ERb Sensitizes NSCLC to Chemotherapy by …...DNA Damage and Repair ERb Sensitizes NSCLC to...
11
DNA Damage and Repair ERb Sensitizes NSCLC to Chemotherapy by Regulating DNA Damage Response Fotis Nikolos, Christoforos Thomas, Igor Bado, and Jan-Åke Gustafsson Abstract The expression of wild-type estrogen receptor b (ESR2/ERb1) correlates with clinical outcome in patients with non–small cell lung cancer (NSCLC). However, the molecular mechanism that accounts for this association is currently poorly understood. ERb1 was previously linked to chemotherapy response in patients with breast cancer and in breast cancer cells. The effect of the receptor in NSCLC cells after chemotherapy treatment, a common remedy for advanced NSCLC, has not been studied. Here, upregulation of ERb1 increases the sensitivity of NSCLC cells to treatment with doxorubicin and etoposide. This effect was primarily observed in p53-defecient NSCLC cells. In these cells, ERb1 either enhanced G 2 –M cell-cycle arrest by activating the checkpoint kinase 1 (Chk1) and altering downstream signaling or induced apoptosis. The expression of p63 target genes that control G 2 –M checkpoint activation was altered by ERb1 suggesting an ERb1–p63 transcriptional cooperation in lung cancer cells that affects DNA damage response (DDR). These results suggest involvement of ERb1 in the mechanism that regulates DNA damage response in NSCLC cells and support the potential predictive and therapeutic value of the receptor in clinical management of the disease. Implications: This study demonstrating the impact of ERb1 on chemosensitivity of NSCLC cells suggests the predictive value of the receptor for successful response of tumors to chemotherapy and the potential benefit of chemotherapy- treated patients from the use of ER ligands. Mol Cancer Res; 16(2); 233–42. Ó2017 AACR. Introduction Lung cancer is the most common cause of cancer-related deaths worldwide (1). Non–small cell lung cancer (NSCLC) comprises more than 85% of the diagnosed lung cancers and has a 5-year survival rate of 18% (2). Despite advances in methods of detection and availability of more treatment options, NSCLC is often diagnosed at an advanced stage and has poor prognosis. The standard of care for advanced NSCLC includes adjuvant chemotherapy and antineoplastic agents (3). These remedies are also indicated for patients with advanced disease and tumors with targetable genetic alterations that acquire resistance to treatment with kinase inhibitors (4). However, the efficacy of chemotherapy is limited due to intrin- sic or acquired resistance (5, 6). Mechanisms that are impli- cated in chemotherapy resistance include drug inactivation by detoxifying enzymes or increased efflux, increased DNA dam- age tolerance and repair, increased resistance to apoptosis, and activation of survival pathways that counteract the effects of the drugs (5, 7). Pathways that mediate drug resistance are currently being investigated to identify biomarkers for better selecting patients that will respond to first-line chemotherapy and targets to combat resistance through novel therapies (8). Cytotoxic agents elicit their effects through various mechan- isms that result in activation of DNA damage response and induction of apoptosis. Treatment with DNA-damaging agents arrests the cells in different phases of the cell cycle in a p53- dependent or independent manner. Nonmalignant cells that normally express functional p53 protein are primarily arrested in G 1 phase due to p53-mediated upregulation of p21, whereas p53-defective tumor cells activate the S- and G 2 –M-phase check- points (9). Targeted disruption of the remaining DNA damage response pathways in cancer cells with p53 deficiency increases the chemotherapy sensitivity through accumulation of DNA damage that activates the apoptotic machinery (9–11). This observation has led to therapeutic strategies that sensitize p53- deficient cancer cells to DNA-damaging agents by targeting the residual in these cells G 2 –M checkpoint (9). The potential role of estrogens in lung cancer biology and therapy is currently under investigation. Despite the suggested association of estrogen signaling with clinical outcome, the exact effects of estrogen on NSCLC and the mechanism of action are still poorly understood (12). Estrogens mediate their effects in target tissues by acting on estrogen receptor (ER) subtypes ERa and ERb (13). The expression of ERs has been associated with prognosis in NSCLC. While, the presence of ERa correlates with poor outcome (14, 15), conflicting data have been published regarding the clinical importance of ERb in the disease. High expression of wild-type ERb (ERb1) has been associated with better survival among men and worse outcome in women and nuclear ERb1 positivity predicts better response of lung adenocarcinoma to tyrosine kinase inhibitors (15–23). In contrast, high cytoplasmic Department of Biology and Biochemistry, Center for Nuclear Receptors and Cell Signaling, University of Houston, Houston, Texas. Note: Supplementary data for this article are available at Molecular Cancer Research Online (http://mcr.aacrjournals.org/). Corresponding Author: Christoforos Thomas, Department of Biology and Biochemistry, Center for Nuclear Receptors and Cell Signaling, University of Houston, 3517 Cullen Blvd, Houston, TX. Phone: 832-842-8806; Fax: 713-743- 0634; E-mail: [email protected] doi: 10.1158/1541-7786.MCR-17-0201 Ó2017 American Association for Cancer Research. Molecular Cancer Research www.aacrjournals.org 233 on August 12, 2020. © 2018 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from Published OnlineFirst November 8, 2017; DOI: 10.1158/1541-7786.MCR-17-0201
Transcript of ERb Sensitizes NSCLC to Chemotherapy by …...DNA Damage and Repair ERb Sensitizes NSCLC to...

DNA Damage and Repair
ERb Sensitizes NSCLC to Chemotherapy byRegulating DNA Damage ResponseFotis Nikolos, Christoforos Thomas, Igor Bado, and Jan-Åke Gustafsson
Abstract
The expression of wild-type estrogen receptor b (ESR2/ERb1)correlates with clinical outcome in patients with non–small celllung cancer (NSCLC). However, the molecular mechanism thataccounts for this association is currently poorly understood.ERb1 was previously linked to chemotherapy response inpatients with breast cancer and in breast cancer cells. The effectof the receptor in NSCLC cells after chemotherapy treatment, acommon remedy for advanced NSCLC, has not been studied.Here, upregulation of ERb1 increases the sensitivity of NSCLCcells to treatment with doxorubicin and etoposide. This effectwas primarily observed in p53-defecient NSCLC cells. In thesecells, ERb1 either enhanced G2–M cell-cycle arrest by activatingthe checkpoint kinase 1 (Chk1) and altering downstreamsignaling or induced apoptosis. The expression of p63 target
genes that control G2–M checkpoint activation was altered byERb1 suggesting an ERb1–p63 transcriptional cooperation inlung cancer cells that affects DNA damage response (DDR).These results suggest involvement of ERb1 in the mechanismthat regulates DNA damage response in NSCLC cells andsupport the potential predictive and therapeutic value of thereceptor in clinical management of the disease.
Implications: This study demonstrating the impact of ERb1on chemosensitivity of NSCLC cells suggests the predictivevalue of the receptor for successful response of tumors tochemotherapy and the potential benefit of chemotherapy-treated patients from the use of ER ligands. Mol Cancer Res;16(2); 233–42. �2017 AACR.
IntroductionLung cancer is the most common cause of cancer-related
deaths worldwide (1). Non–small cell lung cancer (NSCLC)comprises more than 85% of the diagnosed lung cancers andhas a 5-year survival rate of 18% (2). Despite advances inmethods of detection and availability of more treatmentoptions, NSCLC is often diagnosed at an advanced stage andhas poor prognosis. The standard of care for advanced NSCLCincludes adjuvant chemotherapy and antineoplastic agents (3).These remedies are also indicated for patients with advanceddisease and tumors with targetable genetic alterations thatacquire resistance to treatment with kinase inhibitors (4).However, the efficacy of chemotherapy is limited due to intrin-sic or acquired resistance (5, 6). Mechanisms that are impli-cated in chemotherapy resistance include drug inactivation bydetoxifying enzymes or increased efflux, increased DNA dam-age tolerance and repair, increased resistance to apoptosis, andactivation of survival pathways that counteract the effects ofthe drugs (5, 7). Pathways that mediate drug resistance are
currently being investigated to identify biomarkers for betterselecting patients that will respond to first-line chemotherapyand targets to combat resistance through novel therapies (8).
Cytotoxic agents elicit their effects through various mechan-isms that result in activation of DNA damage response andinduction of apoptosis. Treatment with DNA-damaging agentsarrests the cells in different phases of the cell cycle in a p53-dependent or independent manner. Nonmalignant cells thatnormally express functional p53 protein are primarily arrestedin G1 phase due to p53-mediated upregulation of p21, whereasp53-defective tumor cells activate the S- and G2–M-phase check-points (9). Targeted disruption of the remaining DNA damageresponse pathways in cancer cells with p53 deficiency increasesthe chemotherapy sensitivity through accumulation of DNAdamage that activates the apoptotic machinery (9–11). Thisobservation has led to therapeutic strategies that sensitize p53-deficient cancer cells to DNA-damaging agents by targeting theresidual in these cells G2–M checkpoint (9).
The potential role of estrogens in lung cancer biology andtherapy is currently under investigation. Despite the suggestedassociation of estrogen signaling with clinical outcome, the exacteffects of estrogen onNSCLCand themechanismof action are stillpoorly understood (12). Estrogens mediate their effects in targettissues by acting on estrogen receptor (ER) subtypes ERa and ERb(13). The expression of ERs has been associated with prognosis inNSCLC.While, the presence of ERa correlates with poor outcome(14, 15), conflicting data have been published regarding theclinical importance of ERb in the disease. High expression ofwild-type ERb (ERb1) has been associated with better survivalamong men and worse outcome in women and nuclear ERb1positivity predicts better response of lung adenocarcinoma totyrosine kinase inhibitors (15–23). In contrast, high cytoplasmic
Department of Biology and Biochemistry, Center for Nuclear Receptors and CellSignaling, University of Houston, Houston, Texas.
Note: Supplementary data for this article are available at Molecular CancerResearch Online (http://mcr.aacrjournals.org/).
Corresponding Author: Christoforos Thomas, Department of Biology andBiochemistry, Center for Nuclear Receptors and Cell Signaling, University ofHouston, 3517 Cullen Blvd, Houston, TX. Phone: 832-842-8806; Fax: 713-743-0634; E-mail: [email protected]
doi: 10.1158/1541-7786.MCR-17-0201
�2017 American Association for Cancer Research.
MolecularCancerResearch
www.aacrjournals.org 233
on August 12, 2020. © 2018 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 8, 2017; DOI: 10.1158/1541-7786.MCR-17-0201

ERb1 levels define patients with worse overall survival (24).Consistent with the clinical associations, while a significantnumber of publications has reported proapoptotic effects of ERb1in prostate, breast, and colon cancer cells (25–27), other studiesassociated the receptor with the proliferative role of estrogens inbreast cancer cells (28). Similar to other cancers, contradictoryeffects of ERb have been reported on growth of NSCLC cells (29).We previously observed that upregulation of ERb1 induces cell-cycle arrest and apoptosis by inhibiting oncogenic RAS signaling(30). ERb has also been reported to sensitize cancer cells tochemotherapeutic agents. Upregulation of ERb1 or its splicevariant ERb5 enhanced the efficacy of doxorubicin and cisplatinin breast cancer cells (31, 32). Consistently, high expression ofERb1 has recently been associated with better prognosis in che-motherapy-treated ERa-negative breast cancer (33, 34). In addi-tion, ligand-mediated activation of ERb has been shown tosensitize malignant pleural mesothelioma cells to cisplatin andpemetrexed therapy by suppressing AKT signaling that leads toPARP-dependent proapoptotic cell death (35). These findingssuggest the involvement of ERb in the mechanisms that regulateDNAdamage response in cancer cells and indicate the potential ofthe receptor to alter the efficacy of chemotherapy in NSCLC cells.Investigation of the effect of ERb in chemotherapy response ofNSCLC cells was the focus of the current study.Here, we show thatERb1 increases the sensitivity ofNSCLC cells to chemotherapeuticagents by inducing G2–M cell-cycle arrest and apoptosis.
Materials and MethodsCell lines and reagents
NSCLC cancer cell lines (H1299, H661, H1944 and H358)were obtained from ATCC. They were cultured in RPMI-1640(Invitrogen) media supplemented with 10% FBS (Sigma-Aldrich), 13.5 mmol/L D-Glucose and 50 mg/mL kanamycin at37�C in a humidified incubator with 5% CO2. Doxorubicin,etoposide and nocodazole were purchased from Cell SignalingTechnology. Cisplatin (cis-Platinum(II)diammine dichloride)and caffeine were purchased from Sigma-Aldrich. ERb1 (Clone14C8) and p84 antibodies were purchased from GeneTex (36).The primary antibodies against p-Chk1 (S345), p-Chk2 (T68)were from Cell Signaling Technology. b-Actin and FLAG (M2clone) primary antibodies were obtained from Sigma-Aldrich.
Cell transfectionsERb1 expression constructs were generated by cloning the full-
length ERb1 in the pIRESneo or pLenti6/V5 expression vectors(Clontech Laboratories) as described previously (30, 37). H1299cells were transfected with empty pIRESneo vector or the recom-binant pIRESneo-ERb1 plasmid. H661, H1944, and H358 wereinfected with lentiviruses containing the empty plenti6/V5 vectoror the recombinant pLenti6/V5-D-FLAG-ERb1 plasmid asdescribed previously (37). H1299 cells were transiently trans-fected twice with p63-specific siRNAs (Invitrogen), targetsequences 1# 50-ATTCCATGGTCGTGTGAGACAGAAG-3, and2# 50-AACTTAAGCGCCGAGTCGAGTACA-30. A siRNA-targetingluciferase was used as a control (catalog. no. 12935-146,Invitrogen).
Cell survival assayControl and ERb1-expressing H1299, H358, H1944, and
H661 cells were plated onto 96-well dishes in 10% FBS-containing medium at a density of 5,000 cells/well and treated
with increasing concentrations of doxorubicin, etoposide orcisplatin (0–10 mmol/L) in quintuplicates. Seventy-two hourslater, the surviving portion of the cells was measured by theCell Titer-Blue cell viability assay, following the manufacturer'sprotocol (Promega). The IC50 values for the drugs in controland ERb1-expressing cells were calculated using GraphPadPrism 5 after estimating the mean of three independentexperiments.
RNA extraction and real-time PCRTotal RNA was isolated using Aurum Total RNA mini kit (Bio-
Rad) and reverse-transcribed to cDNA using the iScript cDNAsynthesis kit (Bio-Rad). Real-time PCR was performed using theiTaq SYBR Green kit (Bio-Rad). All quantitative data were nor-malized toGAPDH and 36B4. Primers sequences for the real-timePCR analysis of CCNG2 and p63 were CCNG2-FW: 5-TGGA-CAGGTTCTTGGCTCTT-3, CCNG2-RV: 5-GATGGAATATTG-CAGTCTTCTTCA-3, p63-FW: 5-AAGATGGTGCGACAAACAAGand p63-RV: 5-AGAGAGCATCGAAGGTGGAG-3.
Immunoblotting and immunoprecipitationCells were lysed in radioimmunoprecipitation assay (RIPA)
buffer (50 mmol/L Tris-HCl, pH 7.5, 150 mmol/L NaCl, 0.1%SDS, 0.5% deoxycholate, and 1% NP-40) containing protease(1 mmol/L EDTA, Roche protease inhibitor mixture, and2 mmol/L PMSF) and phosphatase inhibitors (1 mmol/L NaF,1 mmol/L Na3VO4, and Sigma phosphatase inhibitor mixture).The lysates were subjected to SDS-PAGE and the proteins weretransferred onto nitrocellulose membranes. Membranes wereblocked with 5% nonfat milk in TBST (0.05% Tween-20) for3 hours at room temperature and probed with the primaryantibodies overnight at 4�C. The membranes were incubatedwith secondary antibodies for 2 hours at room temperature.Proteins were visualized using enhanced chemiluminescence(ECL) detection reagents (Amersham Biosciences). We usedERb1 (Clone 14C8) and anti-FLAG antibodies to detect ERb1expression due to concerns raised recently regarding the efficacyof some ERb antibodies (36).
Flow cytometryCell-cycle progression of control and ERb1-expressing cells
after chemotherapy treatment was assessed by flow cytometry.After treatment, cells were trypsinized and fixed in 70% ice-coldethanol overnight at 4�C. Cells were resuspended in a propidiumiodide (100 mg/mL)/RNase A solution (50 mg/mL) and analyzedon a FACSAria II cell sorter (BD Biosciences). Analysis of cell-cycledata was performed using FlowJo software (Tristar Inc.).
ResultsERb1 sensitizes p53-defective NSCLC cells tochemotherapeutic agents
High expression of ERb1 has been associated with betterprognosis in chemotherapy-treated breast cancer patients (33).To investigate whether a similar association occurs in lungcancer, we tested the correlation between ERb1 and survivalin published Kaplan–Meier plotter datasets (38) and found thatchemotherapy-treated ESR2high NSCLC patients have betterclinical outcome compared with ESR2low patients (Supplemen-tary Fig. S1). We previously showed that induction of ERb1expression in NSCLC cells that express RAS oncoproteins
Nikolos et al.
Mol Cancer Res; 16(2) February 2018 Molecular Cancer Research234
on August 12, 2020. © 2018 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 8, 2017; DOI: 10.1158/1541-7786.MCR-17-0201

inhibits cell growth by disrupting RAS signaling (30). In thisstudy, we investigated whether upregulation of ERb1 sensitizesNSCLC cells to chemotherapy-induced cell death. To addressthis question, we stably expressed ERb1 in NSCLC cells withdifferent p53 status, given that p53 is critical determinant of theDNA damage response (39). We assessed cell survival in H1299and H358 cells that are null for p53, in H661 that carry mutantp53 and H1994 and A549 cells that express wild-type p53protein in the presence of increasing concentrations of cisplat-in, etoposide, or doxorubicin that are used in treatment ofNSCLC (40). Cell viability assays indicated a significant dose-dependent decrease in survival of doxorubicin and etoposide-treated p53-null H1299 and H358 cells after upregulation ofERb1. While in absence of treatment ERb1 decreased thesurvival of H1299 cells by less than 50%, in the presence of1 mmol/L doxorubicin upregulation of the receptor caused a
75% reduction in the viability of the same cells (Fig. 1A and B).In contrast, induction of ERb1 expression did not affect theviability of the cells that express mutant or wild-type p53 aftertreatment with the same chemotherapeutic drugs (Fig. 1C). Theeffect of ERb1 on NSCLC cells was drug-specific as upregulationof ERb1 did not alter the survival of any of the cell lines in thepresence of cisplatin (Fig. 1D). These results suggest a role forERb1 in sensitizing NSCLC cells to chemotherapeutic agents inthe absence of p53 expression.
ERb1 induces different cellular responses to chemotherapyin NSCLC cells
To elucidate the mechanism underlying the increased sensi-tivity of ERb1-expressing NSCLC cells to DNA-damagingagents, p53-defiecient control and ERb1-expressing H1299 andH358 cells were exposed to two different concentrations of
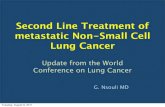
Figure 1.
ERb1 sensitizes p53-defective NSCLCcells to topoisomerase II inhibitors. A–C,Viability of control and ERb1-expressingH1299, H358, H661 (p53-defective), andH1944 (wild-type p53) NSCLC cellsfollowing treatment with increasingconcentrations of the topoisomerase IIinhibitors doxorubicin or etoposide. Bargraphs represent the mean of threeindependent experiments with SEM(P < 0.05). D, Cell viability was assesed incontrol and ERb1-expressing H1299 andH358 cells after treatment with increasingconcentrations of cisplatin. Calculation ofinhibitory concentration 50 (IC50) fordoxorubicin, etoposide and cisplatin incontrol andERb1-expressingH1299, H358,H1944, and H661 cells was performed byGraphPad Prism 6.0. IC50 values shown ineach graph represent mean of threeindependent experiments.
DDR in NSCLC is Regulated by ERb
www.aacrjournals.org Mol Cancer Res; 16(2) February 2018 235
on August 12, 2020. © 2018 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 8, 2017; DOI: 10.1158/1541-7786.MCR-17-0201

doxorubicin and etoposide for 48 hours and analyzed for cell-cycle progression by FACS. As shown in Fig. 2A, treatment withthese drugs arrested both control and ERb1-expressing H1299cells, due to absence of p53, in G2–M phase of the cell cycle in aconcentration-dependent manner. However, the percentage ofcells arrested in G2–M phase was significantly higher in ERb1-expressing compared with the control cells suggesting thatupregulation of the receptor leads to a stronger activation of
the G2–M checkpoint in the presence of DNA damage (Fig. 2A).Relative to H1299 cells, induction of ERb1 expression in H358cells under the same treatment did not increase the number ofcells that were arrested in G2–M phase. Instead, upregulation ofERb1 enhanced apoptosis as indicated by the increased sub-G1
cell population in ERb1-expressing cells after treatment withdoxorubicin and in less extent with etoposide (Fig. 2B). Sur-prisingly, although upregulation of ERb1 in H661 cells did not
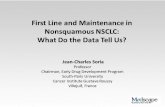
Figure 2.
ERb1 sensitizes NSCLC cells tochemotherapeutic agents throughdifferent mechanisms. A, Control andERb1-expressing H1299 cells weretreated with two differentconcentrations of doxorubicin (top)and etoposide (bottom) for 48 hours.Cell-cycle profiles were analyzed byflow cytometry after staining the cellswith propidium iodide (PI).Experiments were performed at leastthree times. B, Control and ERb1-expressing H358 cells were either leftuntreated or treatedwith two differentconcentrations of doxorubicin (top) oretoposide (bottom). Forty-eight hourslater, the cells were subjected tocell-cycle analysis by flow cytometry.C, Control and ERb1-expressing H661cells were treated with doxorubicinand analyzed by flow cytometry. Thegraphs in the left panels representthe percentage of cells in differentphases of the cell cycle from threeindependent experiments.� ,#, P < 0.05.
Nikolos et al.
Mol Cancer Res; 16(2) February 2018 Molecular Cancer Research236
on August 12, 2020. © 2018 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 8, 2017; DOI: 10.1158/1541-7786.MCR-17-0201

significantly alter their sensitivity to DNA-damaging agents(Fig. 1C), it abrogated the chemotherapy-induced G2–M-phasecell-cycle arrest as shown by the higher percentage of ERb1-expressing cells in G1 phase compared with the control cellsafter treatment with doxorubicin (Fig. 2C). Taken together,these results suggest that different mechanisms mediate theeffects of ERb1 on survival of NSCLC cells in response tochemotherapy treatment.
ERb1 regulates the activity of G2–M checkpoint effectors inNSCLC cells
Upon DNA damage, activation of ataxia telangiectasia,mutated (ATM) and ataxia telangiectasia and RAD3-relatedprotein (ATR) leads to activation of the checkpoint kinaseChk2 through phosphorylation at Thr-68 and Chk1 throughphosphorylation at Ser-345 (41, 42). Activation of Chk1 andChk2 causes G2–M-phase cell-cycle arrest (43). To identify themolecular mechanisms that are responsible for the strongercell-cycle arrest in ERb1-expressing NSCLC cells in presence ofchemotherapeutics, control and ERb1-expressing H1299 cellswere incubated with two different concentrations of doxoru-bicin and etoposide for 24 and 48 hours and the phosphory-lation status of Chk1 and Chk2 that indicates activationwas examined. In response to treatment, ERb1-expressing cellsdisplayed higher levels of Chk1 and Chk2 phosphorylationcompared with the control cells and the effect of the receptorappeared to be dependent on the dose of the drug and the timeof treatment (Fig. 3A). These results strengthen our findings
from the cell-cycle analysis showing that ERb1 induces G2–Marrest in response to DNA damage.
In contrast to H1299 cells, the phosphorylation of Chk1 washigher in control compared with ERb1-expressing H358 andH661 cells after treatment with doxorubicin or etoposide(H358) for 24 and 48 hours suggesting that ERb1 ratherinhibits the G2–M cell-cycle checkpoint in these cells(Fig. 3B and C). The inhibition of this specific DNA damageresponse pathway upon ERb1 upregulation is consistent withthe abrogation of the G2–M cell-cycle arrest that was detected inERb1-expressing H358 and H661 cells and may account for theenhanced apoptosis that was observed in ERb1-expressingH358 cells in cell-cycle analysis (Fig. 2B and C). Taken together,these results suggest that in response to DNA damage, ERb1differentially regulates the G2–M cell cycle checkpoint in dif-ferent p53-defective NSCLC cells.
ERb1 delays G2–M progression of NSCLC cells in responseto chemotherapy
To corroborate that ERb1 regulates the G2–M cell cyclecheckpoint in chemotherapy-treated NSCLC cells, we moni-tored cell-cycle progression in control and ERb1-expressingH1299 cells following treatment with doxorubicin in the pres-ence of nocodazole. Given that nocodazole arrests the cells inG2–M phase, we examined whether ERb1 delays the transitionfrom G2–M to G1 phase after the release of the cells fromnocodazole block (44). Following treatment for 18 hours withnocodazole, cells were released and treated for an additional
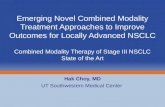
Figure 3.
ERb1 alters DNA damage response pathways in response to chemotherapeutic agents. A and B, Levels of phospho (p)-Chk1(S345), p-Chk2(T68) andERb1 in control and ERb1-expressing H1299 (A) and H358 (B) cells after treatment with two different concentrations of doxorubicin (left) andetoposide (right) for 24 and 48 hours. FLAG-ERb1 in H358 cells was detected with anti-FLAG antibody. Of note, ERb1 expression decreases with increasingconcentrations of etoposide. C, Expression of p-Chk1(S345) and p-Chk2(T68) in control and ERb1-expressing H661 cells following treatment withdoxorubicin for 24 and 48 hours.
DDR in NSCLC is Regulated by ERb
www.aacrjournals.org Mol Cancer Res; 16(2) February 2018 237
on August 12, 2020. © 2018 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 8, 2017; DOI: 10.1158/1541-7786.MCR-17-0201

6 hours with doxorubicin. As seen in Fig. 4A, 6 hours afterrelease from nocodazole block, a significantly higher percent-age of ERb1-expressing cells remained in G2–M phase of the cellcycle compared with the control cells.
Moreover, to strengthen our findings showing that ERb1prolongs G2–M phase arrest by acting on the pathway thatactivates Chk1, we assessed control and ERb1-expressing
H1299 cells after treatment with caffeine, a potent ATM/ATRinhibitor in the presence of doxorubicin (45). As shown inFig. 4B and C, treatment with caffeine reversed the ERb1-induced phosphorylation of Chk1 and the delay of the cellsinto G2–M phase, strengthening our initial hypothesis that inp53-deficient NSCLC cells, the receptor regulates the DNAdamage response pathways that control the G2–M checkpoint.
Figure 4.
ERb1 delays G2–M progression in NSCLC cells in response to chemotherapy. A, Control and ERb1-expressing H1299 cells were treated with doxorubicinin the presence of nocodazole (15 mg/mL) for 18 hours to induce G2–M arrest. Cells were incubated in media containing doxorubicin for another6 hours and the cell cycle was analyzed at 0 and 6 hours after nocodazole release. B, Immunoblot analysis of p-Chk1(S345) following treatment ofcontrol and ERb1-expressing H1299 cells with two different concentrations of doxorubicin in the presence of caffeine for 48 hours. b-Actin was usedas loading control. C, Cell-cycle analysis of ERb1-expressing H1299 cells upon treatment with doxorubicin in the presence of caffeine for 48 hours.Bar graphs on the right represent quantitative data of the percentage of cells in different phases of the cell cycle from three independent experiments.� ,#, P < 0.05.
Nikolos et al.
Mol Cancer Res; 16(2) February 2018 Molecular Cancer Research238
on August 12, 2020. © 2018 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 8, 2017; DOI: 10.1158/1541-7786.MCR-17-0201

Taken together, these results strongly suggest that in response toDNA damage, ERb1 leads to a prolonged G2–M checkpointactivation in NSCLC cells by regulating the induction of theDNA damage response pathway.
ERb1 synergizes with p63 to enhance the chemosensitivityof NSCLC cells
One of the mechanisms by which estrogen receptors elicittheir tumor-associated functions involves their transcriptionalcooperation with the p53-family proteins p53 and p63(46, 47). To further elucidate the molecular pathways thatmediate the effect of ERb1 on chemotherapy response ofNSCLC cells, we investigated whether ERb1 acts through p63in H1299 cells. These p53-null cells express high levels of p63and, thus, rely on this gene to activate the DNA damageresponse (Supplementary Fig. S2). As a transcription factor,p63 affects the expression of several genes that regulate cell-cycle progression including Cyclin G2 (CCNG2) that activatesthe G2–M cell-cycle checkpoint (48). It was previously shownthat CCNG2 is upregulated by ERb1 (46) and repressed by ERaand estrogen in cancer cells (49). We initially examined wheth-er disruption of p63 expression alters the effect of ERb1 onchemotherapy response of H1299 cells. Indeed, downregula-tion of p63 in ERb1-expressing H1299 cells reversed the ERb1-mediated G2–M-phase cell-cycle arrest (Fig. 5A) and phosphor-ylation of Chk1 and Chk2 (Fig. 5B). In addition, in response todoxorubicin treatment, knockdown of p63 in the same cellsreversed the upregulation of CCNG2 that seems to be essentialfor the ERb1-mediated G2–M-phase cell-cycle arrest (Fig. 5C).These results demonstrate the importance of p63 and itsdownstream signaling in mediating the effect of ERb1 onchemotherapy response of H1299 cells (Fig. 5D).
DiscussionChemotherapy remains the standard of care in management
of advanced NSCLC. However, disease progression and treat-ment–related toxicities continue to limit survival. Targetedtherapy is currently being investigated with the aim to improveoutcomes with less toxic effects (50). In addition to identifyingactivating mutations in targetable oncogenes including EGFRand ALK (51), recent studies have reported the expression ofestrogen receptors in NSCLC and implicated estrogen signal-ing in the development and progression of the disease. Thepresence of ERs in lung tumors indicates that targetablesignaling is no longer restricted to receptor tyrosine kinasesand their downstream effectors with the real possibility ofutilizing ERs as complementary prognostic markers and ther-apeutic targets (52). ERs have been associated with outcomesin patients with NSCLC and the regulation of survival inNSCLC cells. We previously observed inhibition of cell-cycleprogression and induction of apoptosis following upregula-tion of ERb1 in NSCLC cells with activating RAS mutations(30). Lung adenocarcinomas with undruggable RAS oncopro-teins belong to a large NSCLC entity that is still treated withconventional chemotherapy (51). In this study, we examinedwhether ERb1 increases the efficacy of chemotherapeuticagents in NSCLC cells.
Our experiments showed decreased cell survival in doxoru-bicin and etoposide-treated NSCLC cells after upregulation ofERb1. In contrast, expression of ERb1 did not alter the efficacy
of cisplatin suggesting that ERb1 acts as chemosensitizer in adrug-specific manner and its effect may be associated with themechanism of drug action. Treatment with doxorubicin andetoposide primarily induces G2–M cell-cycle arrest by inhibit-ing topoisomerase II activity (53) and further enhancement orabrogation of this specific cell-cycle arrest is likely to promotecell death (43). Our cell-cycle analysis shows that ERb1 altersthe activity of G2–M-phase checkpoint in doxorubicin- andetoposide-treated NSCLC cells but not in cells treated withcisplatin that, as an intercalating agent, stalls the cells largelyin S-phase of the cell cycle (54). Despite the common use ofcisplatin and etoposide in treatment of NSCLC, chemotherapyor chemoradiation therapy is complex and the agents neededto achieve optimal outcomes are currently not well defined(55). The chemosensitizing effect of ERb1 in doxorubicin-treated NSCLC cells may indicate the ability of the receptor toincrease the therapeutic index of agents that do not representstandard treatment. In addition to the drug-specific effect, ERb1seems to regulate chemotherapy sensitivity in cell context–dependent manner. We found that ERb1 decreases the viabilityof chemotherapy-treated NSCLC cells that lack p53 tumorsuppressor function. The absence of functional p53 proteinalters the DNA damage response of cancer cells and strategieshave been developed to target p53-defective tumors (56). Forexample, alteration of the increased cell-cycle checkpoint func-tion in G2 phase that occurs preferentially in p53-defectivecancer cells has been suggested to sensitize cancer cells toDNA-damaging agents (57). Thus, the amendment of theG2–M-phase checkpoint that was observed in ERb1-expressingNSCLC cells may account for their decreased survivalfollowing treatment with chemotherapy.
Further analysis of cell-cycle progression revealed two dis-tinct mechanisms of ERb1 action. In H1299 cells, ERb1 pro-longs the chemotherapy-induced G2–M cell-cycle arrest byincreasing the activity of the G2–M cell-cycle checkpoint indu-cers Chk1 and Chk2. This phenotype seems to rely on activa-tion of the DNA damage sensors ATM and/or ATR, as inhibi-tion of the pathway at this early stage diminishes the effect ofthe receptor. On the other hand, ERb1 decreased the viability ofchemotherapy-treated H358 cells by inducing apoptosis. H358cells are more sensitive to doxorubicin than H1299 cellsand this may account for the specific action of ERb1 in thesecells (58). Upon chemotherapy treatment, the active levelsof Chk1 were lower in ERb1-expressing compared with thecontrol H358 cells, suggesting that the receptor abrogates thedrug-induced G2–M cell-cycle checkpoint. The inhibition of theG2–M checkpoint under DNA damage may explain the che-mosensitizing effect of ERb1 in specific type of NSCLC cells (9).
The effect of ERb1 on ATM/ATR in H1299 cells implies thatthe receptor operates at an early stage during the DNA damageresponse to induce G2–M cell-cycle arrest. It is also evident thatERb1 regulates p53-independent DNA damage response path-ways in NSCLC cells. In absence of p53, other members of thep53 family of transcription factors such as p63 and p73 func-tion to activate the DNA damage response (59) and this mayrequire their increased expression in p53-deficient cells (60).Because of its differential expression in NSCLC cells in whichERb1 elicited distinct actions, p63 was considered as a potentialERb1-interacting factor. Knockdown of p63 reversed the effectof ERb1 on cell cycle of chemotherapy-treated NSCLC cells,indicating its involvement in the mechanism of ERb1 action.
DDR in NSCLC is Regulated by ERb
www.aacrjournals.org Mol Cancer Res; 16(2) February 2018 239
on August 12, 2020. © 2018 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 8, 2017; DOI: 10.1158/1541-7786.MCR-17-0201

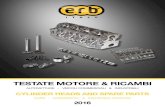
Figure 5.
ERb1 synergizes with p63 to enhance the chemosensitivity of NSCLC cells. A, ERb1-expressing H1299 NSCLC cells were transfected twice with scrambleor siRNA against p63 (sip63). Forty-eight hours later, the cells were treated with doxorubicin for an additional 48 hours and their cell cycle wasanalyzed by flow cytometry. B, Levels of p-Chk1(S345) and p-Chk2(T68) in ERb1-expressing H1299 cells after transfection with scramble or siRNAagainst p63 and treatment with doxorubicin for 48 hours. C, mRNA expression of CCNG2 in ERb1-expressing H1299 cells after transfection withscramble or siRNA against p63 and treatment with doxorubicin for 48 hours. D, Schematic representation of the mechanism employed by ERb1 toinduce G2–M cell-cycle arrest in response to chemotherapy treatment in NSCLC cells. ERb1 increases the activity of Chk1 and Chk2 that prolongs thechemotherapy-induced G2–M cell-cycle arrest. �,#, P < 0.05.
Nikolos et al.
Mol Cancer Res; 16(2) February 2018 Molecular Cancer Research240
on August 12, 2020. © 2018 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 8, 2017; DOI: 10.1158/1541-7786.MCR-17-0201

Moreover, we previously showed that ERb1 interacts with p63to promote upregulation of p63 target genes in breast cancercells (46). Among these, Cyclin G2 (CCNG2) is an estrogen-regulated gene that is activated by p63 to control the G2–M cell-cycle checkpoint (61, 62). We detected upregulation of CCNG2upon DNA damage in ERb1-expressing cells which strengthensour hypothesis that ERb1 influences chemotherapy response inNSCLC cells by regulating major DNA damage response path-ways (63).
In this study, we suggest that ERb1 affects the chemosensi-tivity of NSCLC cells and this may correlate with its ability toregulate DNA damage response pathways. The increased cyto-toxic effect of chemotherapeutics in NSCLC cells that lack p53in the presence of ERb1 suggests that chemotherapy-treatedpatients whose p53-defective lung tumors are positive for thereceptor may benefit from treatment with ER ligands. This effectmay also explain the previously reported association of ERb1with better survival in patients with NSCLC (16, 18). Given theexpression of the receptor in other tumors, its ability to alterchemotherapy response may impact on other types of chemo-therapy-treated cancers. As a support of this, high expression ofERb1 has recently been associated with better prognosis inchemotherapy-treated patients with ERa-negative breast cancer(33, 34). Thus, assessing the expression of ERb in cancerpatients including those with NSCLC might hold a predictivevalue for their successful response to chemotherapy. Furtherunderstanding of the transcriptional activity of ERb on targetgenes that regulate DNA damage response in lung cancer cells
should establish ERb as an important regulator of chemother-apy response in lung cancer.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: F. Nikolos, C. ThomasDevelopment of methodology: F. Nikolos, C. ThomasAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): F. Nikolos, I. Bado, J.A. GustafssonAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): F. Nikolos, C. Thomas, I. Bado, J.A. GustafssonWriting, review, and/or revision of the manuscript: F. Nikolos, C. Thomas,J.A. GustafssonAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): C. ThomasStudy supervision: C. Thomas, J.A. Gustafsson
AcknowledgmentsJ.A. Gustafsson was supported by the Robert A. Welch Foundation
(E-0004). This work was supported by the Swedish Cancer Fund.
The costs of publication of this articlewere defrayed inpart by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received May 9, 2017; revised July 12, 2017; accepted October 16, 2017;published OnlineFirst November 8, 2017.
References1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin
2016;66:7–30.2. Miller KD, Siegel RL, Lin CC, Mariotto AB, Kramer JL, Rowland JH, et al.
Cancer treatment and survivorship statistics, 2016. CA Cancer J Clin2016;66:271–89.
3. Bareschino MA, Schettino C, Rossi A, Maione P, Sacco PC, Zeppa R, et al.Treatment of advanced non small cell lung cancer. J Thorac Dis2011;3:122–33.
4. Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, et al. Gefitinibor carboplatin–paclitaxel in pulmonary adenocarcinoma. N Engl J Med2009;361:947–57.
5. Kim ES. Chemotherapy resistance in lung cancer. Adv Exp Med Biol2016;893:189–209.
6. Dong X, Xu C, Lei P, Zhang W. The new concepts on overcoming drugresistance in lung cancer. Drug Des Devel Ther 2014;8:735.
7. Almeida GM, Duarte TL, Farmer PB, Steward WP, Jones GD. Multiple end-point analysis reveals cisplatin damage tolerance to be a chemoresistancemechanism in a NSCLC model: Implications for predictive testing. Int JCancer 2008;122:1810–9.
8. Lwin Z, Riess JW, Gandara D. The continuing role of chemotherapy foradvanced non-small cell lung cancer in the targeted therapy era. J ThoracDis 2013;5 Suppl 5:S556–64.
9. Dixon H, Norbury CJ. Therapeutic exploitation of checkpoint defects incancer cells lacking p53 function. Cell Cycle 2002;1:362–8.
10. Vogelstein B, Lane D, Levine AJ. Surfing the p53 network. Nature 2000;408:307–10.
11. VousdenKH, Lu X. Live or let die: the cell's response to p53.Nat Rev Cancer2002;2:594–604.
12. Kazmi N, M�arquez-Garb�an DC, Aivazyan L, Hamilton N, Garon EB,Goodglick L, et al. The role of estrogen, progesterone and aromatase inhuman non-small-cell lung cancer. Lung Cancer Manag 2012;1:259–72.
13. Thomas C, Gustafsson JÅ. The different roles of ER subtypes in cancerbiology and therapy. Nat Rev Cancer 2011;11:597–608.
14. Kawai H, Ishii A, Washiya K, Konno T, Kon H, Yamaya C, et al.Combined overexpression of EGFR and estrogen receptor alpha corre-lates with a poor outcome in lung cancer. Anticancer Res 2005;25:4693–8.
15. Rades D, Setter C, Dahl O, Schild SE, Noack F. The prognostic impact oftumor cell expression of estrogen receptor-a, progesterone receptor, andandrogen receptor in patients irradiated for nonsmall cell lung cancer.Cancer 2012;118:157–63.
16. Kawai H, Ishii A, Washiya K, Konno T, Kon H, Yamaya C, et al. Humancancer biology estrogen receptor A and B are prognostic factors in non-small cell lung cancer. Clin Cancer Res 2005;11:5084–9.
17. Nose N, Sugio K,Oyama T, Nozoe T, UramotoH, Iwata T, et al. Associationbetween estrogen receptor-beta expression and epidermal growth factorreceptor mutation in the postoperative prognosis of adenocarcinoma ofthe lung. J Clin Oncol 2009;27:411–7.
18. Nose N, Uramoto H, Iwata T, Hanagiri T, Yasumoto K. Expression ofestrogen receptor beta predicts a clinical response and longer progression-free survival after treatment with EGFR-TKI for adenocarcinoma of thelung. Lung Cancer 2011;71:350–5.
19. Guldhammer B, Fischer BM, Pappot H, Skov BG. Oestrogen receptor betaover expression inmales with non-small cell lung cancer is associated withbetter survival. Lung Cancer 2008;59:88–94.
20. Wang Z, Li Z, Ding X, Shen Z, Liu Z, An T, et al. ERb localization influencedoutcomes of EGFR-TKI treatment inNSCLCpatients with EGFRmutations.Sci Rep 2015;5:11392.
21. Luo Z, Wu R, Jiang Y, Qiu Z, Chen W, Li W. Overexpression of estrogenreceptor beta is a prognostic marker in non-small cell lung cancer: a meta-analysis. Int J Clin Exp Med 2015;8:8686–97.
22. VermaMK,Miki Y, SasanoH. Sex steroid receptors in human lung diseases.J Steroid Biochem Mol Biol 2011;127:216–22.
23. Mah V,Marquez D, Alavi M,Maresh EL, Zhang L, YoonN, et al. Expressionlevels of estrogen receptor beta in conjunction with aromatase predictsurvival in non-small cell lung cancer. Lung Cancer 2011;74:318–25.
DDR in NSCLC is Regulated by ERb
www.aacrjournals.org Mol Cancer Res; 16(2) February 2018 241
on August 12, 2020. © 2018 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 8, 2017; DOI: 10.1158/1541-7786.MCR-17-0201

24. Stabile LP, Dacic S, Land SR, Lenzner DE, Dhir R, Acquafondata M, et al.Combined analysis of estrogen receptor beta-1 and progesterone receptorexpression identifies lung cancer patients with poor outcome. Clin CancerRes 2011;17:154–64.
25. Rajapaksa G, Nikolos F, Bado I, Clarke R, Gustafsson JÅ, Thomas C. ERbdecreases breast cancer cell survival by regulating the IRE1/XBP-1 pathway.Oncogene 2015;34:4130–41.
26. Hartman J, Edvardsson K, Lindberg K, Zhao C, Williams C, Str€om A, et al.Tumor repressive functions of estrogen receptor beta in SW480 coloncancer cells. Cancer Res 2009;69:6100–6.
27. Dey P, Jonsson P, Hartman J, Williams C, Str€omA, Gustafsson JÅ. Estrogenreceptors b1 and b2 have opposing roles in regulating proliferation andbone metastasis genes in the prostate cancer cell line PC3. Mol Endocrinol2012;26:1991–2003.
28. Ma R, Karthik GM, L€ovrot J, Haglund F, Rosin G, Katchy A, et al. Estrogenreceptor b as a therapeutic target in breast cancer stem cells. J Natl CancerInst 2017;109:1–14.
29. Siegfried JM, Hershberger PA, Stabile LP. Estrogen receptor signaling inlung cancer. Semin Oncol 2009;36:524–31.
30. Nikolos F, Thomas C, Rajapaksa G, Bado I, Gustafsson JA. ER regulatesNSCLC phenotypes by controlling oncogenic RAS signaling. Mol CancerRes 2014;12:843–54.
31. Thomas CG, Strom A, Lindberg K, Gustafsson JA. Estrogen receptor betadecreases survival of p53-defective cancer cells after DNA damage byimpairing G2/M checkpoint signaling. Breast Cancer Res Treat 2011;127:417–27.
32. LeeMT,HoSM, Tarapore P, Chung I, LeungYK. Estrogen receptorb isoform5 confers sensitivity of breast cancer cell lines to chemotherapeutic agent-induced apoptosis through interaction with Bcl2L12. Neoplasia2013;15:1262–71.
33. Elebro K, Borgquist S, Rosendahl AH, Markkula A, Simonsson M, Jirstr€omK, et al. High estrogen receptor b expression is prognostic among adjuvantchemotherapy– treated patients—results from a population-based breastcancer cohort. Clin Cancer Res 2017;23:766–77.
34. Wang J, Zhang C, Chen K, Tang H, Tang J, Song C, et al. ERb1 inverselycorrelates with PTEN/PI3K/AKT pathway and predicts a favorable prog-nosis in triple-negative breast cancer. Breast Cancer Res Treat 2015;152:255–69.
35. Pinton G,Manente AG, Daga A, Cilli M, Rinaldi M, Nilsson S, et al. Agonistactivation of estrogen receptor beta (ERb) sensitizes malignant pleuralmesothelioma cells to cisplatin cytotoxicity. Mol Cancer 2014;13:227.
36. Nelson AW, Groen AJ, Miller JL, Warren AY, Holmes KA, Tarulli GA, et al.Comprehensive assessment of estrogen receptor beta antibodies in cancercell line models and tissue reveals critical limitations in reagent specificity.Mol Cell Endocrinol 2017;440:138–50.
37. Thomas C, Rajapaksa G, Nikolos F, Hao R, Katchy A, McCollum CW, et al.ERb1 represses basal-like breast cancer epithelial to mesenchymal transi-tion by destabilizing EGFR. Breast Cancer Res 2012;14:R148.
38. Zhu CQ, Ding K, Strumpf D, Weir BA, Meyerson M, Pennell N, et al.Prognostic and predictive gene signature for adjuvant chemotherapy inresected non–small-cell lung cancer. J Clin Oncol 2010;28:4417–24.
39. Jackson JG, Pant V, LiQ,Chang LL,Quint�as-CardamaA,GarzaD, et al. P53-mediated senescence impairs the apoptotic response to chemotherapy andclinical outcome in breast cancer. Cancer Cell 2012;21:793–806.
40. Cosaert J, Quoix E. Platinum drugs in the treatment of non-small-cell lungcancer. Br J Cancer 2002;87:825–33.
41. Kuntz K, O'Connell MJ. The G(2) DNA damage checkpoint: could thisancient regulator be the Achilles heel of cancer? Cancer Biol Ther 2009;8:1433–9.
42. Zhou BB, Elledge SJ. The DNA damage response: putting checkpoints inperspective. Nature 2000;408:433–9.
43. Taylor WR, Stark GR. Regulation of the G2/M transition by p53. Oncogene2001;20:1803–15.
44. Vasquez RJ, Howell B, Yvon AM, Wadsworth P, Cassimeris L. Nanomolarconcentrations of nocodazole altermicrotubule dynamic instability in vivoand in vitro. Mol Biol Cell 1997;8:973–85.
45. Sarkaria JN, Busby EC, Tibbetts RS, Roos P, Taya Y, Karnitz LM, et al.Inhibition of ATM and ATR kinase activities by the radiosensitizing agent,caffeine. Cancer Res 1999;59:4375–82.
46. Bado I,Nikolos F, RajapaksaG,Gustafsson JÅ, ThomasC. ERbdecreases theinvasiveness of triple-negative breast cancer cells by regulating mutant p53oncogenic function. Oncotarget 2016;7:13599–611.
47. Berger C, Qian Y, Chen X. The p53-estrogen receptor loop in cancer. CurrMol Med 2013;13:1229–40.
48. Dohn M, Zhang S, Chen X. p63a and DNp63a can induce cell cycle arrestand apoptosis and differentially regulate p53 target genes. Oncogene2001;20:3193–205.
49. Stossi F, Madak-Erdogan Z, Katzenellenbogen BS. Estrogen receptor alpharepresses transcription of early target genes via p300 and CtBP1. Mol CellBiol 2009;29:1749–59.
50. Yoon SM, Shaikh T, Hallman M. Therapeutic management options forstage III non-small cell lung cancer. World J Clin Oncol 2017;8:1–20.
51. Collisson EA, Campbell JD, Brooks AN, Berger AH, Lee W, Chmielecki J,et al. Comprehensive molecular profiling of lung adenocarcinoma. Nature2014;511:543–50.
52. Niikawa H, Suzuki T, Miki Y, Suzuki S, Nagasaki S, Akahira J, et al.Intratumoral estrogens and estrogen receptors in human non-small celllung carcinoma. Clin Cancer Res 2008;14:4417–26.
53. Nitiss JL. TargetingDNA topoisomerase II in cancer chemotherapy.Nat RevCancer 2009;9:338–50.
54. Dasari S, Tchounwou PB. Cisplatin in cancer therapy: molecular mechan-isms of action. Eur J Pharmacol 2014;740:364–78.
55. Wang L,Wu S, OuG, Bi N, LiW, RenH, et al. Randomized phase II study ofconcurrent cisplatin/etoposide or paclitaxel/carboplatin and thoracicradiotherapy in patients with stage III non-small cell lung cancer. LungCancer 2012;77:89–96.
56. Reaper PM, Griffiths MR, Long JM, Charrier JD, MacCormick S, CharltonPA, et al. Selective killing of ATM- or p53-deficient cancer cells throughinhibition of ATR. Nat Chem Biol 2011;7:428–30.
57. Wang Q, Fan S, Eastman A, Worland PJ, Sausville EA, O'Connor PM.UCN-01: a potent abrogator of G2 checkpoint function in cancer cells withdisrupted p53. J Natl Cancer Inst 1996;88:956–65
58. Lv Y, Yanan H, Yu X, Liu R, Zhang S, Zheng X, et al. TopBP1 contributesto the chemoresistance in non-small cell lung cancer through upregulationof p53. Drug Des Devel Ther 2016;10:3053–64.
59. Lin YL, Sengupta S, Gurdziel K, Bell GW, Jacks T, Flores ER. p63 and p73transcriptionally regulate genes involved in DNA repair. PLoS Genet 2009;5:e1000680.
60. Suliman Y, Opitz OG, Avadhani A, Burns TC, El-Deiry W, Wong DT, et al.p63 expression is associated with p53 loss in oral-esophageal epithelia ofp53-deficient mice. Cancer Res 2001;61:6467–73.
61. Lin CY, Str€omA, Vega VB, Kong SL, Yeo AL, Thomsen JS, et al. Discovery ofestrogen receptor a target genes and response elements in breast tumorcells. Genome Biol 2004;5:R66.
62. AdornoM,CordenonsiM,MontagnerM,Dupont S,WongC,HannB, et al.A mutant-p53/Smad complex opposes p63 to empower TGFb-inducedmetastasis. Cell 2009;137:87–98.
63. Zimmermann M, Arachchige-Don AS, Donaldson MS, Dallapiazza RF,Cowan CE, Horne MC. Elevated cyclin G2 expression intersects withDNA damage checkpoint signaling and is required for a potent G2/Mcheckpoint arrest response to doxorubicin. J Biol Chem 2012;287:22838–53.
Mol Cancer Res; 16(2) February 2018 Molecular Cancer Research242
Nikolos et al.
on August 12, 2020. © 2018 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 8, 2017; DOI: 10.1158/1541-7786.MCR-17-0201

2018;16:233-242. Published OnlineFirst November 8, 2017.Mol Cancer Res Fotis Nikolos, Christoforos Thomas, Igor Bado, et al. Damage Response
Sensitizes NSCLC to Chemotherapy by Regulating DNAβER
Updated version
10.1158/1541-7786.MCR-17-0201doi:
Access the most recent version of this article at:
Material
Supplementary
http://mcr.aacrjournals.org/content/suppl/2017/11/08/1541-7786.MCR-17-0201.DC1
Access the most recent supplemental material at:
Cited articles
http://mcr.aacrjournals.org/content/16/2/233.full#ref-list-1
This article cites 63 articles, 14 of which you can access for free at:
Citing articles
http://mcr.aacrjournals.org/content/16/2/233.full#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://mcr.aacrjournals.org/content/16/2/233To request permission to re-use all or part of this article, use this link
on August 12, 2020. © 2018 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 8, 2017; DOI: 10.1158/1541-7786.MCR-17-0201