EuroTimes Vol 19. - Issue 10
48
SPECIAL FOCUS PAEDIATRIC OPHTHALMOLOGY GLAUCOMA CONTINUOUS IOP MONITORING FOR 24 HOURS CLOSE TO BECOMING A REALITY EYE ON TECHNOLOGY NEW TECHNIQUE COULD OVERCOME LIMITATIONS OF TRADITIONAL CROSS-LINKING October 2014 | Vol 19 Issue 10 Through Through a Child’s Eye a Child’s Eye
description
A European Outlook on the World of Ophthalmology
Transcript of EuroTimes Vol 19. - Issue 10

SPECIAL FOCUSPAEDIATRIC OPHTHALMOLOGY
GLAUCOMACONTINUOUS IOP MONITORING FOR
24 HOURS CLOSE TO BECOMING A REALITY
EYE ON TECHNOLOGYNEW TECHNIQUE COULD OVERCOME
LIMITATIONS OF TRADITIONAL CROSS-LINKINGOctober 2014 | Vol 19 Issue 10
ThroughThrougha Child’s Eyea Child’s Eye

The Essence of Perfection
When the best engineers and designers give their best, they are bound to develop the best machine. “We have redefined the concept of the operating platform for cataract, glaucoma and retina surgery. The OS4 includes everything we are good at: cutting-edge technology, perfect design, irresistible simplicity, the highest degree of safety and Swiss quality. In short: 100 percent Oertli®.“
From 18 to 21 October 2014, the OS4 will see its world premiere at the AAO in Chicago. At our booth no. 3416, we will have the pleasure of showing you all the details of the device, which will provide you with clear added value.Ec
knau
er+
Sch
och
ASW

Publisher Carol Fitzpatrick
Executive Editor Colin Kerr
Editors Sean Henahan Paul McGinn
Managing Editor Caroline Brick
Production Editor Angela Sweetman
Senior Designer Janice Robb
Designer Lara Fitzgibbon
Circulation Manager Angela Morrissey
Contributing Editors Howard Larkin Dermot McGrath Roibeard Ó hÉineacháin
Contributors Maryalicia Post Leigh Spielberg Pippa Wysong Gearóid Tuohy Priscilla LynchSoosan Jacob
Colour and Print W&G Baird Printers
Advertising Sales Amy BartlettESCRSTel: 353 1 209 1100email: [email protected]
Published by the European Society of Cataract and Refractive Surgeons, Temple House, Temple Road, Blackrock, Co Dublin, Ireland. No part of this publication may be reproduced without the permission of the managing editor. Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review and acceptance.
ESCRS EuroTimes is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS EuroTimes.ISSN 1393-8983
As certified by ABC, the EuroTimes average net circulation for the 10 issues distributed between 01 January 2013 and 31 December 2013 is 40,878.
P.36
P.6
P.43
SPECIAL FOCUSPAEDIATRIC OPHTHALMOLOGY4 Cover Story: Paediatric
patients beginning to reap the benefits of biological science advances
8 New technique could offer several advantages over existing methods
10 Study highlights effect negative attitudes can have on blind children
11 High levels of patient satisfaction found with refined suture technique
12 Good results found with imaging technologies adapted for children
FEATURESCATARACT & REFRACTIVE14 Survey of French
ophthalmologists reports interesting findings
16 Expert says phaco is still ‘gold standard of cataract surgery’
17 Femtosecond laser beneficial in challenging cases
CORNEA19 Symblepharon patients
successfully treated with novel approach
20 Should ophthalmic terms have one precise meaning?
25 Femtosecond laser proving useful for keratoplasty procedures
MEETING REPORT21 News and updates from
London 2014 congresses
GLAUCOMA28 Diagnosing
glaucomatous disease may soon become easier
29 New devices look to provide continual 24-hour IOP monitoring
31 Disc haemorrhages may be an indication for more aggressive treatment
RETINA32 Study highlights
importance of holistic approach when treating AMD patients
33 Book on cell-based ocular therapy should interest broad audience of readers
REGULARS35 JCRS update
36 Industry News
38 Travel
39 Book Reviews
40 Eye on Technology
43 Resident’s Diary
44 Calendar
EUROTIMES | OCTOBER 2014
CONTENTS™
Cover image shows a child with congenital cataract in the right eye.Photographer: Mr S B N Chary, L V Prasad Eye Institute.

2 EDITORIAL
MEDICAL EDITORS
INTERNATIONAL EDITORIAL BOARD Noel Alpins (Australia), Bekir Aslan (Turkey), Bill Aylward (UK), Peter Barry (Ireland), Roberto Bellucci (Italy), Béatrice Cochener (France), Hiroko Bissen-Miyajima (Japan), John Chang (China), Alaa El Danasoury (Saudi Arabia), Oliver Findl (Austria), I Howard Fine (USA), Jack Holladay (USA) , Vikentia Katsanevaki (Greece), Thomas Kohnen (Germany), Anastasios Konstas (Greece), Dennis Lam (Hong Kong), Boris Malyugin (Russia), Marguerite McDonald (USA), Cyres Mehta (India), Thomas Neuhann (Germany), Rudy Nuijts (The Netherlands), Gisbert Richard (Germany), Robert Stegmann (South Africa), Ulf Stenevi (Sweden), Emrullah Tasindi (Turkey), Marie-Jose Tassignon (Belgium), Manfred Tetz (Germany), Carlo Enrico Traverso (Italy), Roberto Zaldivar (Argentina), Oliver Zeitz (Germany)
José GüellEmanuel Rosen Chief Medical Editor Clive PeckarIoannis Pallikaris Paul Rosen
EUROTIMES | OCTOBER 2014
A subject close to my heart is the aRc genetic educators’ course which has helped the L V Prasad Eye Institute Network
WSPOS Sub Specialty Day in London is a big success
These are exciting times for paediatric eye surgeons and I am delighted to have the opportunity to write this editorial for EuroTimes.
This month’s Special Focus is Paediatric Ophthalmology and we have a number of very interesting stories.
The Cover Story discusses the revolution in biological science that began around the middle of the last century, which has transformed the study of genetic eye diseases from being a matter of family trees and relatively crude assays to one of DNA analysis and genotyping and detailed biomolecular analysis.
The World Society of Paediatric Ophthalmology and Strabismus (WSPOS) Sub Specialty Day took place on Friday 12 September, preceding the XXXII Congress of the ESCRS, and was a great success. The theme for this meeting was “A Day With A Child’s Eye” and during the meeting key opinion leaders from all over the world discussed topics including systemic implications of paediatric eye disease, international collaborations in paediatric cataract outcomes, interesting video presentations and ocular motor disorders.
In this issue we look at some of the presentations from the meeting including a study from Prof Clare Gilbert which shows that the negative attitudes of others and lack of support are among the most disabling factors faced by children who are blind in developing countries.
Dr David Granet also reported that the choice of using a closed conjunctival delayed approach to adjustable suture surgery may present some significant advantages to more traditional adjustable suture techniques in the treatment of strabismus.
I was also very interested in the article in this issue where Dr Daniel Mojon discusses how a new minimally invasive strabismus surgery (MISS) technique for rectus and oblique muscle surgery offers a safe, effective means of performing muscle surgery through a smaller conjunctival incision.
So what else is new at WSPOS? Our next major meeting is the 3rd World Congress of Paediatric Ophthalmology and Strabismus in Barcelona, Spain from 4-6 September 2015, but we also have a number of other exciting activities to focus on.
A subject close to my heart is the aRc (areas of Research collaboration) genetic educators’ course which has helped the L V Prasad Eye Institute Network. The genetic educators’ course (as a part of WSPOS aRc) helped us to train eight optometrists across the L V Prasad Eye Institute Network, ie, Hyderabad, Vijayawada, Vizag and Bhubaneshwar. The trained optometrists are helping in collecting a detailed pedigree of patients in our busy and high-volume clinics.
In addition, they are helping in training other junior optometrists collect adequate information. This is helping clinicians to categorise patients and direct them for further
tests with their genetic profile. We are thankful to the Genetic Counselling Team of the Children's hospital, UPMC for their continued support to help our patients.
Information on this and other activities is included in the WSPOS newsletter which was sent to members in August. I am pleased to announce that this electronic
newsletter will be published four times a year, and will include regular updates on all WSPOS activities and also other news of interest to members.
I would also encourage paediatric eye surgeons to visit our website at: www.wspos.org.
A WORD FROM RAMESH KEKUNNAYA MD, FRCS
THE CHILD'S EYE
* Ramesh Kekunnaya MD, FRCS, head of pediatric ophthalmology, strabismus & neuro-ophthalmology, Jasti V Ramanamma Children’s Eye Care Center, L V Prasad Eye Institute (LVPEI), Hyderabad, India

1. Data on File, Dec 2013 © 2014 Novartis 2/14 ACR14008JADi EU
EuroTimes 10/14
He trained you to be the best ophthalmologist you can be
And he chose you to perform his cataract surgery
That’s success story 75 million and one1
CONFIDENCE
87500 ACR14008JADi EU ET.indd 1 9/23/14 10:38 AM

4
revolution in biological science that began around the middle of the last century has transformed the study of ocular pathology from being a matter
of family trees and relatively crude assays to one of DNA analysis and genotyping and detailed bimolecular analysis. However, it wasn’t until this century that these advances had made inroads into ophthalmic medicine and it is only very recently that paediatric ophthalmic patients are beginning to reap the benefits.
Among the newer treatments introduced into paediatric practice in recent years is the use of intravitreal anti-vascular endothelial growth factor (anti-VEGF) agents in infants with retinopathy of
A
EUROTIMES | OCTOBER 2014
process by inactivating VEGF both in the peripheral retina and in the vitreous.
The laser’s advantages include its well-established efficacy and safety, proved through the decades of experience. The laser’s main disadvantage is that if the retinopathy affects a very small area of the posterior retina, as in zone 1 disease, the patient can end up with significant visual field defects and with significant high myopia.
The advantages of anti-VEGF therapy include the preservation of the visual field, minimising the amount of myopia, especially high myopia (Gelonic et al, JAMA Ophthalmol, epub Aug 7, 2014 and Chen et al, Eye, epub Aug 8, 2014), the simplicity of its administration and the lack of any requirement for expensive laser equipment or expertise in the use of these
prematurity (ROP). A product of decades of research into angiogenesis initiated by Judah Folkman in the 1970s, the agents appear to perform significantly better than laser in terms of recurrence when the retinopathy occurs in zone 1, the small posterior part of the retina surrounding the optic nerve.
Laser treatment, the current gold-standard for ROP, like its predecessor cryoablation, is itself, in a sense, an anti-VEGF treatment. It suppresses the production of VEGF by destroying the peripheral ischaemic retinal tissue that secretes the growth factor, but does not effect the VEGF that has been secreted into the vitreous. Intravitreal anti-VEGF has a more immediate effect in that it directly inhibits VEGF temporarily shutting down the vascularisation
Huge scientific strides leading to baby steps in paediatric ophthalmology. Roibeard O'hEineachain reports
BIO-TECH ADVANCES
COVER STORY: PAEDIATRIC OPHTHALMOLOGY

5
EUROTIMES | OCTOBER 2014
or improperly (causing trauma to the lens, retina, etc, or introducing infection), and no systemic complications.
“Thousands of injections for ROP have been given worldwide and no complications in actual human pre-term infants have been reported – only extrapolations and speculations from in vitro retinal cells and in laboratory animals with different doses etc. Specifically the brain, lung, liver etc, develop normally despite anti-VEGF entering the systemic circulation,” she said.
Therefore, ranibizumab is unlikely to have any real safety benefit over bevacizumab. In addition, bevacizumab is much less expensive and is available in almost any hospital that treats cancer patients, she pointed out.
She added that the primary drawback to anti-VEGF treatment for ROP is the longer time required for monitoring for ROP recurrences. She and her associates are preparing another paper that will discuss the risk factors for recurrence, the timing and appearance of recurrence in ROP Stage 3+ and in APROP and suggest a recurrence follow-up schedule.
GENE THERAPYGene therapy in paediatric eye disease has picked up pace since the publication in 2008 of three trials that confirmed that gene therapy can increase cone sensitivity in eyes of young adults with Leber’s
Helen Mintz-Hittner MD a co-author of the BEAT-ROP study told EuroTimes that when considering the risks of anti-VEGF in ROP the considerable benefits in terms of preservation of the peripheral retina (visual field enlarged) and allowing the development of the anterior segment (myopia decreased) should not be ignored.
“In severe ROP cases, especially in zone 1, bevacizumab patients develop better visual function ultimately. The destruction of the peripheral retina does not allow it to function. Thus, a restricted visual field develops. Further, the destruction of the peripheral retina that would occur with laser treatment in such severe cases does not allow the development of a normal anterior segment. Thus, high myopia develops. Additionally, laser causes cystoid macular oedema that does not resolve without impacting function. Thus, imperfect visual acuity develops,” she said.
She added that the signs are pretty good so far regarding long-term ocular and systemic side effects of bevacizumab unless the drug is administered prior to the development of Type 1 ROP preventing normal retinal development, especially of the macula (Lepore et al, Ophthalmology, epub, July 4, 2014). Since 2006, when intravitreal bevacizumab was first used for ROP, there have been no reports of local complications, except when injection is performed too early (before Type 1 ROP)
lasers. The disadvantage of intravitreal anti-VEGF therapy is that there is not yet sufficient data in the published literature to establish the ideal indication, the optimal dosage, or the treatment’s long-term efficacy and long-term safety. Moreover, when recurrences occur after anti-VEGF therapy they tend to occur later than they do after laser treatment. That means that patients need close monitoring for a longer time than is the case with laser therapy.
BEAT-ROPThe BEAT-ROP study is among the most informative of the published studies. It showed that the rate of recurrence for all degrees of ROP Stage 3+ and aggressive posterior ROP in zone I and posterior zone II combined was significantly higher with conventional laser therapy (26 per cent) than it was with intravitreal bevacizumab (six per cent). The mean time to recurrence was 16 weeks following intravitreal bevacizumab therapy, compared with six weeks following conventional laser therapy (Mintz-Hittner et al, N Engl J Med 2011; 364:603-615).
In an interview with EuroTimes, Tim U Krohne MD, FEBO, of University Eye Hospital Bonn, Germany, said that important limitations of the BEAT-ROP study were its short follow-up of only 54 weeks of post-menstrual age and therefore the lack of data regarding late recurrences or complications and functional outcomes. He added that the German ophthalmological and retinal societies are currently recommending restricting the use of intravitreal anti-VEGF therapy for ROP to infants with zone 1 disease and using laser for the more peripheral cases until further data is available.
“The reason is we currently simply don't know what the systemic side effects of the treatment might be. But the drug obviously does leak out of the eye into the systemic circulation and studies show that there is systemic suppression of systemic VEGF activity for weeks in infants who have undergone intravitreal injection of bevacizumab. In contrast to adults, premature babies are still in the process of development, and several organs such as the lung and the brain are known to require VEGF for proper development,” said Dr Krohne.
Dr Krohne added that ranibizumab may have safety advantages in ROP because bevacizumab accumulates to a significantly higher degree in the systemic circulation than is the case with ranibizumab, according to pharmacokinetic research conducted by several teams including his own. This significant difference is illustrated by the systemic half-life of ranibizumab which is only about two hours while that of bevacizumab is about 20 days. A German prospective multicentre trial to investigate the clinical effect of ranibizumab in ROP is ongoing (clinicaltrials.gov: NCT02134457).
COVER STORY: PAEDIATRIC OPHTHALMOLOGY
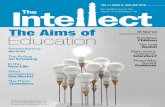
Before and after photographs of the right eye of an infant (whose birth weight was 495 grams and gestational age was 24 weeks). He was treated with bevacizumab mono-therapy at age 2 ½ months (10 weeks) = A; and followed regularly to age 11 months (48 weeks) = B
In contrast to adults, premature babies are still in the process of development, and several organs such as the lung and the brain are known to require VEGF for proper developmentTim U Krohne MD, FEBO
Cour
tesy
of H
elen
Min
tz-Hi
ttner
MD
Thousands of injections for ROP have been given worldwide and no complications in actual human pre-term infants have been reported...Helen Mintz-Hittner MD
A B

6
hereditary retinal disorders. A phase I/IIa study of gene therapy for Stargardt’s Macular Degeneration is currently recruiting patients. In addition, Dr Ali and his associates have approval, for instance, to start a trial for achromatopsia, a macular disorder.
Future developments may include viral vectors that are effective in the retina when injected intravitreally rather than beneath the retina. The exciting possibilities of gene editing may also play an important role in gene therapy in the future. Gene editing involves the use of CRISPR/Cas9 enzyme to replace a bad gene with a good one right in the chromosome where it belongs.
“That would be the ultimate, because you would not have to worry about getting the right levels of expression as you would have appropriate functioning of the corrected gene. I think that might be the future,” Dr Ali said.
Tim U Krohne: [email protected] A Mintz-Hittner: [email protected] Robin Ali: [email protected]
results so far appear to agree with the findings obtained in animal models of the disease that earlier treatment yields better visual outcomes.
“We have not yet published on children – we are about to write up our findings – but we have enrolled eight children in our trial, some as young as five and they received the adeno-associated virus vector. And we've seen improvements in their retinal sensitivity,” Dr Ali said.
He noted that the different centres carrying out the LCA2 gene therapy trials have used slightly different variants of the adeno-associated virus vector and have also used different promoters to promote expression of the gene in the target cells.
He added that he and his associates are planning a second trial, with a new, optimised AAV vector and promoter in the hopes that by enhancing delivery and expression of the gene they may also be able to prevent the retinal degeneration.
Meanwhile, research is continuing at numerous centres around the world on gene therapy for the other types of LCA and other
congenital amaurosis type 2 (LCA2) (Bainbridge JW et al. N Engl J Med 2008; 358: 2231-2239; Hauswirth WW et al. Hum Gene Ther 2008; 19: 979-990; Maguire AM et al. N Engl J Med 2008; 358: 2240-2248).
Up until now, the published trials have been mainly restricted to adult patients in whom the retina has already degenerated, with a considerable and irreversible loss of photoreceptor cells. Moreover, the disease continues to progress in patients who receive gene therapy.
Better results are likely to be achieved in younger patients, who still retain the bulk of their photoreceptors, and who therefore have a greater potential for visual gains and who may also be less prone to retinal degeneration following treatment, said Robin Ali PhD, Moorfields Eye Hospital and University College London, UK, a co-author of one of the first gene therapy trials for LCA2.
“The key to the most effective treatment will always be to treat as early as possible. And that's what we see in all our animal studies where we have genetic models of disease. The earlier we treat, the better the outcome,” he said.
He noted that there are about 15 types of LCA. All are caused by autosomal recessive mutations and they share the characteristic of an absence of, or a severe reduction in, retinal function at birth that is followed by a degeneration of the photoreceptors.
In some types of LCA there are defects in rod function, in others there are defects in both rod and cone function. In the case of LCA2, there is a complete absence of rod function from birth. The disease is caused by defects in the gene for RPE65, a retinoid isomerase expressed in the retinal pigment epithelium. RPE65 plays a critical role in the regeneration of the 11-cis retinal chromophore in the visual cycle.
Patients with LCA2 have problems with night vision and peripheral vision, but pretty good central vision conditions to start with. But then, when patients are about eight or nine years old – and for reasons as yet not fully understood but probably related to the lack of function – the rod photoreceptors begin to die. As the retinal degeneration continues the cones start to die and central vision deteriorates.
On the basis of the results achieved in the first trials – all of which indicated patients receiving the therapy achieved some visual and quality-of-life benefits – investigators are beginning to carry out gene therapy in paediatric patients with LCA2 and the
COVER STORY: PAEDIATRIC OPHTHALMOLOGY
Retina from a mouse deficient in the gene AIPL1, treated with gene therapy using an AAV8 viral vector carrying AIPL1 (green) which ensures that the protein PDE6b (red) localises to the correct part of the retina. In humans, deficiencies in AIPL1 causes Leber Congenital
Amaurosis type 4 (LCA4), a particularly rare and severe form of inherited childhood blindness. (Image by Dr Alexander Smith, PhD.)
The key to the most effective treatment will always be to treat as early as possibleRobin Ali PhD
TürkiyeTURKISH LANGUAGE EDITION ONLINE
Visit: www.eurotimesturkey.org
Cour
tesy
of U
CL
EUROTIMES | OCTOBER 2014

19TH ESCRSWINTER MEETING
www.escrs.org
20 – 22 February 2015Hilton Istanbul, Turkey
ISTANBULIn conjunction with
Turkish Ophthalmology Society Cataract & Refractive Surgery Section
Abstract Submission Deadline 31 October 2014
Registration Opens 1 November 2014

8
even repeat surgery is less visible than primary surgery – that is how minimally invasive it is,” he said.
RADIAL CUTSExplaining the technique for recessing a horizontal muscle in more detail, Dr Mojon said that muscle exposure is performed, as usual for MISS, through two radial cuts, one along the superior and the other along the inferior margin of the horizontal muscles. After muscle separation from surrounding tissue and hooking, the suture is passed between sclera and muscle for 2mm and then passed through the muscle and the conjunctiva. Now, the suture is retrieved in the space between the conjunctiva and the muscle before tying the suture. Then, again using TRASU, the scleral reinsertion is prepared. Postoperatively, openings resulting after TRASU remain totally covered by the lids apart from during upgaze and excessive lateral gaze, he said.
To assess the new technique, Dr Mojon carried out a prospective study at Kantonsspital, St Gallen, Switzerland, in which the first 20 consecutive patients treated with TRASU MISS were matched with a non-concurrent, retrospective comparison group of 20 patients with a traditional MISS opening.
While the long-term results did not differ in the two groups, the MISS technique delivered better visual acuity and less lid swelling in the immediate postoperative period.
“With the transconjunctival suture I am able to position the suture very anteriorally without opening the conjunctiva and without any bleeding,” said Dr Mojon. “Some of the patients are
A new minimally invasive strabismus surgery (MISS) technique for rectus and oblique muscle displacement offers a safe and effective means of performing muscle surgery through a smaller conjunctival incision than was possible with previously reported MISS techniques, according to Daniel S Mojon MD, FEBO, EMHSA, Airport Medical Center Eye Clinic, Zürich, Switzerland.
“The minimally invasive transconjunctival suturing technique (TRASU) allows for the suturing of the muscle at its original insertion and the reattaching of a muscle far behind the original insertion without the need to prolong the cut more anteriorly and posteriorly. The surgery is conducted through an opening that is about two-thirds the size of traditional MISS conjunctival incisions,” he said.
The refined suturing technique, which can be used for recessions, resections, plications, advancements and transpositions, offers several advantages over existing methods, Dr Mojon told EuroTimes.
“This technique has several advantages including faster surgery because we are dealing with a smaller opening that can be closed very quickly. There is also significantly less discomfort for the patient and quicker postoperative rehabilitation. It also results in less scarring, which is particularly important in the event of repeat surgery. In fact, with this technique sometimes
Faster recovery and less discomfort with refined MISS technique. Dermot McGrath reports
MISS TECHNIQUE
EUROTIMES | OCTOBER 2014
SPECIAL FOCUS: PAEDIATRIC OPHTHALMOLOGY
Figure 4: Appearance on the first postoperative day after further recession of the lateral rectus muscle on the right side and medial rectus muscle on the left side because of a horizontal head turn secondary to a congenital pendular nystagmus. Both muscles had been already recessed twice before. The eyes can be perfectly opened and the second repeat surgery is nearly not visible
This technique has several advantages
including faster surgery because
we are dealing with a smaller
opening that can be closed very quickly
Daniel S Mojon MD, FEBO, EMHSA

9
caption
completely amazed afterwards at just how clear their operated eyes are after surgery. There is occasionally some swelling of the eyelids with repeat surgeries but very little discomfort,” he added.
While MISS may be performed with the same instruments used for standard, open surgery, it does require using an operating microscope which can take some adjustment for surgeons used to working with loupes.
Nevertheless, once the learning curve has been negotiated, one of the big advantages of MISS compared to the widely used Parks fornix approach is that it can be used for all types of patient, said Dr Mojon.
“The Parks fornix technique for rectus muscle access is very popular in the United States and while it is an excellent technique that works well, its use is difficult in older patients with inelastic conjunctiva, in young patients with prominent Tenon’s tissue and in cases with significant pre-existing scarring,” he said.
Dr Mojon said that in his hands, only about one patient in every 1,000 is not suitable for the MISS technique.
“This is a big plus because it allows me to be consistent and avoid switching from one technique to another and having to change instruments. This ultimately results in faster surgery which is generally better news for the patient as well,” he concluded.
Daniel S Mojon: [email protected]
Images show transconjunctival suturing (TRASU) for further recession of an already recessed horizontal rectus muscle
EUROTIMES | OCTOBER 2014
SPECIAL FOCUS: PAEDIATRIC OPHTHALMOLOGY
SPECIAL FOCUSCATARACT & REFRACTIVE
September 2014 | Vol 19 Issue 9
APP SEE YOU
SPECIAL FOCUSCATARACT & REFRACTIVE
September 2014 | Vol 19 Issue 9
APP SEE YOU
SPECIAL FOCUSCATARACT & REFRACTIVE
September 2014 | Vol 19 Issue 9
APP SEE YOU
SPECIAL FOCUSCATARACT & REFRACTIVE
September 2014 | Vol 19 Issue 9
APP SEE YOU
EUROTIMES
Full interactivity featuring:
...and more!
Search for ‘ESCRS EuroTimes’
INTERACTIVE!
SLIDESHOWS PODCASTSVIDEO
Figure 1: After applying two small parainsertional cuts (MISS), the muscle insertion is visualised. A spatula is inserted below the muscle (not shown). The needle is advanced in the space between the spatula and the muscle and passed through the muscle and the conjunctiva in order to suture approximately one-third of the muscle width
Figure 2: The needle is grasped close to the tip and advanced until the whole needle has passed the muscle. It should be avoided to pass the needle completely through the conjunctiva
Figure 3: The needle is pushed back in the space between the muscle and the conjunctiva. Now, the suture is tied (not shown)
Cour
tesy
of D
aniel
S M
ojon
MD,
FEB
O, E
MHS
A

10
EUROTIMES | OCTOBER 2014
The negative attitudes of others and lack of support are among the most disabling factors faced by children who are blind in developing countries, according to a study presented at the World Society of Paediatric Ophthalmology and Strabismus (WSPOS) Sub Specialty Day in London.
Clare Gilbert FRCOphth, MD, Disability and Eye Health Group at the London School of Hygiene and Tropical Medicine, told delegates attending the session that more needs to be done to overcome negative attitudes that lead to social exclusion and marginalisation of blind children.
“The research work carried out by Mohammad A Muhit in Bangladesh clearly showed that attitudinal barriers were the most important barriers to participation amongst blind children in that country. Interventions which promote participation need to be developed and evaluated to give these children the best possible chance of development, education and participation in broader social life,” she said.
Prof Gilbert stressed that she was not speaking as an expert in the field of rehabilitation or education of children, but simply wished to highlight the findings of projects that she or her colleagues at the Disability and Eye Health Group had been involved in over the years in relation to the impact of blindness in children in developing countries.
She noted that Dr Muhit’s research also collected some telling insights into the attitudinal barriers facing blind children in their daily activities. “From the supervisor who remarked that ‘those who can see or are sighted do not get any job after completing education… so what will the blind people achieve through education?’ to the mother who wondered ‘what would the child do with education… he is earning good money [begging] and contributing to the cost of the family’, the barriers to inclusion are many and varied,” said Prof Gilbert.
MAINSTREAM ACTIVITIESIn terms of measures that could be taken to overcome such attitudinal barriers, Prof Gilbert told EuroTimes that a lot can be done.
“Some ideas that spring to mind are buddying at school; organising sports events for children who are blind or visually impaired; providing opportunities for parents and children to talk about their experiences, and having more people who are blind in positions of influence in mainstream activities. Moreover, community group sessions with role play has been successful in other areas of disability in children,” she said.
More research is also needed to provide evidence of the best approach for educating children who are blind in low income settings, said Prof Gilbert.
“Is inclusive education alone the best approach, or is a mixed approach better, with some time spent in schools for the blind for intensive skills learning, such as Braille for instance?” she asked.
In a wider context, Prof Gilbert sees some grounds for optimism in the implementation of specific measures for the control of visual loss amongst children.
For instance, programmes for the control of retinopathy of prematurity are expanding in many middle and low income countries, and countries such as China, Russia, Peru, Colombia, Brazil and Mexico now have national guidelines. Mexico and Peru have also passed legislation making eye examination of pre-term infants mandatory.
“Paediatric tertiary level services are expanding, as are school eye health programmes. Several of the international non-government organisations are focusing on visual loss in children, supporting eye care provision for children from community level up to tertiary care. However, there are gender differences in the uptake of treatment, with more boys undergoing cataract surgery than girls, for example, although there is no evidence that non-traumatic cataracts are more common in boys. Reasons for this need to be explored together with interventions which improve uptake of services by parents of girls,” she said.
Clare Gilbert: [email protected]
Negative attitudes heighten social exclusion for blind children in developing countries. Dermot McGrath reports
GLOBAL SURVEYSPECIAL FOCUS: PAEDIATRIC OPHTHALMOLOGY
10th International Congress
of Corneal Cross-Linking
December 5-6, 2014 Zurich, Switzerland
The CXL Congress is an international forum for the most recent advance in
corneal cross-linking
One day instructional course on CXL - all levels Scientific presentation, laboratory science,
clinical results and latest developments
www.cxl-congress.com
Children attending the Outpatient Department after cataract surgery, Islamia Eye Hospital, Dhaka, Bangladesh
Cour
tesy
of C
lare
Gilb
ert F
RCOp
hth,
MD

11
T. +1 416.398.3306 F. +1 416.631.8272 | www.innovativexcimer.com
Improved Clinical Outcomes of CXL and PRK with Amoils Epithelial Scrubber
Epithelial Removal Has Never Been Easier
Corneal Xlinking, PRK & Advanced Surface Ablation
• Uniform epithelium removal in only 5 - 7 seconds
• Avoid alcohol damage to surrounding tissue
• Minimize total procedure time
• No need for subsequent scraping
STRABISMUS TREATMENTDelayed adjustable sutures suitable for complex strabismus surgery. Dermot McGrath reports
he choice of using a closed conjunctival delayed approach to adjustable suture surgery may present some significant advantages to more traditional adjustable suture techniques in the treatment of strabismus, according to David B Granet MD, FACS, FAAP.
Dr Granet said that the technique offers a valuable option for the strabismologist, especially in the case of repeat surgeries and complex strabismus cases.
“Potential advantages include the decreased risk of infection owing to immediate conjunctival closure, decreased interference from pain and oedema on postoperative measurements and less physician and patient time due to the decreased need for postoperative adjustment,” he explained.
He said that the closed conjunctival approach is a refinement of the traditional adjustable suture technique, which allows fine-tuning of surgical outcomes in the immediate postoperative period. The adjustment usually takes place 3-7 days after surgery, and is performed by removing or stretching conjunctival sutures and positioning the globe with the traction suture to enable exposure of the cinch or bow knot. The knots are adjusted until the muscle is in its desired position as confirmed by motility testing before the conjunctiva is re-sutured.
In a large multicentre retrospective review of the technique published in the British Journal of Ophthalmology, postoperative ocular adjustments were required in 26 per cent of patients and were performed from two hours to 14 days after surgery, with an average adjustment time of 2.5 days. The study evaluated outcomes in 440 patients ranging from 10 to 91 years performed at four centres in the US by five surgeons.
PATIENT SATISFACTIONIn the total sample, all strabismus subgroups had high levels of patient satisfaction, defined as no report of diplopia in the chief complaint in target gaze and/or had cosmetic improvement during the follow-up period, noted Dr Granet. The lowest long-term satisfaction group had the highest rate of thyroid-associated ophthalmopathy-induced strabismus.
Complications associated with the procedure were transient and included dellen, poor conjunctival appearance, filamentary keratitis, infection, granuloma, exposed suture and corneal abrasion. There was one case of corneal microperforation treated with glue and contact lens in a patient with severe-trauma-induced dry eye and one case of scleral perforation in a patient with previous retinal detachment and high myopia treated with retinal laser and repeat detachment surgery. The total untoward event rate, including all events, was six per cent (29 of 440) with individual surgeon rates as low as 0.8 per cent said Dr Granet.
While the retrospective study only included patients older than 10 years of age, Dr Granet told EuroTimes that the technique has also been successfully utilised in younger patients.
Summing up, he said that while prospective, randomised trials are needed to validate the closed conjunctival delayed approach to adjustable suture surgery, the technique represents a valuable addition to the armamentarium of the strabismus surgeon.
David B Granet: [email protected]
SPECIAL FOCUS: PAEDIATRIC OPHTHALMOLOGY
T
EUROTIMES | OCTOBER 2014

12
PAEDIATRIC IMAGING
OCT, MRI, ultrasound can be adapted for ophthalmic use in children. Howard Larkin reports
However, technical problems such as reflectivity of instruments and OCT-microscope integration limit visualisation of retinal manipulation during surgery. More development of the technology is needed to be clinically useful, Dr Schuman added.
“In the future we will see the use of real-time OCT in the operating microscope.”
ANTERIOR SEGMENT IMAGINGOCT also is being successfully adapted to paediatric anterior segment applications, said Ken K Nischal MD, FRCOphth, director and professor of paediatric ophthalmology, strabismus and adult motility at the University of Pittsburgh, US. He presented a case in which a specially developed mechanical arm was used to hold an OCT probe steady for imaging the anterior chamber.
The scan showed evidence of palisades of Vogt remaining in the limbus of a child with opaque cornea who had been refused transplant due to apparent limbal deficiency. A transplant was done and the patient successfully re-epithelialised, Dr Nischal said.
“Now we have a way of picking those children out who might benefit from surgery because we have this technology.”
With regard to ultrasound, Dr Nischal recommends using linear transducer ultrasound probes rather than the
populations, he noted (Atemir et al. J Child Neurol 2012; 27:1517-1523).
Normative databases for children are also beginning to appear, Dr Schuman said. These include data for school-age children including retinal nerve fibre layer thickness (Tsai et al. Jpn J Ophthalmol, 2012. 56(4): 362-70) and mean macular thickness (Atemir et al. Am J Ophthalmol, 2013. 155(1): 171-176). These and other published data can be used clinically for diseases including vitreomacular interface disorders, neuro-ophthalmology, retinal dystrophies and anterior segment conditions.
Other OCT applications include imaging for femtosecond laser-assisted cataract surgery and intraoperative use for pars plana vitrectomy for epiretinal membrane, macular holes, proliferative diabetic retinopathy silicone oil removal and primary rhegmatogenous retinal detachment (Binder. Retina, 2011. 31(7): 1332-6), Dr Schuman said.
Imaging technologies developed for adults and for specialties other than ophthalmology are being adapted for ophthalmic use in children with good results, according to presenters at the annual meeting of the American Academy of Ophthalmology in New Orleans.
The advent of spectral domain OCT (SD-OCT) overcomes one big obstacle to using it with children, said Joel S Schuman MD, FACS, distinguished professor and chairman of ophthalmology at the University of Pittsburgh School of Medicine, US.
RELIABILITY OF OCTSD-OCT machines are fast enough to get good scans even in young children who cannot hold still long. One study of 100 healthy children confirmed the reliability and reproducibility of OCT in paediatric
EUROTIMES | OCTOBER 2014
SPECIAL FOCUS: PAEDIATRIC OPHTHALMOLOGY
In the future we will see the use of real-time OCT in the operating microscopeJoel S Schuman MD, FACS

13
However, a standard brain protocol MRI does not reveal the orbital detail required, Dr Demer said. He recommended using orbital surface coils, which are now approved for clinical use on most scanners.
“Alternatively, other small clinical surface coils can be easily adapted for ophthalmic use,” Dr Demer said.
Joel Schuman: [email protected] Nischal: [email protected] L Demer: [email protected]
MD, PhD, of the Stein Eye Institute and the Departments of Ophthalmology and Neurology at the University of California – Los Angeles, US.
Clinical information obtainable from imaging, but unavailable from direct examination, includes congenital and other anomalies of the extraocular muscles and ligaments, their length, details of any trauma and changes in anatomy due to surgery and innervation of extraocular muscles.
vector probes more commonly used in ophthalmology. The linear probe, which is commonly used to find blood vessels in surgery and is available in any operating suite staffed by anaesthesiologists, uses an array of piezoelectric transducers instead of the single scanning transducer in vector devices, he explained. The result is a much more detailed view.
“I don’t understand why the ophthalmic industry makes vector probes and doesn’t make linear probes. For me the liner probe gives much more information anteriorly and within the globe itself.”
STRABISMUSMRI is also useful, but underused, in assessing strabismus, said Joseph L Demer
High-resolution, axial surface coil MRI of orbits of patient fixating a target in right gaze. Large left exotropia is due to slipped left medial rectus (MR) muscle suspended, not from the globe, but from the retracted left medial rectus pulley. Despite disinsertion for many years, the left MR was not atrophic, and was later functional after recovery by orbitotomy and reattachment to the sclera
EUROTIMES | OCTOBER 2014
SPECIAL FOCUS: PAEDIATRIC OPHTHALMOLOGY
3rd World Congress of Paediatric Ophthalmology and Strabismus
www.wspos.org
Fira Gran Via, Barcelona, SpainSeptember 4–6, 2015
... other small clinical surface coils can be
easily adapted for ophthalmic use
Joseph L Demer MD, PhD
Cour
tesy
of J
osep
h L
Dem
er M
D,Ph
D

14 CATARACT & REFRACTIVE
cent of respondents perform 1,000 or more cataract surgeries, and this figure continues to increase every year.
Reflecting the wider global trend, the size of the incisions used by French ophthalmic surgeons for cataract surgery has steadily decreased in recent years, with the percentage of micro-incisions of less than 1.8mm being performed stabilising between five per cent and six per cent in the past few years. The number of surgeons using an incision size between 1.8mm and 2.2mm has climbed steadily from 25 per cent in 2009 to over 50 per cent in 2013.
Looking at premium IOL usage, Dr Gold noted that while growth has been relatively linear for multifocal and add-on IOLs in recent years, it is the toric IOLs that have really taken off, with 51 per cent of respondents in 2013 now implanting toric lenses compared to 13 per cent in 2008.
The use of intracameral antibiotics in cataract surgery is now almost universally applied in France, having been made obligatory by the national health authority in 2011, with cefuroxime the antibiotic of choice in 99 per cent of cases, said Dr Gold.
Turning to refractive surgery trends, an increasing proportion of French surgeons now use refractive surgery for the treatment of presbyopia, with PresbyLASIK the treatment of choice for more than half of respondents.
In terms of topography use, this year confirmed the steady rise in popularity of the Pentacam (50 per cent) which has now displaced Orbscan (48 per cent) from top spot followed by OPD-Scan (17 per cent) in third place. The use of aberrometry also continues to find favour among French refractive surgeons with almost 66 per cent now using an aberrometer in their refractive practice.
The competitive landscape of the excimer laser market is also reflected in Dr Gold’s survey. The Zeiss Mel 80 (31 per cent) is the leading laser among respondents this year, followed by the Alcon Allegretto (28 per cent) and the Bausch + Lomb Technolas (23 per cent).
Richard Gold: [email protected]
he almost universal adoption of intracameral antibiotic use in cataract surgery, a marked trend towards higher-volume cataract surgery to cater for an increasingly older
population and a dramatic increase in the use of toric intraocular lenses (IOLs) are among some of the more interesting findings of the latest survey of French ophthalmologists conducted by Richard Gold MD.
In the 17th annual survey of French practices in ophthalmic surgery, Dr Gold, in private practice in Le Raincy, France, collected 991 responses to an anonymous questionnaire sent to 3,210 French ophthalmologists. The response rate of 12.55 per cent represented a drop of almost 10 per cent compared to the 2012 figure and called into question the viability of continuing with the study in forthcoming years, said Dr Gold.
As well as providing valuable insights into trends and developments in clinical practice, Dr Gold’s questionnaire serves as a useful barometer of the current well-being of French ophthalmology in general.
The proportion of French ophthalmologists with a low volume of cataract surgery continues to decline, with about five per cent performing fewer than 100 cataract surgeries per year, down from 22 per cent in 1998 and 10 per cent in 2007.
The proportion performing between 100 and 199 procedures annually has decreased in recent years to below 15 per cent in 2013 compared to a high of 33 per cent in 2001.
The most striking trend has been the proportion of surgeons performing higher-volume cataract surgery. “This is not surprising given the reduced number of ophthalmologists in France and the fact that the population is getting older,” said Dr Gold.
More than 30 per cent of respondents now perform between 300 and 499 surgeries per year compared to 17 per cent in 2000, while those treating between 500 and 999 patients per year has increased from just eight per cent in 2000 to 18 per cent in the 2012 survey. Eight per
Practice trends revealed in French survey. Dermot McGrath reports
NEW INSIGHTSKR-800S AUTO KERATO- REFRACTOMETERWITH “SUBJECTIVE” FUNCTIONS
· Accurate objective measurement (REF, KRT, R/K)
· Subjective measurement forfar & near
· Glare test
· Contrast test
· Grid test
· Pre- and post-cataract screening
www.topcon-medical.eu
61616_TOP_Adv_KR-800s_56x266.indd 1 08-08-14 10:28
The use of intracameral antibiotics in cataract surgery is now almost universally applied in France...Richard Gold MD
T
EUROTIMES | OCTOBER 2014

Become anESCRS Member
ESCRS
Also free to members:Access to iLearnOnline interactive courses
Subscription to Journal of Cataract & Refractive Surgery
Reduced ESCRS Congress Fees
Visit www.escrs.org today
FREE3 YEAR
MEMBERSHIP
FOR TRAINEES
Catch up on what you missed at the London Congress with ESCRS On DemandAn Online Library of Congress Presentations

16
EUROTIMES | OCTOBER 2014
IS PHACO DEAD?Phaco – safe, effective and continuing to improve. Sean Henahan reports
phthalmic surgeons caught in the throes of infatuation with femtosecond laser-assisted cataract surgery, shouldn’t forget the virtues of their long-term relationship with phaco, cautions Gerd Auffarth MD, PhD, chairman of the Department of Ophthalmology, Heidelberg University.
Asking "is phaco dead?", he told the World Ophthalmology Congress (WOC) in Tokyo the answer had to be an emphatic "no".
Dr Auffarth did not deny that the femtosecond laser brings a number of important potential improvements to cataract surgery, from improving on the capsulorhexis to fragmenting the lens. However, he noted that phacoemulsification has evolved considerably and will continue to do so.
“With phacoemulsification we have 40 years of technological development. You know what you are getting. You know how to handle it. We have evidence-based outcomes research of cost effectiveness. Indeed it is still the gold standard of cataract surgery for the majority of cases. I expect that as we combine the best features of femto and phaco there will be no limit to what we can do. This is just the beginning,” said Dr Auffarth, who is also director of the International Vision Correction Research Centre and the David J Apple International Laboratory for Ocular Pathology.
Following his legendary epiphany in the dentist’s chair, Charles Kelman first introduced the concept of phacoemulsification in 1967. Since that time there has been a steady progression of technical developments. Most notably, the latest generation of phacoemulsification machines all offer advanced systems allowing many ultrasound power options, control of fluidics and chamber stability.
MICROBURST TECHNOLOGYOne of the most important developments has been the advent of more refined ways to attack the lens nucleus. Microburst technology allows the surgeon to apply energy in different ways, while reducing the temperature. The incidence of corneal burns has been markedly reduced by this technology, he explained. Another key development in the evolution of phacoemulsification has been changing how the phaco tip moves. For 30 years, there was only one choice, longitudinal motion. Now phaco systems provide several options including torsional and transversal motion.
“This has led to further reductions in the amount of phaco energy required for cataract surgery. Ten years ago we were counting phaco time in minutes, now we are counting in seconds or even microseconds,” he said.
Pump systems also continue to evolve. Current phaco systems allow the surgeon to move between one, two or three pump systems on the fly. “Now the machine is thinking for you. It is keeping the energy and temperature stable, and keeping a certain pressure in the eye. Previous problems like surge are very rare these days. This gives you the opportunity to extend the option of cataract surgery to more patients, who might have not been good candidates in the past.”
Gerd Auffarth: [email protected]
However you say it -The warm compress patients actually love.
Convenient & effective* with superb complianceProven efficacy and safety†
Microwave & re-use 200 timesTreat Meibomian Gland Dysfunction
Dry Eye and BlepharitisDistributors throughout Europe
*Optometry & Vision Science: February 2014 - Volume 91 - Issue 2 - p 163-170† http://bjo.bmj.com/content/early/2014/07/04/bjophthalmol-2014-305220
Warm CompressWarme KompresseMascara CalienteMasque ChauffantMaschera CaldaCiepły Kompres
Warmte kompresТеплый компресс
EyeBagssold250,000over
www.eyebags.com
Invented and developed byTeifi James, Consultant Ophthalmologist - Halifax UK
patient satisfaction90%more
than
CATARACT & REFRACTIVE
O

17
EUROTIMES | OCTOBER 2014
Femtosecond laser-assisted cataract surgery can allow surgeons to deal with challenging cataract cases that would be difficult or near impossible to treat with
conventional surgery, Soon-Phaik Chee MD told a session of the World Ophthalmology Congress in Tokyo.
“Femtosecond laser capsulotomy and nucleus fragmentation has made the management of complicated cataracts easier for the surgeon and safer for the patient,” said Dr Chee, senior consultant, head, Uveitis and Cataract Subspecialty Service, Singapore National Eye Centre.
She presented a selection of cases from her own practice where the femtosecond laser had proved useful. Her first example was brunescent cataract. “These brunescent cataracts are particularly difficult to treat without compromising the cornea, especially if the anterior chamber is shallow. I routinely do these with the femtosecond laser.”
She said she typically started by performing a 5.0mm capsulotomy with the laser. She uses the Victus platform (Bausch + Lomb), which she noted allows her to make deep cuts close to the posterior capsule, making segmentation easier. She makes up to eight segments depending on the density of the nucleus. She advocates using dye for improved visualisation for those beginning femtosecond laser-assisted cataract surgery, along with a dispersive OVD to protect the cornea. She stressed the importance of having a good phaco machine with high vacuum settings to help hold on to fragments. She also said one should only use minimal ultrasound energy to prevent harming the corneal endothelium.
DOCK CAREFULLYIntumescent cataracts with a white-on-black nucleus are another challenging case where the femtosecond laser can be helpful, she noted. “It is very important in these cases to dock carefully. You want
Femtosecond laser useful for the most challenging cases. Sean Henahan reports
MANAGING CATARACTSCATARACT & REFRACTIVE
C-flex® Aspheric and Superflex® Asphericwith RaySert® PLUS Single Use Injector
rayner.com
C-flex® Advance AsphericPreloaded IOL Injection System
EC201423 08/14
to be meticulous. You need a capsule that is evenly docked, you don't want one that is slanted, or you may have capsulotomy that runs away. You might cut one portion of capsule before the other, which could result in rip of anterior capsule.”
In cases involving intumescent cataracts she also routinely uses IV mannitol to shrink the nucleus before applying the femtosecond laser, another technique for reducing the risk of an anterior capsule rip.
“Staining the capsule is also very useful in these cases. It helps keep the capsule visualised as you chop this very dense nucleus. Even with these white nucleus cataracts I routinely apply the femtosecond laser to segment these.”
Other cases where the femtosecond laser could provide a decisive benefit include Labrador corneal dystrophy, soft posterior polar cataracts, small uveitic cataracts and subluxated cataracts, she told the assembly.
Soon-Phaik Chee: [email protected]

XXXIII Congress of the ESCRS
5 – 9 September 2015Fira Gran Via, Barcelona, Spain
www.escrs.org
Instructional Course Submission Deadline 31 October 2014

19
EUROTIMES | OCTOBER 2014
ive symblepharon patients, including two that failed multiple prior reconstructions, were successfully treated with a novel approach in which keratolimbal allografts were used to cover conjunctival defects, Nancy Lee MD, ophthalmologist at Kaiser Permanente in San Diego, California, US, told the 2014 American
Society of Cataract and Refractive Surgery symposium in Boston.In all five cases ocular motility was restored and diplopia
in primary gaze resolved, Dr Lee reported. No symblepharon recurrences onto the keratolimbal graft segments were observed, though mild recurrences up to the edges of the grafts were seen in two patients. Subsequent placement of additional keratolimbal segments resulted in restoration of full range of ocular motion, she said.
The results suggest that keratolimbal allograft segments are a robust tissue alternative to amniotic membrane or mucosal autografts traditionally used for treating symblepharon, Dr Lee said. The keratolimbal allografts, similar to those used to treat limbal stem cell deficiency, created an effective mechanical deterrent to symblepharon reformation. That they also contained healthy limbal and conjunctival stem cells may also have helped prevent symblepharon recurrences by contributing to a healthy ocular surface, Dr Lee said.
STICKY PROBLEMSymblepharon occurs when trauma, disease or allergy cause adhesion of the palpebral conjunctiva of the eyelid to the bulbar conjunctiva of the eyeball. A frequent result is limitation of ocular movement, which may lead to clinically significant diplopia in primary and/or lateral gaze.
Surgical treatment involves release of symblepharon with resection of associated subconjunctival fibrotic tissue followed by reconstruction of the ocular surface. If not enough conjunctiva is left at the site to cover the entire surface defect, amniotic membrane, conjunctival autograft, or oral or nasal mucosal autografts are typically used to cover the remainder.
However, recurrences are common, even when adjuvant therapies such as intraoperative mitomycin C, symblepharon ring spacers and postoperative subconjunctival steroid injections are employed, Dr Lee noted. Autografts also present issues of tissue availability and potential complications at the donor site.
The technique Dr Lee reported was conceived by Marjan Farid MD, her co-author and preceptor at UC-Irvine, she said. Tissue preparation is similar to limbal cell transplant, using a 7.5mm punch. The central button is discarded and the corneal scleral rim sectioned. The posterior lamella is excised with crescent
blades, and corneal edges tapered. The segments are then custom tailored to cover the conjunctival defect without overlapping and secured with fibrin glue. Typically multiple segments are used.
Symblepharon resulted from trauma in all five patients Dr Lee treated. Two had failed repeated prior treatment, including autografts and subconjunctival steroids, but have now recovered with no recurrence at 12 and 18 months' follow up.
“We have achieved functional and anatomical success in all of our patients so far,” she said.
Nancy Lee: [email protected]
Keratolimbal tissue a promising alternative to amniotic membrane, mucosal autografts for persistent cases. Howard Larkin reports
LIMBAL ALLOGRAFTCORNEA
Tri-Spot FocusInfinitely adjustable Energy Tiltable Display
YAG-Laser
Bessemerstr. 1490411 Nürnberg Germany +49 (0) 911 217 79-0
Tri-Spot
Anzeigenserie-ESCRS EuroTimes_08_2013.indd 2 29.07.2014 18:09:03
F
Patient A (image 1): Fibrous regrowth is seen up to the edge of the most posterior graft at postoperative month three, resulting in symptomatic diplopia
Patient A (image 2): A fourth KLAL segment is placed posteriorly, leading to resolution of diplopia
Patient B (image 1): Extensive symblepharon resulted from a tree branch injury sustained over a decade prior to presentation
Patient B (image 2): There is complete resolution of symblepharon at postoperative month four
Cour
tesy
of N
ancy
Lee
MD

20
EUROTIMES | OCTOBER 2014
the cornea’s front surface’s radius of curvature by means of any of a number of keratometry devices. One thing the instruments all have in common is that they require the patient to fixate on a target. Therefore, the meridians intersect at the line of sight, although there again the terminology can vary.
“To be honest most of us are not really quite clear about that. There is some confusion of terminology and also many of the terms
have been used interchangeably,” said Oliver Findl MD, Hanusch Hospital, Vienna, Austria.
The line of sight is one of the eye’s many axes. Others include the optical axis, the
pupillary axis, the visual axis and the fixation axis. However, some of those definitions are used differently in a purely theoretical sense than they are in a clinical setting.
“Actually it's not complicated per se, but it is confusing because
different communities and different authors and different researchers and
different clinicians have been using different names and different definitions,
so it's really a bit of a mess. I recommend that people include a paragraph explaining their
definitions when they are writing these papers and articles,” said Pablo Artal PhD, University of Murcia, Murcia, Spain.
He noted that the pupillary axis is a line perpendicular to the cornea that passes through the centre of the pupil. The line of sight is the line passing from the centre of the pupil to the object of regard. The visual axis is the line passing from the fovea through the nodal point, near the back of the crystalline lens, to the object of regard. The optical axis is defined as a line extending from the vertex of the cornea through the nodal point of the eye to the posterior pole of the eye, which is, in turn, defined by the geometric centres of the cornea and the lens.
The angle of the pupillary axis to the visual axis is the angle kappa, the angle from the pupillary axis to the line-of-sight is the angle lambda. However, because the line of sight is nearly identical to the visual axis, and because the eye’s nodal point cannot be determined with current technology, angle lambda tends to be referred to clinically as angle kappa.
For similar reasons, the optical axis is more of a theoretical concept which applies best to eye models where the refractive surfaces are centred with respect to each other, Dr Artal noted.
“The optical axis in an optical system is easy to understand as a line that is going through the centre of the curvature of all the refractive surfaces. However, in the case of the human eye, the surfaces of the cornea and the lens are not actually aligned. They are kind of decentred with a bit of tilt. Therefore, in terms of classical optics the eye doesn't really have an optical axis.
Since all of these different axes have their own set of meridians, the question arises as to which axis should be used to gauge IOL centration, tilt and in the case of toric IOLs, rotation. Dr Artal recommended using the pupillary axis for that purpose.
“In my opinion IOLs should be centred with relation to natural undilated pupil because I think that is how the best visual results can be obtained,” he said.
Emanuel Rosen: [email protected] Oliver Findl: [email protected] Pablo Artal: [email protected]
In order for ophthalmic surgeons to communicate their findings clearly and unambiguously, care must be taken to use words in a way that they have one precise meaning in given context. There are several terms that are frequently misused in published research at present, said Emanuel Rosen MD, FRCS, Manchester UK.
A case in point is the use of the word axis with reference to corneal astigmatism, he said. When testing an eye’s refraction with a phoropter lens, the term “axis” is correctly used in the two-dimensional sense of the axes of, for example, an ellipse, which has a steep meridian and a flat meridian. In the case of astigmatism with a steep meridian, for example, at 90 degrees the phoropter astigmatic correcting lens would be said to have an axis @180 degrees ie, its flat meridian would be at 90 degrees to neutralise the cornea’s steep meridian.
However, when referring to the astigmatic component of the cornea, the anatomical term meridian is correct, he noted. The cornea’s astigmatic component is defined in terms, therefore, of steep and flat meridia for the cornea in that sense has no axes. Astigmatic incisions on the cornea, therefore, need to be so defined for their purpose is to flatten the steep meridian and by corresponding coupling steepening the flat meridian.
“The cornea has no axes, only meridians ranging from zero to 180 degrees. The axes of the astigmatic testing lenses put in front of the eye to correct cylindrical refractive error are perpendicular to the steep meridian. Therefore, the use of the term axis to define where action should be taken on the cornea, for example, has to be in meridional terms not in terms of axes,” Dr Rosen said.
AXES AND ANGLES The meridians of the eye correspond to the lines of longitude on a globe. The basis of the meridians is the measurements taken of
A meridian, by any other name, would be misnamed. Roibeard O'hEineachain reports
EYE TERMINOLOGYCORNEA
will take place in Le Palais des Congrès, Paris, on 8-9 May 2015
Applications: Open from October until 15 December 2014
For all further information log on towww.ebo-online.org
Diploma Examination 2015
Seal ofAchievement
in EducationExcellence
[Schematic figure on the axis and angles in the eye]
Courtesy of Pablo Artal PhD

21
EUROTIMES | OCTOBER 2014
EDUCATION TO THE FORE AS ESCRS CONGRESS OPENS
ducation will be the key theme driving future ESCRS initiatives, Roberto Bellucci, president of the ESCRS told delegates at the Opening Ceremony of
the XXXII Congress.“During my term as president of the
ESCRS I will be focusing on education. I want to ensure that the ESCRS is regarded as a leader in the provision of high-quality, expert-led education for ophthalmologists of all levels of experience,” he said.
Dr Bellucci noted that the ESCRS already offers many educational opportunities to its members in the form of annual meetings, ESCRS on Demand and iLearn. He also cited special measures for young ophthalmologists such as bursaries to attend the annual congress and the Observership Programme which enables them to gain valuable experience.
“I would like to build on what we already have, develop it further and look at introducing new educational sources for our members and delegates,” said Dr Bellucci. The ESCRS will also continue its support for important research activities," he said.
Dr Bellucci renewed the commitment of the ESCRS to continue support for the work of the society’s two charities, Orbis and OXFAM and he finished by thanking the 8,000 plus delegates from 125 countries who had come to London for the ESCRS Congress.
“The ESCRS is proud to offer a scientific arena to all its members, delegates, supporters and the ophthalmic industry. All of these form a community in the interest of science and for the advantage of our patients. This community gathers at home once a year – and the name of this home is the ESCRS,” he said.
Dr Bellucci’s address was followed by a brief presentation by Brian Little, president of the United Kingdom & Ireland Society of Cataract and Refractive Surgeons (UKISCRS), who urged delegates to enjoy not just the congress but also “the cultural cornucopia that is London”.
This year’s Ridley Medal Lecture on the topic of “Four decades of cataract surgery – personal visions for the future” was delivered by Gunther Grabner from Austria. A full report of Dr Grabner’s lecture will appear in a forthcoming edition of EuroTimes.
MEETING REPORT
2014
XXXII Congress of the ESCRS
September
E
ESCRS VIDEO COMPETITION WINNERHiroyuki Matsushima, Japan, received First Prize overall in this year’s Video Competition.“Opacification of intraocular lenses”, provides an explanation for a recently observed phenomenon wherein IOLs themselves become opacified over time, in some cases to the point that they must be removed and replaced. Opacification occurs in both hydrophilic and hydrophobic IOLs. However, the opacification is of a markedly different character in the two types of lenses.
In hydrophilic IOLs, surface opacity is clearly visible under slit-lamp examination, the fundus is only faintly visible under transillumination and patients tend to complain of poor vision, leaving lens exchange the only option for recovering vision.
In hydrophilic IOLs, on the other hand, slit-lamp examination shows thin bands of opacity on the front and back of the lens, but the opacification is barely visible under transillumination and the fundus is clearly visible. Moreover, patients tend to complain much less about their vision and lens exchange is seldom necessary.
When Dr Matsushima and his associates examined the surfaces of explanted opacified lenses with scanning electron microscopy, they observed dense deposits of calcium on the surface of the hydrophilic IOLs, but the surface of the hydrophobic IOL had no deposits.
Examination of a cross-section of the hydrophobic lens using a cryogenic FIB scanning electron microscope revealed nanometre-sized water particles distributed widely throughout its outer layers.
The properties observed in the hydrophobic IOLs suggest that the opacification results from a phenomenon called water phase separation, which in turn results in the supersaturation of the lens material.
Dr Gunther Grabner (left), who delivered the Ridley Medal Lecture, with ESCRS president Dr Roberto Bellucci at the ESCRS Opening Ceremony
Hiroyuki Matsushima, winner of the overall prize in this year’s Video Competition

22
EUROTIMES | OCTOBER 2014
LONDON WELCOMES DELEGATES TO 14TH EURETINA CONGRESS
Retinal specialists and researchers from across the globe gathered in London for the 14th annual Congress of the European Society of Retina Specialists (EURETINA).
As one of the world’s most vibrant capital cities, London provided the perfect setting for this year’s
gathering of clinicians and surgeons interested in the research and treatment of retinal and macular diseases.
To add to the appeal of the meeting, the 14th EURETINA Congress was scheduled to precede and overlap with several other important ophthalmic meetings taking place in London: the XXXII Congress of the ESCRS and the 5th EuCornea Congress.
Addressing the assembled crowd at the Opening Ceremony, Francesco Bandello MD, current president of EURETINA and chairman of the Programme Committee, welcomed delegates to London for what he hoped would prove to be the most stimulating and rewarding congress to date.
“I am delighted to announce that we have over 5,000 delegates registered for the congress this year, which is almost 1,000 more since the last meeting in Hamburg and shows that EURETINA continues to go from strength to strength. This is thanks to the participation of highly regarded speakers and the willingness of so many delegates to travel from afar to hear their contributions,” he said.
Dr Bandello said that he believed that the strategy of combining forces with the ESCRS and EuCornea to hold overlapping meetings is the right one for delegates with so many pressing demands on their time.
“I believe that the combination of three superior scientific programmes provides a unique forum for global networking and makes our congress in London a stimulating hub of research and knowledge exchange in worldwide ophthalmology,” he said.
It has never been so simple to adapt new technology into your daily workflow. The truly mobile FEMTO LDV Z8 finally enables you to use next generation femtosecond laser technology for your cataract and refractive surgeries. www.femtoldv.com
The FEMTO LDV Z8 is CE marked but not yet cleared by the FDA for the use in the United States. For other countries, availability may be restricted due to regulatory requirements; please contact Ziemer for details.
It's Time to make a Move
The ONE laser platformfor all your needs
all in one
Perfect integration for a streamlined cataract workflow
Compact and mobile for a multi-site use
Modular platform for laser cataract and cornea procedures
Visit us at AAO
booth #2362
EuroTimes_oct2014_FEMTO_LDV_Z8_Ad_93x266mm.indd 1 24.09.14 14:47
MEETING REPORT
September 2014LONDON14th EURETINA Congress
EURETINA president, Francesco Bandello, addressing delegates at the Opening Ceremony of the 14th EURETINA Congress

23
EUROTIMES | OCTOBER 2014
Medicel AG Tel. + 41 71 727 10 509427 Wolfhalden [email protected] www.medicel.com
True COMICS
with the single-use 23G mono-manual I/A systems for safe, reliable and effi cient capsule cleaning through sub 1.8 mm incisions.
EUCORNEA CONGRESS CONTINUES ON UPWARD TRAJECTORY
orneal experts and researchers from Europe and further afield converged on London for the 5th EuCornea Congress.
Welcoming delegates to London, José Güell, president of EuCornea, said that the congress was continuing the upward trajectory of the society.
The strength of this year’s Scientific Programme underscored the outstanding support that EuCornea has received from its members, said Dr Güell.
“This congress promises to deliver an excellent programme, which includes world leaders in the field of cornea and ocular surface disease, speaking across 11 symposia, four courses and nine free paper sessions. We are delighted to be partnering our congress with the XXXII Congress of the ESCRS and 14th Congress of EURETINA,” he said.
Dr Güell said that the partnership strategy of teaming up with societies such as the ESCRS and EURETINA makes sense for a young organisation such as EuCornea.
“At a time when we all have to choose carefully which congresses we attend, offering delegates more than one meeting at the same time seems to be very valuable. With this in mind, I am pleased to announce that next September EuCornea will once again be partnered with the ESCRS congress in Barcelona. We hope that this alliance of related meetings will be highly beneficial for members and delegates from all organisations,” he said.
Prof Caroline MacEwen, president of the Royal College of Ophthalmologists, also welcomed delegates to London and said that meetings such as the EuCornea Congress provided a vital resource for corneal experts to learn, debate and exchange ideas.
Prof Donald Tan, president of the Asia Cornea Society extended his heartiest congratulations to EuCornea on organising another successful congress and stressed the importance of continued collaboration.
MEETING REPORT
LONDON5th EuCornea Congress
September 2014
C
EuCornea president, Dr José Güell, welcoming delegates to the 5th EuCornea Congress in London

24 MEETING REPORT
PICTURE GALLERY
EUROTIMES | OCTOBER 2014

25
Femtosecond laser enhancing results of a range of keratoplasty techniques. Roibeard O'hEineachain reports
The femtosecond laser can be a useful tool in several types of keratoplasty procedures, including penetrating and endothelial keratoplasty and keratoprosthesis surgery, said Luca Menabuoni
MD, Nuovo Ospedale S Stefano, Prato, Italy, at Femto 2013 an international meeting on anterior segment surgery.
Dr Menabuoni noted that in eyes undergoing penetrating keratoplasty, the femtosecond laser enables the creation of closely matched interlocking trephination profiles in the donor and host corneas.
“The gold standard in penetrating keratoplasty is perfect flap adhesion, internal and external mechanical load resistance and the lowest endothelial cells pool to reduce the chance of rejection. The femtosecond laser can create trephination profiles with complex shapes and a large interface between the host and graft stroma,” Dr Menabuoni said.
Two commonly used profiles are the top-hat and mushroom profiles, he noted. However, because they have a weak load resistance, he has designed a new profile that he calls the anvil profile. Using an iFs 150 femtosecond laser (AMO) he creates matching profiles on the host and donor corneas the diameter of which is 7.5mm at the top, increasing to 8.5mm around the middle, below which is a trunk that is 6.5mm in diameter. This particular shape also preserves the patient’s endothelial cells pool.
When implanting the corneal button, he performs a procedure called corneal welding which is designed to enhance the adhesion of the graft to the host tissue. This technique is the result of a research collaboration with Drs Roberto Pini and Francesca Rossi from the Institute of Applied Physics (CNR) of Florence, Italy. It involves staining the trephined edges of both the host cornea and the donor button with a water solution of indocyanine green and then, after placing the graft in the eye, irradiating the graft-host junction with a near infrared (810 nm) diode laser operating at low power (12W/cm2).
Dr Menabuoni said that in 120 eyes in which he carried out penetrating keratoplasty with the anvil profile and corneal welding all surgeries were successful and without any intraoperative complications. “Short-term visual and refractive results with this technique have compared favourably with those achieved with conventional penetrating keratoplasty, although longer-term follow-up and comparative studies will be necessary to
determine precisely the advantages of this technique,” he said.
OCT-GUIDED ENDOTHELIAL KERATOPLASTYDr Menabuoni noted that he has also developed an endothelial keratoplasty technique in which he uses the femtosecond laser combined with OCT to make grafts that are less than 90 microns in thickness.
When performing the technique he uses OCT to determine the thickness of the donor cornea. He then uses the femtosecond to trephine the cornea down to predetermined depth and then progressively reduces the thickness to 70 microns and then stains the edges of graft on the stromal side with indocyanine green for corneal welding.
He then performs manual stripping of the recipient eye and, using an EndoGlide™ (Angiotech), he draws the graft into position, injects an air bubble in the eye and closes the incisions used for the procedure with standard suturing. He concludes the procedure by welding the graft to the host cornea with a diode laser.
Dr Menabuoni said that, in the eyes he has performed the procedure, the one-year follow-up results have shown that the thin flap it enables the surgeon to create can provide a good recovery of visual functional and a modest endothelial cells loss. “The use of the intraoperative OCT, femtosecond laser for trephination and diode laser for suturing provides an improvement in endothelial keratoplasty
A USEFUL TOOL
and a rapid and better visual recovery once the graft is in place,” he added.
Dr Menabuoni has also developed a technique where he uses the femtosecond laser to prepare the carrier corneal button for the Boston type 1 keratoprosthesis (KPro). He noted that the technique provides better centration of the prosthesis on the visual axis and improves the regularity of the graft/host junction.
When preparing the donor cornea he uses just one applanation to perform the two concentric trephinations with a 150 kHz Intralase™ FS laser. He then makes the first 8.5mm diameter outer trephination followed by a concentric 3.0mm diameter inner trephination.
“The femtosecond laser-assisted double trephination results in a donor cornea correctly prepared, and in an inner side precisely matched with the prosthesis. At the end of the surgery the KPro is correctly centred, and the optimised match of carrier and donor cornea reduces the risk of endophthalmitis and melting due to the migration of coliquative germs and enzymes,” Dr Menabuoni said.
He added that the Boston K-pro has become widely accepted as the treatment of choice for patients with a history of repeated graft failure, Stevens-Johnson syndrome, ocular burns and other conditions likely to have a poor prognosis with penetrating keratoplasty.
“The femtosecond laser enables a new, safer and easier procedure to centre the KPro in the donor cornea,” he concluded.
Luca Menabuoni: [email protected]
EUROTIMES | OCTOBER 2014
CORNEA
The femtosecond laser enables a new, safer and easier procedure to centre the KPro in the donor corneaLuca Menabuoni MD
OCT of an anvil shaped transplanted cornea
Cour
tesy
of L
uca
Men
abuo
ni M
D

and the EPT in the femtosecond laser group also remained significantly lower throughout all stages from 0 to 4 (soft to hard cataracts) as compared with the manual phacoemulsification group.
Furthermore the endothelial cell loss was significantly higher with manual phaco-emulsification than with LenSx® one month after surgery.
Raising the bar for safe, precise cataract surgery Professor Michael Knorz MD, in private practice in Mannheim, Germany, is another early adopter of femtosecond laser technology in cataract surgery, having made the transition to LenSx® in 2011.
Prof. Knorz said that LenSx® was helping to raise the bar for safe, precise and effective cataract surgery, with new innovations continually coming on stream to improve patient outcomes. He cited in particular the recent introduction of the SoftFit™ Patient Interface: a soft contact lens technology which enables the natural curvature of the cornea to conform to the soft contact lens insert.
“The main benefits of using the SoftFit™ Interface in our practice has been the elimination of corneal compression, better control of intraocular pressure and an overall improvement of surgical performance,” he said.
With the aid of the SoftFit™ Interface, Prof. Knorz has achieved a rate of around 97% of free-floating anterior capsulotomies in his surgeries.
86 patients with senile cataract set out to evaluate the impact of cataract grades on EPT using either FLACS on 88 eyes for corneal incisions, capsulotomy and lens fragmentation, or phacoemulsification on 62 eyes by pulsed ultrasound energy using traditional phacoemulsification.
The EPT was defined as the total phaco time (in seconds) multiplied by mean phaco energy (%).The EPT was significantly longer with manual phacoemulsification than with FLACS
Emerging clinical outcomes with FLACS
With many cataract surgery practices now making the transition to femtosecond laser-assisted cataract surgery (FLACS), Professor Thomas Kohnen MD, PhD, FEBO, Professor of Ophthalmology, Goethe-University, Frankfurt, Germany, shared his experience of almost 500 cases with the LenSx® Laser.
Prof. Kohnen’s case series of 150 eyes of
A dvances in phacoemulsification
and intraocular lens (IOL)
technology have radically
transformed the face of cataract
surgery in recent years. In this
new era of patient-driven cataract
refractive surgery, many savvy
surgeons are already reaping the
benefits of Alcon’s Cataract Refractive
Suite to maximise postoperative
visual outcomes for their patients.
The Suite is comprised of four principal technologies designed to work seamlessly to improve patient outcomes and which are already making a real difference in daily clinical practice, as highlighted by several leading surgeons who participated in May 2014 at an Alcon Innovation Day of live surgery sessions and didactic presentations at the Instituto de Microcirugía Ocular (IMO) Clinic in Barcelona, Spain and directed by Dr. José L. Güell.
VERION™ Image Guided System
The drive towards greater precision and enhanced surgical control has gained further momentum thanks to the VERION™ Image Guided System, according to José Güell MD, Coordinator of the Cornea, Cataract and Refractive Surgery Department of the the Instituto de Microcirugía Ocular, Barcelona, Spain.
Dr Güell said that the VERION™ Digital Marker L makes surgical planning much easier by allowing the surgeon to see all incisions and alignment in real-time utilizing a tracking overlay.
“Using the Digital Marker L means we no longer need to manually mark the patient’s eye preoperatively. The patient information is transferred directly to LenSx®, thus avoiding manual entry. Cyclotorsion adjustment and landmark recognition are automatic and the system allows pre-positioning of the surgical incision overlays using the reference image,” he said.
For Paulo Vinciguerra MD, in private practice at the Istituto Clinico Humanitas, Milan, Italy, the VERION™ Digital Marker L represents a significant advance on traditional manual markers by helping to reduce alignment errors in the placement of toric lenses.
Reporting some preliminary results comparing toric implantation with manual ink marking, Dr Vinciguerra said that patients implanted using the VERION™ Digital Marker L achieved more accurate refractive outcomes. Total astigmatism, higher order aberrations (HOAs) and misalignment were reduced as well as coma aberrations.
“The VERION™ Image Guided System allows IOL centration in the non-dilated centre of the pupil as measured pre-operatively and provides an easy way for surgeons to enhance the accuracy of cataract surgery, considering the location of incision, capsulorhexis size, and particularly IOL alignment and centration,” he said.
Patient management and communication With demand for toric IOLs on the rise, surgeons need to reappraise their communication strategies in order to
ensure that the maximum number of patients profit from this innovative technology, said Khiun Tjia MD, consultant ophthalmologist at the Isala Clinics, Zwolle, Netherlands.
“We need to target different messages for different categories of patient. Communication on toric IOLs often focuses on spectacle independence, which cannot always be achieved,” he said.
Dr Tjia said that improved quality of vision should be at the heart of the surgeon’s communication with the patient.
“In my experience, elderly people are often happy with their glasses. Therefore delivering effective communication to this population should differ from how we communicate with patients opting for private care, who are much more sensitive to refractive outcomes.
The concept of better quality of vision is very simple and understandable for the elderly population,” he said.
For Prof. Leonardo Mastropasqua MD, director of the Excellence Eye Centre at the University G d’Annunzio of Chieti-Pescara, Chieti, Italy, today’s cataract patients are more demanding and invariably expect rigorous safety, good visual recovery and excellent vision without glasses.
Prof. Mastropasqua noted that several factors influence the outcome of toric IOL implantation, with regard to efficacy, predictability and stability.
The IOL biomaterial has a major influence on postoperative IOL rotational stability, with hydrophobic acrylic IOLs such as the AcrySof® lenses generally forming the strongest adhesions with the capsular
bag to prevent anterior and posterior capsule opacification (ACO, PCO) and IOL rotation.
The LenSx® femtosecond laser also plays a role in reducing variability in surgically induced astigmatism, ensuring consistent clear corneal incision architecture, accurate wound apposition and sealing, as well as perfect IOL alignment, he said.
Summing up, Prof. Mastropasqua said that the combination of advanced technologies such as Acrysof® (tried-and-trusted material), Verion® (accurate alignment), and LenSx® (improved centration), could help to optimize toric IOL implantation outcomes.
Getting the best from multifocal IOLsThe importance of tailoring multifocal IOL solutions to fit patients’ real-life needs rather than trying to impose a “one size fits all” approach was emphasised by Francesco Carones, MD, Co-founder and Medical Director of the Carones Ophthalmology Center in Milan, Italy.
Discussing the ReSTOR® family of multifocal lenses, Dr Carones said the recent addition of the ReSTOR +2.5 to the existing ReSTOR+3.0 model offers clinicians an additional option for customizing the IOL strategy to specific needs based on patients’ lifestyles, preferences and physiologies.
He said that this can be achieved using specific questionnaires, conducting surveys, chair time and conversation and interviewing friends and relatives.
“The goal is to understand the patient’s various activities to determine his or her preferences and to group activities requiring near, intermediate, and distant vision requirements. There is still no common solution for every patient. The point is to customize the treatment to the patients’ needs,” he said.
INNOVATIVE TECHNOLOGIES in cataract refractive surgery
There is still no common solution for every patient. The point is to customize
the treatment to the patients’ needs. Francesco Carones, MD
10595-Alcon-eurotimes-DPS.indd All Pages 24/09/2014 13:16
26 ADVERTORIAL

and the EPT in the femtosecond laser group also remained significantly lower throughout all stages from 0 to 4 (soft to hard cataracts) as compared with the manual phacoemulsification group.
Furthermore the endothelial cell loss was significantly higher with manual phaco-emulsification than with LenSx® one month after surgery.
Raising the bar for safe, precise cataract surgery Professor Michael Knorz MD, in private practice in Mannheim, Germany, is another early adopter of femtosecond laser technology in cataract surgery, having made the transition to LenSx® in 2011.
Prof. Knorz said that LenSx® was helping to raise the bar for safe, precise and effective cataract surgery, with new innovations continually coming on stream to improve patient outcomes. He cited in particular the recent introduction of the SoftFit™ Patient Interface: a soft contact lens technology which enables the natural curvature of the cornea to conform to the soft contact lens insert.
“The main benefits of using the SoftFit™ Interface in our practice has been the elimination of corneal compression, better control of intraocular pressure and an overall improvement of surgical performance,” he said.
With the aid of the SoftFit™ Interface, Prof. Knorz has achieved a rate of around 97% of free-floating anterior capsulotomies in his surgeries.
86 patients with senile cataract set out to evaluate the impact of cataract grades on EPT using either FLACS on 88 eyes for corneal incisions, capsulotomy and lens fragmentation, or phacoemulsification on 62 eyes by pulsed ultrasound energy using traditional phacoemulsification.
The EPT was defined as the total phaco time (in seconds) multiplied by mean phaco energy (%).The EPT was significantly longer with manual phacoemulsification than with FLACS
Emerging clinical outcomes with FLACS
With many cataract surgery practices now making the transition to femtosecond laser-assisted cataract surgery (FLACS), Professor Thomas Kohnen MD, PhD, FEBO, Professor of Ophthalmology, Goethe-University, Frankfurt, Germany, shared his experience of almost 500 cases with the LenSx® Laser.
Prof. Kohnen’s case series of 150 eyes of
A dvances in phacoemulsification
and intraocular lens (IOL)
technology have radically
transformed the face of cataract
surgery in recent years. In this
new era of patient-driven cataract
refractive surgery, many savvy
surgeons are already reaping the
benefits of Alcon’s Cataract Refractive
Suite to maximise postoperative
visual outcomes for their patients.
The Suite is comprised of four principal technologies designed to work seamlessly to improve patient outcomes and which are already making a real difference in daily clinical practice, as highlighted by several leading surgeons who participated in May 2014 at an Alcon Innovation Day of live surgery sessions and didactic presentations at the Instituto de Microcirugía Ocular (IMO) Clinic in Barcelona, Spain and directed by Dr. José L. Güell.
VERION™ Image Guided System
The drive towards greater precision and enhanced surgical control has gained further momentum thanks to the VERION™ Image Guided System, according to José Güell MD, Coordinator of the Cornea, Cataract and Refractive Surgery Department of the the Instituto de Microcirugía Ocular, Barcelona, Spain.
Dr Güell said that the VERION™ Digital Marker L makes surgical planning much easier by allowing the surgeon to see all incisions and alignment in real-time utilizing a tracking overlay.
“Using the Digital Marker L means we no longer need to manually mark the patient’s eye preoperatively. The patient information is transferred directly to LenSx®, thus avoiding manual entry. Cyclotorsion adjustment and landmark recognition are automatic and the system allows pre-positioning of the surgical incision overlays using the reference image,” he said.
For Paulo Vinciguerra MD, in private practice at the Istituto Clinico Humanitas, Milan, Italy, the VERION™ Digital Marker L represents a significant advance on traditional manual markers by helping to reduce alignment errors in the placement of toric lenses.
Reporting some preliminary results comparing toric implantation with manual ink marking, Dr Vinciguerra said that patients implanted using the VERION™ Digital Marker L achieved more accurate refractive outcomes. Total astigmatism, higher order aberrations (HOAs) and misalignment were reduced as well as coma aberrations.
“The VERION™ Image Guided System allows IOL centration in the non-dilated centre of the pupil as measured pre-operatively and provides an easy way for surgeons to enhance the accuracy of cataract surgery, considering the location of incision, capsulorhexis size, and particularly IOL alignment and centration,” he said.
Patient management and communication With demand for toric IOLs on the rise, surgeons need to reappraise their communication strategies in order to
ensure that the maximum number of patients profit from this innovative technology, said Khiun Tjia MD, consultant ophthalmologist at the Isala Clinics, Zwolle, Netherlands.
“We need to target different messages for different categories of patient. Communication on toric IOLs often focuses on spectacle independence, which cannot always be achieved,” he said.
Dr Tjia said that improved quality of vision should be at the heart of the surgeon’s communication with the patient.
“In my experience, elderly people are often happy with their glasses. Therefore delivering effective communication to this population should differ from how we communicate with patients opting for private care, who are much more sensitive to refractive outcomes.
The concept of better quality of vision is very simple and understandable for the elderly population,” he said.
For Prof. Leonardo Mastropasqua MD, director of the Excellence Eye Centre at the University G d’Annunzio of Chieti-Pescara, Chieti, Italy, today’s cataract patients are more demanding and invariably expect rigorous safety, good visual recovery and excellent vision without glasses.
Prof. Mastropasqua noted that several factors influence the outcome of toric IOL implantation, with regard to efficacy, predictability and stability.
The IOL biomaterial has a major influence on postoperative IOL rotational stability, with hydrophobic acrylic IOLs such as the AcrySof® lenses generally forming the strongest adhesions with the capsular
bag to prevent anterior and posterior capsule opacification (ACO, PCO) and IOL rotation.
The LenSx® femtosecond laser also plays a role in reducing variability in surgically induced astigmatism, ensuring consistent clear corneal incision architecture, accurate wound apposition and sealing, as well as perfect IOL alignment, he said.
Summing up, Prof. Mastropasqua said that the combination of advanced technologies such as Acrysof® (tried-and-trusted material), Verion® (accurate alignment), and LenSx® (improved centration), could help to optimize toric IOL implantation outcomes.
Getting the best from multifocal IOLsThe importance of tailoring multifocal IOL solutions to fit patients’ real-life needs rather than trying to impose a “one size fits all” approach was emphasised by Francesco Carones, MD, Co-founder and Medical Director of the Carones Ophthalmology Center in Milan, Italy.
Discussing the ReSTOR® family of multifocal lenses, Dr Carones said the recent addition of the ReSTOR +2.5 to the existing ReSTOR+3.0 model offers clinicians an additional option for customizing the IOL strategy to specific needs based on patients’ lifestyles, preferences and physiologies.
He said that this can be achieved using specific questionnaires, conducting surveys, chair time and conversation and interviewing friends and relatives.
“The goal is to understand the patient’s various activities to determine his or her preferences and to group activities requiring near, intermediate, and distant vision requirements. There is still no common solution for every patient. The point is to customize the treatment to the patients’ needs,” he said.
INNOVATIVE TECHNOLOGIES in cataract refractive surgery
There is still no common solution for every patient. The point is to customize
the treatment to the patients’ needs. Francesco Carones, MD
10595-Alcon-eurotimes-DPS.indd All Pages 24/09/2014 13:16
27ADVERTORIAL

28
EUROTIMES | OCTOBER 2014
GLAUCOMA
Simple test on the way for glaucoma detection. Roibeard O’hEineachain reports
IDENTIFYING GLAUCOMA
mmunoproteomics may soon provide an easy, non-invasive and objective means of diagnosing glaucomatous disease and may also point to new approaches to therapy, Franz Grus MD, PhD, Medical University Mainz, Mainz, Germany told the 11th Congress of the European
Glaucoma Society in Nice.He noted that, in several clinical studies so far involving
populations from Germany, the US or Australia, he and his associates were able to detect glaucoma with a sensitivity and specificity of more than 90 per cent based solely on their autoantibody profiles. “Our findings from these antibody tests could also open up the way to the development of innovative personalised immunomodulatory treatment options.”
PROTEOMES AND GLAUCOMADr Grus noted that “proteomics” corresponds to proteins as “genomics” corresponds to genes. A good illustration of the importance of proteomics is the transformation of caterpillar to a butterfly. Although the genome remains the same, the proteome is vastly altered from one stage to the other.
Many proteomic biomarkers have been identified for glaucoma, like for example the presence of transthyretin in the aqueous humour and sphingomyelin in the optic nerve. However, there are as yet no non-invasive means of testing for these biomarkers, Dr Grus said.
“The disadvantage of most of these proteomic markers is that they are not easily accessible because they are coming from aqueous humour and optic nerve and the retina. Therefore we asked ourselves if immunoproteomics from easily accessible body fluids, like tears or blood, could be a way to look at it because antibodies are stable and very easy to measure,” he said.
Dr Grus said that studies comparing the immunoreactivity of serum from glaucoma patients and control patients show that there are consistent changes in the autoantibody profile in patients with glaucoma. He noted that glaucoma patients and controls have very complex immunoreactivity patterns and a very high number of antibodies that react with antigens from the optic nerve and retina. The increase (up regulation) and decrease (down regulation) in the production of these autoantibodies in patients with glaucoma may have both a cause and an effect relationship with the disease, he said.
Animal studies on Lewis rats proved the neurodegenerative properties of an induced autoimmunity conducted through systemic immunisation of previously identified antigens and resulted in retinal ganglion cell loss. Using this Experimental Autoimmune Glaucoma (EAG) animal model Dr Grus was able to demonstrate that also a complex alteration in the autoantibody patterns was provoked in these animals and the animals developed a glaucomatous autoantibody profile.
Recent new immunohistological findings in patients with glaucoma include antibody deposits in their retinal ganglion cell layer, microglial activation and probably activation of B lymphocytes.
Franz Grus: [email protected]
EYEFILL® D.C.
D I S P E R S I V E C O H E S I V E
EYEFILL® S.C.S U P R E M E C O H E S I V E
ad ET EYEFILL 1-2hoch ENG 131003v3 pva.indd 1 19.09.14 09:18
I

29
EUROTIMES | OCTOBER 2014
GLAUCOMA
GLAUCOMA MONITORINGNew monitoring devices advance research and therapy.
Sean Henahan reports
ontinuous intraocular pressure (IOP) monitoring would provide researchers and clinicians with information that could help to elucidate the pathophysiology of the disease and revolutionise its treatment. That dream is now close to realisation, reported Kaweh Mansouri MD, MPH at the World
Ophthalmology Congress in Tokyo. “It is no longer a dream to think that we have access or will soon
have access to methods that allow us to monitor IOP continuously for at least 24 hours. These are taking two directions – monitor devices implanted directly in the eye requiring invasive surgery, or temporary contact lens-based approaches,” said Dr Mansouri, a consultant ophthalmologist at the Glaucoma Sector, Geneva University Hospitals, Geneva, Switzerland.
He contrasted the current situation of a glaucoma specialist with that of a diabetes specialist. A diabetes specialist may see a patient only four times a year, but is able to take a standard measurement to help determine how well the patient is controlled. A glaucoma specialist may also see a patient four times in a year, but relies on a single ‘snapshot’ IOP reading, knowing that that measure can fluctuate quite a bit over time.
“You take one measurement that can fluctuate between 15 mmHg and 21 mmHg. Is this patient well controlled or not? It is hard to say. You now also might have access to hospitalisation that can give you a series of 24-hour diurnal measurements, but these are cumbersome and can also fluctuate. We know from research that we miss peak pressures in as many as two of three patients.”
IMPLANTABLE DEVICEOne approach to continuous IOP monitoring that has been tested in animals and is now entering clinical trials is an implantable device with pressure sensors that were borrowed from the automobile industry. The advantage of this approach would be that it provides round-the-clock measurements. However, the downside is that it requires invasive surgery via a 6.0mm limbal incision for implantation of the device.
Researchers at the University of Alabama, US have developed an implantable system that wirelessly records 500 measurements of IOP per second. The sealed telemetric sensor implant has been tested in non-human primates for two-and-a-half years. Such a system could be very useful in that it provides real IOP measurements over long periods of time. However, there are still significant concerns regarding the safety of that approach. If the device drifts, surgery could be required. Moreover, there could be the potential of leakage of toxic compounds from the sealed implant, Dr Mansouri noted.
An entirely different approach involves the use of non-invasive contact lens-based IOP monitoring. Dr Mansouri has been involved in clinical trials with the Triggerfish sensor from the Swiss company Sensimed. The Triggerfish, approved in the EU but not in the US, is a soft contact lens embedded with strain gauges in the periphery that can measure radial deformation of the eye near the corneoscleral junction due to changes in IOP and ocular volume. It includes an antennae that transmits data to an external recorder. It takes measurements every five minutes. This information can then be downloaded by the clinician in the office.
Since the device does not measure actual IOP, its developers are working to devise a system to convert the strain gauge changes with IOP equivalents. In sleep lab and other clinical studies the measurements provided by the device do appear to correspond to
IOP changes. “We are measuring volume changes rather than the intraocular pressure that everyone is familiar with. The changes are relative rather than absolute. The biggest challenge will be how to interpret the data. We are going from looking at two seconds of data to 60,000 seconds of measurements. We are going from a problem of small data to a problem of big data,” Dr Mansouri observed.
Kaweh Mansouri: [email protected]
SLT LaserSelective Laser Trabeculoplasty
Bessemerstr. 1490411 Nürnberg Germany +49 (0) 911 217 79-0
Glaucoma Treatment Made in GermanyReliable ... Trusted
Anzeigenserie-ESCRS EuroTimes_08_2013.indd 1 29.07.2014 18:08:57
Example of 24-hour IOP pattern monitoring with the Triggerfish contact lens sensor. The inbuilt software allows automated cosinor rhythmometry analysis as well as automated detection of blinks and the ocular pulse amplitude
C
Cour
tesy
of K
aweh
Man
sour
i MD,
MPH

NICE15th EURETINA Congress
17 – 20 September 2015Acropolis, Nice, France

31
EUROTIMES | OCTOBER 2014
GLAUCOMA
isc haemorrhages increase the risk of progression threefold in eyes with glaucoma, not because the lesions cause progression, but because they are a manifestation of a progressive neurodegenerative disease process, said Jeffrey Liebmann MD, New York
University School of Medicine, New York, US. “For research, that means we can consider using disc
haemorrhage as an endpoint in our clinical trials. For practising clinicians it means that the disc has to be examined at every visit,” Dr Liebmann told the 11th Congress of the European Glaucoma Society in Nice and that the presence of a disc haemorrhage should alter physician behaviour, either with respect to management and/or surveillance.
Disc haemorrhage has reported prevalence rates of 12 per cent to 15 per cent in primary open-angle glaucoma and 15 per cent to 20 per cent in normal tension glaucoma. Moreover, research suggest that the progression rate in eyes with the lesion ranges can be as high as 80 per cent when one lesion is present and 100 per cent when there are two or more.
The cause of disc haemorrhage is unknown, and some investigators have suggested that it is primarily a vascular injury. However, there is a great deal of evidence that its occurrence is part of the process of glaucoma structural progression.
For example, the haemorrhages always occur at the edge of a nerve fibre layer defect or at the edge of an area of rim abnormality in the disc. They typically appear in areas where there is previous damage or at the edge of those damaged areas and indicate that the disease is worsening at that location.
“This implies that the notch and the nerve fibre layer loss are all part of the same degenerative process of the optic nerve head complex and the disc haemorrhage is just a transient manifestation of that ongoing process,” Dr Liebmann said.
STRONG STRUCTURE/FUNCTION CORRELATIONThe area of the disc haemorrhage almost always corresponds closely to an area of visual field loss. Before the haemorrhage occurs, progressive visual field loss can already present in the area of the visual field corresponding to the haemorrhage.
Because disc haemorrhages are such strong indicators of glaucomatous progression, the treating physician must be vigilant. Other risk factors for glaucoma progression include higher intraocular pressure, older age, exfoliation syndrome, thinner cornea and a beta-zone parapapillary atrophy, he added.
“If you have a disc haemorrhage, I think you have to act. You may want to change the way you monitor the patient, perhaps initiate treatment, if you haven’t already, and consider whether advancing treatment might be in the patient’s best interest,” said Dr Liebmann.
Standard ophthalmoscopy through an undilated pupil is a useful part of every examination for glaucoma. “In spite of the fact that we have very expensive imaging devices, don’t throw away your ophthalmoscope or your indirect lens, and do look for disc haemorrhages at every visit,” he concluded.
Jeffrey Liebmann: [email protected]
Disc haemorrhages a prompt for closer monitoring.Roibeard O’hEineachain reports
STRONG INDICATORS
www.haag-streit.com
LENSTAR LS 900Improving outcomes.
Sophisticated IOL Prediction The on-board Olsen formula, combined with mea-sured lens thickness provides the surgeon with premium IOL power prediction results in all kind of eyes.
T-Cone Toric PlatformTrue Placido-Topography of the optional T-Cone complements the LENSTARs comprehensive meas-urement palette. Intuitive graphical planning of the toric intervention based on latest IOL calculation technology by Prof. Barrett is provided to the sur-geon in the optional EyeSuite IOL Toric Planner.
Automated Positioning System APSTaking biometry measurements has never been easier. LENSTAR APS assists the user with dynamic eyetracking, facilitating measurement acquisition with one click.
See us at
AAO ‘14
Booth #3319
ADV_LENSTAR_APS_Eurotimes_AAO_20-08-2014.indd 1 05.09.2014 14:59:13
D

ctive psychological therapeutic intervention can provide significant benefits in patients with vision loss from bilateral age-related macular degeneration (AMD), a new study suggests.
Published online in the journal Ophthalmology, the Low VIsion Depression Prevention TriAL (VITAL) study highlights
the high risk of depression in patients with AMD and should reinforce for ophthalmologists the importance of a holistic approach to providing services for these individuals.
“Although retina specialists often focus on vision as the outcome of interest in our patients, this study reminds us that people value vision because it allows them to maintain independence and continue to enjoy certain activities. To optimise care for patients with AMD, we need to think about the patient as a whole rather than looking only at vision,” said Allen C Ho MD, director of retina research Wills Eye Hospital and professor of ophthalmology Sidney Kimmel Medical College of Thomas Jefferson University, Philadelphia, PA, US.
Barry W Rovner MD, is principal investigator for VITAL and professor of neurology and psychiatry, Sidney Kimmel Medical College of Thomas Jefferson University. He told EuroTimes that the study is important for getting ophthalmologists to recognise depression in patients with AMD as a preventable and treatable problem. “Depression in older patients who have lost vision is commonly seen as an understandable reaction, but explaining the depression away in that manner is a nihilistic perception that fails to address the problem. The VITAL study helps to underscore that depression is a medical problem that deserves our full medical and psychological attention,” he said.
The study included 188 patients with vision loss from AMD (BCVA <20/70 in the better eye), sub-syndromal depressive
symptoms identified using the Patient Health Questionnaire-9 and moderate difficulty performing a valued vision-dependent activity. All patients initially received low vision rehabilitation services and then were randomised to supportive therapy delivered by a masters-level therapist, or behaviour activation (BA) therapy delivered by an occupational therapist.
Each approach involved six in-home one-hour sessions over an eight-week period. Supportive therapy is a psychological treatment designed to provide emotional support and controls for attention. BA addresses both depression and functional deficits of vision loss and is a structured, individualised treatment plan incorporating environmental modifications and action plans designed to address the specific barriers a patient faces in accomplishing valued personal and functional goals.
“The guiding concept underlying behaviour activation intervention is the link between action, mood and mastery,” said Dr Rovner. “It recognises that when people have greater confidence in their abilities, they can do more and will feel better.”
Progression to major or minor depression (DSM-IV criteria) after four months was evaluated as the primary outcome. BA cut the rate by half. Progression to severe depression occurred in 23.4 per cent of the supportive therapy patients, which is consistent with published data on the prevalence of depression among patients with AMD, but in only 12.6 per cent of patients receiving BA therapy. Follow-up is ongoing and a future analysis will investigate whether the benefit of BA observed after four months is sustained at one year.
Findings from other assessments showed patients who received BA demonstrated greater improvements in near functional vision than the control group and remained more socially engaged.
An effectiveness analysis showed that nine patients would need to be treated to prevent one additional case of depression. Considering the subgroup of patients with worse baseline vision (<20/100 in the better eye), the benefit of BA was even stronger as the number needed to treat (NNT) for that cohort was only five. To put some perspective onto those numbers, the investigators noted the NNT is 38 for intensive glycolic control over four years to prevent one case of clinically important diabetic retinopathy.
Dr Rovner also pointed out that while there are costs involved in delivering the integrated low vision and BA treatment, they are relatively small weighed against the economic and other burdens of depression and the sequelae of an accident and injury that results because of low vision.
Allen C Ho: [email protected] W Rovner: [email protected]
32 RETINA
EUROTIMES | OCTOBER 2014
Collaborative mental healthcare VITAL. Cheryl Guttman Krader reports
DEPRESSION AND AMD
Assistive cooking devices. The spoons allow the user to feel the measurement, identified by the number of rounded black stickers on each spoon, rather than see
the numbers written on the spoon
EYE CHATExclusive interviewsUp to date informationProblem solving
podcastwww.eurotimes.org
Also available on iTunes
Scan this QR code to gain access to EuroTimes podcasts
Dr Oliver Findl talks to Dr Minoru Tomita who has performed more than 15,000 implants
Corneal Inlays
A
Cour
tesy
of B
arry
W R
ovne
r MD

33
EUROTIMES | OCTOBER 2014
Research on cell-based therapy for retinal degenerative disease has progressed from laboratory-based experiments performed in preclinical models to early phase clinical trials. With this transition, cell-based therapy has taken an important step forward toward becoming an innovative strategy for
preserving or restoring vision in patients affected by a variety of incurable blinding diseases. Therefore, the time seemed right to compile and publish the first textbook on cell-based ocular therapy, according to Ricardo P Casaroli-Marano MD, PhD and Marco A Zarbin MD, PhD, volume editors of Cell-Based Therapy for Retinal Degenerative Disease.
“Recent advances in cellular and molecular biology have increased our understanding of the pathophysiological mechanisms underlying retinal degenerative diseases and consequently enabled expansion of translational research. Therefore, it seemed appropriate to develop a text exploring applications of stem cell therapy to the treatment of these major causes of blindness,” said Dr Casaroli-Marano, professor and researcher, Department of Surgery and Surgical Specializations (School of Medicine), University of Barcelona, Spain.
Dr Zarbin noted that with the entry of cell-based therapy for retinal degenerative diseases into human studies and as the numbers of those trials are growing, various groups of individuals will have an interest in learning more about this topic.
“This book provides a comprehensive, scholarly and practical resource for a broad audience of readers,” said Dr Zarbin, the Alfonse Cinotti MD/Lions Eye research professor and chair, Institute of Ophthalmology & Visual Science, Rutgers-New Jersey Medical School, Newark, NJ.
REFERENCED CHAPTERSThe book features 15 referenced chapters that are written by 44 contributors who represent leading experts in their fields. “Potential readers only need to read the preface of the book to determine whether or not it will be helpful to them,” Dr Zarbin said. “Then, with its list of contributors and the references at the end of each chapter, the book provides an excellent starting place for identifying personal contacts and material for further reading for anyone who wants to develop a more mature understanding of a particular topic.”
Marco A Zarbin: [email protected] P Casaroli-Marano: [email protected]
Book explores stem cell therapy and treating causes of blindness. Cheryl Guttman Krader reports
CELL-BASED THERAPY
RETINA
This book provides a
comprehensive, scholarly
and practical resource for a
broad audience of readers
Marco A Zarbin MD, PhD

SAN DIEGOAPRIL 17–21
A joint meeting with
AnnualMeeting.ascrs.orgAll programming will be held in the San Diego Convention Center.
THE LARGEST U.S. MEETING DEDICATED TO THE ANTERIOR SEGMENT SPECIALIST
THE LEADING PRACTICE MANAGEMENT PROGRAM IN OPHTHALMOLOGY
ASCRS GLAUCOMA DAYASOA WORKSHOPSTECHNICIANS & NURSES PROGRAM
BOOK HOUSING TODAY
REGISTRATION OPENS—NOVEMBER 5
FOLLOW @ASCRSTWEETS ON TWITTER. #ASCRSASOA2015

LONG-TERM RELEX RESULTSFemtosecond laser-assisted refractive lenticule extraction (ReLEx-FLEx) is a new treatment for myopia and myopic astigmatism. It uses the femtosecond laser to create a flap and with a second lamellar interface, a refractive lenticule for removal of corneal tissue. It has developed further and uses the laser to create just a lenticule (without a flap), which is removed through a small incision. German researchers report five-year follow-up results of a prospective clinical trial of refractive lenticule extraction. All 41 of the 108 eyes available for follow-up were within 1 D of the intended correction and 73 per cent were within ±0.50 D. No eye had lost two or more Snellen lines. One eye had lost one Snellen line. The mean regression was 0.07 D. “Several long-term studies have been published and provide evidence to support the hypothesis that the refractive lenticule extraction technique is a viable alternative treatment,” notes T Kohnen in an editorial. M Blum et al., JCRS, “Five-year results of refractive lenticule extraction”, Volume 40, Issue 9, 1425-29.
NEW READING EVALUATION TOOL An electronic reading desk (Salzburg Reading Desk-Advanced) was developed to measure different aspects of reading performance under standardised conditions. Contrast and luminance levels can be preset by the examiner, and reading distance, reading acuity and reading speed are measured continuously and automatically during the examination. Any logarithmically scaled reading chart can be used in this setup. A new study compares the utility of this test with conventional methods. The first part of the study evaluated 100 eyes of 50 pseudophakic patients. Differences between the electronic reading desk and the printed version were small and not significant for reading speed, distance and print size. A second study found that reading acuity and the smallest possible read print size decreased with lower contrast and reduced luminance, whereas reading distance and reading speed did not change significantly. The researchers believe the new test could be useful for standardising results in clinical trials. N Hirnschall et al., JCRS, “Evaluation of an electronic reading desk to measure reading acuity in pseudophakic patients”, Volume 40, Issue 9, 1462-68.
SULCUS-FIXATED IOL EXCHANGENegative dysphotopsia following cataract surgery and IOL implantation can produce very unhappy patients. A new prospective study recruited patients who had developed this complication and subsequently underwent IOL exchange. Five eyes of five women with negative dysphotopsia were treated with IOL exchange and replacement with a 3-piece IOL (AcrySof MA60AC) inserted in the ciliary sulcus. The negative dysphotopsia resolved in all patients. One patient had primary insertion of a sulcus IOL in the fellow eye
and did not develop negative dysphotopsia symptoms. T burke et al., JCRS, “Sulcus-fixated intraocular lens implantation for the management of negative dysphotopsia”, Volume 40, Issue 9, 1469-72.
THOMAS KOHNEN European editor of JCRS Become a member of ESCRS to receive a copy of EuroTimes and JCRS journal
JCRSHIGHLIGHTSVOL: 40 ISSUE: 9 MONTH: SEPTEMBER 2014
35JCRS
EUROTIMES | OCTOBER 2014
OCULUS Corvis® ST – the world’s first seeing tonometerTonoPlus® technology – an advancement in tonometry which is leading us out of the dark. Whereas classic tonome-ters merely calculate pressure values, the OCULUS Corvis® ST creates in only one second over 4,000 detailed ultra-high-speed Scheimpflug images of the deforming cornea. This gives you highly precise tonometric values along with a com-pletely new view of the corneal biomechanical properties.
Tonometry has a bright future – and the Corvis® ST is illuminating its path.
www.oculus.de
Times of blindnessare over

EUROTIMES | OCTOBER 2014
36 INDUSTRY NEWS
RETINA CAMERATopcon Medical Systems has announced the release of the fully automatic TRC-NW400 Non-Mydriatic. "This innovative retinal camera introduces a new concept in digital photography of the eye where high-quality imaging meets ease of use," said a Topcon spokeswoman. "Operators no longer have to take time to align, centre, focus and capture colour retinal images. www.topconmedical.com
NEW PRODUCTSCenterVue launched two new products, Eidon and Compass, at the XXXII ESCRS Congress in London. “Eidon is the first true-colour confocal scanner in the eye care market,” said a company spokeswoman.”Eidon provides unsurpassed image quality, 60° field in a single exposure,” she said.
CenterVue also launched Compass which it described as the first fundus perimeter capable of performing standard 24-2 visual field testing while delivering true colour confocal images.
“These devices will benefit eye care specialists by providing highest quality in fundus visualisation and new tools for the management of glaucoma,” said Marco Morales, CenterVue’s chief scientific officer.www.centervue.com
INDUSTRY
NEWS
AT THE INTERSECTION OF IDEAS AND IMPLEMENTATION.
REGISTER AND SECURE YOUR RESERVATION TODAY
sideXside.ascrs.org
FEBRUARY 12–15, 2015
TURNBERRY ISLE MIAMI, AVENTURA, FLThis world-class resort is ideally situated in southern Florida.
Take advantage of deeply discounted group rates.
Join us for a newly designed meeting for anterior segment eye surgeons and practice administrators. This is your step-by-step guide on how to implement the latest ophthalmology innovations into real-world practice.
PHYSICIANS PROGRAMInteractive didactic sessions in the mornings and hands-on skills transfer sessions in the afternoons.
CHAIRSEdward J. Holland, MD Roger F. Steinert, MD Stephen S. Lane, MD
PROGRAM OUTLINE (Subject to Change) • ’Stigmatism • Cataract Surgery Challenges and Complication • Corneal Issues in Cataract Surgery • Glaucoma Therapy in 2015: MIGS, MEDS, and Beyond• Evolving Technology in Cataract Surgery• Retinal Injections

37INDUSTRY NEWS
EUROTIMES | OCTOBER 2014
Pole Position.HigH Performance system:
maximum Performance tHrougH soPHisticated tecHnology.
new!
www.geuder.com
Visit us at tHe
aao / cHicago 18 – 21 october,
bootH no. 2900
RZ_Anz_S4_Eurotimes_AAO_93x266_09_2014.indd 1 29.09.14 16:16
NEWS IN BRIEFEXCELLENT OUTCOMESThe first SCHWIND multicentre study on PresbyMAX Hybrid documents excellent clinical outcomes, said a SCHWIND spokeswoman. “A total of 372 eyes in 186 myopic, hyperopic and emmetropic patients were analysed,” she said. The average patient age was 53±6 (range 44 to 70 years of age). All the patients were observed for six months or longer postoperatively. The preoperative defocus ranged from -8.37 to +5.50 D. Astigmatism was treated up to 3.75 D. The planned addition was up to 2.75 D.www.eye-tech-solutions.com
CE MARK APPROVALQuantel Medical has announced CE Mark approval for its VitraTM PDT photodynamic therapy laser platform, for the treatment of polypoidal choroidal vasculopathy (PCV) and central serous retinopathy (CSR). “Quantel, the sole manufacturer of this laser technology, plans to begin commercialising the laser platform immediately in countries requiring CE PCV registration,” said a company spokeswoman.www.quantel-medical.com
INTREPID STUDYOraya Therapeutics announced that results of three-year safety follow-up data from the INTREPID study of Oraya Therapy for wet AMD demonstrated a favourable safety profile and showed that there was no significant difference in vision outcomes in patients treated with Oraya Therapy compared with those receiving anti-vascular endothelial growth factor (anti-VEGF) injections alone. “Oraya Therapy uses low-energy, highly targeted X-rays to treat wet AMD and is intended as a one-time procedure with the potential to maintain vision while reducing the required number of anti-VEGF injections into the eye,” said a company spokeswoman.www.orayainc.com
CORNEAL ASTIGMATISM FUNCTIONALITYi-Optics has announced new Cassini Corneal Analysis functionality designed to measure both anterior and posterior astigmatism, providing refractive-cataract and cornea surgeons with a Total Corneal Astigmatism (TCA) measurement. “Previous clinical studies have demonstrated that posterior corneal astigmatism could be a factor in generating unexpected postoperative outcomes,” said a company spokesman.
“Cassini provides critical information to properly select the power and position of Toric intraocular lenses (IOLs), as well as surgical planning for arcuate and limbal relaxing incisions,” he said.www.i-optics.com
NEW INTRAOCULAR LENSAbbott announced positive results from studies of
the new TECNIS Symfony Extended Range of Vision Intraocular Lens (IOL) at the XXXII ESCRS
Congress in London. "The data presented at the meeting show the TECNIS Symfony IOL offers
a substantial improvement in the range of vision for patients, while still minimising undesired haloes or glare," said Gerd U Auffarth MD, professor and chairman,
Department of Ophthalmology, Ruprecht-Karls University of Heidelberg, Germany.
www.amo-inc.com

38 TRAVEL
Four key experiences that delegates to the ESCRS winter meeting can enjoy. Maryalicia Post reports
METRO TO ASIAIt’s a purely Istanbul experience... hop on a metro in Europe and find yourself in Asia 19 minutes later. Marmaray, the Number 5 metro line, runs for one-and-a-half kilometres of its journey through a tunnel bored under the Bosphorus. The metro supplements the crowded bridges and ferries that link the two continents. The line was finally inaugurated, after a nine-year delay, in 2013; the tunnel diggers turned up hundreds of thousands of archaeological finds including the submerged remains of 36 Byzantine ships. (A new museum will be built to house the artefacts.) In Uskudar, on the Asian side, the gigantic mosque,Yeni Valide Camii, is inland from the harbour. Explore the streets behind this mosque and you’ll find a covered market plus the colourful Kite Museum. Admission free... Open 9-5, closed Sundays.
BARGAIN IN A MARKETEvery week 200 markets display their wares in Istanbul. The oldest and biggest is the Grand Bazaar which has been doing business since the15th century. Go for the atmosphere and the photo opportunities that are everywhere along its 58 covered streets.You might even spot a bargain. Open 09:00 to 19:00 but closed Sundays. The smaller Egyptian market (also called the Spice Market) is open every weekday 09:00 to 19:00 as well as Sundays from 10:00-18:00. Ozer, Stall 82 in the Spice Market, is a well-regarded antique and textile shop. It specialises in hand-woven silk scarves and restored antique clothes for women.
MARVEL AT A MOSQUE So many mosques (over 3,000), so little time. Which to see? How about the mosque of Suleymaniye the Magnificent. It’s the iconic mosque on Istanbul’s
skyline. It reopened in November 2010 after three years of refurbishment. Some say it is the most beautiful mosque in Istanbul; it is the largest. Built in the 16th century, it is lighter and less ornate than many of its contemporaries and has a peaceful atmosphere all its own. It’s within walking distance of the Spice Market. Visitors welcome except during prayers.
HAVE A HAMAMTurkish baths, hamams, are world famous. Traditionally, men and women bath separately. An exception, and therefore popular with tourists, is the 16th century Suleymaniye Baths next to the Suleymaniye Mosque. Couples and families only. Singles might try the utterly luxurious Kilcali Ali Pasa hamami. It reopened in 2012 after seven years of meticulous restoration. Make a booking, read a guide to the process and acquaint yourself with hamam etiquette on the hamam’s website: www.kilicalipasahamami.com or www.suleymaniyehamami.com.
ESSENCE OF ISTANBUL
ISTANBUL
ISTANBULTIME: Eastern European Standard - GMT+2WEATHER IN FEBRUARY: Average 3oC to 8oCTAXI TIP: Just round up the fare
Curious about the “Maiden’s Tower” on the island off Uskudar? A short boat ride from Salacek (near Uskudar on the Asian side) or Kabatas on the European side is all it takes to reach the island for a close-up look. Since 2000 it has been possible to enjoy a coffee or a meal in the tower’s cafeteria or restaurant. The tower has quite a long history – dating from 340 BC. It has been destroyed and rebuilt a couple of times, served as a tax collection station, a quarantine and a lighthouse and features in at least three legends... only one of which has a happy ending for the Maiden involved. The stories are the subject of a series of murals in the tower. Ferries leave frequently from either shore and cost 5TRY from Asia, 7TRY from Europe; free after 18:45 in the evening. The view at sunset is worth seeing.
You won’t go far in Istanbul without running into Turkish Delight for sale. A box of the gelatinous sweets makes a good packable souvenir. To take home the very best involves a foray into the back streets behind the Spice Market. Enthusiasts agree the most delightful of Turkish Delights is made and sold by Altan Sekerleme, a neighbourhood shop established in 1865. Little English is spoken – but the generous samples say it all. The two most famous varieties are the rosewater and the pistachio. Address: Kible Çesme Caddesi. No: 68 Eminönü, www.altansekerleme.com
Get in touch with your inner Ottoman. If you have ever wondered how you’d have looked as a pasha or a pasha’s favourite, this is your chance to find out; make a booking with Giyeck Nostalgic Photos. You will be encouraged to rummage through their collection of historic costumes and transform yourself. The resultant photos will be a unique souvenir of Istanbul. Prices depend on the number of photos – either printed or digital files – you choose. For example six photos cost 180 TRY. The studio is not far from the Galata Tower and Tunel Square on Istikial Street. Phone for directions and a booking: +90 212 251 8181 or contact them online: www.giyeck.com
3 TO TRY...
Marvel at a mosque
EUROTIMES | OCTOBER 2014
In Istanbul’s famous Spice Market

digital ad_ET September 2014.indd 1 9/24/14 9:34 AM
39BOOK REVIEWS
EUROTIMES | OCTOBER 2014
LEIGH SPIELBERG Books Editor If you have a book you would like to have reviewed please send it to: EuroTimes, Temple House, Temple Road, Blackrock, Co Dublin, Ireland
It is a question that is often asked of me as an ophthalmologist-in-training: “Doctor, why do you still wear glasses? Shouldn’t an eye doctor be able to see perfectly?”
Considering the success of refractive surgery and many patients’ misconceptions that lasers can cure all eye diseases, it’s an understandable question. And it sheds light on the notion that the success of modern eye surgery, and in particular cataract surgery, is increasingly judged by the refractive and astigmatic outcome.
Of course, much has been done to address refractive error at the time of cataract surgery. Significantly, toric lenses have provided ophthalmologists with a way to reliably correct the astigmatic error. A great deal of information exists regarding toric IOLs. However, little has been written about limbal relaxing incisions, an alternative method of astigmatic correction that can be performed at the time of cataract surgery. This need has perhaps become more urgent with the introduction of the femtosecond laser.
Limbal Relaxing Incisions: A Practical Guide, (Slack Incorporated), edited by Louis D Nichamin fills this void. A 100-page book, it is a concise but detailed introduction to the technique that covers the history of surgical correction of corneal astigmatism, the procedure’s indications, its technical aspects and management of potential complications.
Particularly useful is the chapter entitled, “This is How I Do It.” Here, six contributing authors offer their own techniques, including imaging, surgical plan and clinical pearls, such as the oft-repeated suggestion to plan conservatively for a slight undercorrection, as this is simpler to enhance, and more acceptable to most patients, than a slight overcorrection of the corneal astigmatism.
Limbal Relaxing Incisions is intended for novice refractive implant surgeons looking to incorporate incisional astigmatism surgery into their repertoire.
A BROADER VIEWFor those surgeons seeking a broader view of refractive surgery, “Refractive Surgery: An Interactive, Case-Based Approach” (Slack) might be a good choice.
Written by J Bradley Randleman, this 330-page book consists of a 75-page summary of the fundamentals of refractive surgery, followed by 36 fully-fledged case studies. The first half of the case studies cover the preoperative evaluation: the second half deals with the postoperative patient. Questions are posed, to which the reader can respond before proceeding to the answers. The answers are supplemented by detailed information, including corneal topography and analysis,
making this book ideal not only for ophthalmologists-in-training but also for resident and fellowship educators charged with teaching the next generation.
FILLING A VOID
BOOKREVIEWS
PUBLICATIONLIMBAL RELAXING INCISIONS
EDITORS LOUIS D NICHAMIN
PUBLISHED BY SLACK

40
Contact lens-assisted collagen cross-linking aims to overcome limitations of traditional cross-linking. Soosan Jacob reports
Traditional corneal collagen cross-linking (CXL) is limited to corneas with stromal thickness of greater than 400 microns in order to shield the endothelium from damaging UV rays.
In epithelium off cross-linking, 400 microns of stromal thickness above the endothelium should be available after epithelial removal. Thin corneas with pachymetry less than 400 microns after epithelial removal are therefore a challenge to cross-link.
However, there are many patients with keratoconus who have thinning that goes beyond this 400 micron limit for safe cross-linking. Within this sub-group of thin corneas, any amount of cross-linking may not provide sufficient strengthening to prevent progression in patients having advanced disease presenting with severe ectasia and thinning. A deep anterior lamellar keratoplasty (DALK) is a better choice in this group of patients. Within the same sub-group, however, there are also many patients who are not yet thin enough to indicate a DALK, yet thinner than the 400 micron cut-off. The treatment options for this group of patients is limited.
CONTACT LENS-ASSISTED COLLAGEN CROSS-LINKING (CACXL)This technique (which I started in 2013) may be utilised in such patients. CACXL acts by utilising the Beer Lambert law
which states that each unit layer of a solution absorbs an equal fraction of light passing through it. A UV barrier-free riboflavin-soaked soft contact lens is used to increase functional corneal thickness (stroma with contact lens). The contact lens used should be thin and should not have an in-built UV-barrier to avoid negating the effect. This may be checked in the product literature or by checking the UV irradiance that passes through the contact lens using a digital UV meter. We use the Bausch + Lomb daily disposable soft contact lens made of Hilafilcon B (Soflens™) for this purpose.
The minimum pachymetry is confirmed after epithelial removal and the point of minimum pachymetry is marked. The contact lens is then soaked in 0.1 per cent riboflavin solution for the same half hour that the de-epithelialised cornea is soaked. The soaked lens is then placed on the surface of the cornea and the pachymetry is remeasured to confirm that thickness has gone above 400 microns with the lens on. The absolute thickness of the soaked lens is 90 microns. An additional thin film of riboflavin under the contact lens adds slightly more to the thickness.
In our study, we found an average additional thickness of 107.9 ±9.4 microns attained by this technique. Once pachymetry is confirmed to be above 400 microns, UV-A application is done either following the classical Dresden protocol of 3mW/cm2 or as accelerated CXL. In case of accelerated CXL, our preference is to use an irradiance of 10 mW/cm2 for
A BETTER CHOICE
nine minutes. At the end of treatment, the contact lens is removed, riboflavin is washed off and a fresh soft contact lens is applied until complete epithelial healing.
SOLUTION AND PROTOCOLRiboflavin in Dextran T500 is a dehydrating agent and can lead to increased thinning of the cornea. Hence, it may be ideal to decrease the time of exposure to dextran in such patients. This may be done by utilising accelerated cross-linking or by using riboflavin 0.1 per cent in HPMC as a soaking solution.
OTHER TECHNIQUES Hypotonic CXL, epithelium on and epithelial island techniques are other techniques that have been described to perform CXL in this group of patients. Though these are excellent techniques, limitations include intra and inter individual variations in the level of swelling that may be obtained as well as limited penetration of riboflavin through intact epithelium.
COMBINATION TREATMENTSThe current treatment strategy should ideally focus on combination treatments
EUROTIMES | OCTOBER 2014
EYE ON TECHNOLOGY
Figure A: Preoperative ASOCT pachymetric map showing thinnest pachymetry of 421 microns
B: Postoperative ASOCT pachymetric map of same patient
C: 1.5 months’ postoperative slit lamp image of cornea following CACXL
D: Slit view of the cornea showing well-defined demarcation line

41EYE ON TECHNOLOGY
EUROTIMES | OCTOBER 2014
attaining a functional corneal thickness of 400 microns.
SEVERE KERATOCONUSIn very thin and steep corneas, DALK is preferable for the anatomic and visual rehabilitation that it provides. Such patients usually have a decreased best spectacle corrected visual acuity (BSCVA). However, they generally show very good visual potential on examination with a rigid gas permeable contact lens. Performing a DALK in such patients gives very good visual results because of the excellent flattening of the anterior chamber and a decrease in myopia that can be obtained by taking a same-sized graft.
Good astigmatism control may be obtained by intra-operative keratometry and if required by postoperative suture adjustment. A DALK also provides better anatomic rehabilitation in these extremely thin corneas. In contrast, the amount of visual rehabilitation that CXL would provide in these patients would not be sufficient and there would be poor improvement in both BSCVA and myopic astigmatism postoperatively. With CXL, the strengthening of extremely thinned out cornea is also likely to be insufficient and the disease may continue to progress. Such advanced corneas are also at greater risk for haze formation. Hence for the above-mentioned reasons, in advanced keratoconus with high keratometric values, I prefer to do a DALK.
* Dr Soosan Jacob is a senior consultant ophthalmologist at Dr Agarwal's Eye Hospital, Chennai, India and can be reached at: [email protected]
BARCELONAwww.eucornea.org
4 – 5 September 2015Fira Gran Via, Spain
6th EuCornea Congress
according to thickness. CACXL is started and proceeded with when pachymetry is confirmed to be above 400 microns after applying the soft contact lens. However, if thickness is found to be less than 400 microns, a few drops of distilled water is used to swell the cornea just enough to top up the deficient thickness. As the contact lens technique adds approximately 100 microns to thickness, the amount of additional swelling needed to take pachymetry above 400 microns is generally low and can be quickly attained by this means. Thus the principles of both CACXL as well as hypotonic CXL may be combined effectively without the need for large amounts of swelling or special hypotonic solutions. In any event, cross-linking should not be carried out without
E: Demarcation line as seen on ASOCT at a depth of 278 microns
Scan this QR code to go to video link
for surgery

Save the Date!
Make the most of your time whilein Chicago this fall and attend ourEyeWorld programs for additionalCME and an opportunity to network with your colleagues.
Registration opens September 2014
www.EyeWorld.org
CHICAGO 2014 Friday, October 17 –Monday, October 20, 2014
EW at AAO - Sept_Layout 1 8/12/14 8:16 AM Page 1

43RESIDENT’S DIARY
“PIPPA WANTS TO DO IT!” shouted my daughter right into my ear as I reached over
her to pull her ski boots on. “I CAN DO IT MYSELF!” she screamed before she collapsed in a fit of kicking, screaming, frustration and rage. “PIPPA CAN DO IT!”
Philippa is two years old and she wants to do everything to become self-sufficient, independent from the constant need to be helped. It doesn’t matter that everyone around her has to wait – she’s going to practise what she needs to do, because soon she’ll have to do it herself.
I recognise that feeling. I’m currently in the middle of my “Cataract 2” rotation, which is an incredible four-month period of nothing but cataracts. After this rotation, we’re expected to be capable of smoothly completing a standard phaco with reasonable precision. To get to that point, we spend three full days per week in the operating room, for 16 consecutive weeks. It’s surgical heaven.
The attending staff doctors are enthusiastic and motivated instructors. They each take the time to teach us this tricky procedure. However, they’re not interested in spending 40 minutes watching us struggle through an operation. The patient gets restless, the nurse gets bored and the waiting room starts to overflow. We have to be sharp and our learning curve must remain steep. To succeed, we have to fight for the right to operate, and for that, we have to be ready.
We each have our own way of preparing. Some read cataract surgery textbooks, watch surgical videos online or practise on a surgical simulator. Personally, I choose to seriously focus on observing the procedures performed by my attendings. What better way to learn how it’s done correctly than by watching a surgeon who performs more than 1,000 phacos per year?
We all talk with older residents, asking them all kinds of questions, to learn what we can expect from each of the surgical attendings. Each doctor seems to have their own expectations, teaching methods and techniques. “Dr So-and-so is particularly obsessive about the primary incision, so make sure you concentrate on that. Otherwise, he’ll take over before you even get any further.” Other doctors get very annoyed if the sterile drape isn’t perfectly placed, or if you touch the iris when inserting instruments into the anterior chamber, or if you sculpt too deep.
Some doctors perform bevel-up quadrant removal, worried about accidentally perforating the posterior capsule. Others are strictly bevel-down, in order to protect the corneal endothelium. A third group keeps the bevel parallel to the iris plane, realising that most of the quadrants’ movement are determined by the direction of irrigation flow in the eye.
After seeing the many possibilities, I opted for what I considered to be the best possibility for each step. I tried to do my first 100 solo procedures using as little variation as each particular case would allow. The goal was to master my own method from beginning to end.
I copied Dr Creten’s drape technique and emulated Dr van Rooij’s preoccupation with sterility. I tried to replicate Dr Reus’s multiplanar incision and perfectly circular capsulorhexis, followed by his reliable no-touch hydrodissection. I attempted to operate with Dr de Faber’s speed while trying to stay calm and collected, like Dr Zijlmans. Dr Lemij taught me how to perform a post-
op analysis of what could have gone better. Finally, Dr Nieuwendijk was my model for how to interact with the OR staff: firm and decisive but also friendly and fair.
A crucial aspect of being allowed to operate frequently was my selection of cases. Many are simply too risky for a resident, but standard cases are always available, and it is awful to miss those opportunities. So, I make sure to arrive at the operating room very early to screen all the day’s cases to determine which are perfect for my skill level; which are way out of my league; and which I might have to fight for. I then sit down, relax, drink an extra cup of coffee and imagine a flawless phaco in my mind while waiting for the attending to arrive.
Sometimes it’s obvious: a perfect patient and a perfect eye. Other times it’s less so, like a post-vitrectomy eye, or one with pseudoexfoliation. When I’m feeling particularly confident, I really push the envelope: an eye with +6.0 D hypermetropia, a shallow anterior chamber and a relatively small pupil requiring a 27 D IOL.
Sometimes it works and sometimes it doesn’t, but just like a young child, I have to fight to do as much as possible myself, because soon enough, it’ll all be my responsibility. I will do it myself.
Leigh Spielberg says raising a young child can teach trainees valuable lessons
‘PIPPA WANTS TO DO IT!’
Sometimes it works and sometimes it doesn’t, but just like a young child, I have to fight to do as much as possible myself...
EUROTIMES | OCTOBER 2014
Cour
tesy
of E
oin
Cove
ney

SEPTEMBERNEW ENTRYInternational Conference on Ocular Infections (ICOI)3–4 SeptemberBarcelona, Spainwww.ocularinfections.com
NEW ENTRY6th EuCornea Congress4–5 SeptemberBarcelona, Spainwww.eucornea.org
NEW ENTRY3rd World Congress of Paediatric Ophthalmology and Strabismus4–6 SeptemberBarcelona, Spainwww.wspos.org
NEW ENTRYXXXIII Congress of the ESCRS5–9 SeptemberBarcelona, Spainwww.escrs.org
NEW ENTRY15th EURETINA Congress17–20 SeptemberNice, Francewww.euretina.org
OCTOBER 2014EVER 2014 Congress1–4 OctoberNice, Francewww.ever.be
AAO Annual Meeting18–21 OctoberChicago, Illinois, USAwww.aao.org
NOVEMBERFemto Congress 20147–9 NovemberBudapest, Hungarywww.femtocongress2014.hu
94th SOI National Congress21–24 NovemberRome, Italywww.congressisoi.com
27th APACRS Annual Meeting13–16 NovemberJaipur, Indiawww.apacrs2014.org
Joint Irish/UKISCRS Refractive Surgery Meeting21 NovemberDublin, IrelandEmail: [email protected]
DECEMBER6th Amsterdam Retina Debate12 DecemberAmsterdam, The Netherlandswww.amc.nl/retinadebate
JANUARY 20159th International Congress ‘Macula of Paris’9 JanuaryParis, Francewww.maculaofparis.org
5th EURETINA Winter Meeting24 JanuaryOxford, UKwww.euretina.org
FEBRUARY73rd Annual Conference of AIOS5–8 FebruaryNew Delhi, Indiawww.aios.org
FEBRUARYInaugural Asia-Australia Congress on Controversies in Ophthalmology (COPHy A2)5–8 FebruaryHo Chi Minh City, Vietnamwww.comtecmed.com/cophy/aa/2015/
19th ESCRS Winter Meeting20–22 FebruaryIstanbul, Turkeywww.escrs.org
MARCH6th World Congress on Controversies in Ophthalmology (COPHy)26–29 MarchSorrento, Italywww.comtecmed.com/cophy/2015/
APRILASCRS.ASOA Symposium and Congress17–21 AprilSan Diego, CA, USAwww.ascrs.org/meetings-and-events
MAY6th Baltic Congress1–3 May Kiel, Germanywww.baltic-congress.de
ARVO Annual Meeting3–7 MayDenver, Colorado, USAwww.arvo.org
JUNESOE 2015 Congress6–9 JuneVienna, Austriawww.soe2015.org
↙LASTCALL
Istanbul
EURETINA Winter MeetingSaturday 24 January 2015
5th
Merton College, University of Oxford, UK
www.euretina.org
↙
44 CALENDAR

A NEW ERA HAS BEGUN,AND IT LOOKS AMAZING.Introducing TECNIS® IOL, the first and only presbyopia-correcting Extended Range of Vision IOL.
At last, your patients can enjoy increased spectacle independence with a true extended range of vision.1
• A full range of continuous, high-quality vision in all light conditions2
• Incidence of halo and glare comparable to a monofocal IOL1
• TECNIS® Symfony Toric IOL also available
The world will never look the same.
For more information, contact your Abbott Medical Opticssales representative.
1. 166 Data on File_Extended Range of Vision IOL 3-Month Study Results (NZ). 2. TECNIS® Symfony DFUTECNIS® Symfony Extended Range of Vision Lenses are indicated for primary implantation for the visual correction of aphakia and preexisting corneal astigmatism in adult patients with and without presbyopia in whom a cataractous lens has been removed by extracapsular cataract extraction, and aphakia following refractive lensectomy in presbyopic adults, who desire useful vision over a continuous range of distances including far, intermediate and near, a reduction of residual refractive cylinder, and increased spectacle independence. These devices are intended to be placed in the capsular bag. For a complete listing of precautions, warnings, and adverse events, refer to the package insert.TECNIS and TECNIS SYMFONY are trademarks owned by or licensed to Abbott Laboratories, its subsidiaries or affiliates.©2014 Abbott Medical Optics Inc., Santa Ana, CA 92705 www.AbbottMedicalOptics.com PP20140012
CATG-12722 Sept Media Ad-Symfony-EuroTimes.indd 1 8/6/14 11:33 AM

NEW ICARE HOME SELF-TONOMETER FOR EASY 24H IOP MONITORING BY OPHTHALMOLOGIST RECOMMENDATION