
EPIDEMIOLOGY OF DISEASES IN MALAYSIA
11
1 EPIDEMIOLOGY OF DISEASES IN MALAYSIA
Transcript of EPIDEMIOLOGY OF DISEASES IN MALAYSIA

1
EPIDEMIOLOGY OF DISEASES IN MALAYSIA

2
VPDS (VACCINE PREVENTABLE DISEASES )
• All infectious diseases which can be prevented by vaccines are on a downward trend, in line with the national and WHO target.
• No cases of polio, neonatal tetanus and diphtheria.
• No large epidemics • Measles and hepatitis B under control and on a
downward trend.
BCG 99.00%Triple & Double Antigen (3rd Dose) 85.40%
Childhood Immunisation Coverage, Malaysia 2003
Polio Immunisation (3rd Dose) 94.90%Measles Immunisation 75.50%Hep B Immunisation (3rd Dose) 93.10%

3
WATER & FOOD BORNE DISEASES• A drop in the incidence rate of food and
water borne diseases such as typhoid, cholera, para typhoid, hepatitis A and d i 10 (1988 1997)dysentry since 10 years ago (1988-1997)
• Related to improvement of safe water supply and better sanitation.
• However there is an increase of food poisoning incidence.
CHOLERA
• Still a public health problem especially in Sabah and the northern peninsular.
• Related to the use of contaminated waterRelated to the use of contaminated water during drought or water shortage.
• Sabah - GREG storm 1997• Sarawak – use of contaminated rain water
TYPHOID
• Occurs in some states especially Kelantan, Sabah and Terengganu.
• Big outbreak in Tawau 1997 due to theBig outbreak in Tawau 1997 due to the use of contaminated river water (180 cases)
• Outbreak in Kota Baru, Kelantan believed to be related to “sirap ais”.
HEPATITIS A
• Endemic in some states such as Terengganu, Kelantan and Sabah.
DYSENTRY • Most cases occurs at border areas in
Sabah, Sarawak, Kedah, Perlis, Perak and Johor.

4
FOOD POISONING
• A big problem in institutions, schools and factories.R l t d t h i i f d• Related to unhygienic food preparation.
• Mostly due to E. coli, Salmonella spp and Staphyllococcus aureus.
AIDS/HIV
AIDS
• Abbreviation for Acquired Immune Deficiency Syndrome.
• Infected persons will lose their naturalInfected persons will lose their natural immune defence system and minor infections will become life threatening diseases.
• This person will usually die from serious opportunistic infection or due to rare cancers.
The Virus
• Identified in 1983/84.• In 1986, given the name Human Immuno-
deficiency Virus (HIV) by ICTVdeficiency Virus (HIV) by ICTV.• It is a retrovirus that belongs to a large
family of RNA lentiviruses.• 2 types identified
– HIV-1, – HIV-2.
Epidemiology of HIV/AIDS
• Currently more than 34.3 million people with HIV worldwide.
• Malaysia –Malaysia – No cases before 1986– end of 2003, 58012 accumulated cases.
• Malaysia majority are IDU’s, male & Malays.
5
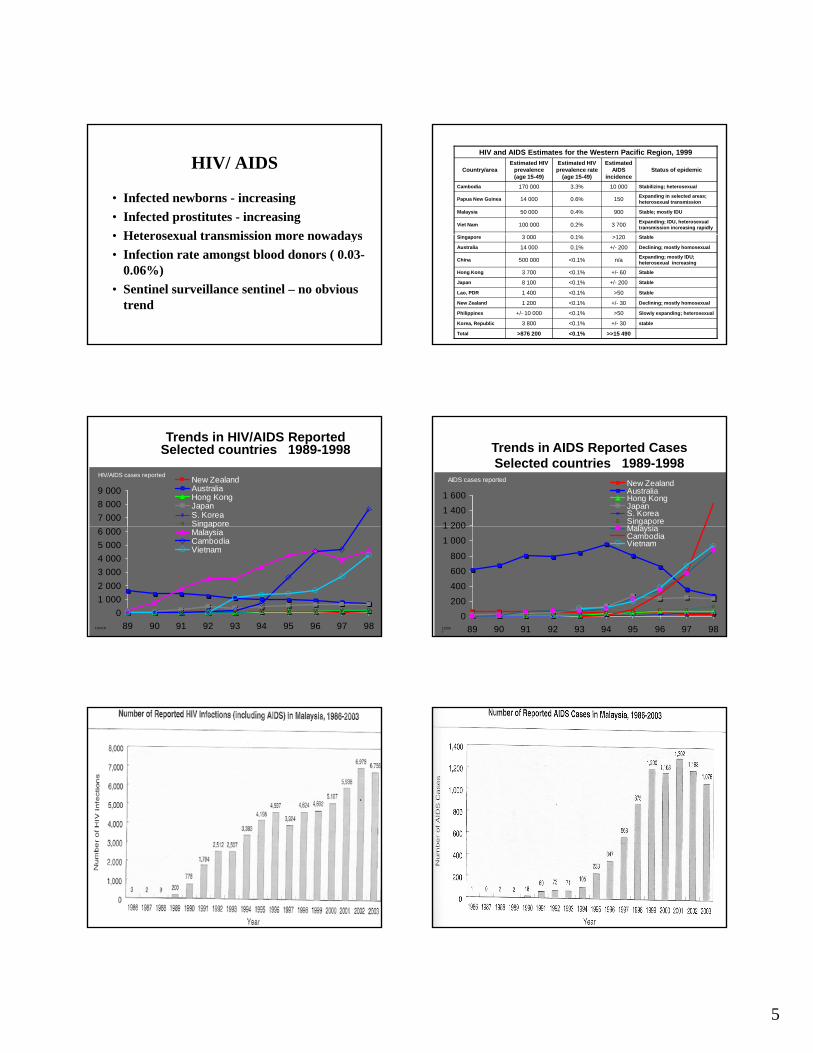
HIV/ AIDS
• Infected newborns - increasing• Infected prostitutes - increasing• Heterosexual transmission more nowadays• Heterosexual transmission more nowadays• Infection rate amongst blood donors ( 0.03-
0.06%)• Sentinel surveillance sentinel – no obvious
trend
HIV and AIDS Estimates for the Western Pacific Region, 1999
Expanding; IDU, heterosexual transmission increasing rapidly3 7000.2%100 000Viet Nam
Stable; mostly IDU9000.4%50 000Malaysia
Expanding in selected areas; heterosexual transmission1500.6%14 000Papua New Guinea
Stabilizing; heterosexual10 0003.3%170 000Cambodia
Status of epidemicEstimated
AIDS incidence
Estimated HIV prevalence rate
(age 15-49)
Estimated HIV prevalence (age 15-49)
Country/area
>>15 490<0.1%>876 200Total
stable+/- 30<0.1%3 800Korea, Republic
Slowly expanding; heterosexual>50<0.1%+/- 10 000Philippines
Declining; mostly homosexual+/- 30<0.1%1 200New Zealand
Stable>50<0.1%1 400Lao, PDR
Stable+/- 200<0.1%8 100Japan
Stable+/- 60<0.1%3 700Hong Kong
Expanding; mostly IDU; heterosexual increasingn/a<0.1%500 000China
Declining; mostly homosexual+/- 2000.1%14 000Australia
Stable>1200.1%3 000Singapore
Trends in HIV/AIDS ReportedSelected countries 1989-1998
7 0008 0009 000
HIV/AIDS cases reported New ZealandAustraliaHong KongJapanS. KoreaSingapore
01 0002 0003 0004 0005 0006 000
89 90 91 92 93 94 95 96 97 98
SingaporeMalaysiaCambodiaVietnam
110418
Trends in AIDS Reported CasesSelected countries 1989-1998
1 200
1 4001 600
AIDS cases reported New ZealandAustraliaHong KongJapanS. KoreaSingaporeM l i
0 200
400
600
800
1 000
1 200
89 90 91 92 93 94 95 96 97 98
MalaysiaCambodiaVietnam
110507
6
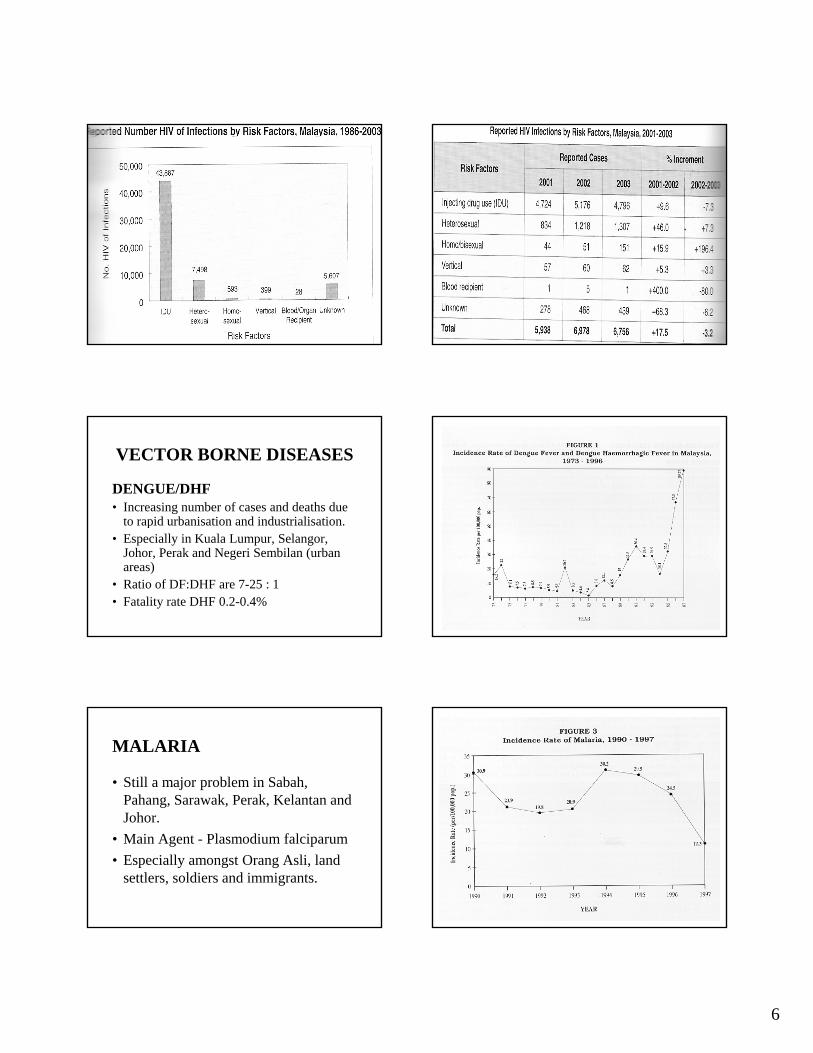
VECTOR BORNE DISEASES
DENGUE/DHF• Increasing number of cases and deaths due
to rapid urbanisation and industrialisation.p• Especially in Kuala Lumpur, Selangor,
Johor, Perak and Negeri Sembilan (urban areas)
• Ratio of DF:DHF are 7-25 : 1• Fatality rate DHF 0.2-0.4%
MALARIA
• Still a major problem in Sabah, Pahang, Sarawak, Perak, Kelantan and JohorJohor.
• Main Agent - Plasmodium falciparum • Especially amongst Orang Asli, land
settlers, soldiers and immigrants.

7
TUBERCULOSIS
Increasing trend, >50% new cases are infectiousNew cases - age 21-40 yrsNew cases age 21 40 yrs.-13% are imigrants (50% in Sabah, 15% in WP,KL)-cure rate 86% (1997)Mortality increasing due to late treatment and HIV/AIDS.
Survival Functions1.2
1.0
.8
.6Ujian ELISA
INTERVAL
16001400
12001000
800600
400200
0-200
Cum
Sur
viva
l .4
.2
0.0
Tidak reaktif
Tidak reaktif
-censored
Reaktif
Reaktif-censored

8
Non-Communicable Disease
Common Risk Factors of Lifestyle Diseases
Share Predisposing Conditions:– Hypertension – Obesity (especially central obesity)
Di b M lli– Diabetes Mellitus– Cancer
And Common Risk Factors:– Tobacco – Physical Inactivity – Irrational Diet (especially high fat intake)– Alcohol over-consumption
Adult Smoking (NHMS 3)
• 27.0% ever smokers• 21.5% current smokers• Higher amongst Malay (24 0%) rural• Higher amongst Malay (24.0%), rural
(32.3%), males (57.6%, females only 2.5%).• Higher in Kelantan (31.7%), Pahang
(29.8%) and Sabah (29.3%). Lowest in Penang (20.7%) - NHMS 2
Physical Inactivity
• NHMS 2 (20 minutes/day, 3x a week)– 11.6% exercised adequately, – 31.7% ever exercised– Nearly 70% of Malaysians do not exercise
• NHMS 3 (WHO-stepwise questionnaire, <150 minutes/week of moderate physical activities & 60 minute/week of vigorous physical activities) – 43.7% physically inactive– higher in woman, older age, urban residence,
unemployed and housewife.
Irrational Diet (NHMS 3)
• Underweight (BMI <18.5kg/m2) - 8.5%• Normal (BMI 18.5-24.9kg/m2) - 48.3% • Overweight (BMI 25 0 29 9 kg/m2) 29 1%• Overweight (BMI 25.0-29.9 kg/m2)-29.1% • Obese (BMI 30kg/m2 & >) - 14.1%• Overweight in 1996 16.6%, now 29.1%• Obese in 1996 4.4%, 2002/2003 12.7% and
now 14.1%.

9
Alcohol (NHMS 3)
• 16.2% ever drank• 7.4% current drinkers• For current drinker the
– age group between 70 – 74 years old (10.4%),
– Christians (25.6%), senior officer /
prevalence was higher in; – Sarawak state (15.0%), – in urban area (8.9%), – among males (11.8%), – Chinese (23.8%),
– senior officer / manager (24.8%), and
– married (7.9%). – tertiary level of
education (13.7%). – earned RM 5000 and
above per month (16.3%)
Major NCD Diseases
• Hypertension - 29.9% 1996, 32.2% in 2006• Cancer - 31,700 cases a year• Diabetes Mellitus 8 3% 1996 11 6% in• Diabetes Mellitus - 8.3% 1996, 11.6% in
2006.• Injury
HYPERTENSION
Increase of cases due to;
i•aging
•Smoking habit
•?life stressors•? Excessive dietary salt intake
HYPERTENSION• According to NHMS ’2006;
– Prevalence of 32.2%• Self-reported 11.5%• Previously undiagnosed 20.7%
• Higher in rural (36.9% vs 29.3%), Malays (33.9% vs 32.4% vs 29.4%) >30 yrs, obese/overweight
• Amongst the hypertensive, 35.8% were previously diagnosed. Among those who were previously diagnosed, 87.7% were on treatment. Of those on treatment, only 26.3% of their BP were under control.
CANCER
One of 5 main cause of death since 20 years ago.
Incidence -150 per 100,000 pop. (31,700 cases a year), the cases and deaths due to cancer are on the rise.
Related to lifestyle and the environment.
Burden of Cancer
• Incidence -150 per 100,000 pop. (30,000 case a year)
• Prevalence – 90,000• Incidence expected to rise with an increase of
aging population.– >60 yrs
• 1957 4.6%• 1990 5.7%• 2020 9.8%
GCC Lim, 2002. Overview of Cancer in Malaysia. Jpn J Clin Oncology

10
Incidence by Gender
• No nationwide population-based cancer registry. Data based on extrapolation.
• Survey between 1988-1990;y– Males 56.3 per 100,000– Females 56.9 per 100,000
• Penang registry 1994;– Males 115.9 per 100,000– Females 119.7 per 100,000
GCC Lim, 2002. Overview of Cancer in Malaysia. Jpn J Clin Oncology
Racial Differences
• Noted in NPC & oral cavity cancer• NPC amongst males by race;
– Malay 0.79 per 100,000Chi 15 9 100 000– Chinese 15.9 per 100,000
– Indian 1.1 per 100,000• NPC amongst females by race;
– Malay 0.8 per 100,000– Chinese 4.1 per 100,000– Indian 0 per 100,000
Incidence by Type Diabetes Mellitus – (NHMS3)
• Overall prevalence was 11.6%. Knowndiabetes was 7.0%. Newly diagnosed diabetes was 4.5%.
• Higher in the urban at 12.1% compared to the rural areas at 10.5%.
• Between ethnicity, Indians have the highest prevalence of 19.9% , followed by Malays 11.9% and Chinese 11.4%.
INJURY
Main cause of death and hospital admission - MVA & fall.
Upward trend.

11
Diseases Due To Migration
Conclusion
• Malaysia is a country undergoing a health transition• Improving socioeconomic status and aging
population leads to chronic & degenerative diseases. Problems such as;
Occupational diseasesChemical poisoning from industry and agricultureDiseases due to air pollutionWork injury and MVADisease related to urbanisation
• Trend of disease approaching those of developed countries and yet unable to shake off the diseases of developing countries. A double burden…………


















