Endobronchial metastasis from rectal adenocarcinoma · showed pneumonic changes distal to the...
4
RESPIRATORY MEDICINE (1997) 91, 245-248 Endobronchial metastasis from rectal adenocarcinoma Y. C. LEE, C. S. WONG, AND G. M. JEFFERY Department of Medicine, Dunedin Hospital, Dunedin, New Zealand A case of endobronchial metastasis 2 yr following treatment of rectal carcinoma is presented. Endobronchial metastases from extrathoracic primary malignancies are uncommon, the estimated frequency and possible mechanisms underlying this complication are discussed. The importance of recognizing possible endobronchial metastasis is in the approach to management and prognosis. RESPIR. MED. (1997) 91, 245-248 Introduction Endobronchial metastases from extrathoracic primary malignancies are uncommon. Breast (1) renal (24) and colonic carcinomas (5-7) are primary sites most likely to give rise to endo- bronchial metastases (16). A number of other tumours have been reported as being compli- cated by endobronchial metastasis, including ovarian (8), thyroid (9), uterine (lo), adrenal (1l), testicular (12) and prostatic carcinomas (19) giant cell tumour of the bone (20), sar- comas (13), melanomas (6) and even Meibomian gland carcinoma of the eyelid (14). Many cases of endobronchial metastasis have only been diagnosed at post mortem. The incidence of endobronchial metastasis has been estimated at 2% in patients who died of metastatic disease (9). The present case report describes a rare case of an endobronchial metastasis from rectal adeno- carcinoma. Also, the relevant literature is reviewed. Case Report A 69-year-old Caucasian male had an abdomino-perineal resection for a moderately differentiated Duke’s C adenocarcinoma of the Received 1 December 1995 and accepted in revised form 2 August 1996. Correspondence to: G. M. Jeffery, Department of Medicine, Dunedin Hospital, Dunedin, New Zealand. 0954-6111/97/040245+04 $12.00/O rectum in April 1993. Eight of 16 local lymph nodes were positive for tumour. Post-operative computed tomography (CT) of the abdomen and chest X-ray were normal. The patient received local radiotherapy and 5-fluorouracil (5-FU) chemotherapy. Fourteen months later, the patient underwent laparoscopic cholecystectomy for gallstone dis- ease. Tumour deposits were noted in the liver during the procedure and CT scan confirmed multiple liver metastases.He was asymptomatic and elected not to recommence chemotherapy at that time. In March 1995, the patient developed symp- toms of increasing tiredness, and his liver function tests became deranged. Palliative chemotherapy (5-FU and folinic acid) was com- menced. He developed dyspnoea while still on chemotherapy. A chest X-ray showed lesions in the lingula and the peripheral right lower lobe consistent with metastases (Plate 1). The patient re-presented in June 1995 with fever, cough and dyspnoea. A chest X-ray showed pneumonic changes distal to the lingular lesion. At fibre-optic bronchoscopy, an endo- bronchial lesion was seen obstructing the seg- mental bronchus of the lingular lobe. Histology of the endobronchial tumour showed adeno- carcinoma (Plate 2). As the lesion was endo- bronchial and the patient had a 50 pack-year smoking history, the initial clinical impression was that of a primary bronchogenic adenocarci- noma. However, the histology of the bronchial 0 1997 W. B. SAUNDERS COMPANY LTD
Transcript of Endobronchial metastasis from rectal adenocarcinoma · showed pneumonic changes distal to the...

RESPIRATORY MEDICINE (1997) 91, 245-248
Endobronchial metastasis from rectal adenocarcinoma
Y. C. LEE, C. S. WONG, AND G. M. JEFFERY
Department of Medicine, Dunedin Hospital, Dunedin, New Zealand
A case of endobronchial metastasis 2 yr following treatment of rectal carcinoma is presented. Endobronchial metastases from extrathoracic primary malignancies are uncommon, the estimated frequency and possible mechanisms underlying this complication are discussed. The importance of recognizing possible endobronchial metastasis is in the approach to management and prognosis.
RESPIR. MED. (1997) 91, 245-248
Introduction
Endobronchial metastases from extrathoracic primary malignancies are uncommon. Breast (1) renal (24) and colonic carcinomas (5-7) are primary sites most likely to give rise to endo- bronchial metastases (16). A number of other tumours have been reported as being compli- cated by endobronchial metastasis, including ovarian (8), thyroid (9), uterine (lo), adrenal (1 l), testicular (12) and prostatic carcinomas (19) giant cell tumour of the bone (20), sar- comas (13), melanomas (6) and even Meibomian gland carcinoma of the eyelid (14). Many cases of endobronchial metastasis have only been diagnosed at post mortem. The incidence of endobronchial metastasis has been estimated at 2% in patients who died of metastatic disease (9).
The present case report describes a rare case of an endobronchial metastasis from rectal adeno- carcinoma. Also, the relevant literature is reviewed.
Case Report
A 69-year-old Caucasian male had an abdomino-perineal resection for a moderately differentiated Duke’s C adenocarcinoma of the
Received 1 December 1995 and accepted in revised form 2 August 1996. Correspondence to: G. M. Jeffery, Department of Medicine, Dunedin Hospital, Dunedin, New Zealand.
0954-6111/97/040245+04 $12.00/O
rectum in April 1993. Eight of 16 local lymph nodes were positive for tumour. Post-operative computed tomography (CT) of the abdomen and chest X-ray were normal. The patient received local radiotherapy and 5-fluorouracil (5-FU) chemotherapy.
Fourteen months later, the patient underwent laparoscopic cholecystectomy for gallstone dis- ease. Tumour deposits were noted in the liver during the procedure and CT scan confirmed multiple liver metastases. He was asymptomatic and elected not to recommence chemotherapy at that time.
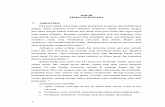
In March 1995, the patient developed symp- toms of increasing tiredness, and his liver function tests became deranged. Palliative chemotherapy (5-FU and folinic acid) was com- menced. He developed dyspnoea while still on chemotherapy. A chest X-ray showed lesions in the lingula and the peripheral right lower lobe consistent with metastases (Plate 1).
The patient re-presented in June 1995 with fever, cough and dyspnoea. A chest X-ray showed pneumonic changes distal to the lingular lesion. At fibre-optic bronchoscopy, an endo- bronchial lesion was seen obstructing the seg- mental bronchus of the lingular lobe. Histology of the endobronchial tumour showed adeno- carcinoma (Plate 2). As the lesion was endo- bronchial and the patient had a 50 pack-year smoking history, the initial clinical impression was that of a primary bronchogenic adenocarci- noma. However, the histology of the bronchial
0 1997 W. B. SAUNDERS COMPANY LTD
246 Y. C. LEE ET AL.
PLATE 1. The PA chest X-ray showing the lingula lobe lesion. There is also a smaller lesion in the right lower peripheral lung field.
PLATE 2. Biopsy of the endobronchial lesion from lingula lobe. Well-differentiated adenocarcinoma with severely dysplastic columnar epithelium with features compatible with colorectal primary (H&E stain, 70 x magnification).
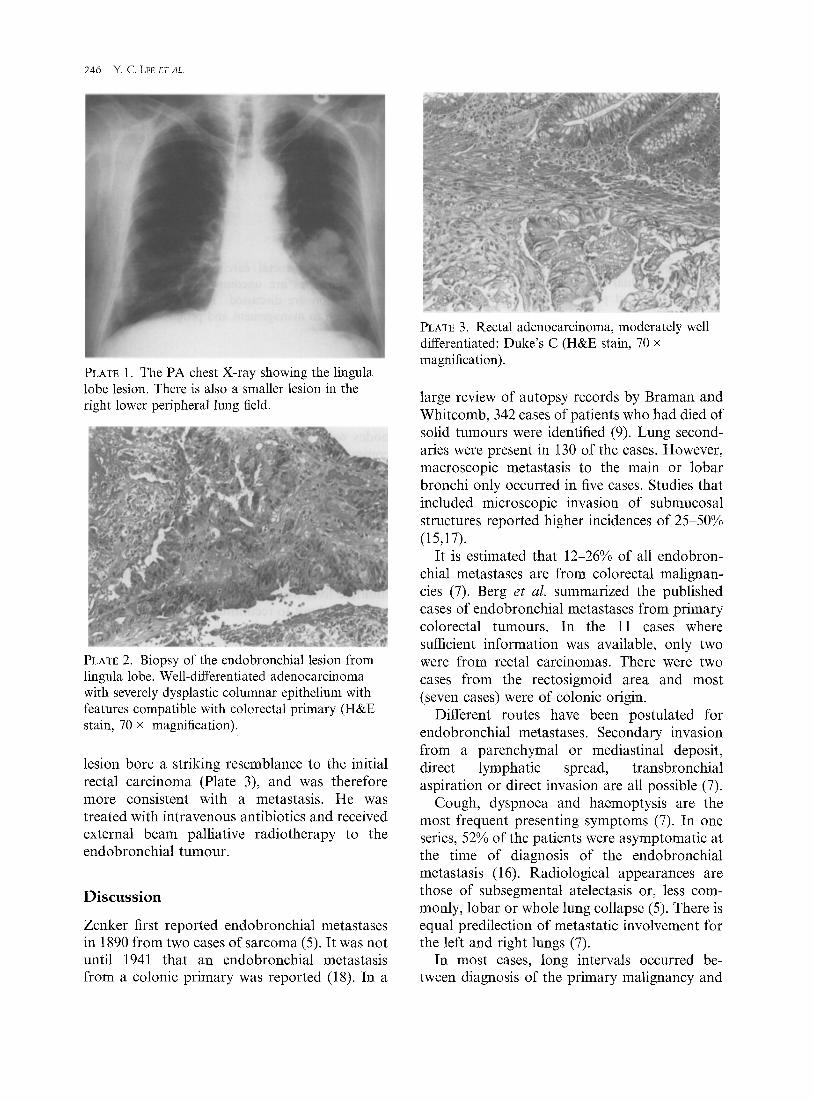
lesion bore a striking resemblance to the initial rectal carcinoma (Plate 3), and was therefore more consistent with a metastasis. He was treated with intravenous antibiotics and received external beam palliative radiotherapy to the endobronchial tumour.
Discussion
Zenker first reported endobronchial metastases in 1890 from two cases of sarcoma (5). It was not until 1941 that an endobronchial metastasis from a colonic primary was reported (18). In a
PLATE 3. Rectal adenocarcinoma, moderately well differentiated: Duke’s C (H&E stain, 70 x magnification).
large review of autopsy records by Braman and Whitcomb, 342 cases of patients who had died of solid tumours were identified (9). Lung second- aries were present in 130 of the cases. However, macroscopic metastasis to the main or lobar bronchi only occurred in five cases. Studies that included microscopic invasion of submucosal structures reported higher incidences of 25-50% (15,17).
It is estimated that 12-26% of all endobron- chial metastases are from colorectal malignan- cies (7). Berg et al. summarized the published cases of endobronchial metastases from primary colorectal tumours. In the 11 cases where sufficient information was available, only two were from rectal carcinomas. There were two cases from the rectosigmoid area and most (seven cases) were of colonic origin.
Different routes have been postulated for endobronchial metastases. Secondary invasion from a parenchymal or mediastinal deposit, direct lymphatic spread, transbronchial aspiration or direct invasion are all possible (7).
Cough, dyspnoea and haemoptysis are the most frequent presenting symptoms (7). In one series, 52% of the patients were asymptomatic at the time of diagnosis of the endobronchial metastasis (16). Radiological appearances are those of subsegmental atelectasis or, less com- monly, lobar or whole lung collapse (5). There is equal predilection of metastatic involvement for the left and right lungs (7).
In most cases, long intervals occurred be- tween diagnosis of the primary malignancy and

discovery of the endobronchial metastasis. Mean and median primary-secondary intervals were reported as 5-6 yr in different series (5,16). However, endobronchial metastasis may be the first presentation of the malignant disease (6,9). In the present patient, the lingula lobe deposit was diagnosed 2 yr after his primary rectal carcinoma.
Endobronchial metastasis is believed to be a late sign and carries a poor prognosis. Survival time following the diagnosis of endobronchial metastasis was 12.5 months (16) and 19 months (5) in two different studies. Most reports have limited sample sizes and large ranges in the survival duration. Survival of more than 10 yr has been reported in one patient with metastatic adenocarcinoma (6). It is, therefore, important to assess each case individually.
Distinguishing between a primary broncho- genie carcinoma and endobronchial metastasis is not always easy. Bronchoscopy with biopsy is mandatory as a histological comparison of the endobronchial lesion, and the original malig- nancy can help to establish the diagnosis, as in the present patient. Bronchoscopic brushing and washings for cytology may be of additional value (16).
Management depends on the type of tumour. In 87% of patients, widespread metastases were present at the time of diagnosis of endobronchial involvement (16). Surgery is, therefore, seldom employed. Chemotherapy, especially in breast carcinoma, and radiotherapy (external beam or brachytherapy) should be used as appropriate. In most cases, treatment is palliative and the main aim is to alleviate symptoms.
Post mortem figures published in the 1970s suggested that macroscopic endobronchial metastases involving the large airways occurred in only 2% of all patients with solid tumours. With advances in surgery, chemotherapy and radiotherapy, patients with some malignant dis- eases now have longer survivals allowing more time for endobronchial secondaries to develop. Pulmonary metastases are common in clinical practice. However, because of the poor progno- sis or poor general condition, few patients will go forward for bronchoscopy, without which it is difficult to differentiate between endobronchial and parenchymal metastases. Few will proceed to autopsy. Thus the exact incidence of
ENDOBRONCHIALMETASTASISFROMRECTALADEIGOCARCINO.MA 247
macroscopic endobronchial metastases in the 1990s may well be underestimated.
Endobronchial metastasis raises some inter- esting questions which reflect our lack of under- standing of cancer pathology. The mechanism of endobronchial spread is unclear. Most pulmonary metastases occur in the lung paren- chyma. Why a certain small proportion arise in the tracheobronchial tree remains unanswered.
Although there are considerable differences in the incidences reported, most series suggest that breast and colonic tumours are the more common primary malignancies associated with endobronchial deposits. Whether this reflects the higher incidences of these two tumours in the general population, or whether there are charac- teristics of these carcinomas that enhance tracheobronchial spread is uncertain.
In summary, endobronchial metastasis from a primary rectal adenocarcinoma is an uncommon phenomenon, and the underlying aetiology is not fully understood. The incidence of endo- bronchial metastasis in the 1990s may well be underestimated. It should always be considered when investigating any endobronchial lesion, especially in patients with previous malignancies, as the management and prognosis are often very different from primary bronchogenic carcinomas.
References
1.
2.
3.
4.
5.
6.
7.
DeBeer RA, Garcia RL, Alexander SC. Endo- bronchial metastasis from cancer of the breast. Chest 1978; 73: 94&96. Nofsinger CD, Vinson PP. Intrabronchial met- astases of hypernephroma simulating primary bronchial carcinoma. JAMA 1942; 42: 944-945. Maytum CK, Vinson PP. Pulmonary metastasis from hypernephroma with ulceration into a bron- chus simulating primary bronchial carcinoma. A& OtolaFyngol 1936; 23: 101-104. Caplan H. Solitary endobronchial metastasis from carcinoma of the kidney. Br J Swg 1959; 46: 624-625. Baumgartner WA, Mark JBD. Metastatic malig- nancies from distant sites to the tracheobronchial tree. J Thorac Cavdiovasc Swg 1980; 79: 499-503. Shepherd MP. Endobronchial metastatic disease. Thorax 1982; 37: 362-365. Berg HK, Petrelli NJ, Herrera L, Lopez C, Mittelman A. Endobronchial metastasis from

248 Y. C. LEE ET AL
colorectal carcinoma. Dis Co1 Rect 1984; 27: 745-74s.
8. Freelander SO, Greenfield J. Hemoptysis in metastatic tumour of the lung simulating bron- chogenic carcinoma. J Thorac Cardiovasc Surg 1942; 12: 109-116.
9. Braman SS, Whitcomb ME. Endobronchial metastasis. Arch Int Med 1975; 135: 543-547.
10. Brezina PS, Lindskog GE. Total pneumonec- tomy for metastatic uterine carcinoma. J Thorac Surg 1943; 12: 728-733.
11. Trinidad S, Lisa JR, Rosenblatt MD. Broncho- genie carcinoma simulated by metastatic tumours. Cancer 1963; 16: 1527-1529.
12. Varkey B, Heckman MG. Diagnosis of a case of embryonal carcinoma by bronchial biopsy. Chest 1972; 62: 758-760.
13. Alexander J, Haight C. Pulmonary resections for solitary metastatic sarcomas and carcinomas. Surg Gynecol Obstet 1947; 85: 1299146.
14. Koyama S, Honde T, Shinozaci S et al. A case of lung metastasis from Meibomian gland
carcinoma of eyelid with effective chemotherapy. Gan-To-Kagaku-Ryoho 1994; 21: 2809-2812.
15. Rosenblatt MB, Lisa JR, Trinidad S. Pitfalls in the clinical and histological diagnosis of bronchogenic carcinoma. Chest 1966; 49: 3966404.
16. Heitmiller RF, Marascow WJ, Hruben RH, Marsh BR. Endobronchial metastasis. J Thorac Cardiovasc Surg 1993; 106: 537-542.
17. King DS, Castleman B. Bronchial involvement in metastatid pulmonary malignancy. J Thorac Surg 1943; 12: 305-315.
18. Raine F. Metastatic carcinoma of the lung invading and obstructing a bronchus. J Thorac Cardiovasc Surg 1941; 11: 216-218.
19. Lee DW, Ro JY, Sahin AA, Lee JS, Ayala AG. Mutinous adenocarcinoma of the prostate with endobronchial metastasis. Am J Clin Path01 1990; 94: 641-645.
20. Boghani A, Gayathri K, Ratnakar KS. Endo- bronchial metastasis from giant cell tumour of bone. Chest 1994; 106: 1599-1601.