Endocarditis Caused by Community-Acquired Klebsiella...
5
Korean J Crit Care Med ■ 증 례 ■ 2013 February 28(1):41-45 / http://dx.doi.org/10.4266/kjccm.2013.28.1.41 41 Endocarditis Caused by Community-Acquired Klebsiella pneumoniae Infection A Case Report Ji-Ae Hwang, M.D., Charles Her, M.D. and Yang-Wook Kim, M.D. Department of Medicine and Anesthesiology, Inje University Haeundae Paik Hospital, Busan, Korea In community-acquired Klebsiella pneumoniae infection, pyogenic liver abscess is common as a primary site of infection, particularly in Asia, that can progress to bacteremia. Diabetes mellitus is a usual predisposing factor. Pneumonia as primary site of infection by community-acquired Klebsiella pneumoniae infection is not common but carries a poor outcome. Early administration of appropriate antibiotics is extremely important to avoid the develop- ment of bacteremia and septicemia. An infective endocarditis caused by community-acquired Klebsiella pneumoniae infection is very rare; particularly, such a case of endocarditis in which pneumonia was the primary site of infection has never been reported previously. In this report we described a case of community-acquired Klebsiella pneumoniae infection that started with pneumonia and progressed to bacteremia, leading to endocarditis, liver abscess, and other systemic septic complications. Delayed administration of appropriate antibiotics may have played a role in this case. Key Words: abscess, antibiotics, bacteremia, septic shock. Received on June 20, 2012, Revised on August 31, 2012 (1st), November 26, 2012 (2nd), Accepted on December 3, 2012 Correspondence to: Charles Her, Medical Intensive Care Unit, Inje University Haeundae Paik Hospital, 1435, Jwa-dong, Haeun- dae-gu, Busan 612-030, Korea Tel: 051-797-0461, Fax: 051-797-0499 E-mail: [email protected] In community-acquired Klebsiella pneumoniae infections, pri- mary pyogenic liver abscess is not uncommon, particularly in Asia.[1-3] Bacteremia from this liver abscess has been reported to cause metastatic endophthalmitis or central nervous system infections.[3] In contrary, liver abscess may develop as a meta- static lesion spreaded by bacteremia from other site of com- munity-acquired Klebsiella pneumoniae infections, such as pneumonia. Likewise, this bacteremia could lead to endo- carditis. However, endocarditis associated with community-ac- quired Klebsiella pneumoniae infection is rare. In this report, we present a case of endocarditis in which community-acquired Klebsiella pneumoniae bacteremia involved both mitral and aortic valves. CASE REPORT A 59 year old man was admitted to another hospital be- cause of change in mentality around 11:30 am one day before admission to this hospital. His prodromal symptoms included general weakness and poor oral intake that started several days prior to admission. His medical history included hypertension, insulin-dependent diabetes mellitus, end-stage renal disease for which he had been on hemodialysis for 10 years. Computed tomography of brain taken at 12:42 pm was unremarkable. A plain chest radiography taken at 12:52 pm showed bilateral in- terstitial infiltrates with nodular opacities. Computed tomog- raphy of the abdomen taken at 3:00 pm showed multiple renal cysts, mild intrahepatic bile duct dilatation of liver with multi- ple lesions that were consistent with either cysts or abscess (it was impossible to differentiate one from the other because of poor quality of images), and bilateral lung consolidations. Re- peated chest radiography taken several hours later showed bi- lateral air space consolidations. Intravenous administration of piperacillin-tazobactam was started. The patient was transferred to this hospital on the following day (Table 1). On the day of admission, the patient arrived at 11:00 am in the emergency room of this hospital. The patient's mental state was stuporous. Initial blood pressure was 100/70 mmHg, pulse 97 beats/min, respiration 24 breaths/min, and body temperature 36.8 o C. SpO2 (oxygen saturation by pulse oximetry) was 90%, while he was breathing oxygen mixture via a face mask with an oxygen flow rate of 10 L/min. Heart sounds were regular
Transcript of Endocarditis Caused by Community-Acquired Klebsiella...

Korean J Crit Care Med 증 례2013 February 28(1)41-45 httpdxdoiorg104266kjccm201328141
41
Endocarditis Caused by Community-Acquired Klebsiella pneumoniae Infection
985103 A Case Report 985103Ji-Ae Hwang MD Charles Her MD and Yang-Wook Kim MD
Department of Medicine and Anesthesiology Inje University Haeundae Paik Hospital Busan Korea
In community-acquired Klebsiella pneumoniae infection pyogenic liver abscess is common as a primary site of
infection particularly in Asia that can progress to bacteremia Diabetes mellitus is a usual predisposing factor
Pneumonia as primary site of infection by community-acquired Klebsiella pneumoniae infection is not common but
carries a poor outcome Early administration of appropriate antibiotics is extremely important to avoid the develop-
ment of bacteremia and septicemia An infective endocarditis caused by community-acquired Klebsiella pneumoniae
infection is very rare particularly such a case of endocarditis in which pneumonia was the primary site of infection
has never been reported previously In this report we described a case of community-acquired Klebsiella pneumoniae
infection that started with pneumonia and progressed to bacteremia leading to endocarditis liver abscess and other
systemic septic complications Delayed administration of appropriate antibiotics may have played a role in this case
Key Words abscess antibiotics bacteremia septic shock
Received on June 20 2012 Revised on August 31 2012 (1st) November
26 2012 (2nd) Accepted on December 3 2012
Correspondence to Charles Her Medical Intensive Care Unit Inje
University Haeundae Paik Hospital 1435 Jwa-dong Haeun-
dae-gu Busan 612-030 Korea
Tel 051-797-0461 Fax 051-797-0499
E-mail charles6133msncom
In community-acquired Klebsiella pneumoniae infections pri-
mary pyogenic liver abscess is not uncommon particularly in
Asia[1-3] Bacteremia from this liver abscess has been reported
to cause metastatic endophthalmitis or central nervous system
infections[3] In contrary liver abscess may develop as a meta-
static lesion spreaded by bacteremia from other site of com-
munity-acquired Klebsiella pneumoniae infections such as
pneumonia Likewise this bacteremia could lead to endo-
carditis However endocarditis associated with community-ac-
quired Klebsiella pneumoniae infection is rare In this report
we present a case of endocarditis in which community-acquired
Klebsiella pneumoniae bacteremia involved both mitral and
aortic valves
CASE REPORT
A 59 year old man was admitted to another hospital be-
cause of change in mentality around 1130 am one day before
admission to this hospital His prodromal symptoms included
general weakness and poor oral intake that started several days
prior to admission His medical history included hypertension
insulin-dependent diabetes mellitus end-stage renal disease for
which he had been on hemodialysis for 10 years Computed
tomography of brain taken at 1242 pm was unremarkable A
plain chest radiography taken at 1252 pm showed bilateral in-
terstitial infiltrates with nodular opacities Computed tomog-
raphy of the abdomen taken at 300 pm showed multiple renal
cysts mild intrahepatic bile duct dilatation of liver with multi-
ple lesions that were consistent with either cysts or abscess (it
was impossible to differentiate one from the other because of
poor quality of images) and bilateral lung consolidations Re-
peated chest radiography taken several hours later showed bi-
lateral air space consolidations Intravenous administration of
piperacillin-tazobactam was started The patient was transferred
to this hospital on the following day (Table 1)
On the day of admission the patient arrived at 1100 am in
the emergency room of this hospital The patients mental state
was stuporous Initial blood pressure was 10070 mmHg pulse
97 beatsmin respiration 24 breathsmin and body temperature
368oC SpO2 (oxygen saturation by pulse oximetry) was 90
while he was breathing oxygen mixture via a face mask with
an oxygen flow rate of 10 Lmin Heart sounds were regular
42 한 환자의학회지제 28 권 제 1 호 2013
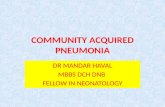
Fig 2 Plain chest radiograph taken on the day of admission to this
hospital showed bilateral air space infiltration
Table 1 Laboratory Data of Blood Analysis
VariableOn presentation
Other Hospital
1st day
This Hospital
2nd day
This Hospital
3rd day
This Hospital
Hematocrit () 294 320 315 237
WBC (per mm3) 10690 22430 26480 21340
Platelets (per mm3) 153000 48000 71000 48000
Total protein (gdl) 58 53 50 48
T Bilirubin (mgdl) 07 08 13 32
ASTa (unitL) 123 225 373 9900
ALTb (unitL) 158 187 250 3077
ALPc (unitL) 341 1250 1115 2379
BUNd (mgdl) 34 608 442 270
Creatinine (mgdl) 446 727 445 281
LDHe (unitL) 251 485 581 7700
Na+ (mEqL) 133 130 135 144
Cl-
(mEqL) 100 95 101 96
K+
(mEqL) 44 45 46 36
Glucose (mgdl) 384 365 152
pH 742 74 726 701 720
PCO2 (mmHg) 28 32 41 35 49
PO2 (mmHg) 58 40 102 129 62
HCO3-
(mEqL) 182 20 187 88 192
CRPf (mgdl) 313 3309 3802
Procalcitonin (ngml) 8019
Lipase (unitL) 116 25
PTINRg (second) 11091 143125 153137
aPTTh (second) 265 491 829
HbA1 Ci () 92
Troponin I (ngml) 003 006
aAspartate aminotransferase
bAlanine aminotransferase
cAlkaline phosphatase
dBlood urea nitrogen
eLactate dehydrogenase
fC-reactive
protein gProthrombin timeinternational neutralization ratio hActivated partial thromboplastin time iGlycated hemoglobin
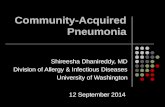
Fig 1 Computed tomography of abdomen taken on the day of
admission to this hospital showed multiple liver abscesses
without murmur There was no sign of infection in the arterio-
venous shunt on his left forearm There was tenderness in
right upper quadrant of abdomen Computed tomography of ab-
domen and pelvis showed multiple liver abscesses (Fig 1) and
right gluteal muscle abscess Chest radiograph showed bilateral
pneumonic consolidation (Fig 2) MRI scan of brain showed
Ji-Ae Hwang et alKlebsiella pneumoniae Endocarditis 43
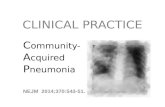
Fig 3 A modified parasternal long axis view of transthoracic
echocardiography showed a large vegetation on the posterior
leaflet (double arrows) and a small vegetation on the aortic
valve (single arrow) LV denotes left ventricle RV right
ventricle AA ascending aorta and LA left atrium
meningitis and multiple small infarctions most likely from sep-
tic embolism Intravenous administration of metronidazole (500
mg every 8 hours) and ceftazidime (2 g) was started SpO2
became 80 and the patients trachea was intubated and he
was placed on mechanical ventilator Intravenous infusions of
dopamine and norepinephrine were started to maintain systolic
blood pressure higher than 100 mmHg (or mean pressure of
65 mmHg) Two large liver abscesses were drained under ul-
trasonographic guidance Vancomycin (1 g) was added The
patient was admitted to ICU Continuous renal replacement
therapy was started
On the second hospital day a severe metabolic acidosis de-
veloped (Table 1) Sodium bicarbonate and fresh frozen plasma
were given A systolic murmur (36) was heard at the left
lower sternum radiating to the left axilla On the third hospital
day a transthoracic echocardiography revealed a large vegeta-
tion involving the posterior mitral leaflet with a moder-
ate-to-severe mitral regurgitation (16times15 cm) and a small veg-
etation (06times045 cm) involving the aortic valve with a moder-
ate regurgitation (Fig 3) There was no evidence of endoph-
thalmitis In the presence of multiple organ dysfunction and
severe septic shock the patients condition was considered too
poor for a surgery for the replacement of cardiac valves to be
done On the fourth hospital day the patient suffered cardiac
arrest and resuscitation was unsuccessful On the following day
the results of culture of liver abscess sputum and blood came
back showing heavy growths of Klebsiella pneumoniae which
was resistant to ampicillin and piperacillin but sensitive to all
other antibiotics
DISCUSSION
Previous studies have identified significant differences be-
tween nosocomial and community-acquired Klebsiella pneumo-
niae infections[12] A primary pyogenic liver abscess develops
almost exclusively in patients with community-acquired in-
fections particularly in Asia Underlying diabetes mellitus was
more common in community-acquired infections
Because of the history of attendance at the hemodialysis
clinic for the regular hemodialysis one may consider this case
in the present report as nosocomial infection However the
presence of underlying diabetes mellitus development of liver
abscess and a low antimicrobial resistance of cultured Kleb-
siella pneumoniae isolates all together support the notion that
the case patient had a community-acquired infection When the
patient was admitted to another hospital the presence of pneu-
monia was apparent by chest radiograph but the presence of
liver abscess was questionable by computed tomography
Moreover despite tremendously elevated inflammatory biomar-
kers such as procalcitonin and C-reactive protein liver en-
zymes were only slightly elevated indicating that systemic in-
flammatory reaction had been activated before the development
of liver abscess In addition upon admission to this hospital a
computed tomography showed multiple liver abscesses which
strongly suggested that the liver abscess in this case was meta-
static rather than primary infection One may argue over the
possibility that the liver abscess was the primary infection site
and the pneumonia was the metastatic infection in this case
However the metastatic lung infection from the liver abscess
is very rare in Korea[4] and is usually presented as septic em-
boli or abscess rather than air space infiltration[5] In addition
primary liver abscess due to Klebsiella pneumoniae infection is
usually not associated with septic shock even with metastatic
infection to lung[4] whereas primary lung infection can be as-
sociated with a much more fulminant course[6] A previous
study has shown that septic shock (51 of cases) and acute
respiratory failure (61 of cases) are initial presentation in
many patients with community-acquired pneumonia due to
Klebsiella pneumoniae and are the independent risk factors for
the mortality[6] Taken together it is most likely that his ful-
minant illness started with pneumonia which was complicated
by septic shock and acute respiratory failure and progressed to
44 한 환자의학회지제 28 권 제 1 호 2013
bacteremia causing liver abscess endocarditis and other sys-
temic septic complications
Several cases of endocarditis that were associated with noso-
comial Klebsiella pneumoniae infections have been reported
previously[7] The urinary tract was the most common source
of bacteremia and the aortic valve was the most commonly
affected But there was no liver abscess in those cases There
is only one case report of infective endocarditis caused by
community-acquired Klebsiella pneumoniae infection Bactere-
mia from the primary liver abscess due to community-acquired
Klebsiella pneumoniae infection has been reported to cause an
infective endocarditis involving mitral valve[8] However the
patient in that previous report[8] initially presented with pneu-
monia which became severe enough to require mechanical
ventilator support Thus it is conceivable that primary infection
site may have been pneumonia rather than liver abscess in that
case considering the fact that none of the previously reported
numerous cases of primary liver abscess caused by commun-
ity-acquired Klebsiella pneumoniae developed endocarditis de-
spite the presence of many other metastatic infections[2-46] It
seems to be that the primary liver abscess is least likely the
source of bacteremia for endocarditis in community-acquired
Klebsiella pneumoniae infection
Many cases of pyogenic liver abscess caused by commun-
ity-acquired Klebsiella pneumoniae infection have been reported
in the United States[910] The isolates mostly were sensitive
to all antibiotics except ampicillin and in most cases piper-
acillin-tazobactam was given empirically as an initial anti-
microbial medication In contrary Klebsiella pneumoniae isolate
in the present case report was resistant to not only ampicillin
but also piperacillin Unfortunately when the patient in the
present report was admitted to another hospital only piper-
acillin-tazobactam was given It has been shown that early
combination antibiotic therapy yields improved survival com-
pared with monotherapy in sepsis particularly when beta-lac-
tams are used[11] Generally two of the guideline-concordant
antimicrobial combinations for severe community-acquired pneu-
monia are either a beta-lactam and fluoroquinolone or beta-lac-
tam and macrolide[12] Interestingly Administration of a mac-
rolide antibiotic within 24 hour upon admission has been
shown to decrease mortality[13] According to a previous
study delay in administration of initial (appropriate) antibiotics
until after the recognition of shock was associated with in-
creased mortality[14] As such a delay in initial appropriate
antibiotics could have contributed to the poor outcome of the
case in the present report While writing this paper there was
another case of community-acquired Klebsiella pneumoniae
causing pneumonia followed by bacteremia and multiple liver
abscesses in our intensive care unit The isolate was also re-
sistant to both ampicillin and piperacillin but sensitive to all
other antibiotics
Klebsiella pneumoniae pyogenic liver abscess is not a dis-
ease limited in Asia but an emerging disease in Europe and
North America[15] Furthermore community-acquired Klebsiella
pneumoniae infection is not limited to Asian who travels to
other continents Previous reports have shown that Caucasian
who have never traveled to Asia get infected with this mi-
crobe causing liver abscess[910] Thus it is not likely that
ethnicity contributes to susceptibility to this organism Anyone
may get this infection particularly if the person has diabetes
mellitus
In summary we described a case of community-acquired
Klebsiella pneumoniae infection that started with pneumonia
and progressed to bacteremia causing liver abscess endocardi-
tis and other systemic septic complications The isolate was
resistant not only to ampicillin and but also piperacillin
REFERENCES
1) Tsay RW Siu LK Fung CP Chang FY Characteristics of
bacteremia between community-acquired and nosocomial
Klebsiella pneumoniae infection risk factor for mortality and
the impact of capsular serotypes as a herald for community-ac-
quired infection Arch Intern Med 2002 162 1021-7
2) Kang CI Kim SH Bang JW Kim HB Kim NJ Kim EC
et al Community-acquired versus nosocomial Klebsiella pneu-
moniae bacteremia clinical features treatment outcomes and
clinical implication of antimicrobial resistance J Korean Med
Sci 2006 21 816-22
3) Fang CT Lai SY Yi WC Hsueh PR Liu KL Chang SC
Klebsiella pneumoniae genotype K1 an emerging pathogen
that causes septic ocular or central nervous system complica-
tions from pyogenic liver abscess Clin Infect Dis 2007 45
284-93
4) Siu LK Yeh KM Lin JC Fung CP Chang FY Klebsiella
pneumoniae liver abscess a new invasive syndrome Lancet
Infect Dis 2012 12 881-7
5) Ko WC Paterson DL Sagnimeni AJ Hansen DS Von
Gottberg A Mohapatra S et al Community-acquired Klebsiel-
la pneumoniae bacteremia global differences in clinical
patterns Emerg Infect Dis 2002 8 160-6
6) Lin YT Jeng YY Chen TL Fung CP Bacteremic commun-
ity-acquired pneumonia due to Klebsiella pneumoniae clinical
and microbiological characteristics in Taiwan 2001-2008
BMC Infect Dis 2010 10 307-7
7) Thomas MG Rowland-Jones S Smyth E Klebsiella pneumo-
Ji-Ae Hwang et alKlebsiella pneumoniae Endocarditis 45
niae endocarditis J R Soc Med 1989 82 114-5
8) Rivero A Gomez E Alland D Huang DB Chiang T K2 se-
rotype Klebsiella pneumoniae causing a liver abscess asso-
ciated with infective endocarditis J Clin Microbiol 2010 48
639-41
9) Lederman ER Crum NF Pyogenic liver abscess with a focus
on Klebsiella pneumoniae as a primary pathogen an emerging
disease with unique clinical characteristics Am J Gastroenterol
2005 100 322-31
10) Fierer J Walls L Chu P Recurring Klebsiella pneumoniae
pyogenic liver abscesses in a resident of San Diego California
due to a K1 strain carrying the virulence plasmid J Clin
Microbiol 2011 49 4371-3
11) Kumar A Zarychanski R Light B Parrillo J Maki D Simon
D et al Cooperative Antimicrobial Therapy of Septic Shock
(CATSS) Database Research Group Early combination anti-
biotic therapy yields improved survival compared with mono-
therapy in septic shock a propensity-matched analysis Crit
Care Med 2010 38 1773-85
12) Wilson BZ Anzueto A Restrepo MI Pugh MJ Mortensen
EM Comparison of two guideline-concordant antimicrobial
combinations in elderly patients hospitalized with severe com-
munity-acquired pneumonia Crit Care Med 2012 40 2310-4
13) Walkey AJ Wiener RS Macrolide antibiotics and survival in
patients with acute lung injury Chest 2012 141 1153-9
14) Puskarich MA Trzeciak S Shapiro NI Arnold RC Horton
JM Studnek JR et al Emergency Medicine Shock Research
Network (EMSHOCKNET) Association between timing of
antibiotic administration and mortality from septic shock in pa-
tients treated with a quantitative resuscitation protocol Crit
Care Med 2011 39 2066-71
15) Turton JF Englender H Gabriel SN Turton SE Kaufmann
ME Pitt TL Genetically similar isolates of Klebsiella pneu-
moniae serotype K1 causing liver abscesses in three
continents J Med Microbiol 2007 56 593-7

42 한 환자의학회지제 28 권 제 1 호 2013
Fig 2 Plain chest radiograph taken on the day of admission to this
hospital showed bilateral air space infiltration
Table 1 Laboratory Data of Blood Analysis
VariableOn presentation
Other Hospital
1st day
This Hospital
2nd day
This Hospital
3rd day
This Hospital
Hematocrit () 294 320 315 237
WBC (per mm3) 10690 22430 26480 21340
Platelets (per mm3) 153000 48000 71000 48000
Total protein (gdl) 58 53 50 48
T Bilirubin (mgdl) 07 08 13 32
ASTa (unitL) 123 225 373 9900
ALTb (unitL) 158 187 250 3077
ALPc (unitL) 341 1250 1115 2379
BUNd (mgdl) 34 608 442 270
Creatinine (mgdl) 446 727 445 281
LDHe (unitL) 251 485 581 7700
Na+ (mEqL) 133 130 135 144
Cl-
(mEqL) 100 95 101 96
K+
(mEqL) 44 45 46 36
Glucose (mgdl) 384 365 152
pH 742 74 726 701 720
PCO2 (mmHg) 28 32 41 35 49
PO2 (mmHg) 58 40 102 129 62
HCO3-
(mEqL) 182 20 187 88 192
CRPf (mgdl) 313 3309 3802
Procalcitonin (ngml) 8019
Lipase (unitL) 116 25
PTINRg (second) 11091 143125 153137
aPTTh (second) 265 491 829
HbA1 Ci () 92
Troponin I (ngml) 003 006
aAspartate aminotransferase
bAlanine aminotransferase
cAlkaline phosphatase
dBlood urea nitrogen
eLactate dehydrogenase
fC-reactive
protein gProthrombin timeinternational neutralization ratio hActivated partial thromboplastin time iGlycated hemoglobin
Fig 1 Computed tomography of abdomen taken on the day of
admission to this hospital showed multiple liver abscesses
without murmur There was no sign of infection in the arterio-
venous shunt on his left forearm There was tenderness in
right upper quadrant of abdomen Computed tomography of ab-
domen and pelvis showed multiple liver abscesses (Fig 1) and
right gluteal muscle abscess Chest radiograph showed bilateral
pneumonic consolidation (Fig 2) MRI scan of brain showed
Ji-Ae Hwang et alKlebsiella pneumoniae Endocarditis 43
Fig 3 A modified parasternal long axis view of transthoracic
echocardiography showed a large vegetation on the posterior
leaflet (double arrows) and a small vegetation on the aortic
valve (single arrow) LV denotes left ventricle RV right
ventricle AA ascending aorta and LA left atrium
meningitis and multiple small infarctions most likely from sep-
tic embolism Intravenous administration of metronidazole (500
mg every 8 hours) and ceftazidime (2 g) was started SpO2
became 80 and the patients trachea was intubated and he
was placed on mechanical ventilator Intravenous infusions of
dopamine and norepinephrine were started to maintain systolic
blood pressure higher than 100 mmHg (or mean pressure of
65 mmHg) Two large liver abscesses were drained under ul-
trasonographic guidance Vancomycin (1 g) was added The
patient was admitted to ICU Continuous renal replacement
therapy was started
On the second hospital day a severe metabolic acidosis de-
veloped (Table 1) Sodium bicarbonate and fresh frozen plasma
were given A systolic murmur (36) was heard at the left
lower sternum radiating to the left axilla On the third hospital
day a transthoracic echocardiography revealed a large vegeta-
tion involving the posterior mitral leaflet with a moder-
ate-to-severe mitral regurgitation (16times15 cm) and a small veg-
etation (06times045 cm) involving the aortic valve with a moder-
ate regurgitation (Fig 3) There was no evidence of endoph-
thalmitis In the presence of multiple organ dysfunction and
severe septic shock the patients condition was considered too
poor for a surgery for the replacement of cardiac valves to be
done On the fourth hospital day the patient suffered cardiac
arrest and resuscitation was unsuccessful On the following day
the results of culture of liver abscess sputum and blood came
back showing heavy growths of Klebsiella pneumoniae which
was resistant to ampicillin and piperacillin but sensitive to all
other antibiotics
DISCUSSION
Previous studies have identified significant differences be-
tween nosocomial and community-acquired Klebsiella pneumo-
niae infections[12] A primary pyogenic liver abscess develops
almost exclusively in patients with community-acquired in-
fections particularly in Asia Underlying diabetes mellitus was
more common in community-acquired infections
Because of the history of attendance at the hemodialysis
clinic for the regular hemodialysis one may consider this case
in the present report as nosocomial infection However the
presence of underlying diabetes mellitus development of liver
abscess and a low antimicrobial resistance of cultured Kleb-
siella pneumoniae isolates all together support the notion that
the case patient had a community-acquired infection When the
patient was admitted to another hospital the presence of pneu-
monia was apparent by chest radiograph but the presence of
liver abscess was questionable by computed tomography
Moreover despite tremendously elevated inflammatory biomar-
kers such as procalcitonin and C-reactive protein liver en-
zymes were only slightly elevated indicating that systemic in-
flammatory reaction had been activated before the development
of liver abscess In addition upon admission to this hospital a
computed tomography showed multiple liver abscesses which
strongly suggested that the liver abscess in this case was meta-
static rather than primary infection One may argue over the
possibility that the liver abscess was the primary infection site
and the pneumonia was the metastatic infection in this case
However the metastatic lung infection from the liver abscess
is very rare in Korea[4] and is usually presented as septic em-
boli or abscess rather than air space infiltration[5] In addition
primary liver abscess due to Klebsiella pneumoniae infection is
usually not associated with septic shock even with metastatic
infection to lung[4] whereas primary lung infection can be as-
sociated with a much more fulminant course[6] A previous
study has shown that septic shock (51 of cases) and acute
respiratory failure (61 of cases) are initial presentation in
many patients with community-acquired pneumonia due to
Klebsiella pneumoniae and are the independent risk factors for
the mortality[6] Taken together it is most likely that his ful-
minant illness started with pneumonia which was complicated
by septic shock and acute respiratory failure and progressed to
44 한 환자의학회지제 28 권 제 1 호 2013
bacteremia causing liver abscess endocarditis and other sys-
temic septic complications
Several cases of endocarditis that were associated with noso-
comial Klebsiella pneumoniae infections have been reported
previously[7] The urinary tract was the most common source
of bacteremia and the aortic valve was the most commonly
affected But there was no liver abscess in those cases There
is only one case report of infective endocarditis caused by
community-acquired Klebsiella pneumoniae infection Bactere-
mia from the primary liver abscess due to community-acquired
Klebsiella pneumoniae infection has been reported to cause an
infective endocarditis involving mitral valve[8] However the
patient in that previous report[8] initially presented with pneu-
monia which became severe enough to require mechanical
ventilator support Thus it is conceivable that primary infection
site may have been pneumonia rather than liver abscess in that
case considering the fact that none of the previously reported
numerous cases of primary liver abscess caused by commun-
ity-acquired Klebsiella pneumoniae developed endocarditis de-
spite the presence of many other metastatic infections[2-46] It
seems to be that the primary liver abscess is least likely the
source of bacteremia for endocarditis in community-acquired
Klebsiella pneumoniae infection
Many cases of pyogenic liver abscess caused by commun-
ity-acquired Klebsiella pneumoniae infection have been reported
in the United States[910] The isolates mostly were sensitive
to all antibiotics except ampicillin and in most cases piper-
acillin-tazobactam was given empirically as an initial anti-
microbial medication In contrary Klebsiella pneumoniae isolate
in the present case report was resistant to not only ampicillin
but also piperacillin Unfortunately when the patient in the
present report was admitted to another hospital only piper-
acillin-tazobactam was given It has been shown that early
combination antibiotic therapy yields improved survival com-
pared with monotherapy in sepsis particularly when beta-lac-
tams are used[11] Generally two of the guideline-concordant
antimicrobial combinations for severe community-acquired pneu-
monia are either a beta-lactam and fluoroquinolone or beta-lac-
tam and macrolide[12] Interestingly Administration of a mac-
rolide antibiotic within 24 hour upon admission has been
shown to decrease mortality[13] According to a previous
study delay in administration of initial (appropriate) antibiotics
until after the recognition of shock was associated with in-
creased mortality[14] As such a delay in initial appropriate
antibiotics could have contributed to the poor outcome of the
case in the present report While writing this paper there was
another case of community-acquired Klebsiella pneumoniae
causing pneumonia followed by bacteremia and multiple liver
abscesses in our intensive care unit The isolate was also re-
sistant to both ampicillin and piperacillin but sensitive to all
other antibiotics
Klebsiella pneumoniae pyogenic liver abscess is not a dis-
ease limited in Asia but an emerging disease in Europe and
North America[15] Furthermore community-acquired Klebsiella
pneumoniae infection is not limited to Asian who travels to
other continents Previous reports have shown that Caucasian
who have never traveled to Asia get infected with this mi-
crobe causing liver abscess[910] Thus it is not likely that
ethnicity contributes to susceptibility to this organism Anyone
may get this infection particularly if the person has diabetes
mellitus
In summary we described a case of community-acquired
Klebsiella pneumoniae infection that started with pneumonia
and progressed to bacteremia causing liver abscess endocardi-
tis and other systemic septic complications The isolate was
resistant not only to ampicillin and but also piperacillin
REFERENCES
1) Tsay RW Siu LK Fung CP Chang FY Characteristics of
bacteremia between community-acquired and nosocomial
Klebsiella pneumoniae infection risk factor for mortality and
the impact of capsular serotypes as a herald for community-ac-
quired infection Arch Intern Med 2002 162 1021-7
2) Kang CI Kim SH Bang JW Kim HB Kim NJ Kim EC
et al Community-acquired versus nosocomial Klebsiella pneu-
moniae bacteremia clinical features treatment outcomes and
clinical implication of antimicrobial resistance J Korean Med
Sci 2006 21 816-22
3) Fang CT Lai SY Yi WC Hsueh PR Liu KL Chang SC
Klebsiella pneumoniae genotype K1 an emerging pathogen
that causes septic ocular or central nervous system complica-
tions from pyogenic liver abscess Clin Infect Dis 2007 45
284-93
4) Siu LK Yeh KM Lin JC Fung CP Chang FY Klebsiella
pneumoniae liver abscess a new invasive syndrome Lancet
Infect Dis 2012 12 881-7
5) Ko WC Paterson DL Sagnimeni AJ Hansen DS Von
Gottberg A Mohapatra S et al Community-acquired Klebsiel-
la pneumoniae bacteremia global differences in clinical
patterns Emerg Infect Dis 2002 8 160-6
6) Lin YT Jeng YY Chen TL Fung CP Bacteremic commun-
ity-acquired pneumonia due to Klebsiella pneumoniae clinical
and microbiological characteristics in Taiwan 2001-2008
BMC Infect Dis 2010 10 307-7
7) Thomas MG Rowland-Jones S Smyth E Klebsiella pneumo-
Ji-Ae Hwang et alKlebsiella pneumoniae Endocarditis 45
niae endocarditis J R Soc Med 1989 82 114-5
8) Rivero A Gomez E Alland D Huang DB Chiang T K2 se-
rotype Klebsiella pneumoniae causing a liver abscess asso-
ciated with infective endocarditis J Clin Microbiol 2010 48
639-41
9) Lederman ER Crum NF Pyogenic liver abscess with a focus
on Klebsiella pneumoniae as a primary pathogen an emerging
disease with unique clinical characteristics Am J Gastroenterol
2005 100 322-31
10) Fierer J Walls L Chu P Recurring Klebsiella pneumoniae
pyogenic liver abscesses in a resident of San Diego California
due to a K1 strain carrying the virulence plasmid J Clin
Microbiol 2011 49 4371-3
11) Kumar A Zarychanski R Light B Parrillo J Maki D Simon
D et al Cooperative Antimicrobial Therapy of Septic Shock
(CATSS) Database Research Group Early combination anti-
biotic therapy yields improved survival compared with mono-
therapy in septic shock a propensity-matched analysis Crit
Care Med 2010 38 1773-85
12) Wilson BZ Anzueto A Restrepo MI Pugh MJ Mortensen
EM Comparison of two guideline-concordant antimicrobial
combinations in elderly patients hospitalized with severe com-
munity-acquired pneumonia Crit Care Med 2012 40 2310-4
13) Walkey AJ Wiener RS Macrolide antibiotics and survival in
patients with acute lung injury Chest 2012 141 1153-9
14) Puskarich MA Trzeciak S Shapiro NI Arnold RC Horton
JM Studnek JR et al Emergency Medicine Shock Research
Network (EMSHOCKNET) Association between timing of
antibiotic administration and mortality from septic shock in pa-
tients treated with a quantitative resuscitation protocol Crit
Care Med 2011 39 2066-71
15) Turton JF Englender H Gabriel SN Turton SE Kaufmann
ME Pitt TL Genetically similar isolates of Klebsiella pneu-
moniae serotype K1 causing liver abscesses in three
continents J Med Microbiol 2007 56 593-7

Ji-Ae Hwang et alKlebsiella pneumoniae Endocarditis 43
Fig 3 A modified parasternal long axis view of transthoracic
echocardiography showed a large vegetation on the posterior
leaflet (double arrows) and a small vegetation on the aortic
valve (single arrow) LV denotes left ventricle RV right
ventricle AA ascending aorta and LA left atrium
meningitis and multiple small infarctions most likely from sep-
tic embolism Intravenous administration of metronidazole (500
mg every 8 hours) and ceftazidime (2 g) was started SpO2
became 80 and the patients trachea was intubated and he
was placed on mechanical ventilator Intravenous infusions of
dopamine and norepinephrine were started to maintain systolic
blood pressure higher than 100 mmHg (or mean pressure of
65 mmHg) Two large liver abscesses were drained under ul-
trasonographic guidance Vancomycin (1 g) was added The
patient was admitted to ICU Continuous renal replacement
therapy was started
On the second hospital day a severe metabolic acidosis de-
veloped (Table 1) Sodium bicarbonate and fresh frozen plasma
were given A systolic murmur (36) was heard at the left
lower sternum radiating to the left axilla On the third hospital
day a transthoracic echocardiography revealed a large vegeta-
tion involving the posterior mitral leaflet with a moder-
ate-to-severe mitral regurgitation (16times15 cm) and a small veg-
etation (06times045 cm) involving the aortic valve with a moder-
ate regurgitation (Fig 3) There was no evidence of endoph-
thalmitis In the presence of multiple organ dysfunction and
severe septic shock the patients condition was considered too
poor for a surgery for the replacement of cardiac valves to be
done On the fourth hospital day the patient suffered cardiac
arrest and resuscitation was unsuccessful On the following day
the results of culture of liver abscess sputum and blood came
back showing heavy growths of Klebsiella pneumoniae which
was resistant to ampicillin and piperacillin but sensitive to all
other antibiotics
DISCUSSION
Previous studies have identified significant differences be-
tween nosocomial and community-acquired Klebsiella pneumo-
niae infections[12] A primary pyogenic liver abscess develops
almost exclusively in patients with community-acquired in-
fections particularly in Asia Underlying diabetes mellitus was
more common in community-acquired infections
Because of the history of attendance at the hemodialysis
clinic for the regular hemodialysis one may consider this case
in the present report as nosocomial infection However the
presence of underlying diabetes mellitus development of liver
abscess and a low antimicrobial resistance of cultured Kleb-
siella pneumoniae isolates all together support the notion that
the case patient had a community-acquired infection When the
patient was admitted to another hospital the presence of pneu-
monia was apparent by chest radiograph but the presence of
liver abscess was questionable by computed tomography
Moreover despite tremendously elevated inflammatory biomar-
kers such as procalcitonin and C-reactive protein liver en-
zymes were only slightly elevated indicating that systemic in-
flammatory reaction had been activated before the development
of liver abscess In addition upon admission to this hospital a
computed tomography showed multiple liver abscesses which
strongly suggested that the liver abscess in this case was meta-
static rather than primary infection One may argue over the
possibility that the liver abscess was the primary infection site
and the pneumonia was the metastatic infection in this case
However the metastatic lung infection from the liver abscess
is very rare in Korea[4] and is usually presented as septic em-
boli or abscess rather than air space infiltration[5] In addition
primary liver abscess due to Klebsiella pneumoniae infection is
usually not associated with septic shock even with metastatic
infection to lung[4] whereas primary lung infection can be as-
sociated with a much more fulminant course[6] A previous
study has shown that septic shock (51 of cases) and acute
respiratory failure (61 of cases) are initial presentation in
many patients with community-acquired pneumonia due to
Klebsiella pneumoniae and are the independent risk factors for
the mortality[6] Taken together it is most likely that his ful-
minant illness started with pneumonia which was complicated
by septic shock and acute respiratory failure and progressed to
44 한 환자의학회지제 28 권 제 1 호 2013
bacteremia causing liver abscess endocarditis and other sys-
temic septic complications
Several cases of endocarditis that were associated with noso-
comial Klebsiella pneumoniae infections have been reported
previously[7] The urinary tract was the most common source
of bacteremia and the aortic valve was the most commonly
affected But there was no liver abscess in those cases There
is only one case report of infective endocarditis caused by
community-acquired Klebsiella pneumoniae infection Bactere-
mia from the primary liver abscess due to community-acquired
Klebsiella pneumoniae infection has been reported to cause an
infective endocarditis involving mitral valve[8] However the
patient in that previous report[8] initially presented with pneu-
monia which became severe enough to require mechanical
ventilator support Thus it is conceivable that primary infection
site may have been pneumonia rather than liver abscess in that
case considering the fact that none of the previously reported
numerous cases of primary liver abscess caused by commun-
ity-acquired Klebsiella pneumoniae developed endocarditis de-
spite the presence of many other metastatic infections[2-46] It
seems to be that the primary liver abscess is least likely the
source of bacteremia for endocarditis in community-acquired
Klebsiella pneumoniae infection
Many cases of pyogenic liver abscess caused by commun-
ity-acquired Klebsiella pneumoniae infection have been reported
in the United States[910] The isolates mostly were sensitive
to all antibiotics except ampicillin and in most cases piper-
acillin-tazobactam was given empirically as an initial anti-
microbial medication In contrary Klebsiella pneumoniae isolate
in the present case report was resistant to not only ampicillin
but also piperacillin Unfortunately when the patient in the
present report was admitted to another hospital only piper-
acillin-tazobactam was given It has been shown that early
combination antibiotic therapy yields improved survival com-
pared with monotherapy in sepsis particularly when beta-lac-
tams are used[11] Generally two of the guideline-concordant
antimicrobial combinations for severe community-acquired pneu-
monia are either a beta-lactam and fluoroquinolone or beta-lac-
tam and macrolide[12] Interestingly Administration of a mac-
rolide antibiotic within 24 hour upon admission has been
shown to decrease mortality[13] According to a previous
study delay in administration of initial (appropriate) antibiotics
until after the recognition of shock was associated with in-
creased mortality[14] As such a delay in initial appropriate
antibiotics could have contributed to the poor outcome of the
case in the present report While writing this paper there was
another case of community-acquired Klebsiella pneumoniae
causing pneumonia followed by bacteremia and multiple liver
abscesses in our intensive care unit The isolate was also re-
sistant to both ampicillin and piperacillin but sensitive to all
other antibiotics
Klebsiella pneumoniae pyogenic liver abscess is not a dis-
ease limited in Asia but an emerging disease in Europe and
North America[15] Furthermore community-acquired Klebsiella
pneumoniae infection is not limited to Asian who travels to
other continents Previous reports have shown that Caucasian
who have never traveled to Asia get infected with this mi-
crobe causing liver abscess[910] Thus it is not likely that
ethnicity contributes to susceptibility to this organism Anyone
may get this infection particularly if the person has diabetes
mellitus
In summary we described a case of community-acquired
Klebsiella pneumoniae infection that started with pneumonia
and progressed to bacteremia causing liver abscess endocardi-
tis and other systemic septic complications The isolate was
resistant not only to ampicillin and but also piperacillin
REFERENCES
1) Tsay RW Siu LK Fung CP Chang FY Characteristics of
bacteremia between community-acquired and nosocomial
Klebsiella pneumoniae infection risk factor for mortality and
the impact of capsular serotypes as a herald for community-ac-
quired infection Arch Intern Med 2002 162 1021-7
2) Kang CI Kim SH Bang JW Kim HB Kim NJ Kim EC
et al Community-acquired versus nosocomial Klebsiella pneu-
moniae bacteremia clinical features treatment outcomes and
clinical implication of antimicrobial resistance J Korean Med
Sci 2006 21 816-22
3) Fang CT Lai SY Yi WC Hsueh PR Liu KL Chang SC
Klebsiella pneumoniae genotype K1 an emerging pathogen
that causes septic ocular or central nervous system complica-
tions from pyogenic liver abscess Clin Infect Dis 2007 45
284-93
4) Siu LK Yeh KM Lin JC Fung CP Chang FY Klebsiella
pneumoniae liver abscess a new invasive syndrome Lancet
Infect Dis 2012 12 881-7
5) Ko WC Paterson DL Sagnimeni AJ Hansen DS Von
Gottberg A Mohapatra S et al Community-acquired Klebsiel-
la pneumoniae bacteremia global differences in clinical
patterns Emerg Infect Dis 2002 8 160-6
6) Lin YT Jeng YY Chen TL Fung CP Bacteremic commun-
ity-acquired pneumonia due to Klebsiella pneumoniae clinical
and microbiological characteristics in Taiwan 2001-2008
BMC Infect Dis 2010 10 307-7
7) Thomas MG Rowland-Jones S Smyth E Klebsiella pneumo-
Ji-Ae Hwang et alKlebsiella pneumoniae Endocarditis 45
niae endocarditis J R Soc Med 1989 82 114-5
8) Rivero A Gomez E Alland D Huang DB Chiang T K2 se-
rotype Klebsiella pneumoniae causing a liver abscess asso-
ciated with infective endocarditis J Clin Microbiol 2010 48
639-41
9) Lederman ER Crum NF Pyogenic liver abscess with a focus
on Klebsiella pneumoniae as a primary pathogen an emerging
disease with unique clinical characteristics Am J Gastroenterol
2005 100 322-31
10) Fierer J Walls L Chu P Recurring Klebsiella pneumoniae
pyogenic liver abscesses in a resident of San Diego California
due to a K1 strain carrying the virulence plasmid J Clin
Microbiol 2011 49 4371-3
11) Kumar A Zarychanski R Light B Parrillo J Maki D Simon
D et al Cooperative Antimicrobial Therapy of Septic Shock
(CATSS) Database Research Group Early combination anti-
biotic therapy yields improved survival compared with mono-
therapy in septic shock a propensity-matched analysis Crit
Care Med 2010 38 1773-85
12) Wilson BZ Anzueto A Restrepo MI Pugh MJ Mortensen
EM Comparison of two guideline-concordant antimicrobial
combinations in elderly patients hospitalized with severe com-
munity-acquired pneumonia Crit Care Med 2012 40 2310-4
13) Walkey AJ Wiener RS Macrolide antibiotics and survival in
patients with acute lung injury Chest 2012 141 1153-9
14) Puskarich MA Trzeciak S Shapiro NI Arnold RC Horton
JM Studnek JR et al Emergency Medicine Shock Research
Network (EMSHOCKNET) Association between timing of
antibiotic administration and mortality from septic shock in pa-
tients treated with a quantitative resuscitation protocol Crit
Care Med 2011 39 2066-71
15) Turton JF Englender H Gabriel SN Turton SE Kaufmann
ME Pitt TL Genetically similar isolates of Klebsiella pneu-
moniae serotype K1 causing liver abscesses in three
continents J Med Microbiol 2007 56 593-7

44 한 환자의학회지제 28 권 제 1 호 2013
bacteremia causing liver abscess endocarditis and other sys-
temic septic complications
Several cases of endocarditis that were associated with noso-
comial Klebsiella pneumoniae infections have been reported
previously[7] The urinary tract was the most common source
of bacteremia and the aortic valve was the most commonly
affected But there was no liver abscess in those cases There
is only one case report of infective endocarditis caused by
community-acquired Klebsiella pneumoniae infection Bactere-
mia from the primary liver abscess due to community-acquired
Klebsiella pneumoniae infection has been reported to cause an
infective endocarditis involving mitral valve[8] However the
patient in that previous report[8] initially presented with pneu-
monia which became severe enough to require mechanical
ventilator support Thus it is conceivable that primary infection
site may have been pneumonia rather than liver abscess in that
case considering the fact that none of the previously reported
numerous cases of primary liver abscess caused by commun-
ity-acquired Klebsiella pneumoniae developed endocarditis de-
spite the presence of many other metastatic infections[2-46] It
seems to be that the primary liver abscess is least likely the
source of bacteremia for endocarditis in community-acquired
Klebsiella pneumoniae infection
Many cases of pyogenic liver abscess caused by commun-
ity-acquired Klebsiella pneumoniae infection have been reported
in the United States[910] The isolates mostly were sensitive
to all antibiotics except ampicillin and in most cases piper-
acillin-tazobactam was given empirically as an initial anti-
microbial medication In contrary Klebsiella pneumoniae isolate
in the present case report was resistant to not only ampicillin
but also piperacillin Unfortunately when the patient in the
present report was admitted to another hospital only piper-
acillin-tazobactam was given It has been shown that early
combination antibiotic therapy yields improved survival com-
pared with monotherapy in sepsis particularly when beta-lac-
tams are used[11] Generally two of the guideline-concordant
antimicrobial combinations for severe community-acquired pneu-
monia are either a beta-lactam and fluoroquinolone or beta-lac-
tam and macrolide[12] Interestingly Administration of a mac-
rolide antibiotic within 24 hour upon admission has been
shown to decrease mortality[13] According to a previous
study delay in administration of initial (appropriate) antibiotics
until after the recognition of shock was associated with in-
creased mortality[14] As such a delay in initial appropriate
antibiotics could have contributed to the poor outcome of the
case in the present report While writing this paper there was
another case of community-acquired Klebsiella pneumoniae
causing pneumonia followed by bacteremia and multiple liver
abscesses in our intensive care unit The isolate was also re-
sistant to both ampicillin and piperacillin but sensitive to all
other antibiotics
Klebsiella pneumoniae pyogenic liver abscess is not a dis-
ease limited in Asia but an emerging disease in Europe and
North America[15] Furthermore community-acquired Klebsiella
pneumoniae infection is not limited to Asian who travels to
other continents Previous reports have shown that Caucasian
who have never traveled to Asia get infected with this mi-
crobe causing liver abscess[910] Thus it is not likely that
ethnicity contributes to susceptibility to this organism Anyone
may get this infection particularly if the person has diabetes
mellitus
In summary we described a case of community-acquired
Klebsiella pneumoniae infection that started with pneumonia
and progressed to bacteremia causing liver abscess endocardi-
tis and other systemic septic complications The isolate was
resistant not only to ampicillin and but also piperacillin
REFERENCES
1) Tsay RW Siu LK Fung CP Chang FY Characteristics of
bacteremia between community-acquired and nosocomial
Klebsiella pneumoniae infection risk factor for mortality and
the impact of capsular serotypes as a herald for community-ac-
quired infection Arch Intern Med 2002 162 1021-7
2) Kang CI Kim SH Bang JW Kim HB Kim NJ Kim EC
et al Community-acquired versus nosocomial Klebsiella pneu-
moniae bacteremia clinical features treatment outcomes and
clinical implication of antimicrobial resistance J Korean Med
Sci 2006 21 816-22
3) Fang CT Lai SY Yi WC Hsueh PR Liu KL Chang SC
Klebsiella pneumoniae genotype K1 an emerging pathogen
that causes septic ocular or central nervous system complica-
tions from pyogenic liver abscess Clin Infect Dis 2007 45
284-93
4) Siu LK Yeh KM Lin JC Fung CP Chang FY Klebsiella
pneumoniae liver abscess a new invasive syndrome Lancet
Infect Dis 2012 12 881-7
5) Ko WC Paterson DL Sagnimeni AJ Hansen DS Von
Gottberg A Mohapatra S et al Community-acquired Klebsiel-
la pneumoniae bacteremia global differences in clinical
patterns Emerg Infect Dis 2002 8 160-6
6) Lin YT Jeng YY Chen TL Fung CP Bacteremic commun-
ity-acquired pneumonia due to Klebsiella pneumoniae clinical
and microbiological characteristics in Taiwan 2001-2008
BMC Infect Dis 2010 10 307-7
7) Thomas MG Rowland-Jones S Smyth E Klebsiella pneumo-
Ji-Ae Hwang et alKlebsiella pneumoniae Endocarditis 45
niae endocarditis J R Soc Med 1989 82 114-5
8) Rivero A Gomez E Alland D Huang DB Chiang T K2 se-
rotype Klebsiella pneumoniae causing a liver abscess asso-
ciated with infective endocarditis J Clin Microbiol 2010 48
639-41
9) Lederman ER Crum NF Pyogenic liver abscess with a focus
on Klebsiella pneumoniae as a primary pathogen an emerging
disease with unique clinical characteristics Am J Gastroenterol
2005 100 322-31
10) Fierer J Walls L Chu P Recurring Klebsiella pneumoniae
pyogenic liver abscesses in a resident of San Diego California
due to a K1 strain carrying the virulence plasmid J Clin
Microbiol 2011 49 4371-3
11) Kumar A Zarychanski R Light B Parrillo J Maki D Simon
D et al Cooperative Antimicrobial Therapy of Septic Shock
(CATSS) Database Research Group Early combination anti-
biotic therapy yields improved survival compared with mono-
therapy in septic shock a propensity-matched analysis Crit
Care Med 2010 38 1773-85
12) Wilson BZ Anzueto A Restrepo MI Pugh MJ Mortensen
EM Comparison of two guideline-concordant antimicrobial
combinations in elderly patients hospitalized with severe com-
munity-acquired pneumonia Crit Care Med 2012 40 2310-4
13) Walkey AJ Wiener RS Macrolide antibiotics and survival in
patients with acute lung injury Chest 2012 141 1153-9
14) Puskarich MA Trzeciak S Shapiro NI Arnold RC Horton
JM Studnek JR et al Emergency Medicine Shock Research
Network (EMSHOCKNET) Association between timing of
antibiotic administration and mortality from septic shock in pa-
tients treated with a quantitative resuscitation protocol Crit
Care Med 2011 39 2066-71
15) Turton JF Englender H Gabriel SN Turton SE Kaufmann
ME Pitt TL Genetically similar isolates of Klebsiella pneu-
moniae serotype K1 causing liver abscesses in three
continents J Med Microbiol 2007 56 593-7

Ji-Ae Hwang et alKlebsiella pneumoniae Endocarditis 45
niae endocarditis J R Soc Med 1989 82 114-5
8) Rivero A Gomez E Alland D Huang DB Chiang T K2 se-
rotype Klebsiella pneumoniae causing a liver abscess asso-
ciated with infective endocarditis J Clin Microbiol 2010 48
639-41
9) Lederman ER Crum NF Pyogenic liver abscess with a focus
on Klebsiella pneumoniae as a primary pathogen an emerging
disease with unique clinical characteristics Am J Gastroenterol
2005 100 322-31
10) Fierer J Walls L Chu P Recurring Klebsiella pneumoniae
pyogenic liver abscesses in a resident of San Diego California
due to a K1 strain carrying the virulence plasmid J Clin
Microbiol 2011 49 4371-3
11) Kumar A Zarychanski R Light B Parrillo J Maki D Simon
D et al Cooperative Antimicrobial Therapy of Septic Shock
(CATSS) Database Research Group Early combination anti-
biotic therapy yields improved survival compared with mono-
therapy in septic shock a propensity-matched analysis Crit
Care Med 2010 38 1773-85
12) Wilson BZ Anzueto A Restrepo MI Pugh MJ Mortensen
EM Comparison of two guideline-concordant antimicrobial
combinations in elderly patients hospitalized with severe com-
munity-acquired pneumonia Crit Care Med 2012 40 2310-4
13) Walkey AJ Wiener RS Macrolide antibiotics and survival in
patients with acute lung injury Chest 2012 141 1153-9
14) Puskarich MA Trzeciak S Shapiro NI Arnold RC Horton
JM Studnek JR et al Emergency Medicine Shock Research
Network (EMSHOCKNET) Association between timing of
antibiotic administration and mortality from septic shock in pa-
tients treated with a quantitative resuscitation protocol Crit
Care Med 2011 39 2066-71
15) Turton JF Englender H Gabriel SN Turton SE Kaufmann
ME Pitt TL Genetically similar isolates of Klebsiella pneu-
moniae serotype K1 causing liver abscesses in three
continents J Med Microbiol 2007 56 593-7