Endocrine Diseases
76
Adrenal disorders Adrenal insufficiency From Wikipedia, the free encyclopedia Adrenal insufficiency Classification and external resources Adrenal gland ICD -10 E 27.1 -E 27.4 ICD -9 255.4 eMedicine emerg/16 MeSH D000309 Adrenal insufficiency is a condition in which the adrenal glands do not produce adequate amounts of steroid hormones , primarily cortisol ; but may also include impaired production of aldosterone (a mineralocorticoid ), which regulates sodium conservation, potassium secretion, and water retention. [1] [2] Craving for salt or salty foods due to the urinary losses of sodium is common. [3] Addison's disease and congenital adrenal hyperplasia can manifest as adrenal insufficiency. If not treated, adrenal insufficiency may result in severe abdominal pains, vomiting, profound muscle weakness and fatigue, depression ,
-
Upload
shobanaaaradhana -
Category
Documents
-
view
18 -
download
4
description
Notes for civil service preparation
Transcript of Endocrine Diseases

Adrenal disorders
Adrenal insufficiencyFrom Wikipedia, the free encyclopedia
Adrenal insufficiency
Classification and external resources
Adrenal gland
ICD-10 E 27.1 -E 27.4
ICD-9 255.4
eMedicine emerg/16
MeSH D000309
Adrenal insufficiency is a condition in which the adrenal glands do not produce adequate amounts
of steroid hormones, primarily cortisol; but may also include impaired production
of aldosterone (a mineralocorticoid), which regulates sodium conservation, potassium secretion, and water
retention.[1][2] Craving for salt or salty foods due to the urinary losses of sodium is common.[3]
Addison's disease and congenital adrenal hyperplasia can manifest as adrenal insufficiency. If not treated,
adrenal insufficiency may result in severe abdominal pains, vomiting, profound muscle weakness and
fatigue, depression, extremely low blood pressure (hypotension), weight loss, kidney failure, changes in
mood and personality, and shock (adrenal crisis).[4] An adrenal crisis often occurs if the body is subjected to
stress, such as an accident, injury, surgery, or severe infection; death may quickly follow. [4]

Adrenal insufficiency can also occur when the hypothalamus or the pituitary gland does not make adequate
amounts of the hormones that assist in regulating adrenal function.[1][5][6] This is called secondary or tertiary
adrenal insufficiency and is caused by lack of production of ACTH in the pituitary or lack of CRH in the
hypothalamus, respectively.[7]
Contents
[hide]
1 Types
2 Signs and symptoms
3 Causes
4 Diagnosis
5 Treatment
6 See also
7 References
8 External links
Types[edit]
There are three major types of adrenal insufficiency.
Primary adrenal insufficiency is due to impairment of the adrenal glands.
80% are due to an autoimmune disease called Addison's disease or autoimmune adrenalitis.
One subtype is called idiopathic, or of unknown cause.
Other cases are due to congenital adrenal hyperplasia or an adenoma (tumor) of the adrenal
gland.
Secondary adrenal insufficiency is caused by impairment of the pituitary gland or hypothalamus.[8] The
most common cause in the United States is exogenous steroid use. Other causes are a pituitary
adenoma or microadenoma; a hypothalamic tumor (surgical removal of a pituitary tumor can also
suppress production of ACTH and lead to adrenal deficiency); and Sheehan's syndrome, which is
associated with impairment of only the pituitary gland.
Tertiary adrenal insufficiency is due to hypothalamic disease and decrease in corticotropin releasing
factor (CRF).[9]
Signs and symptoms[edit]
Symptoms include: hypoglycemia, dehydration, weight loss, and disorientation. Symptoms may also
include weakness, tiredness, dizziness, low blood pressure that falls further when standing (orthostatic
hypotension), cardiovascular collapse, muscle aches, nausea, vomiting, and diarrhea. These problems
may develop gradually and insidiously. Addison's disease can present with tanning of the skin that may be

patchy or even all over the body. Characteristic sites of tanning are skin creases (e.g. of the hands) and the
inside of the cheek (buccal mucosa). Goitre and vitiligomay also be present.[4]
Causes[edit]
Causes of acute adrenal insufficiency are mainly Waterhouse-Friderichsen syndrome, sudden withdrawal
of long-term corticosteroid therapy, and stress in patients with underlying chronic adrenal insufficiency.[10] The latter is termed critical illness–related corticosteroid insufficiency.
For chronic adrenal insufficiency, the major contributors are autoimmune adrenalitis, tuberculosis, AIDS,
and metastatic disease.[10] Minor causes of chronic adrenal insufficiency are systemic amyloidosis, fungal
infections, hemochromatosis, and sarcoidosis.[10]
Autoimmune adrenalitis may be part of Type 2 autoimmune polyglandular syndrome, which can
include type 1 diabetes, hyperthyroidism, and autoimmune thyroid disease (also known asautoimmune
thyroiditis, Hashimoto's thyroiditis, and Hashimoto's disease).[11] Hypogonadism and pernicious anemia may
also present with this syndrome.
Adrenoleukodystrophy can also cause adrenal insufficiency.[12]
Adrenal insufficiency can also result when a patient has a craniopharyngioma, which is a histologically
benign tumor that can damage the pituitary gland and so cause the adrenal glands not to function. This
would be an example of secondary adrenal insufficiency syndrome.
Adrenal insufficiency can also occur when a patients suffers from Chronic Fatigue Syndrome long term.[citation needed] This can induce Adrenal Insufficiency through oxidative damage to any of theHypothalamic–
pituitary–adrenal axis (HPA-Axis) organs[citation needed]: the Hypothalamus, the Pituitary gland or the Adrenal
gland. Onset in these cases is often insidious.
Diagnosis[edit]
If the person is in adrenal crisis, the ACTH stimulation test [13] may be given. If not in crisis, cortisol, ACTH,
aldosterone, renin, potassium, and sodium are tested from a blood sample before the decision is made
whether the ACTH stimulation test needs to be performed. X-rays or CT of the adrenals may also be done.[1] The best test for adrenal insufficiency of autoimmune origin, representing more than ninety percent of all
cases in a Western population, is measurement of 21-hydroxylase autoantibodies.
Source of pathology
CRHACT
HDHE
ADHEA-S
cortisol
aldosterone
renin
Na K Causes5
hypothalamus
(tertiary)1
low low low low low3 low lowlow
lowtumor of the hypothalamus
(adenoma), antibodies, environment (i.e. toxins), head injury
pituitary hig low low low low3 low low lo low tumor of the pituitary

(secondary) h2 w
(adenoma), antibodies, environment, head injury,
surgical removal6, Sheehan's syndrome
adrenal glands
(primary)7
high high high high low4 low highlow
high
tumor of the adrenal (adenoma), stress, antibodies,
environment, Addison's Disease, trauma, surgical
removal (resection), miliary tuberculosis
of the adrenal
1 Automatically includes diagnosis of secondary (hypopituitarism)
2 Only if CRH production in the hypothalamus is intact
3 Value doubles or more in stimulation
4 Value less than doubles in stimulation
5 Most common, does not include all possible causes
6 Usually because of very large tumor (macroadenoma)
7 Includes Addison's disease
Treatment[edit]
Adrenal crisis
Intravenous fluids[4]
Intravenous steroid (Solu-Cortef/injectable hydrocortisone) later hydrocortisone, prednisone or
methylpredisolone tablets[4]
Rest
Cortisol deficiency (primary and secondary)
Hydrocortisone (Cortef)
Prednisone (Deltasone)
Prednisolone (Delta-Cortef)
Methylprednisolone (Medrol)
Dexamethasone (Decadron)
Mineralocorticoid deficiency (low aldosterone)

Fludrocortisone Acetate
(To balance sodium, potassium and increase water retention)[4]
Addison's diseaseFrom Wikipedia, the free encyclopedia
Addison's disease
Classification and external resources
ICD-10 E 27.1 -E 27.2
ICD-9 255.4
DiseasesDB 222
MedlinePlus 000378
eMedicine med/42
MeSH D000224
Addison’s disease (also Addison disease, chronic adrenal insufficiency, hypocortisolism,
and hypoadrenalism) is a rare, chronic endocrinedisorder in which the adrenal glands do not produce
sufficient steroid hormones (glucocorticoids and often mineralocorticoids). It is characterized by a number
of relatively nonspecific symptoms, such as abdominal pain and weakness, but under certain
circumstances, these may progress toAddisonian crisis, a severe illness which may include very low
blood pressure and coma.
The condition arises from problems with the adrenal gland, "primary adrenal insufficiency", and can be
caused by damage by the body's own immune system, certain infections, or various rarer causes.
Addison's disease is also known as chronic primary adrenocortical insufficiency, to distinguish it from acute
primary adrenocortical insufficiency, most often caused by Waterhouse-Friderichsen syndrome. Addison's
disease should also be distinguished from secondary and tertiary adrenal insufficiency, which are caused
by deficiency of ACTH (produced by the pituitary gland) and CRH(produced by the hypothalamus),
respectively. Despite this distinction, Addisonian crises can happen in all forms of adrenal insufficiency.
Addison's disease and other forms of hypoadrenalism are generally diagnosed via blood tests and medical
imaging.[1] Treatment involves replacing the absent hormones (oral hydrocortisone and fludrocortisone).

[2] Lifelong, continuous steroid replacement therapy is required, with regular follow-up treatment and
monitoring for other health problems.[1]
Addison’s disease is named after Dr. Thomas Addison, the British physician who first described the
condition in 1849. The adjective "Addisonian" is used to describe features of the condition, as well as
patients suffering from Addison’s disease.[1]
Contents
[hide]
1 Signs and symptoms
o 1.1 Clinical signs
o 1.2 Addisonian crisis
2 Causes
o 2.1 Adrenal dysgenesis
o 2.2 Impaired steroidogenesis
o 2.3 Adrenal destruction
o 2.4 Corticosteroid withdrawal
3 Diagnosis
o 3.1 Suggestive features
o 3.2 Testing
4 Treatment
o 4.1 Maintenance
o 4.2 Crisis
5 Epidemiology
6 Prognosis
7 History
o 7.1 Discovery and development
o 7.2 Notable cases
8 In other animals
9 References
10 External links

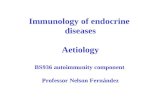
Signs and symptoms[edit]
Classic hyperpigmentation as seen in Addison's disease
The symptoms of Addison's disease develop insidiously and may take some time to be recognized. The
most common symptoms are fatigue,lightheadedness upon standing or while upright, muscle
weakness, fever, weight loss, difficulty in standing up,
anxiety, nausea, vomiting, diarrhea,headache, sweating, changes in mood and personality,
and joint and muscle pains. Some have marked cravings for salt or salty foods due to the urinary losses of
sodium.[1] Hyperpigmentation of the skin may be noted, particularly in sun-exposed areas, as well as
darkening of the palmar creases, sites of friction, recent scars, the vermilion border of the lips, and genital
skin.[3] This is not encountered in secondary and tertiary hypoadrenalism.[2]
Clinical signs[edit]
The negative feedback loop for glucocorticoids
On examination, the following may be noticed:[1]
Low blood pressure that falls further when standing (orthostatic hypotension)

Most people with primary Addison's have darkening (hyperpigmentation) of the skin, including areas
not exposed to the sun; characteristic sites are skin creases (e.g. of the hands), nipple, and the inside
of the cheek (buccal mucosa); also, old scars may darken. This occurs becausemelanocyte-stimulating
hormone (MSH) and adrenocorticotropic hormone (ACTH) share the same precursor molecule, pro-
opiomelanocortin(POMC). After production in anterior pituitary gland, POMC gets cleaved into gamma-
MSH, ACTH and beta-lipotropin. The subunit ACTH undergoes further cleavage to produce alpha-
MSH, the most important MSH for skin pigmentation. In secondary and tertiary forms of Addison's, skin
darkening does not occur.
Medical conditions, such as type I diabetes, thyroid disease (Hashimoto's thyroiditis and goiter),
and vitiligo often occur together with Addison's (often in the setting of autoimmune polyendocrine
syndrome). Hence, symptoms and signs of any of the former conditions may also be present in the
individual with Addison's. The occurrence of Addison's disease in someone who also has Hashimoto's
thyroiditis is called Schmidt syndrome.
Addisonian crisis[edit]
Main article: Adrenal crisis
An "Addisonian crisis" or "adrenal crisis" is a constellation of symptoms that indicate severe adrenal
insufficiency. This may be the result of either previously undiagnosed Addison's disease, a disease process
suddenly affecting adrenal function (such as adrenal hemorrhage), or an intercurrent problem (e.g.
infection, trauma) in someone known to have Addison's disease. It is a medical emergency and potentially
life-threatening situation requiring immediate emergency treatment.
Characteristic symptoms are:[4]
Sudden penetrating pain in the legs, lower back or abdomen
Severe vomiting and diarrhea, resulting in dehydration
Low blood pressure
Syncope (loss of consciousness and ability to stand)
Hypoglycemia (reduced level of blood glucose)
Confusion, psychosis, slurred speech
Severe lethargy
Hyponatremia (low sodium level in the blood)
Hyperkalemia (elevated potassium level in the blood)
Hypercalcemia (elevated calcium level in the blood)
Convulsions
Fever

Causes[edit]
Causes of adrenal insufficiency can be grouped by the way they cause the adrenals to produce insufficient
cortisol. These are adrenal dysgenesis (the gland has not formed adequately during development),
impaired steroidogenesis (the gland is present but is biochemically unable to produce cortisol) or adrenal
destruction (disease processes leading to the gland being damaged).[1]
Adrenal dysgenesis[edit]
All causes in this category are genetic, and generally very rare. These include mutations to
the SF1 transcription factor, congenital adrenal hypoplasia (CAH) due to DAX-1 gene mutations and
mutations to the ACTH receptor gene (or related genes, such as in the Triple A or Allgrove
syndrome). DAX-1 mutations may cluster in a syndrome with glycerol kinase deficiency with a number of
other symptoms when DAX-1 is deleted together with a number of other genes.[1]
Impaired steroidogenesis[edit]
To form cortisol, the adrenal gland requires cholesterol, which is then converted biochemically into steroid
hormones. Interruptions in the delivery of cholesterol include Smith-Lemli-Opitz
syndrome and abetalipoproteinemia.
Of the synthesis problems, congenital adrenal hyperplasia is the most common (in various forms: 21-
hydroxylase, 17α-hydroxylase, 11β-hydroxylase and 3β-hydroxysteroid dehydrogenase),lipoid CAH due to
deficiency of StAR and mitochondrial DNA mutations.[1] Some medications interfere with steroid synthesis
enzymes (e.g. ketoconazole), while others accelerate the normal breakdown of hormones by
the liver (e.g. rifampicin, phenytoin).[1]
Adrenal destruction[edit]
Autoimmune adrenalitis is the most common cause of Addison's disease in the industrialized
world. Autoimmune destruction of the adrenal cortex is caused by an immune reaction against the
enzyme 21-hydroxylase (a phenomenon first described in 1992).[5] This may be isolated or in the context
of autoimmune polyendocrine syndrome (APS type 1 or 2), in which other hormone-producing organs, such
as the thyroid and pancreas, may also be affected.[6]
Adrenal destruction is also a feature of adrenoleukodystrophy (ALD), and when the adrenal glands are
involved in metastasis (seeding of cancer cells from elsewhere in the body,
especially lung),hemorrhage (e.g. in Waterhouse-Friderichsen syndrome or antiphospholipid syndrome),
particular infections (tuberculosis, histoplasmosis, coccidioidomycosis), deposition of abnormal protein
inamyloidosis.[7]
Corticosteroid withdrawal[edit]
Use of high-dose steroids for more than a week begins to produce suppression of the patient's adrenal
glands because the exogenous glucocorticoids suppress hypothalamic corticotropin-releasing hormone
(CRH) and pituitary adrenocorticotropic hormone (ACTH). With prolonged suppression, the adrenal glands

atrophy (physically shrink), and can take months to recover full function after discontinuation of the
exogenous glucocorticoid. During this recovery time, the patient is vulnerable to adrenal insufficiency
during times of stress, such as illness.[8]
Diagnosis[edit]
Suggestive features[edit]
Routine investigations may show:[1]
Hypercalcemia
Hypoglycemia , low blood sugar (worse in children due to loss of glucocorticoid's glucogenic effects)
Hyponatremia (low blood sodium levels), due to the kidney's inability to excrete free water in the
absence of sufficient cortisol, and also the effect of corticotropin-releasing hormone to stimulate
secretion of ADH. That hyponatremia occurs even in secondary adrenal insufficiency (i.e. due
to pituitary disease), in which aldosterone deficiency is not a feature, underscores the fact that
hyponatremia in Addison's disease is not due to lack of aldosterone.
Hyperkalemia (raised blood potassium levels), due to loss of production of the hormone aldosterone.
Eosinophilia and lymphocytosis (increased number of eosinophils or lymphocytes, two types of white
blood cells)
Metabolic acidosis (increased blood acidity), also is due to loss of the hormone aldosterone because
sodium reabsorption in the distal tubule is linked with acid/hydrogen ion (H+) secretion. Low levels of
aldosterone stimulation of the renal distal tubule leads to sodium wasting in the urine and H+ retention
in the serum.
Testing[edit]
Cortisol

Aldosterone
In suspected cases of Addison's disease, one needs to demonstrate that adrenal hormone levels are low
even after appropriate stimulation (called theACTH stimulation test) with synthetic pituitary ACTH
hormone tetracosactide. Two tests are performed, the short and the long test. It should be noted that
dexamethasone does not cross-react with the assay and can be administered concomitantly during testing.
The short test compares blood cortisol levels before and after 250 micrograms of tetracosactide
(intramuscular or intravenous) is given. If, one hour later,plasma cortisol exceeds 170 nmol/l and has risen
by at least 330 nmol/l to at least 690 nmol/l, adrenal failure is excluded. If the short test is abnormal, the
long test is used to differentiate between primary adrenal insufficiency and secondary adrenocortical
insufficiency.
The long test uses 1 mg tetracosactide (intramuscular). Blood is taken 1, 4, 8, and 24 hr later. Normal
plasma cortisol level should reach 1000 nmol/l by 4 hr. In primary Addison's disease, the cortisol level is
reduced at all stages, whereas in secondary corticoadrenal insufficiency, a delayed but normal response is
seen.
Other tests may be performed to distinguish between various causes of hypoadrenalism,
including renin and adrenocorticotropic hormone levels, as well as medical imaging - usually in the form
of ultrasound, computed tomography or magnetic resonance imaging.
Adrenoleukodystrophy, and the milder form, adrenomyeloneuropathy, cause adrenal insufficiency
combined with neurological symptoms. These diseases are estimated to be the cause of adrenal
insufficiency in about 35% of male patients with idiopathic Addison’s disease, and should be considered in
the differential diagnosis of any male with adrenal insufficiency. Diagnosis is made by a blood test to
detect very long chain fatty acids.[9]
Treatment[edit]
Maintenance[edit]
Treatment for Addison's disease involves replacing the missing cortisol, sometimes in the form
of hydrocortisone tablets, or prednisone tablets in a dosing regimen that mimics the physiological
concentrations of cortisol. Alternatively, one-quarter as much prednisolone may be used for equal

glucocorticoid effect as hydrocortisone. Treatment must usually be continued for life. In addition, many
patients require fludrocortisone as replacement for the missing aldosterone. Caution must be exercised
when persons with Addison's disease become unwell with infection, have surgery or other trauma, or
become pregnant. In such instances, their replacement glucocorticoids, whether in the form of
hydrocortisone, prednisone, prednisolone, or other equivalent, often must be increased. Inability to take
oral medication may prompt hospital admission to receive steroids intravenously. People with Addison's are
often advised to carry information on them (e.g., in the form of a MedicAlert bracelet) for the attention
of emergency medical services personnel who might need to attend to their needs.
Crisis[edit]
Standard therapy involves intravenous injections of glucocorticoids and large volumes of intravenous saline
solution with dextrose (glucose). This treatment usually brings rapid improvement. When the patient can
take fluids and medications by mouth, the amount of glucocorticoids is decreased until a maintenance dose
is reached. If aldosterone is deficient, maintenance therapy also includes oral doses of fludrocortisone
acetate.[10]
Epidemiology[edit]
The frequency rate of Addison's disease in the human population is sometimes estimated at roughly one in
100,000.[11] Some research and information sites put the number closer to 40-60 cases per million
population. (1/25,000-1/16,600)[12] (Determining accurate numbers for Addison's is problematic at best and
some incidence figures are thought to be underestimates.[13]) Addison's can afflict persons of any age,
gender, or ethnicity, but it typically presents in adults between 30 and 50 years of age. [14] Research has
shown no significant predispositions based on ethnicity.[12]
Prognosis[edit]
With proper medication, especially hormone replacement therapy, patients can expect to live relatively
normal lives.[15]
People with adrenal insufficiency should always carry identification stating their condition in case of an
emergency. The card should alert emergency personnel about the need to inject 100 mg of cortisol if its
bearer is found severely injured or unable to answer questions. The card should also include the doctor's
name and telephone number and the name and telephone number of the nearest relative to be notified. [16]
When traveling, a needle, syringe, and an injectable form of cortisol should be carried for emergencies. A
person with Addison's disease also should know how to increase medication during periods of stress or
mild upper respiratory infections. Immediate medical attention is needed when severe infections, vomiting,
or diarrhea occurs, as these conditions can precipitate an Addisonian crisis. A patient who is vomiting may
require injections of hydrocortisone, since oral hydrocortisone supplements cannot be adequately
metabolised.[17]

History[edit]
Discovery and development[edit]
Addison’s disease is named after Dr. Thomas Addison, the British physician who first described the
condition in On the Constitutional and Local Effects of Disease of the Suprarenal Capsules(1849).[18] All of
Addison's six original patients had tuberculosis of the adrenal glands.[19] While Addison's six patients in
1855 all had adrenal tuberculosis, the term "Addison's disease" does not imply an underlying disease
process.
The condition was initially considered a form of anemia associated with the adrenal glands. Because little
was known at the time about the adrenal glands (then called "Supra-Renal Capsules"), Dr. Addison’s
monograph describing the condition was an isolated insight. As the adrenal function became better known,
Dr. Addison’s monograph became known as an important medical contribution and a classic example of
careful medical observation.[20]
Notable cases[edit]
United States president John F. Kennedy(1917-63), probably the single most famous case of Addison's disease
United States President John F. Kennedy was one of the best-known Addison's disease sufferers. He
was possibly one of the first Addisonians to survive major surgery.[21] Substantial secrecy surrounded
his health during his years as president.[22]
Eunice Kennedy Shriver , one of John F. Kennedy's sisters, was believed to have Addison's disease as
well.[23]
Popular singer Helen Reddy [24]
Scientist Eugene Merle Shoemaker, co-discoverer of the Comet Shoemaker-Levy 9.[25]
French Carmelite nun and religious writer Blessed Elizabeth of the Trinity [26]

American artist Ferdinand Louis Schlemmer died from Addison's disease.
Some have suggested Jane Austen was an avant la lettre case, but others have disputed this.[27]
According to Dr. Carl Abbott, a Canadian medical researcher, Charles Dickens may also have been
affected.[28]
Australia's youngest rugby league football international, Geoff Starling [29]
Osama bin Laden may have been an Addisonian. Lawrence Wright noted that bin Laden manifested
all the key symptoms, such as "low blood pressure, weight loss, muscle fatigue, stomach irritability,
sharp back pains, dehydration, and an abnormal craving for salt". Bin Laden was known to have
consumed large amounts of the drug sulbutiamine to treat his symptoms.[30]
Basque nationalist and founder of the Basque Nationalist Party, Sabino Arana died in Sukarrieta at the
age of 38 after falling ill with Addison's disease during time spent in prison.
One of Canada's top gymnasts, Nathan Gafuik, was diagnosed with Addison's disease when he was
15.[31]
In other animals[edit]
Main article: Addison's disease in canines
The condition has been diagnosed in all breeds of dogs. In general, it is underdiagnosed, and one must
clinically suspect it as an underlying disorder for many presenting complaints. Females are
overrepresented, and the disease often appears in middle age (4–7 yr), although any age or either gender
may be affected. Genetic continuity between dogs and humans helps to explain the occurrence of
Addison's disease in both species.[32]
Hypoadrenocorticism is treated with fludrocortisone or a monthly injection called Percorten V
(desoxycorticosterone pivlate (DOCP)) and prednisone. Routine blood work is necessary in the initial
stages until a maintenance dose is established. Most of the medications used in the therapy of
hypoadrenocorticism cause excessive thirst and urination, making it important to provide enough drinking
water. If the owner knows about an upcoming stressful situation (shows, traveling, etc.), patients generally
need an increased dose of prednisone to help deal with the added stress. Avoidance of stress is important
for dogs with hypoadrenocorticism.
HypoaldosteronismFrom Wikipedia, the free encyclopedia
(Redirected from Mineralocorticoid deficiency)
Hypoaldosteronism
Classification and external resources

Aldosterone
ICD-10 E 27.4
DiseasesDB 20960
MeSH D006994
In medicine (endocrinology), hypoaldosteronism refers to decreased levels of the hormone aldosterone.
The term "isolated hypoaldosteronism" is used to describe lowered aldosterone without corresponding changes in cortisol.[1] (The two hormones are both produced by the adrenals.)
Contents
[hide]
1 Causes
2 Treatment
3 Effects
4 See also
5 References
Causes[edit]
There are several causes for this condition, including primary adrenal insufficiency, congenital adrenal hyperplasia, and medications (certain diuretics,NSAIDs, and ACE inhibitors).
Aldosterone deficiency-Primary (rare)
1. Primary adrenal insufficiency2. Congenital adrenal hyperplasia (21 and 11β but not 17)3. Aldosterone synthase deficiency
Hyporeninemic hypoaldosteronism (due to decreased angiotensin 2 production as well as intra-adrenal dysfunction)[2]

1. Renal dysfunction-most commonly diabetic nephropathy2. ACE inhibitors 3. NSAIDs 4. Cyclosporine
Treatment[edit]
Aldosterone deficiency should be treated with a mineralocorticoid (such as fludrocortisone), as well as possibly a glucocorticoid for cortisol deficiency, if present.
Hyporeninemic hypoaldosteronism is amenable to fludrocortisone treatment,[2] but the accompanying hypertension and edema can prove a problem in these patients, so often a diuretic (such as the thiazide diuretic, bendrofluazide,or a loop diuretic, such as furosemide) is used to control the hyperkalemia.[3]
Effects[edit]
This condition may result in hyperkalemia, when it is sometimes termed 'type 4 renal tubular acidosis' even though it doesn't actually cause acidosis. It can also cause urinary sodium wasting, leading to volume depletion and hypotension.
Na+ is lost in the urine. K+ is retained, and the plasma K+ rises.[citation needed]
When adrenal insufficiency develops rapidly, the amount of Na+ lost from the extracellular fluid exceeds the amount excreted in the urine, indicating that Na+ also must be entering cells. When the posterior pituitary is intact, salt loss exceeds water loss, and the plasma Na+ falls. However, the plasma volume also is reduced, resulting in hypotension, circulatory insufficiency, and, eventually, fatal shock. These changes can be prevented to a degree by increasing the dietary NaCl intake. Rats survive indefinitely on extra salt alone, but in dogs and most humans, the amount of supplementary salt needed is so large that it is almost impossible to prevent eventual collapse and death unless mineralocorticoid treatment is also instituted.[citation needed]
See also[edit]
Diabetes mellitusFrom Wikipedia, the free encyclopedia
(Redirected from Diabetes)
"Diabetes" redirects here. For other uses, see Diabetes (disambiguation).
Diabetes mellitus
Classification and external resources

Universal blue circle symbol for diabetes.[1]
ICD-10 E 10 –E 14
ICD-9 250
MedlinePlus 001214
eMedicine med/546 emerg/134
MeSH C18.452.394.750
Diabetes mellitus, or simply diabetes, is a group of metabolic diseases in which a person has high blood
sugar, either because the pancreas does not produce enough insulin, or because cells do not respond to
the insulin that is produced.[2] This high blood sugar produces the classical symptoms of polyuria (frequent
urination), polydipsia (increased thirst), and polyphagia (increased hunger).
There are three main types of diabetes mellitus (DM).
Type 1 DM results from the body's failure to produce insulin, and currently requires the person to inject
insulin or wear an insulin pump. This form was previously referred to as "insulin-dependent diabetes
mellitus" (IDDM) or "juvenile diabetes".
Type 2 DM results from insulin resistance, a condition in which cells fail to use insulin properly,
sometimes combined with an absolute insulin deficiency. This form was previously referred to as non
insulin-dependent diabetes mellitus (NIDDM) or "adult-onset diabetes".
The third main form, gestational diabetes, occurs when pregnant women without a previous diagnosis
of diabetes develop a high blood glucose level. It may precede development of type 2 DM.

Other forms of diabetes mellitus include congenital diabetes, which is due to genetic defects of insulin
secretion, cystic fibrosis-related diabetes, steroid diabetes induced by high doses of glucocorticoids, and
several forms of monogenic diabetes.
Untreated, diabetes can cause many complications. Acute complications include diabetic
ketoacidosis and nonketotic hyperosmolar coma. Serious long-term complications include cardiovascular
disease, chronic renal failure, and diabetic retinopathy (retinal damage). Adequate treatment of diabetes is
thus important, as well as blood pressure control and lifestyle factors such as stopping smoking and
maintaining a healthy body weight.
All forms of diabetes have been treatable since insulin became available in 1921, and type 2 diabetes may
be controlled with medications. Insulin and some oral medications can cause hypoglycemia (low blood
sugars), which can be dangerous if severe. Both types 1 and 2 are chronic conditions that cannot be cured.[3] Pancreas transplants have been tried with limited success in type 1 DM; gastric bypass surgery has been
successful in many with morbid obesity and type 2 DM. Gestational diabetes usually resolves after delivery.
Contents
[hide]
1 Classification
o 1.1 Type 1 diabetes
o 1.2 Type 2 diabetes
o 1.3 Gestational diabetes
o 1.4 Other types
2 Signs and symptoms
o 2.1 Diabetic emergencies
o 2.2 Complications
3 Causes
o 3.1 Type 1
o 3.2 Type 2
4 Pathophysiology
5 Diagnosis
6 Management
o 6.1 Lifestyle
o 6.2 Medications
o 6.3 Support
7 Epidemiology
8 History
o 8.1 Etymology

9 Society and culture
10 Other animals
11 References
12 Further reading
13 External links
Classification
Comparison of type 1 and 2 diabetes[4]
Feature Type 1 diabetes Type 2 diabetes
Onset Sudden Gradual
Age at onset Mostly in children Mostly in adults
Body habitus Thin or normal[5] Often obese
Ketoacidosis Common Rare
Autoantibodies Usually present Absent
Endogenous insulin
Low or absentNormal, decreasedor increased
Concordancein identical twins
50% 90%
Prevalence ~10% ~90%
Diabetes mellitus is classified into four broad categories: type 1 , type 2 , gestational diabetes, and "other
specific types".[2] The "other specific types" are a collection of a few dozen individual causes. [2] The term
"diabetes", without qualification, usually refers to diabetes mellitus. The rare disease diabetes insipidus has
similar symptoms to diabetes mellitus, but without disturbances in the sugar metabolism (insipidus means
"without taste" in Latin) and does not involve the same disease mechanisms.
The term "type 1 diabetes" has replaced several former terms, including childhood-onset diabetes, juvenile
diabetes, and insulin-dependent diabetes mellitus (IDDM). Likewise, the term "type 2 diabetes" has
replaced several former terms, including adult-onset diabetes, obesity-related diabetes, and noninsulin-

dependent diabetes mellitus (NIDDM). Beyond these two types, there is no agreed-upon standard
nomenclature.
Type 1 diabetesMain article: Diabetes mellitus type 1
Type 1 diabetes mellitus is characterized by loss of the insulin-producing beta cells of the islets of
Langerhans in the pancreas, leading to insulin deficiency. This type can be further classified as immune-
mediated or idiopathic. The majority of type 1 diabetes is of the immune-mediated nature, in which beta cell
loss is a T-cell-mediated autoimmune attack.[6] There is no known preventive measure against type 1
diabetes, which causes approximately 10% of diabetes mellitus cases in North America and Europe. Most
affected people are otherwise healthy and of a healthy weight when onset occurs. Sensitivity and
responsiveness to insulin are usually normal, especially in the early stages. Type 1 diabetes can affect
children or adults, but was traditionally termed "juvenile diabetes" because a majority of these diabetes
cases were in children.
"Brittle" diabetes, also known as unstable diabetes or labile diabetes, is a term that was traditionally used to
describe the dramatic and recurrent swings in glucose levels, often occurring for no apparent reason
in insulin-dependent diabetes. This term, however, has no biologic basis and should not be used. [7] There
are many reasons for type 1 diabetes to be accompanied by irregular and unpredictable hyperglycemia,
frequently with ketosis, and sometimes serious hypoglycemia, including an impaired counterregulatory
response to hypoglycemia, occult infection, gastroparesis (which leads to erratic absorption of dietary
carbohydrates), and endocrinopathies (e.g., Addison's disease).[7] These phenomena are believed to occur
no more frequently than in 1% to 2% of persons with type 1 diabetes.[8]
Type 2 diabetesMain article: Diabetes mellitus type 2
Type 2 diabetes mellitus is characterized by insulin resistance, which may be combined with relatively
reduced insulin secretion.[2] The defective responsiveness of body tissues to insulin is believed to involve
the insulin receptor. However, the specific defects are not known. Diabetes mellitus cases due to a known
defect are classified separately. Type 2 diabetes is the most common type.
In the early stage of type 2, the predominant abnormality is reduced insulin sensitivity. At this stage,
hyperglycemia can be reversed by a variety of measures and medications that improve insulin sensitivity or
reduce glucose production by the liver.
Gestational diabetesMain article: Gestational diabetes
Gestational diabetes mellitus (GDM) resembles type 2 diabetes in several respects, involving a
combination of relatively inadequate insulin secretion and responsiveness. It occurs in about 2–5% of

all pregnancies and may improve or disappear after delivery. Gestational diabetes is fully treatable, but
requires careful medical supervision throughout the pregnancy. About 20–50% of affected women develop
type 2 diabetes later in life.
Though it may be transient, untreated gestational diabetes can damage the health of the fetus or mother.
Risks to the baby include macrosomia (high birth weight), congenital cardiac and central nervous system
anomalies, and skeletal muscle malformations. Increased fetal insulin may inhibit
fetal surfactant production and cause respiratory distress syndrome. Hyperbilirubinemia may result from
red blood cell destruction. In severe cases, perinatal death may occur, most commonly as a result of poor
placental perfusion due to vascular impairment. Labor induction may be indicated with decreased placental
function. A Caesarean section may be performed if there is marked fetal distress or an increased risk of
injury associated with macrosomia, such as shoulder dystocia.
A 2008 study completed in the U.S. found the number of American women entering pregnancy with pre-
existing diabetes is increasing. In fact, the rate of diabetes in expectant mothers had more than doubled
from 1999 to 2005.[9] This is particularly problematic as diabetes raises the risk of complications during
pregnancy and increases the potential for the children of diabetic mothers to become diabetic in the future.
Other types
Prediabetes indicates a condition that occurs when a person's blood glucose levels are higher than normal
but not high enough for a diagnosis of type 2 DM. Many people destined to develop type 2 DM spend many
years in a state of prediabetes which has been termed "America's largest healthcare epidemic." [10]:10–11
Latent autoimmune diabetes of adults (LADA) is a condition in which type 1 DM develops in adults. Adults
with LADA are frequently initially misdiagnosed as having type 2 DM, based on age rather than etiology.
Some cases of diabetes are caused by the body's tissue receptors not responding to insulin (even when
insulin levels are normal, which is what separates it from type 2 diabetes); this form is very uncommon.
Genetic mutations (autosomal or mitochondrial) can lead to defects in beta cell function. Abnormal insulin
action may also have been genetically determined in some cases. Any disease that causes extensive
damage to the pancreas may lead to diabetes (for example, chronic pancreatitis and cystic fibrosis).
Diseases associated with excessive secretion of insulin-antagonistic hormones can cause diabetes (which
is typically resolved once the hormone excess is removed). Many drugs impair insulin secretion and some
toxins damage pancreatic beta cells. The ICD-10 (1992) diagnostic entity, malnutrition-related diabetes
mellitus (MRDM or MMDM, ICD-10 code E12), was deprecated by the World Health Organization when the
current taxonomy was introduced in 1999.[11]

Signs and symptoms
Overview of the most significant symptoms of diabetes
The classic symptoms of untreated diabetes are loss of weight, polyuria (frequent
urination), polydipsia (increased thirst), and polyphagia(increased hunger).[12] Symptoms may develop
rapidly (weeks or months) in type 1 diabetes, while they usually develop much more slowly and may be
subtle or absent in type 2 diabetes.
Prolonged high blood glucose can cause glucose absorption in the lens of the eye, which leads to changes
in its shape, resulting in vision changes. Blurred vision is a common complaint leading to a diabetes
diagnosis. A number of skin rashes that can occur in diabetes are collectively known as diabetic
dermadromes.
Diabetic emergencies
People (usually with type 1 diabetes) may also present with diabetic ketoacidosis, a state of metabolic
dysregulation characterized by the smell of acetone, a rapid, deep breathing known as Kussmaul
breathing, nausea, vomiting and abdominal pain, and altered states of consciousness.
A rare but equally severe possibility is hyperosmolar nonketotic state, which is more common in type 2
diabetes and is mainly the result of dehydration.
ComplicationsMain article: Complications of diabetes mellitus
All forms of diabetes increase the risk of long-term complications. These typically develop after many years
(10–20), but may be the first symptom in those who have otherwise not received a diagnosis before that

time. The major long-term complications relate to damage toblood vessels. Diabetes doubles the risk
of cardiovascular disease.[13] The main "macrovascular" diseases (related to atherosclerosis of larger
arteries) are ischemic heart disease (angina andmyocardial infarction), stroke, and peripheral vascular
disease.
Diabetes also damages the capillaries (causes microangiopathy).[14] Diabetic retinopathy, which affects
blood vessel formation in the retina of the eye, can lead to visual symptoms including reduced vision and
potentially blindness. Diabetic nephropathy, the impact of diabetes on the kidneys, can lead to scarring
changes in the kidney tissue, loss of small or progressively largeramounts of protein in the urine, and
eventually chronic kidney disease requiring dialysis.
Another risk is diabetic neuropathy, the impact of diabetes on the nervous system — most commonly
causing numbness, tingling, and pain in the feet, and also increasing the risk of skin damage due to altered
sensation. Together with vascular disease in the legs, neuropathy contributes to the risk of diabetes-related
foot problems (such as diabetic foot ulcers) that can be difficult to treat and occasionally
require amputation. Additionally, proximal diabetic neuropathy causes painful muscle wasting and
weakness.
Several studies suggest[15] a link between cognitive deficit and diabetes. Compared to those without
diabetes, the research showed that those with the disease have a 1.2 to 1.5-fold greater rate of decline in
cognitive function, and are at greater risk.
In the United States, there were approximately 675,000 diabetes-related emergency department (ED) visits
in 2010 that involved neurological complications, 409,000 ED visits with kidney complications, and 186,000
ED visits with eye complications.[16]
Causes
The cause of diabetes depends on the type.
Type 1
Type 1 diabetes is partly inherited, and then triggered by certain infections, with some evidence pointing
at Coxsackie B4 virus. A genetic element in individual susceptibility to some of these triggers has been
traced to particular HLA genotypes (i.e., the genetic "self" identifiers relied upon by the immune system).
However, even in those who have inherited the susceptibility, type 1 DM seems to require an
environmental trigger. The onset of type 1 diabetes is unrelated to lifestyle.
Type 2
Type 2 diabetes is due primarily to lifestyle factors and genetics.[17] A number of lifestyle factors are known
to be important to the development of type 2 diabetes, including obesity (defined by abody mass index of
greater than thirty), lack of physical activity, poor diet, stress, and urbanization.[4] Excess body fat is
associated with 30% of cases in those of Chinese and Japanese descent, 60-80% of cases in those of

European and African descent, and 100% of Pima Indians and Pacific Islanders.[2] Those who are not
obese often have a high waist–hip ratio.[2]
Dietary factors also influence the risk of developing type 2 diabetes. Consumption of sugar-sweetened
drinks in excess is associated with an increased risk.[18][19] The type of fats in the diet is also important,
with saturated fats and trans fatty acids increasing the risk and polyunsaturated and monounsaturated
fat decreasing the risk.[17] Eating lots of white rice appears to also play a role in increasing risk.[20] A lack of
exercise is believed to cause 7% of cases.[21]
The following is a comprehensive list of other causes of diabetes:[22]
Genetic defects of β-cell function
Maturity onset diabetes of the young
Mitochondrial DNA mutations
Genetic defects in insulin processing or insulin action
Defects in proinsulin conversion
Insulin gene mutations
Insulin receptor mutations
Exocrine pancreatic defects
Chronic pancreatitis
Pancreatectomy
Pancreatic neoplasia
Cystic fibrosis
Hemochromatosis
Fibrocalculous pancreatopathy
Endocrinopathies
Growth hormone excess (
Cushing syndrome
Hyperthyroidism
Pheochromocytoma
Glucagonoma
Infections
Cytomegalovirus infection
Coxsackievirus B
Drugs
Glucocorticoids
Thyroid hormone
β-adrenergic agonists
Statins [23]
Pathophysiology
This section does not cite any references or sources. Please help improve this section by adding citations to reliable sources. Unsourced material may be challenged and removed. (November 2009)

The fluctuation of blood sugar (red) and the sugar-lowering hormone insulin (blue) in humans during the course of a day
with three meals - one of the effects of a sugar-rich vs a starch-rich meal is highlighted.
Mechanism of insulin release in normal pancreatic beta cells - insulin production is more or less constant within the beta
cells. Its release is triggered by food, chiefly food containing absorbable glucose.
Insulin is the principal hormone that regulates uptake of glucose from the blood into most cells (primarily
muscle and fat cells, but not central nervous system cells). Therefore, deficiency of insulin or the
insensitivity of its receptors plays a central role in all forms of diabetes mellitus.
Humans are capable of digesting some carbohydrates, in particular those most common in food; starch,
and some disaccharides such as sucrose, are converted within a few hours to simpler forms, most notably
the monosaccharide glucose, the principal carbohydrate energy source used by the body. The rest are
passed on for processing by gut flora largely in the colon. Insulin is released into the blood by beta cells (β-
cells), found in the islets of Langerhans in the pancreas, in response to rising levels of blood glucose,
typically after eating. Insulin is used by about two-thirds of the body's cells to absorb glucose from the blood
for use as fuel, for conversion to other needed molecules, or for storage.
Insulin is also the principal control signal for conversion of glucose to glycogen for internal storage in liver
and muscle cells. Lowered glucose levels result both in the reduced release of insulin from the β-cells and
in the reverse conversion of glycogen to glucose when glucose levels fall. This is mainly controlled by the
hormone glucagon, which acts in the opposite manner to insulin. Glucose thus forcibly produced from
internal liver cell stores (as glycogen) re-enters the bloodstream; muscle cells lack the necessary export
mechanism. Normally, liver cells do this when the level of insulin is low (which normally correlates with low
levels of blood glucose).
Higher insulin levels increase some anabolic ("building up") processes, such as cell growth and
duplication, protein synthesis, and fat storage. Insulin (or its lack) is the principal signal in converting many
of the bidirectional processes of metabolism from a catabolic to an anabolic direction, and vice versa. In
particular, a low insulin level is the trigger for entering or leaving ketosis (the fat-burning metabolic phase).
If the amount of insulin available is insufficient, if cells respond poorly to the effects of insulin (insulin
insensitivity or resistance), or if the insulin itself is defective, then glucose will not have its usual effect, so it
will not be absorbed properly by those body cells that require it, nor will it be stored appropriately in the liver

and muscles. The net effect is persistent high levels of blood glucose, poor protein synthesis, and other
metabolic derangements, such as acidosis.
When the glucose concentration in the blood is raised to about 9-10 mmol/L (except certain conditions,
such as pregnancy), beyond its renal threshold(i.e. when glucose level surpasses the transport
maximum of glucose reabsorption), reabsorption of glucose in the proximal renal tubuli is incomplete, and
part of the glucose remains in the urine (glycosuria). This increases the osmotic pressure of the urine and
inhibits reabsorption of water by the kidney, resulting in increased urine production (polyuria) and increased
fluid loss. Lost blood volume will be replaced osmotically from water held in body cells and other body
compartments, causing dehydration and increased thirst.
Diagnosis
See also: Glycated hemoglobin and Glucose tolerance test
Diabetes diagnostic criteria[24][25] edit
Condition 2 hour glucose Fasting glucose HbA1c
mmol/l(mg/dl) mmol/l(mg/dl) %
Normal <7.8 (<140) <6.1 (<110) <6.0
Impaired fasting glycaemia <7.8 (<140) ≥ 6.1(≥110) & <7.0(<126) 6.0–6.4
Impaired glucose tolerance ≥7.8 (≥140) <7.0 (<126) 6.0–6.4
Diabetes mellitus ≥11.1 (≥200) ≥7.0 (≥126) ≥6.5
Diabetes mellitus is characterized by recurrent or persistent hyperglycemia, and is diagnosed by
demonstrating any one of the following:[11]
Fasting plasma glucose level ≥ 7.0 mmol/l (126 mg/dl)
Plasma glucose ≥ 11.1 mmol/l (200 mg/dL) two hours after a 75 g oral glucose load as in a glucose
tolerance test
Symptoms of hyperglycemia and casual plasma glucose ≥ 11.1 mmol/l (200 mg/dl)

Glycated hemoglobin (Hb A1C) ≥ 6.5%.[26]
A positive result, in the absence of unequivocal hyperglycemia, should be confirmed by a repeat of any of
the above methods on a different day. It is preferable to measure a fasting glucose level because of the
ease of measurement and the considerable time commitment of formal glucose tolerance testing, which
takes two hours to complete and offers no prognostic advantage over the fasting test. [27] According to the
current definition, two fasting glucose measurements above 126 mg/dl (7.0 mmol/l) is considered
diagnostic for diabetes mellitus.
People with fasting glucose levels from 110 to 125 mg/dl (6.1 to 6.9 mmol/l) are considered to
have impaired fasting glucose.[28] Patients with plasma glucose at or above 140 mg/dL (7.8 mmol/L), but not
over 200 mg/dL (11.1 mmol/L), two hours after a 75 g oral glucose load are considered to have impaired
glucose tolerance. Of these two prediabetic states, the latter in particular is a major risk factor for
progression to full-blown diabetes mellitus, as well as cardiovascular disease.[29]
Glycated hemoglobin is better than fasting glucose for determining risks of cardiovascular disease and
death from any cause.[30]
Management
Main article: Diabetes management
Diabetes mellitus is a chronic disease, for which there is no known cure except in very specific situations.
Management concentrates on keeping blood sugar levels as close to normal ("euglycemia") as possible,
without causing hypoglycemia. This can usually be accomplished with diet, exercise, and use of
appropriate medications (insulin in the case of type 1 diabetes; oral medications, as well as possibly insulin,
in type 2 diabetes).
Patient education, understanding, and participation is vital, since the complications of diabetes are far less
common and less severe in people who have well-managed blood sugar levels.[31][32]The goal of treatment
is an HbA1C level of 6.5%, but should not be lower than that, and may be set higher. [33] Attention is also
paid to other health problems that may accelerate the deleterious effects of diabetes. These
include smoking, elevated cholesterol levels, obesity, high blood pressure, and lack of regular exercise.[33] Specialised footwear is widely used to reduce the risk of ulceration, or re-ulceration, in at-risk diabetic
feet. Evidence for the efficacy of this remains equivocal, however.[34]
LifestyleSee also: Diabetic diet
There are roles for patient education, dietetic support, and sensible exercise, with the goal of keeping both
short-term and long-term blood glucose levels within acceptable bounds. In addition, given the associated
higher risks of cardiovascular disease, lifestyle modifications are recommended to control blood pressure.[35]

MedicationsSee also: Anti-diabetic medication
Metformin is generally recommended as a first line treatment for type 2 diabetes, as there is good evidence
that it decreases mortality.[36] Routine use of aspirin, however, has not been found to improve outcomes in
uncomplicated diabetes.[37]
Type 1 diabetes is typically treated with a combinations of regular and NPH insulin, or synthetic insulin
analogs. When insulin is used in type 2 diabetes, a long-acting formulation is usually added initially, while
continuing oral medications.[36] Doses of insulin are then increased to effect.[36]
Support
In countries using a general practitioner system, such as the United Kingdom, care may take place mainly
outside hospitals, with hospital-based specialist care used only in case of complications, difficult blood
sugar control, or research projects. In other circumstances, general practitioners and specialists share care
of a patient in a team approach. Home telehealth support can be an effective management technique.[38]
Epidemiology
Main article: Epidemiology of diabetes mellitus
Prevalence of diabetes worldwide in 2000 (per 1,000 inhabitants) - world average was 2.8%.
no data
≤ 7.5
7.5–15
15–22.5
22.5–30
30–37.5
37.5–45
45–52.5
52.5–60
60–67.5
67.5–75
75–82.5
≥ 82.5

Disability-adjusted life year for diabetes mellitus per 100,000 inhabitants in 2004
No data
<100
100–200
200–300
300–400
400–500
500–600
600–700
700–800
800–900
900–1,000
1,000–1,500
>1,500
Globally, as of 2010, an estimated 285 million people had diabetes, with type 2 making up about 90% of
the cases.[4] Its incidence is increasing rapidly, and by 2030, this number is estimated to almost double.[39] Diabetes mellitus occurs throughout the world, but is more common (especially type 2) in the more
developed countries. The greatest increase in prevalence is, however, expected to occur in Asia and
Africa, where most patients will probably be found by 2030.[39] The increase in incidence in developing
countries follows the trend of urbanization and lifestyle changes, perhaps most importantly a "Western-
style" diet. This has suggested an environmental (i.e., dietary) effect, but there is little understanding of the
mechanism(s) at present, though there is much speculation, some of it most compellingly presented. [39]
History
Main article: History of diabetes
Diabetes was one of the first diseases described,[40] with an Egyptian manuscript
from c. 1500 BCE mentioning "too great emptying of the urine".[41]The first described cases are believed to
be of type 1 diabetes.[41] Indian physicians around the same time identified the disease and classified it
asmadhumeha or "honey urine", noting the urine would attract ants.[41] The term "diabetes" or "to pass
through" was first used in 230 BCE by the GreekAppollonius of Memphis.[41] The disease was considered
rare during the time of the Roman empire, with Galen commenting he had only seen two cases during his
career.[41] This is possibly due the diet and life-style of the ancient people, or because the clinical symptoms
were observed during the advanced stage of the disease. Galen named the disease "diarrhea of the urine"
(diarrhea urinosa). The earliest surviving work with a detailed reference to diabetes is that of Aretaeus of
Cappadocia (2nd or early 3rd century CE). He described the symptoms and the course of the disease,

which he attributed to the moisture and coldness, reflecting the beliefs of the "Pneumatic School". He
hypothesized a correlation of diabetes with other diseases and he discussed differential diagnosis from the
snakebite which also provokes excessive thirst. His work remained unknown in the West until the middle of
the 16th century when, in 1552, the first Latin edition was published in Venice.[42]
Type 1 and type 2 diabetes were identified as separate conditions for the first time by the Indian physicians
Sushruta and Charaka in 400-500 CE with type 1 associated with youth and type 2 with being overweight.[41] The term "mellitus" or "from honey" was added by the Briton John Rolle in the late 1700s to separate the
condition from diabetes insipidus, which is also associated with frequent urination.[41] Effective treatment
was not developed until the early part of the 20th century, when Canadians Frederick Banting and Charles
Herbert Best isolated and purified insulin in 1921 and 1922.[41] This was followed by the development of the
long-acting insulin NPH in the 1940s.[41]
Etymology
The word diabetes (/ ̩ d aɪ . ə ̍ b i ː t i ː z / or / ̩ d aɪ . ə ̍ b i ː t ɨ s / ) comes from Latin diabētēs, which in turn comes
from Ancient Greek διαβήτης (diabētēs) which literally means "a passer through; a siphon."[43] Ancient
Greek physician Aretaeus of Cappadocia (fl. 1st century CE) used that word, with the intended meaning
"excessive discharge of urine", as the name for the disease.[44][45] Ultimately, the word comes from Greek
διαβαίνειν (diabainein), meaning "to pass through,"[43] which is composed of δια- (dia-), meaning "through"
and βαίνειν (bainein), meaning "to go".[44] The word "diabetes" is first recorded in English, in the
form diabete, in a medical text written around 1425.
The word mellitus (/ m ɨ ̍ l aɪ t ə s / or / ̍ m ɛ l ɨ t ə s / ) comes from the classical Latin word mellītus, meaning
"mellite"[46] (i.e. sweetened with honey;[46] honey-sweet[47]). The Latin word comes from mell-, which comes
from mel, meaning "honey";[46][47] sweetness;[47] pleasant thing,[47] and the suffix -ītus,[46] whose meaning is
the same as that of the English suffix "-ite".[48] It was Thomas Willis who in 1675 added "mellitus" to the
word "diabetes" as a designation for the disease, when he noticed the urine of a diabetic had a sweet taste
(glycosuria).[45] This sweet taste had been noticed in urine by the ancient Greeks, Chinese, Egyptians,
Indians, and Persians.
Society and culture
Further information: List of films featuring diabetes
The 1989 "St. Vincent Declaration"[49][50] was the result of international efforts to improve the care accorded
to those with diabetes. Doing so is important not only in terms of quality of life and life expectancy, but also
economically—expenses due to diabetes have been shown to be a major drain on health—and
productivity-related resources for healthcare systems and governments.
Several countries established more and less successful national diabetes programmes to improve
treatment of the disease.[51]

Diabetic patients with neuropathic symptoms such as numbness or tingling in feet or hands are twice as
likely to be unemployed as those without the symptoms.[52]
In 2010, diabetes-related emergency department (ED) visit rates in the United States were higher among
patients from the lowest income communities (526 per 10,000 population) than from the highest income
communities (236 per 10,000 population). Approximately 9.4% of diabetes-related ED visits were for the
uninsured.[53]
Other animals
Main articles: Diabetes in dogs and Diabetes in cats
In animals, diabetes is most commonly encountered in dogs and cats. Middle-aged animals are most
commonly affected. Female dogs are twice as likely to be affected as males, while according to some
sources, male cats are also more prone than females. In both species, all breeds may be affected, but
some small dog breeds are particularly likely to develop diabetes, such asMiniature Poodles.[54] The
symptoms may relate to fluid loss and polyuria, but the course may also be insidious. Diabetic animals are
more prone to infections. The long-term complications recognised in humans are much rarer in animals.
The principles of treatment (weight loss, oral antidiabetics, subcutaneous insulin) and management of
emergencies (e.g. ketoacidosis) are similar to those in humans.[54]
Conn's syndromeFrom Wikipedia, the free encyclopedia
Main article: Primary aldosteronism
Conn syndrome
Classification and external resources
Aldosterone

ICD-10 E 26.0
ICD-9 255.12
DiseasesDB 3073
MeSH D006929
Conn syndrome is an aldosterone-producing adenoma. Conn's syndrome is named after Jerome W.
Conn (1907–1994), the American endocrinologistwho first described the condition at the University of
Michigan in 1955.[1]
Contents
[hide]
1 Causes
2 Pathogenesis
3 Diagnosis
4 Differential diagnosis
5 Therapy
6 Prognosis
7 See also
8 References
Causes[edit]
Primary hyperaldosteronism has many causes, including adrenal hyperplasia and adrenal carcinoma.[2]
The syndrome is due to:
Bilateral (micronodular) adrenal hyperplasia, 40%
Adrenal (Conn) adenoma, 60%
Glucocorticoid-remediable hyperaldosteronism (dexamethasone-suppressible hyperaldosteronism),
<1%
rare forms, including disorders of the renin-angiotensin system, <1%[3]
Pathogenesis[edit]
Aldosterone has effects on most or all cells of the body but, clinically, the most important actions are on
cells of the late distal tubule and medullary collecting duct. In the principal cells aldosterone increases
activity of basolateral membrane sodium-potassium ATPase and apical epithelial sodium channels, ENaC,
as well as potassium channels, ROMK. These actions increase sodium reabsorption and potassium

secretion. Since more sodium is reabsorbed than potassium secreted, it also makes the lumen more
electrically negative, causing chloride to follow sodium. Water then follows sodium and chloride by
osmosis. In Conn syndrome, these actions cause increased extracellular sodium and fluid volume and
reduced extracellular potassium. Aldosterone also acts on intercalated cells to stimulate an apical proton
ATPase, acidifying urine and alkalizing extracellular fluid.
Finer notes on aldosterone include the fact that it stimulates sodium-potassium ATPase in muscle cells,
increasing intracellular potassium and also increases sodium reabsoption all along the intestine and
nephron, possibly due to widespread stimulation of sodium-potassium ATPase. Finally, epithelial cells of
sweat gland ducts and distal colon surface respond exactly the same as the principal cells of the nephron.
These responses are important in climate adaptation and as a cause of constipation with elevated
aldosterone.
The high pH of the blood makes calcium less available to the tissues and causes symptoms
of hypocalcemia (low calcium levels).
The sodium retention leads to plasma volume expansion and elevated blood pressure. The increased
blood pressure will lead to an increased glomerular filtration rate and cause a decrease inrenin release
from the granular cells of the juxtaglomerular apparatus in the kidney. If a patient is thought to suffer from
primary hyperaldosteronism, the aldosterone:renin activity ratio is used to assess this. The decreased renin
levels and in turn the reactive down-regulation of angiotensin II are thought to be unable to down-regulate
the constitutively formed aldosterone, thus leading to an elevated [plasma aldosterone:plasma renin
activity] ratio (lending the assay to be a clinical tool for diagnostic purposes).
Aside from hypertension, other manifesting problems include myalgias, weakness, and chronic headaches.
The muscle cramps are due to neuron hyperexcitability seen in the setting of hypocalcemia, muscle
weakness secondary to hypoexcitability of skeletal muscles in the setting of low blood potassium
(hypokalemia), and headaches which are thought to be due to both electrolyte imbalance (hypokalemia)
and hypertension.
Secondary hyperaldosteronism is often related to decreased cardiac output, which is associated with
elevated renin levels.
Diagnosis[edit]
Measuring aldosterone alone is not considered adequate to diagnose primary hyperaldosteronism. The
screening test of choice for diagnosis is the plasma aldosterone:plasma renin activity ratio. Renin activity,
not simply plasma renin level, is assayed. Both aldosterone and renin are measured, and a ratio greater
than 30 is indicative of primary hyperaldosteronism.[4][5]

Differential diagnosis[edit]
Hyperaldosteronism can be mimicked by Liddle syndrome, and by ingestion of liquorice and other foods
containing glycyrrhizin. In one case report, hypertension and quadriparesis resulted fromintoxication with a
nonalcoholic pastis (an anise-flavored aperitif containing glycyrrhizinic acid).[6]
Therapy[edit]
In patients with a single benign tumor (adenoma), surgical removal (adrenalectomy) may be curative. This
is usually performed laparoscopically, through several very small incisions. For patients with hyperplasia of
both glands, successful treatment is often achieved with spironolactone or eplerenone, drugs that block the
effect of aldosterone. In males, one common side effect of spironolactone drug therapy sometimes seen
is gynecomastia. Gynecomastia usually does not occur with eplerenone drug therapy. Additionally, a 2008
study conducted in Germany and Argentina proves that the endocannabinoid receptors regulate
aldosterone at the level of the adrenal.[7] Anandamide inhibited basal release and stimulated release of the
adrenocortical steroids corticosterone and aldosterone. Since cannabinoid receptors are affected by the
active ingredient in marijuana, THC, the same way as anandamide, aldosterone would be lowered by this
therapy, according to the conclusions presented in this study.
Prognosis[edit]
In the absence of proper treatment, individuals with hyperaldosteronism often suffer from poorly controlled
high blood pressure, which may be associated with increased rates of stroke, heart disease, and kidney
failure. With appropriate treatment, the prognosis is excellent.[8]
Cushing's syndromeFrom Wikipedia, the free encyclopedia
Not to be confused with Cushing's triad, a disease state resulting from increased intracranial pressure.
Not to be confused with Cushing's disease.
Cushing's syndrome
Classification and external resources
ICD-10 E 24
ICD-9 255.0
MedlinePlus 000410

eMedicine article/117365
MeSH D003480
Cushing's syndrome describes the signs and symptoms associated with prolonged exposure to
inappropriately high levels of the hormone cortisol. This can be caused by taking glucocorticoid drugs, or
diseases that result in excess cortisol, adrenocorticotropic hormone (ACTH), or CRH levels.[1]
Cushing's disease refers to a pituitary-dependent cause of Cushing's syndrome: a tumor (adenoma) in the
pituitary gland produces large amounts ofACTH, causing the adrenal glands to produce elevated levels of
cortisol. It is the most common non-iatrogenic cause of Cushing's syndrome, responsible for 70% of cases
excluding glucocorticoid related cases.[2][3] An easy way to distinguish Cushing's syndrome from Cushing's
disease is that the measured ACTH levels are lower in the former. The decrease in ACTH is due to
increased negative feedback of cortisol on the hypothalamus and anterior pituitary.
This pathology was described by Harvey Cushing in 1932.[4][5] The syndrome is also called Itsenko-
Cushing syndrome,[6][7] hyperadrenocorticismor hypercorticism.
Cushing's syndrome is not confined to humans and is also a relatively common condition in
domestic dogs and horses. It also occurs in cats, however, rarely.
Contents
[hide]
1 Signs and symptoms
2 Cause
o 2.1 Exogenous vs. endogenous
o 2.2 Pseudo-Cushing's syndrome
3 Epidemiology
4 Pathophysiology
5 Diagnosis
o 5.1 Mnemonic
6 Treatment
7 See also
8 References
9 External links
Signs and symptoms[edit]
Symptoms include rapid weight gain, particularly of the trunk and face with sparing of the limbs (central
obesity). Common signs include the growth of fat pads along the collarbone, on the back of the neck or

"buffalo hump" and on the face "moon facies". Other symptoms include hyperhidrosis (excess
sweating), telangiectasia (dilation of capillaries), thinning of the skin (which causes easy bruising and
dryness, particularly the hands) and other mucous membranes, purple or red striae (the weight gain in
Cushing's syndrome stretches the skin, which is thin and weakened, causing it to hemorrhage) on the
trunk, buttocks, arms, legs or breasts, proximal muscle weakness (hips, shoulders), and hirsutism (facial
male-pattern hair growth), baldness and/or extremely dry and brittle hair. In rare cases, Cushing's can
cause hypocalcemia. The excess cortisol may also affect other endocrine systems and cause, for
example, insomnia, inhibited aromatase, reduced libido,impotence in
men, amenorrhoea/oligomenorrhea and infertility in women due to elevations in androgens. Studies have
also shown that the resultant amenorrhea is due to hypercortisolism, which feeds back onto the
hypothalamus resulting in decreased levels of GnRH release.[8]
Cognitive conditions, including memory and attention dysfunctions, as well as depression are commonly
associated with elevated cortisol[9] and may be early indicators of exogenous or endogenous Cushing's.
Patients frequently suffer various psychological disturbances, ranging
from euphoria to psychosis. Depression and anxiety are also common.[10]
Other striking and distressing skin changes that may appear in Cushing's syndrome include facial acne,
susceptibility to superficial dermatophyte and malassezia infections, and the characteristic purplish,
atrophic striae on the abdomen.[11]:500
Other signs include polyuria (and accompanying polydipsia), persistent hypertension (due to cortisol's
enhancement of epinephrine's vasoconstrictive effect) and insulin resistance (especially common
in ectopic ACTH production), leading to hyperglycemia (high blood sugar) and insulin resistance which can
lead to diabetes mellitus. Insulin resistance is accompanied by skin changes such as acanthosis
nigricans in the axilla and around the neck, as well as skin tags in the axilla. Untreated Cushing's syndrome
can lead to heart disease and increased mortality. Cortisol can also exhibit mineralcorticoid activity in high
concentrations, worsening the hypertension and leading to hypokalemia (common in ectopic ACTH
secretion). Furthermore, excessive cortisol may lead to gastrointestinal disturbances, opportunistic
infections and impaired wound healing related to cortisol's suppression of the immune and inflammatory
responses. Osteoporosis is also an issue in Cushing's syndrome since osteoblast activity is inhibited.
Additionally, Cushing's syndrome may cause sore and aching joints, particularly in the hip, shoulders, and
lower back. Cushing’s syndrome includes all the causes of increased cortisol leading to the diseased state.
Cushing’s disease is a specific type of Cushing’s syndrome caused by a pituitary tumor leading to
excessive production of ACTH (Adrenocorticotropic hormone). Excessive ACTH stimulates the adrenal
cortex to produce high levels of cortisol, producing the disease state. Cushing's disease due to
excess ACTH may also result in hyperpigmentation. This is due to Melanocyte-Stimulating
Hormone production as a byproduct of ACTH synthesis from Pro-opiomelanocortin (POMC). A variant of
Cushing's disease can be casused by ectopic, i.e. extra-pituitary, ACTH production from for example a
small cell lung cancer. When Cushing's syndrome is caused by an increase of cortisol at the level of the

adrenal glands (via an adenoma or hyperplasia), negative feedback ultimately reduces ACTH production in
the pituitary. In these cases, ACTH levels remain low and no hyperpigmentation develops. While all
Cushing’s disease is Cushing’s syndrome, not all Cushing’s syndrome is Cushing’s disease.
In summary:
Rapid weight gain
Moodiness, irritability, or depression
Muscle and bone weakness
Memory and attention dysfunction
Osteoporosis
Diabetes mellitus
Hypertension
Immune suppression
Sleep disturbances
Menstrual disorders such as amenorrhea in women and decreased fertility in men
Hirsutism
Baldness
Hypercholesterolemia
Cause[edit]
There are several possible causes of Cushing's syndrome.
Exogenous vs. endogenous[edit]
The most common cause of Cushing's syndrome is exogenous administration of glucocorticoids prescribed
by a health care practitioner to treat other diseases (called iatrogenic Cushing's syndrome). This can be an
effect of corticosteroid treatment of a variety of disorders such as asthma and rheumatoid arthritis, or
in immunosuppression after an organ transplant. Administration of synthetic ACTH is also possible, but
ACTH is less often prescribed due to cost and lesser utility. Although rare, Cushing's syndrome can also be
due to the use of medroxyprogesterone.[12][13] In this form of Cushing's, the adrenal glands atrophy due to
lack of stimulation by ACTH, since glucocorticoids downregulate production of ACTH. Cushing syndrome in
childhood usually results from use of glucocorticoid medication.[14]
Endogenous Cushing's syndrome results from some derangement of the body's own system of secreting
cortisol. Normally, ACTH is released from the pituitary gland when necessary to stimulate the release of
cortisol from the adrenal glands.
In pituitary Cushing's, a benign pituitary adenoma secretes ACTH. This is also known as Cushing's
disease and is responsible for 70% of endogenous Cushing's syndrome.[3]

In adrenal Cushing's, excess cortisol is produced by adrenal gland tumors, hyperplastic adrenal
glands, or adrenal glands with nodular adrenal hyperplasia.
Tumors outside the normal pituitary-adrenal system can produce ACTH (occasionally with CRH) that
affects the adrenal glands. This etiology is called ectopic or paraneoplastic Cushing's disease and is
seen in diseases like small cell lung cancer.[15]
Finally, rare cases of CRH-secreting tumors (without ACTH secretion) have been reported, which
stimulates pituitary ACTH production.[16][16]
Pseudo-Cushing's syndrome[edit]
Elevated levels of total cortisol can also be due to estrogen found in oral contraceptive pills that contain a
mixture of estrogen and progesterone, leading to Pseudo-Cushing's syndrome. Estrogen can cause an
increase of cortisol-binding globulin and thereby cause the total cortisol level to be elevated. However, the
total free cortisol, which is the active hormone in the body, as measured by a 24 hour urine collection for
urinary free cortisol, is normal.[17]
Epidemiology[edit]
Iatrogenic Cushing's syndrome (caused by treatment with corticosteroids) is the most common form of
Cushing's syndrome. Cushing's disease is rare, a Danish study found an incidence of less than one case
per million people per year.[18] However, asymptomatic microadenomas (less than 10mm in size) of the
pituitary are found in approximately one in six individuals.[19]
Pathophysiology[edit]
The hypothalamus is in the brain and the pituitary gland sits just below it. The paraventricular nucleus
(PVN) of the hypothalamus releases corticotropin-releasing hormone (CRH), which stimulates the pituitary
gland to release adrenocorticotropin (ACTH). ACTH travels via the blood to the adrenal gland, where it
stimulates the release of cortisol. Cortisol is secreted by the cortex of the adrenal gland from a region
called the zona fasciculata in response to ACTH. Elevated levels of cortisol exert negative feedback on the
pituitary, which decreases the amount of ACTH released from the pituitary gland.
Strictly, Cushing's syndrome refers to excess cortisol of any etiology (as Syndrome means a group of
symptoms). One of the causes of Cushing's syndrome is a cortisol secreting adenoma in the cortex of the
adrenal gland (primary hypercortisolism/hypercorticism). The adenoma causes cortisol levels in the blood
to be very high, and negative feedback on the pituitary from the high cortisol levels causes ACTH levels to
be very low.
On the other hand, Cushing's disease refers only to hypercortisolism secondary to excess production of
ACTH from a corticotroph pituitary adenoma (secondary hypercortisolism/hypercorticism) or due to excess
production of hypothalamus CRH (Corticotropin releasing hormone)
(tertiary hypercortisolism/hypercorticism). This causes the blood ACTH levels to be elevated along with

cortisol from the adrenal gland. The ACTH levels remain high because the tumor is unresponsive to
negative feedback from high cortisol levels.
Cushing's disease is not to be confused with Ectopic Cushing syndrome [20] (a.k.a. Ectopic ACTH
syndrome), which is often seen in Paraneoplastic syndrome. See its ICD-10 classification.
Cushing's Syndrome was also the first autoimmune disease identified in humans. [21]
Diagnosis[edit]
When Cushing's syndrome is suspected, either a dexamethasone suppression test (administration of
dexamethasone and frequent determination of cortisol and ACTH level), or a 24-hour urinary measurement
for cortisol offer equal detection rates.[22] Dexamethasone is a glucocorticoid and simulates the effects of
cortisol, including negative feedback on the pituitary gland. When dexamethasone is administered and a
blood sample is tested, cortisol levels >50nmol/L (1.81 µg/dL) would be indicative of Cushing's syndrome
because there is an ectopic source of cortisol or ACTH (such as adrenal adenoma) that is not inhibited by
the dexamethasone. A novel approach, recently cleared by the US FDA, is sampling cortisol in saliva over
24 hours, which may be equally sensitive, as late night levels of salivary cortisol are high in Cushingoid
patients. Other pituitary hormone levels may need to be ascertained. Performing a physical examination to
determine any visual field defect may be necessary if a pituitary lesion is suspected, which may compress
the optic chiasm causing typical bitemporal hemianopia.
When any of these tests are positive, CT scanning of the adrenal gland and MRI of the pituitary gland are
performed to detect the presence of any adrenal or pituitary adenomas or incidentalomas(the incidental
discovery of harmless lesions). Scintigraphy of the adrenal gland with iodocholesterol scan is occasionally
necessary. Very rarely, determining the ACTH levels in various veins in the body by venous catheterization,
working towards the pituitary (petrosal sinus sampling) is necessary.
Plasma CRH levels are inadequate at diagnosis (with the possible exception of tumors secreting CRH)
because of peripheral dilution and binding to CRHBP.[23]
Mnemonic[edit]
C - Central obesity, Clavical fat pads, Collagen fibre weakness, Comedones (acne)
U - Urinary free cortisol and glucose increase
S - Striae, Suppressed immunity
H - Hypercortisolism, Hypertension, Hyperglycemia, Hypercholesterolemia, Hirsutism, Hypernatremia,
Hypokalemia
I - Iatrogenic (Increased administration of corticosteroids)
N - Noniatrogenic (Neoplasms)
G - Glucose intolerance, Growth retardation

Treatment[edit]
Most Cushing's syndrome cases are caused by corticosteroid medications (iatrogenic), such as those used
for asthma, arthritis, and other inflammatory conditions. Consequently, most patients are effectively treated
by carefully tapering off (and eventually stopping) the medication that causes the symptoms.
If an adrenal adenoma is identified it may be removed by surgery. An ACTH-secreting
corticotrophic pituitary adenoma should be removed after diagnosis. Regardless of the adenoma's location,
most patients will require steroid replacement postoperatively at least in the interim as long-term
suppression of pituitary ACTH and normal adrenal tissue does not recover immediately. Clearly, if both
adrenals are removed, replacement with hydrocortisone or prednisolone is imperative.
In those patients not suitable for or unwilling to undergo surgery, several drugs have been found to inhibit
cortisol synthesis (e.g. ketoconazole, metyrapone) but they are of limited efficacy[citation needed]. Mifepristone is
a powerful glucocorticoid type II receptor antagonist and, since it does not interfere with normal cortisol
homeostatis type I receptor transmission, may be especially useful for treating the cognitive effects of
Cushing's syndrome.[24] However, the medication faces considerable controversy due to its use as
an abortifacient. In February 2012 the FDA approved mifepristone in order to control high blood sugar level
(hyperglycemia) in adult patients who are not candidates for surgery, or who did not respond to prior
surgery, with the warning that mifepristone should never be used by pregnant women. [25]
Removal of the adrenals in the absence of a known tumor is occasionally performed to eliminate the
production of excess cortisol. In some occasions, this removes negative feedback from a previously occult
pituitary adenoma, which starts growing rapidly and produces extreme levels of ACTH, leading to
hyperpigmentation. This clinical situation is known as Nelson's syndrome.[26]
Glucocorticoid remediable aldosteronismFrom Wikipedia, the free encyclopedia
Glucocorticoid remediable aldosteronism
Classification and external resources
ICD-9 255.11
OMIM 103900
Glucocorticoid remediable aldosteronism (GRA), also describable as aldosterone synthase
hyperactivity, is an autosomal dominant disorder in which the increase in aldosterone secretion produced
by ACTH is no longer transient.
It is a cause of primary hyperaldosteronism.[1]

Contents
[hide]
1 Normal Physiology
2 Pathophysiology
3 Symptoms
4 Treatment
5 See also
6 References
Normal Physiology[edit]
Steroidogenesis, showing aldosterone synthase at right.
Main article: Aldosterone synthase
Aldosterone synthase is a steroid hydroxylase cytochrome P450 oxidase enzyme involved in the
generation of aldosterone. It is localized to the mitochondrial inner membrane. The enzyme has steroid 18-
hydroxylase activity to synthesize aldosterone and other steroids. Aldosterone synthase is found within
the zona glomerulosa at the outer edge of the adrenal cortex. Aldosterone synthase normally is not ACTH
sensitive, and only activated by angiotensin II.
Aldosterone causes the tubules of the kidneys to retain sodium and water. This increases the volume of
fluid in the body, and drives up blood pressure.

Steroid hormones are synthesized from cholesterol within the adrenal
cortex. Aldosterone and corticosterone share the first part of their biosynthetic pathway. The last part is
either mediated by the aldosterone synthase (for aldosterone) or by the 11β-
hydroxylase (for corticosterone).
Aldosterone synthesis is stimulated by several factors:
by increase in the plasma concentration of angiotensin III.
by increased plasma angiotensin II, ACTH, or potassium levels.
The ACTH stimulation test is sometimes used to stimulate the production of aldosterone along
with cortisol to determine if primary or secondary adrenal insufficiency is present.
by plasma acidosis.
by the stretch receptors located in the atria of the heart.
by adrenoglomerulotropin, a lipid factor, obtained from pineal extracts. It selectively stimulates
secretion of aldosterone.
The secretion of aldosterone has a diurnal rhythm.
Control of aldosterone release from the adrenal cortex:
The role of the renin-angiotensin system:
Angiotensin is involved in regulating aldosterone and is the core regulator. Angiotensin II acts
synergistically with potassium.
The role of sympathetic nerves:
Aldosterone production is also affected to one extent or another by nervous control which
integrates the inverse of carotid artery pressure, pain, posture, and probably emotion (anxiety,fear,
and hostility)(including surgical stress).
The role of baroreceptors:
Pressure in the carotid artery decreases aldosterone
The role of the juxtaglomerular apparatus
The plasma concentration of potassium:
The amount of aldosterone secreted is a direct function of the serum potassium as probably
determined by sensors in the carotid artery.
The plasma concentration of sodium:
Aldosterone is a function of the inverse of the sodium intake as sensed via osmotic pressure.
Miscellaneous regulation:

ACTH, a pituitary peptide, also has some stimulating effect on aldosterone probably by
stimulating deoxycorticosterone formation which is a precursor of aldosterone.
Aldosterone is increased by blood loss, pregnancy, and possibly by other circumstances such
as physical exertion, endotoxin shock, and burns.
Aldosterone feedback:
Feedback by aldosterone concentration itself is of a non-morphological character (that is, other
than changes in cell number or structure) and is relatively poor, so that electrolyte feedback
predominates in the short term.
Pathophysiology[edit]
The genes encoding aldosterone synthase and 11-hydroxylase are 95% identical and are
close together on chromosome 8. In individuals with GRA, there is unequal crossing over so
that the 5'regulatory region of the 11-hydroxylase gene is fused to the coding region of the
aldosterone synthase.
The product of this hybrid gene is aldosterone synthase that is ACTH-sensitive[2] in the zona
fasciculata of the adrenal gland.[3]
Although in normal subjects, ACTH accelerates the first step of aldosterone
synthesis, ACTH normally has no effect on the activity of aldosterone synthase. However, in
subjects with glucocorticoid-remediable aldosteronism, ACTH increases the activity of
existing aldosterone synthase, resulting in an abnormally high rate of aldosterone synthesis
and hyperaldosteronism.
Symptoms[edit]
Patients with GRA may be asymptomatic, but the following symptoms can be present:
Fatigue
Headache
High blood pressure
Hypokalemia
Intermittent or temporary paralysis
Muscle spasms
Muscle weakness
Numbness
Polyuria
Polydipsia
Tingling
Hypernatraemia

Metabolic alkalosis
Treatment[edit]
In GRA, the hypersecretion of aldosterone and the accompanying hypertension are remedied
when ACTH secretion is suppressed by administering glucocorticoids.
Dexamethasone, spironolactone and eplerenone have been used in treatment.[4]
PheochromocytomaFrom Wikipedia, the free encyclopedia
Pheochromocytoma
Classification and external resources
High magnification micrograph of apheochromocytoma, showing the
nested arrangement of cells (Zellballen) and stippled chromatin. H&E stain.
ICD-10 D 35.0 , C 74.1
ICD-9 227.0, 194.0, 255.6
ICD-O: M 8700/0
OMIM 171300
DiseasesDB 9912
MedlinePlus 000340
eMedicine med/1816 radio/552 ped/1788
MeSH D010673

This article needs additional citations for verification. Please help improve this article by adding citations to reliable sources. Unsourced material may be challenged and removed. (August 2011)
A pheochromocytoma (from Greek phaios "dark", chroma "color", kytos "cell", -oma "tumor")
or phaeochromocytoma (PCC) is a neuroendocrine tumor of the medulla of the adrenal
glands (originating in the chromaffin cells), or extra-adrenal chromaffin tissue that failed to involute after
birth[1] and secretes high amounts of catecholamines, mostly norepinephrine, plus epinephrine to a lesser
extent.[2] Extra-adrenal paragangliomas (often described as extra-adrenal pheochromocytomas) are closely
related, though less common, tumors that originate in the ganglia of the sympathetic nervous system and
are named based upon the primary anatomical site of origin.
Contents
[hide]
1 Signs and symptoms
2 Cause
3 Diagnosis
o 3.1 Testing
o 3.2 Tumor location
o 3.3 Differential diagnosis
4 Treatment
5 Complications
6 Epidemiology
7 History
8 References
o 8.1 Additional references
9 External links
Signs and symptoms[edit]
The signs and symptoms of a pheochromocytoma are those of sympathetic nervous system hyperactivity,
including:
Skin sensations
Flank pain
Elevated heart rate

Elevated blood pressure , including paroxysmal (sporadic, episodic) high blood pressure, which
sometimes can be more difficult to detect; another clue to the presence of pheochromocytoma
is orthostatic hypotension (a fall in systolic blood pressure greater than 20 mmHg or a fall in diastolic
blood pressure greater than 10 mmHg upon standing)
Palpitations
Anxiety often resembling that of a panic attack
Diaphoresis (excessive sweating)
Headaches – most common symptom
Pallor
Weight loss
Localized amyloid deposits found microscopically
Elevated blood glucose level (due primarily to catecholamine stimulation of lipolysis (breakdown of
stored fat) leading to high levels of free fatty acids and the subsequent inhibition of glucose uptake by
muscle cells. Further, stimulation of beta-adrenergic receptors leads to glycogenolysis and
gluconeogenesis and thus elevation of blood glucose levels).
A pheochromocytoma can also cause resistant arterial hypertension. A pheochromocytoma can be fatal if it
causes malignant hypertension, or severely high blood pressure. This hypertension is not well controlled
with standard blood pressure medications.
Not all patients experience all of the signs and symptoms listed. The most common presentation is
headache, excessive sweating, and increased heart rate, with the attack subsiding in less than one hour.
Tumors may grow very large, but most are smaller than 10 cm.
Cause[edit]
Up to 25% of pheochromocytomas may be familial. Mutations of the genes VHL, RET, NF1 (Gene 17
Neurofibromatosis type 1), SDHB and SDHD are all known to cause familial pheochromocytoma/extra-
adrenal paraganglioma.
Pheochromocytoma is a tumor of the multiple endocrine neoplasia syndrome, type IIA and type IIB (also
known as MEN IIA and MEN IIB, respectively). The other component neoplasms of that syndrome
include parathyroid adenomas, and medullary thyroid cancer. Mutations in the autosomal RET proto-
oncogene drives these malignancies .[3] Common mutations in the RET oncogenemay also account
for medullary sponge kidney as well.[4]
Pheochromocytoma linked to MEN II can be caused by RET oncogene mutations. Both syndromes are
characterized by pheochromocytoma as well as thyroid cancer (thyroid medullary carcinoma). MEN IIA also
presents with hyperparathyroidism, while MEN IIB also presents with mucosal neuroma. It is now
postulated that Abraham Lincoln suffered from MEN IIB, rather thanMarfan's syndrome as previously
thought, though this is uncertain.

Pheochromocytoma is also associated with neurofibromatosis.[5]
Diagnosis[edit]
Histopathology of adrenal pheochromocytoma. Adrenectomy specimen.
Pheochromocytoma (dark circular shadow near body center) localized byMIBG scintigraphy. Front and back views also
show radioiodine collection in thyroid (neck) and bladder (pelvis)
The diagnosis can be established by measuring catecholamines and metanephrines in plasma (blood) or
through a 24-hour urine collection. Care should be taken to rule out other causes of adrenergic (adrenalin-
like) excess like hypoglycemia, stress, exercise, and drugs affecting the catecholamines
like stimulants, methyldopa,dopamine agonists, or ganglion blocking antihypertensives. Various foodstuffs
(e.g. coffee, tea, bananas, chocolate, cocoa, citrus fruits, and vanilla) can also affect the levels of
urinary metanephrine and VMA (vanillylmandelic acid).[6]
Imaging by computed tomography or a T2 weighted MRI of the head, neck, and chest, and abdomen can
help localize the tumor. Tumors can also be located using an MIBG scan, which

is scintigraphy using iodine-123-marked metaiodobenzylguanidine. Even finer localization can be obtained
in certain PET scan centers using PET/CT with F-18-fluorodopamine (FDOPA)[7]
Pheochromocytomas occur most often during young-adult to mid-adult life.
These tumors can form a pattern with other endocrine gland cancers which is labeled multiple endocrine
neoplasia (MEN). Pheochromocytoma may occur in patients with MEN 2 and MEN 3 (MEN 2B). Von Hippel
Lindau patients may also develop these tumors.[8]
Patients experiencing symptoms associated with pheochromocytoma should be aware that it is rare.
However, it often goes undiagnosed until autopsy; therefore patients might wisely choose to take steps to
provide a physician with important clues, such as recording whether blood pressure changes significantly
during episodes of apparent anxiety.
Testing[edit]
Epinephrine
Norepinephrine
Blood tests : Some authorities[weasel words] (Buters et al.) have suggested that analysis of free
metanephrines (normetanephrine and metanephrine) in blood plasma is the most accurate test for
detecting phaeochromocytoma.
Urine tests : Although this test is slightly less effective than plasma testing it is still considered highly
effective in diagnosis. Usually the metabolites
of norepinephrine and epinephrine, normetanephrine (NMN) and metanephrine (MN), are found in
relatively small amounts in normal humans. The increased excretion of these metabolites is indicative
of the disease, but does not completely rule out other diseases which may cause the same excretion
values.
Other Tests:

One diagnostic test used in the past for a pheochromocytoma is to administer clonidine, a
centrally-acting alpha-2 agonist used to treat high blood pressure. Clonidine mimics
catecholamines in the brain, causing it to reduce the activity of the sympathetic nerves
controlling the adrenal medulla. A healthy adrenal medulla will respond to the clonidine
suppression test by reducing catecholamine production; the lack of a response is evidence of
pheochromocytoma.
Chromogranin A is elevated in case of pheochromocytoma.[9]
Another test is for the clinician to press gently on the adrenal gland. A pheochromocytoma will
often release a burst of catecholamines, with the associated signs and symptoms quickly
following. This method is NOT recommended because of possible complications arising from
a potentially massive release of catecholamines.
Micrograph of pheochromocytoma.
Micrograph of pheochromocytoma.
Micrograph of pheochromocytoma.

Bilateral pheochromocytoma inMEN2.
Pheochromocytoma. CT abdomen.
Pheochromocytoma. CT abdomen.
Tumor location[edit]
In adults, approximately 80% of pheochromocytomas are unilateral and solitary, 10% are
bilateral, and 10% are extra-adrenal. In children, a quarter of tumors are bilateral, and an
additional quarter are extra-adrenal. Solitary lesions inexplicably favor the right side. Although
pheochromocytomas may grow to large size (>3 kg), most weigh <100 g and are <10 cm in
diameter. Pheochromocytomas are highly vascular.
The tumors are made up of large, polyhedral, pleomorphic chromaffin cells. Fewer than 10%
of these tumors are malignant. As with several other endocrine tumors, malignancy cannot be
determined from the histologic appearance; tumors that contain large number of aneuploid or
tetraploid cells, as determined by flow cytometry, are more likely to recur. Local invasion of
surrounding tissues or distant metastases indicate malignancy.
Extra-adrenal pheochromocytomas: Extra-adrenal pheochromocytomas usually weigh 20
to 40 g and are <5 cm in diameter. Most are located within the abdomen in association with
the celiac, superior mesenteric, and inferior mesenteric ganglia and the Organ of
Zuckerkandl. Approximately 10% are in the thorax, 1% are within the urinary bladder, and

less than 3% are in the neck, usually in association with the sympathetic ganglia or the
extracranial branches of the ninth cranial nerves.
Differential diagnosis[edit]
The differential diagnoses of pheochromocytoma include:
Anxiety disorders , including Benzodiazepine withdrawal syndrome
Paragangliomas
Von Hippel–Lindau Disease
Essential hypertension
Hyperthyroidism
Insulinoma
Mercury poisoning
Paroxysmal supraventricular tachycardia
Renovascular hypertension
Carcinoid [10]
Treatment[edit]
Surgical resection of the tumor is the treatment of first choice, either by open laparotomy or
else laparoscopy.[11] Given the complexity of perioperative management, and the potential for
catastrophic intra and postoperative complications, such surgery should be performed only at
centers experienced in the management of this disorder. In addition to the surgical expertise
that such centers can provide, they will also have the necessary endocrine and anesthesia
resources. It may also be necessary to carry out adrenalectomy, a complete surgical removal
of the affected adrenal gland(s).
Either surgical option requires prior treatment with the non-specific and irreversible alpha
adrenoceptor blocker Phenoxybenzamine or a short acting alpha antagonist
(e.g. prazosin, terazosin, ordoxazosin).[12] Doing so permits the surgery to proceed while
minimizing the likelihood of severe intraoperative hypertension (as might occur when the
tumor is manipulated). Some authorities would recommend that a combined alpha/beta
blocker such as labetalol also be given in order to slow the heart rate. Regardless, a "pure"
beta blocker such as atenolol must never be used in the presence of a pheochromocytoma
due to the risk of such a treatment leading to unopposed alpha agonism and, thus, severe
and potentially refractory hypertension.
The patient with pheochromocytoma is invariably volume depleted. In other words, the
chronically elevated adrenergic state characteristic of an untreated pheochromocytoma leads
to near-total inhibition of renin-angiotensin activity, resulting in excessive fluid loss in the urine
and thus reduced blood volume. Hence, once the pheochromocytoma has been resected,

thereby removing the major source of circulating catecholamines, a situation arises where
there is both very low sympathetic activity and volume depletion. This can result in
profound hypotension. Therefore, it is usually advised to "salt load" pheochromocytoma
patients before their surgery. This may consist of simple interventions such as consumption
of high salt food pre-operatively, direct salt replacement or through the administration of
intravenous saline solution.
Complications[edit]
The massive release of catecholamines in pheochromocytoma can cause damage to cardiac
cells (myocytes).[13] This damage may be due to either compromising the coronary
microcirculation or by direct toxic effects on the heart cells.[13]
Epidemiology[edit]
Pheochromocytoma is seen in between 2–8 in 1,000,000, with approximately 1000 cases
diagnosed in United States yearly. It mostly occurs in young or middle age adults, though
presents earlier in hereditary cases and it is also called 10% tumor .
About 10% of adrenal cases are bilateral (suggesting hereditary disease)
About 10% of adrenal cases occur in children (also suggesting hereditary disease)
About 15% are extra-adrenal (located in any orthosympathetic tissue): of these 9% are in
the abdomen and 1% are located elsewhere. Some extra-adrenal pheochromocytomas
are probably actually paragangliomas, but the distinction is only possible after surgical
resection.
About 11.1% of adrenal cases are malignant, but this rises to 30% for extra-adrenal
cases
About 15-20% are hereditary[14]
About 5% are caused by VHL disease
About 3% recur after being resected
About 14% of affected individuals do not have arterial hypertension (Campbell's Urology)
History[edit]
In 1886, Felix Fränkel made the first description of a patient with pheochromocytoma. The
term "pheochromocytoma" was first coined by Ludwig Pick, a pathologist, in 1912. In
1926, César Roux(in Switzerland) and Charles Horace Mayo (in the U.S.A.) were the first
surgeons to successfully remove pheochromocytomas.
In the 1970s, Greene and Tischler derived a line of cells, called the PC12 cell line, from a rat
pheochromocytoma.[15]

Congenital adrenal hyperplasiaFrom Wikipedia, the free encyclopedia
"Adrenal hyperplasia" redirects here. You may also be interested in Primary aldosteronism or Cushing's
syndrome.
Congenital adrenal hyperplasia
Classification and external resources
ICD-10 E 25.0
ICD-9 255.2
OMIM 201910 201710 202110 201810 202010
DiseasesDB 1854 1832 4 1841 2565
MedlinePlus 000411
eMedicine ped/48
MeSH D000312
Congenital adrenal hyperplasia (CAH) refers to any of several autosomal recessive diseases resulting
from mutations of genes for enzymesmediating the biochemical steps of production
of cortisol from cholesterol by the adrenal glands (steroidogenesis).[1]
Most of these conditions involve excessive or deficient production of sex steroids and can alter
development of primary or secondary sex characteristics in some affected infants, children, or adults.[2]
Contents
[hide]
1 Signs and symptoms
2 Genetics
o 2.1 Penetrance
3 Diagnosis
o 3.1 Clinical Evaluation
o 3.2 Laboratory Studies

o 3.3 Classification
4 Screening
5 Treatment
6 Epidemiology
7 History
o 7.1 Before 20th century
o 7.2 20th and 21st century
8 See also
9 References
10 External links
Signs and symptoms[edit]
The symptoms of CAH vary depending upon the form of CAH and the sex of the patient. Symptoms can
include:
Due to inadequate mineralocorticoids:
vomiting due to salt-wasting leading to dehydration and death
Due to excess androgens:
functional and average sized penis in cases involving extreme virilization (but no sperm)
ambiguous genitalia , in some females, such that it can be initially difficult to determine sex
early pubic hair and rapid growth in childhood
precocious puberty or failure of puberty to occur (sexual infantilism: absent or delayed puberty)
excessive facial hair , virilization, and/or menstrual irregularity in adolescence
infertility due to anovulation
enlarged clitoris and shallow vagina [3]
Genetics[edit]
The gene for 21-hydroxylase is found on 6p21.3 as part of the HLA complex. 21-hydroxylase deficiency
results in a unique mutation with two highly homologous near-copies in series consisting of an active gene
(CYP21A) and an inactive pseudogene (CYP21P). Mutant alleles result from recombination between the
active and pseudo genes (gene conversion).[4]
Penetrance[edit]
Further variability is introduced by the degree of enzyme inefficiency produced by the specific alleles each
patient has. Some alleles result in more severe degrees of enzyme inefficiency. In general, severe degrees
of inefficiency produce changes in the fetus and problems in prenatal or perinatal life. Milder degrees of

inefficiency are usually associated with excessive or deficient sex hormone effects in childhood or
adolescence, while the mildest form of CAH interferes with ovulation and fertility in adults.
Diagnosis[edit]
Clinical Evaluation[edit]
Female infants with classic CAH have ambiguous genitalia due to exposure to high concentrations of
androgens in utero. CAH due to 21-hydroxylase deficiency is the most common cause of ambiguous
genitalia in genotypically normal female infants (46XX). Less severely affected females may present with
early pubarche. Young women may present with symptoms of polycystic ovarian syndrome
(oligomenorrhea, polycystic ovaries, hirsutism).
Males with classic CAH generally have no signs of CAH at birth. Some may present with
hyperpigmentation and possible penile enlargement. Age of diagnosis of males with CAH varies and
depends on the severity of aldosterone deficiency. Boys with salt-wasting disease present early with
symptoms of hyponatremia and hypovolemia. Boys with non-salt-wasting disease present later with signs
of virilization.[5]
Laboratory Studies[edit]
In classic 21-hydroxylase deficiency, laboratory studies will show very high concentrations of 17-
hydroxyprogesterone (greater than 242 nmol/L in random blood sample; with the normal being less than 3
nmol/L at 3 days age in a full-term infant). Salt-wasting patients tend to have higher 17-
hydroxyprogesterone levels than non-salt-wasting patients.
False positive results from neonatal screening for CAH may be seen in premature infants. Many screening
programs have specific reference ranges depending of weight and gestational age.
In borderline cases concerning for CAH, a corticotrophin stimulation test may be performed.
Genetic analysis can be helpful to confirm a diagnosis of CAH but it is not necessary if classic clinical and
laboratory findings are present.
Classification[edit]
Cortisol is an adrenal steroid hormone that is required for normal endocrine function. Production begins in
the second month of fetal life. Poor cortisol production is a hallmark of most forms of CAH. Inefficient
cortisol production results in rising levels of ACTH, which in turn induces overgrowth (hyperplasia) and
overactivity of the steroid-producing cells of the adrenal cortex. The defects causing adrenal hyperplasia
are congenital (i.e. present at birth).

Steroidogenesis. The enzymes affected in CAH are represented by one red and four green bars on the top half of the
diagram (for example, "21α-hydroxylase" is visible near the top center. "17α-hydroxylase" and "17,20 lyase" are carried
out by a single enzyme.) Depending upon which enzyme is unavailable, there is a reduced production
of androgens (lower left) ormineralocorticoids (upper right). This in turn can lead to increased production of other
molecules, due to a buildup of precursors.
Cortisol deficiency in CAH is usually partial, and not the most serious problem for an affected person.
Synthesis of cortisol shares steps with synthesis of mineralocorticoids such
as aldosterone, androgens such as testosterone, andestrogens such as estradiol. The resulting excessive
or deficient production of these three classes of hormones produce the most important problems for people
with CAH. Specific enzyme inefficiencies are associated with characteristic patterns of over- or
underproduction of mineralocorticoids or sex steroids.
Common medical
term % OMIM
Enzyme(s)
Locus Substrate(s) Product(s)Mineralocorticoid
sAndrogen
s
21-hydroxylase CAH
90-95%
201910
P450c21 6p21.3
17OH-progesterone→progesterone→
11-deoxycortisolDOC
↓ ↑

11β-hydroxylase CAH
5%202010
P450c11β8q21-22
11-deoxycortisol→DOC→
cortisolcorticosterone
↑ ↑
3β-HSD CAH
very rare
201810
3βHSD II 1p13
pregnenolone→17OH-pregnenolone→DHEA→
progesterone17OH-progesteroneandrostenedione
↓ ↓
17α-hydroxylase CAH
very rare
202110
P450c1710q24.3
pregnenolone→progesterone→17OH-pregnenolone→
17OH-pregnenolone17OH-progesteroneDHEA
↑ ↓
lipoid CAH(20,22-desmolase)
very rare
201710
StARP450scc
8p11.215q23-q24
transport ofcholesterolcholesterol→
into mitochondriapregnenolone
↓ ↓
Since the 1960s most endocrinologists have referred to the forms of CAH by the traditional names in the
left column, which generally correspond to the deficient enzyme activity. As exact structures and genes for
the enzymes were identified in the 1980s, most of the enzymes were found to be cytochrome P450
oxidases and were renamed to reflect this. In some cases, more than one enzyme was found to participate
in a reaction, and in other cases a single enzyme mediated in more than one reaction. There was also
variation in different tissues and mammalian species.
In all its forms, congenital adrenal hyperplasia due to 21-hydroxylase deficiency accounts for about 95% of
diagnosed cases of CAH. Unless another specific enzyme is mentioned, "CAH" in nearly all contexts refers
to 21-hydroxylase deficiency. (The terms "salt-wasting CAH", and "simple virilizing CAH" usually refer to
subtypes of this condition.) CAH due to deficiencies of enzymes other than 21-hydroxylase present many of
the same management challenges as 21-hydroxylase deficiency, but some
involve mineralocorticoid excess or sex steroid deficiency.
Screening[edit]
Currently, in the United States and over 40 other countries, every child born is screened for CAH at birth.
This test will detect elevated levels of 17-hydroxy-progesterone (17-OHP). Detecting high levels of 17-OHP

enables early detection of CAH. Newborns detected early enough can be placed on medication and live a
relatively normal life.
Treatment[edit]
Treatment of all forms of CAH may include any of:
1. supplying enough glucocorticoid to reduce hyperplasia and overproduction
of androgens or mineralocorticoids
2. providing replacement mineralocorticoid and extra salt if the person is deficient
3. providing replacement testosterone or estrogen at puberty if the person is deficient
4. additional treatments to optimize growth by delaying puberty or delaying bone maturation
All of these management issues are discussed in more detail in congenital adrenal hyperplasia due to 21-
hydroxylase deficiency.
Dexamethasone is used as an off-label early pre-natal treatment for the symptoms of CAH in female
fetuses, but it does not treat the underlying congenital disorder. A 2007 Swedish clinical trial found that
treatment may cause cognitive and behavioural defects, but the small number of test subjects means the
study cannot be considered definitive. A 2012 American study found more positive than adverse
outcomes. [6] Administration of pre-natal dexamethasone has been the subject of controversy over issues
of informed consent and because treatment must predate a clinical diagnosis of CAH in the female fetus.[7] Especially because in utero Dexamethasone may cause metabolic problems that are not evident until
later in life.[citation needed]
The treatment has also raised concerns in the LGBT community following an essay posted to the forum of
the Hastings Center, a think tank devoted to bioethics, which quoted published research that suggested
that pre-natal treatment of female fetuses could prevent those fetuses from becoming lesbians after birth,
may make them more likely to engage in "traditionally" female-identified behaviour and careers, and more
interested in bearing and raising children. Citing a known attempt by a man using his knowledge of
the fraternal birth order effect to avoid having a homosexualson by using a surrogate, the essayists
(Professor Alice Dreger of Northwestern University's Feinberg School of Medicine, Professor Ellen Feder of
American University and attorney Anne Tamar-Mattis) suggest that pre-natal "dex" treatments constitute
the first known attempt to use in utero protocols to reduce the incidence of homosexuality and bisexuality in
humans.[8] They find such tampering to be morally objectionable.
Since CAH is a recessive gene, both the mother and father must be recessive carriers of CAH for a child to
have CAH. Due to advances in modern medicine, those couples with the recessive CAH genes have an
option to prevent CAH in their offspring through preimplantation genetic diagnosis (PGD). In PGD, the egg
is fertilized outside the women's body in a petri dish (IVF). On the 3rd day, when the embryo has developed
from one cell to about 4 to 6 cells, one of those cells is removed from the embryo without harming the
embryo. The embryo continues to grow until day 5 when it is either frozen or implanted into the mother.

Meanwhile, the removed cell is analyzed to determine if the embryo has CAH. If the embryo is determined
to have CAH, the parents may make a decision as to whether they wish to have it implanted in the mother
or not.[citation needed]
Meta-analysis of the studies supporting the use of dexamethasone on CAH at-risk fetuses found "less than
one half of one percent of published 'studies' of this intervention were regarded as being of high enough
quality to provide meaningful data for a meta-analysis. Even these four studies were of low quality" ... "in
ways so slipshod as to breach professional standards of medical ethics"[9]and "there were no data on long-
term follow-up of physical and metabolic outcomes in children exposed to dexamethasone". [10]
Epidemiology[edit]
The incidence varies geographically. In the United States, congenital adrenal hyperplasia is particularly
common in Native Americans and Yupic Eskimos (incidence 1/280). Among American Caucasians, the
incidence is approximately 1/15,000.[11]
History[edit]
Before 20th century[edit]
An Italian anatomist, Luigi De Crecchio provided the earliest known description of a case of probable CAH.
I propose in this narrative that it is sometimes extremely difficult and even impossible to determine sex
during life. In one of the anatomical theaters of the hospital..., there arrived toward the end of January a
cadaver which in life was the body of a certain Joseph Marzo... The general physiognomy was decidedly
male in all respects. There were no feminine curves to the body. There was a heavy beard. There was
some delicacy of structure with muscles that were not very well developed... The distribution of pubic
hair was typical of the male. Perhaps the lower extremities were somewhat delicate, resembling the female,
and were covered with hair... The penis was curved posteriorly and measured 6 cm, or with stretching, 10
cm. The corona was 3 cm long and 8 cm in circumference. There was an ample prepuce. There was a first
grade hypospadias... There were two folds of skin coming from the top of the penis and encircling it on
either side. These were somewhat loose and resembled labia majora.
De Crecchio then described the internal organs, which included a normal vagina, uterus, tubes,
and ovaries.
It was of the greatest importance to determine the habits, tendencies, passions, and general character of
this individual... I was determined to get as complete a story as possible, determined to get at the base of
the facts and to avoid undue exaggeration which was rampant in the conversation of many of the people
present at the time of the dissection.

He interviewed many people and satisfied himself that Joseph Marzo "conducted himself within the sexual
area exclusively as a male, "even to the point of contracting the "French disease" on two occasions. The
cause of death was another in a series of episodes of vomiting and diarrhea. [12]
This account was translated by Alfred Bongiovanni from De Crecchio (Sopra un caso di apparenzi virili in
una donna. Morgagni 7:154-188, 1865) in 1963 for an article in the New England Journal of Medicine.
20th and 21st century[edit]
The association of excessive sex steroid effects with diseases of the adrenal cortex have been recognized
for over a century. The term adrenogenital syndrome was applied to both sex-steroid producing tumors and
severe forms of CAH for much of the 20th century, before some of the forms of CAH were understood.
Congenital adrenal hyperplasia, which also dates to the first half of the century, has become the preferred
term to reduce ambiguity and to emphasize the underlying pathophysiology of the disorders.
Much of our modern understanding and treatment of CAH comes from research conducted at Johns
Hopkins Medical School in Baltimore in the middle of the 20th century. Lawson Wilkins, "founder"
of pediatric endocrinology, worked out the apparently paradoxical pathophysiology: that hyperplasia and
overproduction of adrenal androgens resulted from impaired capacity for making cortisol. He reported use
of adrenal cortical extracts to treat children with CAH in 1950. Genital reconstructive surgery was also
pioneered at Hopkins. After application of karyotyping to CAH and other intersex disorders in the
1950s, John Money, JL Hampson, and JG Hampson persuaded both the scientific community and the
public that sex assignment should not be based on any single biological criterion, and gender identity was
largely learned and has no simple relationship with chromosomes or hormones. See Intersex for a fuller
history, including recent controversies over reconstructive surgery.
Hydrocortisone, fludrocortisone, and prednisone were available by the late 1950s. By 1980 all of the
relevant steroids could be measured in blood by reference laboratories for patient care. By 1990 nearly all
specific genes and enzymes had been identified.
However, the last decade has seen a number of new developments, discussed more extensively
in congenital adrenal hyperplasia due to 21-hydroxylase deficiency:
1. debate over the value of genital reconstructive surgery and changing standards
2. debate over sex assignment of severely virilized XX infants
3. new treatments to improve height outcomes
4. newborn screening programs to detect CAH at birth
5. increasing attempts to treat CAH before birth
Adrenocortical carcinomaFrom Wikipedia, the free encyclopedia
Adrenocortical carcinoma

Classification and external resources
Micrograph of an adrenocortical carcinoma (left of image – dark blue) and
the adrenal cortex it arose from (right-top of image – pink/light blue).
Benign adrenal medulla is present (right-middle of image –
gray/blue). H&E stain.
ICD-10 C 74.0
ICD-9 194
ICD-O: M 8370/3
OMIM 202300
MedlinePlus 001663
eMedicine ped/41
MeSH D018268
Adrenocortical carcinoma, also adrenal cortical carcinoma (ACC) and adrenal cortex cancer, is an
aggressive cancer originating in the cortex(steroid hormone-producing tissue) of the adrenal gland. Adrenocortical
carcinoma is a rare tumor, with incidence of 1–2 per million population annually.[1][2] Adrenocortical carcinoma has a
bimodal distribution by age, with cases clustering in children under 5, and in adults 30–40 years old.[1]Adrenocortical
carcinoma is remarkable for the many hormonal syndromes which can occur in patients with steroid hormone-
producing ("functional") tumors, including Cushing's syndrome, Conn syndrome, virilization, and feminization.
Adrenocortical carcinoma has often invaded nearby tissues ormetastasized to distant organs at the time of diagnosis,
and the overall 5-year survival rate is only 20–35%.[1]

Contents
[hide]
1 Signs and symptoms
2 Pathophysiology
3 Diagnosis
o 3.1 Laboratory findings
o 3.2 Radiology
o 3.3 Pathology
o 3.4 Differential Diagnosis
4 Treatment
5 Prognosis
6 References
7 External links
Signs and symptoms[edit]
Adrenocortical carcinoma may present differently in children and adults. Most tumors in children are functional,
and virilization is by far the most common presenting symptom, followed by Cushing's syndrome and precocious
puberty.[1] Among adults presenting with hormonal syndromes, Cushing's syndrome alone is most common, followed
by mixed Cushing's and virilization (glucocorticoid and androgen overproduction). Feminization and Conn
syndrome (mineralocorticoidexcess) occur in less than 10% of cases. Rarely, pheochromocytoma-like hypersecretion
of catecholamines has been reported in adrenocortical cancers.[3] Non-functional tumors (about 40%, authorities vary)
usually present with abdominal or flank pain, or they may be asymptomatic and detected incidentally.[2]
All patients with suspected adrenocortical carcinoma should be carefully evaluated for signs and symptoms of
hormonal syndromes. For Cushing's syndrome (glucocorticoid excess) these includeweight gain, muscle wasting,
purple lines on the abdomen, a fatty "buffalo hump" on the neck, a "moonlike" face, and thinning, fragile skin.
Virilism (androgen excess) is most obvious in women, and may produce excess facial and body hair, acne,
enlargement of the clitoris, deepening of the voice, coarsening of facial features, cessation of menstruation. Conn
syndrome (mineralcorticoidexcess) is marked by high blood pressure which can result
in headache and hypokalemia (low serum potassium, which can in turn produce muscle weakness, confusion,
and palpitations) low plasma renin activity, and high serum aldosterone. Feminization (estrogen excess) is most
readily noted in men, and includes breast enlargement, decreased libido and impotence.[1][2][4]
Pathophysiology[edit]
The main etiologic factor of adrenocortical cancer is unknown. Families with Li–Fraumeni syndrome have increased
risk. The p53, retinoblastoma protein (RB) tumor suppressor genes located on chromosomes 17p, 13q respectively,
may be changed. The genes h19, insulin-like growth factor II (IGF-II), p57kip2 are important for fetal growth and
development. They are located on chromosome 11p. Expression of the h19 gene is markedly reduced in both

nonfunctioning and functioning adrenal cortical carcinomas, especially in tumors producing cortisol and aldosterone.
There is also a loss of activity of the p57kip2 gene product in virilizing adenomas and adrenal cortical carcinomas. In
contrast, IGF-II gene expression has been shown to be high in adrenal cortical carcinomas. Finally, c-myc gene
expression is relatively high in neoplasms, and it is often linked to poor prognosis.[5]
Diagnosis[edit]
Laboratory findings[edit]
Hormonal syndromes should be confirmed with laboratory testing. Laboratory findings in Cushing syndrome include
increased serum glucose (blood sugar) and increased urine cortisol. Adrenal virilism is confirmed by the finding of an
excess of serum androstenedione and dehydroepiandrosterone. Findings in Conn syndrome include low serum
potassium, low plasma renin activity, and high serum aldosterone. Feminization is confirmed with the finding of
excess serum estrogen
Radiology[edit]
Radiological studies of the abdomen, such as CT scans and magnetic resonance imaging are useful for identifying the
site of the tumor, differentiating it from other diseases, such asadrenocortical adenoma, and determining the extent of
invasion of the tumor into surrounding organs and tissues. CT scans of the chest and bone scans are routinely
performed to look formetastases to the lungs and bones respectively. These studies are critical in determining whether
or not the tumor can be surgically removed, the only potential cure at this time.[2]
Pathology[edit]
Gross of a large adrenal cortical carcinoma.

Cell block preparation from a fine-needle aspiration biopsy of a large ACC shows tumor cells with compact, eosinophilic cytoplasm
and a mild degree of nuclear pleomorphism.
Adrenal tumors are often not biopsied prior to surgery, so diagnosis is confirmed on examination of the surgical
specimen by a pathologist. Grossly, adrenocortical carcinomas are often large, with a tan-yellow cut surface, and areas
of hemorrhage and necrosis. On microscopic examination, the tumor usually displays sheets of atypical cells with
some resemblance to the cells of the normal adrenal cortex. The presence of invasion and mitotic activityhelp
differentiate small cancers from adrenocortical adenomas.[3] There are several relatively rare variants of adrenal
cortical carcinoma:
Oncocytic adrenal cortical carcinoma
Myxoid adrenal cortical carcinoma
Carcinosarcoma
Adenosquamous adrenocortical carcinoma
Clear cell adrenal cortical carcinoma
Differential Diagnosis[edit]
Differential diagnosis includes:[citation needed]
Adrenocortical adenoma
Renal cell carcinoma
Adrenal medullary tumors
Hepatocellular carcinoma
Treatment[edit]
The only curative treatment is complete surgical excision of the tumor, which can be performed even in the case of
invasion into large blood vessels, such as the renal vein or inferior vena cava. The 5-year survival rate after successful
surgery is 50–60%, but unfortunately, a large percentage of patients are not surgical candidates. Radiation
therapy and radiofrequency ablation may be used for palliation in patients who are not surgical candidates.[1]
Chemotherapy regimens typically include the drug mitotane, an inhibitor of steroid synthesis which is toxic to cells of
the adrenal cortex,[6] as well as standard cytotoxic drugs. A retrospective analysis showed a survival benefit for
mitotane in addition to surgery when compared to surgery alone.[7]
The two most common regimens are cisplatin, doxorubicin, etoposide + mitotane and streptozotocin + mitotane. It is
unknown which regimen is better. Researchers at Uppsala University Hospital initiated a collaboration between
adrenocortical cancer specialists in Europe, USA and Australia, to conduct the first ever randomized controlled trial in
adrenocortical cancer (FIRM-ACT study [8] ), comparing these two regimens.

Prognosis[edit]
ACC, generally, carries a poor prognosis[9] and is unlike most tumours of the adrenal cortex, which
are benign (adenomas) and only occasionally cause Cushing's syndrome. Five-year disease-free survival for a
complete resection of a stage I–III ACC is approximately 30%.[9]
The most important prognostic factors are age of the patient and stage of the tumor. Poor prognostic factors: mitotic
activity, venous invasion, weight of 50g+; diameter of 6.5 cm+, Ki-67/MIB1 labeling index of 4%+, p53+.[citation needed]