
Epid 600 Class 7 Experimental Studies
41
EPID 600; Class 7 Experimental studies University of Michigan School of Public Health 1
Transcript of Epid 600 Class 7 Experimental Studies
EPID 600; Class 7 Experimental studies
University of Michigan School of Public Health
1
Three key dimensions to epidemiologic studies
Measures of association Relative measures (relative risks, rates, and odds) Absolute measures (risk and rate differences) Study design Observational Cohort Case-control Cross-sectional Experimental Randomized trial Field trials Group randomized trials Units of analysis Individual Group
2
Three key dimensions to epidemiologic studies
Measures of association Relative measures (relative risks, rates, and odds) Absolute measures (risk and rate differences) Study design Observational Cohort Case-control Cross-sectional Experimental Randomized trial Field trials Group randomized trials Units of analysis Individual Group
3
The world
persons “exposed” persons “unexposed”
4

The experimental study
persons “exposed” persons “unexposed”
5
What is an experimental study?
Randomized controlled trials are sub-types of cohort studies in which exposure (i.e., treatment) is randomly assigned by the investigator (or by some other, observable phenomenon) Have a long history in clinical medicine Although experimental studies come in many types, principles are the same and clinical trials dominate the field
6
Clinical trials
In clinical trials, the participants are typically patients Point of trial is to assess the influence of a drug and to ensure that taking a drug does not increase complications unduly Example of a clinical trial: Patients with HIV are randomized to treatment Z vs placebo and followed for 2 years for development of infection
7
(Almost) aside 1...field trials
Participants are not patients, but rather persons in the general community The primary objective of field trials is typically the primary prevention of disease Classic example is the Salk Polio Vaccine Trials in 1954
8

(Almost) aside 2…group randomized trials
Exposure is assigned to groups of people, not to individuals Example: A trial of a particular form of advertising message aimed at decreasing drunk driving where the message is shown in one community but not in another and then drunk driving rates are assessed
9
Randomized controlled trials
Have variously been described as “gold standard” or “most rigorous” study in epidemiology Reason for epidemiologists’ fealty to RCTs is the ability of RCTs to, in theory, control confounding
10
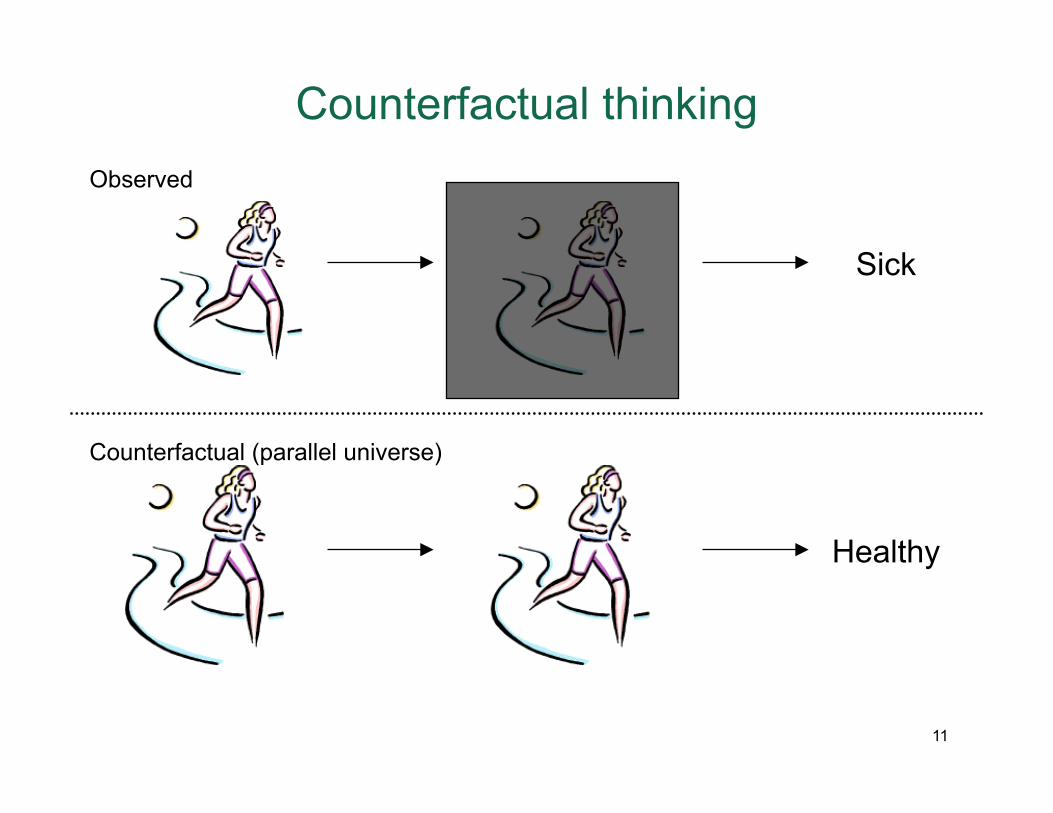
Sick
Healthy
Observed
Counterfactual (parallel universe)
Counterfactual thinking
11
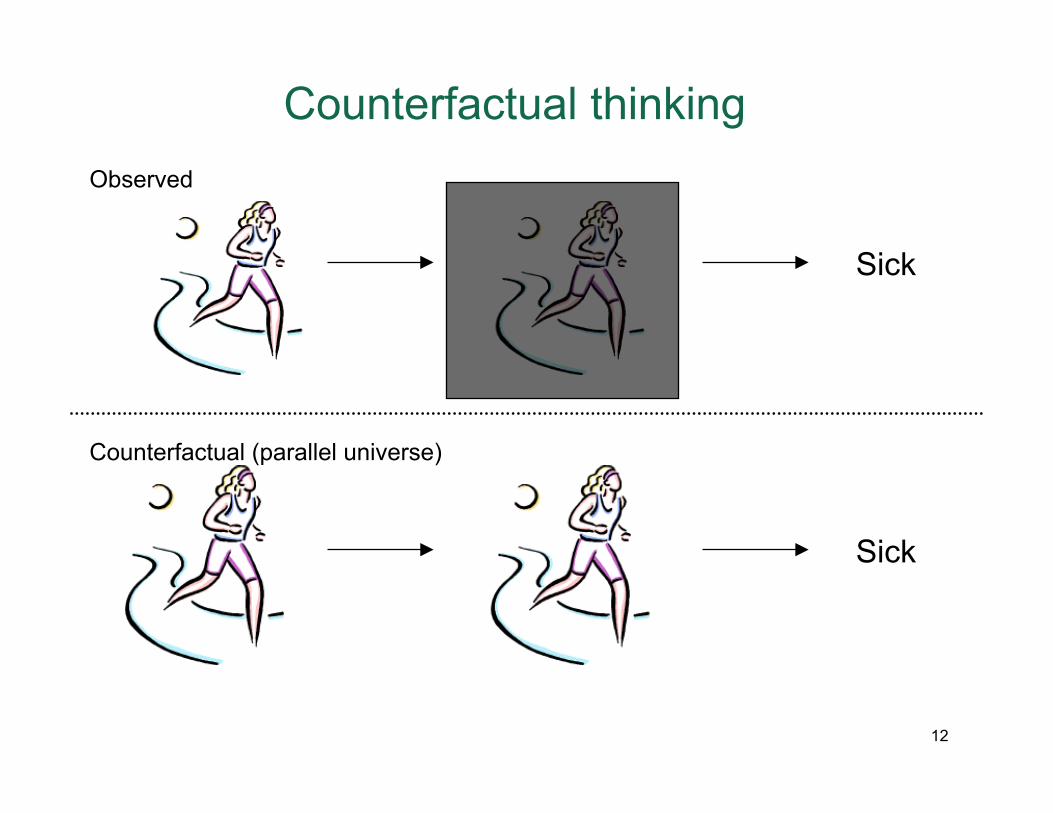
Counterfactual thinking
Sick
Sick
Observed
Counterfactual (parallel universe)
12
Central features of clinical trial... randomization
Randomization is the process by which each participant’s treatment is determined by some random mechanism The primary purpose of randomization is the minimizing of confounding
Why?
When we randomize we, in theory, create groups (experimental and control) that are not determined by any other factor other than by chance, so groups should be as similar to one another as possible, hence minimizing confounding.
13

Randomization procedures
Randomization can be carried out in many different ways Simple random allocation assigns participant to a trial group based on a pre-determined allocation plan (e.g., table of random numbers, or flipping a coin) Randomization may also happen in conjunction with other techniques to control confounding For example, pre-determined strata of key variables (e.g., gender) can be chosen and then randomization happens within these strata
14
Thwarting randomization
If technical process of randomization (e.g., random number selection) is flawed If participants are aware of result of un-blinded trial arm (i.e., “I don’t want to participate if I only get the placebo”) Some degree of reassurance about success of randomization can be obtained by comparing characteristics of intervention and control group (e.g., age, gender distributions etc)
15
Blinding
Trials can be unblinded, i.e., where both investigator and participant know what arm they are in e.g., trial of a particular dietary regimen, where participant knows what she is eating, as does investigator
Trials can be single blinded, i.e., where participant does not know but investigator does know treatment assignment e.g., trial of a video-based cognitive therapy, where participant does not know if s/he is watching experimental or control video, but investigator does
Trials can be double blinded; i.e., where neither participant nor investigator know treatment assignment e.g., drug trials, where participants simply take a “blue” or “red” pill and no one knows which pill is which; data are coded and code only broken by outside monitors or at the end of the study 16
Purpose of blinding
The purpose of blinding is to remove bias or systematic error
Bias can also be in the form of selection bias; study recruiters can be eager to recruit “sick persons” into experimental arm e.g., Nurses in hospital recruiting participants for an experimental drug will, wanting to do good by the sick patient, differentially recruit those who are “sicker” into experimental arm
Bias can be in the form of information bias, where investigators who are monitoring a study draw different conclusions depending on their knowledge of which study arm particular participant is in e.g., In a study where the end point is hypertension, investigators taking blood pressure may be more likely to accept a low blood pressure on someone they know is in experimental arm
Bias can be in the form of differential care given to persons in different study arms e.g., Clinicians may more aggressively treat persons known to be in the study experimental arm taking a new drug to “make sure” the drug “works” 17
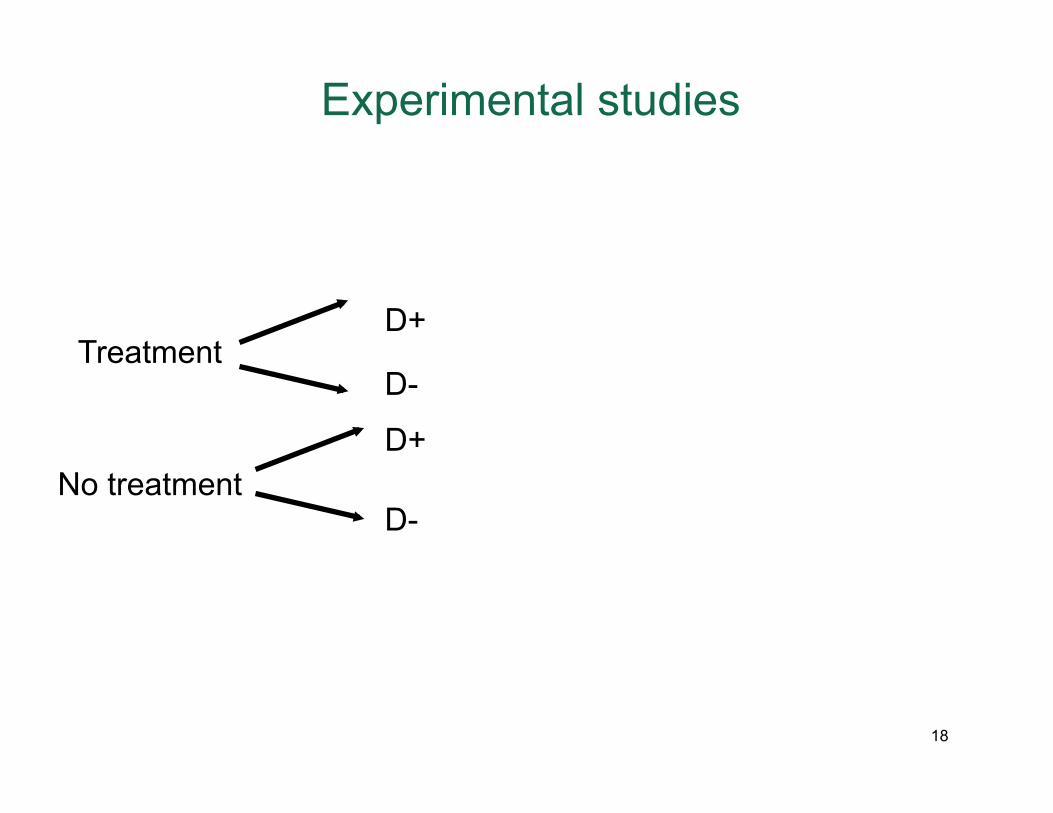
Treatment
No treatment
D+
D-
D+
D-
Experimental studies
18
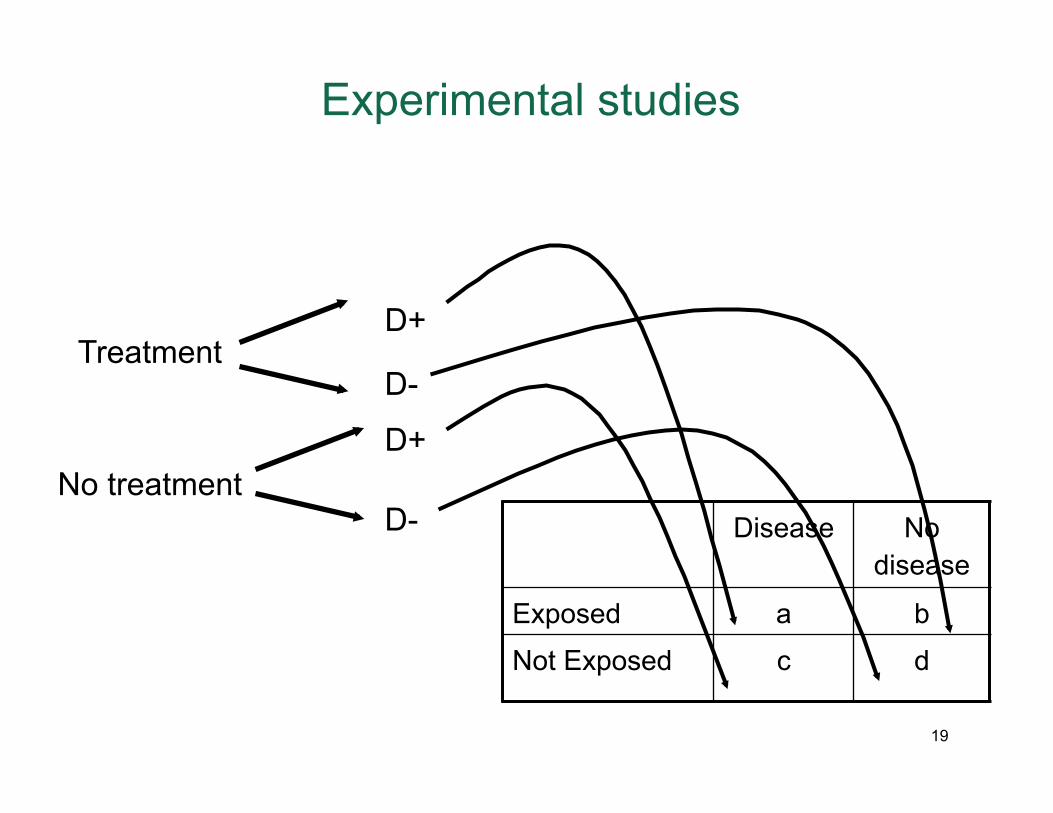
Treatment
No treatment Disease No
disease
Exposed a b
Not Exposed c d
D+
D-
D+
D-
Experimental studies
19
Depression outreach: a RCT
Depression costs the US economy billions of dollars largely due to productivity losses Employers are hesitant to invest in enhanced depression screening-treatment programs ostensibly because of worries about whether this investment will be returned Researchers evaluated the effects of depression outreach-treatment programs on workplace outcomes
Wang et al. Telephone screening, outreach, and care management of depressed workers and impact on clinical and work productivity outcomes: a randomized controlled trial. JAMA. 2007; 298:1401-1411.
20
Depression outreach RCT: set up
Investigators decide who gets exposed and who doesn’t Participants: 604 employees covered by a managed behavioral health plan identified as having significant depression
Exposure: the intervention Outcome: depression scores and work performance outcomes
Wang et al. Telephone screening, outreach, and care management of depressed workers and impact on clinical and work productivity outcomes: a randomized controlled trial. JAMA. 2007; 298:1401-1411.
21
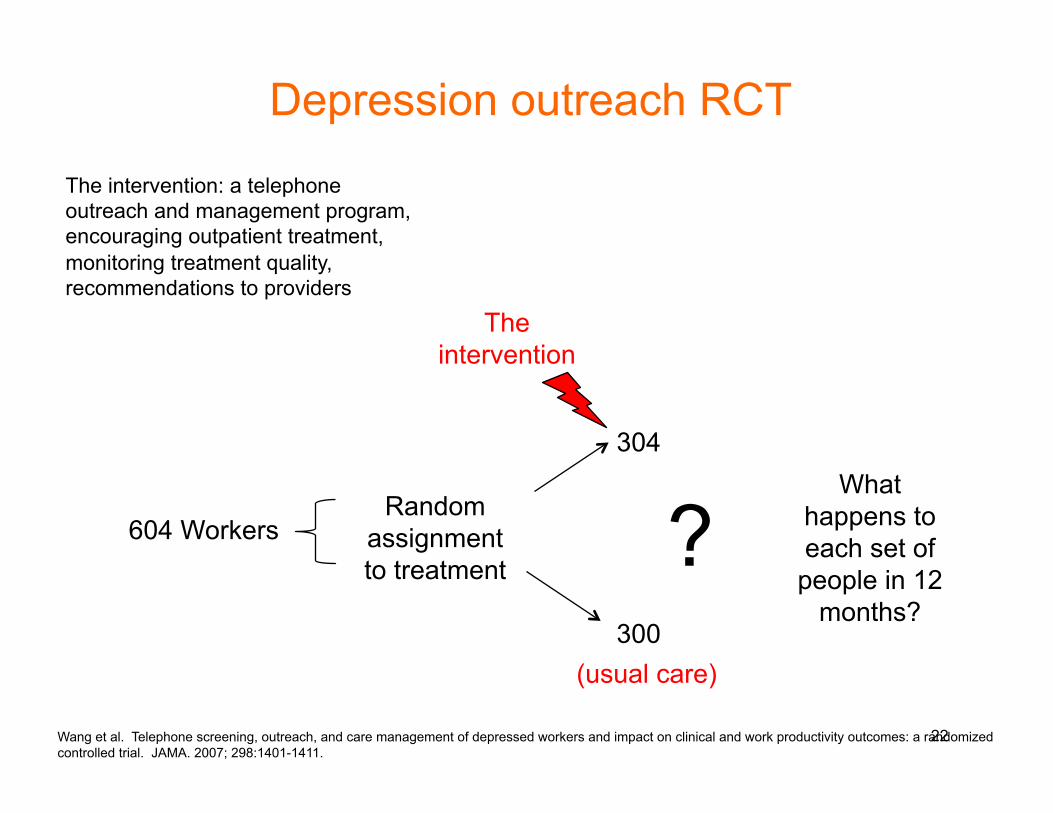
Depression outreach RCT
The intervention: a telephone outreach and management program, encouraging outpatient treatment, monitoring treatment quality, recommendations to providers
What happens to each set of
people in 12 months?
604 Workers Random
assignment to treatment
304
300
The intervention
(usual care)
?
Wang et al. Telephone screening, outreach, and care management of depressed workers and impact on clinical and work productivity outcomes: a randomized controlled trial. JAMA. 2007; 298:1401-1411.
22
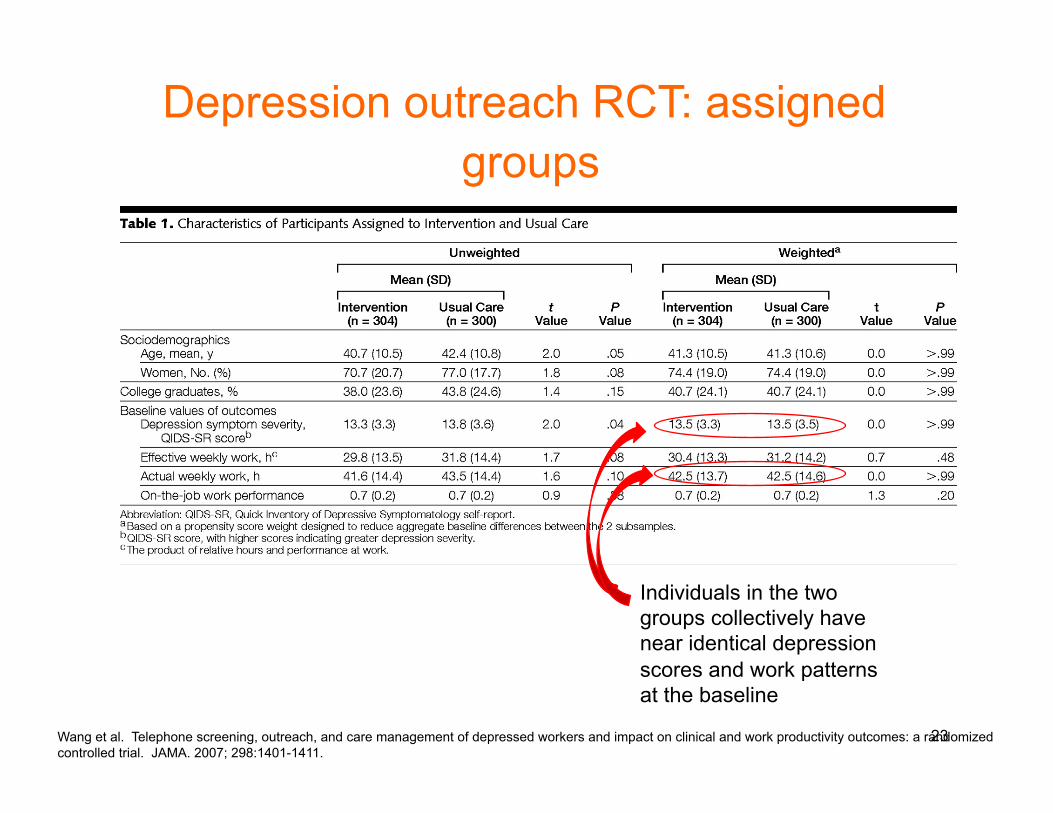
Depression outreach RCT: assigned groups
Individuals in the two groups collectively have near identical depression scores and work patterns at the baseline
Wang et al. Telephone screening, outreach, and care management of depressed workers and impact on clinical and work productivity outcomes: a randomized controlled trial. JAMA. 2007; 298:1401-1411.
23

Depression outreach RCT: findings
Those individuals assigned to the intervention had a greater odds of substantial improvement and recovery from depression (OR=1.4 for both) at the end of one year
Wang et al. Telephone screening, outreach, and care management of depressed workers and impact on clinical and work productivity outcomes: a randomized controlled trial. JAMA. 2007; 298:1401-1411.
24
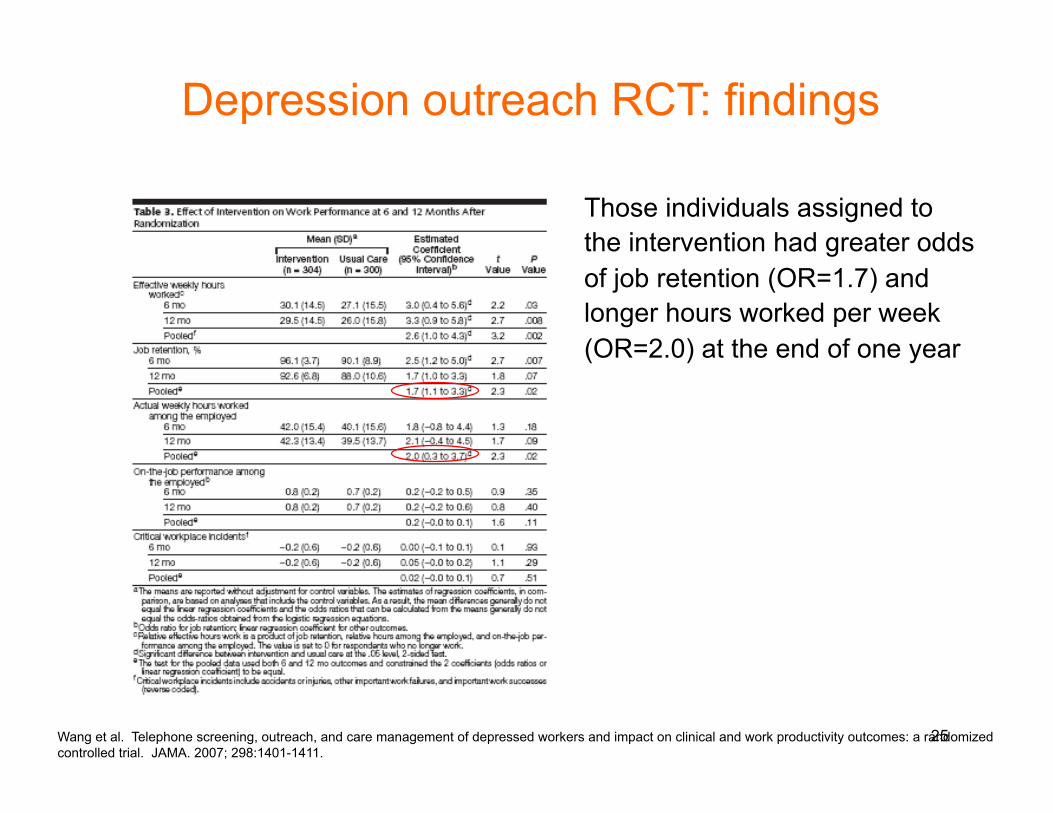
Depression outreach RCT: findings
Those individuals assigned to the intervention had greater odds of job retention (OR=1.7) and longer hours worked per week (OR=2.0) at the end of one year
Wang et al. Telephone screening, outreach, and care management of depressed workers and impact on clinical and work productivity outcomes: a randomized controlled trial. JAMA. 2007; 298:1401-1411.
25
When might an RCT be indicated?
Exposure is a modifiable factor which persons will let you modify, e.g., taking a pill, trying a different diet When there is ethical equipoise, that is when we really do not know whether a particular exposure is associated with benefit or with harm A particular exposure may have an influence on multiple outcomes of tremendous importance In experimental trials, in contrast with other epidemiologic study designs we have discussed, we are doing something to participants so we have to be certain that, first, we do no harm
26
Typical comparison (control) groups in RCTs
Placebo Pills that are biologically inert (e.g., filled with olive oil) Designed to resemble test drug as much as possible, but without the active component Placebos to be able to account for potential “placebo effect”, i.e., improvement in clinical condition due simply to the taking of a drug, rather than to a drug’s active component An alternate intervention May be used to compare interventions to identify best alternative May involve “usual care” which may well include some form of ongoing treatment May involve a standardized “attention control” where, for the implementation of a behavioral intervention, as much attention is given to controls to make sure that intervention effects are not simply due to the fact that participants are part of a trial 27
Considerations in selecting a study population for an RCT
Source population is the population for whom the results of the intervention are thought to be applicable The study population is the group in which the intervention is applied Clearly, we would like the results of the study to be generalized beyond the study population, so we have to be concerned with being able to validly draw inference beyond those actually studied
28
Aside...internal vs. external validity
Internal validity is the ability to reach the correct conclusion among those actually studied, i.e., the absence of methodologic problems in a particular study Internal validity can be threatened by potential confounders and biases, to be discussed in next few lectures
External validity is the generalizability of the study to the rest of the population; i.e., are nurses recruited at a particular point in time really representative of the general population today
29
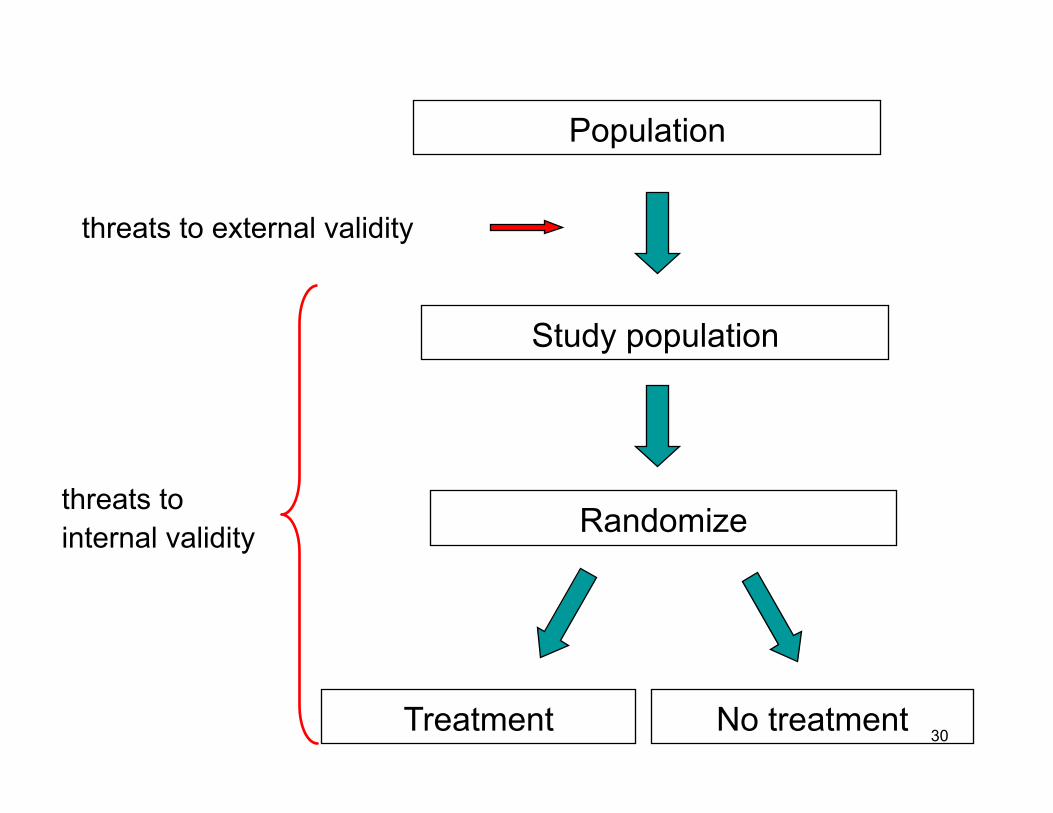
Population
Study population
Randomize
Treatment No treatment
threats to external validity
threats to internal validity
30
Participant selection; factors to consider in determining eligibility criteria
1.Potential benefits and risks of intervention i.e., who would benefit from intervention; for whom would the
intervention pose unacceptable risk interventions should not be “tried” on those who may not benefit
from it (e.g., different racial/ethnic groups) 2. Enhancing power of trial trial may be restricted to persons with known high incidence of a
particular outcome 3. Concerns about internal validity participants may be selected who will provide valid and reliable
data (e.g., issues re: mental status, language fluency) minimize persons who are likely to be “lost to follow-up”
NOTE: some of the above factors may then end up jeopardizing external validity 31
Informed consent in experimental studies
By federal regulations participants must be told: That they would be participating in research The research procedures involved The potential risks and discomfort The potential benefits (including to society) Alternative procedures of possible advantage to participant Extent to which information gathered will remain confidential Medical services available in the event of an injury Whom to contact with questions Voluntary nature of participation and right to withdraw without penalty or loss of benefits
32
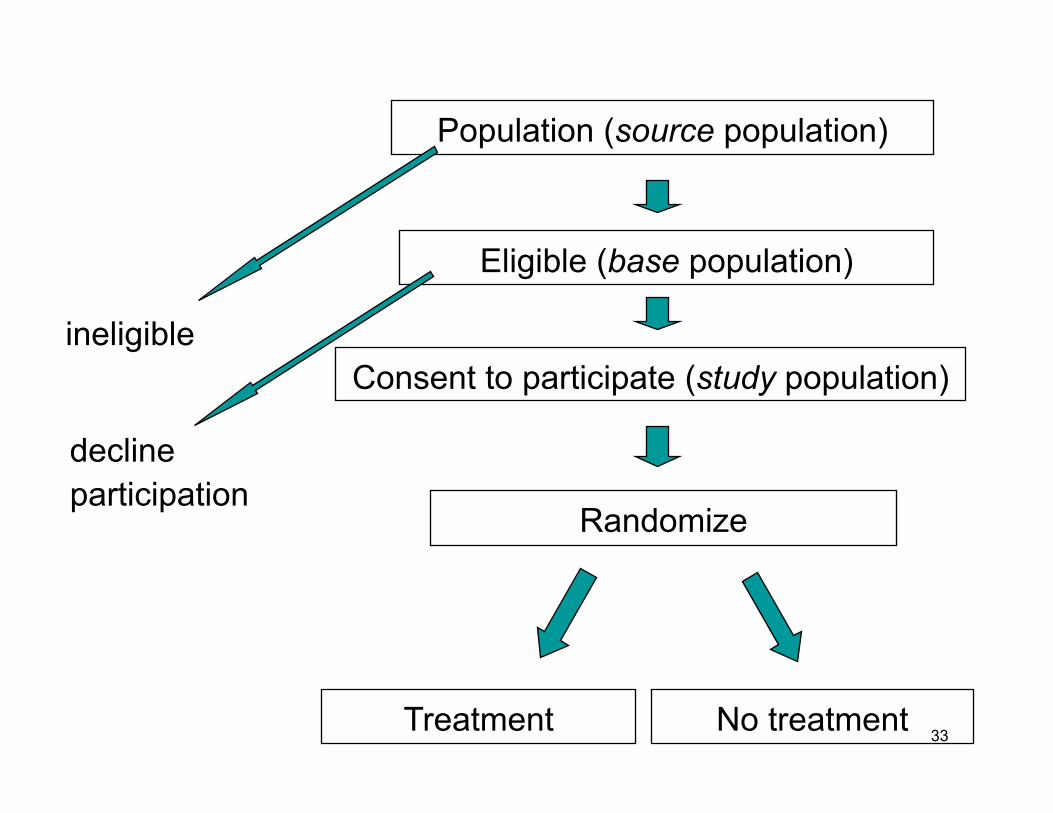
Population (source population)
Eligible (base population)
Randomize
Treatment No treatment
Consent to participate (study population) ineligible
decline participation
33
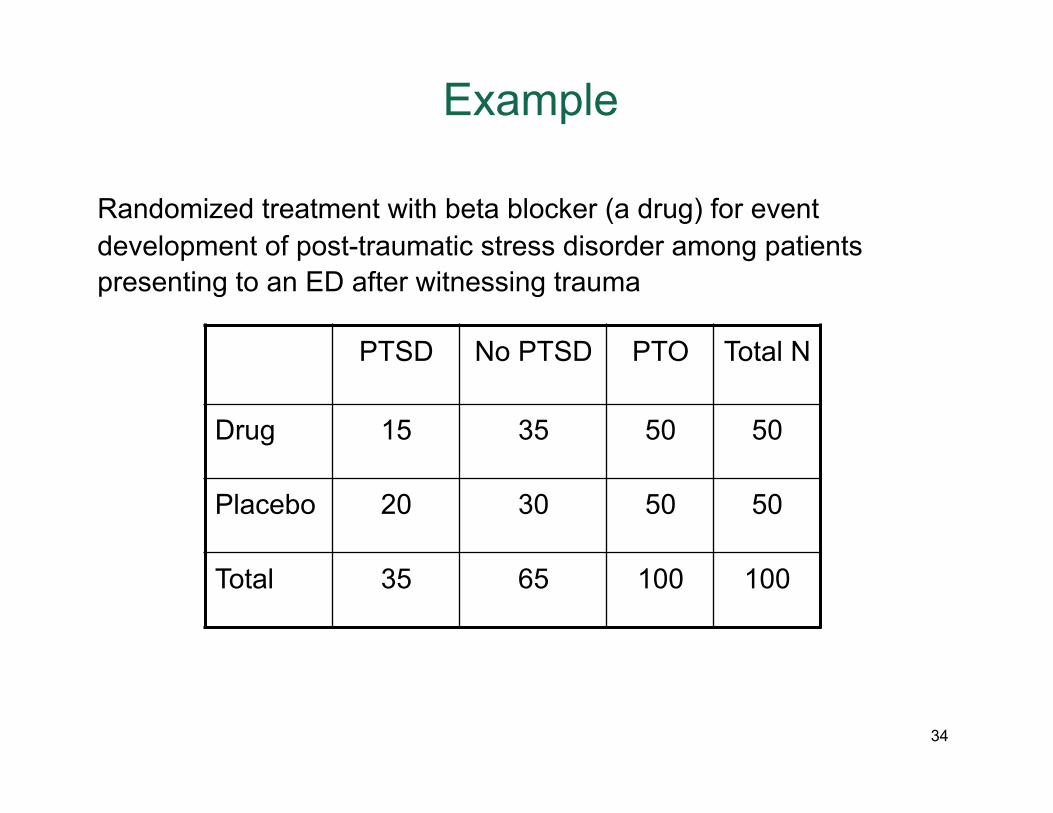
Example
Randomized treatment with beta blocker (a drug) for event development of post-traumatic stress disorder among patients presenting to an ED after witnessing trauma
PTSD No PTSD PTO Total N
Drug 15 35 50 50
Placebo 20 30 50 50
Total 35 65 100 100
34
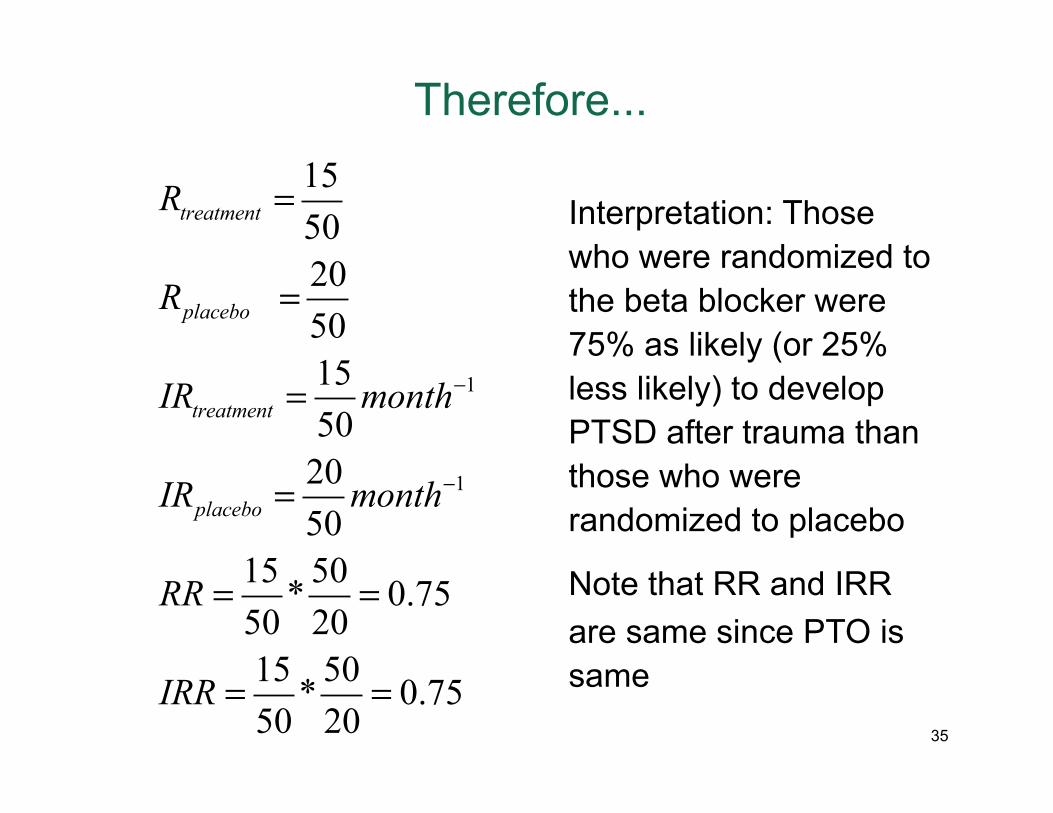
Therefore...
1
1
1550205015502050
15 50* 0.7550 2015 50* 0.7550 20
treatment
placebo
treatment
placebo
R
R
IR month
IR month
RR
IRR
−
−
=
=
=
=
= =
= =
Interpretation: Those who were randomized to the beta blocker were 75% as likely (or 25% less likely) to develop PTSD after trauma than those who were randomized to placebo
Note that RR and IRR are same since PTO is same
35
Intent to treat approach
An “intent to treat” approach considers the effect of the intervention as it was “intended”, not as it actually happened Therefore, persons who were randomized to treatment and to control are analyzed as such This minimizes non-comparability between groups (since group comparability was based on original randomization not on who did eventually take treatment vs. not) As we will discuss in next lectures, if we do not carry out ITT analyses we are introducing confounding
36
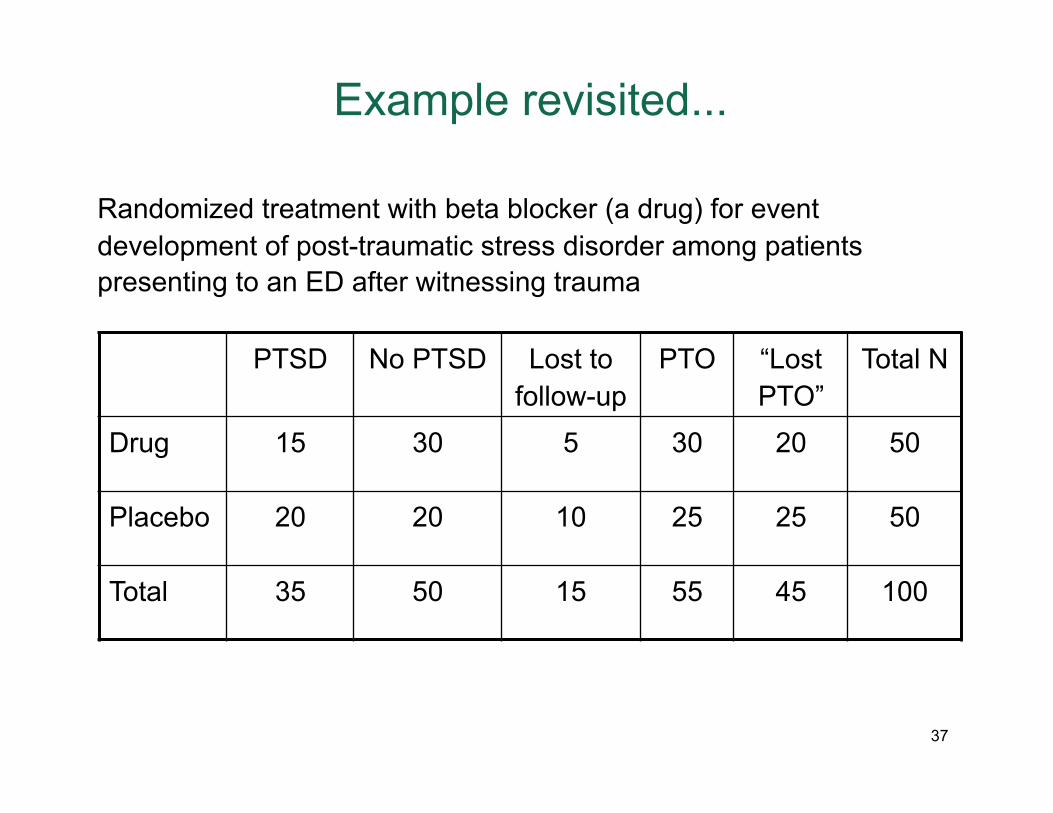
Example revisited...
Randomized treatment with beta blocker (a drug) for event development of post-traumatic stress disorder among patients presenting to an ED after witnessing trauma
PTSD No PTSD Lost to follow-up
PTO “Lost PTO”
Total N
Drug 15 30 5 30 20 50
Placebo 20 20 10 25 25 50
Total 35 50 15 55 45 100
37
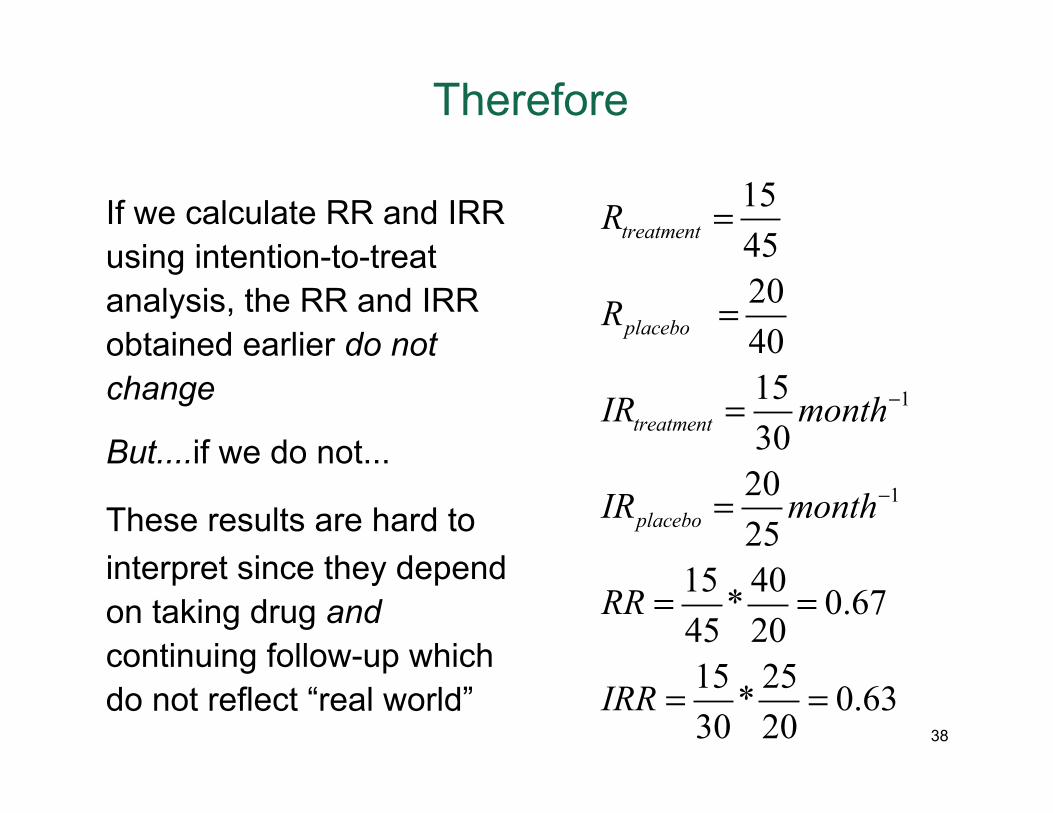
Therefore
If we calculate RR and IRR using intention-to-treat analysis, the RR and IRR obtained earlier do not change
But....if we do not...
These results are hard to interpret since they depend on taking drug and continuing follow-up which do not reflect “real world”
1
1
1545204015302025
15 40* 0.6745 2015 25* 0.6330 20
treatment
placebo
treatment
placebo
R
R
IR month
IR month
RR
IRR
−
−
=
=
=
=
= =
= =38
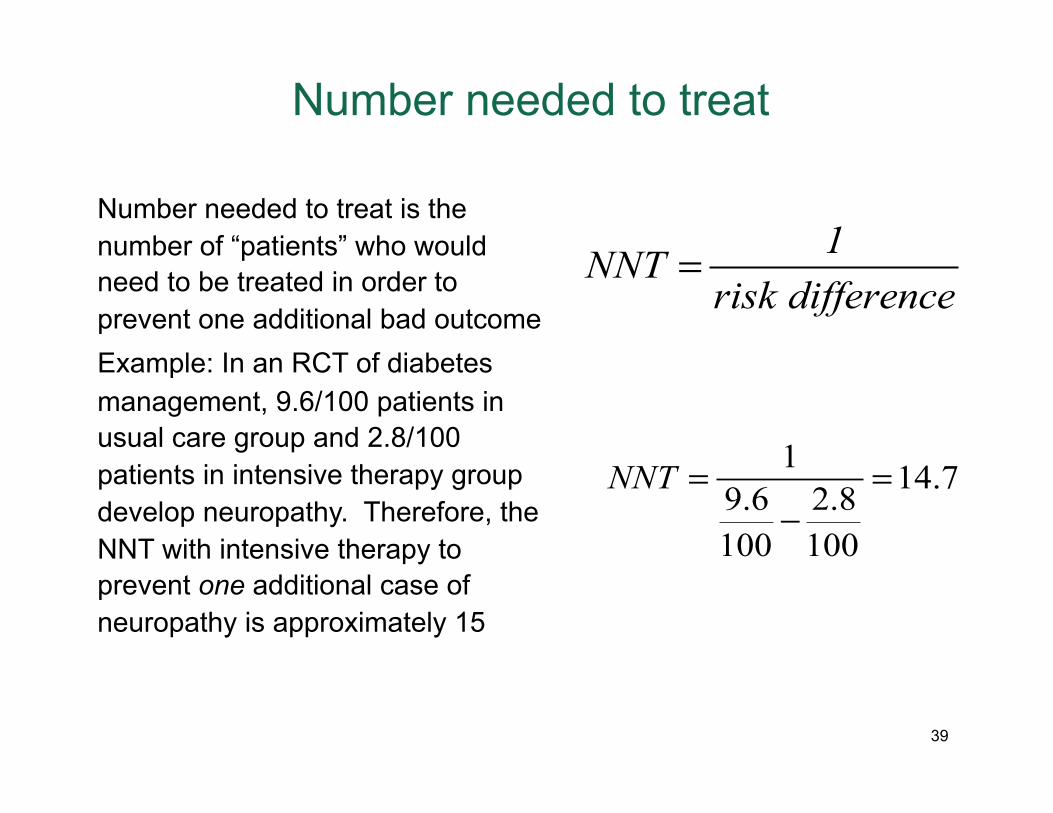
Number needed to treat
Number needed to treat is the number of “patients” who would need to be treated in order to prevent one additional bad outcome Example: In an RCT of diabetes management, 9.6/100 patients in usual care group and 2.8/100 patients in intensive therapy group develop neuropathy. Therefore, the NNT with intensive therapy to prevent one additional case of neuropathy is approximately 15
1NNT risk difference
=
1 14.79.6 2.8100 100
NNT = =−
39
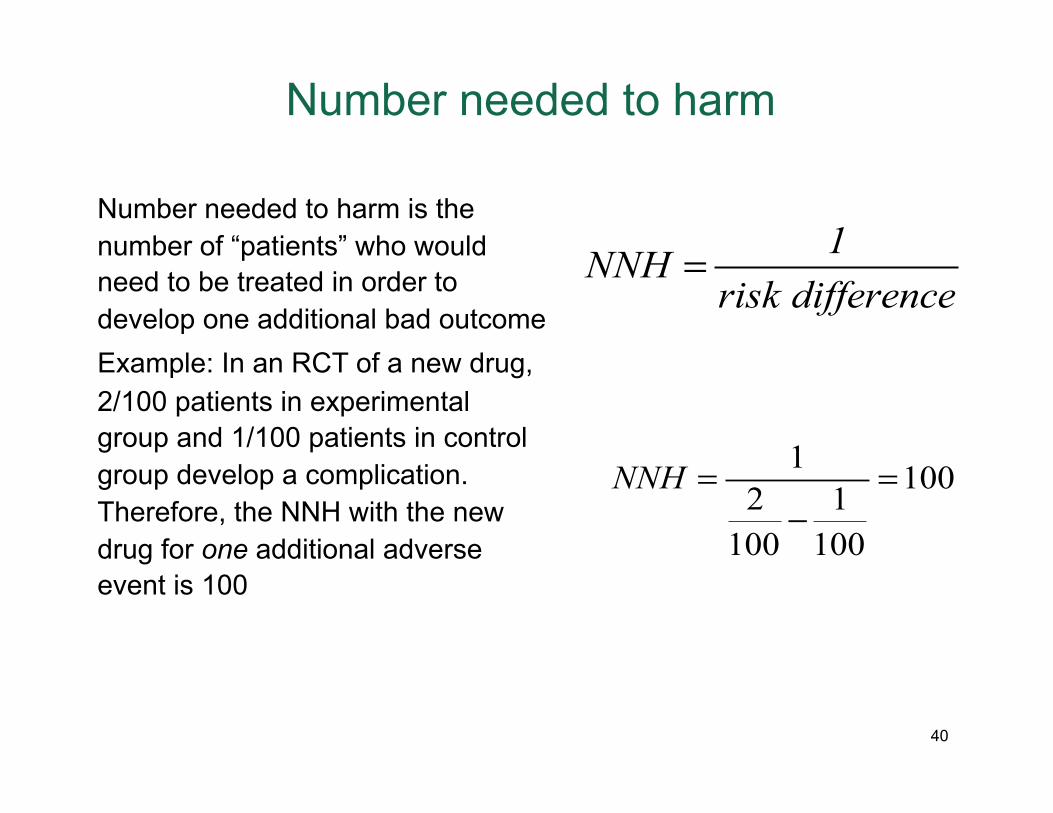
Number needed to harm
Number needed to harm is the number of “patients” who would need to be treated in order to develop one additional bad outcome Example: In an RCT of a new drug, 2/100 patients in experimental group and 1/100 patients in control group develop a complication. Therefore, the NNH with the new drug for one additional adverse event is 100
1NNH risk difference
=
1 1002 1100 100
NNH = =−
40
Other useful concepts
Run-in-period: A period before the actual start of the intervention where no intervention (typically a drug) is given to screen out for ineligibility/noncompliance; sometimes called a “washout” period Contamination: Situation where the experimental (intervention) group influences the control group and there is experimental “contamination”
41


















