Epi 246 Intro to Theories of Health Behavior/ Health Behavior Change Focusing on Individuals’...
36
Epi 246 Intro to Theories of Health Behavior/ Health Behavior Change Focusing on Individuals’ Behavior Margaret Handley, PhD MPH Assistant Professor Dept. Epidemiology and Biostatistics and Center for Vulnerable Populations, DGIM-SFGH April 1, 2010
-
Upload
colleen-gilmore -
Category
Documents
-
view
219 -
download
1
Transcript of Epi 246 Intro to Theories of Health Behavior/ Health Behavior Change Focusing on Individuals’...

Epi 246
Intro to Theories of Health Behavior/ Health Behavior Change Focusing on
Individuals’ Behavior
Margaret Handley, PhD MPHAssistant Professor
Dept. Epidemiology and Biostatistics and
Center for Vulnerable Populations, DGIM-SFGH
April 1, 2010

Outline of Today’s Lecture
1. Course overview and structure
2. Behavioral theory’s role in implementation sciences
3. A few to start:
Health Belief Model Theory of Planned Behavior Trans-theoretical Model-Stages of Change
4. Examples/ Discussion
Implementation & Dissemination Sciences
“Implementation and dissemination sciences is research aimed at enhancing the adoption and appropriate adaptation (e.g. translation) of best evidence-based practices and policies in clinical care and public health; and the development of best evidence through community engagement.”
-UCSF TICR Program in Implementation and Dissemination Sciences

Epi 246 Learning Objectives
1. Using an ecological frame for how behaviors change in society, understand how health behavior theory focused on individuals is critical to implementation and dissemination sciences/ real world application
2. Understand key behavioral theory components with strong evidence for effect and HOW they are used
3. Be able to apply different components to planning, implementing and evaluating health-related behavior and behavior change interventions
4. Understand gaps in different approaches to theory

Which Health Behavior/Behavior Change Theories are Included?
1. Psychological theories with evidence base in health behavior and behavior change
2. Theories that focus on health communication
3. Theories on dissemination of information
4. Theories related to behavioral economics
5. Theories of community building/empowerment
Which Models and Frameworks?
1. Ecological Models
1. Logic models and Intervention Mapping
1. Models with planning and evaluation components
4. Models that integrate across multiple levels

Links between Behavior Theory and Improving Evidence-Based Practice
“Increasing evidence suggests that public
health and health promotion interventions based in social and behavioral sciences are more effective than those lacking a theoretical base” – Glanz and Bishop
“Making research more theory-based will improve evidence-based practice” -Green
Glanz K and Bishop D. Annu Rev Public Health. 31:3990418. 2010Green, L.W. American Journal of Public Health 96(3): 406-409, Mar. 2006.

Learning Objectives – Lecture 1
1. Understand why health behavior change theory is helpful for implementation and dissemination sciences research and real world application
2. Understand components of Health Belief Model, Theory of Planned Behavior and Trans-Theoretical Model, and how they can be integrated into ecological models
3. Be able to apply components of these theories to health-related behaviors – including both understanding behavior and intervention planning/evaluation

Evidence Continuum – Begin with Theory
Eccles, M e al, 2005. J Clin Epi 107-112. Medical Research Council, 2000
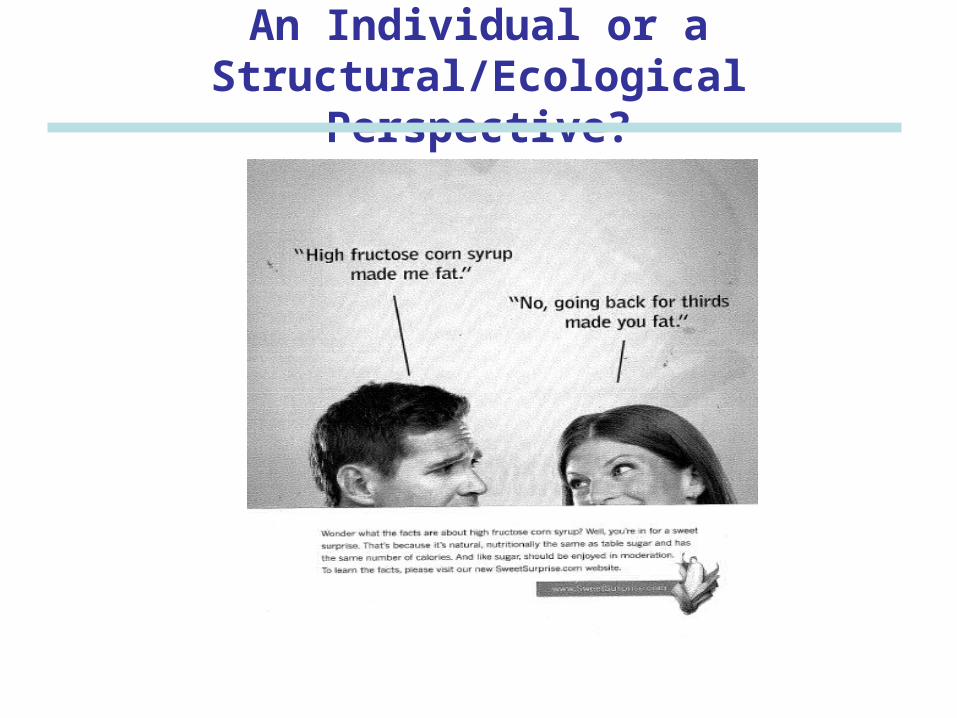
An Individual or a Structural/Ecological Perspective?

A Public Health Ecological Perspective
“The use of collective action to support personal responsibility is central to public health”
Brownell et al, Health Affairs 2010

HOW Individual –Focused Health Behavior Theories Can Be Useful
1. Provide a road map for answering difficult questions on
which behaviors to target and for whom
e.g. Do you target the providers’ behavior re guidelines or focus on structural or policy barriers? Or both?
2. Can understand environmental factors that reinforce or undermine individual behaviors
e.g. Neighborhood ‘walkability’, # of TVs per house
3. Help understand the mechanisms underlying effective interventions – then you can tailor/scale up interventions
NIH Science of Behavior Change, Meeting Summary, June 15-16, 2009

Behavioral Sciences Theory
Theory – a set of inter-related concepts, definitions, and propositions that explain or predict events or situations
(can also specify relationships among these variables)
Behavioral Sciences Theory an amalgamation of approaches, methods, and strategies/tools from social and health sciences that is accessible to both researchers and practitioners
-- Glanz and Bishop, Ann Rev Public Health 2010

Intensity Continuum for Use of Theory
1. Informed by theory – Framework or constructs
identified, but not specifically applied
2. Applied theory - Framework or constructs identified, and
at least one construct specifically applied
3. Testing theory - Framework or constructs identified
and constructs are tested against one another
4. Building/creating theory – Developing new or revised theory using constructs specified, measured, and analyzed in a study
Increasing level of theory in research
Painter, et al, 2008
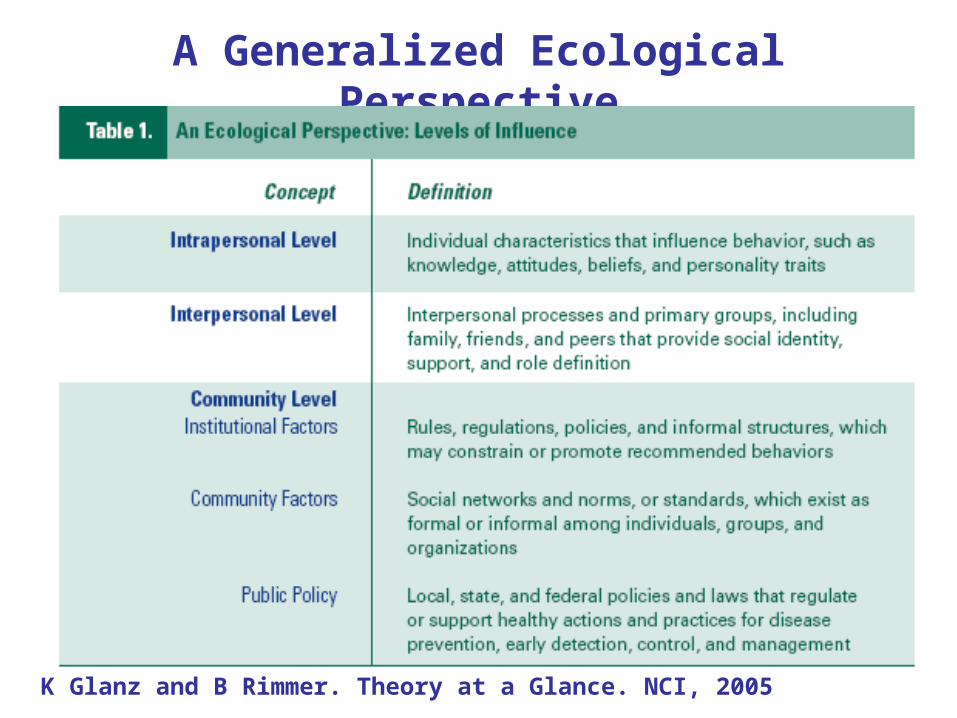
A Generalized Ecological Perspective
K Glanz and B Rimmer. Theory at a Glance. NCI, 2005

Picture from Glanz book

1. Risk appraisal
2. Self perception
3. Emotions
4. Relationships & social influences
5. Environment, community, cultural & structural influences
e.g. SOCIAL NORMS
e.g. SELF-EFFICACY
e.g. PERCEIVED CONSEQUENCES
e.g.FOOD POLICIES, TRANSPORTATION

K Glanz and B Rimmer. Theory at a Glance. NCI, 2005.

Health Belief Model
Focus: Key Concepts
Individuals’ perceptions of the threat posed by a health problem,
The benefits of avoiding the threat, and
factors influencing the decision to act
- Perceived susceptibility
- Perceived severity
- Perceived benefits
- Perceived barriers
- Cues to action
- (Self-efficacy)
Strong Health Beliefs translates into MOTIVATION and ACTION to prevent, screen for or control illness

Action
FOCUS ON INDIVIDUAL BELIEFS THAT AFFECT MOTIVATION
Perceived susceptibility, perceived severity (combined = perceived THREAT) Perceived benefits Perceived barriers Perceived self-efficacy
Motivation
Cues to action
MODIFYING FACTORSAND ENVIRONMENTAge, gender, socioeconomics, Knowledgepersonality
Health Belief Model

Health Belief Model
Example: TB Treatment Adherence
Munro et al, 2007. BMC Public Health; Munro et al, 2007. PlosMedicine

Examples- Using HBMConcept Condom Use Education STI Screen or HIV Testing1. Perceived Susceptibility
Youth believe they can get STIs or HIV or create pregnancy.
Youth believe they may have been exposed to STIs or HIV.
2. Perceived Severity
Youth believe consequences of getting STIs or HIV or creating a pregnancy are significant enough to try to avoid.
Youth believe consequences of having STIs or HIV without knowledge or treatment are significant enough to try to avoid.
3. Perceived Benefits
Youth believe that the recommended action of using condoms would protect them
Youth believe that the recommended action of getting tested for STIs and HIV would benefit them
4. Perceived Barriers
Youth identify their personal barriers to using condoms and explore ways to eliminate or reduce these barriers
Youth identify their personal barriers to getting tested and explore ways to eliminate or reduce these barriers
5. Cues to Action
Reminder cues for action - incentives or reminders
Reminder cues for action -incentives or reminders
6. Self-Efficacy
Youth confident in using a condom correctly in all circumstances
Youth receive guidance or training (such as practice in making an appointment).

Action
APPLICATIONS FOR CHANGING INDIVIDUAL BELIEFS
Perceived THREAT: personalize risk, educate on risk
Perceived benefits: operationalize specific actions and benefits
Perceived barriers: reduce perceptions, problem-solve, incentives
Perceived self-efficacy: support and training, goal setting
INCREASE MOTIVATION
Cues to action: Increase awareness, media/marketing, prompts, reminders
Health Belief Model

Theory of Planned Behavior
Focus: Key Concepts
Individual’s attitude towards a behavior, perceptions of norms, and beliefs about ease of difficulty of changes
Behavioral intention:
- Attitude
- Subjective norm
- Perceived control
and Self-efficacy
Strong Planned Behavior translates into INTENTION to ACT to prevent, screen for or control illness

Action
FOCUS ON BELEIFS THAT AFFECT INTENTION
Beliefs , Evaluation of Behavioral Outcomes (combined=ATTITUDES),
normative beliefs, Motivation (combined=SUBJECTIVE NORM)
Control beliefs, perceived power (self-efficacy)(combined=PERCEIVED CONTROL)
MODIFYINGFACTORS ANDENVIRONMENT
Demographic
Attitudes to target Behavior
Personality
INTENTION
Theory of Planned Behavior

Action
APPLICATIONS TO CHANGE FACTORS THAT AFFECT INTENTION ATTITUDES: Increase exposure to pro-behavior attitudes
SUBJECTIVE: Social marketing to ‘naturalize’ desired behavior NORM
PERCEIVED CONTROL: Identify behaviors within control, then train and guide, goal setting, reinforce, demonstrate skills
INCREASE INTENTION
Theory of Planned Behavior

Theory of Planned BehaviorExample- Factors influencing compliance with
guidelines for induced abortion
Measured behavioral intention, attitudes, subjective norm, perceived behavioral control, open-ended barriers
Perceived behavioral control was low, perceptions that organizational barriers were important
Interventions were recommended to target: Professional control over appointments, staff social
marketing re 5 day window, training staff in family planning, more contraceptive choices available
Foy R et al Intl J Qual in Healthcare 2005

Example- Overall Model to Guide the Study
Process of Care Quality Indicator
Intermediate health outcomes:HA1C, LDL Blood pressure
Retinopathy
Nephropathy
Patient-Important Outcomes
1. Quality of Life
2. Disabilities
3, Actual adverse health events
4. Functional status
5. Goal attainment
6. Utilization
Clinician Factors (Figure 2)
Patient Risk StatusAge, Co-morbidities
Clinical Intervention
Patient Factors(Figure 2)

Example - Application of TPB to Adherence to Screening Recommendations
Attitude toward
adherence Adherence intention
Beliefs that clinician adherence to recommendations will lead to outcomes and the evaluation of such outcomes
Normative beliefs that recommended services should be performed and comply
CLINICIAN:External variables: DemographicsAttitudes towards targetsAttitudes towards patients Subjective
Norm
PATIENT:External variables: DemographicsAttitudes towards targetsAttitudes towards providers
Beliefs that patient adherence to recommendations will lead to outcomes and the evaluation of such outcomes
Normative beliefs that recommended services should be performed and comply
Attitude toward
adherence
Subjective Norm
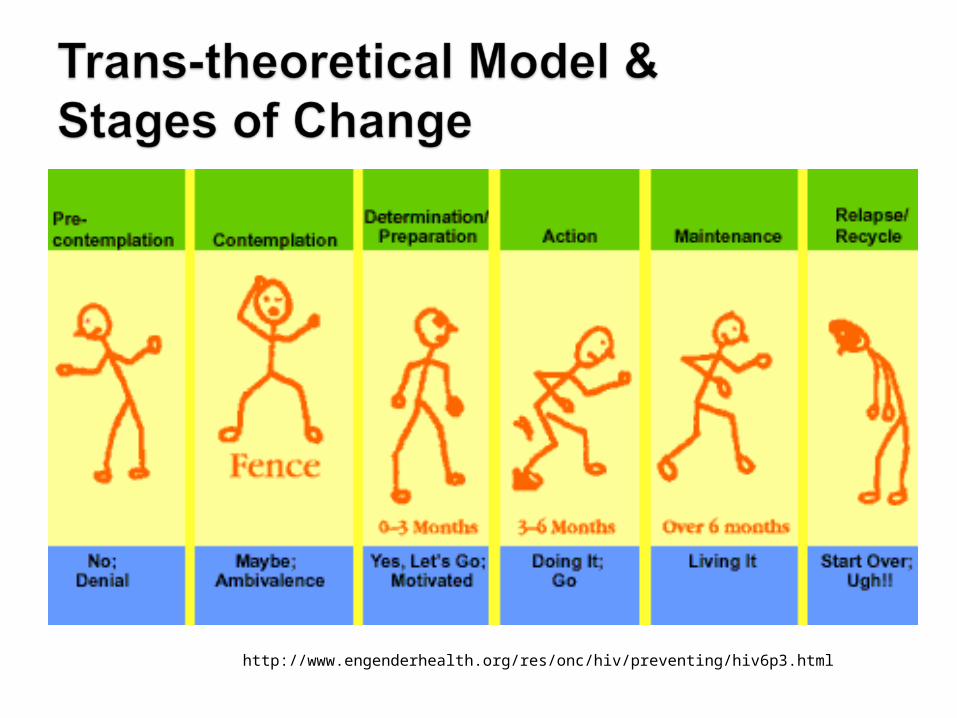
http://www.engenderhealth.org/res/onc/hiv/preventing/hiv6p3.html

Prochaska-Driven Intervention Design
Pre-Contemplation
Preparation
Contemplation
Action
Maintenance
Mass Media, Motivational Interviewing, etc Skill-Building, Social Support, etc.
Intervention Strategies
Education; Feedback CQI; Incentives; Detailing Regulatory; CQI
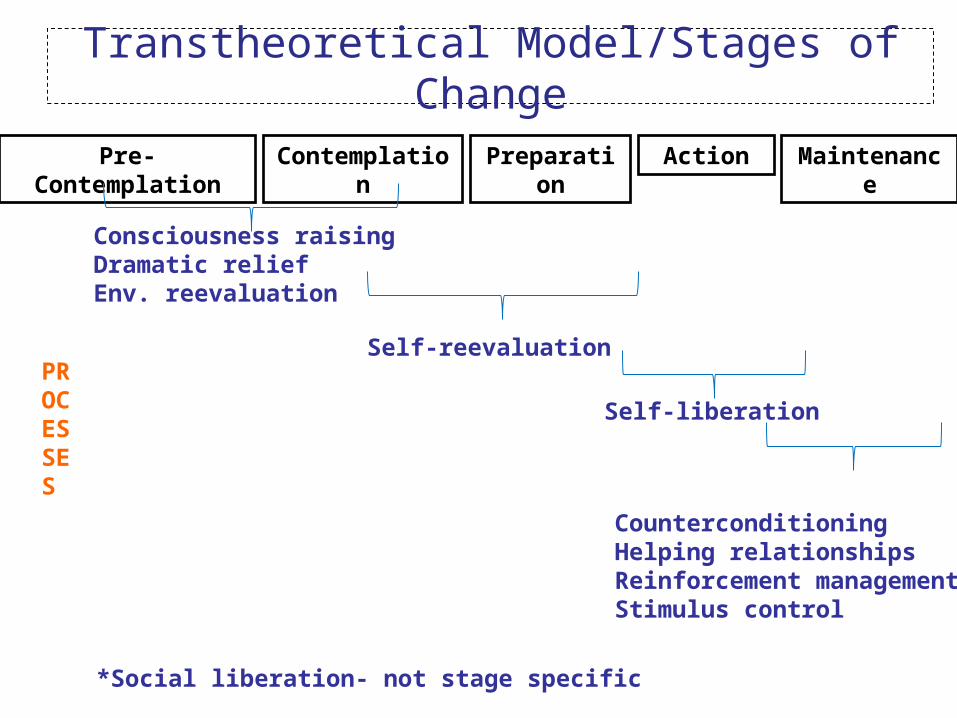
Transtheoretical Model/Stages of Change
Action MaintenanceContemplation PreparationPre- Contemplation
PROCESSES
Consciousness raisingDramatic reliefEnv. reevaluation
Self-reevaluation
Self-liberation
CounterconditioningHelping relationshipsReinforcement managementStimulus control
*Social liberation- not stage specific

Applications to Affect Stage with TTM
Chilvers, R British Journal of Psychiatry, 2002

Example – Testing/Building/Creating a Hybrid Theory for Understanding Mammography Utilization
Testing views about: perceived benefits, susceptibility, self-efficacy, intention and subjective norms among Filipina and Latina women using qualitative interviews and the role of context
Found constructs of: relational culture, social capital, and transnationalism, that then were applied to understanding social norms, self-efficacy, and perceived susceptibility in this population
Augmentation of Behavioral Theories to Take Diversity Into Account
Pasick R, et al. Health Ed and Behavior, 2009

Homework For students applying theory to an active project
For one of the behaviors relevant to your outcome, complete atable or diagram relating variables relevant to your behavior to theories presented in class. Describe which theory they relate to and your rationale for choosing. How can you expand on these individual factors, to include others at multiple levels?
For students not applying theory to an active project
Select a behavior of interest to your work. Which levels do you think have the most significant roles? Who would you engage to develop a formative project to understand more about this behavior and how could you include elements of the theories from class?
Using examples from theories or frameworks presented in class, create a table or diagram to organize related concepts. Which theory do they relate to and how would you measure them?
How am I supposed to think about the consequences before they happen?