ENROLLMENT BOOKLET - Home - Brand New DayBrand …€¦ · · 2017-10-26ENROLLMENT BOOKLET Los...
54
In Control Drug Savings (HMO C-SNP) Plan 26 In Control Choice for Medi-Medi (HMO C-SNP) Plan 27 2018 ENROLLMENT BOOKLET Los Angeles County Orange County Riverside County San Bernardino County Kings County Kern County H0838_EnrKit_Cover_2018.B Approved
Transcript of ENROLLMENT BOOKLET - Home - Brand New DayBrand …€¦ · · 2017-10-26ENROLLMENT BOOKLET Los...

In Control Drug Savings (HMO C-SNP) Plan 26In Control Choice for Medi-Medi (HMO C-SNP) Plan 27
2018 ENROLLMENT BOOKLET
Los Angeles CountyOrange CountyRiverside CountySan Bernardino CountyKings CountyKern County
H0838_EnrKit_Cover_2018.B Approved

HEALTHCARE YOU CAN FEEL GOOD ABOUT.
It’s more than a tagline; it’s what Universal Care, now known as Brand New Day, has made its mission for more than 30 years. We have focused on the importance of helping our members navigate the complex healthcare system with the goal of improving the quality of life for our members and physicians. It starts with our unique approach to help our members address their healthcare needs. The Brand New Day model of care has been designed with a focus on our members, their caregivers, and physicians in supporting each member’s healthcare needs.
Brand New Day offers comprehensive benefit programs designed to address our members’ unique healthcare needs. We offer programs for individuals with Medicare only, Medicare and Medi-Cal, and for individuals with ongoing medical conditions, such as Diabetes, Cardiovascular Disease, Dementia, or Mental Illness. Our focused approach is personalized to help keep our members healthy and independent.
Brand New Day offers a team of caring healthcare professionals whose sole purpose is to improve the overall well-being of each member. The Brand New Day team is empowered to make your experience so good you will agree that you have healthcare you can feel good about.
We invite you to learn more about our health plan and look forward to welcoming you as the newest member of Brand New Day.
Yours in good health,
Jeffrey DavisChief Executive Officer

SCOPE OF SALES APPOINTMENT CONFIRMATION FORM
The Centers for Medicare and Medicaid Services requires agents to document the scope of a marketing appointment prior to any face-to-face sales meeting to ensure understanding of what will be discussed between the agent and the Medicare candidate (or their authorized representative). All information provided on this form is confidential and should be completed by each person with Medicare or his/her authorized representative.
Please initial below in the box beside the plan type that you want the agent to discuss with you.
Medicare Advantage Plans (Part C)
Medicare Health Maintenance Organization (HMO) — A Medicare Advantage Plan that provides all original Medicare Part A and Part B health coverage and sometimes covers Part D prescription drug coverage. In most HMOs, you can only get your care from doctors or hospitals in the plan’s network (except emergencies).
Medicare Special Needs Plan (SNP) — A Medicare Advantage Plan that has a benefit package designed for people with special healthcare needs. Examples of the specific groups served include people who have both Medicare and Medicaid, people who reside in a nursing home, and people who have certain chronic medical conditions.
By signing this form, you agree to a meeting with a sales agent to discuss the types of products you initialed above. Please note, the person who will discuss the products is either employed or contracted by a Medicare plan. They do not work directly for the Federal Government. This individual may also be paid based on your enrollment in a plan.
Signing this form does NOT obligate you to enroll in a plan, affect your current enrollment, or enroll you in a Medicare plan.
Candidate Signature: __________________________________ Date: ____________
If you are the authorized representative, you must sign above and provide the following information:
Authorized Representative Name: _______________________________________________________
Your Relationship to Candidate: _________________________________________________________
To be completed by Agent:
Agent Name: Agent Phone:
Candidate Name: Candidate Phone: (optional)
Candidate Address: (optional)
Initial Method of Contact: (Indicate here if candidate was a walk-in)
Agent Signature: Date Appt. Completed:
Agent, if the form was signed by the candidate at time of appointment, provide explanation why SOA was not documented prior to meeting:
[Plan Use Only:]
H0838_Scope_SOA_2018 Accepted


PLAN 025 – Classic Care Drug Savings (HMO)
3
WHICH PLAN IS RIGHT FOR YOU?
Plan 26 - In Control Drug Savings (HMO C-SNP) PAGE 6This plan is designed for individuals who have Diabetes Type II and Medicare coverage (not Medi-Cal). The benefits will reduce drug costs and will reduce many copayments for Medicare members.
This plan is an excellent choice for anyone who have Diabetes Type II and Medicare coverage and who doesn’t qualify for Medi-Cal or the Brand New Day Special Needs Plans for Dementia or Mental Illness.
Plan 27 - In Control Choice for Medi-Medi (HMO C-SNP) PAGE 14
This plan is designed for individuals who have both Medicare coverage and Medi-Cal coverage. These benefits are designed to maximize the benefits to coordinate Medicare and Medi-Cal to give the member more coverage. There are many services provided at no cost to the member. Remember, some copayments listed in this booklet will be paid for by Medi-Cal.
This plan is an excellent choice for anyone who has both Medi-Cal and Medicare coverage and who doesn’t qualify for the Brand New Day Special Needs Plans for Dementia or Mental Illness.
THERE ARE TWO DIFFERENT HEALTH INSURANCEBENEFIT PLANS INSIDE THIS BOOK.
H0838_SB_26-27_2018.b Accepted

4
Introduction to Summary of Benefits
THINGS TO KNOW:
Brand New Day In Control Drug Savings (HMO C-SNP) Plan 26 and In Control Choice for Medi-Medi (HMO C-SNP) Plan 27 are special programs for individuals who have Diabetes. The program has important elements which help support management of this disease. Some benefits of this extra support are (when medically necessary): • Health Coach • Individualized Care Plan • Glucometer
Hours of operation • From October 1 to February 14, you can call us 7 days a week from 8:00 a.m.
to 8:00 p.m. Pacific time. • From February 15 to September 30 you can call us Monday through Friday from
8:00 a.m. to 8:00 p.m. Pacific Time
Brand New Day In Control Drug Savings (HMO C-SNP) Plan 26 and In Control Choice for Medi-Medi (HMO C-SNP) Plan 27 phone number and website • You can call toll-free 1-866-255-4795 or for TTY users, 1-866-321-5955. • Our website: www.bndhmo.com• If you want to know more about the coverage and costs of Original Medicare, look in your
current “Medicare & You” handbook. View it online at http://medicare.gov or get a copy by calling 1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week. TTY users should call 1-877-486-2048.
Who can join? To join Brand New Day In Control Drug Savings (HMO C-SNP) Plan 26 or In Control Choice for Medi-Medi (HMO C-SNP) Plan 27, you must be entitled to Medicare Part A, be enrolled in Medicare Part B. Brand New Day In Control Drug Savings (HMO C-SNP) Plan 26 and In Control Choice for Medi-Medi (HMO C-SNP) Plan 27 is available to anyone who has been diagnosed with Diabetes. You must also live in our service area: Los Angeles, Orange, Riverside, San Bernardino, Kings and Kern.
In Control Drug Savings (HMO C-SNP) Plan 26In Control Choice for Medi-Medi (HMO C-SNP) Plan 27

PLAN 025 – Classic Care Drug Savings (HMO)
5
Which doctors, hospitals, and pharmacies can I use? Brand New Day In Control Drug Savings (HMO C-SNP) Plan 26 and In Control Choice for Medi-Medi (HMO C-SNP) Plan 27 has a network of doctors, hospitals, pharmacies, and other providers. If you use the providers that are not in our network, the plan may not pay for these services.You must generally use network pharmacies to fill your prescriptions for covered Part D drugs. You can see our plan’s provider and pharmacy directory on our website (www.bndhmo.com).Or, call us and we will send you a copy of the provider and pharmacy directories.
How will I determine My Drug Costs? We cover Part D drugs. In addition, we cover Part B drugs such as chemotherapy and some drugs administered by your provider. • You can see the complete plan formulary (list of Part D prescription drugs) and any
restrictions on our website, www.bndhmo.com. • Or, call us we will send you a copy of the formulary.
Brand New Day Health Plan is an HMO with a Medicare contract and a contract with the California State Medicaid Program. Enrollment in Brand New Day Health Plan depends on contract renewal.

6
IN CONTROL DRUG SAVINGS (HMO C-SNP) -PLAN 26
In Control Drug Savings (HMO C-SNP) -Plan 26
Premiums and Benefits
Brand New Day (HMO) What You Should Know
Monthly Plan Premium You pay nothing In addition, you must keep paying your Medicare Part B premium.
Deductible You pay nothing
Maximum Out-Of-Pocket Responsibility (Does not include prescription drugs)
$3,400 If you reach the limit on out-of-pocket costs, you will continue to have hospital and medical services and the Plan will pay the full cost for the rest of the year.
Inpatient Hospital Care You pay nothing This plan covers 90 days per benefit period for an inpatient hospital stay.This plan also covers 60 “Lifetime Reserve Days.” These are “extra” days that the Plan covers. If your hospital stay is longer than 90 days, you can use these extra days. But once you have used up these extra 60 days, your inpatient hospital coverage will be limited to 90 days.
Doctor’s Office Visits • Primary • Specialist
You pay nothing$5 Copay
Prior authorization is required per specialist visit.
Preventive Care You pay nothing This plan covers many preventive services;Any additional preventive services approved by Medicare during the contract year will be covered.Services require authorization and a referral.

PLAN 025 – Classic Care Drug Savings (HMO)
7
Premiums and Benefits
Brand New Day (HMO) What You Should Know
Emergency CareWorldwide emergency
$100 Copay$100 Copay
If you are admitted to the hospital within 3 days of an ER visit, you do not have to pay your share of cost for emergency care. See the ”Inpatient Hospital Care” section of this booklet for other costs.
Urgent Care You pay nothing
Diagnostic Tests, Lab and Radiology Services, and X-Rays • Diagnostic radiology
services • Lab services • Diagnostic tests
and procedures • Outpatient x-rays
You pay nothing
You pay nothingYou pay nothing
You pay nothing
Costs for these Services be different if received in an outpatient surgery setting.Services require authorization and a referral.
Hearing Services • Hearing Exam • Hearing Aid
You pay nothingHearing aids are not covered.
This plan covers the exam to diagnose and treat hearing and balance issues.Services require authorization and a referral.Hearing aids are not a covered benefit.
Dental Services • Oral Exam • Cleaning • Fluoride treatment • Dental x-rays
You pay nothing$15 - $55 Copay$0 - $12 CopayYou pay nothing
This plan provides enhanced dental coverage.Limitations and exclusions on Services apply.
Vision Services • Exam & Diagnose • Routine eye exam • Eyeglasses (frames and
lenses)
You pay nothingYou pay nothingPlan pays up to $250
This plan covers up to $250 every two years for eyeglasses (frames and lenses).
IN CONTROL DRUG SAVINGS (HMO C-SNP) -PLAN 26
In Control Drug Savings (HMO C-SNP) -Plan 26

8
IN CONTROL DRUG SAVINGS (HMO C-SNP) - PLAN 26
In Control Drug Savings (HMO C-SNP) - Plan 26
Premiums and Benefits
Brand New Day (HMO) What You Should Know
Mental Health • Inpatient Visit
• Outpatient group therapy visit
• Outpatient individual therapy visit
$100 days 1-8 $0 days 9-90You pay nothing
You pay nothing
This plan covers 90 days for an inpatient hospital stay.Plan also covers 60 “Lifetime Reserve Days.” These are “extra” days that the Plan covers. If your hospital stay is longer than 90 days, you can use these extra days. But once you have used up these extra 60 days, your inpatient hospital coverage will be limited to 90 days.Services require authorization and a referral
Skilled Nursing Facility In 2017 the amounts for each benefit period are:You pay nothing for days 1 through 20You pay a $164.50 Copay per day for days 21 through 100These amounts may change in 2018.
This plan covers up to 100 days in a SNF. Services require authorization and a referral.
Rehabilitation Services • Cardiac rehabilitation
services • Occupational
therapy visit • Physical therapy • Speech language
therapy visit
You pay nothing $5 Copay
$5 Copay$5 Copay
Services require authorization and a referral.
Ambulance $125 Copay
Transportation You pay nothing This plan covers unlimited transportation to and from plan approved doctor visits.
Services require authorization and a referral.

PLAN 025 – Classic Care Drug Savings (HMO)
9
Premiums and Benefits
Brand New Day (HMO) What You Should Know
Foot Care (Podiatry Services) • Foot exams and treatment
You pay nothing This plan covers foot exams and treatment if you have diabetes-related nerve damage and/or meet certain conditions.Services require authorization and a referral.
Medical Equipment/Supplies • Durable Medical Equipment
(e.g.; wheelchairs, oxygen) • Prosthetics (e.g; braces,
artificial limbs) • Medical Supplies • Diabetes monitoring
supplies • Telecare meter • Therapeutic shoes or inserts • Diabetes self- management
training
20% of the cost
20% of the cost
You pay nothingYou pay nothing
You pay nothingYou pay nothingYou pay nothing
Services require authorization and a referral.
Wellness Programs • Health club membership • Diabetic Health Coach • Nutrition Couseling • 24 hour nurse advice line • 24 hour doctor advice line • Brand New Day smart
phone application
You pay nothing
Medicare Part B Drugs You pay nothing This plan covers Part B drugs such as chemotherapy and some drugs administered by your provider. Services require prior authorization and a referral.
Acupuncture You pay nothing This plan covers up to 24 visits every year. Subject to medical necessity.
IN CONTROL DRUG SAVINGS (HMO C-SNP) - PLAN 26
In Control Drug Savings (HMO C-SNP) - Plan 26

10
IN CONTROL DRUG SAVINGS (HMO C-SNP) - PLAN 26
In Control Drug Savings (HMO C-SNP) - Plan 26
Premiums and Benefits
Brand New Day (HMO) What You Should Know
Chiropractic Care You pay nothing Manipulation of the spine to correct a subluxation (when 1 or more of the bones of your spine move out of position). Services require prior authorization and a referral.This does not include routine chiropractic care.
Outpatient Surgery • Ambulatory Surgical Center
(ASC) • Outpatient Hospital
You pay nothing
0-20%
Services require prior authorization and a referral.
Over-the-Counter (OTC) $100 allowance This plan covers $100 per quarter for approved OTC items. Instructions about how to obtain this benefit can be found on www.bndhmo.com and in the member handbook.
Renal Dialysis 20% of the cost Services require prior authorization and a referral.
Hospice You pay nothing You pay nothing for hospice care from a Medicare-certified hospice. You may have to pay part of the cost for drugs and respite care.
PLAN 025 – Classic Care Drug Savings (HMO)
11
Premiums and Benefits
Brand New Day (HMO) What You Should Know
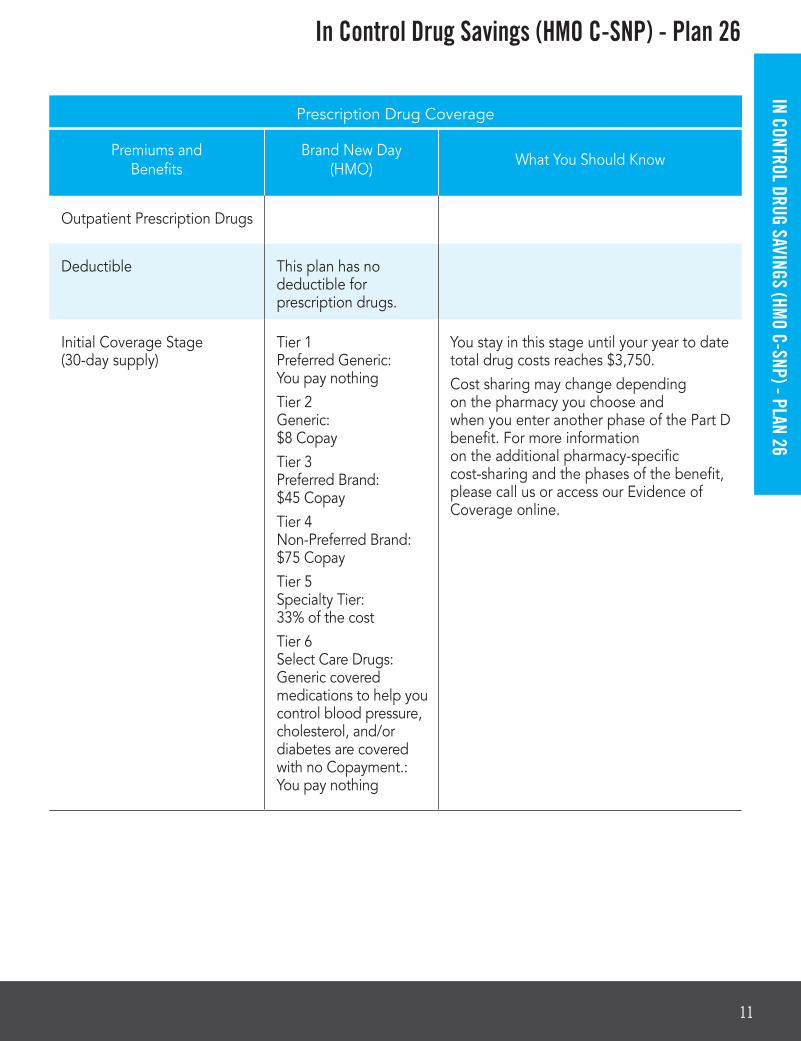
Outpatient Prescription Drugs
Deductible This plan has no deductible for prescription drugs.
Initial Coverage Stage (30-day supply)
Tier 1 Preferred Generic: You pay nothing Tier 2 Generic: $8 CopayTier 3 Preferred Brand: $45 CopayTier 4 Non-Preferred Brand: $75 CopayTier 5 Specialty Tier: 33% of the costTier 6 Select Care Drugs: Generic covered medications to help you control blood pressure, cholesterol, and/or diabetes are covered with no Copayment.: You pay nothing
You stay in this stage until your year to date total drug costs reaches $3,750.Cost sharing may change depending on the pharmacy you choose and when you enter another phase of the Part D benefit. For more information on the additional pharmacy-specific cost-sharing and the phases of the benefit, please call us or access our Evidence of Coverage online.
Prescription Drug Coverage
IN CONTROL DRUG SAVINGS (HMO C-SNP) - PLAN 26
In Control Drug Savings (HMO C-SNP) - Plan 26

12
IN CONTROL DRUG SAVINGS (HMO C-SNP) - PLAN 26
In Control Drug Savings (HMO C-SNP) - Plan 26
Premiums and Benefits
Brand New Day (HMO) What You Should Know
Coverage Gap(30-day supply)
You pay 35% of the plan’s cost for covered brand name drugs and44% of the plan’s cost for covered generic drugs. For Tier 1 covered medications: You pay nothing
Except for Tier 1, most Medicare drug plans have a coverage gap (also called the “donut hole”). This means that there’s a temporary change in what you will pay for your drugs.You stay in this stage until your year-to-date “out-of-pocket costs” (your payments) reach a total of $5,000
Catastrophic Coverage(30-day supply)
You pay whichever amount is the greater of:• 5% of the cost, or• $3.35 Copay for
generic (including brand drugs treated as generic) and $8.35 Copay for all other drugs.
Prescription Drug Coverage

PLAN 025 – Classic Care Drug Savings (HMO)
13
This Summary of Benefits booklet gives you a summary of what the In Control Drug Savings (HMO C-SNP) Plan 26 covers and what you pay.
• If you want to compare this plan with other Medicare health plans, ask the other plans for their Summary of Benefits booklets, or use the Medicare Plan Finder at http://www.medicare.gov.
• If you want to know more about the coverage and costs of Original Medicare, look in your current “Medicare & You” handbook. View it online at http://www.medicare.gov or get a copy by calling 1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week. TTY users should call 1-877-486-2048.
Copays and coinsurance, may vary based on the level of extra help you receive. Please contact Brand New Day for further details.
Medicare beneficiaries may also enroll in Brand New Day In Control Drug Savings (HMO C-SNP) Plan 26 through the CMS Medicare Online Enrollment Center located at http://www.medicare.gov.
This information is available for free in other languages. Please call the Brand New Day customer service number at 1-866-255-4795 or for TTY users, 1-866-321-5955. Customer Service Representatives are available to help you from 8 a.m. to 8 p.m. Monday through Friday and weekends from October 1st through February 14th.
Esta informacion esta disponible gratis en otros idiomas. Por favor llame al departamento de servicio al miembro at 1-866-255-4795 o para usuarios de TTY, 1-866-321-5955. Los representates del servicio al miembro estan disponibles para asistirle de 8:00am a 8:00pm, de Lunes a Viernes y fines de semana de Octubre 1 a Febrero 14.
In Control Drug Savings (HMO C-SNP) - Plan 26
IN CONTROL DRUG SAVINGS (HMO C-SNP) - PLAN 26

14
IN CONTROL CHOICE FOR MEDI-M
EDI (HMO C-SNP) - PLAN 27
In Control Choice for Medi-Medi (HMO C-SNP) - Plan 27
Premiums and Benefits
Brand New Day (HMO) What You Should Know
Monthly Plan Premium $35.50 In addition, you must keep paying your Medicare Part B premium.
Deductible In 2017, the inpatient hospital deductible is $1,316.In 2017, the inpatient hospital psychiatric services deductible is $1,316.These amounts may change in 2018.
Maximum Out-Of-Pocket Responsibility (Does not include prescription drugs)
$6,700 In this plan, you might pay nothing for Medicare-covered services, depending on your level of Medi-Cal eligibility. In this Plan, the amount you can pay out of pocket for services you receive from in-network providers is limited to $6,700. If you reach the limit on out-of-pocket costs, you will continue to have hospital and medical services and the Plan will pay the full cost for the rest of the year.

PLAN 025 – Classic Care Drug Savings (HMO)
15
IN CONTROL CHOICE FOR MEDI-M
EDI (HMO C-SNP) - PLAN 27
In Control Choice for Medi-Medi (HMO C-SNP) - Plan 27
Premiums and Benefits
Brand New Day (HMO) What You Should Know
Inpatient Hospital Care In 2017, the amounts for each benefit period were: $1,316 deductible for days 1-60$329 Copay per day for days 61-90$658 Copay per day for 60 lifetime reserve daysThese amounts may change in 2018.
This plan covers 90 days per benefit period for an inpatient hospital stay.This plan also covers 60 “Lifetime Reserve Days.” These are “extra” days that the Plan covers. If your hospital stay is longer than 90 days, you can use these extra days. But once you have used up these extra 60 days, your inpatient hospital coverage will be limited to 90 days.
Doctor’s Office Visits • Primary • Specialist
$35 Copay$50 Copay
Prior authorization is required for specialist visits.
Preventive Care You pay nothing This plan covers many preventive services. Any additional preventive services approved by Medicare during the contract year will be covered.Services require prior authorization and a referral.

16
Premiums and Benefits
Brand New Day (HMO) What You Should Know
Emergency CareWorldwide emergency
$80 Copay$80 Copay
If you are admitted to the hospital within 3 days of an ER visit, you do not have to pay your share of the emergency care visit. See the “Inpatient Hospital Care” section of this booklet for other costs.
Urgent Care You pay nothing If you are admitted to the hospital within 3 days of an Urgent Care visit, you do not have to pay your share of the cost for urgently needed services.
Diagnostic Tests, Lab, Radiology Services, and X-Rays • Diagnostic radiology
services • Lab services • Diagnostic tests and
procedures • Outpatient x-rays
20% of the cost
You pay nothing20% of the cost
20% of the cost
Costs for these Services be different if received in an outpatient surgery setting.Services require prior authorization and a referral.
Hearing Services • Hearing Exam • Hearing Aid
You pay nothingNot a covered benefit
This plan covers the exam to diagnose and treat hearing and balance issues.Services require prior authorization and a referral.Hearing aids are not a covered benefit.
Dental Services • Oral Exam • X-rays
You pay nothingYou pay nothing
This plan provides enhanced dental coverage.Limitations and exclusions on services may apply.
In Control Choice for Medi-Medi (HMO C-SNP) - Plan 27
IN CONTROL CHOICE FOR MEDI-M
EDI (HMO C-SNP) - PLAN 27

PLAN 025 – Classic Care Drug Savings (HMO)
17
Premiums and Benefits
Brand New Day (HMO) What You Should Know
Vision Services • Routine eye exam • Eyeglasses
(frames and lenses)
You pay nothing This plan pays up to $500 every two years for eyeglasses (frames and lenses)
This plan pays up to $500 every two years for eyeglasses (frames and lenses).
Mental Health • Inpatient Mental Health
• Outpatient Mental Health
In 2017 you pay $1,316 deductible for days 1-60 $329 Copay per day for days 61-90$658 Copay per day for 60 lifetime reserve days These amounts may change in 2018.
Group Therapy: You pay nothing Individual Therapy: You pay nothing
Inpatient visit: Our plan covers up to 190 days in a lifetime for inpatient mental health care in a psychiatric hospital. The inpatient hospital care limit does not apply to inpatient mental services in a general hospital.This plan covers 90 days for an inpatient hospital stay.This plan also covers 60 “lifetime reserve days.” These are “extra” days that we cover. If your hospital stay is longer than 90 days, you can use these extra days. But once you have used up these extra 60 days, your inpatient hospital coverage will be limited to 90 days.The Copays for hospital and skilled nursing facility (SNF) benefits are based on benefit periods. A benefit period begins the day you’re admitted as an inpatient and ends when you haven’t received any inpatient care (or skilled care in a SNF) for 60 days in a row. If you go into a hospital or a SNF after one benefit period has ended, a new benefit period begins. You must pay the inpatient hospital deductible for each benefit period.Services require authorization and a referral.
In Control Choice for Medi-Medi (HMO C-SNP) - Plan 27 IN CONTROL CHOICE FOR M
EDI-MEDI (HM
O C-SNP) - PLAN 27

18
Premiums and Benefits
Brand New Day (HMO) What You Should Know
Skilled Nursing Facility (SNF) In 2017, the amounts for each benefit period were: You pay nothing for days 1-20You pay $164.50 for days 21-100
These amounts may change in 2018.
This plan covers up to 100 days in a SNF. Services require authorization and a referral.
Rehabilitation Services • Cardiac Rehabilitation • Occupational therapy visit • Physical therapy • Speech language therapy visit • Pulmonary Rehab services
20% of the cost$40 Copay$40 Copay$40 Copay
20% of the cost
Services require authorization and a referral.
Ambulance 20% of the cost
Transportation You pay nothing This plan covers unlimited transportation to and from plan approved doctor visits. Services require authorization and a referral.You are entitled to a monthly bus pass at no cost.
Foot Care (Podiatry Services) • Foot exams and
treatment
20% of the cost
This plan covers foot exams and treatment if you have diabetes-related nerve damage and/or meet certain conditions.Services require authorization and a referral.
In Control Choice for Medi-Medi (HMO C-SNP) - Plan 27
IN CONTROL CHOICE FOR MEDI-M
EDI (HMO C-SNP) - PLAN 27

PLAN 025 – Classic Care Drug Savings (HMO)
19
Premiums and Benefits
Brand New Day (HMO) What You Should Know
Medical Equipment/ Supplies • Durable Medical
Equipment(e.g.: wheelchairs, oxygen)
• Prosthetics (e.g.: braces, artificial limbs)
20% of the cost
20% of the cost
Services require authorization and a referral.
Diabetes Supplies & Services • Diabetes Monitoring
supplies • Diabetes
self-management training
• Therapeutic shoes or inserts
You pay nothing
You pay nothing
You pay nothing
Services require authorization and a referral.
Wellness Programs • Health club benefit • Diabetic health coach • Nutrition counseling • 24 hour nurse
advice line • 24 hour doctor
advice line
You pay nothing Services require authorization and a referral.
Medicare Part B Drugs You pay nothing Services require authorization and a referral.
Acupuncture You pay nothing This plan covers up to 24 visits every year. Subject to medical necessity.
In Control Choice for Medi-Medi (HMO C-SNP) - Plan 27 IN CONTROL CHOICE FOR M
EDI-MEDI (HM
O C-SNP) - PLAN 27

20
Premiums and Benefits
Brand New Day (HMO) What You Should Know
Chiropractic Care You pay nothing Manipulation of the spine to correct a subluxation (when 1 or more of the bones of your spine move out of position).Services require authorization and a referral.This does not include routine chiropractic care.
Outpatient Surgery • Ambulatory Surgical
Center (ASC) • Outpatient Hospital
20% of the cost
20% of the cost
Services require authorization and a referral.
Over-the-Counter (OTC) $70 allowance This plan covers $70 per quarter for approved OTC items. Instructions about how to obtain benefit can be found on www.bndhmo.com or in the member handbook.
Renal Dialysis 20% of the cost Services require authorization and a referral.
Hospice You pay nothing You pay nothing for hospice care from a Medicare-certified hospice. You may have to pay part of the cost for drugs and respite care.
In Control Choice for Medi-Medi (HMO C-SNP) - Plan 27
IN CONTROL CHOICE FOR MEDI-M
EDI (HMO C-SNP) - PLAN 27

PLAN 025 – Classic Care Drug Savings (HMO)
21
Prescription Drug Coverage
Premiums and Benefits
Brand New Day (HMO) What You Should Know
Deductible $405 Deductible does not apply to Tier 1 (Preferred generic) and Tier 6 (Select Diabetic Drugs).
Initial Coverage Stage(30-day supply)
Tier 1 Preferred Generic: You pay nothingTier 2 Generic: 25% of costTier 3 Preferred Brand: 25% of costTier 4 Non-Preferred Brand: 25% of costTier 5 Specialty Tier: 25% of costTier 6 Select Care Drugs: Generic covered medications to help you control blood pressure, cholesterol, and/or diabetes are covered with no copayment. You pay nothing
You stay in this stage until your year to date total drug costs reaches $3,750.Cost sharing may change depending on the pharmacy you choose and when you enter another phase of the Part D benefit. To more information on the additional pharmacy-specific cost-sharing and the phases of the benefit, please call us or access our Evidence of Coverage online.
In Control Choice for Medi-Medi (HMO C-SNP) - Plan 27 IN CONTROL CHOICE FOR M
EDI-MEDI (HM
O C-SNP) - PLAN 27

22
Prescription Drug Coverage
Premiums and Benefits
Brand New Day (HMO) What You Should Know
Coverage Gap(30-day supply)
35% of the plan’s cost for covered brand name drugs44% of the plan’s cost for covered generic drugs
Except for Tier 1, most Medicare drug plans have a coverage gap (also called the “donut hole”). This means that there’s a temporary change in what you will pay for your drugs.You stay in this stage until your year-to-date “out-of-pocket costs” (your payments) reach a total of $5,000
Catastrophic Coverage (30-day supply)
You pay whichever amount is the greater of:• 5% of the cost, or• $3.35 Copay for
generic (including brand drugs treated as generic) and a $8.35 copayment for all other drugs
In Control Choice for Medi-Medi (HMO C-SNP) - Plan 27
IN CONTROL CHOICE FOR MEDI-M
EDI (HMO C-SNP) - PLAN 27

PLAN 025 – Classic Care Drug Savings (HMO)
23
In Control Choice for Medi-Medi (HMO C-SNP) - Plan 27This Summary of Benefits booklet gives you a summary of what In Control Choice for Medi-Medi (HMO C-SNP) Plan 27 covers and what you pay. If you want to compare this Plan with other Medicare health plans, ask the other plans for their Summary of Benefits booklets, or use the Medicare Plan Finder at http://www.medicare.gov.
If you want to know more about the coverage and costs of Original Medicare, look in your current “Medicare & You” handbook. View it online at http://www.medicare.gov or get a copy by calling 1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week. TTY users should call 1-877-486-2048.
Copays and coinsurance, may vary based on the level of extra help you receive. Please contact the plan for further details.
Medicare beneficiaries may also enroll in Brand New Day, “In Control Choice for Medi-Medi (HMO C-SNP),” through the CMS Medicare Online Enrollment Center located at http://www.medicare.gov.
This information is available for free in other languages. Please call the Brand New Day customer service number at 1-866-255-4795 or for TTY users, 1-866-321-5955. Customer Service Representatives are available from 8 a.m. to 8 p.m. Monday through Friday and weekends between October 1st and February 14th.
Esta informacion esta disponible gratis en otros idiomas. Por favor llame al departamento de servicio al miembro at 1-866-255-4795 o para usuarios de TTY, 1-866-321-5955. Los representates del servicio al miembro estan disponibles para asistirle de 8:00am a 8:00pm, de Lunes a Viernes y fines de semana de Octubre 1 a Febrero 14.
IN CONTROL CHOICE FOR MEDI-M
EDI (HMO C-SNP) - PLAN 27


PLAN 025 – Classic Care Drug Savings (HMO)
25
ENHANCED BENEFITS BEYOND ORIGINAL MEDICAREBrand New Day offers you enhanced benefits above what Original Medicare alone provides. Brand New Day has partnered with specialized companies for these additional benefits. Brand New Day is pleased to be able to provide our members with added value through these programs.

26
ROUTINE TRANSPORTATION
Brand New Day Transportation
• Schedule Routine Transportation (to and from doctor): 1-855-804-3340 Monday-Friday 8:00 am - 6:00 pm
• Schedule Medical Transportation (non-urgent): 1-855-804-3484 Monday - Friday, 8:00 am - 6:00 pm
• Request a Buss Pass: 1-855-804-3661 Monday - Friday, 8:00 am - 6:00 pm
For TTY users: 1-866-321-5955
DENTAL
DeltaCare USA 1-800-422-4234
• Preventive services • Restorative care• Dentures
ROUTINE OPTOMETRY
MES Vision1-800-877-6372 or 1-714-619-4660Monday - Friday8:00 am - 5:00 pm (PST)
• Exam and Diagnose• Routine eye exam• Eyeglasses (frames and lenses)
FITNESS
Silver&Fit Gym Membership 1-877-427-4788 • www.SilverandFit.com
• No cost gym membership with access to all basic amenities (pool, spa, classes)
• Specialized fitness classes for older adults• Walking groups and social events• Online access to healthy recipes and fitness advice
SPECIALTY HEALTH
American Specialty Health (ASH)1-800-678-9133
• Acupuncture services • Chiropractice services

PLAN 025 – Classic Care Drug Savings (HMO)
27
SPECIALTY HEALTH
1-800-835-2362
• 24/7/365 access to Medical Care• Board Certified Doctors• Access by phone or video • Treatment for many conditions
24-HOUR HELP
NURSE ADVICE LINE1-888-687-7321
• 24 hours a day/7 days a week• Advice and assistance
Additional Enhanced Benefits include: • Brand New Day Care Management Programs • Brand New Day Smart Phone App • Transportation Bus Pass • UCLA Memory Enhancement Group Classes

28
SAVE MONEY ON YOUR PRESCRIPTION DRUGS!
Choice 90
Choice 90 = Lower Copayments!
Tiers 1-4 and 6: Buy two, get one free! If you choose to pick up a 90-day supply of your prescription drugs you will only pay for two months and get the third month free! This applies to prescriptions filled at the pharmacy and mail order.
It is easy to save on prescription drugs with Brand New Day. You can request a 90-day supply from your pharmacy and/or physician and you will pay only one copayment and have one trip to the drug store every three months. You can also request home delivery.
Ask your pharmacy for the “Choice 90” program!
You can tell the pharmacist you want to get your medications with the Choice 90 program. The pharmacist can do the rest. This works for all medications that you take every month. You can drop the program at any time if you decide you don’t like it.
More Savings!
Extra Help - from Medicare
You may qualify for extra help with your prescription drug costs. If you don’t qualify for Medi-Cal but you have a limited income, you can apply for extra help. To apply, call:
• Brand New Day at 1-866-255-4795; TTY users call 1-866-321-5955 and talk to a customer service representative; or call
• Social Security at 1-800-772-1213; TTY users call 1-800-325-0778;
• Or apply online at www.ssa.gov/prescriptionhelp
If you qualify for extra help, Medicare will pay all or part of your Part D premium and you will have lower copayments at the pharmacy.
Other Ways to Save
Generic vs. Brand
Generic medications have the exact same ingredients as the brand name drugs, but you aren’t paying for the “name.” Always ask the pharmacy for generic instead of brand name. Save your money for something special.

1 of 6
To enroll in Brand New Day Health Maintenance Organization (HMO) or Special Needs Plan (SNP), please provide the following information.
TO ENROLL IN BRAND NEW DAY, PLEASE PROVIDE THE FOLLOWING INFORMATION
PROPOSED EFFECTIVE COVERAGE DATE:
IN CONTROL DRUG SAVINGS (HMO C-SNP) PLAN 26 IN CONTROL CHOICE FOR MEDI-MEDI (HMO C-SNP) PLAN 27
Los Angeles, Orange, Riverside, San Bernardino, Kings and Kern Counties $0 per month
Los Angeles, Orange, Riverside, San Bernardino, Kings and Kern Counties $35.50 per month
Please Select a Plan: If you have Medi-Cal with no share of cost and the State pays your premium, the plans with a premium may be your best choice. Please contact Brand New Day if you need information in another language or format (Braille).
H0838_IEF_2018.G_26-27 Approved

INFORMATION ABOUT YOU
2 of 6
INFORMATION ABOUT YOU
CITY
BIRTH DATE (MM/DD/YYYY)
PERMANENT RESIDENCE STREET ADDRESS
CITY
EMERGENCY CONTACT NAME (OPTIONAL)
STATE
STATE
PHONE NUMBER (OPTIONAL)
ZIP
APT # OR SPACE #
APT # OR SPACE #
ZIP
MAILING ADDRESS IF DIFFERENT THAN PERMANENT ADDRESS
EMAIL ADDRESS (OPTIONAL)
RELATIONSHIP TO APPLICANT
MALE FEMALE
LAST NAME
HOME PHONE NUMBER
FIRST NAME
CELL PHONE NUMBER
M.I.
/ /
ENGLISH SPANISH VIETNAMESECHINESE KOREANPREFERRED LANGUAGE FOR WRITTEN MATERIALS
WHITE-NON HISPANIC ASIAN
NATIVE AMERICAN/PACIFIC ISLANDER TWO OR MORE RACES (NOT HISPANIC OR LATINO)
BLACK-NON HISPANICAMERICAN INDIAN/ALASKAN NATIVE
HISPANIC OR LATINORACE/ETHNIC GROUP (OPTIONAL)
MEDICARE HEALTH INSURANCEPlease use your red, white and blue Medicare card to complete this section.
• Fill out this information as it appears on your Medicare card.-OR-
• Attach a copy of your Medicare card or your letter from Social Security or Railroad Retirement Board
Name (as is appears on your Medicare card.)
Medicare Number Is Entitled to Effective DateHOSPITAL (Part A) MEDICAL (Part B)
You must have Medicare Part A and Part B to join a Medicare Advantage plan.
PLEASE PROVIDE YOUR MEDICARE INSURANCE INFORMATION
CA

PLEASE READ AND ANSWER THESE IMPORTANT QUESTIONS

3 of 6
PLEASE READ AND ANSWER THESE IMPORTANT QUESTIONS
1) Are you a resident in a long-term facility, such as a nursing home? (e.g. nursing facility, rest home, rehabilitation hospital, convalescent home, etc.)?2) Are you a resident of a group home, assisted living or Board and Care? If yes, please provide the following information:
Yes
Yes
Yes
Yes
Yes
No
No
No
No
No4) Do you have End-Stage Renal Disease (ESRD)? If you have had a successful kidney transplant and/or you don’t need regular dialysis any more, please attach a note or records from your doctor showing you have had a successful kidney transplant or you don’t need dialysis, otherwise we may need to contact you to obtain additional information.
NAME OF INSTITUTION OR HOME
ADDRESS & PHONE NUMBER OF INSTITUTION (NUMBER AND STREET)
NAME OF CHOSEN PRIMARY CARE PHYSICIAN (PCP, CLINIC OR HEALTH CENTER)
CONTRACTED DENTIST (ONE WILL BE ASSIGNED IF LEFT BLANK)
PCP PROVIDER CODE & IPA#
DENTAL FACILITY #
PLEASE PROVIDE YOUR DOCTOR CHOICE
6) Will you have this medical or prescription drug coverage in addition to Brand New Day? If yes, please list your other coverage and your identification (ID) number(s) for this coverage:
NAME OF OTHER MEDICAL OR DRUG COVERAGE
ID # FOR THIS MEDICAL OR DRUG COVERAGE
GROUP # FOR THIS MEDICAL OR DRUG COVERAGE
5) Do you, on your own or through your spouse, have any other health insurance other than Medicare such as private insurance, TRICARE, Federal Employee Health Benefits Program, Union Plan, workers’ compensation, third party liability, state pharmaceutical assistance program or VA benefits?
Yes No3) Do you have Medi-Cal? If yes, please provide your Medi-Cal number.


4 of 6
I am new to Medicare
I have a diagnosis that qualifies for a Brand New Day Special Needs Plan
I recently moved outside of the service area for my current plan or I recently moved and this plan is a new option for me. I moved on (insert date) __ __/ __ __/ __ __
I have both Medicare and Medicaid (Medi-Cal) or my state helps pay for my Medicare premiums
I have lost my Medicaid (Medi-Cal) coverage
I get extra help paying for Medicare prescription drug coverage
I no longer qualify for extra help paying for my Medicare prescription drugs. I stopped receiving extra help on (insert date) __ __/ __ __/ __ __
I am leaving my employer or union coverage on (insert date) __ __/ __ __/ __ __
I was enrolled in a Special Needs Plan (SNP) but I have lost the special needs qualification required to be in that plan. I was disenrolled from the SNP on (insert date) __ __/ __ __/ __ __
If none of these statements apply to you or you are not sure, please contact Brand New Day at 1-866-255-4795 TDD/TYY users call 1-866-321-5955
Other: Please Explain __________________________________________________________
ATTESTATION OF ELIGIBILITY FOR AN ENROLLMENT PERIOD
EXTRA HELP FOR MEDICATION COVERAGE
People with limited incomes may qualify for extra help to pay for their prescription drug costs. If eligible, Medicare could pay for 75% or more of your drug costs including monthly prescription drug premiums, annual deductibles, and coinsurance. Additionally, those who qualify will not be subject to the coverage gap or a late enrollment penalty. Many people are eligible for these savings and don’t even know it. For more information about this extra help, contact your local Social Security office, or call Social Security at 1-800-772-1213. TYY users should call 1-800-325-0778.
You can also apply for extra help online at www.ssa.gov/prescriptionhelp. If you qualify for extra help with your Medicare prescription drug coverage costs, Medicare will pay all or part of your plan premium. If Medicare pays only a portion of this premium, we will bill you for the amount that Medicare doesn’t cover. If you don’t select a payment option, you will get a coupon book.
You can pay your monthly premium (including any late enrollment penalty that you currently have or may owe) by mail each month. You can also choose to pay your premium by automatic deduction from your Social Security or Railroad Retirement Board (RRB) Benefit check each month. If you are assessed a Part D-Income related monthly adjustment amount, you will be notified by the Social Security Administration. You will be responsible for paying this extra amount in addition to your plan premium. You will either have the amount withheld from your Social Security benefit check or be billed directly by Medicare or the RRB. DO NOT PAY Brand New Day the Part D-IRMAA.
If you currently have health coverage from an employer or union, joining Brand New Day could affect your employer or union health benefits. You could lose your employer or union health coverage if you join Brand New Day. Read the communications your employer or union sends you. If you have questions, visit their website, or contact the office listed in their communications. If there isn’t any information on whom to contact, your benefits administrator or the office that answers questions about your coverage can help.


5 of 6
EXTRA HELP FOR MEDICATION COVERAGE
PLEASE SELECT A PREMIUM PAYMENT OPTION:
Get a Bill
Automatic deduction from your Social Security Railroad Retirement Board (RRB) benefit check. The Social Security/RRB deduction may take two or more months to begin after Social Security or RRB approves the deduction. In most cases, if Social Security or RRB accepts your request for automatic deduction, the first deduction from your Social Security or RRB benefit check will include all premiums due from your enrollment effective date up to the point withholding begins. If Social Security or RRB does not approve your request for automatic deduction, we will send you a paper bill for your monthly premiums.
Get a Coupon Book
By joining this Medicare health plan, I acknowledge that the Medicare health plan will release my information to Medicare and other plans as necessary for treatment, payment and healthcare operations. I also acknowledge that Brand New Day will release my information to Medicare, who may release it for research and other purposes, which follow all applicable Federal statutes and regulations. The information on this enrollment form is correct to the best of my knowledge. I understand that if I intentionally provide false information on this form, I will be disenrolled from the plan. I understand that my signature (or the signature of the person authorized to act on my behalf under the laws of the state where I live) on this application means that I have read and understand the contents of this application. If signed by an authorized individual (as described above), this signature certifies that (1) this person is authorized under state law to complete this enrollment and (2) documentation of this authority is available upon request from Medicare.
PLEASE READ AND SIGN BELOW
If you are the authorized representative, you must sign above and provide the following information:
SIGNATURE
NAME
ADDRESS PHONE NUMBER
RELATIONSHIP TO APPLICANT
TODAY’S DATE
DOCUMENTATION TYPE:
Please submit documentation with enrollment paperwork.
DPOA Legal GuardianDPAHC Written Advance Directive


6 of 6
If anyone helped the individual fill out this form or assisted in enrollment (with the exception of the effective date) she/he must sign the following line:
Please Fax Application with Scope of Appointment to Brand New Day’s Enrollment DepartmentFax Number 1-657-400-1207
Date of Receipt:
Group #:
Notes:
Date E4 Letter Sent:
Name of Staff Member/Agent/Broker (if assisted):
Date E6 Letter Sent: Rep:
Date:
Part D Premium:
Plan: Initials of Verification:
NAME OF STAFF/AGENT/BROKER (print name)
SIGNATURE
RELATIONSHIP TO APPLICANT
DATE
AGENT PHONE NUMBER AGENT LICENSE NUMBER FMO
DATE APPLICATION WAS RECEIVED
SALES AGENT INFORMATION
OFFICE USE ONLY
LISSEP Not EligibleICEP/IEP AEP


POST ENROLLMENT CONTINUITY OF CARE FORMAfter you have completed the enrollment packet, please ask the member the following questions and do the following: 1. Attach completed Post Enrollment document to the enrollment forms 2. Fax to 1-657-400-1207 with completed enrollment packet.
Member Name:_______________________________Phone:__________________Date:_____________
Post Enrollment Questions
1. Are you currently using durable medical equipment or medical devices? Yes No
1a. If “Yes”Please specify which one of the following:
1b. If “Yes”Who is servicing the equipment or medical devices?
Name: ___________________________________Phone :___________________________________Address :__________________________________
2. Are you receiving active care from a medical specialist?
Yes No (If Yes, who?)Name: ___________________________________Phone :___________________________________Address :__________________________________
3. Are you currently receiving home health services?
Yes No (If Yes, who?)Company: _________________________________Phone :____________________________________Address :__________________________________
4. Do you have transportation to and from your appointments?
Yes No If no, Brand New Day will provide transportation. Call 1-866-255-4795.
Additional contact information: caretaker, relative(s) or support person(s)
Name_______________________________________ Phone: _______Relationship: __________
Name_______________________________________ Phone: _______Relationship: __________
Bath Chair Oxygen Cane Pressure mattress Catheters Toilet seats Commode Walker CPAP machine Wheel chair
/Sleep Apnea Diapers Other:_______________ Hospital Bed Other:_______________
H0838_PostEnroll_Cont of Care_2018.B Approved.


PRE-ENROLLMENT QUALIFICATION ASSESSMENT TOOL FOR DIABETES
First Name: MI: Last Name:
Gender: Male Female DOB:
Address:
City: State: Zip:
Is this a licensed nursing home?: Yes No Do you receive SSI or SSDI?: Yes No
MEDICARE Do you have Medicare Part A? Yes No Not Sure Do you have Medicare Part B? Yes No Not Sure (If the answer is “No” to either question, the candidate does not qualify. If not sure, then the candidate’s name will be sent for an eligibility check.)
CLINICAL QUALIFYING QUESTIONS (If any of the following are checked, candidate pre-qualifies) Have you ever been told by a doctor that you have any of the following illnesses? (Check all that apply)
Diabetes Borderline Diabetes High Blood Sugar
MEDICATION QUESTIONS1. Are you now or have you ever taken medication for an illness listed above? Yes No2. Have you ever been on Insulin injections? Yes No 3. Have you ever taken Metformin? Yes No2. What medications are you currently taking? ________________________________________________
______________________________________________________________________________________
PRIMARY PHYSICIAN: _______________________________________________________________________
Name of physician and his/her clinic or location/phone number
SPECIALIST: ________________________________________________________________________ ___ ___
Name of physician and his/her clinic or location/phone number
Candidate Signature: Date:
Agent Signature: Agent Printed Name:
This form must be submitted with the enrollment application for Embrace Care Drug Savings (HMO C-SNP) Plan 35 & In Control Choice for Medi-Medi (HMO C-SNP) Plan 27.


MULTI-LANGUAGE INTERPRETER SERVICESEnglish: We have free interpreter services to answer any questions you may have about our health or drug plan. To get an interpreter, just call us at 1-866-255-4795. Someone who speaks English can help you. This is a free service.
Spanish: Tenemos servicios de intérprete sin costo alguno para responder cualquier pregunta que pueda tener sobre nuestro plan de salud o medicamentos. Para hablar con un intérprete, por favor llame al 1-866-255-4795. Alguien que hable español le podrá ayudar. Este es un servicio gratuito.
Chinese Mandarin: 注意:如果您使用廣東話,我們將免費為您提供語言協助服務。電話
1-866-255-4795(聽障或語障用戶撥打:1-866-255-4795)。
Chinese Cantonese: 您對我們的健康或藥物保險可能存有疑問,為此我們提供免費的翻譯 服務。如需翻譯服務,請致電 1-866-255-4795 。我們講中文的人員將樂意為您提供幫助。 這是一項免費服務。
Tagalog: Mayroon kaming libreng serbisyo sa pagsasaling-wika upang masagot ang anumang mga katanungan ninyo hinggil sa aming planong pangkalusugan o panggamot. Upang makakuha ng tagasaling-wika, tawagan lamang kami sa 1-866-255-4795. Maaari kayong tulungan ng isang nakakapagsalita ng Tagalog. Ito ay libreng serbisyo.
French: Nous proposons des services gratuits d’interprétation pour répondre à toutes vos questions relatives à notre régime de santé ou d’assurance-médicaments. Pour accéder au service d’interprétation, il vous suffit de nous appeler au 1-866-255-4795. Un interlocuteur parlant Français pourra vous aider. Ce service est gratuit.
Vietnamese: Chúng tôi có dịch vụ thông dịch miễn phí để trả lời các câu hỏi về chương sức khỏe và chương trình thuốc men. Nếu quí vị cần thông dịch viên xin gọi 1-866-255-4795 sẽ có nhân viên nói tiếng Việt giúp đỡ quí vị. Đây là dịch vụ miễn phí .
German: Unser kostenloser Dolmetscherservice beantwortet Ihren Fragen zu unserem Gesundheits- und Arzneimittelplan. Unsere Dolmetscher erreichen Sie unter 1-866-255-4795. Man wird Ihnen dort auf Deutsch weiterhelfen. Dieser Service ist kostenlos.
Korean: 당사는 의료 보험 또는 약품 보험에 관한 질문에 답해 드리고자 무료 통역 서비스를 제공하고 있습니다. 통역 서비스를 이용하려면 전화 1-866-255-4795 번으로 문의해 주십시오. 한국어를 하는 담당자가 도와 드릴 것입니다. 이 서비스는 무료로 운영됩니다.
45 H0838_MultiLang_insert Accepted

46
Russian: Если у вас возникнут вопросы относительно страхового или медикаментного плана, вы можете воспользоваться нашими бесплатными услугами переводчиков. Чтобы воспользоваться услугами переводчика, позвоните нам по телефону 1-866-255-4795. Вам окажет помощь сотрудник, который говорит по-pусски. Данная услуга бесплатная.
Arabic: إننا نقدم خدمات المترجم الفوري المجانية لإلجابة عن أي أسئلة تتعلق بالصحة أو جدول األدوية لدينا. للحصول على بمساعدتك. هذه - مترجم فوري، ليس عليك سوى االتصال بنا على 1-866-255-4795. سيقوم شخص ما يتحدث العربية.خدمة مجانية
Italian: È disponibile un servizio di interpretariato gratuito per rispondere a eventuali domande sul nostro piano sanitario e farmaceutico. Per un interprete, contattare il numero 1-866-255- 4795. Un nostro incaricato che parla Italianovi fornirà l’assistenza necessaria. È un servizio gratuito.
Portugués: Dispomos de serviços de interpretação gratuitos para responder a qualquer questão que tenha acerca do nosso plano de saúde ou de medicação. Para obter um intérprete, contacte-nos através do número 1-866-255-4795. Irá encontrar alguém que fale o idioma Português para o ajudar. Este serviço é gratuito.
French Creole: Nou genyen sèvis entèprèt gratis pou reponn tout kesyon ou ta genyen konsènan plan medikal oswa dwòg nou an. Pou jwenn yon entèprèt, jis rele nou nan 1-866- 255-4795. Yon moun ki pale Kreyòl kapab ede w. Sa a se yon sèvis ki gratis.
Polish: Umożliwiamy bezpłatne skorzystanie z usług tłumacza ustnego, który pomoże w uzyskaniu odpowiedzi na temat planu zdrowotnego lub dawkowania leków. Aby skorzystać z pomocy tłumacza znającego język polski, należy zadzwonić pod numer 1-866-255-4795. Ta usługa jest bezpłatna.
Hindi: हमारे स्ासस् ्ा द्ा क ्ोजना के बारे म आपके कसी भी प्न के ज्ाब देने के लए हमारे पास मुफ् दभा ष्ा से्ाएँ उपलब् ह. एक दभा ष्ा पार् करने के लए, बस हम 1-866-255-4795 पर फोन कर. कोई व्यि् जो हनदद बोल्ा है आपक मदद कर सक्ा है. ्ह एक मुफ् से्ा है.
Japanese: 注意:日本語をお話しになる場合は、言語支援サービスを無料でご利用いただけす。
1-866-255-4795 までお電話ください。

47
NOTICE OF NON-DISCRIMINATION
Brand New Day HMO complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex. Brand New Day does not exclude people or treat them differently because of race, color, national origin, age, disability, or sex.Brand New Day provides free aids and services to people with disabilities to communicate effectively with us, such as:
• Qualified sign language interpreters• Written information in other formats (large print, audio,
accessible electronic formats, other formats)
Brand New Day also provides free language services to people whose primary language is not English, such as:
• Qualified interpreters• Information written in other languages
If you need these services, contact the Brand New Day Customer Service Department at 1-866-255-4795 (TTY 1-866-321-5955).Hours are: October 1 – February 14: 7 days a week, 8:00 a.m. – 8:00 p.m. February 15 – September 30: Monday – Friday, 8:00 a.m. – 8:00 p.m.If you believe that Brand New Day has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance by calling our Customer Service Department or mailing a letter to:
Brand New Day Appeals and Grievances DepartmentAttn: Appeals & Grievances Manager5455 Garden Grove Blvd, Suite 500Westminster, California 92683Fax: 1-657-400-1217Email: [email protected]
You can file a grievance in person or by mail, fax, or email. If you need help filing a grievance, our Customer Service Department is available to help you. You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights, electronically through the Office for Civil Rights Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at:
U.S. Department of Health and Human Services200 Independence Avenue, SWRoom 509F, HHH BuildingWashington, D.C. 202011-800-368-1019, 1-800-537-7697 (TDD)Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html
H0838_NOND Accepted

Call toll-free: 1-877-427-4788, TTY 1-877-710-2746 Monday through Friday, 5 am to 6 pm
H0838_EnrKit_AccessBen_2018 Approved
A monthly membership to the Silver&Fit program is part of Brand New Day’s health plans. Designed specifically for older adults, Silver&Fit can help you stay fit by working with you to exercise regularly and meet new people. Or if you prefer, Silver&Fit will help you stay fit from home with their Home Fitness kits!
Benefits include:
• Fitness Facility Program• Home Fitness Program• Resource Library• Fitness Challenges• Silver&Fit Connected!™
• Rewards Program

Benefits include:
• 10 minute median doctor response time • 24/7 assistance anytime, anywhere• 92% of issues resolved after first visit • 95% member satisfaction
Connecting to a doctor within minutes is easy with Teladoc. Request a visit with a doctor 24 hours a day, 365 days a year, by web, phone, or mobile app. Talk to the doctor. Take as much time as you need…there’s no limit! If medically necessary, a prescription will be sent to the pharmacy of your choice. Quality care from quality providers, with the convenience you want!
The Online Doctor can be reached at www.Teladoc.com The Telephone Doctor can be reached by dialing 1-800-Teladoc or 1-800-835-2362 There is no cost to you for telephoning or communicating with a doctor online. They are available for you 24 hours a day, 7 days a week.

50
2017 MEDICARE STAR RATINGS*The Medicare Program rates all health and prescription drug plans each year, based on a plan’s quality and performance. Medicare Star Ratings help you know how good a job our plan is doing. You can use these Star Ratings to compare our plan’s performance to other plans. The two main types of Star Ratings are:1. An Overall Star Rating that combines all of our plan’s scores.2. Summary Star Rating that focuses on our medical or our prescription
drug services.
Some of the areas Medicare reviews for these ratings include: • How our members rate our plan’s services and care; • How well our doctors detect illnesses and keep members healthy; • How well our plan helps our members use recommended and safe prescription
medications.
For 2016, Brand New Day received the following Overall Star Rating from Medicare.
3 Stars
We received the following Summary Star Rating for Brand New Day’s health/drug plan services:
Health Plan Services: 3 Stars
Drug Plan Services: 3 Stars
The number of stars show how well our plan performs
5 Stars – Excellent 4 Stars –Above Average 3 Stars –Average 2 Stars –Below Average 1 Star –Poor
Learn more about our plan and how we are different from other plans at www.medicare.gov. You may also contact us 7 days a week from 8:00 a.m. to 8:00 p.m. Pacific time at 1-866-255-4795 (toll-free) or 1-866-321-5955 (TTY), from October 15 to December 7. Our hours of operation for the rest of the year are Monday through Friday from 8:00 a.m. to 8:00 p.m. Pacific time.
Current members please call 1-866-255-4795 (toll-free) or 1-866-321-5955 (TTY).*Star Ratings are based on 5 Stars. Star Ratings are assessed each year and may change from one year to the next.
H0838_StarRating_2018.A Accepted

51
WHAT TO EXPECT NEXT?
You’ve submitted your Brand New Day Enrollment Form -- so now what happens?
Enrollment Forms Received Your enrollment is sent to Brand New Day by phone, mail, fax, agent, or via the internet. We will begin processing your application immediately.
Letter of Approval Within 10 days of enrollment, you will receive a letter that will confirm your enrollment with Brand New Day has been approved by Medicare.
Your Brand New Day Member ID Card You will receive your Brand New Day Member ID in the mail. Make sure to place this card somewhere handy! You will need it when you visit your doctor, pharmacy, or hospital.
Welcome Packet You will receive a package containing important plan documents, it will include the Evidence of Coverage and Drug Formulary.
Dental CardYou will receive a separate dental card to show at your dentist’s office.
Help with Medicare Costs If you qualify for the state’s “Extra Help”, you will receive a “LIS” (Low Income Subsidy) letter within 10 days of verified enrollment.
We look forward to welcoming you to Brand New Day!If you have any questions please call our Customer Service department at 1-866-255-4795.
H0838_EnrKit_BackCover_2018.A Approved

1-866-255-4795TTY 1-866-321-5955
www.bndhmo.com