Epilepsy and Seizures - Dr Ted Williamsdrtedwilliams.net/cop/752/752AntiepilepticAgents.pdfEpilepsy...
62
Epilepsy and Seizures Epilepsy: Two or more unprovoked seizures that arise from abnormal electrical discharges in the brain Often Unknown Etiology: infections, tumors, trauma, toxins, metabolic disorders, cerebrovascular disorders, developmental abnormalities such as cortical dysplasia, genetic disorders Epileptogenesis - Factors leading to the development of epilepsy (changes in gene expression/protein function, cell death, abnormal synaptic circuitry)
Transcript of Epilepsy and Seizures - Dr Ted Williamsdrtedwilliams.net/cop/752/752AntiepilepticAgents.pdfEpilepsy...

Epilepsy and Seizures
Epilepsy:Two or more unprovoked seizures that arise from abnormalelectrical discharges in the brain
Often Unknown Etiology:infections, tumors, trauma, toxins, metabolic disorders,cerebrovascular disorders, developmental abnormalities suchas cortical dysplasia, genetic disorders
Epileptogenesis - Factors leading to the development ofepilepsy (changes in gene expression/protein function, celldeath, abnormal synaptic circuitry)

a change in behavior caused by an abnormalsynchronous electrical discharge in the brain
Seizure:
Too muchexcitation or toolittle inhibition
Excessive, randomdischarge of a group ofneurons in the brain
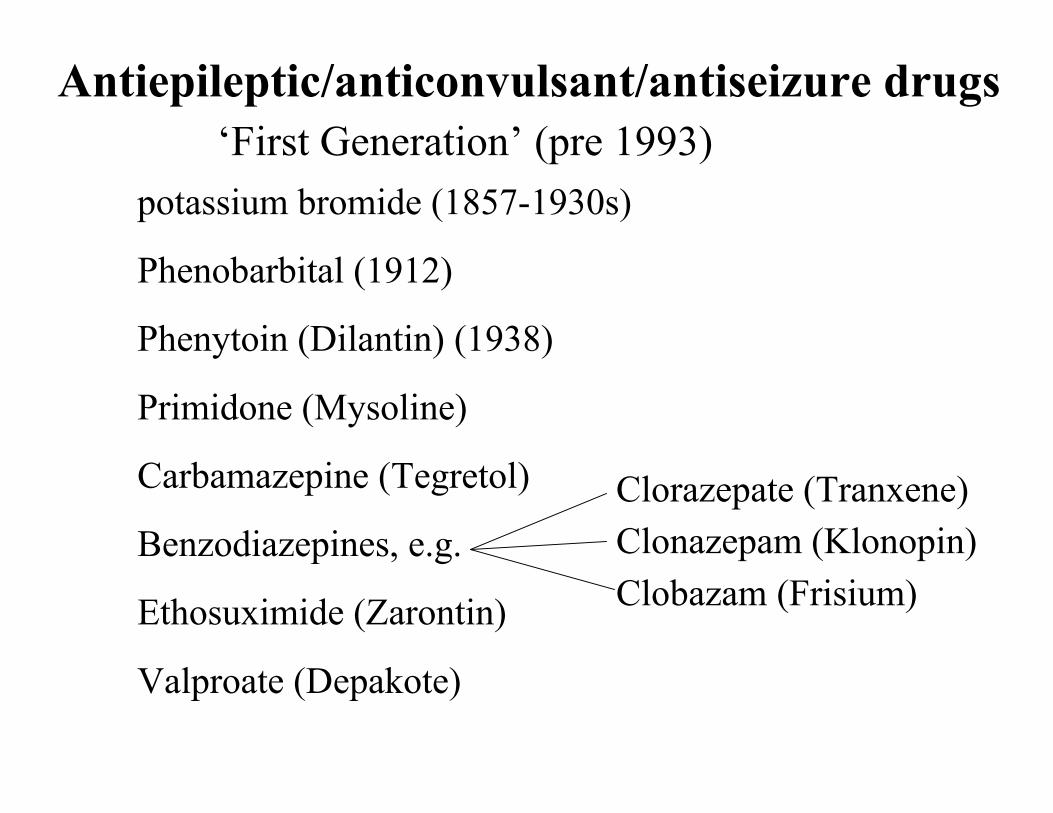
Antiepileptic/anticonvulsant/antiseizure drugs
Carbamazepine (Tegretol)
Phenytoin (Dilantin) (1938)
Valproate (Depakote)
Phenobarbital (1912)
Primidone (Mysoline)
Ethosuximide (Zarontin)
Clonazepam (Klonopin)
‘First Generation’ (pre 1993)potassium bromide (1857-1930s)
Benzodiazepines, e.g.Clorazepate (Tranxene)
Clobazam (Frisium)

Antiepileptic/anticonvulsant/antiseizure drugs
Zonisamide (Zonegran)
Vigabatrin (Sabril)
‘Second Generation’ (since 1993)Felbamate (Felbatol)
Gabapentin (Neurontin)
Lamotrigine (Lamictal)
Topiramate (Topamax)
Tiagabine (Gabitril)
Oxcarbazepine (Trileptal)
Levetiracetam (Keppra)
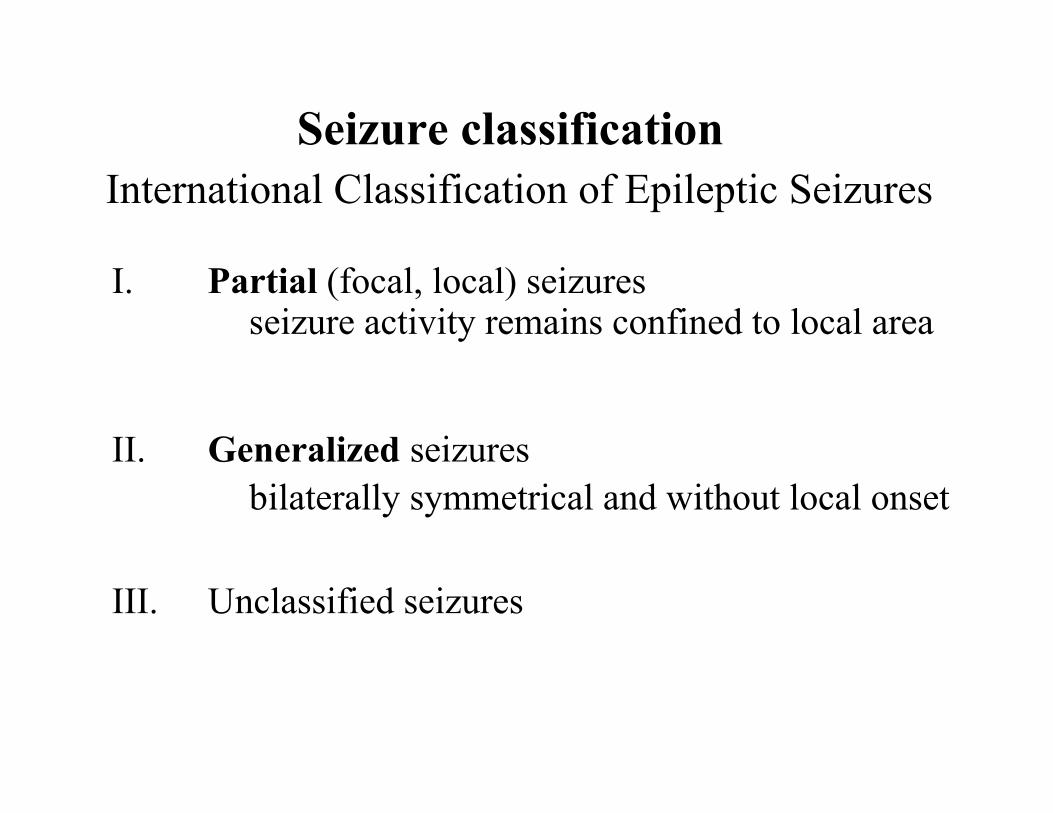
Seizure classificationInternational Classification of Epileptic Seizures
I. Partial (focal, local) seizures
II. Generalized seizures
III. Unclassified seizures
seizure activity remains confined to local area
bilaterally symmetrical and without local onset

A. Simple partial seizures (consciousness not impaired)
1. with motor symptoms (changes in movement)2. with somatosensory or special sensory symptoms
(e.g. tingling, flashing lights)3. with autonomic symptoms (e.g. heart rate)4. with psychic symptoms (alteration of consciousness,
e.g. hallucinations)
I Partial seizures
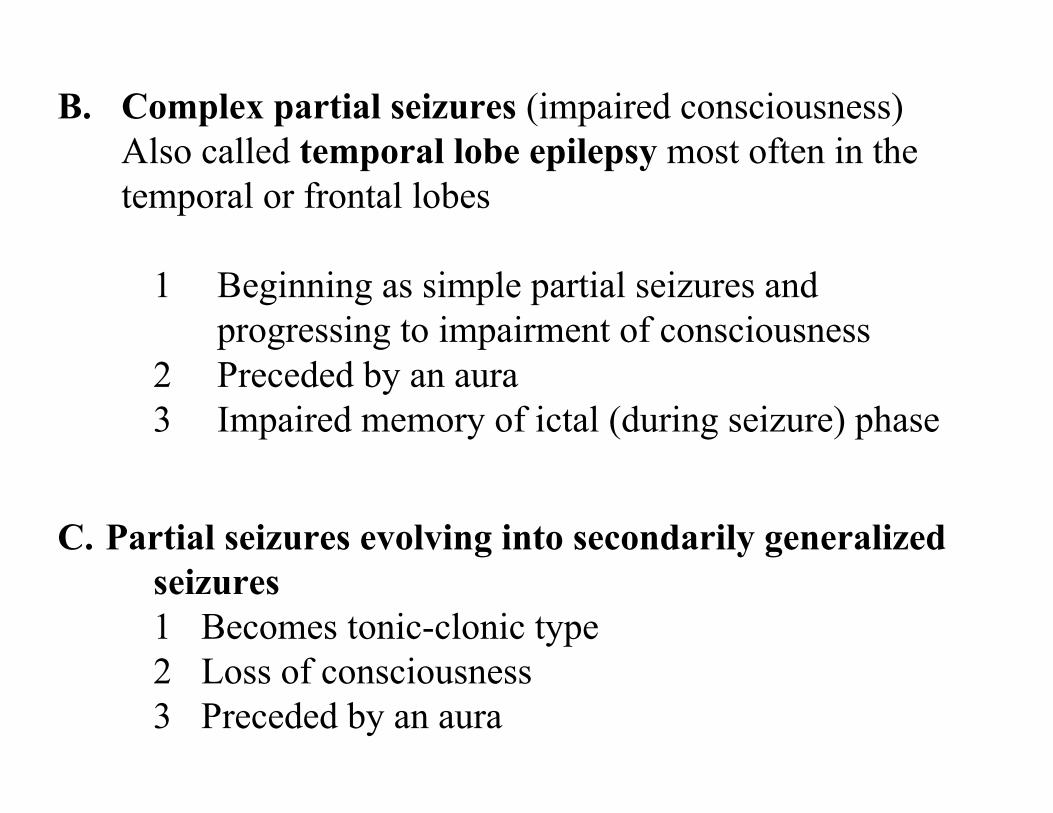
B. Complex partial seizures (impaired consciousness)Also called temporal lobe epilepsy most often in thetemporal or frontal lobes
1 Beginning as simple partial seizures andprogressing to impairment of consciousness
2 Preceded by an aura3 Impaired memory of ictal (during seizure) phase
C. Partial seizures evolving into secondarily generalizedseizures1 Becomes tonic-clonic type2 Loss of consciousness3 Preceded by an aura

II. Generalized seizures
A. Absence seizures (petit mal seizures)sudden interruption of consciousness, blank stare no aura
B. Myoclonic seizures (random discharges in motor cortex)C. Tonic-clonic seizures (grand mal seizures)
abrupt onset usually no aurano symptoms of partial or complex seizuretonic - contractionclonic - shakingpostictal-flaccid and unconscious

Reading Perception of fear Alteredconsciousness
Righthemi-sphere
Lefthemi-sphere
EEG

Epileptic syndromes
Idiopathic epilepsies
Idiopathic epilepsies with partial seizurese.g. frontal lobe, temporal lobe
Idiopathic epilepsies with generalized seizuresmany childhood epilepsy syndromesneonatal convulsions, benign myoclonic seizures,absence seizures
Symptomatic epilepsies - e.g. trauma, tumor

Status Epilepticus
Seizures occurring acutely in greater intensity,number, or length than usual
A prolonged seizure that lasts longer than 10 minutes orrepeated seizures over the course of 30 minutes
Life threatening - emergency care should begin immediately
Treated with benzodiazepines: Diazepam or Lorazepam

Secondary generalized seizure
Primary generalized seizure
Seizurefocus
Seizurefocus
SeizureFocus
Thalamus
Partial seizure

Progression of a Partial Seizure:
1 Initiation - increased electrical activity in a single cell2 Synchronization of surrounding neurons3 Spread to adjacent areas (aura)4 Seizure begins when a group of neurons depolarize
suddenly
Paroxysmal depolarizing shiftLeads to abnormal succession of action
potentialsSurround inhibition normally should prevent
synchronization

Focal epileptiform activity (partial seizures)
EEG
Membrane potential
spike
Slow wave
Depolarizingshift (DS)
Post-DS hyperpolarization
Interictal discharge

Excitatory center Inhibitorysurround
Surround inhibition is critical for normalfunction of the CNS

Complex-partial / Temporal lobe epilepsy
• Usually caused by abnormal activity intemporal lobe/hippocampus + amygdala
• Classically preceded by aura• Altered consciousness• Impaired memory• Can be drug resistant/pharmacoresistant

Entorhinalcortex
Dentate gyrus
CA3
CA1subiculum
Perforant pathMossy fibers
Schaffercollaterals
cortex
Hippocampus circuitry
Normal activity

Entorhinalcortex
Dentate gyrus
CA3
CA1subiculum
Perforant pathMossy fibers
Schaffercollaterals
cortex
Hippocampus circuitry
interictal activity (abnormal )

Entorhinalcortex
Dentate gyrus
subiculum
Perforant pathMossy fibers
cortex
Hippocampus circuitry
ictal activity (seizure )
mesial temporal sclerosis due to excitotoxic cell death
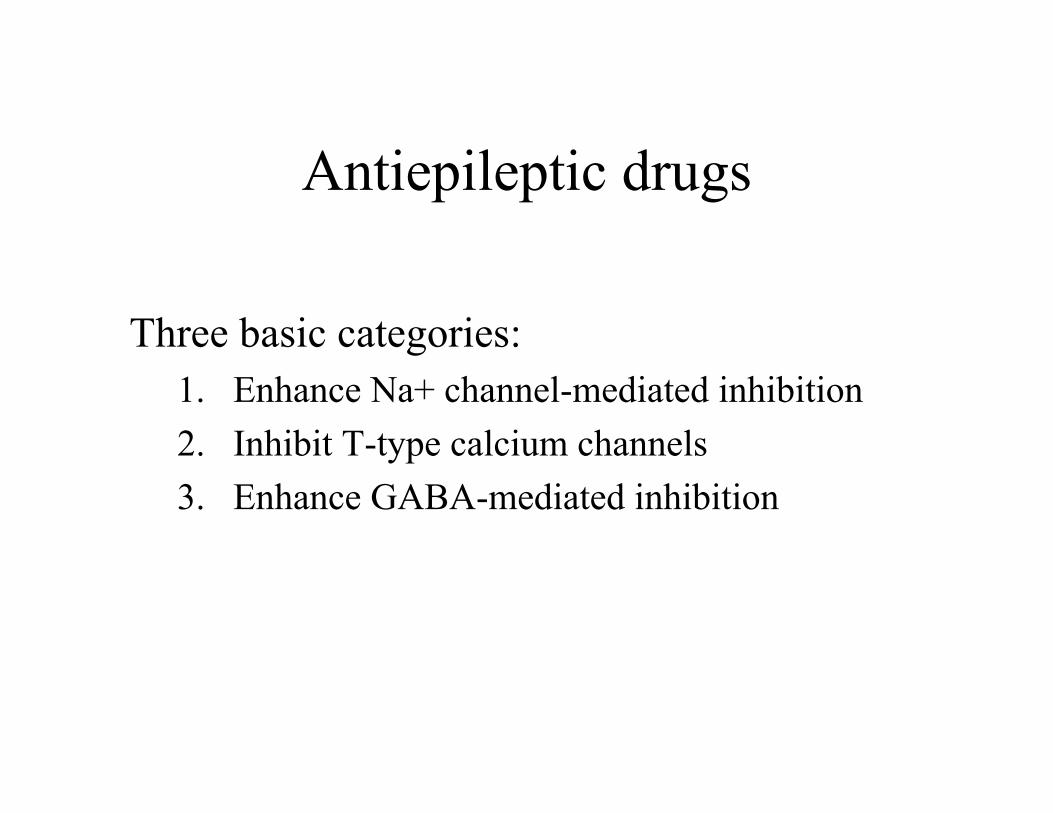
Antiepileptic drugs
Three basic categories:1. Enhance Na+ channel-mediated inhibition2. Inhibit T-type calcium channels3. Enhance GABA-mediated inhibition
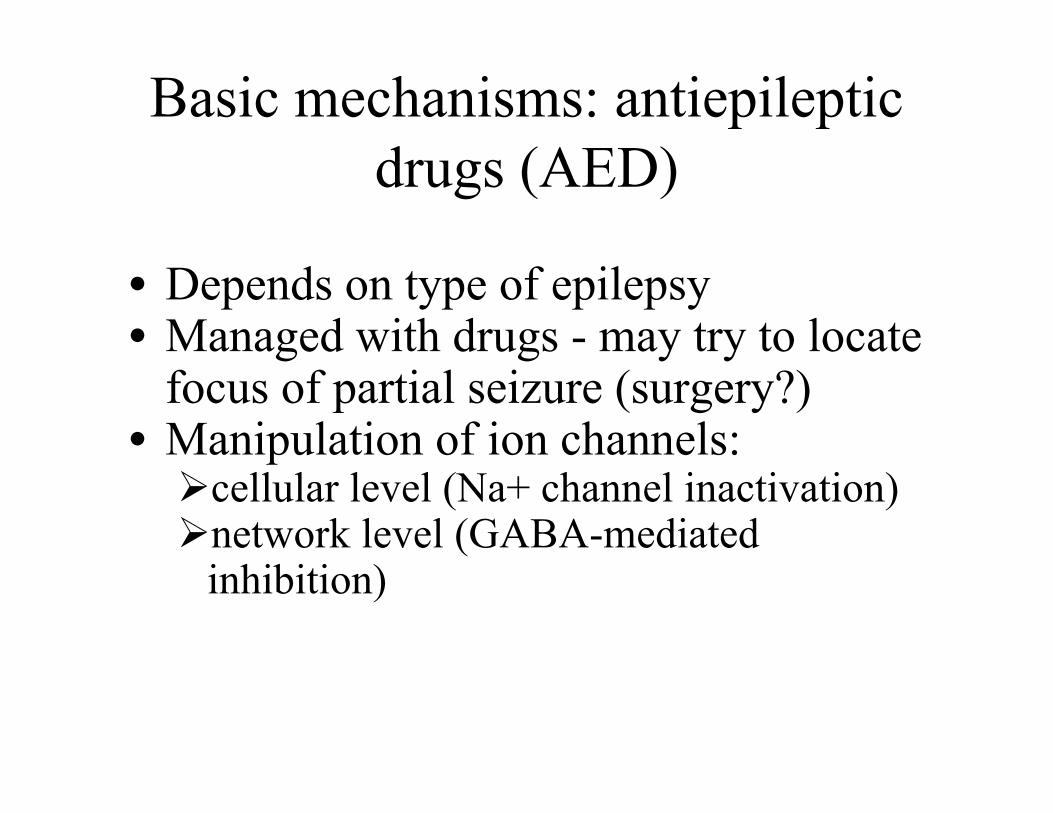
Basic mechanisms: antiepilepticdrugs (AED)
• Depends on type of epilepsy• Managed with drugs - may try to locate
focus of partial seizure (surgery?)• Manipulation of ion channels:
cellular level (Na+ channel inactivation)network level (GABA-mediated
inhibition)

Drug choice by seizure type Partial seizures
Carbamazepine (Tegretol)Phenytoin (Dilantin)Valproate (Depakote)
Drugs of choice:
Alternatives:
Zonisamide (Zonegran)
Gabapentin (Neurontin)Lamotrigine (Lamictal)
Topiramate (Topamax)Tiagabine (Gabitril)
Oxcarbazepine (Trileptal)Levetiracetam (Keppra)
PhenobarbitalPrimidone (Mysoline)
Vigabatrin (Sabril)Felbamate (Felbatol)
Drug choice by seizure type:Tonic-clonic (grand mal) seizures
Drugs of choice:Carbamazepine (Tegretol)Phenytoin (Dilantin)
Valproate (Depakote)
Alternatives:
Zonisamide (Zonegran)
Lamotrigine (Lamictal)Topiramate (Topamax)
Oxcarbazepine (Trileptal)Levetiracetam (Keppra)
PhenobarbitalPrimidone (Mysoline)
Felbamate (Felbatol)
Drugs that block voltage-dependent Na+ channelsInhibit high frequency repetitive firing
Carbamazepine (Tegretol)Phenytoin (Dilantin)Valproate (Depakote)
Zonisamide (Zonegran)
Felbamate (Felbatol)
Gabapentin (Neurontin)Lamotrigine (Lamictal)
Topiramate (Topamax)Oxcarbazepine (Trileptal) [active metabolite HCBZ]

Voltage/frequency/use-dependent block
Drug stabilizes inactivated state
open‘resting’ inactivated
open‘resting’ inactivatedblocked
voltage-gatedNa+ channels
depolarization

No drug drug
Lowfrequency
Highfrequency
Membranepotential
inactivation
time time
Drugs that increase GABA levels in brain
Valproate (Depakote)
Gabapentin (Neurontin)
Tiagabine (Gabitril)
Vigabatrin (Sabril)

glutamic acid
GABAaminotransferase
succinatesemialdehydedehydrogenase
GABA
GAT-1
GABA transporterGABA
glutamic aciddecarboxylase
valproate
+ valproate--
tiagabine
-- vigabatrin
gabapentin
decrease inefficacy.
increase inefficacy
inhibitory synapsesrepetitively activated
excitatory synapsesrepetitively activated
(might be desensitization of the GABAA receptor)
Interictal to Ictal transition
Inhibitory surround breaks down

GABAergicinterneuron
Glutamatergicpyramidalneuron
Cerebral cortex

Inhibitorysurround
Excitatory center
Pyramidalcell(glutamatergic)
Inhibitoryinterneuron(GABAergic)
- --- -
-- -
+
+ +
+
+
-
Excitatorysynapse
Inhibitorysynapse
Membrane potential
Inhibitory post-synaptic potential
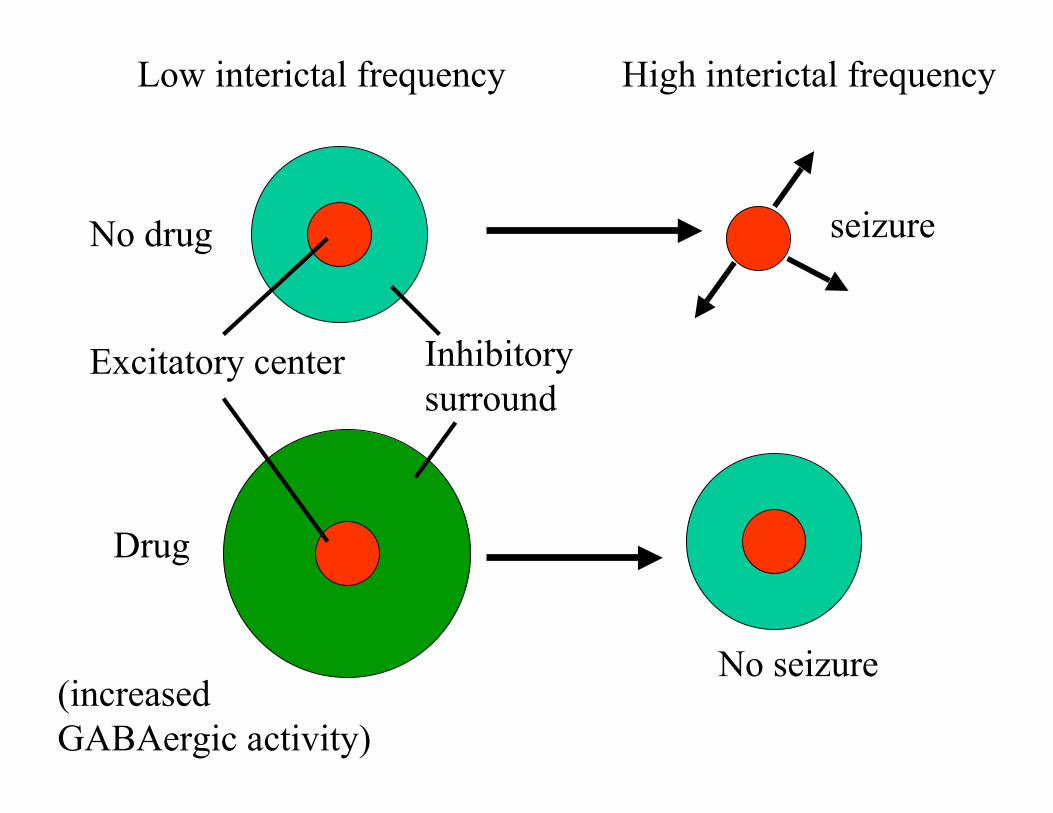
Low interictal frequency High interictal frequency
No drug
(increasedGABAergic activity)
Drug
seizure
Excitatory center Inhibitorysurround
No seizure
Drugs that Increase activity of GABAA receptors
Barbiturates: Phenobarbital
Benzodiazepines Clonazepam (Klonopin)Clorazepate (Tranxene)
Clobazam (Frisium)
Topiramate (Topamax) - not fully understood
Levetiracetam (Keppra)- - not fully understood

GABABarbituratesIncrease
Efficacy ofGABA
Increaseduration
of opening
Benzodiazepenespotentiate GABAbinding enhance
the affinityIncrease
frequency ofchannel openingCl-

Treatment of status epilepticus is unique:
Diazepam (Diastat)
Lorazepam (Atavan)

Drug choice by seizure type:Absence (petit mal) seizures
Drugs of choice:
Alternatives:
Valproate (Depakote)
Ethosuximide (Zarontin)
Zonisamide (Zonegran)
Lamotrigine (Lamictal)Clonazepam (Klonopin)

Drug choice by seizure type
Drugs of choice:
Alternatives:
Atypical absence, myoclonic, atonic seizures
Valproate (Depakote)
Lamotrigine (Lamictal)
Clonazepam (Klonopin)
Zonisamide (Zonegran)Felbamate (Felbatol)
Topiramate (Topamax)
Drugs that block T-type Ca2+ channels
Valproate (Depakote)
Ethosuximide (Zarontin)
Zonisamide (Zonegran)
Clonazepam at reticular thalamicnucleus*may be a unique BDZ

EEGAbsence seizure
1 s50uV
‘Spike and wave’ activity in typical absence seizure

Slow wave sleep EEGAwake EEG
1 sec

cortex
nucleus reticularisthalami (NRT)
Thalamic relaynucleus
Ascending arousal systemand sensory afferents
+
+
GABAergicneurons


Thalamic neuronsAwakeRelay neurons “transmission mode” to cortex (single
spikes on EEG)Sleep“Burst mode” sensory information is not transmitted
to cortex (T-type calcium channel is active )Absence seizureInappropriate activation of T-type channel in an
awake state
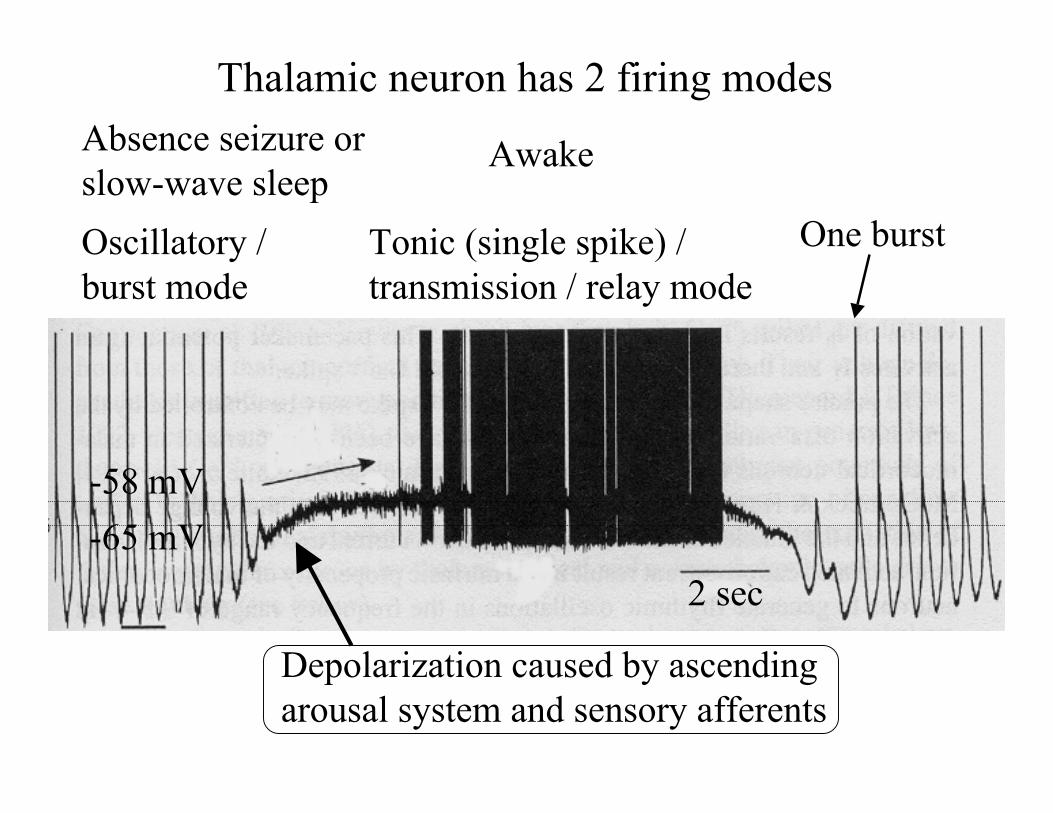
Thalamic neuron has 2 firing modes
Oscillatory /burst mode
Tonic (single spike) /transmission / relay mode
Depolarization caused by ascendingarousal system and sensory afferents
2 sec-65 mV-58 mV
Absence seizure orslow-wave sleep
Awake
One burst

Thalamic neurons
T-type Ca2+ channels (IT)
Ih channels(hyperpolarization-activatedcation channels)
Voltage-dependent Na+ channelsVoltage-dependent K+ channels
Na+-dependent actionpotentials (spikes)
Pacemaker activity;enables oscillatorymode
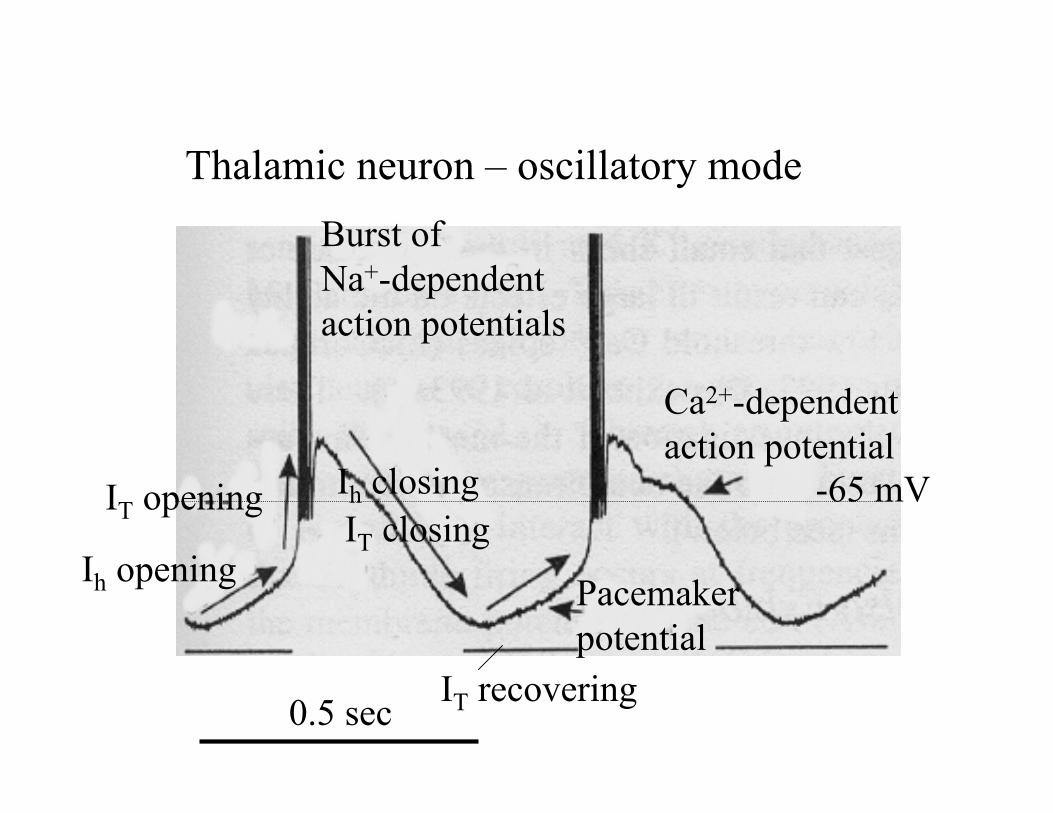
Thalamic neuron – oscillatory mode
Ih opening
IT opening
Burst ofNa+-dependentaction potentials
Ih closingIT closing
Pacemakerpotential
IT recovering
Ca2+-dependentaction potential
-65 mV
0.5 sec

Thalamic neurons
At ‘awake’ resting potential: T-type Ca2+ channels inactivated
Hyperpolarization by NRT neurons(GABAA and GABAB receptors)
T-type channels recover (de-inactivate)
Oscillatory mode(slow-wave sleep or absence seizure)

?
+ -
K+ Ca2+GABA
GABAB
G-protein
Activation of GABAB receptors causes hyperpolarization

1 sec
Cortical neuron
Thalamic neuronNRTthalamus
cortex
+
++
+
-
---
Synchronized activity in Absence seizure
GABAAGABAB
GABAA

TiagabineVigabatrin
Barbiturates
Exacerbate absenceseizures(make them worse)
Valproate
Clonazepam
EthosuximideValproateZonisamide
Suppress absenceseizures
IncreaseGABA levels
ActivateGABAAreceptors
Block T-typeCa2+ channels
Drug effect

valvalval,gab,tia,vig
valIncreaseGABAlevels
bzd(clon),top
bzd(clon)barb,bzd,top,lev
barbActivateGABAA
val,zoneth,val,zonval,zonval,zonBlock T-type Ca2+
val,lam,top,zon,fel
val,lam,zoncar,pht,vallam,gab,topzon,oxc,fel
val,car,pht,lam,top,zon
oxc,fel
Block Na+
channels
Atypicalabsence,
myoclonic,atonic
Typicalabsence
PartialGeneralizedTonic-clonic
Drug treatment of seizuresModes of action
Block Na+ channels
Enhance GABAA receptor activityBlock T-type Ca2+ channels
Inhibit glutamate receptors?
Multiple actions, e.g. valproate
Increase GABA synthesisblock GABA degradationblock GABA reuptake
IncreaseGABAlevels
Block L-type Ca2+ channels?
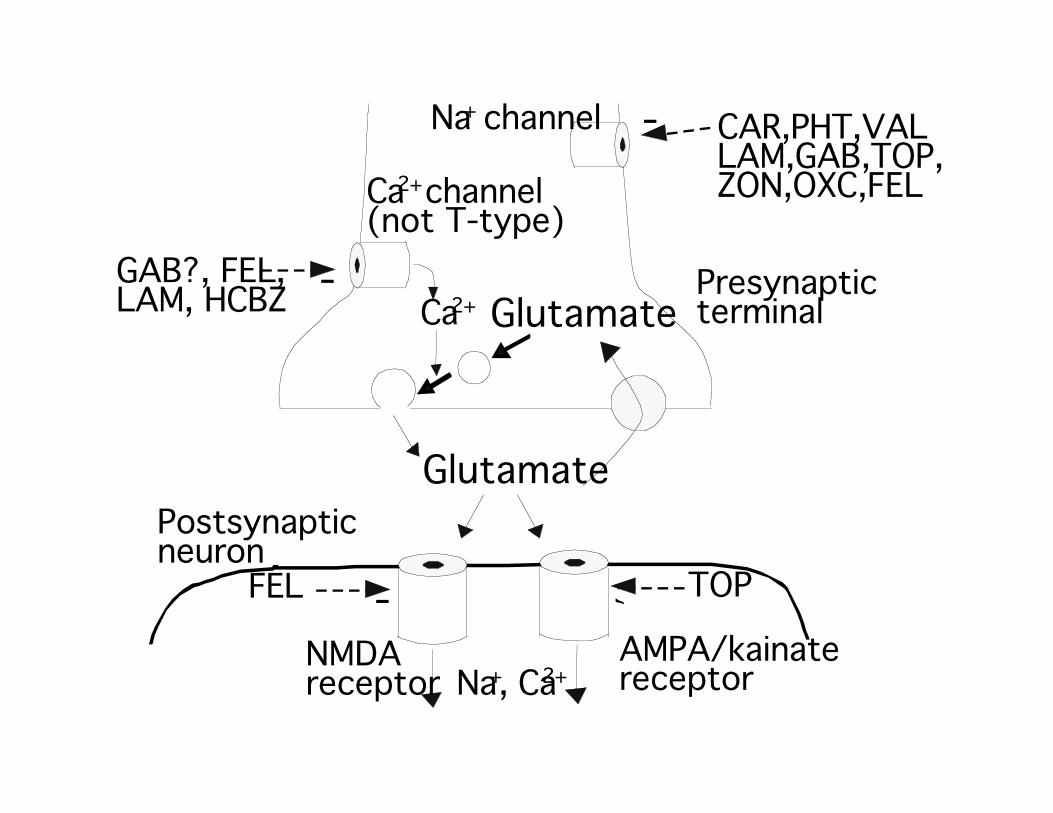
Glutamate
Glutamate
Postsynapticneuron
Presynapticterminal
-
GAB?, FEL,LAM, HCBZ
TOP
-
Ca2+ channel(not T-type)
NMDAreceptor
AMPA/kainatereceptor
-FEL
Ca2+
Na+ channel
Na+, Ca2+
CAR,PHT,VALLAM,GAB,TOP,ZON,OXC,FEL

GABA
GABA-T
GABAGABA-T
GAD
Cl-
SSA
SSADH
GABAA receptorPostsynapticneuron
Presynapticterminal
Glial cell
VAL
-
-
-
VAL+
+
TIA
-
-
VIG
-
-
BZD, Barb,TOP, LEV
K+
GABAB
receptor
+
T-type Ca2+
channel
ETH, VAL,ZON
-GAT-1

Epileptogenesis
Changes in gene expression or protein function
NMDA receptorsAltered subunit expression in epileptic cortex
AMPA receptorsIncreased expression in epileptic cortex
GABAA receptorsDecreased expression in epileptic cortex
Genetics – nACh receptor
‘A-type’ K+ channelsLost in epileptic hippocampus

Loss of ‘A-type’ K+ channels
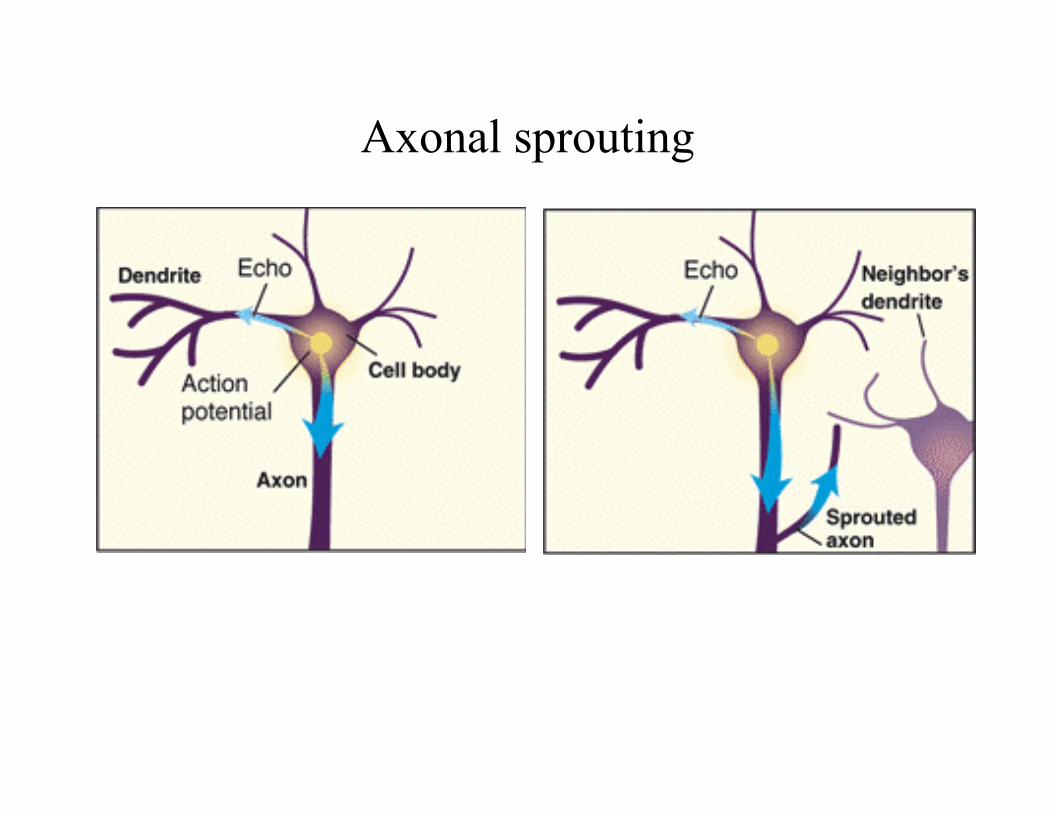
Axonal sprouting

SUMMARY
Epilepsy is characterized by recurrent seizures
Seizures are due to abnormal electrical activity in the brain
Epilepsy has many different causes
There are different types of seizure
Status epilepticus is life threatening

Main points (continued)
Voltage/frequency/use-dependent block of voltage-gatedNa+ channels suppresses high frequency firing in tonic-clonic and partial seizures.
We can make some rationalizations about relationshipsbetween mode of drug action and seizure type.

Main points (continued)
Interictal discharges are abnormal (may be containedin a focus no symptomatic pathology but seen on EEG)
An increase in interictal activity may lead to a seizureby breaking down the inhibitory surround.
Drugs that increase GABAergic transmission may suppresspartial seizures by enhancing the inhibitory surround.

Synchronized thalamocortical rhythms occur in slow-wavesleep and absence seizures.
Main points (continued)
T-type Ca2+ channels are required for the oscillatorymode of the thalamus.
Hyperpolarization of thalamic neurons allows theT-type Ca2+ channels to recover from inactivation.
Drugs that block T-type Ca2+ channels can suppressabsence seizures.
Drugs that increase GABA levels can exacerbateabsence seizures.

Main points (continued)
Epileptogenesis is a poorly understood process in which aninitial event leads to the development of epilepsy.
We don’t have any drugs that prevent epileptogenesis
Available antiepileptics only control seizures