Endothelial progenitor cells: Cellular biomarkers in vascular disease
5
Click here to load reader
-
Upload
mihail-hristov -
Category
Documents
-
view
216 -
download
0
Transcript of Endothelial progenitor cells: Cellular biomarkers in vascular disease

MECHANISMS
DRUG DISCOVERY
TODAY
DISEASE
Endothelial progenitor cells: Cellularbiomarkers in vascular diseaseMihail Hristov1,2,*, Christian Weber1
1Institut fur Molekulare Herz-Kreislaufforschung (IMCAR), Universitatsklinikum der RWTH Aachen, Pauwelsstr. 30, 52074 Aachen, Germany2IZKF ‘‘BIOMAT’’, Universitatsklinikum der RWTH Aachen, Pauwelsstr. 30, 52074 Aachen, Germany
Drug Discovery Today: Disease Mechanisms Vol. 5, No. 3–4 2008
Editors-in-Chief
Toren Finkel – National Heart, Lung and Blood Institute, National Institutes of Health, USA
Charles Lowenstein – The John Hopkins School of Medicine, Baltimore, USA
Cardiology
Recently, the research on adult endothelial progenitor
cells (EPCs) in peripheral blood raised great interest.
EPCs were significantly involved in endothelial regen-
eration after arterial injury and in neovascularisation of
ischemic tissue. Moreover, EPC counts might correlate
with clinical outcomes in patients with heart disease or
cancer. This mini-review intends to discuss the validity
of some circulating EPC subsets as surrogate prognos-
tic/diagnostic cellular biomarkers for monitoring vas-
cular homeostasis in atherosclerosis and cancer.
Introduction
Along leukocyte recruitment, lipid accumulation, chronic
inflammation and immune cues, a crucial involvement of
vascular progenitor cells in the pathogenesis of atherosclero-
sis has been newly emerged [1–3]. For instance, endothelial
progenitor cells (EPCs) were identified in adults and these
cells have been shown to play an essential role in arterial
remodelling [4,5]. Adult EPCs were intensively investigated
within the past decade by several groups and numerous
published data revealed their contribution in the pathogen-
esis of transplant arteriosclerosis, neovascularisation of
ischemic tissue and regeneration of the arterial wall after
injury [3–5]. Along atherosclerotic disease EPCs were also
involved in other pathological conditions such as cancer,
diabetes and renal failure, thus highlighting broadly based
and multidisciplinary research on EPC biology within the
medical community [3,6]. Moreover, EPCs have recently
*Corresponding author: M. Hristov ([email protected])
1740-6765/$ � 2008 Elsevier Ltd. All rights reserved. DOI: 10.1016/j.ddmec.2008.07.001
Section Editor:Christian Weber – Institute for Molecular CardiovascularResearch (IMCAR), RWTH, Aachen University, Germany
generated great attention as potential novel diagnostic/prog-
nostic biomarkers for vascular integrity and therapeutic clin-
ical approaches using these cells are on the way.
Origin and characterization of circulating adult EPCs
During the embryonic development primitive capillary net-
works were formed by angioblasts, a process known as vas-
culogenesis [7]. Some of these primordial vascular structures
gradually sprout and become stabilised by peri-endothelial
matrix, smooth muscle cells and pericytes, thus transforming
into pressure resistant contracting arteries, a process defined
as arteriogenesis [7]. Parallel to these mechanisms, a common
precursor cell positive for the vascular endothelial growth
factor receptor-2 (VEGFR2) exists, which can give rise to both,
endothelial and smooth muscle lineage during vessel devel-
opment in the embryo [8]. Of note, the above mechanisms
still persist in adults since several recent studies have
described adult vascular progenitor cell subtypes correspond-
ing to embryonic stem cell progeny. These vascular precur-
sors have the ability to promote postnatal vasculogenesis and
neovascularisation of ischemic tissue by assuming for
instance endothelial phenotype and by paracrine delivery
of angiogenic compounds [3–5,9].
As the adult progenitor cell most widely studied, the
putative EPC can be localised in bone marrow and peripheral
blood or reside on ‘stand-by’ within the vascular wall [3–
5,10]. Despite comprehensive amount of published results,
an exact definition of the EPC remains rather controversial
e267

Drug Discovery Today: Disease Mechanisms | Cardiology Vol. 5, No. 3–4 2008
and inconsistent, based in part on the plasticity of distinct
adult haematopoietic or mesenchymal cell subpopulations
(e.g. CD34+/�, CD14+) in acquiring the endothelial pheno-
type [11,12]. Nevertheless, standard lineage marker combi-
nations commonly established and largely used for
identifying functional circulating EPCs comprise CD133/
CD34/VEGFR2 or CD34/VEGFR2 [3–5]. Some groups have
additionally identified even ‘late’ circulating EPCs with a
CD34+CD144+ phenotype [13,14]. These cells were mainly
located within the CD3� lymphocyte subpopulation [14].
Recent data advocate to include also circulating CD14+
myeloid cell subtypes (e.g. CD14+CD34low, CD14lowCD16+
Tie-2+, CD14+VEGFR2+CXCR2+/�) which were characterized
as functional endothelial-like cells with significant contri-
bution to endothelial regeneration, ischemic or tumour
angiogenesis [15–17]. Thus, the heterogeneous pool of adult
EPCs includes subsets of multiple origin, phenotype and
differentiation stage, which commonly share expression of
progenitor, myeloid and endothelial differentiation mar-
kers (e.g. CD133, CD34, VEGFR2, CD14, CD31, CD144, Tie-
2, von Willebrand factor) together with clonogenic capa-
city, generation of endothelial outgrowth and formation of
vascular network.
Contribution of EPC subsets in arterial remodelling
and tumour angiogenesis
Studies in animal models have revealed that infused or endo-
genously mobilised EPCs effectively contributed to endothe-
lial regeneration and reduction of neointimal formation after
arterial injury [17–19]. EPCs have also been shown to partially
regenerate damaged endothelial cells in atherosclerosis-
prone ApoE�/� mice and a large percentage of renewed
endothelial cells in vascular grafts originated from circulating
progenitors [20,21]. Translating this knowledge to the clinics
has introduced the application of in vitro expanded autolo-
gous angiogenic mononuclear cells as a cell-based additive
therapy for acute or chronic myocardial ischemia [22]. How-
ever, the outcome on recovery of heart function remains
altogether moderate and controversial as this has been also
revealed during intracoronary application of bone marrow
mononuclear cells after acute myocardial infarction [22].
These modest effects in left ventricular functional recovery
very probably associated with improved neovascularisation
and paracrine action, but not with transdifferentiation of
infused cells into cardiomyocytes [3,22,23]. Current clinical
concepts further claim a protective role of EPCs in athero-
sclerotic disease. Reduced numbers of CD34+VEGFR2+ EPCs
and impaired clonogenic capacity have been shown to cor-
relate with the Framingham risk factor score and to predict
cardiovascular events [24]. By contrast, some trials revealed
that EPC numbers were unaffected by cardiovascular risk
factors but rather associated with the severity of stenotic
coronary artery disease (CAD) [25–27]. These results may also
e268 www.drugdiscoverytoday.com
be ascribed to ischemia occurring in severe CAD or reflect the
delicate equilibrium between EPC mobilisation and periph-
eral demand. The different diagnostic/therapeutic effects of
EPCs may also be related to the distinct cell models used. For
instance, only the fraction of CD34+ cells has been shown to
independently predict functional improvement at follow-up
after acute myocardial infarction [28]. However, many of the
clinical studies above have therapeutically used the entire
mononuclear cell fraction including also neutrophils and
inflammatory monocytes, thus inducing secondary leukocy-
tosis. Such an elevation in leukocyte counts has been still
demonstrated to associate per se with incidence of CAD [29].
Furthermore, published data from animal trials have shown
that infusion of EPCs increased plaque size and decreased
plaque stability in ApoE�/� mice [30]. This observation could
be explained in part by pro-angiogenic and proteolytic prop-
erties of EPCs. Influx of EPCs may also be involved in cancer
progression due to increased tumour vascularisation and
assessment of circulating EPCs might adequately support
the monitoring of anti-angiogenic therapy [6]. This knowl-
edge introduced EPCs as potential targets for manipulating
tumour growth and metastasis. Conversely, other data
showed that bone marrow-derived EPCs failed to maintain
tumour vascular endothelium [31]. Nevertheless, the level of
EPC contribution to cancer vessels might depend on tumour
type, grade and localisation [6]. For instance, evidence from
research on multiple myeloma has shown that circulating
EPCs are related to the neoplastic clone and this represent one
potential mechanism for up-regulation of tumour neovascu-
larisation [32]. Very recent data have further identified selec-
tive accumulation of pro-angiogenic CD14lowCD16+Tie-2+
monocyte subsets within the neoplastic tissue and their
contribution in promoting tumour angiogenesis and cancer
growth, respectively [15]. This specific, even resident mono-
cyte subpopulation differ from the classical CD14high inflam-
matory monocytes and parallel to elevated expression of Tie-
2 also demonstrate higher levels of the chemokine receptors
CXCR4 and CCR5 [15,33].
Accordingly, the ambiguous contribution of circulating
CD34+VEGFR2+ EPCs and myeloid CD14low/+ angiogenic cells
to vascular remodelling during arterial injury, advanced
atherosclerosis and cancer disease requires a meticulous re-
evaluation.
Effect of various conditions, cytokines and
pharmacological compounds on the number of EPCs
Published data from animal studies and clinical trials have
reported effects of some conditions, cytokines and therapeu-
tics on the number of EPCs (Fig. 1). For instance, ischemia and
exercise training associated with mobilisation and improved
homing of EPCs in patients with peripheral arterial occlusion
[34]. Furthermore, VEGF, erythropoietin and granulocyte
colony-stimulating factor have been shown to mobilise EPCs

Vol. 5, No. 3–4 2008 Drug Discovery Today: Disease Mechanisms | Cardiology
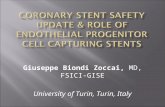
Figure 1. Circulating putative progenitors for endothelial cells as fundamental players in vascular homeostasis. The heterogeneous pool of adult
endothelial progenitor cells in peripheral blood includes subsets of multiple origin, phenotype and differentiation stage, which commonly share expression
of progenitor (CD133, CD34), myeloid (CD14) and endothelial (VEGFR2, CD144, Tie-2) differentiation markers. These cells obviously participate in
endothelial repair and angiogenesis, and their number is differentially affected by several conditions, cytokines and therapeutic compounds. A routine
quantification of circulating endothelial progenitor cells by using multi-parametric flow cytometry analysis of peripheral blood may strengthen their
significance as novel cellular biomarkers for monitoring drug activity and endothelial maintenance during atherosclerosis and cancer disease. ACE,
angiotensin-converting enzyme; G-CSF, granulocyte colony-stimulating factor; VEGF(R), vascular endothelial growth factor (receptor).
[3]. Therapeutically, the HMG-CoA reductase inhibitors
(statins) induce a transient mobilisation of circulating
CD34+VEGFR2+ EPCs and stimulate their neo-endothelial
incorporation which may also assist in preventing neointimal
hyperplasia [3,18]. Interestingly, long-term treatment with
statins dose-dependently decreased the number of circulating
CD34+VEGFR2+ EPCs but increased the number of the even
more mature CD34+CD144+ EPCs in peripheral blood of
patients with CAD [13,27]. Further data have revealed a rise
in circulating EPCs after application of peroxisome prolifera-
tor-activated receptor-gamma agonists (thiazolidinediones)
or the angiotensin-converting enzyme inhibitor enalapril
[35,36]. Conversely, the number of circulating EPCs has been
reduced after treatment with bevacizumab (a specific mono-
clonal antibody against VEGF) in cancer patients [37]. Simi-
larly, application of small molecule VEGFR2-antagonist was
reported to inhibit the mobilisation of EPCs in mice [6].
EPCs: cellular biomarkers in vascular disease
From the diagnostic/prognostic clinical point of view quan-
tification and functional assessment of circulating EPCs have
been reported to reflect endothelial complexity and main-
tenance [3,6,24]. Thus, such a procedure could be routinely
introduced as an alternative predictive and/or diagnostic
biomarker of several vascular disorders (e.g. acute coronary
syndrome, restenosis, transplant vasculopathy, diabetic
angiopathy, etc.) but also in cancer [6,37,38]. To date, direct
ex vivo flow cytometry from anti-coagulated peripheral blood
and in vitro enumeration of colony forming units (CFUs; a
marker for clonal expansion capacity) are the most com-
monly used methods for evaluation of adult EPCs [3,38].
Flow cytometry from freshly drawn peripheral venous
blood offers the advantage of high sensitive and reproducible
multi-parameter approach allowing direct quantification of
the target population. This is a quickly done and minimally
invasive procedure which requires very small blood volume
parallel to convenient laboratory equipment, expenses and
efforts. However, a general agreement for enumeration of
circulating EPCs is still absent. This may in part explain some
controversial results in published clinical trials [24–27]. Basi-
cally, the direct quantification of circulating CD34+ haema-
topoietic progenitor subsets by flow cytometry is well
established in haematology and haematooncology. Of note,
analysis of CD34+ cells in peripheral blood may also reflect
endogenous vascular homeostasis and endothelial regenera-
tive potential. For example, an increase in circulating CD34+
cells after coronary stent implantation independently pre-
dicted in-stent stenosis and may be suggestive for the invol-
vement of CD34+ subpopulations in the pathogenesis of
neointimal hyperplasia [39]. Other clinical trials revealed a
significant increase of circulating CD34+ cells in patients with
acute myocardial infarction and a biphasic response during
the early and advanced phases of chronic heart failure,
respectively [3]. Despite variations in the methodology for
www.drugdiscoverytoday.com e269

Drug Discovery Today: Disease Mechanisms | Cardiology Vol. 5, No. 3–4 2008
quantifying EPCs by flow cytometry from peripheral blood,
the most commonly used combination of surface marker
currently encompasses analysis of CD34+ subpopulations
defined as (CD133+)CD34+VEGFR2+ cells [38]. Principally,
this approach is performed within the mononuclear (lym-
pho/monocyte) population of lysed whole blood by addi-
tionally sub-gating on CD45low/� events [37]. Such a double-
gating strategy allows more exact identification of the very
low number of circulating EPCs (0.01–0.2% of the peripheral
blood mononuclear cells) [37]. Because of these very low
numbers of positive cells additional efforts are necessary to
increase analytical sensitivity, for example, the use of bright
fluorochrome for dimly expressed marker, automatic com-
pensation in the multicolour experiments, minimizing back-
ground noise, smooth fixation and recording more events
(e.g. at least 50,000) within the target gate [6,14,37,38].
The second approach for quantifying EPCs by in vitro
cultivation to obtain CFUs has also been used several times
[24–26]. The number of EPCs (measured by CFU assay) has
been shown to significantly increase in patients with unstable
angina, although their function (determined as adhesion to
fibronectin) did not differ as compared to patients with stable
CAD [40]. These results imply that enhanced number of EPC-
CFU do not necessarily associate with improved function.
However, recent data revealed that the CFU count did not
correlate with the number of circulating CD34+VEGFR2+ cells
[38]. Thus, the ability of separated mononuclear cells to form
CFUs in vitro may rather represent a functional assay for
clonogenic capacity but the enumeration of CFUs is not
the method of choice for direct ex vivo quantification of
circulating EPCs.
Taken together, some controversial findings in the clinical
studies above may also reflect the different methods and
definitions used to assess EPCs in peripheral blood as well
as interpretation of rather functional in vitro parameters (e.g.
CFU count) as quantitative ex vivo marker. Hence, consider-
ing the growing evidence in support of circulating vascular
progenitor cells as predictive biomarkers (positive or nega-
tive) of endothelial maintenance during atherosclerosis and
cancer, it would be crucial for the clinic to establish further
definitive standards for routinely monitoring endothelial-
like cells in peripheral blood. To adequately address the
multiple EPC phenotypes, a simultaneous ex vivo measure-
ment by flow cytometry of ‘classical’ CD34+VEGFR2+C-
D45low/� EPCs in conjunction with CD14low/+ myeloid cells
(e.g. CD14lowCD16+Tie-2+ monocyte subsets) may be more
meaningful in terms of potential prognostic/diagnostic target
(Fig. 1).
Summary and conclusions
Diverse subpopulations of circulating or tissue resident adult
progenitor cells may acquire endothelial phenotype and
functional characteristics of mature endothelial cells, thus
e270 www.drugdiscoverytoday.com
obviously participating in vascular repair and angiogenesis.
Parallel to inflammatory and immunological cues, these cells
are recognised as fundamental players in the pathology of
atherosclerosis, arterial remodelling after injury but also in
cancer disease. Recent basic and clinical research intensively
discusses the relevance of EPCs as surrogate cellular biomar-
kers in vascular disorder. Standardisation of the multi-para-
metric flow cytometry protocols currently used is crucial for
the direct quantification of circulating angiogenic progenitor
cells as vascular biomarkers. In terms of clinical prognosis and
diagnosis this will strengthen the significance of EPCs in
routinely monitoring drug activity and endothelial home-
ostasis. Last but not least, simultaneous express analysis of
more than one circulating progenitor cell subpopulation (e.g.
as a biomarker package) may substantially contribute to a
more complex prognostic and diagnostic statement.
Acknowledgement
This work was supported by a grant from the Interdisciplinary
Centre for Clinical Research ‘‘BIOMAT’’ within the Faculty of
Medicine at the RWTH Aachen University (NTV B113-a).
References1 Libby, P. and Aikawa, M. (2002) Stabilization of atherosclerotic plaques:
new mechanisms and clinical targets. Nat. Med. 8, 1257–1262
2 Hansson, G.K. and Libby, P. (2006) The immune response in
atherosclerosis: a double-edged sword. Nat. Rev. Immunol. 6, 508–519
3 Hristov, M. and Weber, C. (2004) Endothelial progenitor cells:
characterization, pathophysiology, and possible clinical relevance. J. Cell
Mol. Med. 8, 498–508
4 Asahara, T. et al. (1997) Isolation of putative progenitor endothelial cells
for angiogenesis. Science 275, 964–967
5 Peichev, M. et al. (2000) Expression of VEGFR-2 and AC133 by circulating
human CD34(+) cells identifies a population of functional endothelial
precursors. Blood 95, 952–958
6 Bertolini, F. et al. (2006) The multifaceted circulating endothelial cell in
cancer: towards marker and target identification. Nat. Rev. Cancer 6,
835–845
7 Carmeliet, P. (2003) Angiogenesis in health and disease. Nat. Med. 9,
653–660
8 Yamashita, J. et al. (2000) Flk1-positive cells derived from embryonic stem
cells serve as vascular progenitors. Nature 408, 92–96
9 Yoon, Y.S. et al. (2005) Clonally expanded novel multipotent stem cells
from human bone marrow regenerate myocardium after myocardial
infarction. J. Clin. Invest. 115, 326–338
10 Zengin, E. et al. (2006) Vascular wall resident progenitor cells: a source for
postnatal vasculogenesis. Development 133, 1543–1551
11 Harraz, M. et al. (2001) CD34-blood-derived human endothelial cell
progenitors. Stem Cells 19, 304–312
12 Zhao, Y. et al. (2003) A human peripheral blood monocyte-derived subset
acts as pluripotent stem cells. Proc. Natl. Acad. Sci. U. S. A. 100, 2426–2431
13 Deschaseaux, F. et al. (2007) Two types of circulating endothelial
progenitor cells in patients receiving long term therapy by HMG-CoA
reductase inhibitors. Eur. J. Pharmacol. 562, 111–118
14 Redondo, S. et al. (2008) High-reproducible flow cytometric endothelial
progenitor cell determination in human peripheral blood as CD34+/
CD144+/CD3-lymphocyte sub-population. J. Immunol. Methods 335, 21–27
15 De Palma, M. et al. (2007) Tie2-expressing monocytes: regulation of tumor
angiogenesis and therapeutic implications. Trends Immunol. 28, 519–524
16 Elsheikh, E. et al. (2005) Only a specific subset of human peripheral-blood
monocytes has endothelial-like functional capacity. Blood 106, 2347–2355

Vol. 5, No. 3–4 2008 Drug Discovery Today: Disease Mechanisms | Cardiology
17 Hristov, M. et al. (2007) Importance of CXC chemokine receptor 2 in the
homing of human peripheral blood endothelial progenitor cells to sites of
arterial injury. Circ. Res. 100, 590–597
18 Walter, D.H. et al. (2002) Statin therapy accelerates reendothelialization: a
novel effect involving mobilization and incorporation of bone marrow-
derived endothelial progenitor cells. Circulation 105, 3017–3024
19 Werner, N. et al. (2003) Intravenous transfusion of endothelial
progenitor cells reduces neointima formation after vascular injury. Circ.
Res. 93, e17–24
20 Rauscher, F.M. et al. (2003) Aging, progenitor cell exhaustion, and
atherosclerosis. Circulation 108, 457–463
21 Hu, Y. et al. (2003) Endothelial replacement and angiogenesis in
arteriosclerotic lesions of allografts are contributed by circulating
progenitor cells. Circulation 108, 3122–3127
22 Hristov, M. et al. (2006) Intracoronary infusion of autologous bone
marrow cells and left ventricular function after acute myocardial
infarction: a meta-analysis. J. Cell Mol. Med. 10, 727–733
23 Gruh, I. et al. (2006) No evidence of transdifferentiation of human
endothelial progenitor cells into cardiomyocytes after coculture with
neonatal rat cardiomyocytes. Circulation 113, 1326–1334
24 Werner, N. and Nickenig, G. (2006) Influence of cardiovascular risk factors
on endothelial progenitor cells: limitations for therapy? Arterioscler.
Thromb. Vasc. Biol. 26, 257–266
25 Guven, H. et al. (2006) The number of endothelial progenitor cell colonies
in the blood is increased in patients with angiographically significant
coronary artery disease. J. Am. Coll Cardiol. 48, 1579–1587
26 Xiao, Q. et al. (2007) Endothelial progenitor cells, cardiovascular risk
factors, cytokine levels and atherosclerosis – results from a large
population-based study. PLoS ONE 2, e975
27 Hristov, M. et al. (2007) Reduced numbers of circulating endothelial
progenitor cells in patients with coronary artery disease associated with
long-term statin treatment. Atherosclerosis 192, 413–420
28 Leone, A.M. et al. (2005) Mobilization of bone marrow-derived stem cells
after myocardial infarction and left ventricular function. Eur. Heart J. 26,
1196–1204
29 Madjid, M. et al. (2004) Leukocyte count and coronary heart disease:
implications for risk assessment. J. Am. Coll Cardiol. 44, 1945–1956
30 George, J. et al. (2005) Transfer of endothelial progenitor and bone marrow
cells influences atherosclerotic plaque size and composition in
apolipoprotein E knockout mice. Arterioscler. Thromb. Vasc. Biol. 25,
2636–2641
31 Purhonen, S. et al. (2008) Bone marrow-derived circulating endothelial
precursors do not contribute to vascular endothelium and are not needed
for tumor growth. Proc. Natl. Acad. Sci. U. S. A. 105, 6620–6625
32 Braunstein, M. et al. (2006) Endothelial progenitor cells display clonal
restriction in multiple myeloma. BMC Cancer 6, 161
33 Weber, C. et al. (2000) Differential chemokine receptor expression and
function in human monocyte subpopulations. J. Leukoc. Biol. 67, 699–704
34 Sandri, M. et al. (2005) Effects of exercise and ischemia on mobilization
and functional activation of blood-derived progenitor cells in patients
with ischemic syndromes: results of 3 randomized studies. Circulation 111,
3391–3399
35 Pistrosch, F. et al. (2005) PPARgamma-agonist rosiglitazone increases
number and migratory activity of cultured endothelial progenitor cells.
Atherosclerosis 183, 163–167
36 Wang, C.H. et al. (2006) Enalapril increases ischemia-induced endothelial
progenitor cell mobilization through manipulation of the CD26 system. J.
Mol. Cell Cardiol. 41, 34–43
37 Duda, D.G. et al. (2007) A protocol for phenotypic detection and
enumeration of circulating endothelial cells and circulating progenitor
cells in human blood. Nat. Protoc. 2, 805–810
38 Van Craenenbroeck, E.M. et al. (2008) Quantification of circulating
endothelial progenitor cells: a methodological comparison of six flow
cytometric approaches. J. Immunol. Methods 332, 31–40
39 Schober, A. et al. (2005) Peripheral CD34+ cells and the risk of in-stent
restenosis in patients with coronary heart disease. Am. J. Cardiol. 96,
1116–1122
40 George, J. et al. (2004) Circulating endothelial progenitor cells in patients
with unstable angina: association with systemic inflammation. Eur. Heart
J. 25, 1003–1008
www.drugdiscoverytoday.com e271