Emerging Problems in the Management of Paediatric Acute Otitis Media and Other Bacterial Infectio
29
ICSS Emerging Problems in the Management of Paediatric Acute Otitis Media and Other Bacterial Infections Contributions from Albert M Collier, Hyman W Fisher, Christopher Harrison, Michael R Jacobs, Craig Martin INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES 270 5.)6%23)49/&+%.45#+9 0HARMACYAND-EDICINE #ONTINUING%DUCATION
description
Health
Transcript of Emerging Problems in the Management of Paediatric Acute Otitis Media and Other Bacterial Infectio

ICSSEmerging Problems in the
Management of Paediatric Acute Otitis Media and Other
Bacterial Infections
Contributions from
Albert M Collier, Hyman W Fisher,Christopher Harrison, Michael R Jacobs, Craig Martin
ICSS INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES 270

ICSSEditor-in-Chief: Dr Jack Tinker
Emerging Problems in the
Management of Paediatric Acute
Otitis Media and Other
Bacterial Infections
Contributions from
Albert M Collier, Hyman W Fisher,
Christopher Harrison, Michael R Jacobs, Craig Martin
Containing a summary of the proceedings of a meeting held in Baltimore, Maryland, USA,
in July 2006, which were published in the International Congress and Symposium
Series 265: Acute Otitis Media: Translating Science into Clinical Practice (2007).
These edited extracts and additional material reflect the experience and opinions of the
panellists and do not necessarily reflect the opinions of the Royal Society of Medicine Press
or the recommendations of Lupin Pharmaceuticals, Inc.
This activity is jointly sponsored by the University of Kentucky Colleges of Pharmacy and
Medicine Continuing Education Office and the Royal Society of Medicine Press. It is
supported by an unrestricted educational grant from Lupin Pharmaceuticals, Inc.
INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES 270

© 2007 Royal Society of Medicine Press Ltd
Published by the Royal Society of Medicine Press Ltd
1 Wimpole Street, London W1G 0AE, UK
Tel: +44 (0)20 7290 2921
Fax: +44 (0)20 7290 2929
E-mail: [email protected]
Website: www.rsmpress.co.uk
Apart from any fair dealing for the purposes of research or private study, criticism
or review, as permitted under the UK Copyright Designs and Patents Act, 1988,
no part of this publication may be reproduced, stored or transmitted, in any form
or by any means, without the prior permission in writing of the publishers or in the
case of reprographic reproduction in accordance with the terms of licences issued
by the Copyright Licensing Agency in the UK, or in accordance with the terms of
licences issued by the appropriate Reproduction Rights Organization outside the
UK. Enquiries concerning reproduction outside the terms stated here should be
sent to the publishers at the UK address printed on this page.
These proceedings are published by the Royal Society of Medicine Press Ltd with
financial support from the sponsor. The contributors are responsible for the
scientific content and for the views expressed, which are not necessarily those of
the sponsor, of the editor of the series or of the volume, of the Royal Society of
Medicine or of the Royal Society of Medicine Press Ltd. Distribution has been in
accordance with the wishes of the sponsor but a copy is available to any fellow of
the Society at a privileged price.
British Library Cataloguing in Publication Data
A catalogue record for this book is available from the British Library
ISBN 978-1-85315-756-1
ISSN 0142-2367
Distribution in Europe and Rest of World: Distribution in Australia and New Zealand:
Marston Book Services Ltd Elsevier Australia
PO Box 269 30–52 Smidmore Street
Abingdon Marrikville NSW 2204, Australia
Oxon OX14 4YN, UK Tel: +61 2 9517 8999
Tel:+44 (0)1235 465 500 Fax: +61 2 9517 2249
Fax: +44 (0)1235 465 555 Email: [email protected]
Email: [email protected]
Distribution in the USA and Canada:
Royal Society of Medicine Press Ltd
c/o BookMasters, Inc
30 Amberwood Parkway
Ashland, Ohio 44805, USA
Tel: +1 800 247 6553 / +1 800 266 5564
Fax: +1 419 281 6883
Email: [email protected]
Phototypeset by Phoenix Photosetting, Chatham, Kent
Printed in Europe by the Alden Group, Oxford
INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES 270

iii
Contents
ivContributors
1Introduction
Section 1: Management of Acute Otitis Media
2Susceptibility and resistance of acute otitis media pathogens
MICHAEL R JACOBS
8The changing microbiology of acute otitis media
CHRISTOPHER HARRISON
11Clinical application to paediatrics
ALBERT M COLLIER
Section 2: Management of Other Common Bacterial Infections
15Therapeutic developments in the management of other common
bacterial infectionsHYMAN W FISHER
20Conclusion
21University of Kentucky Medical Center:
CME, CPE, CNE accreditation
INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES 270

Contributors
Dr Albert M Collier, MDPROFESSOR OF PEDIATRICS AND CHIEF OF PEDIATRIC INFECTIOUS DISEASE,
UNIVERSITY OF NORTH CAROLINA MEDICAL SCHOOL, CHAPEL HILL, NORTH CAROLINA, USA
Dr Hyman W Fisher, MD, FACPLECTURER, DEPARTMENT OF COMMUNITY AND PREVENTIVE MEDICINE,
MOUNT SINAI SCHOOL OF MEDICINE, NEW YORK UNIVERSITY MEDICAL CENTER, NEW YORK, USA
Dr Christopher Harrison, MDPROFESSOR OF PEDIATRICS AND PEDIATRIC INFECTIOUS DISEASES,
UNIVERSITY OF MISSOURI/CHILDREN’S MERCY HOSPITAL AND CLINICS, KANSAS CITY, MISSOURI, USA
Dr Michael R Jacobs, MD, PhD, MRCPROFESSOR OF MICROBIOLOGY, CASE WESTERN UNIVERSITY AND DIRECTOR OF CLINICAL
MICROBIOLOGY, UNIVERSITY HOSPITALS OF CLEVELAND, CLEVELAND, OHIO, USA
Dr Craig Martin, PharmD, BCPSCLINICAL PHARMACY SPECIALIST IN INFECTIOUS DISEASES,
UNIVERSITY OF KENTUCKY MEDICAL CENTER, LEXINGTON, KENTUCKY, USA
INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES 270
iv

University of Kentucky Medical CenterCME, CNE or CPE Accreditation
The University of Kentucky College of Medicine is accredited by the Accreditation Council for
Continuing Medical Education (ACCME) to sponsor continuing medical education for physicians.
Accreditation Statement
This activity has been planned and implemented in accordance with the Essential Areas and poli-
cies of the Accreditation Council for Continuing Medical Education through the joint sponsorship
of the University of Kentucky College of Medicine and the Royal Society of Medicine Press. The
University of Kentucky College of Medicine is accredited by the ACCME to provide continuing
medical education for physicians.
The University of Kentucky College of Medicine designates this educational activity for a
maximum of one (1.0) AMA PRA Category 1 Credits™. Physicians should only claim credit com-
mensurate with the extent of their participation in the activity.
The University of Kentucky College of Medicine presents this activity for educational purposes
only. Participants are expected to utilize their own expertise and judgment while engaged in the
practice of medicine. The content of the presentations is provided solely by presenters who have
been selected for presentations because of recognized expertise in their field.
The University of Kentucky College of Pharmacy is approved by the Accreditation
Council for Pharmacy Education as a provider of continuing pharmacy education.
This activity has been assigned ACPE # 022-999-07-074-H04 and will award one
(1.0) contact hours (0.1 CEUs) of continuing pharmacy education credit in states that
recognize ACPE providers. Statements of credit will indicate hours and CEUs based on success-
ful completion of a posttest (score 70% or higher) and will be issued within ten business days. The
college complies with the Criteria for Quality for continuing education programming.
Educational Review Systems is an approved provider of continuing education in nursing by ASNA,
an accredited provider by the ANCC/Commission on Accreditation. Provider # 5-115-07-029.
This program is approved for up to one (1.0) hour.
Educational Review Systems is also approved for nursing continuing education by the state of
California and the District of Columbia.
Disclosure Statement and Information
Faculty presenters of continuing education activities sponsored by the University of Kentucky
Colleges of Pharmacy and Medicine Continuing Education Office are expected to disclose any
real or perceived conflict of interest related to the content of their presentations.
The University of Kentucky Colleges of Pharmacy and Medicine Continuing Education Office
endorses the standards of the Accreditation Council for Continuing Medical Education and the
guidelines of the Association of American Medical Colleges that the speakers at continuing med-
ical education activities disclose relevant relationships with commercial companies whose prod-
ucts or services are discussed in educational presentations.
v
✂✂

Relevant relationships include receiving from a commercial company: research grants, consultant
fees, honoraria, and travel or other benefits, or having a self-managed equity interest in a com-
pany. Disclosure of a relationship is not intended to suggest or condone any bias in any presen-
tation, but is made to provide participants with information that might be of potential importance
to their evaluation of a presentation.
Relevant relationships exist with the following companies/organizations whose products or ser-
vices may be discussed:
Dr Albert M Collier MD has disclosed the following:
Speakers Bureau – Abbott Pharmaceuticals; Aventis Pharmaceuticals; GlaxoSmithKline
Pharmaceuticals; Lupin Pharmaceuticals; MedImmune Pharmaceuticals; Merck Pharmaceuticals;
Pfizer Pharmaceuticals; Wyeth Pharmaceuticals
Dr Hyman W Fisher MD:
Has nothing to disclose
Dr Christopher Harrison MD has disclosed the following:
Research grants – Wyeth Laboratories; Sanofi-Pasteur; Astellas Inc
Consultant – Abbott Pharmaceuticals; Sanofi-Aventis Pharmaceuticals; TM-Bioscience; Lupin
Pharmaceuticals
Speakers Bureau – Sanofi-Pasteur; Merck Inc; Abbott Pharmaceuticals
Dr Michael R Jacobs MD has disclosed the following:
Research grants – Abbott Pharmaceuticals; ARPIDA Pharmaceuticals; Aventis Pharmaceuticals;
Basilea Pharmaceuticals; Bristol-Myers Squibb Pharmaceuticals; Bayer Pharmaceuticals; Daiichi
Pharmaceuticals; Dr Reddy’s Laboratory; Eli Lilly & Co; GlaxoSmithKline Pharmaceuticals; Meji
Pharmaceuticals; Ortho-McNeil Pharmaceutical; Pfizer, Inc; Rambaxy Laboratories; Roche
Pharmaceuticals; TAP Pharmaceuticals; Warner-Lambert Pharmaceuticals; Wockhardt
Pharmaceuticals; Wyeth Ayerst/Lederle Pharmaceuticals
Consultant – Abbott Pharmaceuticals; Aventis Pharmaceuticals; Bristol-Myers Squibb
Pharmaceuticals; Bayer Pharmaceuticals; GenSoft Pharmaceuticals; Lupin Pharmaceuticals;
Ortho-McNeil Pharmaceutical; Sanofi-Aventis Pharmaceuticals; TAP Pharmaceuticals;
Wockhardt Pharmaceuticals; Wyeth Ayerst/Lederle Pharmaceuticals
Speakers Bureau – Bayer Pharmaceuticals; GlaxoSmithKline Pharmaceuticals; Ortho-McNeil
Pharmaceutical
Dr Craig Martin PharmD, BCPS:
Research grants – Ortho-McNeil Pharmaceutical
Speakers Bureau – Astellas Inc; Schering-Plough; Cubist Pharmaceuticals; Ortho-McNeil
Pharmaceutical; Wyeth Pharmaceuticals
vi
✂✂

INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES 270
Introduction
Needs statement
The management of common bacterial infections is a continually changing field. Muchdiscussion surrounds the relevance of new developments in scientific understanding, as wellas the most appropriate approach to the management of these troublesome conditions.Acute otitis media (AOM) in particular poses management problems because, if untreated ortreated inappropriately in children younger than two years, it can lead to seriouscomplications. Although treatment of AOM with antibiotics is not always essential in theolder and non-symptomatic patient, antibiotics do resolve symptoms more often in the firstfour days, and, in almost half of patients, effective antibiotic therapy more rapidly resolvesthe problem compared with no antibiotic treatment.
Learning objectives
This publication discusses the management of common bacterial infections, focusing onAOM. In July 2006, a number of physicians with differing interests in the field of AOM metto attempt to translate the science into clinical practice. Their objectives were to:
● review the scientific literature specific to antibacterial resistance and susceptibility in AOM● discuss the shift in pathogens that has occurred since the introduction of the
pneumococcal 7-valent conjugate vaccine (PCV-7)● discuss how to translate scientific data into clinical application ● discuss the role of other therapeutic alternatives in the current environment and their
position in the treatment armamentarium.
This publication contains a summary of some of the presentations that took place duringthat meeting, which were published as part of the Royal Society of Medicine Press’sInternational Congress and Symposium Series (ICSS) – ICSS 265: Acute Otitis Media:Translating Science into Clinical Practice (2007), and also a review of treatment approaches inother common bacterial infections.
Target audience
This activity is designed for general practitioners, paediatricians, nurses and pharmacists.
Release date: July 1, 2007Expiration date: July 1, 2008
1
EMERGING PROBLEMS IN THE MANAGEMENT OF PAEDIATRIC ACUTE OTITIS MEDIA AND OTHER BACTERIAL INFECTIONS.
EDITED BY ALBERT M COLLIER, HYMAN W FISHER, CHRISTOPHER HARRISON, MICHAEL R JACOBS, CRAIG MARTIN, 2007
INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES NO 270 PUBLISHED BY THE ROYAL SOCIETY OF MEDICINE PRESS LIMITED

Susceptibility and resistance of acute otitis
media pathogensMICHAEL R JACOBS
Many physicians assume that an organism will be susceptible to an antibiotic because it hasnot developed resistance to that antibiotic, but this is a common misconception. In fact,the drug must have adequate pharmacokinetic characteristics to treat baseline or wild-typeorganisms. Furthermore, some organisms have intrinsic resistance to antibiotics, but this isoften overlooked, as acquired resistance has been the focus of most research in this field.
In vitro activity
To make decisions on prescribing in clinical practice, the in vitro susceptibility of abacterium must first be measured in the laboratory. This is achieved by identifying theminimum inhibitory concentration (MIC) of the micro-organism. The MIC50 is theconcentration of antibiotic needed to inhibit 50% of the strains in a population and theMIC90 the concentration needed to inhibit 90% of strains. It is important to note that thesevalues do not indicate 50% or 90% inhibition of one strain: even when the MIC90, forexample, is low, some strains may still be resistant.
A population of bacteria with no acquired mechanism of resistance produces a distributionof MIC values – the baseline MIC range – which usually has one peak, similar to a bell-shaped curve. When a mechanism of resistance is developing in a population of bacteria, abimodal population, which has two peaks, is usually produced; widely separated MIC50 andMIC90 values provide a clue that this may be the case. Unfortunately, the literature usuallyonly provides MIC50 or MIC90 values rather than the full MIC distribution.
Susceptibility breakpoints are discriminatory antimicrobial concentrations that can be usedto differentiate MICs into susceptible, intermediate and resistant categories.
In vivo activity
The most important determinant of clinical outcome in an infectious disease, such as acuteotitis media (AOM), is eradication of infection, as bacterial survival is likely to lead toclinical failure. Two factors are important in overcoming bacterial infections: host defences
2
EMERGING PROBLEMS IN THE MANAGEMENT OF PAEDIATRIC ACUTE OTITIS MEDIA AND OTHER BACTERIAL INFECTIONS.
EDITED BY ALBERT M COLLIER, HYMAN W FISHER, CHRISTOPHER HARRISON, MICHAEL R JACOBS, CRAIG MARTIN, 2007
INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES NO 270 PUBLISHED BY THE ROYAL SOCIETY OF MEDICINE PRESS LIMITED
INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES 270

3
MICHAEL R JACOBS
and antibiotics. Without host defences, antibiotics cannot eradicate bacteria – they kill orinhibit most of the bacteria but never eradicate the entire population. The role of anantibiotic, therefore, is to aid host defences.
With respiratory tract infections (RTIs) treated on an outpatient basis, it is difficult to showwhether or not antibiotics have a significant impact, as these diseases have high rates ofspontaneous resolution. Most clinical outcome studies are comparative and do not includeplacebo arms. Unfortunately, therefore, they are unable to demonstrate the efficacy ofantibiotics. Studies that determine bacterial outcome, however, can show differencesbetween agents.
Pharmacokinetics and pharmacodynamics
A drug’s pharmacokinetics (PK) consider its serum concentration profile and penetration tothe site of infection, providing an indication of the drug’s fate after administration. A drug’spharmacodynamics (PD) consider its in vivo efficacy, based on whether it producesconcentration- or time-dependent killing and whether it has persistent (post-antibiotic)effects. Integration of PK and PD parameters has allowed us to predict in vivo efficacy basedon in vitro susceptibility and the PK/PD interactions discussed above.
Time-dependent and concentration-dependent agents
For time-dependent agents, such as β-lactams, in vivo killing does not occur until the serumconcentration of unbound drug reaches the MIC. After the concentration reaches the MIC,organisms are killed until the drug concentration falls to below the MIC, and the populationthen increases until the next dose is given and the concentration again reaches the MIC.
For concentration-dependent agents, such as macrolides and quinolones, bacterial killingbegins once an inhibitory concentration is reached; this is followed by a post-antibioticeffect by which killing or inhibition continues. Only when the post-antibiotic effect stopscan the bacterial population begin to increase again.
Studies have shown that the drug concentration needs to be above the MIC for 40% of thedosing interval for penicillins and 50% for cephalosporins.1 The efficacy of drugs againstpenicillin-susceptible Streptococcus pneumoniae varies considerably, and, as spontaneousresolution occurs in about 15–20% of cases in placebo studies with S. pneumoniae, any drugsthat achieve 20% eradication are no more effective than placebo, with the host defences infact eradicating the bacteria. The situation is similar with Haemophilus influenzae, for whichplacebo studies show spontaneous resolution in almost 50% of cases.
Susceptibility breakpoints based on PK/PD parameters
For time-dependent agents, the breakpoint that will differentiate between clinicalsusceptibility and resistance is the free serum concentration present for 40–50% of thedosing interval. For concentration-dependent agents, the breakpoint is the unbound serum24-hour area under the curve (AUC24) divided by 30. Table 1 shows the susceptibility ofisolates at PK/PD breakpoints;2 it is important to note that these data were reported beforethe pneumococcal 7-valent conjugate vaccine (PCV-7) was introduced to the US.

SUSCEPTIBILITY AND RESISTANCE OF ACUTE OTITIS MEDIA PATHOGENS
Clinical studies
Marchant et al showed very elegantly that a comparison of the bacteriological efficacies oftheoretical drug A and theoretical drug B could be used to determine the sample size neededto distinguish between a drug with differing activities by calculating bacteriological efficacyof theoretical drug A versus B (%) against the number of patients required.3 The resultsshowed that studies that use bacteriological diagnoses and outcomes (where a repeat tap istaken after 4–6 days) need to include about 660 patients to show a difference between a drugwith 80% bacteriological efficacy and one with 90% bacteriological efficacy, but only about100 patients to show a difference between a drug with 60% bacteriological efficacy and onewith 90% bacteriological efficacy. For a study involving a bacteriological diagnosis but aclinical outcome after 7–10 days (an initial tap but clinical criteria for outcome), about 250patients are needed to distinguish between a good drug and placebo, while about 800patients are needed to distinguish between a good drug and a mediocre drug. With theweakest study design, where both diagnosis and outcome are judged on clinical terms only,540 patients are needed just to distinguish a good drug from placebo. Most studies in AOMuse this last study design, but if a study includes fewer than 500 patients, it is not powered toshow a difference – irrespective of the efficacy of the drugs compared.
The results of a study in which children were given amoxicillin orally at a dose of 15mg/kg/day three times a day or 25 mg/kg/day twice a day (45–50 mg/kg/day) and serumdrug levels were measured can be used to show the application of pharmacokinetics.4 Whenthe PK/PD parameter for amoxicillin is applied (i.e. serum concentration greater than theMIC for ≥40% of the dosing interval) to these amoxicillin dosing regimens (45–50
4
Table 1 Susceptibility of isolates at pharmacokinetic/pharmocodynamic breakpoints. Adapted from Sinus and
Allergy Health Partnership.2
Drug Susceptible PK/PD Percentage of strains susceptible at PK/PD breakpoint
breakpoint (µg/ml)
S. pneumoniae H. influenzae M. catarrhalis
Co-amoxiclav 2† 92 98 100
Co-amoxiclav 4‡ 95 100 100
Amoxicillin 2† 92 70 7
Amoxicillin 4‡ 95 70 7
Cefaclor 0.5 20 4 9
Cefixime 1 66 100 100
Cefpodoxime 0.5 75 100 85
Cefprozil 1 72 23 9
Cefuroxime axetil 1 73 83 51
Cefdinir 0.25 69 78 78
Azithromycin 0.12 71 2 100
Clindamycin* 0.25 91 0 0
Levofloxacin 2 99 100 99
Trimethoprim–
sulfamethoxazole** 0.5† 64 78 19
*Based on NCCLS breakpoints
†Based on amoxicillin at 45 mg/kg/day
‡ Based on amoxicillin at 90 mg/kg/day
**Based on trimethoprim component.

5
MICHAEL R JACOBS
52
80
75
67
57
37
27
17
20
4
5
7
0
0
0
0 20 40 60 80 100
Placebo
Clarithromycin
Erythromycin
Azithromycin
Cefprozil
Cefaclor
Cefdinir 25QD
Cefuroxime
Amox-clav45
Amox-clav90
Cefpodoxime
Cefixime
Ceftriaxone 1 dose
Ceftriaxone 3 doses
Gatifloxacin
(a)
(b)
52
63
50
806040200
Placebo
Amoxicillin 45
Trimethoprim–
sulfamethoxazole
23
0
Susceptible
Resistant
Figure 1 Bacteriological failure rates in studies of AOM: H. influenzae for antibiotics excluding amoxicillin and
trimethoprim–sulfamethoxazole (a); and for amoxicillin and trimethoprim–sulfamethoxazole (b).5-10
mg/kg/day in divided doses), a serum drug concentration of 1 mg/ml was present for ≥40%of the dosing interval in 99% of subjects. A serum drug concentration of 2 mg/ml for ≥40%of the dosing interval was achieved in 82% of subjects. These results support the use of thesusceptible amoxicillin breakpoint established for a dose of 45 mg/kg/day in divided doses at2 mg/ml, while a breakpoint of 4 µg/ml can be achieved at a dose of 90 mg/kg/day in twodivided doses. These data predict that isolates with MICs of up to 2 µg/ml would beeradicated by amoxicillin at 45 mg/kg/day. Indeed, Dagan et al 5 found that eradication of S.pneumoniae was achieved in most patients, with only a few failures seen at amoxicillin MICsof 2 and 4 µg/ml. Only occasional failures were found when the dose was increased to 90mg/kg/day.6 The calculated breakpoint for azithromycin6 is 0.1 µg/ml; when organismswere resistant with MICs >0.1 µg/ml, the failure rate was about 80% – exactly the same aswas found in initial placebo studies. That more failures occurred around the breakpoint withazithromycin-susceptible strains than with amoxicillin shows that azithromycin is not aseffective as amoxicillin against susceptible strains.
Figures 1 and 2 show bacteriological failure rates from all published studies in AOM with abacteriological outcome obtained via tympanocentesis on day 2–6 of treatment.5–10 For H.influenzae, placebo resulted in 52% bacteriological failure, and the figures show that manyagents have efficacy only as good as or even worse than placebo, with the macrolidesclarithromycin, erythromycin and azithromycin, as well as cefprozil, having no activityagainst this organism. Cefixime and ceftriaxone are highly active against H. influenzae, withvery low bacteriological failure rates. For S. pneumoniae,8,9 the failure rate for placebo isabout 80%. When the results are divided into subsets of penicillin-susceptible andpenicillin-non-susceptible strains, most of the cephalosporins have relatively good efficacyand amoxicillin excellent efficacy against penicillin-susceptible strains, but for penicillin-

SUSCEPTIBILITY AND RESISTANCE OF ACUTE OTITIS MEDIA PATHOGENS
non-susceptible strains, many of the antibiotics show failure. This is not surprising, aspenicillin-non-susceptibility also predicts non-susceptibility to oral cephalosporins. Evenone-dose ceftriaxone was not adequate to treat some penicillin-non-susceptible S.pneumoniae.
Summary
In vitro susceptibility can be accurately interpreted on the basis of PK/PD parameters. Theprinciples of PK and PD can be used to:
● develop effective dosing regimens for antimicrobials● develop new formulations and dosage regimens● contribute to guideline recommendations
References
6
Placebo
Cefprozil*
Cefaclor
Cefdinir 25QD
Cefuroxime
Amox-clav45
Amoxicillin 45
Amox-clav90
Cefpodoxime*
Cefixime*
Ceftriaxone 1 dose
Ceftriaxone 3 doses
Gatifloxacin
(a)
(b)
81
92
73
100806040200
81
27
17
8
10
962
43
219
1020
1000
0
0
9
9
7
0 20 40 60 80 100
Placebo
Azithromycin
Trimethoprim–
sulfamethoxazole
5
0
53
Susceptible
Resistant
Penicillin–susceptible
Penicillin–non-susceptible
Figure 2 Bacteriological failure rates in studies of AOM: S. pneumoniae for antibiotics excluding azithromycin
and trimethoprim–sulfamethoxazole (a); and for azithromycin and trimethoprim–sulfamethoxazole (b).5-10 *, No
penicillin-non-susceptible isolates in these studies.
1. Craig WA. Basic pharmacodynamics of
antibacterials with clinical applications to the use
of beta-lactams, glycopeptides, and linezolid.
Infect Dis Clin North Am 2003: 17: 479–501.
2. Sinus and Allergy Health Partnership.
Antimicrobial treatment guidelines for acute
bacterial rhinosinusitis. Otolaryngol Head Neck
Surg 2000; 123(Suppl 1): S1–32.

MICHAEL R JACOBS
3. Marchant CD, Carlin SA, Johnson CE, Shurin
PA. Measuring the comparative efficacy of
antibacterial agents for acute otitis media: the
‘Pollyanna phenomenon’. J Pediatr 1992; 120:
72–7.
4. Fonseca W, Hoppu K, Rey LC, Amaral J, Qazi S.
Comparing pharmacokinetics of amoxicillin given
twice or three times per day to children older
than 3 months with pneumonia. Antimicrob Agents
Chemother 2003; 47: 997–1001.
5. Dagan R, Hoberman A, Johnson C et al.
Bacteriologic and clinical efficacy of high dose
amoxicillin/clavulanate in children with acute
otitis media. Pediatr Infect Dis J 2001; 20: 829–37.
6. Hoberman A, Dagan R, Leibovitz E et al. Large
dosage amoxicillin/clavulanate, compared with
azithromycin, for the treatment of bacterial acute
otitis media in children. Pediatr Infect Dis J 2005;
24: 525–32.
7. Hoberman A. Extra-strength amoxicillin/
clavulanate (A/C-ES) versus azithromycin (AZI)
for acute otitis media (Ace) in children. Abstract
presented at the 43rd Annual Interscience Conference
on Antimicrobial Agents and Chemotherapy,
Chicago, IL, USA, 14–17 September 2003
(Abstract G-459).
8. Jacobs MR. Optimisation of antimicrobial therapy
using pharmacokinetic and pharmacodynamic
parameters. Clin Microbiol Infect 2001; 7: 589–96.
9. Arguedas A, Dagan R, Leibovitz E et al. A
multicenter, open label, double tympanocentesis
study of high dose cefdinir in children with acute
otitis media at high risk of persistent or recurrent
infection. Pediatr Infect Dis J 2006; 25: 211–18.
10. Leibovitz E, Piglansky l, Raiz S et al.
Bacteriological efficacy of gatifloxacin (GATI) in
the treatment of recurrent/non-responsive acute
otitis media (RNR-AOM). Abstract presented at the
41st Annual Interscience Conference on Antimicrobial
Agents and Chemotherapy, Chicago, IL, USA,
16–19 December 2001 (Abstract G-1558a).
7

8
The changing microbiology of acute
otitis mediaCHRISTOPHER HARRISON
The three major middle ear pathogens over the years have been Streptococcus pneumoniae(pneumococcus), non-typeable Haemophilus influenzae, and Moraxella catarrhalis. AsMoraxella is much less difficult to treat, the focus for choosing antimicrobials to treat acuteotitis media (AOM) has been directed by resistance patterns among pneumococcus and non-typeable H. influenzae. In pneumococci, the major mechanism of antibiotic resistance(penicillin resistance caused by alterations in penicillin-binding proteins (PBPs)) alsoproportionally conveys resistance to the cephalosporins and increases the likelihood that thesame strain contains acquired resistance to trimethoprim–sulfamethoxazole and macrolides.β-lactamase production has been the major mechanism of resistance among non-typeable H.influenzae in the USA for the last 30 years.
When clinicians choose an antibiotic to treat AOM, they must have a clear understanding ofthe patterns of antibiotic resistance in their geographical area and the advantages or adverseeffects of the candidate antibiotics. Resistance patterns in the literature can vary by thepopulation of patients studied as well as the era in which the studies are performed. It is alsoimportant to understand that the rate of spontaneous cure of AOM depends on thepathogen, age of the patient (more commonly older than two years), immune status andfunction of the Eustachian tube.
Otopathogens in the 2000s – the effect of PCV-7
Pneumococcal 7-valent conjugate vaccine (PCV-7) came into universal use as part of theinfant immunization schedule in the US, but not other countries, in 2000. This introductionseems to have had a striking impact on middle ear pathogens from patients failing initialantibiotic therapy. This became clear when a study from rural Kentucky and a study fromsuburban Rochester revealed remarkably similar results when comparing the dominantpathogens and their resistance patterns from before and after introduction of PCV-7.1,2
In the pre-vaccine era, S. pneumoniae accounted for nearly 50% of isolates (with equalnumbers of middle ear isolates with high and intermediate penicillin resistance andpenicillin-susceptibility) and H. influenzae for around 40%. The proportion of β-lactamase-producing H. influenzae was higher in rural Kentucky than in suburban Rochester (about40% vs 25–30%), although the increase in β-lactamase production seen in Rochester wasstill sizeable. After the vaccine was introduced, the pneumococcal contribution to AOM
INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES 270
EMERGING PROBLEMS IN THE MANAGEMENT OF PAEDIATRIC ACUTE OTITIS MEDIA AND OTHER BACTERIAL INFECTIONS.
EDITED BY ALBERT M COLLIER, HYMAN W FISHER, CHRISTOPHER HARRISON, MICHAEL R JACOBS, CRAIG MARTIN, 2007
INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES NO 270 PUBLISHED BY THE ROYAL SOCIETY OF MEDICINE PRESS LIMITED

9
CHRISTOPHER HARRISON
pathogens decreased by about one-half and the H. influenzae contribution increased byabout one-third. Among patients who had failed previous antibiotic therapy, non-typeableH. influenzae now made up 56% of isolates in rural Kentucky and suburban New York, andtwo-thirds of these produced β-lactamase. A proportional decrease was also seen inpenicillin-resistant strains of S. pneumoniae in both centres. The comparability of data fromthese geographically distinct centres gives credence to a change to non-typeable H.influenzae as the dominant middle ear pathogen and an increase in β-lactamase-producingHaemophilus strains during this part of the post PCV-7 era.
Figure 1 shows a series of isolates from patients with AOM and acute bacterial rhinosinusitis(ABRS) obtained in Louisville during 2000–05 (Harrison C, unpublished data). Prior to fullimplementation of PCV-7 (2000 to 2001), vaccine types predominated, including serotypes19F, 14, 9V and 6B. Type 4 was observed in small numbers. During 2002–05, when morechildren had been immunized with PCV-7, serotypes 14 and 9B had disappeared, whileserotypes 6B, 19F and 23F had maintained a presence, although at a lower level than beforethe vaccine was introduced.
Serotype substitution was also observed, as non-vaccine serotypes 3, 11 and 33 became morecommon after introduction of the vaccine. This confirms the observation of a group inFinland that non-vaccine serotypes of S. pneumoniae might emerge to take advantage ofEustachian tube dysfunction in young children, even when they have antibody against theseven vaccine strains.3 The data from Finland did not suggest that serotypes that were cross-reactive with the vaccine types would emerge; however, data from the US obtained since theintroduction of PCV-7 revealed that 6A and particularly 19A had become major players
30%
25%
20%
15%
10%
5%
0%
3 7 11 15 33
V 4
V 6
B
V 9
V
V 1
4
V 1
8C
V 1
9F
V 2
3F
X 6
X 6
A
X 6
C
X 1
8
X 1
8F
X 9
X 1
9
X 1
9A
X 2
3
2000-22001-12001-22002-12002-22003-12003-22004-12004-22005-1
2005-2
Isolates of S. pneumoniae
Figure 1 Isolates of S. pneumoniae obtained from patients with AOM and acute bacterial rhinosinusitis in
Louisville, 2000–05. V designates PCV-7 types and X designates PCV-7 cross-reactive types.

10
THE CHANGING MICROBIOLOGY OF ACUTE OTITIS MEDIA
among S. pneumoniae causing AOM and acute bacterial rhinosinusitis in immunized childrenin the Louisville area. Interestingly, in 2002, serotype 19F alone comprised almost 30% ofthe total AOM isolates. However, while serotype 19F had decreased by 2005, serotype 19Ahad increased so that 19A together with 19F comprised the same 30% of total AOMisolates. It thus seems that 19A serotype substituted sufficiently for 19F so that no realchange in serogroup 19 isolates occurred. Of more concern is that 19A isolates seem to havehigher levels of amoxicillin resistance than the previously commonly seen 19F strains.
Summary
In 1970–80, H. influenzae was at least as important as, if not more important than S.pneumoniae in AOM. Neither β-lactamase-producing H. influenzae nor penicillin-resistant S.pneumoniae were seen in clinically important numbers. In the 1980s, a gradual increase inthe proportion of cases of AOM caused by S. pneumoniae was seen, and β-lactamase-producing organisms (mostly non-typeable H. influenzae) became more important inrecurrent AOM. Non-typeable β-lactamase-producing H. influenzae became the main targetfor therapy in patients failing previous antibiotic therapy and those patients who sufferedfrequent recurrences. In the 1990s, the situation changed because of the increase inpenicillin-non-susceptible S. pneumoniae. S. pneumoniae therefore became the majorpathogen in patients with treatment failures and frequent AOM recurrences. β-lactamase-producing H. influenzae was still a concern, but it had dropped to second place as a cause oftreatment failures when compared with penicillin-non-susceptible S. pneumoniae. Since year2000, with the advent of universal use of PCV-7 in infancy, a decrease in the proportion ofpenicillin-non-susceptible S. pneumoniae was observed, and H. influenzae (particularlyβ-lactamase-producing H. influenzae) have become more important causes of AOMtreatment failure. Despite this, it is essential to remember that S. pneumoniae is still thepathogen involved in about one-third of treatment failures and that about half of those aredue to penicillin-non-susceptible S. pneumoniae.
References
1. Casey JR, Pichichero ME. Changes in frequency
and pathogens causing acute otitis media in
1995–2003. Pediatr Infect Dis J 2004; 23: 824–8.
2. Block SL, Hedrick J, Harrison CJ et al.
Community-wide vaccination with the
heptavalent pneumococcal conjugate significantly
alters the microbiology of acute otitis media.
Pediatr Infect Dis J 2004; 23: 829–33.
3. Eskola J, Kilpi T, Palmu A et al. Efficacy of a
pneumococcal conjugate vaccine against acute
otitis media. N Engl J Med 2001; 344: 403–9.

11
Clinical application to paediatricsALBERT M COLLIER
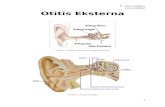
Relationship between immunity in the foetus and young child andrespiratory illnesses
The pathogenesis of acute otitis media (AOM) and the balance between host and pathogenare important in understanding the aims of treatment with antibiotics. Immunoglobulin G(IgG) is an important molecule for immunity. Figure 1 illustrates the pattern of levels ofIgG in a child from conception through to the age of nine years.1 After the fourth month offoetal age, the pregnant mother begins to pass her own IgG molecules through the placenta,so that, by birth, the baby has a level of IgG greater than 100% of the mother’s. Althoughbabies born premature and weighing <1000 g are much more likely to survive now thanmany years ago, they are still more susceptible to infections because, in part, they have notreceived the maximum amount of IgG from their mother before birth. After birth andseparation from the placenta, levels of IgG decrease very rapidly, with viral antibodiesremaining longer than bacterial antibodies. At about 10–11 months, all of the maternalantibodies for bacteria have disappeared.
At about 7.5 months of foetal age, the foetal immune system itself begins to manufactureIgG, but the levels increase very slowly, with much maturation of the immune systemoccurring after birth. Not until the child is aged two years does it have a levelcommensurate with even 80% of that of its mother. The nadir of IgG concentration is atnine months, which, in longitudinal studies, is the time of the peak incidence of AOM andprior to conjugate (Hib) vaccine of Hib meningitis.2 Indeed, Figure 2, when compared withFigure 1, shows an inverse relation between the incidence of respiratory illnesses by age andlevels of IgG antibodies by age in children, with the incidence of respiratory illnessespeaking in the second six months of life, when the mother’s antibodies are diminishing andthe child’s own immune system is still maturing, with the IgG levels slowly rising.
Otopathogens
Currently, the major pathogens of interest in AOM are Haemophilus influenzae andStreptococcus pneumoniae.
S. pneumoniae was discovered in 1880 by Pasteur, who also disproved spontaneousgeneration and proved the tenet of infectious diseases – that a person must be colonized
INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES 270
EMERGING PROBLEMS IN THE MANAGEMENT OF PAEDIATRIC ACUTE OTITIS MEDIA AND OTHER BACTERIAL INFECTIONS.
EDITED BY ALBERT M COLLIER, HYMAN W FISHER, CHRISTOPHER HARRISON, MICHAEL R JACOBS, CRAIG MARTIN, 2007
INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES NO 270 PUBLISHED BY THE ROYAL SOCIETY OF MEDICINE PRESS LIMITED

12
CLINICAL APPLICATION TO PAEDIATRICS
with an organism before that organism can cause disease. Most often, the organism isacquired through contact with another person infected or colonized with the organism,which is important in explaining the changing epidemiology of AOM in children. In 1968 inNorth Carolina, for example, only 1% of children younger than five years were in day careand children had little regular contact with other children, perhaps attending Sunday schoolonce a week during the first years of life; in 2006, however, 78% of children younger thanfive years were in day care and thus having regular contact with other young children.
H. influenzae was discovered by Pfeiffer in 1892, when the organism was isolated from anumber of patients during the influenza pandemic. In the 1930s, Dr Margaret Pittman, as aproject for her PhD in microbiology at the University of Pennsylvania, Philadelphia, wasasked to obtain isolates of H. influenzae from children with meningitis, to produce antiserain rabbits and to identify any different serotypes. She identified six types, which she nameda–f, by making antibodies to the polysaccharides in the capsules that surrounded the
2 3 4 5 6 7 8 9
Age (years)Fetal age (months)
100
Transplacentally acquired Endogenous production
Total
80
60
40
20
0
Perc
enta
ge o
f adult v
alu
es
Birth
1 2 3 4 5 6 7 8 9
0–1/20
2
4
6
8
10
8.1
1.2 1.10.4 0.5 0.4 0.3 0.5
10.4
7.7
6.3
4.63.8
Total respiratory illnesses
Lower respiratory illnesses
Re
sp
ira
tory
ill
ne
sse
s p
er
chil
d–y
ea
r
6.5
12
1/2–1 1–2 2–3
Age (years)
3–4 4–5 All ages
Figure 1 Levels of immunoglobulin G (IgG) at different ages. Adapted with permission from Goldman and
Goldblum.1
Figure 2 Frequency of respiratory illnesses by age.2

13
ALBERT M COLLIER
organisms. When the antibodies were added to the isolates and observed under themicroscope, each bacterial serotype could be identified by its reaction to the antisera, withthe correct antisera causing the capsule to swell up.
Dr John Robbins and Dr David Smith, who worked in competing laboratories, both isolatedthe serotype b polysaccharide, which helps the bacteria to evade phagocytosis and remain inthe bloodstream long enough to reach the large joints, pericardial space and meninges.They hypothesized that administration of this polysaccharide to children at two, four and sixmonths of age – before the peak incidence of meningitis – would encourage the children toproduce antibodies against H. influenzae type b. Disappointingly, the polysaccharide did nothave the desired effect, because children are unable to produce good antibodies topolysaccharide antigens until they reach the age of 18–24 months. The polysaccharide wasthen linked to a protein, which changed the evoked response from T-cell-independent toT-cell-dependent and resulted in the production of good antibodies against H. influenzaetype b as early as two months of age. The resultant vaccine produced a reduction in cases ofH. influenzae type b systemic disease from 20 000 cases a year in the US to around 100 casesin 2005. Unfortunately, as the H. influenzae that cause AOM are non-typeable, the vaccinehad no effect on surface infections such as AOM.
Of the 90 types of S. pneumoniae, seven serotypes were observed to predominate in invasivedisease. These seven are the types conjugated to protein carriers in the pneumococcal 7-valent conjugate vaccine (PCV-7). In contrast with the H. influenzae type b conjugatedvaccine, the same types of S. pneumoniae included in the pneumococcal conjugated vaccinealso predominate in AOM, so PCV-7 has had an effect on the incidence of mucosal surfaceinfections such as AOM. Furthermore, a high percentage (reportedly 30–65%) of thesePCV-7 strains had penicillin minimum inhibitory concentrations (MIC) >2 µg/ml. PCV-7not only promotes production of humoral circulating antibodies, but some antibody in theform of IgG seems to reach the mucosa. The surface antibody can prevent attachment andreduce colonization, which, ultimately, prevents disease.
Evolution of the spectrum of otopathogens
In the 1970s, S. pneumoniae and H. influenzae were common in children with AOM, butthere was no penicillin resistance in S. pneumoniae and minimal β-lactamase-positive H.influenzae.3–5 In the 1980s, a gradual increase was seen in S. pneumoniae and about 25% ofnon-typeable H. influenzae were β-lactamase-positive, which were the main pathogens seenin patients with treatment failure or recurrence.6 In the 1990s, there was an increase inpenicillin-non-susceptible S. pneumoniae, which became the major pathogen in failures andrecurrences; β-lactamase-positive H. influenzae remained an issue, but were less importantthan penicillin-non-susceptible S. pneumoniae.7–9 The 2000s have seen the conjugatedvaccine effect, in which there has been a decrease in the numbers of penicillin-non-susceptible S. pneumoniae, although with more of an effect with the intermediate thanresistant S. pneumoniae.10,11 A study by Casey and Pichichero highlights this gradual shift inincidence of pathogens found in cases of persistent AOM and treatment failures (Figure 3).In 1995–97, S. pneumoniae was the dominant organism, with H. influenzae having a lesserrole. By 1998–2000, around the time that the pneumococcal vaccine was introduced, thenumber of cases caused by each pathogen were comparable, but by 2001–03, H. influenzaewas the dominant organism and S. pneumoniae the minor contributor.12 Increases have beenseen in β-lactamase-positive H. influenzae, which, again, is the major pathogen in treatmentfailures and recurrences.10,11 It is important to note, however, that penicillin-non-susceptibleS. pneumoniae have not been completely eradicated, as recent serotype substitution may be

14
CLINICAL APPLICATION TO PAEDIATRICS
1995–97
30
40
50
60
Pe
rce
nta
ge
1998–2000 2001–03
S. pneumoniae
p � 0.017
H. influenzae
p � 0.012
Figure 3 Shift in incidence of pathogens found in persistent acute otitis media and treatment failures. Reproduced
from Casey and Pichichero.12
1. Goldman AS, Goldblum RM. Primary
deficiencies in humoral immunity. Pediatr Clin
North Am 1977; 24: 277–91.
2. Collier AM, Henderson FW. Respiratory disease
in infants and toddlers. In: Cryer D, Harms T, eds.
Infants and Toddlers in Out-of-Home Care.
Baltimore: Paul Brookes Publishing, 2000; 163–77.
3. Howie VM, Ploussard JH. Efficacy of fixed
combination antibiotics versus separate
components in otitis media. Effectiveness of
erythromycin estrolate, triple sulfonamide,
ampicillin, erythromycin estolate–triple
sulfonamide, and placebo in 280 patients with
acute otitis media under two and one-half years of
age. Clin Pediatr (Phila) 1972; 11: 205–14.
4. Leibovtiz E, Jacobs MR, Dagan R. Haemophilus
influenzae: a significant pathogen in acute otitis
media. Pediatr Infect Dis J 2004; 23: 1142–52.
5. Schwartz R, Rodriguez W, Khan W, Ross S. The
increasing incidence of ampicillin-resistant
Haemophilus influenzae. A cause of otitis media.
JAMA 1978; 239: 320–3.
6. Bluestone CD, Stephenson JS, Martin LM. Ten-
year review of otitis media pathogens. Pediatr
Infect Dis J 1992; 11: S7–11.
7. Harrison CJ, Chartrand SA, Pichichero ME.
Microbiology and clinical aspects of a trial of once
daily cefixime vs twice daily cefaclor for treatment
of AOM in infants and children. Pediatr Infect Dis
J 1993; 12: 62–9.
8. Gooch WM, III, Blair E, Puopolo A et al. Clinical
comparison of cefuroxime axetil and
amoxicillin/clavulanate in the treatment of
pediatric patients with AOME. Clin Ther 1995;
17: 838–51.
9. Pichichero ME, McLinn S, Aronovitz G et al.
Cefprozil treatment of persistent and recurrent
AOM. Pediatr Infect Dis J 1997; 16: 471–8.
10. Block SL, Hedrick JA et al. Five-day twice daily
cefdinir therapy for AOM: microbiologic and
clinical efficacy. Pediatr Infect Dis J 2000; 19:
S153–8.
11. Hoberman A, Dagan R, Leibovitz E et al. Large
dosage amoxicillin/clavulanate, compared with
azithromycin, for the treatment of bacterial AOM
in children. Pediatr Infect Dis J 2005; 24: 525–32.
12. Casey JR, Pichichero ME. Changes in frequency
and pathogens causing acute otitis media in
1995–2003. Pediatr Infect Dis J 2004; 23: 824–8.
13. Eskola J, Kilpi T, Palmu A et al. Efficacy of a
pneumococcal conjugate vaccine against acute
otitis media. N Engl J Med 2001; 344: 403–9.
14. Farrell D. Emergence and spread of
multiresistant Streptococcus pneumoniae serotype
19A clone in USA: focus on the pediatric
population. Abstract presented at the 46th
Interscience Conference on Antimicrobial Agents
and Chemotherapy, San Francisco, CA, USA,
27–30 September 2006.
occurring.13,14 Protection from the vaccine is thus not 100% and it only protects against thetypes in the vaccine. It is time to consider adding conjugated type 19A polysaccharide to thepneumococcal vaccine.
References

Therapeutic developments in the
management of other common
bacterial infectionsHYMAN W FISHER
The management of bacterial infections requires constant re-evaluation of the resistance toantibiotics of the bacteria that typically cause them. Susceptibility and resistance patterns ofthe pathogens found in acute otitis media (AOM) and the subsequent problems arising inthe management of this condition are discussed in other articles in this publication. Thisarticle considers how changes have been occurring in the antibiotic therapy of othercommonly encountered infections, including uncomplicated urinary tract infections (UTIs),pharyngitis, tonsillitis, acute bronchitis, acute exacerbations of chronic bronchitis, acutebacterial rhinosinusitis, and uncomplicated cervical and urethral gonorrhoea.
Uncomplicated urinary tract infections
Uncomplicated UTIs continue to be a common problem, and treatment of these infectionshas become more difficult because of the rising levels of resistance to commonly usedantibiotics.1,2
The 1999 guideline of the Infectious Diseases Society of America recommends a 3-daycourse of trimethoprim plus sulfamethoxazole (TMP-SMZ) as standard therapy for acutecystitis if the community resistance among uropathogens is <20%.3 The resistance ofEscherichia coli to TMP-SMZ has been increasing and is in the range of 20% or higher insome parts of the US and other countries; this has led to the testing of alternative agents,including b-lactams and fluoroquinolones, for the treatment of uncomplicated UTIs.3–5
A 2004 Swedish study of the distribution of and antimicrobial resistance in urinary tractpathogens, primarily E. coli, in children �2 years of age and adults 18 to 50 years of age,over a period of 12 years found that E. coli was the most common pathogen in both agegroups. E. coli resistance to ampicillin and trimethoprim was higher in children than inadults and increased over time in both age groups, while resistance to fluoroquinolones washigher in adults than in children, but also increased over time in both groups. It wasconcluded that the steadily increasing and now high E. coli resistance levels in children toampicillin and trimethoprim rendered empirical therapy with these drugs doubtful.6
INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES 270
EMERGING PROBLEMS IN THE MANAGEMENT OF PAEDIATRIC ACUTE OTITIS MEDIA AND OTHER BACTERIAL INFECTIONS.
EDITED BY ALBERT M COLLIER, HYMAN W FISHER, CHRISTOPHER HARRISON, MICHAEL R JACOBS, CRAIG MARTIN, 2007
INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES NO 270 PUBLISHED BY THE ROYAL SOCIETY OF MEDICINE PRESS LIMITED
15

MANAGEMENT OF OTHER COMMON BACTERIAL INFECTIONS
A randomized, prospective, multicentre study in Israel compared once-daily oral cefixime (8mg/kg) with twice daily oral TMP-SMZ (8/40 mg/kg/day) in the treatment of acute UTIsin children aged 6 months to 13 years. All Gram-negative organisms were susceptible tocefixime and 85% were susceptible to TMP-SMZ. It was concluded that the efficacy andsafety of cefixime administered once daily compared favourably with TMP-SMZadministered twice daily for acute uncomplicated UTIs in children.7
In a South African randomized study of acute uncomplicated UTIs in 528 patients whoreceived cefixime 400 mg once daily, cefixime 200 mg twice daily, or TMP-SMZ two tabletstwice daily for 10 days, cefixime 200 mg twice daily was found to be an effective and safealternative to TMP-SMZ.4
In a double-blind, randomized study of uncomplicated cystitis in Israeli women, it wasfound that a 3-day regimen of 400 mg cefixime administered once daily was as efficient as a3-day regimen of 200 mg ofloxacin administered twice a day.8
Pharyngitis and tonsillitis
Although penicillin has in the past been the primary agent recommended for the treatmentof tonsillo-pharyngitis caused by group A b-haemolytic streptococci (GABHS), there hasbeen, since the early 1980s, an increase in GABHS infections not cured by penicillintreatment, and this has led to the testing of alternative antibiotics.
A meta-analysis of randomized controlled trials comparing a cephalosporin versus penicillinin the treatment of bacteriologically confirmed GABHS tonsillo-pharyngitis included 35trials involving 7125 children. The overall summary odds ratios for both bacteriological andclinical cure rates significantly favoured cephalosporins compared with penicillin, with theindividual cephalosporins cephalexin, cefadroxil, cefuroxime, cefpodoxime, cefprozil,cefixime, ceftibuten and cefdinir showing superior bacteriological cure rates. This meta-analysis indicates that the likelihood of bacteriological and clinical success in GABHStonsillo-pharyngitis is significantly greater if an oral cephalosporin is prescribed, comparedwith oral penicillin.9
Although cephalosporins are in general active against Streptococcus pyogenes and are thereforeof value in the treatment of tonsillo-pharyngitis, they have not yet been shown to preventrheumatic fever.10
Acute bronchitis and acute exacerbations of chronic bronchitis
Acute bronchitis and acute exacerbations of chronic bronchitis are frequently caused byStreptococcus pneumoniae and Haemophilus influenzae – organisms that are becoming moreresistant to narrow-spectrum b-lactams such as penicillin and amoxicillin. Extended-spectrum cephalosporins are among the antibiotics that retain activity against many resistantstrains of these organisms.
Comparative trials have shown that the clinical and bacteriological efficacy of cefixime200–400 mg daily administered as a single dose or in two divided doses is comparable withthat of cefaclor, amoxicillin, or amoxicillin/clavulanic acid in acute lower RTIs. Cefixime isconsidered a suitable alternative to cefaclor or amoxicillin in acute lower RTIs.11
16

17
HYMAN W FISHER
A multicentre trial involving 167 patients in Germany compared a 5-day course of cefixime400 mg/day with a standard 10-day course of the same daily dose of cefixime in thetreatment of acute exacerbations of chronic bronchitis, and found that the 5-day course oftherapy was equivalent in efficacy to the standard 10-day course, and may offer costadvantages.12
Acute bacterial rhinosinusitis
The most common bacterial species isolated from the maxillary sinuses of patients withacute bacterial rhinosinusitis are S. pneumoniae, H. influenzae, and Moraxella (Branhamella)catarrhalis, the latter being more common in children. Other streptococcal species,anaerobic bacteria, and Staphylococcus aureus cause a small percentage of cases.13 Bacterialresistance is a growing problem in the treatment of rhinosinusitis. Approximately 25% of S.pneumoniae strains are penicillin-resistant and about 30% of H. influenzae and essentially allM. catarrhalis isolates produce b-lactamases. Resistance of H. influenzae to TMP-SMZ isalso common.14
Treatment of acute maxillary sinusitis (AMS) with amoxicillin has been reported to render S.pneumoniae and H. influenzae in recurrences resistant not only to amoxicillin but also to otherantibiotics.14 A study in the US of the antimicrobial susceptibility of organisms isolated fromthe nasopharynx of 70 children presenting with AMS or maxillary sinusitis that recurred afteramoxicillin therapy (RMS) found that treatment of AMS with amoxicillin increases thedevelopment of resistance of S. pneumoniae and H. influenzae isolates found subsequently,relative to treatment with co-amoxiclav, TMP-SMZ, cefprozil, cefuroxime axetil, cefdinir,cefixime or azithromycin. After amoxicillin therapy, resistance to cefprozil was present in 5%of AMS and 15% of RMS, to cefuroxime axetil in 5% and 10%, to cefdinir in 5% and 15%,and to cefixime in 11% and 30%, respectively.
The Sinus and Allergy Health Partnership, in the 2004 update of its 2000 treatmentguidelines for acute bacterial rhinosinusitis, recommends a respiratory fluoroquinolone orhigh-dose amoxicillin/clavulanate for initial therapy of adults with moderate acute bacterialrhinosinusitis or with mild disease who have received antibiotics in the previous 4–6 weeks.Alternative recommendations include parenteral ceftriaxone or combination therapy withhigh-dose amoxicillin or clindamycin plus cefixime, or high-dose amoxicillin or clindamycinplus rifampin.13
Support for the use of combination therapy consisting of ampicillin plus cefixime comesfrom in vitro studies showing synergy of these two agents against S. pneumoniae, includingpenicillin-resistant strains.15,16
Uncomplicated cervical or urethral gonorrhoea
The Centers for Disease Control and Prevention (CDC) updated its guidelines for thetreatment of gonorrhoea in April 2007 due to widespread resistance to the fluoroquinolones(increasing from 0.6% in 2001 to 6.7% in 2006 in the US). In some cities the increasesreported were more dramatic (e.g. Philadelphia rose from 1% in 2004 to 27% in 2006). Therecommended treatment alternatives for gonorrhoea include oral cefixime and intra-muscular ceftriaxone, these being the only two cephalosporin compounds recommended bythe CDC.17 Oral cefixime and intramuscular ceftriaxone are also the only recommended

MANAGEMENT OF OTHER COMMON BACTERIAL INFECTIONS
alternative first-line agents for the treatment of gonorrhoea in the UK. The general use ofciprofloxacin as first-line treatment stopped when resistance to it increased to >9% in2002.18
The French Agency for Health Product Safety recommends presumptive, simultaneoustreatment for both Neisseria gonorrhoeae and Chlamydia trachomatis in cases of uncomplicatedurethritis and cervicitis. For presumptive gonorrhoea, the Agency suggests a single dose ofcefixime (oral), ceftriaxone (intramuscular or intravenous), spectinomycin (intramuscular) orciprofloxacin (oral).19
Summary
Bacteria that cause common infections in children and adults are becoming increasinglyresistant to antibiotics, especially to b-lactam antibiotics. Extended-spectrum cephalosporinsprovide broad-spectrum coverage of Gram-positive and Gram-negative organismsassociated with many of the bacterial infections commonly encountered in clinical practice,including uncomplicated urinary tract infections, AOM, pharyngitis, tonsillitis, acutebronchitis, acute exacerbations of chronic bronchitis, acute sinusitis, and uncomplicatedgonorrhoea. These agents are important options in the therapeutic armamentarium for suchinfections, particularly in this era of increasing antimicrobial resistance and dwindlingtreatment choices.
References
18
1. Czaja CA, Hooton TM. Update on acute
uncomplicated urinary tract infection in women.
Postgrad Med 2006; 119: 39–45.
2. Wagenlehner FM, Naber KG. Treatment of
bacterial urinary tract infections: presence and
future. Eur Urol 2006; 49: 235–44.
3. Warren JW, Abrutyn E, Hebel JR et al.
Guidelines for antimicrobial treatment of
uncomplicated acute bacterial cystitis and acute
pyelonephritis in women. Infectious Diseases
Society of America (IDSA). Clin Infect Dis 1999;
29: 745–58.
4. Levenstein J, Summerfield PJ, Fourie S et al.
Comparison of cefixime and co-trimoxazole in
acute uncomplicated urinary tract infection. A
double-blind general practice study. S Afr Med J
1986; 70: 455–60.
5. Le TP, Miller LG. Empirical therapy for
uncomplicated urinary tract infections in an era
of increasing antimicrobial resistance: a decision
and cost analysis. Clin Infect Dis 2001; 33:
615–21.
6. Abelson SK, Osterlund A, Kahlmeter G.
Antimicrobial resistance in Escherichia coli in urine
samples from children and adults: a 12 year
analysis. Acta Paediatr 2004; 93: 487–91.
7. Dagan R, Einhorn M, Lang R et al. Once daily
cefixime compared with twice daily trimethoprim/
sulfamethoxazole for treatment of urinary tract
infection in infants and children. Pediatr Infect Dis
J 1992; 11: 198–203.
8. Raz R, Rottensterich E, Leshem Y, Tabenkin H.
Double-blind study comparing 3-day regimens of
cefixime and ofloxacin in treatment of
uncomplicated urinary tract infections in women.
Antimicrob Agents Chemother 1994; 38: 1176–7.
9. Casey JR, Pichichero ME. Meta-analysis of
cephalosporin versus penicillin treatment of
group A streptococcal tonsillopharyngitis in
children. Pediatrics 2004; 113: 866–82.
10. Chambers ST, Murdoch DR, Pearce MJ. Clinical
and economic considerations in the use of third-
generation oral cephalosporins. Pharmacoeconomics
1995; 7: 416–27.
11. Brogden RN, Campoli-Richards DM. Cefixime.
A review of its antibacterial activity.
Pharmacokinetic properties and therapeutic
potential. Drugs 1989; 38: 524–50.
12. Lorenz J. Comparison of 5-day and 10-day
cefixime in the treatment of acute exacerbation of
chronic bronchitis. Chemotherapy 1998; 44 (Suppl
1): 15–8.

19
13. Sinus and Allergy Health Partnership.
Antimicrobial treatment guidelines for acute
bacterial rhinosinusitis. Otolaryngol Head Neck
Surg 2000; 123 (Suppl 1): S1–32.
14. Brook I, Gober AE. Antimicrobial resistance in
the nasopharyngeal flora of children with acute
maxillary sinusitis and maxillary sinusitis
recurring after amoxicillin therapy. J Antimicrob
Chemother 2004; 53: 399–402.
15. Jones RN, Johnson DM. Combinations of orally
administered beta-lactams to maximize spectrum
and activity against drug-resistant respiratory
tract pathogens: I. Synergy studies of amoxicillin
and cefixime with Streptococcus pneumoniae. Diagn
Microbiol Infect Dis 1998; 31: 373–6.
16. Matsumoto Y. Combination cefixime/amoxicillin
against penicillin-resistant Streptococcus pneumoniae
infection. Chemotherapy 1998; 44 (Suppl 1): 6–9.
17. Centers for Disease Control and Prevention
(CDC). Update to CDC’s sexually transmitted
disease treatment guidelines, 2006: fluoro-
quinolones no longer recommended for treat-
ment of gonococcal infections. MMWR Morb
Mortal Wkly Rep 2007; 56: 332–6.
18. Ison CA, Mouton JW, Jones K et al. Which
cephalosporin for gonorrhoea? Sex Transm Infect
2004; 80: 386–8.
19. French Agency for Health Product Safety.
Antibiotherapy applied to uncomplicated
urethritis and cervicitis. Med Mal Infect 2006; 36:
27–35.
HYMAN W FISHER

Conclusion
The bacterial aetiology of common infections is changing and evolving, and this isparticularly evident with the spectrum of pathogens changing in response to, for example,immunization practices such as the introduction of the pneumococcal 7-valent conjugatevaccine (PCV-7). The existing recommendations for the management of AOM have somelimitations, and while high-dose amoxicillin certainly should be used initially, as per theAAP/AAFP’s guideline,1 physicians need to cover the emergence of resistant organisms,particularly Streptococcus pneumoniae and Haemophilus influenzae, in patients failing antibiotictherapy. Microbiological data suggest that cefixime has distinct advantages in specificsettings, such as the treatment of AOM where first-line therapy may be failing due tob-lactamase-producing H. influenzae. Furthermore, a prescription of combinationamoxicillin and cefixime oral suspension would bring economic implications in terms ofreducing the number of follow-up visits. Clinical studies and evaluation will add credence tothis approach.
Reference
EMERGING PROBLEMS IN THE MANAGEMENT OF PAEDIATRIC ACUTE OTITIS MEDIA AND OTHER BACTERIAL INFECTIONS.
EDITED BYALBERT M COLLIER, HYMAN W FISHER, CHRISTOPHER HARRISON, MICHAEL R JACOBS, CRAIG MARTIN, 2007
INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES NO 270 PUBLISHED BY THE ROYAL SOCIETY OF MEDICINE PRESS LIMITED
1. American Academy of Pediatrics/American
Academy of Family Physicians Subcommittee on
Management of Acute otitis Media. Clinical
Practice Guideline. Diagnosis and Management
of Acute Otitis Media. Leawood, KS. American
Academy of Pediatrics/American Academy of
Family Physicians, 2004. Available at:
www.aafp.org.
INTERNATIONAL CONGRESS AND SYMPOSIUM SERIES 270
20

Emerging Problems in the Managementof Paediatric Acute Otitis Media and
Other Bacterial Infections
Released: July 1, 2007 Expires: July 1, 2008
TEST CODE: XEN07247
To claim CE credit, participants must complete the activity, posttest and evaluation. To do so
online and receive your statement of credit immediately, go to www.CECentral.com/getcredit
and enter code XEN07247
You can also mail this form, postmarked by July 1, 2008, to: Attn: Distance Education,
University of Kentucky Pharmacy and Medicine, Continuing Education Office, One Quality
Street, 6th Floor, Lexington, KY 40507-1428
Name: ________________________________________________________________________
Credentials: __________________________ Speciality: ________________________________
Address: ______________________________________________________________________
City: __________________________________________ State: __________ Zip: __________
Daytime Phone: ______________________________ Fax: _____________________________
E-mail: ________________________________________________________________________
Please specify what type of credit you are claiming:
I claim (1.0) AMA PRA Category 1 CreditsTM.
I claim (1.0) contact hour (0.1 CEU) of continuing pharmacy education credit
I claim (1.0) hour of continuing nursing education credit
Signature: _____________________________________________________________________
Post-Test Answers (circle the correct answer)
1. TRUE FALSE 6. A B C D
2. A B C D 7. A B C
3. A B C D 8. TRUE FALSE
4. TRUE FALSE 9. A B C
5. TRUE FALSE 10. A B C D
Evaluation Poor Satisfactory Excellent
1. Extent to which the objectives were achieved: 1 2 3 4 5
2. Potential impact on your practice: 1 2 3 4 5
3. Detail of information presented: 1 2 3 4 5
4. Extent to which commercial bias appeared: 1 2 3 4 5
5. Overall evaluation of CME, CPE or CNE activity: 1 2 3 4 5
6. Suggestions for future CME, CPE or CNE topics: 1 2 3 4 5
The Univeristy of Kentucky is an equal opportunity university
21
✂✂

University of Kentucky Medical Center
Emerging Problems in the Management of Paediatric Acute
Otitis Media and Other Bacterial Infections (XEN07247)
1. It is common knowledge that pathogens that have not developed resistance to an antibiotic
will be susceptible to that antibiotic.
True � False �
2. Studies have shown that to be effective the drug concentration for cephalosporins needs to
be above the MIC for what percentage of the dosing interval?
a. 15–20% c. 40%
b. 25% d. 50%
3. Marchant et al showed that to differentiate between a drug with 60% bacteriological effi-
cacy and one with 90% a clinical study using both bacteriological diagnoses and outcomes
would require how many patients?
a. 100 c. 540
b. 250 d. 660
4. Non-typeable b-lactamase producing H.influenzae remains as the major pathogen in
patients with treatment failures and frequent AOM recurrences.
True � False �
5. The polysaccharide-protein linked vaccine that has resulted in a marked reduction in cases
of H. influenzae type b systemic disease is proving to be equally effective in the treatment of
AOM.
True � False �
6. The rate of spontaneous cure of AOM depends upon which of the following:
a. the pathogen c. the patient’s immune status
b. the age of the patient d. all of the above
7. Comparative trials have shown that cefixime is a suitable alternative to which of the fol-
lowing in the treatment of acute, uncomplicated urinary tract infections?
a. trimethoprim plus sulfamethoxazole c. both of the above
b. amoxicillin
8. According to the results of a meta-analysis of trials comparing a cephalosporin against
penicillin in cases of bacteriologically confirmed tonsillo-pharyngitis due to group A beta-
haemolytic streptococci in children, the likelihood of bacteriological and clinical success is
significantly greater with a penicillin than with a cephalosporin.
True � False �
9. According to a multicenter trial conducted in Germany, the standard 10-day course of
cefixime 400 mg/day may be shortened to how many days of the same dose of cefixime and
still have the same efficacy in the treatment of acute exacerbations of chronic bronchitis?
a. 3 days c. 7 days
b. 5 days
10. Which of the following pathogens commonly implicated in bacterial rhinosinusitis is/are
presenting a problem due to an increasing number of strains producing b-lactamases?
a. S. pneumoniae c. M. catarrhalis
b. H. influenzae d. All of the above
22
✂✂