
Epidemiology of Babesiosis, including Transfusion-Associated Infection Barbara L. Herwaldt, MD, MPH...
63
Epidemiology of Babesiosis, including Transfusion-Associated Infection Barbara L. Herwaldt, MD, MPH Centers for Disease Control and Prevention Parasitic Diseases Branch
-
Upload
ross-sullivan -
Category
Documents
-
view
221 -
download
0
Transcript of Epidemiology of Babesiosis, including Transfusion-Associated Infection Barbara L. Herwaldt, MD, MPH...

Epidemiology of Babesiosis, including Transfusion-Associated
Infection
Barbara L. Herwaldt, MD, MPHCenters for Disease Control and Prevention
Parasitic Diseases Branch

Babesiosis Basics
The views expressed are those of the speaker and do not necessarily represent
those of CDC

Point …
Counterpoint …

•. . . are intraerythrocytic microbes BUT they are NOT Plasmodium parasites
•. . . are tickborne in nature BUT they are NOT bacteria
• . . . are transmissible by transfusion BUT they are NOT viruses
Babesia: Yes . . . But . . .

Babesiosis: Don’t assume
•Don’t assume ring forms = malaria Consider babesiosis
•Don’t assume route of transmission = tickborne Consider blood transfusion, regardless of
region or season
•Don’t assume the species = B. microti Consider other etiologic agents

Temporal and spatial
dimensions

1979: 1st described transfusion case (MA; B. microti)
1956: 1st documented zoonotic case (Yugoslavia)
1966: 1st documented U.S. case (California); species?
1969: 1st documented case on Nantucket (B. microti)
1888: Viktor Babes ― febrile hemoglobinuria in “Rumanian” cattle caused by intraerythrocytic microbe
1893: Smith & Kilbourne ― Texas cattle fever caused by tickborne parasite (B. bigemina); 1st demonstration of an arthropod vector

Geographic distribution of reported human cases of babesiosis:
the bulk in the USA (several thousand)
some in Europe (several dozen)
a few in various other regions


NASA/GSFC/JPL, MISR Team
Cape Cod
Nantucket

Babesia microti


NASA/GSFC: J Schmaltz, MODIS Rapid Response Team

Tickborne transmission of B. microti is predominantly seasonal and regional, particularly in evolving foci in the Northeast (CT, MA, NJ, NY, and RI) and the upper Midwest
(MN and WI)
Babesiosis is reportable (under surveillance) in these and multiple other states and will become nationally notifiable in January 2011

I. scapularis eg, deer mice (Peromyscus leucopus)
Babesia microti
Ecologic niche
Babesia microti in U.S. foci
The risk for zoonotic transmission is dynamic in time & place
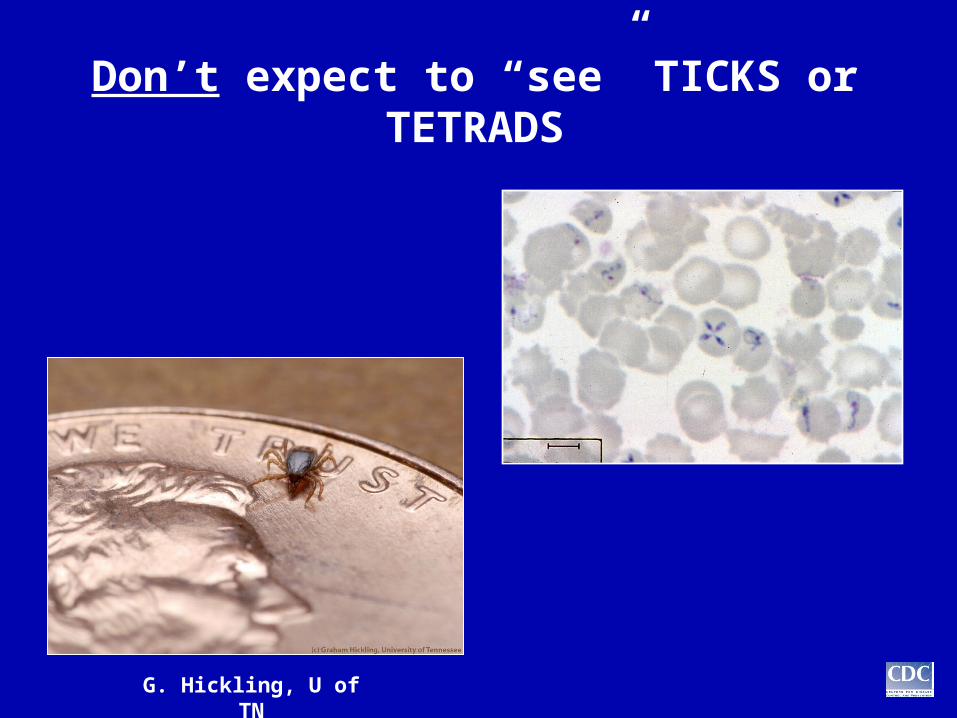
Don’t expect to “see” TICKS or TETRADS
G. Hickling, U of TN
“Other” zoonotic Babesia agents
• Since the 1990s, sporadic U.S. cases caused by other etiologic agents have been described, such as:
B. duncani (the WA1-type parasite) and related organisms (CA1-type parasites) in several western states
B. divergens “like” agents (eg, MO1) in various regions
• Their geographic ranges, tick vectors, and reservoir hosts largely remain unknown
• Infection with these parasites is not detected by molecular or serologic tests for B. microti

Taxonomy 101

Babesiosis: Taxonomy
• Phylum: Apicomplexa
• Order: Piroplasmidora
• Family: Babesiidae
• Genus: Babesia
• Species: Reportedly, ~100 Babesia “species” that infect
mammals have been described
Traditionally, taxonomy has been based primarily on morphology and host specificity

Examples of “novel agents”
B. divergens “like”EU1
B. duncani (WA1 type)CA1 type
MO1

WA1, WA2, WA3
Isolate Patient (year)
Index patient (1991)WA1
WA2 Blood recipient (1994)
WA3 Blood donor (1994)

Asplenic
Asplenic (died)
Asplenic
Asplenic
DNA only
DNA only
DNA only
DNA only
DonorTick (presumed)1994YesWA3
Recipient (elderly patient)Blood (RBCs)1994 YesWA2
Index case-patient Tick (presumed)1991YesWA1
Tick (presumed)
Tick (bitten 19d before onset)
Tick (presumed)
Tick (presumed)
1994
1993
1992
1991
CA4
CA3
CA2
CA1
Recipient (premature infant)Blood (RBCs) 2000YesCA5DonorTick (presumed; CA or Oregon)2000 YesCA6
CharacteristicsTransmissionYearIsolated? Name
The initial WA’s and CA’s

Description of Babesia duncani n.sp. and its differentiation from other piroplasms
Conrad, Kjemtrup, Carreno, Thomford, Wainwright, Eberhard, Quick, Telford, Herwaldt
Intern J Parasitol 2006

Babesia duncani (WA1 type)

Old name New name
WA1 B. duncani (syntype isolate)
WA2 B. duncani
WA3 B. duncani
CA1CA1-type parasitesCA2
CA3
CA4
CA5 (~ a “WA”!) B. duncani (syntype isolate)
CA6 (~ a “WA”!) B. duncani
The Christening

Examples of “novel agents”
B. divergens “like”EU1
B. duncani (WA1 type)CA1 type
MO1

Babesia divergens
“LIKE”(but not “sensu stricto”)

MO1(index case occurred in 1992 in an asplenic
patient)
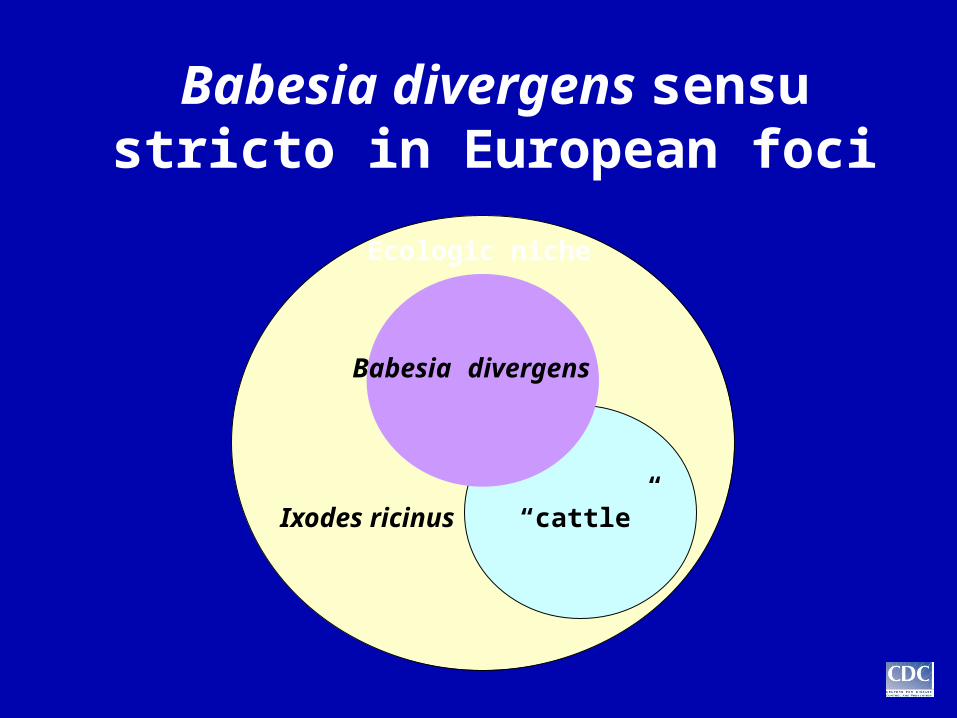
Ixodes ricinus “cattle”
Babesia divergens
Ecologic niche
Babesia divergens sensu stricto in European foci

Europe: B. divergens vs B. divergens “like”
• 1st reported human case occurred in 1956 in an asplenic patient in Yugoslavia
• >30 tickborne cases have been reported: Most were in asplenic patients and reportedly
were caused by B. divergens; but the type and quality of evidence varied
In 1998 and 2000, the index cases caused by “EU1” (European Union 1) were identified in asplenic patients in Italy and Austria


Back to Washington

(the case occurred in 2002 in an asplenic patient)

Back to the basics

Babesiosis: Clinical aspects
• Regardless of the route of transmission, Babesia infection can
range from asymptomatic to severe
• Regardless of their severity, the manifestations are nonspecific;
diagnostic testing is required
• Symptoms, if any, usually develop within several weeks or
months of the exposure BUT they may 1st appear much later (eg, after splenectomy)
• Risk factors for severe babesiosis include asplenia, advanced
age, and various other causes of immune dysfunction
BUT “immunosuppressed” patients may be afebrile and/or
have subacute, remitting-relapsing clinical courses

Babesiosis: Clinical aspects
• Even persons who have asymptomatic infection or whose symptoms resolve may have low-level parasitemia for weeks to months, sometimes for longer than a year
• People can meet all of the criteria for donating blood despite being infected and infective

Persistent parasitemia after acute babesiosis
(Krause, et al. N Eng J Med, 1998)

Serologic
Parasitologic(including molecular)
Laboratory evidence of infection

Laboratory approaches
in different settings

Diagnostic testing
versus
Donor screening

What’s the gold
standard?

Cautionary notes
• Although some commercial laboratories offer Babesia serologic and molecular testing, there are no FDA-cleared “test kits” for in vitro diagnostic use (even for B. microti)
• Testing is done with “reagents” assembled and evaluated by the individual laboratory
• Inter- and intra-laboratory variability may be noted with respect to the sensitivity, specificity, reliability, and validity of “the assay” (patient data/results)

Babesiosis: “Diagnosis”
•Parasitologic diagnosis (“direct”) Detects parasites (DNA) BUT not sufficiently sensitive to reliably
detect low-level infection
•Serodiagnosis (“indirect”) Highly sensitive BUT may be negative early in infection; does
not reliably distinguish active from past infection (an advantage in retrospective transfusion investigations)
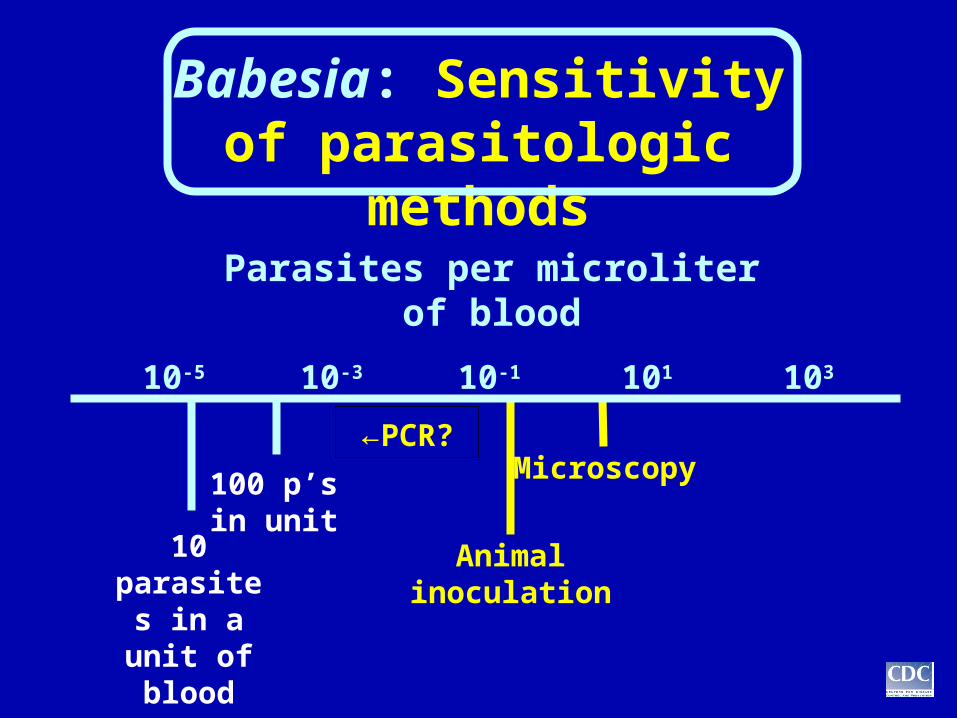
Babesia: Sensitivity of parasitologic methods
←PCR?Microscopy
Animal inoculation
Parasites per microliter of blood
10-5 10-3 10-1 101 103
10 parasites in a unit of blood
100 p’s in unit
PCR results are helpful if positive
But negative results do not exclude low-level parasitemia
(low concentrations of parasites / DNA; small volumes tested vs transfused)

Cautionary notes
• In transfusion investigations, blood donors typically are implicated on the basis of seropositivity (with or without PCR positivity) and epidemiologic plausibility
• In our experience, the likelihood of PCR positivity is higher for segments than for follow-up (postdonation) specimens but does not approach 100%

Case counts
Surveillance(biovigilance)

How many tickborne and transfusion-
associated cases have been
“reported” to date?

Also . . .
How, where, when, and by whom/what
were cases detected, diagnosed,
investigated, “reported,” and tallied?
Case cr
iteria
?

Basic tools

Case counts: the log scale

There’s typically a “story”
Even severe cases often are serendipitously
detected


To date, >100 U.S. transfusion-associated Babesia cases have been “reported”

To date . . .
Among “reported” cases . . .

Babesiosis: U.S. transfusion cases
• Etiologic agents Most cases were caused by B. microti
Several were caused by B. duncani
• Blood components Most cases were linked to RBCs
Several were linked to platelets
• Incubation period: weeks to many months

Multi-donation cluster of cases—Minnesota, 1999-2000
Donor Recipients
7/12/99 RBCs (7/22): PCR+ Platelets (7/16): IFA-1
9/23/99 RBCs (10/7): PCR+2
11/19/99RBCs (11/29): Index patientPlatelets (11/23): IFA-
3
1/21/00 Platelets (1/25): IFA+ 4
The donor was still PCR+ in April ‘00, 10 months postexposure (during a camping trip in Minnesota in June ‘99)
(Herwaldt, et al. Transfusion, 2002)

─Unrecognized, protracted infection in some donors─
─Donor travel to & from foci of endemicity─
─Intraregional distribution & interregional shipment of blood─
Translate into the potential for
Transmission by transfusion
any time (year-round)
─ any where ─

Transmission in all 4 seasons

Babesiosis without borders
(but not equal risk)

Whither Babesia?
Point …
Counterpoint …



















