Enhanced Monitoring of HIV/AIDS in South Asia
17
Enhanced Monitoring of HIV/AIDS in South Asia International Studies of HIV/AIDS (ISHA) Research Group: Paul Arora, Rajesh Kumar, Prabhat Jha, Neeraj Dhingra, Prem Mony, Prakash Bhatia, Peggy Millson, Li Chen, Madhulekha Bhattacharya, Robert Remis, Sema Sgaier, PV Lakshmi, Nico Nagelkerke, Mariam Claeson Centre for Global Health Research, St. Michael’s Hospital, University of Toronto, Canada [email protected]
description
Enhanced Monitoring of HIV/AIDS in South Asia. International Studies of HIV/AIDS (ISHA) Research Group: - PowerPoint PPT Presentation
Transcript of Enhanced Monitoring of HIV/AIDS in South Asia

Enhanced Monitoring of HIV/AIDS in South AsiaInternational Studies of HIV/AIDS (ISHA)
Research Group: Paul Arora, Rajesh Kumar, Prabhat Jha, Neeraj
Dhingra, Prem Mony, Prakash Bhatia, Peggy Millson, Li Chen, Madhulekha Bhattacharya, Robert
Remis, Sema Sgaier, PV Lakshmi, Nico Nagelkerke, Mariam Claeson
Centre for Global Health Research, St. Michael’s Hospital, University of Toronto, Canada

www.cghr.org
Summary1. Enhanced independent monitoring focusing on
programs (vs projects) that is simple, routine, reliable, low-cost, long-term is needed to evaluate the success of HIV/AIDS control programs (including of “universal access”).
2. Key pillars include: (a) understanding sexual networks, esp. of males; (b) enhanced ANC and STI surveillance; (d) mortality measurement; (d) transparent modelling; and (e) capacity building in countries.
3. A multi-country effort to implement these pillars is urgently needed, and would be a low-cost, high-impact activity.
Source: Authors, 2006

www.cghr.org Source: Kumar et al, Lancet 367 (2006)

www.cghr.org
FEMALES-Summary ORs of all risk factors Meta-analyses of 79 epidemiological studies in Africa
Summary OR
.1 1 2 3 4 5 10
Sexual Risk Factor
Summary OR
(95% CI)
CSW 2.36 ( 1.60, 3.48)
No. sex partners 2+ 3.64 ( 2.87, 4.62)
No. sex partners 0-2 0.27 ( 0.22, 0.35)
HSV-2 sero-positive 4.00 ( 2.89, 5.55)
STI 2.16 ( 1.78, 2.63)
Source: Chen et al, forthcoming

www.cghr.org
Summary OR
.1 1 2 3 4 5 10
Sexual Risk Factor
Summary OR
(95% CI)
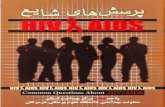
Male client 1.91 ( 1.52, 2.41)
No. sex partners 2+ 2.40 ( 1.86, 3.09)
No. sex partners 0-2 0.29 ( 0.22, 0.37)
HSV-2 sero-positive 5.61 ( 3.42, 9.21)
STI 2.87 ( 2.04, 4.03)
Uncircumcised 2.47 ( 1.81, 3.36)
MALES- Summary ORs of all risk factors: Meta-analyses of 79 epidemiological studies in Africa
Source: Chen et al, forthcoming

www.cghr.org Source: Chen et al, forthcoming

www.cghr.org
Regions of analysis<0/5%
0.5% to <1%
1% to <1.5%
>=1.5%
• Maximum state-level HIV-1 seroprevalence among ANC attendees from1998 to 2003
• Two regions of analysis :
1) South2) North and other
Source: Kumar et al, Lancet 367 (2006)

www.cghr.org Source: Kumar et al, Lancet 367 (2006)

www.cghr.org
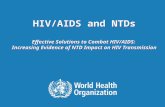
Figure 5: Age-standardised HIV-1 prevalence in men aged 20–29 years attending STI clinics in 2000–04, and in those with genital ulcers in the south and north of India HIV-positive/tested=number of HIV-positive individuals/number of individuals tested. Boxes and lines are prevalence and 95% CI.
YearSouth
No. of sites 20 28 38 38 41 20 28 38 38 41HIV+/tested 244/1 132 220/1 253 278/2 068 269/1 983 304/2 198 130/592 108/582 122/885 118/856 180/1 192
Diff '00 vs '04 z=5.39, p<0.01 z=3.46, p<0.01North
No. of sites 44 73 84 88 91 44 73 84 88 91 HIV+/tested 56/2 013 90/3 209 118/3 978 152/4 440 108/4 577 40/1 047 53/1 490 57/1 686 75/1 989 54/1 984
Diff '00 vs '04 z=0.94, p=0.34 z=1.59, p=0.11
Age 20 to 29 years
13.312.9
20.9
12.8
16.6
2.7 2.82.3
3.42.9
0.0
5.0
10.0
15.0
20.0
25.0
2000 2001 2002 2003 2004
Ag
e st
and
ard
ized
HIV
-1 p
reva
len
ce (
%)
North
p trend= <0.0001
p trend=0.59
Age 20 to 29 years with ulcer
14.413.2
21.2
13.1
17.5
3.8 3.5
2.7
3.73.3
0.0
5.0
10.0
15.0
20.0
25.0
2000 2001 2002 2003 2004
North
p trend= 0.0008
p trend=0.13
SouthSouth
Source: Kumar et al, Lancet 367 (2006)

www.cghr.org

www.cghr.org
Sum: 1/3 decline in South: 1. Not due to major changes in women who go to
pregnancy clinics2. Not due to changes in sites chosen3. Not due to mortality4. Only changes in husband’s use of female sex work
(less often or with condoms when done) is only plausible explanation
5. Consistent with increased peer intervention programs to reach sex workers starting about 1999
6. Gaps exist in South however: esp. Karnataka and Andhra Pradesh
7. Goal: 100% coverage in each of 115 districts
Source: Kumar, Jha, Arora et al; 2006

www.cghr.org
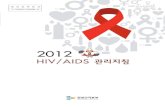
TRENDS IN GONORRHEA
Source: Murphy, G. et. al. AIDS 2004, 18:
United Kingdom: AIDS treatment, deaths and STI trends among males having
sex with males
% MSM ON ARV
AIDS DEATHS

www.cghr.org
Proportion of urban TB to total deaths by high HIV state (AP, KN, MH, TN) and other
states, 1990-2000
Source: Jha et al, forthcoming

www.cghr.org
AIDS mortality in IndiaPreliminary results of the RGI-CGHR Million Death Study
(n=150,000 deaths 2001-3, 22,000 analyzed here)(All cause deaths at ages 15-59 total 3,772,000)
% of all deaths at ages 15-59
Number
WHO indirect estimate (2002) 6.2% 233
RGI-CGHR preliminary direct estimates (2002-3)
AIDS only 1.0% 36
AIDS+ lymphomas+ fevers 2.3% 88
AIDS + lymphomas + fevers + all tuberculosis in South
4.6% 175
Source: Jha et al, forthcoming

www.cghr.org
HIV-1 prevalence (adults aged 15-59) projections in India: past and current estimates
Source: Jha et al, forthcoming

www.cghr.org Source: Jha et al, forthcoming

www.cghr.org
Summary1. Enhanced independent monitoring focusing on
programs (vs. projects) that is simple, routine, reliable, low-cost, long-term is needed to evaluate the success of HIV/AIDS control programs (including of “universal access”).
2. Key pillars include: (a) understanding sexual networks, esp. of males; (b) enhanced ANC and STI surveillance; (d) mortality measurement; (d) transparent modelling; and (e) capacity building in countries.
3. A multi-country effort to implement these pillars is urgently needed, and would be a low-cost, high-impact activity.
Source: Authors, 2006