiting the first published results from the trial but all the indications are that the treatment has been safe and successful,” said Dr Leroy. These have in the meantime been published, and support a positive outlook on gene therapy in choroideraemia (www.thelancet.com Published online January 16, 2014 http://dx.doi.org/10.1016/S0140-6736(13)62117-0).
As well as the first human trial for achromatopsia, which is scheduled to probably start next year, a phase iii trial for RPE65-related LCA is also under recruitment at the Children’s hospital of Philadelphia.
Bart P Leroy – [email protected]
cont
act
GENE THERAPY Clinical trials reaching critical mass for rare retinal diseases by Dermot McGrath
6 Special focus
rETINa
Right eye of patient CH07 from the Phase 1 AAV2-RPE65 gene therapy trial, seven months after subretinal injection; arrow indicates atrophic scar area, indicating administration site
Left eye of a 34-year-old female patient with Stargardt disease, showing whitish flecks on the fundus picture (FP), which hyperautofluoresce on blue-light autofluorescence images (BAF); fluorescein angiography (FA) shows relative dark choroid consequent
upon accumulation of lipofuscin in retinal pigment epithelial cells
Cour
tesy
of B
art P
Ler
oy M
D, P
hD.

EUROTIMES | Volume 19 | Issue 3
A multimodal approach, combining spectral domain optical coherence tomography (sD-OCT) and fundus autofluorescence, can
provide very useful means of quantifying the extent and morphology of atrophic lesions in eyes with geographic atrophy, said Ramzi G sayegh MD, Medical University of Vienna, Vienna, Austria, at the 13th EURETiNA Congress in hamburg.
“Until recently imaging of geographic atrophy consisted in two dimensional en-face imaging with fundus photography and fundus autofluorescence, and OCT’s role in geographic atrophy had yet to be established. But our findings show it is now possible to reliably delineate the area of atrophic lesions with spectral domain OCT,” Dr sayegh said.
he noted that fundus autofluorescence enables an exact assessment of the atrophic lesion area and that the autofluorescence patterns have a prognostic value, in the lesions' progression. Lesions with a banded or diffuse pattern grow more rapidly than those with a focal pattern or those with no fundus autofluorescence abnormalities. however, fundus autofluorescence does not provide insights into the changes in retinal morphology.
On the other hand, research conducted at the University of Vienna shows that modern spectral domain optical coherence tomography enables the visualisation of ultrastructural alterations of retinal and
subretinal layers which is highly diagnostic and which correlates closely with vision loss, Dr sayegh said. But unlike fundus autofluorescence, sD-OCT cannot as yet distinguish any features that can predict the rapidity of the disease’s progression.
SD-OCT vs. fundus autofluorescence Dr sayegh outlined a series of studies he and his associates conducted comparing the findings obtained through sD-OCT with those obtained through fundus autofluorescence, time domain OCT and other technologies.
in the first study they compared complete sD-OCT datasets of 81eyes of 42 patients with geographic atrophy and looked at specific morphological changes in the lesion area and compared them with fundus autofluorescence images from the same eyes. Two readers of the Vienna Reading Centre graded all of the imaging obtained with the two techniques.
The researchers found that the OCT parameters which correlated most closely with FAF were choroidal signal enhancement, with a 96 per cent correlation, the area of outer plexiform layer shifting from 84 per cent, and external limiting membrane loss with a 93 per cent correlation. A follow-up of 48 eyes produced very similar results, Dr sayegh noted.
“We found a very good agreement between OCT and fundus autofluorescence measurement results at baseline and at
follow-up. however, we also saw that the area of complete RPE loss correlated to only 40 per cent of the lesion area detected by fundus autofluorescence at baseline and follow-up,” he said.
Further comparisons To determine which alterations in retinal morphology corresponded to loss of visual function, Dr sayegh and his associates conducted another study in which they combined sD-OCT imaging with microperimetry fundus images overlaid with an infrared image (MP1, Nidek). To perform their analysis they used the OCT-tool-kit, a suite of software designed by the Vienna Reading Centre that enables the delineation of the lesion area in sD-OCT volume scans and which locates the sensitivity points obtained through microperimetry in their precise relationship to the retina’s anatomy.
The study involved 43 eyes of patients with geographic atrophy. The researchers graded 1,005 sensitivity points in each eye. They found that in regions where the external limiting membrane was lost, the sensitivity was reduced by 1.3 decibels, and where both the the external limiting membrane and the retinal pigment epithelium were lost there was a complete loss of sensitivity.
“From this we concluded that grading outer retinal layers in addition to the retinal pigment epithelium is important,” Dr sayegh said.
in yet another study, involving 81 eyes of patients with geographic atrophy, the Vienna researchers compared spectral domain OCT with the Cirrus® (Carl-Zeiss Meditec) and the spectralis® (heidelberg-Engineering), to time domain OCT stratus® OCT imaging (Carl-Zeiss Meditec) and to fundus autofluorescence and fundus autofluorescence combined with infrared imaging. For external parameters they also measured visual acuity and performed
microperimetry and fixation testing (MP1, Nidek).
That study showed that visual acuity correlated significantly more closely with grading of the fovea in OCT images than with FAF imaging (p<0.0001), and that the sD-OCT performed significantly better than time domain OCT. in addition, central fixation correlated closely with foveal sparing as detected by OCT.
summarising, Dr sayegh said that the studies show that sD-OCT can precisely determine the size of geographic lesions and that the best parameters are choroidal signal enhancement, outer plexiform layer shifting and external limiting membrane loss. in addition, their research also showed that external limiting membrane loss corresponds with sensitivity reduction and that foveal sparing is best detected by sD-OCT.
“however, since we still haven’t found any OCT parameter that corresponds to the lesion growth rate, multimodal imaging in geographic atrophy with fundus autofluorescence and OCT is required,” he added.
Ramzi Sayegh – [email protected]
cont
act
BRIDGING THE GAPFundus autofluorescence and SD-oCT aid in charting geographic atrophy progressionby Roibeard O’hEineachain
7Special focus
rETINa
XXXII Congress of the ESCRS
13-17 September
14th EURETINA Congress
11-14 September
5th EuCornea Congress
12-13 September
WSPOS PaediatricSub Specialty Day
12 September
Eu C o r n e
a
European Society of Cornea andOcular Surface Disease Specialists
Eu
C o r n ea
Until recently imaging of geographic atrophy consisted in two dimensional en-face imaging with fundus photography and fundus autofluorescence, and OCT’s role in geographic atrophy had yet to be established
“
Ramzi G Sayegh MD

EUROTIMES | Volume 19 | Issue 3
in an effort to reduce the number of cases that develop endophthalmitis following intravitreal anti-VEGF injections, Peter Barry FRCs has
extended an invitation to retinal specialists across Europe to participate in the newly launched EsCRs Endophthalmitis Registry.
“The idea of the registry is that it will enable us to track any changing patterns of microbial susceptibility and antimicrobial resistance, which is just as important to retinal specialists who perform anti-VEGF injections as it is to cataract surgeons,” said Dr Barry, st Vincent’s University hospital, Dublin ireland, at the 13th EURETiNA meeting in hamburg.
Easy data entry The EsCRs Endophthalmitis Registry is based on the swedish Endophthalmitis Registry, and is operated through the EsCRs office in Dublin, ireland. By and large, the information it requires of participating retinal surgeons performing anti-VEGF injections is the same as is required of cataract surgeons.
Participating surgeons will make an anonymised entry into the registry when they first suspect that an eye may have endophthalmitis following a cataract procedure or an anti-VEGF injection. The entry will include a reference number for the patient, the name of the surgeon, the name and location of the hospital and the date of the tentative diagnosis of endophthalmitis.
“For data protection reasons we don't want the name of the patient, who is given an
arbitrary number which will help you identify which case you're sending details from,” Dr Barry explained.
Three months after entering a suspect case of endophthalmitis into the registry database, participating surgeons will receive a computer-generated form that will first inquire whether or not the case was confirmed.
in cases of confirmed endophthalmitis, additional information requested include the bacteria identified and the method used to confirm the infection, whether by Gram stain, culture, PCR or a combination of techniques. Other information requested include whether prophylactic topical and/or intracameral antibiotics were used, and if so, which agent or agents were used, and also whether the patient used antibiotic eye drops postoperatively and finally the patient’s outcome in terms of visual acuity.
Dr Barry noted that an important distinction between the swedish Endophthalmitis Registry and the EsCRs registry is that it will not determine the rate at which the complication occurs, since it will not catch every case.
instead, it will serve a purpose more similar to that of the TRUsT (Tracking bacterial Resistance in the Us Today) bacterial surveillance programme, in which an independent central laboratory performs in vitro susceptibility testing on bacterial isolates submitted from hundreds of clinical centres around the country.
“The findings of the EsCRs registry could help EURETiNA provide evidence-
based guidelines regarding the prophylaxis of endophthalmitis following anti-VEGF injections,” Dr Barry added.
Registries yield results Dr Barry noted that it was findings from the swedish Cataract Registry that first put the EsCRs Endophthalmitis study in motion. The subsequent drop in endophthalmitis following cataract surgery in centres using intracameral cefuroxime is therefore evidence of the type of result that can be achieved using a registry approach.
The EsCRs Prophylaxis of Endophthalmitis study for its part showed that in cataract patients randomised to preoperative povidone iodine alone the rate of endophthalmitis was 0.35 per cent. That compared to a rate of 0.05 per cent among patients randomised to receive intracameral injections of cefuroxime.
Critics of the study, particularly those in North America, said that the endophthalmitis rate in the control group was unduly high, making the results of the study irrelevant to their practice, Dr Barry said.
“some American colleagues actually told me that their conclusion from the EsCRs study was that European cataract patients should travel to the United states because Europe was dirty and that if they travelled to America all they would need is topical antibiotic drops to avoid endophthalmitis. however, i would argue that this figure of 0.35 per cent is very close to the reality on both sides of the Atlantic,” he added.
That conclusion is supported by a recent study from California, he noted. The study’s authors adopted the use of intracameral antibiotics in 2007 when they found that their previous prophylactic regimen, povidone iodine and postoperative antibiotic eye drops, was leaving them with an endophthalmitis rate of 0.31 per cent. When they switched to intracameral antibiotics the rate dropped to 0.014 per cent (Shorstein et al J Cataract Refract Surg 2013;39:8-14).
Furthermore, the recent introduction of a new single-dose preparation of cefuroxime (Aprokam®, Thea) for intracameral use may remove an additional source of resistance to using intracameral cefuroxime – namely the potential medicolegal consequences of using a product in an off-label way. it is now approved in 14 European countries and more will be added this year.
“The EsCRs study has achieved most of its objectives, in that it has proved the safety and efficacy of intracameral cefuroxime in the prevention of endophthalmitis after cataract surgery. That, in turn has encouraged industry to provide a standard preparation which we now have, and we’re simply waiting for worldwide acceptance,” Dr Barry concluded.
Peter Barry – [email protected]
cont
act
ENDoPHTHALMITISNew registry aims to reduce endophthalmitis after cataract surgery and anti-VEGF injectionsby Roibeard O’hEineachain
8 Special focus
rETINa
EUROTIMESESC
RS ™
Türkiye
TURKISH LANGUAGE EDITIONNOW ONLINE
Visit: www.eurotimesturkey.org
The idea of the registry is that it will enable us to track any changing patterns of microbial susceptibility and antimicrobial resistance...
“
Peter Barry FRCS

cont
act
Results of a prospective comparative study evaluating macular thickness changes after uneventful cataract surgery indicate that further
study is warranted to establish the safety of intracameral lidocaine for surgical anaesthesia.
The research was conducted by ophthalmologists from Balikesir University Medical Centre, Balikesir, Turkey, and presented by sitki samet Ermis MD, at the XXXi EsCRs Congress in Amsterdam.
The study randomised 78 eyes of 59 consecutive patients with senile cataract to receive anaesthesia using topical lidocaine alone or supplemented at the beginning of the
procedure with an intracameral injection of 0.5 cc preservative-free lidocaine one per cent.
All patients underwent spectral domain optical coherence tomography (sD-OCT) imaging preoperatively and at one week, one month and three months postoperatively. Macular thickness values were determined for each of nine sectors defined by the Early Treatment Diabetic Retinopathy study, and the data were used to calculate changes from baseline in the central fovea and the inner and outer macular zones.
Mean thickness for each of the three areas did not differ significantly between the two study groups preoperatively and
increased in both groups at all follow-up visits. Comparisons between groups showed no significant difference at any time point for the changes in the central fovea and outer macular zone. however, the increase in inner macular zone thickness was significantly greater in the supplementary intracameral lidocaine group compared with eyes receiving topical lidocaine at both the one week (3.21 vs. 2.83 microns; p=0.04) and one month (7.94 vs. 6.35; p=0.03) assessments.
Study limitation “The main limitation of this study is its relatively small sample size, which is due to the elimination of a considerable number of eyes with lens opacities preventing reliable preoperative sD-OCT measurements. however, the results are fortified by its prospective, randomised, double-masked design,” said Dr Ermis.
“We believe further in vivo human studies with a larger sample size are needed in order to reach a definitive conclusion about the fate of ganglion cells after cataract surgery under intracameral lidocaine anaesthesia.”
Dr Ermis noted that cystoid macular
oedema remains one of the most common causes of unfavourable visual outcomes after uneventful cataract surgery. While its pathogenesis is thought to involve breakdown of the blood-retina barrier leading to fluid accumulation in the outer retinal layers, an inflammatory process in the neurosensory retina, including the ganglion cell layer, may also play a role.
“The architecture of the perifoveal macular area includes four to six layers of ganglion cells. These perifoveal ganglion cells may be primarily affected by a surgically-induced inflammatory process, but also by the posterior accumulation of lidocaine after intracameral administration. The latter phenomenon could explain the greater increase in perifoveal macular thickness in the intracameral lidocaine group,” he said.
he added that findings from previous experimental and human studies show that intracameral lidocaine is potentially toxic to the retina if it diffuses to the posterior segment. There have been reports of patients experiencing transient vision loss after receiving intracameral lidocaine.
9
ANAESTHESIAIntracameral lidocaine and macular changesby Cheryl Guttman Krader
Sitki Samet Ermis – [email protected]
EC201348 Copyright Rayner Intraocular Lenses Limited. rayner.com
• Minimal touch• More Convenience• 2.2 mini incision• Aberration Neutral Optic
Streamline and optimise your workflow with the C-flex® Advance Aspheric
C-flex® Advance AsphericMini Incision Preloaded IOL Injection System
C
M
Y
CM
MY
CY
CMY
K
October CRSTE ADVANCE AD 18 SEPT FINAL.pdf 1 18/09/2013 10:25:23
EUROTIMES | Volume 19 | Issue 3
Update
caTaracT & rEfracTIvE

EUROTIMES | Volume 19 | Issue 3
A number of new surgical and pharmacological approaches currently under investigation show promise in reducing the
incidence of posterior capsule opacification (PCO) after cataract surgery, according to research presented at the XXXi Congress of the EsCRs in Amsterdam.
PCO remains one of the most common complications of cataract surgery, despite advances in surgical techniques, intraocular lens materials and designs over recent years, according to Guy Kleinmann MD.
“PCO is still a problem after lens implantation and particularly in the case of so-called premium iOLs. however, we believe that our approach, which is to open the capsular bag instead of shrinking it, could reduce the rate even further,” he said.
Dr Kleinmann, Kaplan Medical Centre, Rehovat, israel, said that initial studies in rabbits and cadaver eyes have yielded encouraging results for the open bag device (CleaRing, hanita Lenses), which is implanted in the capsular bag prior to iOL implantation.
“The ring, which is made of either hydrophilic or hydrophobic material, is
placed in the capsular bag before the iOL implantation. The concept is that the ring acts as a support for the anterior capsule and creates a barrier to lens epithelial migration across the iOL optic. implanting such a device also means that the surgeon is free to implant whatever lens they desire,” he said. The ring features several unique characteristics: 1. A special square-edge design; 2. A groove for iOL haptics fixation; 3. “Windows” which allow aqueous flow to the equator LECs; and 4. A “roof” for anterior capsule lifting and support.
in the phase i rabbit trial, the ring was tested in conjunction with two iOLs: the Tecnis (AMO) hydrophobic iOL and the seeLens AF (hanita Lenses) hydrophilic iOL. Both iOLs have a total diameter of 13.0mm, an optic diameter of 6.0mm and incorporate a 360 square-edge design.
in the control group, six Tecnis and six seeLens iOLs were implanted in rabbit eyes with no open capsule ring. in the treatment groups, a hydrophilic and hydrophobic version of the ring was implanted in addition to the iOLs.
Dr Kleinmann said that implantation of the hydrophilic ring was found to be easier
and could be compared to standard iOL implantation.
“The insertion of iOL haptics into the groove of the ring device was not automatic and required some manipulation to put it into place. some ovalization of the capsular bag was observed, perhaps due to large diameter of the ring. The capsule remained open in the eyes with the ring implanted,” he said.
Overall the study showed encouraging PCO prevention results for both hydrophilic and hydrophobic ring materials, with no significant difference found between hydrophilic and hydrophobic iOLs.
“Our results suggested primary PCO prevention due to inhibition of soemmerring’s ring formation, indicating suppression of cell proliferation and not only a mechanical blockage. We observed about 75 per cent less PCO in the treatment eyes compared to control. in Miyake-Apple view of the capsular bag, we also saw a significant reduction of around 80 per cent in soemmerring’s ring development in groups with the CleaRing compared to control,” he said.
The cadaver study, which used a smaller ring diameter of 9.5mm, was found to fit all capsular bag sizes of eyes tested with no ovalization or deformation, noted Dr Kleinmann.
Dr Kleinmann suggests that the device’s special design of having windows in its side walls also plays an important role, as suggested by Leishman et al (Leishman L, Werner L, Bodnar Z et al. Prevention of capsular bag opacification with a modified hydrophilic acrylic disk shaped intraocular lens. J Cataract Refract Surg. 2012;38(9):1664–1670). These windows allow aqueous humor flow to the equatorial LEC, thereby maintaining nutrition and oxygen supply to those cells.
it is possible that the primary trigger for soemmerring’s ring formation and the subsequent formation of PCO is a consequence of chronic ischemia and lack of nutrition of the equatorial LECs. This hypothesis is supported by reports describing the prevention of LEC migration by transforming growth factor β2 (TGFβ2), which is normally found in the aqueous humor (Saika S, Okada Y, Miyamoto T, Ohnishi Y, Ooshima A, McAvoy JW. Smad translocation and growth suppression in lens epithelial cells by endogenous TGF beta2 during wound repair. Exp Eye Res. 2001;72(6):679-686. Kurosaka D, Nagamoto T. Inhibitory effect of TGF-beta 2 in human aqueous humor on bovine lens epithelial cell proliferation. Invest Ophthalmol Vis Sci. 1994;35(9):3408-3412.)
in a separate presentation, Julie Eldred PhD presented another prototype open capsular bag device, the Zephyr iOL (Anew Optics inc.), which has shown promising results in PCO prevention in both rabbit and human cadaver studies.
“We wanted to elucidate the effect of the Zephyr open bag iOL in comparison to the Acrysof (Alcon) of the lens cell progression in the open and closed bags,” she said.
Dr Eldred noted that Zephyr iOL is a hydrophilic acrylic iOL designed to keep the anterior and posterior capsule separated with the haptics configured so as to allow the natural curvature of the capsular bag to be retained. The iOL also incorporates five fenestrations between the haptic and the optic to allow fluid and nutrient flow throughout the capsular bag system.
in Dr Eldred’s study, cataract operations were performed on match-paired human donor eyes in which one eye was implanted with the Acrysof iOL and the other with the Zephyr lens. The capsular bag was then removed from the globe and suspended in culture for 28 days using either serum-free media or media supplemented with two per cent human serum and TGF beta 2.
Overall, the open bag iOL showed a reduced rate of cell coverage of the posterior capsule compared to the single piece iOL in both culture conditions, said Dr Eldred. This difference was more pronounced in the serum supplemented capsular bags.
“in our study, the Zephyr open bag iOL performs consistently better than the Acrysof iOL regardless of culture condition. We believe that the benefits observed with the Zephyr iOL result from a barrier function and a reduction in growth factor levels available within the capsular bag. Furthermore, the presence of serum enhanced the shrink-wrapping of the capsular bag around the iOL which we hypothesise creates an enhanced barrier to cell growth,” she concluded.
Guy Kleinmann – [email protected] Eldred – [email protected]
cont
acts
PCo FoRMATIoNGood study results for device implanted in the capsular bag prior to IoL implantationby Dermot McGrath
10 Update
caTaracT & rEfracTIvE
Reduced anterior lens epithelial cell growth onto the posterior capsule in human match-paired capsular bags implanted with Anew Zephyr™ compared to Acrysof IOLs maintained for 28 days in two per cent Human serum + TGFβ2 (10ng/ml)
Cour
tesy
of J
ulie
Eldr
ed P
hD
Design of the CleaRing device
Cour
tesy
of G
uy K
lein
man
n M
D

Observed changes in wavefront aberrations between near, intermediate and far vision in patients implanted with the
WiOL-CF accommodative iOL (Medicem, Czech Republic) offer objective evidence of accommodation and insight about its mechanisms, said ioannis G Pallikaris MD, PhD, at the XXXi EsCRs Congress in Amsterdam.
“Obtaining objective proof of accommodation with ‘accommodating’ iOLs is a major challenge. We used quantitative analysis of optical aberrations to help us understand what is happening with the WiOL-CF iOL during the accommodation process,” said Dr Pallikaris, professor of ophthalmology, institute of Vision and Optics, University of Crete Medical school, heraklion, Greece.
“Our findings show that the WiOL-CF has at least 0.8 D of real accommodation that is driven by a change in defocus. in addition, there are also changes in higher order aberrations that result in an increase in depth of focus. Combined, this information provides at least partial justification for the satisfactory near vision achieved in patients implanted with the WiOL-CF.”
Described as a “bioanalogic lens”, the WiOL-CF iOL is designed to mimic key properties of the natural crystalline lens. it has a large diameter (~9mm) polyfocal optic and is made of a flexible hydrogel material so that it is able to change shape in response to ciliary muscle contraction and relaxation, leading to changes in refractive power.
Wavefront aberrations To evaluate accommodation with the WiOL-CF iOL, changes in wavefront aberrations were measured at three years postoperatively in 15 patients who had undergone uneventful cataract surgery with binocular implantation of the WiOL-CF iOL. The patients had a mean age of 65 years with a range between 53 and 83 years.
Zernike coefficients from second to fourth order were obtained using a ray-tracing unit (iTrace, Tracey Technologies) that has a view-through device allowing wavefront capture at different distances.
The measurements were performed at the natural pupil diameter under
photopic conditions with patients looking at an illuminated target at three different distances: far (4m), intermediate (60cm) and near (33cm). All measurements were performed twice with the same pupil size and centred first on the pupil and then at the visual axis. Differences maps were generated from measurements obtained at far and intermediate and from far and near.
Myopic shift The results for defocus showed there was a myopic shift in all patients with the change from the far to intermediate distance stimulus (mean -1.02 D, range -0.24 D to -2.15 D) and from the far to near distance stimulus (mean -0.87 D, range -0.4 to -1.58 D).
The shifts from far to intermediate and from far to near were also associated with changes in third and fourth higher order aberrations whether the measurements were performed with centration on the pupil or the visual axis, although the changes were more pronounced with pupil centration. For the latter measurements, the mean (±standard deviation) change in vertical coma was 0.04 ±0.07 microns with the shift from far to near and 0.08±0.09 microns. The shift from far to intermediate; spherical aberration showed negative shifts with changes of -0.05±0.03 microns from far to near and -0.03±0.03 microns from far to intermediate.
11
ACCoMMoDATIoNWavefront analyses support visual performance of bioanalogic IoLby Cheryl Guttman Krader
Ioannis Pallikaris – [email protected]
contact
C
M
Y
CM
MY
CY
CMY
K
add_march2014.pdf 1 2/10/14 11:00 AM
EUROTIMES | Volume 19 | Issue 3
Update
caTaracT & rEfracTIvE
Our findings show that the WIOL-CF has at least 0.8 D of real accommodation that is driven by a change in defocus
“
Ioannis G Pallikaris MD, PhD

EUROTIMES | Volume 19 | Issue 3
A novel treatment paradigm that combines corneal parameters with refractive measurements can be used to deliver safe and effective excimer laser treatments in patients with mild or forme
fruste keratoconus, according to Noel Alpins FRANZCO, FRCOphth, FACs.
“Our long-term data shows that patients with forme fruste and mild keratoconus can be safely and effectively treated with photoastigmatic refractive keratectomy (PARK),” Dr Alpins told delegates attending the XXXi EsCRs Congress in Amsterdam. “Eyes treated using vector planning1 were shown to have a stable refraction and corneal topography up to 10 years after surgery, with no incidence of progressing ectasia or increase in corneal irregularity,” he said.
Dr Alpins noted that treating forme fruste and mild keratoconic patients using refraction parameters alone would generate an excess amount of corneal astigmatism on the cornea, resulting in potentially adverse effects on postoperative visual outcomes. “in keratoconus, this is evidenced by the greater than average calculated ocular residual astigmatism (ORA) in any group of eyes having treatment for astigmatism with myopia. The ORA is defined as the vectorial difference between the corneal astigmatism and the refractive cylinder at the corneal plane, and is expressed in dioptres. On the other hand, treating by corneal data alone will attempt to make the cornea more spherical but will leave excess astigmatism measurable in the manifest refraction postoperatively, which is likely to be unacceptable to the patient,” he said.
Combining both approaches gives these patients the best of both worlds, said Dr Alpins.
“Using vector planning the refractive cylinder outcome is not compromised as one might perhaps expect with a technique that also takes account of corneal parameters. Using this approach, the corneal astigmatism remaining is less than with using refractive parameters alone, essentially because we are treating somewhere closer to the corneal steep meridian and magnitude rather than treating by refraction alone. The end result is less astigmatism on the cornea and a better quality of vision,” he said.
Advances in diagnostic and imaging technologies over the last decade have helped greatly in the identification of potentially suspect keratoconus corneas, said Dr Alpins.
“There has been a real evolution in the terminology of keratoconus since George Waring iii first used the term “suspect keratoconus” in 1993. That designation was based mainly on observation whereas today there are many other qualitative and quantitative keratoconic indices to help us identify such corneas. The sensitivity of these new tools is now of such a high calibre that it has sometimes flagged a cornea as potentially keratoconic that we initially did not suspect ourselves on first appearance,” he said.
The results obtained in most of the earlier studies of excimer laser treatment for mild and forme fruste keratoconus patients were not particularly impressive, said Dr Alpins. “however, we need to bear in mind that the treatments were usually based only on refraction or on corneal parameters, not a combination of the two. The outcomes in these studies show only a partial decrease in refractive astigmatism and there was progression of the keratoconus in some patients. Furthermore, most of the early studies did not even report the postoperative corneal astigmatism parameters,” he said.
The data presented by Dr Alpins included 45 eyes of patients with mild or forme fruste keratoconus.
“We adhered to very strict criteria and only treated myopic astigmatism patients, over 25 years of age with non-progressive keratoconus. All patients had to have a stable refractive and corneal status for two years. We excluded patients with mean K-readings of 50.00 D or greater, best-corrected visual acuity less than 20/40, those with signs of apical thinning, visible ectasia or scarring on slit lamp examination, and those with residual stromal bed less than 300 μm, assuming an epithelial thickness of 60 μm,” he said.
Patients were treated with the Visx star s1 excimer laser (eight eyes until 1997) or s2 excimer laser (37 eyes from 1997 forward), said Dr Alpins. Unlike earlier studies, the technique used vector planning to incorporate both corneal topographical data and refractive astigmatism data in the treatment plan.
Dr Alpins explained that the simulated keratometry value derived from the topography was incorporated into the treatment plan by calculating the ORA.
in the study group, all treatments were optimised, directing only part of the neutralisation to the cornea and a theoretical part to the refraction, targeting 0.75 D or less remaining on the cornea and 0.50 D or less in the refraction. in cases in which the ORA was more than 1.50 D, the proportion was selected as 50 per cent in the theoretic manifest refraction and 50 per cent on the cornea, hence targeting greater amounts of remaining astigmatism than with a lower ORA.
Refractive results overall were very good, said Dr Alpins, with uncorrected visual acuity of 20/20 or better in 56 per cent of eyes and 20/40 or better in all eyes. seven eyes lost best-corrected visual acuity compared to a gain of BCVA in 16 eyes. Moreover the refraction remained stable over time with no evidence of progression of the keratoconus.
1 Alpins NA. New method of targeting vectors to treat astigmatism. J Cataract Refract Surg 1997; 23(1):65- 75.
Noel Alpins – [email protected]
cont
act
KERAToCoNUS AND LASERPositive long-term outcomes with excimer laser treatments in keratoconic eyesby Dermot McGrath
12 Update
caTaracT & rEfracTIvE
Cour
tesy
of N
oel A
lpin
s FR
ANZC
O, F
RCOp
hth,
FAC
S

The EsCs-funded PREvention of Macular EDema after cataract surgery (PREMED) study should help to provide evidence-based
recommendations for clinical guidelines to prevent the occurrence of cystoid macular oedema (CME) after cataract surgery in patients with and without diabetes mellitus (DM). The PREMED study is an initiative of the University Eye Clinic Maastricht UMC, the Netherlands, under the supervision of Prof Rudy Nuijts MD, PhD.
“To our knowledge, only few well-designed randomised studies have compared non-steroidal anti-inflammatory drugs (NsAiDs) and corticosteroids as a solitary anti-inflammatory treatment in the prevention of CME after cataract surgery. The incidence of CME varies in the scientific literature between four per cent and 20 per cent in healthy subjects after cataract surgery. however, the majority of these patients have no reduction of visual acuity. Therefore, the incidence of clinically significant macular oedema (CsME) is estimated between zero and 5.8 per cent,” Laura h P Wielders MD told delegates at the XXXi Congress of the EsCRs in Amsterdam.
The enhanced risk of CME after cataract surgery in diabetic patients has also been factored into the study design, said Dr Wielders.
“About 16 per cent of all patients undergoing cataract surgery are diabetics and 50 per cent of postoperative CME patients also have DM. it is known that patients with DM have a higher risk of developing CME after cataract surgery: in up to 56 per cent in previous studies,” she said.
Current preventive measures to reduce the potential risk of CME after cataract surgery vary widely from centre to centre, noted Dr Wielders.
“There is a lot of variety in clinical practice. Of 12 centres currently participating in the PREMED study, most use an NsAiD and a corticosteroid to prevent inflammation and CME after cataract surgery. however, some centres use no NsAiDs and others do not use corticosteroids at all. it should also be borne in mind that none of these centres has a separate protocol for patients with DM,” she said.
When enrolment is complete, the PREMED study will include 1,050 non-diabetic and 300 diabetic patients.
All patients undergoing routine phacoemulsification will be included in the study, except those meeting exclusion criteria such as previous ocular surgery, history of glaucoma or increased iOP, retinal vein occlusion, uveitis or macular pathology that might influence visual acuity. The final results of the study are expected in the 2015-2016 time frame.
Further treatment Only one eye per patient will be included in the study. The choice of antibiotics used will be left to the participating centre, although the chief investigators recommend intracameral cefuroxime as per the EsCRs Endophthalmitis study.
Further treatment will differ for diabetic and non-diabetic patients, noted Dr Wielders. Non-diabetic patients will be randomised to receive topical Bromfenac, topical Dexamethasone or both of these drugs, while diabetic patients, with a higher risk of CME, will receive both. Diabetic patients will be randomised to receive no additional drugs, a subconjunctival injection of Triamcinolone Acetonide, an intravitreal injection of Bevacizumab or both.
The primary endpoint of the study is the change in central subfield mean macular thickness (CsMT) as compared to baseline at six weeks postoperatively. The secondary endpoint is the occurrence of CsME within 12 weeks postoperatively.
in case of CsME, treatment will be initiated and its effect will be part of the evaluation at 12 weeks. Medical data of all patients who develop CsME during the study will be checked at the end of the study and at least six months after surgery.
13
CME MANAGEMENT The ESCRS PREMED study aims to shed light on CME management after surgeryby Dermot McGrath
Laura H P Wielders – [email protected]
contactwww.oculus.de
The best choice for Cataract and Refractive surgeons
OCULUS Pentacam® HR
OCULUS is prepared for your daily tasks. The Pentacam® HR – The Gold Standard in Anterior Segment Tomography – offers you just the best hardware and most efficient software. Customize the clever software packages to your personal needs and use them in your local network with the new OCULUS Floating License Key.
Plea
se n
ote:
The
ava
ilabi
lity
of t
he p
rodu
cts
and
feat
ures
may
diff
er in
you
r co
untr
y.
Spec
ifica
tions
and
des
ign
are
subj
ect
to c
hang
e. P
leas
e co
ntac
t yo
ur lo
cal d
istr
ibut
or f
or d
etai
ls.
EUROTIMES | Volume 19 | Issue 3
Update
caTaracT & rEfracTIvE
The enhanced risk of CME after cataract surgery in diabetic patients has also been factored into the study design
“
Laura H P Wielders MD

14
EUROTIMES | Volume 19 | Issue 3
Wavefront-guided LAsiK using the iDesign (Abbott Medical Optics inc.) system can produce highly
predictable refractive outcomes in eyes with myopia and myopic astigmatism, with no loss of corrected visual acuity and no loss in quality of vision, said sarah Moussa MD, University Eye Clinic, Paracelsus Medical University, salzburg, Austria.
“LAsiK treatments using the new iDesign system for treatment planning is effective, safe and reliable, providing excellent refractive outcomes and good results in terms of postoperative higher-order aberrations,” she said at the XXXi Congress of the EsCRs.
Dr Moussa presented the results achieved at two months’ follow-up in a consecutive series of 100 eyes of 56 patients who underwent wavefront-guided LAsiK using the iDesign system. The patients had a mean age of 35 years. Their preoperative manifest refraction spherical equivalent had a mean value of -3.8 D and ranged from -7.88 D to -038 D. Their preoperative
cylinder had a mean value of -0.99 D and ranged from -4.75 D to 0.0 D.
A single surgeon, Josef Ruckhofer MD, performed all the LAsiK procedures. in every case, he used the iDesign system for planning the treatment, the iFs™ femtosecond laser (AMO) to create corneal flaps, and the sTAR s4iR excimer laser system, with iris registration and active 3-D eye tracking, for performing the ablations.
The new iDesign system provides five measurements within a single capture sequence, including autorefraction, wavefront aberrometry, corneal topography, keratometry and pupillometry, Dr Ruckhofer noted in an interview with EuroTimes.
“The iDesign system offers several key advantages, the higher resolution of the hartmann-shack sensor provides more accurate information to the laser for treatment, iDesign can capture 600 to over 1200 data points, depending on pupil size, compared to the maximum of 240 data points with the Wavescan system. The addition of a full gradient topography in the same capture sequence allows us to analyse
the wavefront map and the topography at the same time. That in turn enables us to detect if the aberrations are coming only from the cornea or more from the lens,” he added.
At a follow-up of two months, uncorrected visual acuity was 1.0 or better in 99 per cent of eyes, 1.25 or better in 73 per cent of eyes and 1.6 or better in 32 per cent of eyes. in addition, no eyes lost lines of corrected visual acuity, 49 per cent gained one line and five eyes gained two lines.
Furthermore, all eyes were within 0.5 D of attempted correction and 96 per cent were within 0.25 D. in all, 21 per cent of eyes were slightly under-corrected and three per cent were slightly over-corrected. Furthermore, residual cylinder was less than 0.25 D in 90 eyes and ranged from 0.26 to 0.5 D in the remaining 10 eyes.
“iDesign is easy to use, providing refractive surgeons with a simple and quick transition from the Wavescan system. in the treatment of astigmatism, the use of the higher-resolution system resulted in fewer outliers, less chance of an axial shift, and a tighter correlation coefficient
compared with standard aberrometry. since these are the first eyes we’ve treated with this new technology in our centre, the results will probably improve after time when nomograms are refined,” Dr Ruckhofer said.
Sarah Moussa – [email protected] Ruckhofer – [email protected]
WAVEFRoNT LASIKVery promising preliminary results with LASIK using new planning system by Roibeard O’hEineachain
LASIK treatments using the new iDesign System for treatment planning is effective, safe and reliable, providing excellent refractive outcomes and good results...
“
Sarah Moussa MD
iDesign is easy to use, providing refractive surgeons with a simple and quick transition from the Wavescan System
“
Josef Ruckhofer MD
femto_hirdetes_245x100mm_20140203_PRESS.indd 1 2014.02.03. 13:28:42
Update
caTaracT & rEfracTIvE cont
acts

EUROTIMESESC
RS ™
* Average net circulation for the 10 issues circulated between 1 January 2013 and 31 December 2013. See www.abc.org.uk
** Results � om the EuroTimes Readership Study 2011
customers in over150 countries with your ad
Advertise with EUROTIMESESC
RS ™
Europe’s number one with the highest audited circulationfor any ophthalmic news magazine in Europe
59 per cent of our readers surveyed in an independent research survey have decision-making power when it comes to the purchase of surgical/medical equipment or supplies. A further 20 per cent are usually consulted before a � nal decision is made**
40,878REACH
*

EUROTIMES | Volume 19 | Issue 3
The risk of posterior capsule (PC) rupture during irrigation and aspiration (i/A) is decreased with the use of a silicone tip instrument, a new analysis indicates.
The study was conducted by ophthalmologists at the MidYorkshire hospitals Nhs Trust, UK, where in september 2011, the department switched from using a metal tip i/A instrument to a silicone tip device (CapsuleGuard, Bausch + Lomb storz). it was reported by Atul Varma FRCOphth, Ms, consultant ophthalmologist, at the XXXi EsCRs Congress in Amsterdam.
information on intraoperative complications was extracted from patient electronic records for all procedures performed during a four-year period beginning two years prior to the introduction of the silicone tip i/A instrument and ending two years after the change. All procedures were performed using either the Millennium or stellaris phacoemulsification units (Bausch + Lomb). About 10 per cent of cases during both periods were performed by trainees.
Complications occurred in 159 (3.4 per cent) of 4,754 eyes operated on during the first two years of the study period using the metal tip i/A instrument and in 192 (4.1 per cent) of 4,681 eyes operated on using the silicone instrument during the last two years.
PC rupture (with or without vitreous loss) or zonular dialysis occurred in 96 cases performed with the metal tip i/A instrument (2.0 per cent) and in 87 cases (1.9 per cent) of the silicone tip i/A series.
While the vast majority of the capsule rupture/zonular dialysis complications in both study groups occurred during phacoemulsification, 16 (16.6 per cent) of the 96 events in the metal tip i/A group but only one (1.14 per cent) of the 87 cases in the silicone i/A tip series occurred during i/A, reported Dr Varma.
“The UK Cataract National Database Electronic Patient Record systems audit of 55,567 cataract operations performed by 406 surgeons from 12 Nhs Trusts found posterior capsule rupture and/or vitreous loss occurred in 1.92 per cent of eyes. i/A was one of the steps where a number of the posterior capsule ruptures occurred, and the rate of posterior capsule rupture for cases performed by trainees was up to 16 per cent,” said Dr Varma.
“Our study found a dramatic reduction in the rate of this complication during i/A after switching to the silicone tip device, and our findings are consistent with data reported by
other investigators. similar results as ours were also reported by Blomquist and Plienneke in 2005 published in JCRS and also had similar reduction in PC rupture rates. Therefore, we believe it should be the i/A handle of choice, especially when training young ophthalmologists.”
Dr Varma also presented a video to demonstrate the safety of i/A, cortex removal and capsule polishing using the silicone tip i/A handpiece.
“The only precaution is that surgeons must take care in correctly aligning the silicone tip so that no part of the straight metal portion of the handpiece is visible in the curved region of the silicone tip,” he said.
Atul Varma – [email protected]
cont
act
CATARACT SURGERY SAFETYSilicone tip I/A handpiece reduces complicationsby Cheryl Guttman Krader
16 Update
caTaracT & rEfracTIvE
Posterior capsule caught by I/A tip
No damage to posterior capsule after being released from I/A tip
Safe to do I/A behind IOL
I/A was one of the steps where a number of the posterior capsule ruptures occurred, and the rate of posterior capsule rupture for cases performed by trainees was up to 16 per cent
“
Atul Varma FRCOphth, MS
don’t miss Outlook on Industry, see page 37
Information on intraoperative complications was extracted from patient electronic records for all procedures performed during a four-year period beginning two years prior to the introduction of the silicone tip I/A instrument and ending two years after the change
Cour
tesy
of A
tul V
arm
a FR
COph
th, M
S

A dual topical medication regimen including an NsAiD started preoperatively and continued after surgery with
a corticosteroid is better than using the corticosteroid alone suggest the results of a recent randomised, double-masked, placebo-controlled trial.
The study was undertaken by cataract surgeons at sahlgrenska University hospital, Mölndal, sweden and st Erik’s Eye hospital, stockholm, sweden, and was presented by Anna Zaczek MD, PhD, at the XXXi Congress of the EsCRs in Amsterdam. it included 152 eyes of 152 patients selected for having uncomplicated cataract surgery and no other ocular disease.
All patients were treated postoperatively with dexamethasone 0.1 per cent suspension three times daily for three weeks, but they were randomised to receive nepafenac 0.1 per cent ophthalmic suspension (Nevanac, Alcon) or artificial tears three times daily, starting two days before surgery and continued for three weeks postoperatively.
"Postoperative BCVA was excellent in both treatment groups with no statistically significant differences found between groups at three and six weeks after surgery," Dr Zaczek said.
“Combination treatment had benefits for reducing postoperative ocular pain and discomfort, macular swelling and anterior chamber inflammation. These results may be considered to offer one step forward to finding the optimal medication regimen for cataract surgery,” she added.
Laser flare higher anterior chamber inflammation in the control eyes was observed by laser flare meter readings on the first postoperative day. Macular swelling was measured by OCT and the results showed a significantly greater increase in total macular volume at both three and six weeks in the control eyes versus those receiving combination treatment.
Changes in macular thickness from baseline to six weeks at each of nine measured areas were also analysed to determine the proportion of eyes with a thickness increase > 10 microns. This level of swelling in the central macula occurred at a significantly lower rate in the combination group compared with controls (40 per cent vs. 60 per cent) at six weeks. There were also
statistically significant differences favouring the combination group at each of the other eight sites, with the difference in rates consistently ranging between 20 per cent and 24 per cent.
“These macular changes were subclinical overall as mean BCVA was better than 20/20 in both groups at three and six weeks. however, at three weeks, there was one case of clinically significant CME and one case of subclinical CME diagnosed by OCT, both in the control group,” Dr Zaczek said.
More combination-treated patients compared with controls reported being pain-free during surgery, although the difference was not statistically significant. however, there was a statistically significant difference favouring the combination group over the controls in the proportion of patients pain-free on postoperative day one (59 per cent vs. 22 per cent) (see figure above) as well as in the proportion free of ocular discomfort at day one (80 per cent vs. 55 per cent) and three weeks (95 per cent vs. 83 per cent).
At three weeks, eyes in the combination group were more likely than the controls to have mild to moderate punctate corneal epithelial defects (27 per cent vs. 10 per cent). No eye had severe epithelial defects.
17
A STEP FoRWARDCombination regimen outperforms steroid aloneby Cheryl Guttman Krader
Anna Zaczek – [email protected]
contact
EUROTIMES | Volume 19 | Issue 3
Update
caTaracT & rEfracTIvE
Percentage of pain-free patients during the surgical procedure and one day after operation in both study groups. *P < .05
statistically significant difference, Fisher’s Exact test
Cour
tesy
of A
nna
Zacz
ek M
D, P
hD

18
EUROTIMES | Volume 19 | Issue 3
surgeons can employ a number of surgical techniques to avoid astigmatism post-keratoplasty, with the use of femtosecond laser having
many benefits in particular, the XXXVii UKisCRs Congress in Manchester heard.
sheraz Daya FRCs(Ed), FRCOphth noted that with post-keratoplasty ametropia the refractive error is primarily due to astigmatism and spherical error, saying surgeons need to consider how they can perform better corneal transplant procedures.
he quoted data showing that penetrating keratoplasty (PK) operations are decreasing, at least in Europe, and lamellar keratoplasty is increasing, particularly deep anterior lamellar keratoplasty (DALK) and endothelial keratoplasty.
Dr Daya advised if performing cataract surgery in conjunction with Descemet's stripping automated endothelial keratoplasty (DsAEK) the surgeon should aim for -1.25 D. The amount of induced hyperopia is dependent on the DsAEK thickness and cannot be precise, he noted, however it is always better to be left slightly myopic than hyperopic.
he acknowledged that the principles of PK and DALK are similar – the goal being to create a perfectly circular opening in the cornea; ie, suture a circular cornea into a circular host, but that can be quite challenging no matter what device is used. Dr Daya recommended using a shott speculum, emphasising that centration and alignment are key. Careful tailoring of the suturing will also help to minimise postoperative astigmatism.
he also advised making sure the eye is horizontal to get optimum centration and to avoid ovalisation.
“if you are off centre with your graft, you are going to have some astigmatism and you can also have higher order aberrations,” Dr Daya remarked. The axis should be marked out and confirmed with calipers before surgery.
The optimum trephine size is 8.0mm, according to Dr Daya. if the graft size is too small, the sutures will interfere with the visual axis and cause astigmatism and if too large there is the risk of rejection and iris incarceration, narrow angle and glaucoma.
“The goals with trephination are a round, vertical cut, controlled anterior chamber entry, and a bevelled edge fashioned with curved corneal scissors,” he explained.
in relation to suturing, Dr Daya confirmed the second cardinal suture is the most important suture affecting postoperative astigmatism; with symmetrical alignment key to ensuring a good closure and minimising astigmatism risk.
“i’m also in favour of ledges as with four cardinal stitches and still have a self-sealing incision and a formed chamber, there is no need for tight sutures, and a formed anterior chamber protects the endothelium,” he told the congress.
Dr Daya spoke favourably about the emerging use of femtosecond laser in corneal grafting, citing positive data on Femtosecond laser DALK. The procedure allows more precise incisions, creating a mechanically stronger wound, good apposition anteriorly, and allows rapid wound and visual healing, and good patient acceptability. it is also easier to deal with potential ametropia, he added.
summarising, Dr Daya said surgeons must adhere to good corneal grafting principles to avoid ametropia and the cycle of requiring several procedures for transplant patients.
contact Sheraz Daya – [email protected]
AVoID AMETRoPIAFemtosecond laser helpful in avoiding post-keratoplasty astigmatismby Priscilla Lynch
www.euretina.org
11-14 September 2014LONDON14th EURETINA Congress
Update
caTaracT & rEfracTIvE
If you are off centre with your graft, you are going to have some astigmatism and you can also have higher order aberrations
“
Sheraz Daya FRCS(Ed), FRCOphth
Cour
tesy
of S
hera
z Day
a FR
CS(E
d), F
RCOp
hth
Nine months following a modified mushroom femtosecond laser DALK. Notice two circular areas of graft host interface

EUROTIMES | Volume 19 | Issue 3
Monovision with monofocal iOLs offers a viable modality for presbyopia correction in pseudophakic patients.
however, what constitutes the desired refractions for pseudophakic monovision is a matter of controversy.
According to Kristian Næser MD, surgeons should consider targeting -0.25 D pure sphere for the distance eye and -1.25 D pure sphere for the near eye as that strategy optimises the range of functional vision without introducing any significant downsides.
his recommendation was based on the findings from a mathematical model used to determine the binocular distribution of refractions yielding the least defocus over the most extended fixation interval and the subsequent confirmation of the theoretical prediction in a small clinical study (Næser K, Hjortdal JØ, Harris WF. Pseudophakic monovision:optimal distribution of refractions. Acta Ophthalmol 2013; doi: 10.1111/aos.12148. Electronic publication ahead of print).
“Our aim in conducting this research was to determine the distribution of refractions that yields not just mediocre visual acuity, but the best uncorrected visual acuity over the most extended fixation interval in patients with binocularly implanted monofocal iOLs,” said Dr Næser, Dept of Ophthalmology, Randers Regional hospital, Randers, Denmark.
“According to our data, monovision with spherical refractions of approximately -0.25 D and -1.25 D may yield spectacle independence
for distance and intermediate vision along with some near vision, although patients may need an add for close reading,” he said.
Dr Naeser addressed the potential compromises with monovision. “Binocular problems, such as insufficient suppression of the defocused eye leading to haloes and glare at night, reduced stereoacuity and
binocular inhibition should be minimal with this monovision strategy that creates just 1.0 D of anisometropia, and so we expect patients will not be seeking iOL exchange for optical reasons. And, if this moderate monovision is not tolerated, it can be fully reversed with spectacle correction because the induced aniseikonia is minimal.”
The mathematically-derived set of binocular refractions was determined through application of a formula for describing monocular defocus at any fixation distance as a function of refractive sphere and cylinder [Næser K, Hjortdal J. Acta Ophthalmol. 2011;89:111-115]. Applying the model to the binocular situation involved solving simultaneous equations to identify the combination of refractions that gave the smallest area under the individual defocus curves for the chosen fixation interval. Considering the fixation interval of 0.33m to 6.0m, -0.27 D pure sphere for the distance eye and -1.17 D pure sphere for the near eye were identified as the optimal refractions. “Astigmatism must be avoided at all costs, since any astigmatism will cause blur throughout the fixation interval,” Dr Næser said.
The clinical evaluation included 22 patients bilaterally implanted with an aspheric monofocal iOL who were over-refracted to have a spherical refractive error of -0.25 D in both eyes and then the desired monovision targets of -0.25 D and -1.25 D (rounded from the model for practical purposes). The results showed that with monovision, patients enjoyed good visual acuity (<0.2 logMAR) over a distance range between 7.0m and about 55cm and had no loss in distance visual acuity for the fixation interval from 6.0m to 33cm.
Kristian Næser – [email protected]
cont
act
PSEUDoPHAKIC MoNoVISIoNSuggested refractions target anisometropia of 1.0 D by Cheryl Guttman Krader
19Update
caTaracT & rEfracTIvE
Endo-LaserCLASSIC
PORTABLE 532 nmFor All Retinal Photocoagulation ProceduresVarious Endo Hand Pieces 20-25 G Optional Battery Pack Bessemerstraße 14
90411 Nuremberg Germany +49 911 217 79-0
Anzeigen EuroTimes.indd 2 06.02.2014 08:58:14
Astigmatism must be avoided at all costs, since any astigmatism will cause blur throughout the fixation interval
“
Kristian Næser MD
The monocular defocus as a function of the fixations distance for the pure spherical refractions of -0.25 D and -1.25 D. The defocus (blur) is zero for fixation distances of 4.0 and 0.8m, respectively. The defocus increases with the distance from these two far points.
The binocular defocus function in each fixation point is the monocular defocus function with the lowest value. The cumulative binocular defocus is the integral of the binocular defocus function and is the area under the binocular defocus curve. The combination of refractions yielding minimal cumulative binocular defocus (the smallest area under the curve) is identified by differentiation and is determined only by
the chosen fixation interval. These refractions define the minimal blur and therefore the optimal monovision in the fixation interval
Cour
tesy
of K
ristia
n Næ
ser M
D

EUROTIMES | Volume 19 | Issue 3
There is no “one-size-fits-all” solution for every presbyopic cataract or refractive lens exchange patient, and surgeons
need to take due account of criteria such as lifestyle, occupation and expectations in guiding their choice of treatment for these patients, according to hiroko Bissen-Miyajima MD, PhD.
“Today nobody has the perfect solution for presbyopic cataract or refractive lens exchange, so to provide the best fit it is very important to take enough time to talk with the patients and understand what their requirements are. We need to take due account of the patient’s lifestyle and expectations and then we can select the ideal intraocular lens to accomplish the best surgery,” she told delegates attending the JCRs symposium at the XXXi Congress of the EsCRs in Amsterdam.
With the population ageing in Japan, as elsewhere in the developed world, there is an ever-increasing need to find viable solutions for the vast numbers of patients that will reach presbyopic age in the coming years, said Dr Bissen-Miyajima.
“We can see the situation from the population pyramid in Japan with over 50 per cent of the population now of presbyopic age. if these patients want to have presbyopic correction at the time of cataract surgery or refractive lens exchange, iOLs offer the best solution whether it is monovision with a monofocal iOL, or an accommodative or multifocal iOL,” she said.
The needs of the majority of presbyopic patients, outside of specialised careers that might require excellent near or distance vision, are to be able to perform daily tasks such as watching television, reading and
driving without dependence on glasses, said Dr Bissen-Miyajima.
Looking at the current iOL options to achieve those aims, she noted that all of the currently available lens approaches have their benefits and drawbacks.
“As a monovision patient myself after LAsiK, i have personal experience of the method’s advantages and limitations. On average, bilateral uncorrected distance visual acuity is 20/20 but near vision is usually around the J-3 range. so monovision can provide good distance vision and acceptable near vision but often requires reading glasses for small print. it is also a low-risk option for the surgeon since spectacles will solve the visual problem if the patients have some astigmatism or if they complain about their near vision,” she said.
For accommodative iOLs, the drawbacks include issues with near vision and low predictability, higher rates of posterior capsule opacification (PCO) and question marks over their long-term stability.
The newer-generation dual optic accommodating iOLs require a larger incision and astigmatic control and refractive stability may also be potential issues. Likewise, the effect of PCO and long-term stability of these lenses are currently uncertain, she said.
“While these lenses show a lot of potential we need to see more published data before we can recommend these iOLs as a first choice for presbyopia correction today,” she said.
Turning to multifocal iOLs, these lenses offer good distance and near vision for most presbyopic patients, said Dr Bissen-Miyajima.
“if the patient has very good distance vision, then my experience has been that the
patient will automatically have good near vision as well,” she said.
As with monofocal iOL platforms, the multifocal lenses currently on the market have incorporated many of the evolutions in terms of lens design and material over the years, said Dr Bissen-Miyajima.
“We have seen iOLs evolve to become foldable, acrylic, sharp-edged, single piece, aspheric yellow tinted and toric, and multifocal lenses have been able to take advantage of many of these developments,” she said.
While the refractive stability and long-term safety of multifocal iOLs are not an issue, patients need to be made aware of the possibility of some loss of contrast sensitivity after multifocal implantation, she said.
“The personal preferences and expectations of each patient are always difficult to predict. When we compare the performance of the multifocal iOL to the ideal scenario, it is perhaps easier to understand why most patients are very happy while a minority may complain of waxy vision,” she said.
While surgeons have the option to implant the same lens, either unilaterally or bilaterally, or to “mix and match” with different iOL types and designs in each eye, Dr Bissen-Miyajima said her own preference is to wait until the first eye has been implanted before deciding what to do with the contralateral eye.
“if the patient is happy with the first operation then i will implant the same lens again in the second eye. if they are less satisfied, i might implant a lens with additional add power in the other eye. With bilateral implantation, the good news is that we can improve the visual acuity and also the contrast sensitivity, especially at higher spatial frequencies,” she added.
Hiroko Bissen-Miyajima – [email protected]
cont
act
PRESBYoPIC CATARACTPatient choice should dictate optimal presbyopic IoL solutionby Dermot McGrath
20 Update
caTaracT & rEfracTIvE
WSPOSWorld Society of Paediatric
Ophthalmology & Strabismus
PAEDIATRIC SUB SPECIALTY DAY
www.wspos.org
Preceding the XXXII Congress of the ESCRS
13 – 17 September 2014 London, UK
FRIDAY 12 SEPTEMBER 2014
Today nobody has the perfect solution for presbyopic cataract or refractive lens exchange, so to provide the best fit it is very important to take enough time to talk with the patients and understand what their requirements are. We need to take due account of the patient’s lifestyle and expectations...
“
Hiroko Bissen-Miyajima MD, PhD
“As a monovision patient myself after LASIK, I have personal experience of the method’s advantages and limitations”

21
EUROTIMES | Volume 19 | Issue 3
Teifi James – [email protected]
cont
act
The incidence of dry eye is very significant but is not being adequately addressed. One place to start would be simply to get
patients to blink more to relieve symptoms, Teifi James FRCOphth, consultant ophthalmologist and surgeon, West Yorkshire, UK, told the XXXVII UKISCRS Annual Congress in Manchester.
Dr James gave a comprehensive update on meibomian gland dysfunction, stressing that dry eye affects up to 40 per cent of the population.
He said most ophthalmologists find the condition an “irritation” and that it is a “lottery” for patients to find a clinician who is interested in treating it.
“About 90 per cent of dry eye is evaporative. Sjogren's syndrome is actually quite rare, and most of the time it is lipid layer issues. It is an inflammatory condition, and blinking is crucial,” he told the congress.
Explaining how dry eye occurs, Dr James said the lipid layer stabilises the tear film and reduces aqueous evaporation, and problems occur if the layer is inadequate or the meibomian glands are blocked.
“So if your lipid layer is not there and you are not blinking, your eyeball will dry out,” he said.
If unsure if a patient has Sjogren's syndrome or dry eye, Dr James advised asking the patient if they produced tears when chopping onions, for example. If they do, then their lacrimal gland function is there, and a dry tongue will also help confirm if they have Sjogren's syndrome.
Blinking Dr James confirmed that patients with meibomian gland dysfunction clearly do not blink enough. Most people nowadays spend far too much time staring intently at computer and TV screens.
“Everybody is spending hours a day in close attentive gaze and this is farming meibomian gland dysfunction. People really do not realise how little they blink,” he remarked.
Quoting a blinking rate data study he conducted with 118 Scottish clinicians, Dr James said the average number of blinks over a 30-second period when talking was 15 while when reading or in close attentive gaze the average number was just four,
with 16 people not blinking at all, 15 only blinked once and 14 blinked twice.
“That cohort of people who hardly blink during close attentive gaze represent the ones who get symptomatic evaporative dry eye, and consequently meibomian gland dysfunction,” he remarked.
He called on ophthalmologists and opticians to encourage their patients to blink more regularly and to explain to them why this is so important.
“We should rename the return key on computer keyboards the blink button. Tell your patients that every time they hit the button, click send on an email, etc, that they should blink, as it’s the only way you will get them to re-wet their corneal surface,” Dr James told the congress, noting that about one third of dry eye symptoms would disappear if patients blinked more.
Treatment Dr James said there is now compelling clinical data that omega-3 supplements are very helpful in addressing dry eye.
Good eye hygiene is also key, Dr James noted, adding there are now plenty of good quality lid wipes available from opticians, as well as lubricant drops.
He dismissed the common treatment of bathing the eyes with baby shampoo diluted in warm water as ineffective, confusing, unscientific, with poor compliance.
Blocked eyelid glands are helped by warmth, he acknowledged, but said the classic approach of using warmed flannels is ineffective, because to work
the temperature must remain at about 40 degrees, as solid meibomian secretions melt at 39 degrees.
To address this issue, Dr James created his own heated eye pad, which would remain above this temperature for about 10 minutes. He consequently set up the EyeBag Company Ltd in April 2004, which sells the MGDRx EyeBag for the treatment of meibomian gland dysfunction. There are also other heated eye pads on the market.
Dr James said that regularly applying a warm MGDRx EyeBag for 10 minutes two or three times a day can improve meibomian gland dysfunction symptoms dramatically. A study of patients with Sjogren's syndrome found that 90 per cent reported a significant benefit too, he told delegates.
With regards to antibiotic treatment for severe cases, Dr James said that he no longer uses doxycycline and recommended using lymecycline, which he
said is “incredibly effective”.For ophthalmologists interested in
learning more about meibomian gland dysfunction, Dr James recommended the website of the Tear Film and Ocular Surface Society (TFOS) – www.tearfilm.org, which contains very useful data and disease staging and treatment charts.
Speaking to EuroTimes, Dr James said the key issue with treating dry eye is poor compliance with “homemade remedies”.
“I think we’ve underestimated as a profession how little patients do what we’ve been advising them to do for years. I think providing them with an easy way of warming their lids and an easy way of cleaning their lids is the biggest step forward in managing this,” he concluded.
by Priscilla Lynch
Key issue with treating dry eye is poor compliance with ‘homemade remedies’BLINK MORE
Glaucoma Day2014
ESCRS
Scientific Programme organised by
www.escrs.org
Friday 12 September
Update
CORNEA
About 90 per cent of dry eye is evaporative. Sjogren’s syndrome is actually quite rare, and most of the time it is lipid layer issues. It is an inflammatory condition, and blinking is crucial
“
Teifi James FRCOphth

22Yuri McKee – [email protected]
cont
act
EUROTIMES | Volume 19 | Issue 3
While Descemet’s membrane endothelial keratoplasty (DMEK) is a technically more difficult procedure,
it provides better visual results with fewer problems than Descemet’s stripping endothelial keratoplasty (DSEK), so it is worth the extra effort, reports Yuri McKee MD. “The finding that DMEK reduces the rejection risk is the real game-changer in its favour, and now we are finding the lower rejection risk probably allows for a decrease in the steroid burden after DMEK with the potential for decreasing steroid-related complications,” he said.
Dr McKee is in private practice at the Price Vision Group, Indianapolis, IN, where more than 1,100 DMEK cases have been performed since March 2008. Speaking at the 4th EuCornea Congress in Amsterdam, he reported findings from outcomes analyses in a series of eyes that had DMEK, DSEK and penetrating keratoplasty (PK).
Data on vision outcomes came from follow-up to one year in a group of patients who underwent DMEK and DSEK in fellow eyes. Mean logMAR BSCVA was better in the DMEK eyes than after DSEK, 0.07 vs. 0.20. Moreover, 85 per cent of patients stated they preferred the vision in their DMEK eye due to better quality.
Data on risk of transplant rejection were reported in a published study that included 141 DMEK eyes, 598 DSEK eyes and 30 PK eyes [Ophthalmology. 2012;119(3):536-40]. Based on Kaplan-Meier survival analysis and defining rejection as any amount of corneal oedema after initial clearing with any amount of inflammation, the two-year cumulative probability of rejection was less than one per cent for DMEK, 12 per cent for DMEK and 18 per cent for PK.
“The DMEK eyes had a 15-fold lower risk of rejection than the DSEK eyes and a 20-fold lower risk than the PK group. Those differences were highly statistically significant and importantly, they were found in cohorts of patients that were operated on at a single centre, had similar indications for surgery, represented a similar racial mix and received the same steroid dosing regimen,” Dr McKee said.
He added that there have been only nine rejection episodes among the more than 1,100 DMEK procedures performed in the past 5.5 years. Those events occurred
between two weeks and four years after surgery, and in only one case was rejection associated with graft failure.
Data on primary graft failures highlighted the learning curve with DMEK, showing that the cornea failed to clear in six of the first 80 cases and in four of the second 80. In contrast, there were five primary failures in the first 80 DSEK eyes, but only one in the next 80 cases.
“The graft is more difficult to prepare, manipulate and attach when performing DMEK compared with DSEK. However, in more recent studies of DMEK, the graft preparation failure rate is only one per cent, and now there are eye banks preparing the DMEK graft,” Dr McKee said.
Other data Dr McKee presented showed similar outcomes for DMEK and DSEK. Both had better long-term endothelial cell survival than PK. Based on follow-up of 3-5 years, DMEK and DSEK are associated with excellent mid- to long-term graft survival.
DMEK graft survival rates were analysed using data from cases performed at the Price Vision Group between March 2008 and September 2010. Focusing on the 143 eyes with Fuchs' dystrophy, Dr McKee reported there were only three late failures, including an endothelial failure without rejection, an endothelial failure after rejection and a regraft for poor vision. In a DSEK cohort of 147 eyes with Fuchs' dystrophy, six late failures occurred during follow-up to five years, of which four were regrafts for poor vision.
Two randomised studies have been undertaken to investigate whether the intensity of steroid treatment could be reduced after DMEK. In both studies, patients received prednisolone acetate four times daily for the first month and then are randomised to continue prednisolone acetate
or to receive fluorometholone 0.1 per cent in one study or to loteprednol etabonate 0.5 per cent in the other trial. The same tapering regimen is used over the next 11 months in all steroid groups.
Dr McKee reported that preliminary findings from the study comparing prednisolone acetate and fluorometholone, which enrolled 325 eyes, show no difference in rejection rates between the two groups.
However, prednisolone acetate was associated with a significantly higher rate of IOP elevation than fluorometholone.
“The risk of cataract from steroid treatment is less of a concern among DMEK patients because most are pseudophakic. However, we know that steroid use is a balancing act between avoiding rejection risk and IOP elevation,” Dr McKee said.
Better functional outcomes and lower rejection risk tip the balance in favour of DMEKby Cheryl Guttman Krader
ENDOTHELIAL KERATOPLASTY
Update
CORNEA
We prepare the donor graft using the SCUBA technique as described by Art Giebel
The DMEK graft preferentially forms a scroll with donor endothelium on the outside of the scroll
Often within days or weeks after DMEK the host cornea is crystal clear with little evidence of a corneal graft. Rejection
episodes occur in less than one per cent of cases
Once the graft is opened up and well centred it is held in place with a 90 per cent air fill in the anterior chamber
Cour
tesy
of Y
uri M
cKee
MD

23Laurent Laroche – [email protected]
cont
act
EUROTIMES | Volume 19 | Issue 3
Routine use of optical coherence tomography (OCT) and in vivo confocal microscopy could improve corneal disease
screening, diagnosis, monitoring and research much as they have retinal disease, Laurent Laroche MD told the 4th EuCornea Congress in Amsterdam.
“I still use the slit lamp as a first step for corneal examination. But higher resolution allows better visualisation of structural features of the cornea,” said Dr Laroche, of Quinze-Vingts National Ophthalmology Hospital, Paris, France.
Dr Laroche currently uses Fourier-domain OCT on all corneal patients, and confocal microscopy on a few. He uses OCT-RTVue (Optovue) with a corneal adaptor, which provides micron-scale cross-sectional imaging and automatic corneal epithelium thickness mapping.
For confocal microscopy, Dr Laroche uses HRT 3-RCM (Heidelberg Engineering), which provides high-quality images for assessing microstructural morphologic changes occurring in pathology – in vivo cytology, if you will. Both can be highly effective in refining diagnoses for infectious and non-infectious disease, and assessing treatment follow-up.
OCT can be helpful in confirming diagnoses of diseases that can be hard to visualise, such as Cogan’s dystrophy, Dr Laroche said. “Cogan’s disease sometimes is obvious on slit lamp examination, but sometimes you don’t really see the cysts very well. OCT cross-sections clearly reveal cysts and separations between the epithelium and Bowman’s membrane, while HRT can show detailed images of the cysts,” he noted.
High-resolution imaging also can be useful for diagnosing and determining treatment for infectious keratitis, Dr Laroche said. For acanthamoeba keratitis, the slit lamp shows a characteristic immunological ring in the cornea, but OCT better shows infiltration sites while HRT can image cysts as well as trophozoites.
In fungal keratitis, OCT shows the depth of ulcerations and inflammation, Dr Laroche noted. “You can clearly see when Descemet’s membrane is involved, which is of utmost importance for treatment strategy.”
OCT can be used to track inflammation and ulceration to determine the effectiveness of treatment. Similarly, OCT
can show the extent of infection in bacterial keratitis. The depth of the scar will be important for deciding the right treatment, Dr Laroche said.
OCT also clearly shows features of Reis-Bucklers dystrophy, including involvement of the anterior stroma, and granular corneal dystrophy, involving the full stroma. Differentiating the disease is important for treatment.
Perhaps the most significant recent
application of OCT for corneal disease is in staging keratoconus, said Dr Laroche. He was one of a team of researchers who developed the scale now used (Ophthalmology Dec 2013; 120 (12):2403-2012).
OCT imaging Blinded evaluations of 218 patients with keratoconus established five stages of keratoconus clearly identifiable based on OCT imaging. The criteria were found to be highly reproducible and
specific and correlated well with clinical characteristics of keratoconus, including visual acuity, corneal epithelium and stromal thickness changes, as well as corneal topography, biomechanical corneal characteristics and microstructural changes observed on confocal microscopy, Dr Laroche noted.
Stage 1 demonstrates thinning of apparently normal epithelial and stromal layers at the conus. Stage 2 demonstrates hyper-reflective anomalies occurring at the Bowman's layer level with epithelial thickening at the conus. Stage 3 demonstrates posterior displacement of the hyper-reflective structures occurring at the Bowman's layer level with increased epithelial thickening and stromal thinning. Stage 4 demonstrates pan-stromal scar with thinning of residual stroma. Stage 5 demonstrates hydrops, with 5a detailing acute onset with Descemet’s membrane rupture and cyst formation, and 5b healing with pan-stromal scarring.
OCT images and the staging classifications can be very helpful in clinical practice, Dr Laroche said. “When you set the indication for corneal cross-linking in thin corneas, it is not the same problem if your cornea is 400 microns thick and epithelium represents 25 per cent of thickness compared with [a 400 micron cornea with] over 300 microns epithelium. The effect will be very different.”
OCT is also helpful in cross-liking follow-up. Variations in patient response can be seen and tracked, infiltrates observed and monitored, and the effectiveness of cross-linking assessed.
“Sometimes you can see a demarcation line, and sometimes you can see increased response in some patients.”
OCT is also useful to monitor results of intracorneal ring segments, including any response to the implants. In lamellar keratoplasty, OCT helps evaluate remaining bed in anterior grafts, and attachment of posterior grafts. Graft-host junction can be monitored after penetrating procedures. “When you have a giant astigmatism, it may give you some idea of how to treat it.”
OCT provides accurate pachymetry readings and epithelial thickness maps, which may provide early warning of forme fruste keratoconus. Follow-up after PRK helps track sub-epithelial healing, while post-LASIK imaging can determine the extent of epithelial ingrowth.
High-resolution imaging routinely used is as informative for the cornea compared with slit lamp examination as OCT is for the retina compared with fundus examination, Dr Laroche concluded. He believes it will revolutionise corneal treatment and research.
by Howard Larkin
Routine use aids precise screening, diagnosis, monitoring and researchOCT, HRT FOR CORNEA
Update
CORNEA
Increased epithelial thickening and stromal thinning are clearly seen
OCT cross-sections clearly reveal cysts and separations between the epithelium and Bowman’s membrane
The extent of epithelial ingrowth is obvious
Cour
tesy
of L
aure
nt L
aroc
he M
D

24Harminder S Dua – [email protected]
cont
act
One thing Harminder S Dua MD, PhD does now that he didn’t in years past is delay surgery for limbal deficiency in patients who retain a central island of corneal epithelium and reasonable
vision (Figure 1). While a good supply of limbal stem cells is essential to replace corneal epithelium once it is lost, his research suggests the limbus plays a minimal role in normal physiological corneal epithelial homeostasis.
“It is only in response to injury that the limbus comes in a big way,” Prof Dua, of Nottingham University, UK, told the 4th EuCornea Congress in Amsterdam. He has observed central corneal epithelium remain clear and stable for years in patients with total limbal stem cell deficiency and conjunctivalised epithelium in the peripheral cornea. What’s more, these patients often see quite well.
“Limbal deficiency is compatible with good vision in patients where a central island survives. Even if I see it gradually shrinking over time, I will not rush in for surgery until vision is seriously compromised,” said Prof Dua.
He presented several emerging limbal deficiency treatments based on a growing understanding of the roles the limbus and conjunctiva play in generating and maintaining corneal epithelium.
One challenge of autologous and living relative donor limbal grafts is they only partially surround the cornea, leaving wide paths for conjunctival epithelial ingrowth. This blocks corneal epithelium growing from limbal grafts from fully covering the corneal surface.
Sequential sector conjunctival epitheliectomy (SSCE), can solve the problem. But while periodically scraping away competing conjunctival epithelium does help corneal epithelium spread, it can be difficult and painful, and risks complications such as bleeding, Prof Dua said.
Amnion assisted conjunctival redirection (ACER), can eliminate the need for SSCE, Prof Dua said. He places an amniotic membrane over the cornea after the limbal grafts are attached, tucking the membrane edge under the conjunctiva, but leaving the edge over the limbal grafts. This
directs conjunctival epithelium growth over the membrane, allowing unobstructed transplanted limbus derived corneal epithelium growth beneath the membrane.
In two to four weeks, corneal epithelium covers the entire corneal surface while conjunctival epithelium covers the outside of the membrane, Prof Dua said. Often the membrane then separates spontaneously, but it also may be removed surgically.
“This is what I do now standard in all my autologous and living related grafts so I don’t have to repeatedly brush or scrape advancing conjunctival epithelium” he said.
Conjunctival alternatives Keeping conjunctival epithelium off the cornea is usually desirable. But if the alternative is no epithelium at all, it may be better to let the conjunctiva grow, Prof Dua said. “Any epithelium is better than no epithelium. Even if it is very thin cornea, if it is epithelialised the risk of melting and perforation is low.”
In some cases, the conjunctival epithelium may even develop into a phenotype indistinguishable from corneal epithelium, Prof Dua said. He discovered this in a patient with a chemical burn that had destroyed the entire corneal and limbal surfaces along with much of the conjunctiva. Epithelium began growing from a remote undamaged portion of the conjunctiva, so Prof Dua let it grow.
Within a month, the entire cornea re-epithelialised with what appeared under confocal microscopy to be normal corneal epithelium – even though the limbus was destroyed, Prof Dua said. “We saw it happen before our eyes and on long-term follow up the cornea remains completely clear.”
Prof Dua has now seen the effect in five eyes of four patients. How it happens is not known. Conjunctiva transforming into corneal phenotype is a possibility. Or palisade-like structures found in bulbar conjunctiva of pigmented individuals may provide stem cells much as do palisades near the limbus. Or conjunctiva growing onto the cornea without vascularisation may produce epithelium of a more normal phenotype in the absence of limbus.
“I look at the conjunctiva very differently now, as a friend rather than a foe,” Prof Dua said.
Another use of conjunctiva is free autografts when corneal melting is not responding to other measures, and as an alternative to tenoplasty, Prof Dua said.
In a patient with a chemical burn and an amniotic membrane that fell off, Prof Dua took a conjunctiva graft from the fellow eye, and stitched it to pink (viable) tenon’s tissue. This resulted in vascular conjunctiva covering the corneal surface. The conjunctival graft vessels establish connections with the tenon’s vessels thus bringing blood to the ischaemic limbus. When the eye was quiet, he removed the conjunctiva and performed an auto limbal transplant. The result was a clear cornea with 20/60 vision unaided, and 20/30 with a rigid gas-permeable contact lens.
Peripheral cornea and limbus transplant? In some cases, Prof Dua transplants peripheral cornea from donor cornea-scleral discs to preserve central cornea in patients for which limbal donors are not available. In one case he observed both the peripheral and central cornea survive with sustained epithelialisation. In another patient the epithelium over the transplanted peripheral corneal strip was lost, but conjunctival epithelium grew in to replace it and continued to migrate centrally to cover the corneal surface. Central corneal epithelium was maintained, apparently by cells migrating from the recipient conjunctiva across the donor peripheral corneal stroma.
“The question I am asking myself is, if I just have the niche, which is the stroma of the peripheral cornea and the distant sclera, and the cells come from the conjunctiva on it, do they change phenotype? Does the niche influence the cells to start coming off the other end as more cornea-like cells, or is it just conjunctiva coming off and behaving like cornea?” he said.
by Howard Larkin
New surgical techniques develop as understanding growsLIMBAL DEFICIENCY
EUROTIMES | Volume 19 | Issue 3
Update
CORNEA
Figure 1: Surviving central island of corneal epithelium after hydrogen peroxide (used with hair dye) injury had caused ocular surface injury followed by re-epithelisation and
chronic 360 degrees of conjunctivalisation. In vivo confocal microscopy in four quadrants showed all the signs of limbal stem cell deficiency
Figure 2a: Autologous limbal stem cell transplant (two clock hours of donor limbal explants at 12 and 6 o’clock of recipient limbus) with a large patch of amniotic membrane
covering the cornea and explants
Figure 2b: Immediated postoperative showing that the amniotic membrane stains with fluorescein
Figure 2c: One week later showing the conjunctival epithelium, which would otherwise have grown on to the recipient cornea and required sequential sector conjunctival
epitheliectomy, is now growing on the amniotic membrane, which can be later removed, leaving the underlying cornea to be covered by limbal explant derived corneal epithelium
Cour
tesy
of H
arm
inde
r S D
ua M
D, P
hD

25
12-13 September 2014
www.eucornea.org
Abstract submission deadline:14 March 2014
LONDON5th EuCornea Congress
EUROTIMES | Volume 19 | Issue 3
Despite the improvements in surgical and medical therapy that have taken place over recent decades, a considerable
proportion of glaucoma patients will end up with significant visual impairment by the end of their lives, said Carroll Webers MD, PhD at a Glaucoma Day session at the XXXI Congress of the ESCRS in Amsterdam.
“We can talk about surgery and diagnostic techniques but this is what it all comes down to, can we improve the end-of-life visual impairment in glaucoma patients? Therefore, it is relevant to know the extent of the problem,” said Dr Webers, University Eye Clinic Maastricht, The Netherlands.
He presented the findings from a systematic review of published studies concerned with determining the rate and the level of end-of-life visual disability among glaucoma patients as well as the factors associated with that visual disability.
They used Medline to do their literature search, employing the “snowball” method, which meant that all the references of each paper were followed up as well. To be eligible, the studies had to be written in English, Dutch, German or French.
Differences between studies In all, they found five studies which fit their eligibility criteria. All of the studies were retrospective follow-up studies, but they varied in terms of the years patients died and the type of centre or clinic where they were treated. They also varied in terms of the types of glaucoma diagnosed and the criteria for visual disability and blindness. Therefore, a straightforward meta-analysis was not possible.
The mean age at diagnosis was fairly high, ranging from 72 years to 74 years in the different studies. The mean age at death was also high, ranging from 82.2 years to 85 years. The mean IOP at last visit ranged from 15.2 mmHg to 20.4 mmHg. The mean IOP was highest in a study concerning patients who died during the years 1991 to 2002. That may have been because it involved patients diagnosed at a time prior to the introduction of prostaglandin analogues, Dr Webers said.
The proportion of patients who were visually impaired by glaucoma ranged
from nine per cent to 15 per cent, the proportion that were unilaterally blind because of glaucoma ranged from 11 per cent to 24 per cent and the proportion that were bilaterally blind because of glaucoma ranged from zero to 10 per cent. In addition, the proportion of patients who were ineligible to drive because of glaucoma ranged from 18 per cent to 28 per cent.
The factors associated with end-of-life visual impairment from glaucoma were more advanced baseline visual field loss, higher IOP, older age and longer duration of disease.
Dr Webers noted that the findings of the study regarding prognostic factors of glaucoma progression were in accordance with another study he and his associates published in March 2013 (Ernest et al, Ophthalmology. 2013 Mar;120:512-9).
That study involved a review of 85 articles on the topic and identified older age and optic disc haemorrhage (in normal-tension glaucoma) as definite prognostic factors and more advanced baseline visual field loss and higher baseline IOP as probable prognostic factors.
by Roibeard O’hEineachain
Visual disability and blindness remains the eventual fate of many glaucoma patients
END-OF-LIFE VISION
25Update
GLAUCOMA
Carroll Webers – [email protected]
contact
We can talk about surgery and diagnostic techniques but this is what it all comes down to, can we improve the end-of-life visual impairment in glaucoma patients? Therefore, it is relevant to know the extent of the problem
“
Carroll Webers MD, PhD

26Philippe Denis – [email protected]
cont
act
There are measures that can be taken at every step of surgery that will help insure the best possible outcome from trabeculectomy
procedures and avoid many common complications, according to Philippe Denis MD, Hopital de la Croix-Rousse, Lyon, France.
“Trabeculectomy is currently the most effective primary glaucoma surgical procedure and certain refinements to the technique can improve the outcomes and improve the safety and reduce the risk of complications,” Dr Denis said at a Glaucoma Day session of the XXXI Congress of the ESCRS in Amsterdam.
For example, there are anti-metabolites that enhance filtration by preventing scar formation. There is also laser suture lysis or releasable sutures for greater early postoperative safety. In addition, there are a range of stents that provide a micro-conduit for the outflow of aqueous from the anterior chamber.
Older style tube shunts like the Baerveldt and Ahmed devices produce similar results to trabeculectomy in terms of long-term safety and efficacy but have lower rates of re-operation. The devices are particularly useful in eyes undergoing cataract surgery, but are rarely indicated as a first-line choice.
Other techniques that rival trabeculectomy in terms of efficacy but have safety advantages are the non-penetrating techniques such as deep sclerectomy, which results in lower rates of hypotony but it is technically more demanding.
Preparing the eye Dr Denis noted that when possible, it is best to stop eye drops before surgery because several studies have shown that long-term anti-glaucoma therapy is associated with increased rates of surgical failure and that the risk increases with the duration of treatment and the number of agents used.
He noted that an important cause for the poor outcomes in patients receiving topical therapy over a long period is the result of the toxic effect of preservatives such as benzalkonium chloride.
However, benzalkonium chloride’s toxicity is reversible. Eyes can have a
complete recovery of their corneal nerve network by four weeks after withdrawal of agents containing the preservative. (Sarkar J et al, Invest Ophthalmol Vis Sci. 2012;53(4):1792-802.)
Pre-treating the eye before surgery with topical NSAIDs has been shown to increase this success of trabeculectomy. In eyes with neovascular glaucoma, intravitreal bevacizumab with or without panretinal photocoagulation can induce a reduction of the neovascularisation in the cornea and in the retina.
In eyes with inflammatory glaucoma with uveitis the optimal approach is to select a time for surgery when the uveitis has been quiescent for three months. However, in cases where the requirement for surgery is urgent, it is necessary to treat the inflammation aggressively to avoid a relapse, which can increase the risk of failure.
In terms of anaesthesia, Dr Denis noted that although general anaesthesia may be the simplest approach it entails the risk of nausea and vomiting which can in turn increase the risk of choroidal haemorrhage.
Retrobulbar anaesthesia, meanwhile, carries the risk of optic nerve injury and it has limited effect on the conjunctiva. Local anaesthesia is generally less traumatic to the eye and enables the surgeon to tell the
patient to move his head when necessary during surgery. Among the products available is lidocaine gel, which can be applied subconjunctivally with a cannula.
Surgical pearls The best location for the conjunctival flap is at 12:00 at the limbus. This protects the bleb and reduces the risk of diplopia. In addition, placing a traction suture in the clear cornea helps prevent bleeding from the episclera. In cases of repeat trabeculectomy the choice of site should be guided by the conjunctival mobility test.
Dr Denis noted that conjunctival flaps have the advantage of healing rapidly, a greater distance between the conjunctival suture and the sclerectomy site, and, potentially, a reduced amount of bleb leaks. Fornix-based flaps have the advantage of being easier to perform because they provide better visualisation of the sclera.
When using mitomycin-C, the agent should be applied at a concentration of 0.2 to 0.5 mg/ml for one to three minutes, followed by an intensive rinsing of the eye.
Some recent studies are showing anti-
VEGF agents bevacizumab and ranibizumab delivered by various means may produce better results than mitomycin-C in terms of IOP and bleb morphology. The parameters that remain to be defined include the optimal dose, the route of administration and the time and duration of use, Dr Denis said.
He noted that iridectomy cures pupillary block and prevents the risk of obstructing the ostium. However, it is not necessary in eyes undergoing combined procedures or in pseudophakic eyes.
Postoperatively, steroids are a mainstay of treatment for reducing inflammation. In eyes where the visual field loss is within 10 degrees of the fixation special postoperative care is necessary to avoid systemic and ocular hypotension in order to prevent the loss of the remaining visual field.
“Trabeculectomy is the mainstay of surgical treatment for glaucoma. Recent innovations are welcome, as it is important to improve our treatment and they may have an increasing role in the future. But for the time being, don't be afraid even in the most difficult case," Dr Denis advised.
by Roibeard O’hEineachain
Preventing and fixing common complications of filtration surgeryTRABECULECTOMY PROCEDURES
EUROTIMES | Volume 19 | Issue 3
Update
GLAUCOMA
Monocystic bleb after trabeculectomy
Trabeculectomy is the mainstay of surgical treatment for glaucoma. Recent innovations are welcome, as it is important to improve our treatment and they may have an increasing role in the future. But for the time being, don’t be afraid...
“
Philippe Denis MD
Don’t Miss Industry News, see page 39
Cour
tesy
of P
hilip
pe D
enis
MD

27David Thomson – [email protected]
cont
act
Caring for the health and welfare of athletes and their support teams has become an important part of organising the Olympic
Games. Providing eye care services is now an important part of this provision and in this respect, London 2012 set new standards, the XXXVII UKISCRS Congress in Manchester heard.
Prof David Thomson, City University, London, gave a detailed presentation on the dedicated eye clinic he organised and led with Dr Penny D’Ath (City University) and Dr Clare Wilson (UCL Institute of Ophthalmology) during the 2012 London Olympics and Paralympics.
The London 2012 Eye Clinic combined a multi-disciplinary team of optometrists, ophthalmologists, contact lens opticians and dispensing opticians with state-of-the-art instrumentation to provide the highest level of eye care and to showcase UK healthcare, he explained, adding that there was a “huge amount of work involved” in planning, organising and running the service.
Facilities The purpose-built medical polyclinic allocated five rooms to the eye clinic. Most of the equipment was top of the range and was provided on free loan or at a very low cost from the major suppliers, as were the spectacles and contact lenses.
“The facilities were world class at London 2012. Good vision is obviously important in many sports, so the eye clinic has been an important part of the health services offered at certainly the last three games, and probably before then though there is very little in the way of records on that,” he told the congress, adding that the London experience was fully documented to provide a legacy for future organisers of such clinics at other events.
The clinic provided a full range of completely free-of-charge eye care. Everyone who attended the clinic was given a full eye examination, which included refraction, binocular vision assessment, fundus imaging, OCT, visual fields, tonometry and an ophthalmological assessment if required. A wide range of spectacles, contact lenses and low vision aids were dispensed.
All the staff worked on a voluntary basis and required four days training and a
minimum of 10 days availability to work during the games. The clinic was open from 7am to 11pm to accommodate the training and competitive schedules of the games.
“Despite this, we had over 200 optometrists, dispensing opticians and ophthalmologists volunteer. The challenge was reducing the numbers and selecting the personnel needed, which for the Olympics turned out to be 16 optometrists, 10 dispensing opticians and eight ophthalmologists. For the Paralympics we had eight optometrists, six dispensing opticians and six ophthalmologists,” Prof Thomson commented.
Services provided The eye clinic saw a total of 1,406 patients, representing some 154 countries during the period of the Olympic Games. A total of 870 patients representing 102 countries were seen by the clinic during the period of the Paralympic Games. “More than 90 per cent of patients at both games attended for a full eye examination and 973 pairs of spectacles and 50 pairs of contact lenses were dispensed during the Olympics, while 749 pairs of spectacles and 14 pairs of contact lenses were dispensed during the Paralympics,” Prof Thomson reported.
“Many of those we examined did not have access to the services that we could provide and we were able to make a significant improvement to the vision of many of them by providing a proper refractive correction,” he commented.
However, only one fifth – approximately 20 per cent – of those seen during the Olympics were athletes; the remaining 80 per cent were members of the support teams.
“From a professional point of view, the Paralympics were more challenging as around 20 per cent of the competitors were visually impaired, including some with eye conditions rarely seen in the UK,” said Prof Thomson. It was immensely rewarding to be able to help some of them with refractive correction, low vision aids and to provide expert ophthalmological advice.
In addition to providing routine eye care, the clinic was responsible for managing any acute conditions and eye injuries. “There were a variety of abrasions but no significant eye injuries during the
games,” Prof Thomson told the congress. A variety of eye conditions were
detected by the screening with glaucoma and diabetic retinopathy being the most common reason for referral to the ophthalmologists in the clinic.
Prof Thomson said the predictions for staffing for the clinic worked out well: “The only change we would have made would have been to have had a few orthoptists on board as we did have some quite complex binocular vision problems, in particular at the Paralympics, and we could have done with some more dispensing opticians as well.”
“In summary, it was a fantastic experience. We made a great team and it was an experience that most of those involved considered to be a highlight of their professional careers,” he concluded.
by Priscilla Lynch
Glaucoma-related referrals followed by diabetic retinopathy commonest reasons patients saw ophthalmologists in London Olympics eye clinic
OLYMPIC EYE CARE
EUROTIMES | Volume 19 | Issue 3
Update
OCULAR
Prof David Thomson and Dr Penny D’Ath who led the eye care team at London 2012
Prof David Thomson and fellow volunteers in the athletes village where the polyclinic was based
Cour
tesy
of P
rof D
avid
Tho
mso
n

28
08_1402_04 ESASO_Anz_EUT_120x300_March_RZ.indd 1 07.02.14 11:38
For young and talented ophthalmologists who have completed residency training and are seeking to advance in their
profession, the career ladder can seem complex and difficult to navigate.
There are many opportunities to advance in the ophthalmic profession, however.
More than 350 enthusiastic young ophthalmologists attended ESASO modules in 2013. While over 70 per cent of the participants hailed from Europe, 14 per cent came from Asia, five per cent from South America and four per cent each from the Middle East and Africa.
ESASO believes that the high level of participation in the modules indicates that the quality of tuition and opportunities for hands-on learning under expert direction is internationally recognised. Together, the diverse student body and faculty form the ESASO community, an intercontinental network of knowledge and friendship.
This is in keeping with the school’s “Vision of Collaboration”, which sees prestigious universities and hospitals teaming up to develop career paths for talented young colleagues and establish a network of personal bonds throughout the world.
2014 programme The educational programme in 2014 is covering the entire field of ophthalmology, offering participants the chance to broaden their knowledge in key subspecialties such as orbital, lacrimal and ophthalmic plastic surgery, medical and surgical retina (with advanced and intermediate levels), cornea and corneal refractive surgery and glaucoma.
In January, the oculoplastic course directors Ramón Medel and Luz María Vásquez focused on concepts related to the eyelid, orbital examination, surgical approaches to the orbit, trauma management, tumours, DRC and C-DRC, aesthetic surgery and midface lifting.
In February, the first course took place on the Lugano Campus. The programme directors, Borja Corcóstegui and Bruno Falcomata provided insights into new therapies of non-infectious uveitis, new treatments for proliferative diabetic retinopathy, presented clinical cases on central serous chorioretinopathy, intravitreal anti-VEGF treatment for neovascular AMD, diabetic macular edema, OCT therapies and
patient management in retinal vein occlusion. For the first time, ESASO provided
training in the Middle East where two modules on Medical and Surgical Retina were held. The first module, a basic course, took place at the Dubai Hospital where programme director Moza Ali Dekhain taught her colleagues surgical approaches in pneumatic retinopexy, episcleral surgery, vitrectomy, OCT, challenging retinal detachments, clinical cases and proliferative diabetic retinopathy. Live surgeries were conducted by Borja Corcóstegui and Marco Mura.
The fourth ESASO module will take place in Tel Aviv in early March. Anat Loewenstein together with Itay Chowers, and Joseph Moisseiev have assembled a first-rate faculty to present information on DME, PDR, VMT, AMD, PCV, RAP, lesions mimicking CNV, CRVO, BRVO, OCT, PPV, PRRD. In addition, panel discussions will be held in order to make the programme more engaging. The module will conclude with Wetlabs and a pipeline showcase.
All of these modules have similarities: Leading faculty members exchanging innovative knowledge in an open atmosphere and providing many useful tips on performing surgery. ESASO looks forward to meeting you too!
Detailed programmes and application forms for upcoming courses are available at: www.esaso.org.
Borja Corcóstegui – [email protected]
contact
Developing world-class ophthalmologistsEDUCATION
EUROTIMES | Volume 19 | Issue 3
News
EsAsO
Borja Corcóstegui, president Scientific Council ESASO

29
Trabeculectomy has remained essentially unchanged since it was first described by Cairns in 1968. However, bugbears such as
sub-conjunctival fibrosis and failure as well as flap-related problems such as uneven flap; maceration/tears in the flap; irritation, foreign body reaction and rarely, abscess secondary to flap sutures; sealing of the triplanar flap etc, are problems associated with it.
Creation of either a limbal- or fornix-based conjunctival flap for any kind of procedure invariably induces sub-conjunctival fibrosis which can lead on to filtration failure secondary to scarring. Wound modulators such as Mitomycin-C or 5-Flurouracil are used intraoperatively for decreasing the fibrotic tendency, however, these may be associated with other problems such as thin, avascular blebs, blebitis etc.
A new technique Stab Incision Glaucoma Surgery (SIGS) is a new guarded filtration procedure that I described which aims at getting rid of many of the disadvantages of trabeculectomy and tunnel trabeculectomy, at making bleb function less dependent on scarring while at the same time making the anti-glaucoma procedure easier and faster to perform. The technique consists of using a 2.8mm bevel-up keratome in a single step to create a sclero-corneal tunnel which is then intentionally compromised by punching the posterior corneal lip.
The technique consists of first making the anterior chamber (AC) firmer by instilling viscoelastic with a 26 G needle introduced at the limbus. A site with mobile conjunctiva is selected and the conjunctiva slid forwards with a blunt instrument. The keratome is used to make a stab incision through the conjunctiva and into lamellar sclera starting about 2.5mm behind the limbus and avoiding major blood vessels. It is passed in a single movement through conjunctiva into lamellar sclera. While holding the globe firmly at the limbus with a toothed forceps, a superficial lamellar scleral tunnel is then dissected forwards with the keratome with careful side-to-side movements up to the limbus. The ideal plane of dissection is such that the blade is just visible through the conjunctiva. The keratome then enters about 1mm into lamellar cornea and is pushed further forwards into the anterior chamber.
Downward push Downwards push on the posterior corneal lip should be avoided while entering the AC as it may cause a trapdoor hinging of the posterior lip of the corneal tunnel. The blade is then withdrawn gently in a single smooth movement without allowing aqueous leak through the incision.
The entire tunnel is thus created in a single step with a single instrument. Viscoelastic is again injected into the AC through the paracentesis/SIGS tunnel. While holding the globe rotated downwards,
a Kelly's Descemet's punch (1mm) is slid along the tunnel into the AC and the internal lip of the corneal section engaged and punched.
Additional punches are taken posteriorly in the clear cornea up to the limbus. Care should be taken that the punch faces downwards while punching and that the iris is pushed away with sufficient viscoelastic. The AC is then gently irrigated through the tunnel to wash away excess viscoelastic and the now punched and thereby compromised SIGS tunnel is checked for leakage by irrigating through the side port.
The end point is a free flow of fluid on irrigation. Additional punches towards the limbus are taken in case of inadequate leak. However, it is not extended beyond the limbus to avoid excessive leak and postoperative shallow AC. A peripheral iridectomy (PI) need not be done in cases of open angle glaucoma.
In cases with angle closure, peripheral anterior synechiae, shallow AC or cases showing tendency to intraoperative iris prolapse into the SIGS tunnel on irrigation, a PI is done by simply grasping the iris with a non-toothed forceps and cutting with a Vannas scissors. The single, small, 2.8mm conjunctival cut is then sutured with a running or figure-of-eight suture.
BSS is again injected through the side-port to cause physiological hydrostatic ballooning of the bleb. SIGS can also be combined with Mitomycin-C (MMC) by
dissecting the tunnel into lamellar cornea, applying intra-tunnel MMC, rinsing well and then entering the AC. Sub-conjunctival MMC is not required as there is no sub-conjunctival dissection in SIGS.
SIGS may also be combined easily with phaco by first making the SIGS stab incision, followed by phaco and IOL implantation. THE SIGS tunnel is self-sealing before it is intentionally compromised by punching it, hence it does not interfere with phaco in any way. The posterior corneal lip of the tunnel is punched before viscoelastic removal. Care should be taken to construct the SIGS incision at a site where it does not intersect with phaco incisions.
Advantages of SIGS include complete absence of sub-conjunctival dissection and thereby lesser risk of failure from scarring. Creation of the tunnel is easy and one step. Problems associated with flap tearing, laceration etc, that sometimes occur in trabeculectomy are done away with. Bleb elevation is by sub-conjunctival dissection via hydrostatic pressure of fluid from side port irrigation or from the I/A probe when combined with phaco rather than by scissor dissection as in other procedures, hence there is lesser chance of scarring. Virgin conjunctiva is maximised for any future procedures that may be required as compared to trabeculectomy and other procedures. It allows faster surgery, is less traumatic and may be combined easily with phaco or MMC if required. Surgery is easier and as conjunctival drainage channels are almost intact, trans-conjunctival absorption of aqueous is likely to be better.
n Dr Soosan Jacob is a senior consultant ophthalmologist at Dr Agarwal's Eye Hospital, Chennai, India and can be reached at: [email protected]
by Soosan Jacob
Advantages of Stab Incision Glaucoma Surgery include complete absence of sub-conjunctival dissection and thereby lesser risk of failure from scarring
SIGS AND GLAUCOMA SURGERY
EUROTIMES | Volume 19 | Issue 3
News
EyE ON tEChNOLOGy
A: The conjunctiva is slid forwards and a 2.8mm keratome used to create a single-step biplanar entry into the anterior chamber; B: The blade should be just visible through the conjunctiva to avoid premature entry into angle of AC; C: The blade is introduced to the full horizontal extent into the AC after dissecting into 1mm clear cornea; D: A Kelly’s Descemet’s punch (1mm) punches the posterior corneal lip up to the
limbus, thereby intentionally compromising the tunnel; E: Viscoelastic is washed away; F: Adequate leakage is checked for by irrigating through the side port; G: Conjunctiva is sutured and bleb is formed by more physiological hydrostatic ballooning from side port irrigation; H: Postoperative appearance; I: Slit view of ostium and bleb; J: ASOCT view of ostium, arrow shows flap
Scan this QR code to go to video link for surgery.

30
Residency is like a roller-coaster ride, with intense highs and dramatic lows. There are the short-term fluctuations, measured
in moments: making a correct diagnosis of a rare entity is fantastic; completing a successful operation makes you feel like you’re on the top of the world; a surgical complication makes you wonder what you’re doing there with a scalpel in your hand; and answer incorrectly to a supervisor’s question and you feel like you don’t belong. All of these things can happen within one day.
And then there are the long-term variations that are built into the rotations from one sub-specialty to the next. As each four-month rotation comes to a close, I have the feeling that I know what I am doing. I'm able to see patients without making people wait for an hour in the waiting room. The advice I seek from my supervisors becomes less frequent, and my questions sound more knowledgeable.
When assisting in the operating room, I feel like an asset, rather than a burden. During Grand Rounds, I take the time to research and present an interesting case or two and hopefully initiate a discussion on a tricky topic. I generally have the feeling that I have a certain understanding of the topic and overall, I'm feeling pretty good about my knowledge, my abilities and myself.
And when the rotation ends, this feeling of competence seems to spill over into the next rotation. Although I am aware of my limited knowledge of this new sub-specialty, I seem to view my expertise through a rosy mist of self-assurance generated during the previous rotation.
Glaucoma: Sure, no problem. What’s the IOP? Too high? Prescribe a drop and see the patient in three months.
Surgical retina: Simple! If the retina is detached, operate; if not, do nothing.
Medical retina: Is there bleeding? Oedema? Occlusion? Start up the laser and fire away, and if that does not work, inject anti-VEGF.
Cataract? That sounds too easy to discuss.
The right questions And then I step into the role of sub-specialist and realise that I know very little, at least in terms of practical, executive knowledge. I am back to page one. Sure, I have read the literature
and I know what the pathology should look like.
But successfully playing the role of sub-specialist is more than just knowing what is in the books. It involves asking the right questions, noticing subtle abnormalities and recognising variants of the norm. After the first half-day clinic, my confidence has been severely, and justifiably, diminished; any previously developed feelings of aptitude and even usefulness have totally disappeared.
And yet, in the clinic, residents are often the first doctors the patient sees. Their trusted general ophthalmologist, often a doctor who they have known for many
years, or even decades, has referred them. Those eye docs, some of whom started practising before I was even born, have in these cases decided that, with this particular patient, they have reached the limit of their own sub-specialty knowledge and need to entrust their patient to the care of a tertiary referral centre. And there I am, on the first week of my rotation, still trying to figure out what I need to know to come to some sort of an intelligent conclusion.
This feeling was particularly acute at the start of my glaucoma rotation. The glaucoma specialists each have about 25 years of experience. The fellows had been seeing exclusively glaucoma patients for
the past 12 months. And then there was me. I had read a book or two on glaucoma, treated a few cases of angle closure in the emergency room and referred many a patient with excavated optic discs to the glaucoma clinic. Needless to say, I felt under-qualified.
So, on my first day, with my first patient, I started out simply, with a family history.
The patient had been referred to the glaucoma clinic, but he evidently had not been told too many details:
I asked him, “Does anyone in your family have glaucoma?”
“Pardon?” Keep it simple, I thought. “Do any of your
relatives have eye disease?” “Yes, almost all of them.”OK, I though to myself, now we’re getting
somewhere. “Really?” I answer, “Which disease? What kind of problems do they have?”
“We all wear glasses. We’re practically blind without them.”
Oh no, I thought, back to square one. I had started a whole line of conversation that was clearly going nowhere. Time to backtrack. “Did they have to use eye drops?”
“No, not that I know of.”I moved on. I asked about his personal
history, according to what I had heard the glaucoma specialists ask patients, like whether they scuba-dive, play horn instruments, or regularly stand on their heads while practising yoga. That line of questioning, I later realised, makes patients wonder whether you’re serious or joking.
I moved on to more familiar territory: refraction, visual acuity, cornea, anterior chamber, iris, gonioscopy, lens and optic nerve. Other than a glaucomatous optic nerve, I found no abnormalities. Primary open-angle glaucoma, I wrote. Great, a first diagnosis!
I walked to the supervisor and presented my first case with confidence. At the end of my case presentation, he looked at me, expecting more. “That’s it,” I said.
“But what’s the IOP?” he asked. I practically disintegrated from
embarrassment. Just a week earlier I had been doing multiple solo strabismus operations per day. Now I had examined my first glaucoma patient and forgotten to measure the intraocular pressure.
The roller-coaster never stops.
by Leigh Spielberg
BACK TO PAGE ONEWelcome to the roller-coaster ride of residency
EUROTIMES | Volume 19 | Issue 3
Feature
REsIDENt’s DIARy
Illus
tratio
n by
Eoi
n Co
vene
y

31
rinco
n.de
www.geuder.Com
UNO COLORLINE MACH2 23 G*G-42302 – 1 pc. per box
G-46302 – 6 pcs. per box
*) fits Megatron/Megatron S3/Megatron S4
C o L o r L I N e
PERMANENtLy OPEN Fast core vitrectomy
CUtRAtEUp to 12,000 cpm
CONstANt FLOw Controlled and safe shaving
tHE NEw HIGH-sPEED vItREOUs CUttER MACH2
immediatelyavailable
DOUbLE-bLADELong lasting,excellent cuttingquality
RZ_Anz Mach2_Eurotimes_GB_120x300_02_2014.indd 1 04.02.14 08:47
Beyond our comfort zone The Seventh Edition of the “Neuro-Ophthalmology Review Manual” is a 250-page summary of neuro-ophthalmology, edited by Lanning B Kline and Rod Foroozan and published by Slack. Referred to in the introduction as a “readable compendium of ‘no-nonsense’ neuro-ophthalmology”, this text is a strong reference manual for learning and reviewing this subspecialty.
It seems that many ophthalmologists are less comfortable with neuro-ophthalmology than with most other fields of ophthalmology. We have to adopt an entirely different mindset and another set of tools to arrive at a diagnosis.
In terms of the mindset, we must look at the eye not as the seat of the disease, but as an indicator of what is wrong behind it. For most ophthalmic disease we can simply look inside the eye to make a diagnosis, as an auto mechanic would look under the hood and into the engine.
However, for neuro-ophthalmic disease, there is often nothing wrong within the eye itself. Instead, we must observe how the eye functions in terms of visual fields and motility. This is similar to the same mechanic being forced to watch a car drive from afar in order to determine what is wrong with it. The tools we need are not a slit lamp and an OCT, but rather a pocket lamp and our minds.
With this in mind, the book’s structure is simple and concise. As mentioned in the introduction, the book is written in a “clear and direct style in order to demystify but not oversimplify the core material of neuro-ophthalmology.” As such, the information is organised as a bulleted outline rather than as prose. This allows the reader to quickly find the topic at hand and review the most important points as efficiently as possible.
Chapter 1 starts with what seems to be among the most relevant topics for general ophthalmologists: visual fields. Because of the relative rarity of many neuro-ophthalmic visual field defects, the generalist frequently needs a refresher to get back up to speed, and this book provides it.
The next two chapters cover the supranuclear and internuclear gaze pathways and nystagmus and related ocular oscillations, starting with unambiguous definitions like, “Saccades: purpose is to shift gaze to a new location in the visual scene.”
Chapters 4, 5, 6, 12 and 13 cover the many syndromes of the abducens, oculomotor, trochlear, trigeminal and facial nerves,
complete with drawings of the relevant anatomy, syndrome etiology and several charts for use as diagnostic aids.
Specific syndromes Some chapters cover a single, very specific syndrome, such as Chapter 7: Cavernous Sinus Syndrome. Others tackle a broad topic, like Chapter 8: The Pupil. Particularly interesting are the chapters on the optic disc, whether swollen (Chapter 9) or pale (Chapter 10). These two signs each have a seemingly endless list of etiologies, and this text helps the reader organise his or her observational proficiency, diagnostic process and treatment options.
Other topics receiving full-chapter coverage are myasthenia and other ocular myopathies; eyelid disorders; headache; carotid artery disease and the eye; the phakomatoses; nonorganic visual disorders; and disorders of higher visual function.
The last chapter focuses exclusively on neuroimaging, with particular emphasis placed on the most appropriate imaging modality for each of the most common indications. The table titled “General Guidelines for Neuroimaging Studies Depending on Clinical Scenario,” is an especially useful guide for quick reference.
As an outline-structured review text, this book is appropriate for residents preparing for their neuro-ophthalmology rotation or studying for board exams. It is also a good resource for neuro-ophthalmology fellows who need to review and master the material and for general ophthalmologists.
EUROTIMES | Volume 19 | Issue 3
Feature
BOOk REVIEW
If you have a book you would like to have reviewed please send it to: EuroTimes, Temple House, Temple Road, Blackrock, Co Dublin, Ireland
BOOKS EDITORLeigh Spielberg
PUBLICATIONNEURO-OPHTHALMOLOGY REVIEW MANUAL
EDITORS IN CHIEFLanning B. Kline & Rod Foroozan
PUBLISHED BY SLACK INCORPORATED

32
Iconic buildings When old and new buildings vie for the snapshot – Westminster Abbey, Buckingham Palace, and 10 Downing Street finding new competition for celebrity status in London – London’s iconic buildings will always top the roster of “Things to see in London”.
But the city’s new skyscrapers are moving up to take their place on the list. These newer “celebrity buildings” challenge the perception of conservative London because celebrity buildings do not blend in.
They don’t meld into the ancient streetscapes. They have funny names and quirky stories and like other ‘celebrities’ defiantly stand out from the crowd.
Tours of these architectural newcomers can take almost four hours, if outlying areas such as Southwark are to be included. With only an hour to spare, though, I contacted Insider’s London, who assigned a young architecture buff named Tobias to organise
a tour covering many of the buildings I wanted to see. We met near Liverpool Street Underground station and were off on a mile-long hike from there to the river that took in six of the City of London’s most spectacular new structures.
Heron Tower The Heron Tower, at 110 Bishopsgate, is a 46-storey building designed by Kohn, Pedersen Fox and completed in 2011. Controversial because of its perceived proximity to St Paul’s Cathedral when viewed from Waterloo Bridge, a public inquiry was held which ruled in favour of the developer. Peek into the reception to see the largest private aquarium in the UK. Two attendants are charged with piscine health and safety while a team of part-time divers clean the rock work and glass regularly. On Bishopsgate, there’s an entrance to the Heron Building with lifts to a restaurant and sky bar.
Tower 42 Tower 42 or the former "Nat West Tower", on Old Bond Street, was designed by Richard Seifert. Noted for its vertical steel fins and black glass facade, it was the first skyscraper in the city when opened in 1980 by Queen Elizabeth. It attracted considerable opposition when opened and made headlines when severely damaged by an IRA bomb in 1993. Ultimately, the building was refurbished and sold by Nat West. Renamed Tower 42 it is now a general purpose office building. The tower features in the early sequences of The Hitchhiker’s Guide to the Galaxy and was used in the BBC-TV drama series, Sherlock. A bird study group tracks the migration of bird species over London from the tower’s roof.
The Gherkin The Gherkin, at 30 St Mary Axe, is officially known as the Swiss Re Building, but was nicknamed the "Gherkin" to mock its pickle shape. The nickname stuck as affection grew for this most celebrated of London’s new-look buildings. Completed in 2004, the 41-storey structure by Norman Foster rears up unabashedly behind a church built in 1532. The Gherkin is made up of flat glass panels. Only the "lens" at the top is curved. The base of the structure
is slightly indented, catching rainwater and channelling it inward. Entrances are reached over small bridges.
The Cheese Grater "The Cheese Grater," or officially the Leadenhall Building, is one architect's answer to a policy of the City of London Corporation known as the “St Paul’s Heights”. Since 1938, the policy has protected local views of St Paul’s Cathedral. Leadenhall’s wedge shape was architect Richard Rodger’s solution for preserving the view of the cathedral from Fleet Street. The chief planning officer of the City of London famously remarked that it looked like something you’d use for grating Parmesan cheese – and its name was born. To be completed in 2014, the building will feature a 30-metre high atrium, open to the public.
Lloyds Lloyds of London (1 Lime St.) is the Cheese Grater’s neighbour. Lloyds, the three-centuries-old insurance company, gave Richard Rodgers the brief for its new headquarters in 1980. The "Inside-Out" building was the result; all of its services – including staircases, lifts and water pipes – are located outside, giving tenants uncluttered interior space. The Lutine Bell, recovered from a ship wreck in 1858, hangs in the Rostrum. Traditionally it was rung once for the loss of a ship, twice for an overdue ship returning. Since 1989, having developed a crack, the bell has tolled only on Armistice Day, for the death of a member of the Royal Family or to commemorate a disaster like the Asian Tsunami.
Walkie-Talkie "Walkie-Talkie Tower," at 20 Fenchurch Street, was designed by Rafael Viñoly. The nickname derives from the building’s fancied resemblance to an old style walkie-talkie. However, in 2013 some journalists were calling it the "Walkie Scorchie" and others the "Fryscraper", after its concave south-facing facade focussed the sun’s rays down on the street, causing bits of a parked Jaguar to melt and setting fire to the paintwork of neighbouring buildings. To be completed in 2014, plans for the building’s top three storeys include a large viewing deck and sky garden, cafe and restaurant open to the public.
Plastic Building My guide, Tobias led us past the "Plastic Building", known formally as the Walbrook Building. From that vantage point, we had a distant view of the "Electric Razor", the residential Strata Tower that incorporates three wind generators on the roof and has been voted the "ugliest building in London". We then ducked into a passageway leading out to the Hanseatic Walk for a splendid view of the 72-storey "Shard" across the Thames. Designed by Renzo Piano, it is at this writing the tallest building in Europe.
by Maryalicia Post
Delegates attending the congresses in London next September can discover eight extraordinary structures in an hour’s walk in the city
CELEBRITY BUILDINGS
EUROTIMES | Volume 19 | Issue 3
Feature
EyE ON tRAVEL
As visitor interest in London’s modern architecture has grown, new tours have appeared. They include Insider London’s "Join In" modern architecture walking tours. The tours, which run 3-1/2 hours’ long, include a coffee break - begin at 10am on Sundays and at 1pm on Wednesdays. To book a place on a ‘Join-In’ tour or arrange a private tour at your own convenience, contact: www.insider-london.co.uk.
New tours
The Gherkin’s neighbour, St Andrew Undershaft, was built in 1532 Europe’s tallest building, The Shard Lloyd’s old entrance still stands

33Review
At the heart of EVA is a revolutionary fluid control system called VacuFlow VTi using Valve Timing intelligence technology. It just effortlessly delivers the precise flow and fast vacuum required by you, the surgeon.
Put simply, EVA VacuFlow VTi technology puts you in absolute control, all of the time.
109-1166 ADV-Masterpiece-120x300.indd 1 27-11-13 16:29
Costing the cataract learning curveTeaching residents cataract surgery is an expensive undertaking in terms of both time and money. US researchers sought to quantify theses costs in a comparative case series. They evaluated the differences in the time of completion of cataract surgery for nine residents and six attending surgeons.
The mean attending surgeon case time was 25.75 minutes ± 12.32 and the mean resident case time, 46.35 ± 16.75 minutes. Using a dollar cost of approximately $11.24 per minute at the institution, the cost difference was calculated to be $138,926.40 had both groups performed the same number (600) of procedures. They note that if the completion of a case for residents could be lowered on average by five minutes for 600 cases, the cost savings to our hospital would approach $33,720. The researchers posit that investments in time and money for classroom, wet lab and simulation instruction before allowing residents to perform surgery might reduce costs and prove to be cost effective.
n MJ Taravella et al., JCRS, “Time and cost of teaching cataract surgery”, Volume 40, Issue 2, 212-216.
Refractive surprises with toric IOLsRefractive cylinder surprises can occur after toric intraocular lens (IOL) implantation, even when state-of-the-art measurement devices and planning software are used. The orientation of the IOL must be considered in addition to the cylinder power and the spherical power of the IOL. Other factors include surgically induced astigmatism and ocular residual astigmatism. In an experimental study, Alpins and colleagues employed vergence formulas using a standard eye model to bring all lens powers to the corneal plane. Double-angle vector diagrams were then used to determine the refractive cylinder effect of rotating a toric IOL and show how the prevailing astigmatism and the various planning and surgical steps involved in implanting a toric IOL contribute to the postoperative manifest refractive cylinder. They demonstrate how to calculate the angle of rotation, which is the toric IOL rotation, to minimise the amount of manifest refractive cylinder in any eye using optimised lens constants to account for eye-specific and surgeon-specific factors that affect the equivalent power of the toric IOL at the corneal plane. They conclude that understanding the causes
of refractive surprise enables surgeons to address contributory factors and choose an appropriate surgical method for managing individual cases of refractive cylinder surprise.
n N Alpins et al., JCRS, “Refractive surprise after toric intraocular lens implantation: Graph analysis”, Volume 40, Issue 2, 283-294.
Multifocal IOL indicationsWhich cataract patients are most suitable for multifocal IOL implantation? Braga-Mele and colleagues reviewed preoperative diagnostic evaluations, patient selection criteria and counselling practices. The comprehensive US study concludes that appropriately selected patients can achieve spectacle independence and good visual outcomes at both near and distance with current multifocal IOLs. The selection process begins with proper patient education and individualised weighing of benefits and side-effects of multifocal IOLs. Given the high sensitivity of multifocal IOL function to minor ocular aberrations, preoperative clinical evaluation is crucial to postoperative success. While some patients will experience unsatisfactory outcomes due to issues that are unique to this class of IOLs, suitable postoperative management of both satisfied and dissatisfied patients will ultimately improve the visual benefits of these IOLs, they note.
n R Braga-Mele, et al., JCRS, “Multifocal intraocular lenses: Relative indications and contraindications for implantation”, Volume 40, Issue 2, 313-322.
FURTHER STUDYBecome a member of ESCRS to receive a copy of EuroTimes and JCRS journal
Thomas Kohnenassociate editor of jcrs
EUROTIMES | Volume 19 | Issue 3
JCRs hIGhLIGhtsJournal of Cataract and Refractive Surgery

ENHANCE YOUR EXPERIENCE IN BOSTON
FRIDAY, APRIL 25SEPARATE REGISTRATION IS REQUIRED
“An excellent overview of corneal innovations and challenges in anterior
segment surgery and disease management.”
“Glaucoma is among the leading causes of blindness; we should all be experts
in its diagnosis and treatment.”
This activity has been approved for AMA PRA category 1 credit.TM
This activity has been approved for AMA PRA category 1 credit.TM
Sponsored by the ASCRS Glaucoma Clinical Committee
GLAUCOMA DAYASCRS
2014
“Specialized training and leadership conditioning expands my career
opportunities.”
2014
These activities have been approved for COE credit.
www.ascrs.org www.asoa.org
SYMPOSIUM & CONGRESS
2014 APRIL 25–29B O S T O N

35Review
OPHTHALMOLOGICA
Become an ESCRS MemberIntegral to your continuing education
FREE TO MEMBERS:
ESCRS On Demand
iLearn – online CME accredited learning platform
In addition to:
Subscription to the Journal of Cataract and Refractive Surgery
Reduced ESCRS Congress Fees
ESCRS
FREE3 YEAR
MEMBERSHIP
FOR TRAINEES
visit www.escrs.org today
José Cunha-VazEDITOR OF OPHTHALMOLOGICA,The peer-reviewed journal of EURETINA
Spectral domain OCT reliable Spectral-domain optical coherence tomography (SD-OCT) appears to have a reliability comparable to that of fundus fluorescein angiography (FFA) in the diagnosis of choroidal neovascularisation (CNV) subtypes in neovascular AMD, according to the results of a retrospective, observational study. In 100 eyes initiated on ranibizumab for neovascular AMD, SD-OCT showed high sensitivity (85.7-98.3 per cent) and specificity (84.2-100 per cent) compared to FFA in the diagnosis of the CNV subtype. The area under the receiver-operating characteristic curve ranged from 0.9 to 0.93 (p value <0.0001) for the different CNV subtypes. Moreover, weighted kappa statistics showed a near-perfect agreement of 0.85 between the diagnostic procedures.
n Mathew R et al Ophthalmologica, “Correlation of Fundus Fluorescein Angiography and Spectral-Domain Optical Coherence Tomography in Identification of Membrane Subtypes in Neovascular Age-Related Macular Degeneration” (DOI:10.1159/000355091)
Implant shows sustained effectIntravitreal treatment with a dexamethasone implant (Ozurdex®) is safe and effective in the treatment of long-standing refractory DME, according to a retrospective study. A review of the medical records of 58 patients showed that, following injection of the implant, the mean BCVA improved baseline 0.66 to 0.52 logMAR (p = 0.0001) after one month, and 0.44 logMAR (p = 0.0001) after three months. At the six-month follow-up visit, the mean BCVA increased to 0.51 ± 0.31 logMAR (p = 0.0001). In addition, the reduction of mean foveal thickness compared to baseline was significant (p = 0.0001) at every follow-up visit. The mean foveal thickness decreased from a baseline value of 543.24 μm to 346.82 μm at one month, and to 341.12 29.64 μm at three months, but increased slightly to 420.16 μm at six months.
n M Dutra Medeiros et al, Ophthalmologica, “Dexamethasone Intravitreal Implant for Treatment of Patients with Persistent Diabetic Macular Edema” (DOI:10.1159/000356413)
Telemedicine screening for AMDNonmydriatic colour fundus photography and telemedicine is an effective means of screening for AMD, according to the results of a prospective study. The study involved 1,022 patients from whom a total of 1,363 color fundus photographs were obtained, without mydriasis, at a health examination centre and interpreted by telemedicine at an ophthalmology department. Eighty per cent of images were gradable and among these, 83.7 per cent had no AMD (grade 0), eight per cent had grade 1 AMD, 5.6 per cent had grade 2, 2.3 per cent were grade 3, and 0.4 per cent were grade 4.
n F De Bats et al Ophthalmologica, “Age-Related Macular Degeneration Screening Using a Nonmydriatic Digital Color Fundus Camera and Telemedicine” (DOI:10.1159/000356695).
PDT more effective in juxtafoveal myopic CNV In myopic CNV patients, photodynamic therapy (PDT) has limited long-term effect on subfoveal CNV but can achieve satisfactory results in eyes with juxtafoveal, according to a retrospective study. The 10-year analysis of PDT’s effect on 19 eyes with subfoveal and juxtafoveal CNV showed that during 10 years of follow-up mean BCVA progressively worsened, from 0.68 to 0.80, in seven eyes with subfoveal, but improved from 0.59 to 0.33 logMAR in 12 eyes with juxtafoveal CNV.
n M Varano et al, Ophthalmologica, “Photodynamic Therapy in Subfoveal and Juxtafoveal Myopic Choroidal Neovascularization: A 10-year Retrospective Analysis” (DOI:10.1159/000357504)
EUROTIMES | Volume 19 | Issue 3

SYMPOSIUM & CONGRESS
2014 APRIL 25–29B O S T O N
Additional Programming
Cornea DayASCRS Glaucoma Day
ASOA WorkshopsTechnicians & Nurses Program
REGISTER NOW
www.ascrs.orgwww.asoa.org
The Only U.S. Meeting Dedicated to the Anterior Segment Specialist
&The Leading Practice Management
Program in Ophthalmology
Follow @ASCRStweets on Twitter.#ASCRSASOA2014
AMER
ICAN
SOC
IETY O
F CATARACT AND REFRACTIVE SURGERY
Y E A R S
19742014

37
ShareLearn
Connect.
Join Us On Social Media
• Be sure to check out our social networking sitesand like or follow us to join the conversation
• Get real time access to the latest congress updates,society news and event information
• Our social media sites are a great way tocommunicate and share your congress experiences, connect with members of our team and others inthe ophthalmic community
www.facebook.com/ESCRSwww.facebook.com/eurotimesnews
@ESCRSoffi cial@eurotimestweets
www.linkedin.com/company/eurotimeswww.linkedin.com/company/escrs
Interact with the ESCRS
www.escrs.org www.eurotimes.org
Jim Taylor, president and CEO of Oraya Therapeutics, has seen first-hand how difficult repeated anti-VEGF injections can be on patients. Several years ago
his mother was diagnosed with neovascular age-related macular degeneration, and received over 25 intraocular injections.
“I know how difficult and unsustainable that is,” said Mr Taylor, who has 30 years of executive experience in medical technology.
His mother’s experience is one reason Mr Taylor, who was CEO at Carl Zeiss Meditec Inc at the time, got involved with Oraya. The firm’s targeted X-ray treatment approach held promise for reducing the frequency of injections needed to treat wet AMD.
That promise is now a reality. At the one year end point of a sham controlled trial, patients already undergoing anti-VEGF monotherapy who received a single treatment with the Oraya Therapy™ Stereotactic Radiotherapy device required 32 per cent fewer injections of ranibizumab to control their disease.
Perhaps just as significant, the trial helped identify a group of patients who may benefit even more from the X-ray therapy. Identified at one year through post-hoc analysis of the 230 trial participants in the INTREPID trial, these patients maintained vision with a 45 per cent mean reduction in injections over two years compared to anti-VEGF monotherapy. In addition, 23 per cent required zero injections in two years.
These “target group” patients all had significant fluid in the retina at baseline and lesion sizes of 4mm or less with minimal fibrosis or scarring. The fluid indicates the disease is in a proliferative phase, making it especially responsive to X-ray treatment, while the size allows the 4mm beam of the Oraya device to completely cover the lesion. About 60 to 70 per cent of wet AMD patients meet these criteria, suggesting that Oraya Therapy can be widely used, Mr Taylor said. At two years, just one per cent of patients showed micro-vascular changes that might have some effect on vision. An early look at three-year safety results also show that some of these micro-vascular changes resolved spontaneously, he added.
Commercial launch The Oraya Therapy device uses a highly collimated low-power X-ray to irradiate AMD lesions from several angles in a procedure that takes
about 20 minutes.The X-ray disrupts the proliferation of neovascular endothelial cells but spares surrounding tissue.
The successful trial means Oraya Therapy is ready for commercial use. Oraya systems are already up and running at private clinics in the UK, as well as in a clinic in Switzerland. The first commercial unit has been installed in Germany, with commitments of additional sites through 2014, Mr Taylor said. "Based on the potential to achieve equal or better vision outcomes at a reduced treatment burden, we have the support of some of the top retinal specialists in Germany,” Mr Taylor said. This will make it possible to apply for payment on a basis similar to how Lucentis is paid for in Germany. In the UK, 10 hospital trusts are considering adopting Oraya Therapy.
Oraya Therapy is an obvious addition to the wet AMD treatment paradigm. It’s priced so that it saves money on the overall cost of care, including anti-VEGF agents, staff time and facilities and equipment costs.
“This is all made possible by the two-year data. People can see two years of efficacy and cost-benefit data, and we have early three-year safety data. Now it is a matter of doing the hard work of making the technology available for the patient,” Mr Taylor said. “I only wish it had been available when my mother was diagnosed.”
by Howard Larkin
Successful two-year trial boosts radiation as adjunct for wet AMD disease
ORAYA FOR AMD
EUROTIMES | Volume 19 | Issue 3
Feature
OUtLOOk ON INDUstRy
IRay® Radiotherapy Device for Oraya Therapy Treatments
Jackie Ferreira – [email protected]
contact

Save the DateFriday, April 25 –Monday, April 28, 2014Make the most of your time at theASCRS•ASOA Symposium & Congress andattend our EyeWorld programs for additionalCME and an opportunity to network withyour colleagues.
Visit www.EyeWorld.org for more details.
BOSTON 2014
Among the topics to be covered in these AMA PRA Category 1 CreditsTM designated sessions are:
• A discussion on recent developments in anti-infective and anti-inflammatory therapeutic treatments
• Updates on diagnosing and treating the ocular surface, including dry eye disease
• New developments in allergy therapeutics• New considerations and continuing discussions
regarding laser-assisted cataract refractive surgery• Maximizing outcomes with refractive IOLs• Update on the prevalence and alternative treatment
for meibomian gland disease• Generic vs. brand therapeutics: a discussion on the
risks and benefits
These non-CME, ASCRS-authorized educational programs will provide timely andimportant information on:
• Options and considerations in the use of premiumIOLs
• Advances in technologies, techniques, and outcomes in laser vision correction surgery
• An interactive discussion on the applications offemtosecond and excimer lasers for ophthalmic surgery
• Micro-invasive glaucoma surgery (MIGS),bridging basic science with clinical application
Topics are subject to change.
Ew event ad - March Ad ASCRS Auth and CME-DL_Layout 1 2/10/14 11:15 AM Page 1

39
THE PRESBYOPIA SOLUTION THEY’VE BEEN WAITING FOR.
Across the page.
Across the room.
Across the years.
20/200
20/125
20/80
20/50
20/32
20/20
20/12.5
0 10 20 30 40 50 60
SNEL
LEN
ACUI
TY
MONTH
UNCORRECTED NEAR VISUAL ACUITY (INLAY EYE ONLY)*
INLAY EYE
J2
LOSS OVER TIME IN EYE WITHOUT INLAY
Mean near acuity improved 3.2 lines to 20/25 at 1 month and was maintained over the 5 year follow-up.
* Data presented by Prof. Dr. Günther Grabner at the 2013 DOC in Nuremberg, Germany.
KAMRA; the KAMRA logo; Across the page. Across the room. Across the years; and The Presbyopia Solution are trademarks of AcuFocus, Inc. ©2014 AcuFocus, Inc. CE Mark since 2005.
The KAMRA inlay is an investigational device in the United States. It is limited by United States federal law to investigational use. All rights reserved. MK-1158 Rev A
The KAMRA™ inlay provides a full range of vision and long-term performance, while leaving the
natural lens in place.
Silicone bandage lensGeuder and LensWista have agreed on a sales cooperation for the first bandage lens from pure silicone.
"The fields of application of the bandage lens are corneal injuries, PK, LASIK, crosslinking and recurrent corneal erosion," said a company spokeswoman. "Due to its eight times higher oxygen permeability compared to conventional contact lenses, this special contact lens from biocompatible pure silicone contributes to fast wound healing and significant pain relief. The innovative surface technology gives the lens a maximum and durable hydrophility," she said.n www.geuder.com
EUROTIMES | Volume 19 | Issue 3
Feature
INDUstRy NEWsRecent developments in the vision care industry
Combination laser platformQuantel Medical has received CE Mark approval for its Optimis Fusion integrated laser platform. “The Fusion system combines advanced selective laser trabeculoplasty (SLT) photoregeneration therapy and traditional YAG photodisruption treatments to offer ophthalmologists a versatile armamentarium for treating both cataract and glaucoma. Quantel will immediately begin commercialisation in all CE Mark-approved countries,” said a company spokesman.n www.quantel-medical.com
Small incision lenticule extractionThe SMILE procedure developed by Carl Zeiss Meditec for refractive surgery stands for Small Incision Lenticule Extraction. Zeiss says the procedure combines state-of-the-art femtosecond laser technology and precise lenticule extraction providing a micro-invasive laser vision correction method. Unlike LASIK, in which an excimer laser ablates tissue inside the cornea after opening the corneal surface by cutting a corneal flap, the SMILE procedure is performed without a flap. The ZEISS femtosecond laser VisuMax® is used to create a very thin disc of tissue (lenticule) inside the intact cornea, which can then be extracted through a small incision. An excimer laser is not required, according to the company.
“With SMILE, ophthalmic surgeons now for the first time have a refractive surgery procedure that provides great benefits for their patients with the least possible intervention: the cornea of the eye remains intact as much as possible; the predictability of the correction is very good,” says Ludwin Monz, president and CEO of Carl Zeiss Meditec AG.nwww.meditec.zeiss.com
Exclusive agreementNicox SA and Sequenom, Inc have announced that their affiliate companies Nicox Inc. and Sequenom Laboratories have entered into an exclusive agreement in the AMD field. “As part of this agreement, Nicox has been granted the North American promotional rights to the Sequenom Laboratories RetnaGene(TM) AMD laboratory-developed test, for the evaluation of a patient’s risk of AMD disease progression within two, five and 10 years,” said a company spokeswoman. n www.nicox.com

Reference
CALENDAR OF EVENtsDates for your Diary
2014
40
MARCH Frankfurt Retina Meeting 201415-16 MarchFrankfurt, Germanywww.eckardt-frankfurt.de
Th e 5th World Congress on Controversies in Ophthalmology (COPHy)20-23 MarchLisbon, Portugalhttp://www.comtecmed.com/cophy
APRIL XIII International Congress of Cataract and Refractive Surgery 2-5 AprilRio de Janeiro, Brazilhttp://www.cataratarefrativa2014.com.br/
World Ophthalmology Congress2-6 AprilTokyo, Japanwww.woc2014.org
International Symposium on Cornea: Clinical Approach11 AprilBelgrade, Serbiawww.cornea-belgrade2014.org
ASCRS•ASOA Symposium and Congress25-29 AprilBoston, USAwww.ascrs.org
MAY ARVO4–8 MayOrlando, Florida, USAwww.arvo.org
SOI International Congress21-24 MayMilan, Italywww.congressisoi.com
JUNE 11th EGS Congress7-11 June Nice, Francehttp://www.eugs.org/eng/default.asp
AUGUST Nordic Congress of Ophthalmology (NOK 2014)20-23 AugustStockholm, Swedenhttp://www.nok2014.se/Default.aspx
SEPTEMBER 14th EURETINA Congress11-14 SeptemberLondon, UKwww.euretina.org
SEPTEMBER ESCRS Glaucoma Day12 SeptemberLondon, UKwww.escrs.org
WSPOS Paediatric Sub Speciality Day12 SeptemberLondon, UKwww.wspos.org
5th EuCornea Congress12-13 SeptemberLondon, UKwww.eucornea.org
XXXII Congress of the ESCRS13-17 SeptemberLondon, UKwww.escrs.org
International Annual Course and Workshop on Diagnostic Ultrasound in Ophthalmology22-26 SeptemberVienna, Austriawww.echography.com
Th e 112th DOG Congress of Ophthalmology25-28 SeptemberLeipzig, Germanywww.dog-kongress.org
SEPTEMBER 2nd Asia-Pacifi c Glaucoma Congress10th International Symposium of Ophthalmology 26-28 SeptemberHong Konghttp://www.apgc-isohk-2014.org/
OCTOBER AAO Annual Meeting18-21 OctoberChicago, Illinois, USAwww.aao.org
NOVEMBER NEW ENTRYFemto Congress 20147-9 NovemberBudapest, Hungarywww.femtocongress2014.hu
SOI National Congress12-15 NovemberRome, Italywww.congressisoi.com
27th APACRS Annual Meeting13-16 NovemberJaipur, Indiawww.apacrs2014.org
If you would like to see your classifi ed ad here, please contact Mairin Condon: [email protected].
Advertising Directory: AcuFocus: Page: 39; Alcon: Page: OBC; A.R.C Laser: Page: 19; ASCRS/Eyeworld: Pages: 34, 36, 38; Croma-Pharma GmbH: Page: 5; D.O.R.C. International BV: Page: 33; ESASO: Page: 28; Femto Congress 2014: Page: 14; Geuder: Page: 31; Innovative Excimer Solutions: Page: 3; Medicel Ag: Page: 40; Nidek: Page: 17; Oculus Optikgerate GmbH: Page: 13; Oertli Instruments AG: Page: IFC; Rayner Intraocular Lenses Ltd: Page: 9; VSY Biotechnology: Page: 11
New engineered Biofi lmTM Coating
provides outstanding Benefi ts to enable
safe and effective Injection of Premium IOLS.
• enables an incision size as small as
subMICS 1.5 mm
• no additive transfer
• no lens scratches
• no splitting cartridges
• for hydrophilic and hydrophobic IOLs
State-of-the-Art

London2014
XXXII Congress of the ESCRS
13-17 September
www.escrs.org
Free paper, poster and videoabstracts submission deadline:
15 March 2014

Welcome to the new possible.
It’s time to rewrite the rules of vitreoretinal surgery.
• The ULTRAVIT® 7500cpm probe provides the benefi t of faster cutting and smaller vitreous biteswithout fl uidic compromise.1
• Trust in integrated and stable IOP compensation2
• Enhance patient outcomes and achieve faster visual recovery with ALCON® MIVS platforms3
• Increase effi ciency during cataract removal with OZil® Torsional Handpiece4, 6
• Improve your OR set up time by 36% with V-LOCITY® Effi ciency Components5
smaller vitreous bites
In 1968, Dick Fosbury revolutionized the high jump by developing a technique that elevated him to Olympic gold, raising the bar for athletes the world over.
Game Changer
EuroTimes 3/14
© 2013 Novartis 9/13 CON13032JAD-EU
*ULTRAVIT® 7500 Vitrectomy Probe
1. Abulon, et al. Porcine Vitreous Flow Behavior During High Speed Vitrectomy up to 7500 Cuts Per Minute. ARVO Poster, 2012. 2. Claes, et al. Clinical and laboratory evaluation of valved cannulas. EVRS Presentation, 2010. 3. Nagpal M, et al. Comparison of clinical outcomes and wound dynamics of sclerotomy ports of 20, 25, and 23 gauge vitrectomy. Retina. 2009;29(2):225-231. 4. Davison JA, Cumulative tip travel and implied follow ability of longitudinal and torsional phacoemulsifi cation J Cataract Refract Surg 2008; 34:986–990 5. Alcon data on fi le 954-0000-004. 6. Fernández de Castro, L. E. et al. (2010). Bead-fl ow pattern: Quantization of fl uid movement during torsional and longitudinal phacoemulsifi cation. J Cataract Refract Surg 36(6): 1018-1023.
CON13032JAD-EU ET.indd 1 2/6/14 9:16 AM