Emergency Medicine Approach To Pleural Effusion
60
Approach To Pleural Effusion = On Short Notice = By Dr. Nawaf Al-Amri M.D Saudi Board Emergency Medicine Riyadh Military Hospital
-
Upload
dr-nawaf-al-amri -
Category
Education
-
view
6.504 -
download
2
description
An Approach To Pleural Effusion From Emergency Medicine Point Of View , Done On Short Notice Referenced From Rosen , Tentennali , UpToDate , JAMA , BMJ
Transcript of Emergency Medicine Approach To Pleural Effusion

Approach To
Pleural Effusion= On Short Notice =
By
Dr. Nawaf Al-Amri M.DSaudi Board Emergency Medicine
Riyadh Military Hospital

What Should You Grasp After This ?
• 1- You Cant Do A Proper Presentation In 5 Days• 2- Definition Of Pleural Effusion• 3- Normal Physiology & Pathophysology• 4- Causes ?• 5- Types & Classification• 6- Clinical Features & Assessment• 7- Diagnosis And Treatment • 8- Most Recent Evidence In Emergency Medicine

Definitions
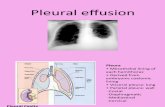
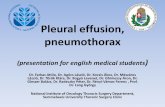
- What Is Pleural Effusion ?
• Pleural effusion results from fluid accumulating in the potential space between the visceral and parietal pleurae When there is an imbalance between formation and absorption in various disease states , in response to injury , inflammation, or both locally and systematically .

More Definitions ?
• Parapneumonic Effusion : pleural effusion associated with bacterial pneumonia, bronchiectasis, or lung abscess .
• Complicated Parapneumonic Effusion : refers to parapneumonic effusions that require tube thoracostomy for their resolution .
• Loculated Effusion : Fluid anatomically confined and not freely flowing in the pleural space when there are adhesions between the visceral and the parietal pleura .
• Sub-Pulmonic Effusion: accumulation of fluid between the lung & the diaphragm which gives the false impression of an elevated hemi-diaphragm


Normal Physiology• Up to 25 ml of pleural fluid is normally present in the pleural space which is an
amount not detectable on conventional chest radiographs , and is secreted from the parietal pleura into the pleural space where it is absorbed by the visceral pleural microcirculation .
• This small amount of pleural fluid reduces friction between the pleural layers and allows for smooth lung expansion and contraction with respiration.
• Rate entry into the pleural space in normally 0.01 ml/kg per hour.
• Any process that increases fluid production or interferes with fluid absorption will result in accumulation in the pleural space.
• Normal amount 8.4 ml per hemithorax with a WBC count of 1700 per c.mm 75% of which are macrophages and 23% lymphocytes. Protein concentration is low about 15% of plasma protein concentration.

Pathophysiology
• Pleural fluid is produced from systemic capillaries at the parietal pleural surface and absorbed into pulmonary capillaries at the visceral pleural surface.
• Lymphatics also play an important role in removing pleural fluid. Movement of fluid across the pleural surfaces is governed by Starling’s law.
• Under normal circumstances, the direction of pleural fluid flow is largely governed by the difference in hydrostatic pressure between the systemic and the pulmonary circulations

Pathophysiology• Pleural fluid exists in a dynamic equilibrium in which influx equals
efflux, with approximately 1 L of fluid traversing the pleural space in 24 hours.
• Under normal conditions, the amount of fluid that remains in the pleural space is small ( 0.1–0.2 mL/kg body weight) and clinically or ∼radiographically undetectable.
• Pleural effusion develops whenever influx of fluid into the pleural space exceeds efflux.
• Numerous disorders can lead to formation of a pleural effusion. Pleural effusions classically are divided into two groups—transudates and exudates—according to the composition of the pleural fluid

Pathophysiology
Rate of Fluid Rate of FluidAccumulation Removal
1. Altered Pleural Membrane Permeability2. Decreased Intravascular Oncotic Pressure3. Increased Capillary Hydrostatic Pressure4. Lymphatic Obstruction5. Abnormal Sites of Entry


Pathophysiology
• Pulmonary Capillary Pressure (CHF)
• Capillary Permeability (Pneumonia)
• Intrapleural Pressure (Atelectasis)
• Plasma Oncotic Pressure (Hypoalbuminemia)
• Pleural Membrane Permeability (Malignancy)
• Lymphatic Obstruction (Malignancy)
• Diaphragmatic Defect (Hepatic Hydrothorax)
• Thoracic Duct Rupture (Chylothorax)
Pleural effusion has several origins :

Causes ?
• These Are The Most Common :
- Congestive Heart Failure (MCC)- Malignancy
- Bacterial Pneumonia- Pulmonary Embolism
- TB

Other Causes & Associates ?• Cirrhosis • Ascites• Peritoneal dialysis• Nephrotic syndrome• All kinds of infections of the lung parenchyma or pleura ( B , V , F , P )• Uremia• Myxedema• Ovarian hyperstimulation syndrome• Collagen vascular diseases ( SLE , RA )• Intra-abdominal processes ( Acute pancreatitis, subphrenic abscess) • Esophageal perforation • Bacterial pneumonia with parapneumonic effusion • Post Chemo-Radiotherapy• Drug-related : Amiodarone, Nitrofurantoin , Dantrolene ,
Methysergide , Bromocriptine , Procarbazine • Lung & breast cancer • Lymphoma• Meigs syndrome .• Psuedocyst . • Mesothelioma • SVC syndrome• Yellow-nail syndrome
• Diaphragmatic hernia• Post abdominal surgery • Endoscopic variceal sclerotherapy • Post liver transplant• Immunoblastic lymphadenopathy • Sjögren's syndrome • Wegener's granulomatosis• Churg-Strauss syndrome• Post-coronary artery bypass surgery • Asbestos exposure • Sarcoidosis• Trapped lung • Radiation therapy • Post-cardiac injury syndrome • Hemothorax • Iatrogenic injury • Pericardial disease • Chylothorax• Urinothorax• Postpartum• Glomerulonephritis

Types ?
– Transudate : result from an imbalance between hydrostatic (e.g., CHF) and oncotic (e.g., nephrotic syndrome) pressures. This imbalance results in the production of an ultrafiltrate with low protein content across the pleural membrane.
– Exudate : result from pleural disease, usually inflammation or neoplasia, that results in active fluid secretion or leakage with high protein content.
– Empyema : Requires the presence of bacteria on Gram’s staining of the pleural fluid.
– Hemothorax & Chylothorax : From rupture of the thoracic duct are special instances of pleural effusion

Types ?

Types ?

Types ?
• Transudates are essentially ultrafiltrates of plasma, contain ing very little protein. A transudative effusion develops when there is an increase in the hydrostatic pressure or decrease in the oncotic pressure within pleural microvessels.
• The primary cause of increased hydrostatic pressure is congestive heart failure, which is responsible for about 90% of transudative effusions. In hepatic cirrhosis and nephrotic syndrome, increased hydrostatic pressure is combined with loss of plasma oncotic pressure because of significant decreases in serum albumin.
• Patients with severe malnutrition may develop transudative effusions resulting from severe isolated hypoalbuminemia.

Types ?
• Exudates contain relatively high amounts of protein, reflecti ng an abnormality of the pleura itself.
• An exudative effusion is the result of increased membrane permeability or defective lymphatic drainage. Any pulmonary or pleural process associ ated with inflammation can result in an exudative effusion.
• In the absence of clinically apparent effusion, pleuritic symptoms may still be present.
• The most common form of exudative effusion is a parapneumonic effusion, in which infection of the adjacent lung elicits an intense inflammatory response in pleura, disrupting normal membrane permeability.

Types ?
• Malignant effusions are the second most common form of exudative effu sion and often reflect alterations in pleural permeability and problems with lymphatic drainage.
• Exudative effusions also may arise in response to inflammatory abdominal processes, such as pancreatitis or subphrenic abscess, presumably owing to altered permeability of the diaphragm itself.
• Exudative effusions may be reabsorbed or organize into fibrous tissue, resulting in pleural adhesions.

Types ?
• Some pleural effusions can present as either transudates or exudates or may have characteristics of both. In the case of pulmonary embolism, the pathogenesis of pleural effusion is often multifactorial, reflecting increased pulmonary vascular pressure (a transudative process) and ischemia and breakdown of the pleural membrane (an exudative process).
• Massive effusions (>1.5–2 L) are most commonly associated with malignancy but also can arise in the setting of congestive heart failure, cirrhosis, and other conditions.
• Massive effusions may restrict respiratory movement, compress the lungs, and result in intrapulmonary shunting. In extremely rare cases, tension hydrothorax can develop, with mediastinal shift and circulatory embarrassment.

Transudates Vs. Exudates

Clinical Features
• History :– Dyspnea– Pleuritic chest pain– Cough – Fever– Hemoptysis– Wt. loss– Trauma– Hx. of cancer– Cardiac surgery
• Physical :– Dullness to percussion– Decreased breath sounds– Absent tactile fremitus– Other findings: ascites,
JVP, peripheral edema, friction rub, unilateral leg swelling

Clinical Features• Symptoms associated with pleural effusion are most often due to the
underlying disease process and not the effusion itself.
• Small pleural effusions can be entirely asymptomatic.
• A new pleural effusion may be heralded by localized pain or pain referred to the shoulder.
• Viral pleuritis and pulmonary infarction commonly are associated with pleuritic chest pain.
• When the volume of pleural fluid reaches 500 mL, dyspnea on exertion or at rest may occur as a result of compromised pulmonary function.

Clinical Features• The patient’s history often helps to establish the diagnosis for pleural effusion or pleural
inflammation.
• A history of congestive heart failure, liver disease, uremia, or malignancy can direct subsequent evaluation.
• The pain of viral pleuritis usually is preceded by several days of a typical viral prodrome, with low-grade fever, sore throat, and other upper respiratory or constitutional symptoms.
• In the absence of such prodromal symptoms, an alternate etiology for pleuritis such as pulmonary embolism must be sought.
• Physical findings depend on the size of the effusion but are often either dominated or obscured by the underlying disease process.
• Classic physical signs of pleural effusion include diminished breath sounds, dullness to percussion, decreased tactile fremitus, and occasionally a localized pleural friction rub.

Clinical Features• The simple technique of auscultatory percussion (i.e., percussing
the chest while listening for a dullness with the stethoscope) may be even more sensitive and specific for the physical diagnosis of pleural effusion.
• Egophony and enhanced breath sounds can often be appreciated at the superior border of the effusion because of underlying atelectatic lung tissue.
• In the setting of pleuritis, a pleural friction rub may be appreciated. With massive effusions, signs of mediastinal shift may be present.

Clinical Features• A pleural effusion may be clinically silent or come to detection from either
symptoms of an underlying disease, an increase in volume of the effusion with the production of dyspnea, or the development of inflammation and associated pain with respiration.
• Physical findings of a pleural effusioninclude percussion dullness and decreased breath sounds.
• Because pleural fluid typically pools in the dependent portions of the hemithorax, small or moderate size effusions have percussion dullness and decreased breath sounds at the lung base with relatively normal lung findings above the level of fluid.
• With large or massive effusions, it may be impossible to distinguish a fluid level on clinical examination.

Clinical Features
• Large Effusions that prevent contact between the Visceral & Parietal Pleura during respiration are
seldom associated with pleuritic chest pain.
• Tumors involving the parietal pleura generally produce constant dull pain
• Large effusions interfere with expansion of the lung and produce dyspnea, shortness of breath, and atelectasis

Clinical Features
• Distended neck veins, an S3 gallop, or peripheral edema suggests >>>> CHF
• A right ventricular heave or thrombophlebitis and sinus tachycardia suggests >>>> PE
• The presence of lymphadenopathy or hepatosplenomegaly suggests >>>> Cancer
• Ascites may suggests >>>> ESLD
• Signs of consolidation above the level of the fluid in a febrile patient suggests >>>> Parapneumonic Effusion.

Diagnosis

Diagnosis
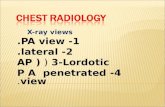
Role Of Chest X-Rays
- Detection and the differential diagnosis are highly dependent upon imaging of the pleural space.
- Conventional radiographic methods used are frontal, lateral, oblique and decubitus radiographs.
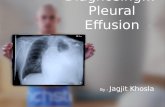
- Blunting of either costophrenic angle is indicative of the accumulation of between 250 - 500 ml of fluid
- Lateral-Decubitus films (that allow fluid to shift to the dependent portion of the thoracic cavity) help differentiate fluid from pleural thickening & fibrosis
- Because of gravity, fluid accumulates in subpulmoniclocation and then spills over into the costophrenic sulcus posteriorly, anteriorly, and laterally and then surrounds the lung forming a cylinder, seen as a meniscoid arc.

Diagnosis
– 75 mL-subpulmonic space without spillover, can obliterate the posterior costophrenic sulcus,
– 175 mL is necessary to obscure the lateral costophrenic sulcus on an upright chest radiograph
– 500 mL will obscure the diaphragmatic contour on an upright chest radiograph;
– 1000 ml of effusion reaches the level of the fourth anterior rib,
– On decubitus radiographs and CT scans, less than 10 mL, and possibly as little as 2 mL, can be identified

Diagnosis
– Small effusions are thinner than 1.5 cm, moderate effusions are 1.5 to 4.5 cm thick, and large effusions exceed 4.5 cm.
– Effusions thicker than one cm are usually large enough for sampling by thoracentesis, since at least 200 mL of liquid are already present
• A significant pleural effusion is large enough to produce a pleural fluid strip >10 mm wide on lateral decubitus radiographic views

Diagnosis

Diagnosis
Role of CT scan
– Visualization of underlying lung parenchymal processes that are obscured on chest radiographs by large pleural effusions
– Very Sensitive
– Can distinguish between Lung Abscess & Empyema

Diagnosis

Diagnosis
Role of Ultrasonography
– Free vs loculated pleural effusions, and iloculated effusions vs solid masses.
– Thoracentesis of loculated pleural effusions is facilitated by ultrasound marking or guidance.
– Helpful in Confirming the Presence of a Small Pleural Effusion.

Diagnosis

Diagnosis
Role of MRI
– Can display pleural effusions, pleural tumors, and chest wall invasion.
– Can characterize the content of pleural effusions.
– Can determine the age of the hemorrhage.

Diagnosis

Diagnosis
Diagnostic Thoracentesis- An unexplained pleural effusion requires further investigation. Unless required
to rule out an immediately life-threatening condition such as empyema or hemothorax, pleural fluid evaluation may be deferred to an inpatient or outpatient setting.
- Likely indicated in most patients .
- > 1 cm layering on lateral decubitus
- No need for thoracentesis for patient with obvious cause may not need further study (CHF with bilateral effusions) .
- Indicated if the effusion is clinically significant with no known cause.

Diagnosis
• Also indicated in a patient with CHF if any of the following are present.
A unilateral effusion, particularly if it is left-sided, Bilateral effusions, but are of disparate sizes There is evidence of pleurisy or feverThe cardiac silhouette appears normal on CXR If no response to diuresis in 48-72 hrs.The alveolar-arterial oxygen gradient is widened out
of proportion to the clinical setting

DiagnosisContraindications :
- None Absolute.
- Relative include :
• Patient on anticoagulation or with bleeding diathesis
• Very small volume of fluid.
• Patients are mechanical ventilation though not at increased risk for pneumothorax are at high risk for tension pneumothorax or persistent airleak
• Active skin infection at the port of entry.

Diagnosis• Post procedure CXR :
- Indicated only if air is obtained during the procedure or if cough, pain or dyspnea develops.
• Complications :
- Pain >>> Give Pain Medications NSAIDs Sometimes Opiods - Bleeding (hematoma, hemothorax, or hemoperitoneum) >>> Fluids - Pneumothorax >>> Multi-Dependence - Empyema >>> Sterility - Soft tissue infection >>> Sterility - Spleen or liver puncture >>> Ultrasound Guided - Vasovagal events >>> Multi-Dependence - Seeding the needle tract with tumor >>> Very Unfortunate !! - Adverse reactions to lidocaine or topical antiseptic solutions >>> Ask About it - Retained intrapleural catheter fragments >>> CXR

Diagnosis
Thoracentesis: Transudate vs. Exudate
1. Gross Appearance2. Cell Count & Differential3. Gm Stain, C & S4. Cytology5. LDH6. Protein7. Glucose, Amylase

Transudate
straw-colored, clear, odorless fluid with a WBC less than 1000 / ul
• Pleural Membranes are Intact • Secondary to Altered Starling Forces• Low in Protein & other Large Molecules
CHF, Cirrhosis, Nephrotic SyndromeHypoalbuminemia, Constrictive
Pericarditis, SVC Obstruction, PE

Exudate
• Characterized by Increased Protein & LDH[Pleural Fluid vs. Serum Levels]
• Secondary to Disruption of Pleural Membrane or Obstruction of Lymphatic Drainage
Parapneumonic, Infections, Malignancy, Vasculitic Disease, GI Disease, TB, PE

Appearance
- Bloody : Cancer, PE, Trauma, Pneumonia.
- Turbid : either due to cells or debris or a high lipid level.
- Putrid Odor : Anaerobic infection
- Ammonia Odor : Urinothorax

a bloody pleural effusionoccurring in a patient without a history of trauma
or pulmonary infarctionis
Indicative of Neoplasm in 90 % of cases!
• Because a RBC count as low as 5000 - 10,000 /ul, can cause a pleural effusion to turn red, the finding of blood-tinged fluid per se has little diagnostic value
(usually from needle trauma)
• A True Hemothorax is when the Pleural Fluid Hct exceeds 50 % of the Peripheral Blood Hct !
• Beware Of Aortic Aneurisms !!!

Further Workup Based On Appearance
• Bloody : Hematocrit compared to the blood :– <1% is nonsignificant– 1-20% indicates either cancer, PE or trauma– >50% indicates hemothorax.
• Cloudy or Turbid – Centrifugation : – Turbid supernatant indicates high lipid levels– Check TG - >110mg/dl – chylothorax– If TG>50mg/dl and cholesterol>250 – pseudochylothorax
• Putrid odour – Stain and Culture = Bacterial

Treatment
• Transudative Effusion :
focus on the systemic cause , rule out a diagnosis of congestive heart failure, cirrhosis, or pulmonary embolism.
• Exudative Effusion :
dependent on the exact sub-type , send for total and differential cell counts, smears and cultures for organisms, measurement of glucose and lactate dehydrogenase levels, cytologic analysis, and testing for a pleural-fluid marker of tuberculosis.
• Consider Chest Thoracostomy :
• Gross Pus / Empyema• pH < 7.2• Hemothorax• Complicated Parapneumonic Processes• Malignant Effusions…but remember the role of pleurodesis!

PORCEL et al. AFP 2006; 73: 1212
Other Pleural Fluid Tests

PORCEL et al. AFP 2006; 73: 1212
Other Pleural Fluid Tests

PORCEL et al. AFP 2006; 73: 1212
Other Pleural Fluid Tests

PORCEL et al. AFP 2006; 73: 1212
Other Pleural Fluid Tests

Evidence Anyone ?• The diagnosis of pleural effusion by ultrasonic and radiologic techniques.• J Gryminski, • P Krakówka, and • G Lypacewicz
• Abstract• The value of the A-mode ultrasonic technique and the radiologic method in the diagnosis of pleural
effusion was assessed in 116 patients with diseases of the pleura. Ultrasonic and radiologic examinations, as well as needle punctures, were performed, and the results were compared statistically. The pleural fluid was detected by ultrasound in 93 percent (74) and by radiologic examination in 83 percent (66) of the 80 cases with such fluid. The absence of fluid was established by ultrasound in 89 percent (32/36) and by radiologic examination in 61 percent (22/36). For the first time the superiority of the ultrasonic method over the radiologic one was demonstrated, and the difference was most obvious in cases of small pleural effusion. Ultrasound permitted the detection of very small amounts (even 3 to 5 ml) of loculated pleural fluid. In contrast to the radiologic method, ultrasound permitted easy differentiation between loculated pleural fluid and pleural thickenings. The ultrasonic method appeared especially useful in the accurate localization and precise indicating of the site for needle aspiration of even the smallest fluid collections. It made possible thoracocentesis in 94 percent (154) of 163 instances. The practical value of the ultrasonic method, both in establishing diagnosis and in treatment, is emphasized.

Evidence Anyone ?• Intensive Care Med. 2011 Sep;37(9):1488-93. Epub 2011 Aug 2.• Lung ultrasound in critically ill patients: comparison with bedside chest radiography.• Xirouchaki N, Magkanas E, Vaporidi K, Kondili E, Plataki M, Patrianakos A, Akoumianaki E, Georgopoulos D.• Source• Department of Intensive Care Medicine, University Hospital of Heraklion, University of Crete, Heraklion, Crete, Greece.• Abstract• PURPOSE:• To compare the diagnostic performance of lung ultrasound and bedside chest radiography (CXR) for the detection of various
pathologic abnormalities in unselected critically ill patients, using thoracic computed tomography (CT) as a gold standard.• METHODS:• Forty-two mechanically ventilated patients scheduled for CT were prospectively studied with a modified
lung ultrasound protocol. Four pathologic entities were evaluated: consolidation, interstitial syndrome, pneumothorax, and pleural effusion. Each hemithorax was evaluated for the presence or absence of each abnormality.
• RESULTS:• Eighty-four hemithoraces were evaluated by the three imaging techniques. The sensitivity, specificity, and diagnostic
accuracy of CXR were 38, 89, and 49% for consolidation, 46, 80, and 58% for interstitial syndrome, 0, 99, and 89% for pneumothorax, and 65, 81, and 69% for pleural effusion, respectively. The corresponding values for lung ultrasound were 100, 78, and 95% for consolidation, 94, 93, and 94% for interstitial syndrome, 75, 93, and 92% for pneumothorax, and 100, 100, and 100% for pleural effusion, respectively. The relatively low sensitivity of lung ultrasound for pneumothorax could be due to small number of cases (n = 8) and/or suboptimal methodology.
• CONCLUSIONS:
• In our unselected general ICU population lung ultrasound has a considerably better diagnostic performance than CXR for the diagnosis of common pathologic conditions and may be used as an alternative to thoracic CT.

Evidence Anyone ?• Value of sonography in determining the nature of
pleural effusion: analysis of 320 cases.• P C Yang, K T Luh, D B Chang, H D Wu, C J Yu and S H Kuo
• Department of Internal Medicine, National Taiwan University Hospital, Taipei, Republic of China.
• Abstract
• To assess the value of sonography in determining the nature of pleural effusions, we prospectively analyzed the sonographic findings in 320 patients with pleural effusion of various causes (224 with exudates and 96 with transudates). The nature of the effusions was established on the basis of chemical, bacteriologic, and cytologic examination of pleural fluid; pleural biopsy; and clinical follow-up. All patients had high-frequency, real-time sonography performed by one of three sonographers who had no clinical information concerning the patients. The sonographer evaluated the images for internal echogenicity of the effusion, thickness of the pleura, and associated parenchymal lesions of the lung. The images were also printed out and interpreted a second time by the other two sonographers to reach a consensus.
• Our results showed that the two types of effusions could be distinguished on the basis of sonographic findings. Transudates were anechoic, whereas an anechoic effusion could be either a transudate or an exudate. Pleural effusions with complex septated, complex nonseptated, or homogeneously echogenic patterns were always exudates (p less than .01). Sonographic findings of thickened pleura and associated parenchymal lesions in the lung also were indicative of an exudate (p less than .01). Homogenous echogenic effusions were due to hemorrhagic effusion or empyema. Sonographic evidence of a pleural nodule was a specific finding in patients with a malignant effusion. We conclude that sonography is useful in determining the nature of pleural effusion.

Evidence Anyone ?• Sonographic Septation in Lymphocyte-Rich Exudative Pleural
Effusions A Useful Diagnostic Predictor for Tuberculosis
• Done By A Bunch Of Chinese MD’s ( Names Were Long And Annoyingly Hard To Spell )
• Division of Pulmonary and Critical Care Medicine, Department of Medicine, China Medical University Hospital, Taichung, Taiwan.
• Abstract• Objective. The purpose of this study was to evaluate the role of the sonographic features of lymphocyte-rich exudative
pleural effusions in the differential diagnosis of tuberculosis and lung cancer in an area with a high incidence of tuberculosis. Methods. Medical records of patients undergoing chest sonography between January 2003 and June 2005 (30 months) were reviewed retrospectively. The enrolled patients included 73 with lung cancer-related pleural effusions and 93 with tuberculous pleural effusions. The sonographic appearances of the pleural effusions were defined in terms of 4 patterns: anechoic, homogeneously echogenic, complex septated, and complex nonseptated. Results. Among the 73 lung cancer-related pleural effusions, there were sonographic appearances of an anechoic pattern in 11% (8/73), a complex septated pattern in 4% (3/73), and a complex nonseptated pattern in 85% (62/73). In 93 tuberculous pleural effusions, there were sonographic appearances of an anechoic pattern in 12% (11/93), a complex septated pattern in 47% (44/93), and a complex non-septated pattern in 41% (38/93). Apparently, a complex septated pattern in the sonographic appearance of lymphocyte-rich pleural effusions is a useful diagnostic predictor for differentiating tuberculosis from lung cancer (95% confidence interval, −0.57 to −0.29). If we define the complex septated pattern in the sonographic appearance of lymphocyte-rich exudative pleural effusions as a predictor for tuberculous pleural effusions, we can achieve sensitivity, specificity, positive predictive value, negative predictive value, and positive likelihood ratio values of 47%, 96%, 94%, 59%,
and 12, respectively.Conclusions. A complex septated pattern in the sonographic appearance is a useful predictor of tuberculosis in lymphocyte-rich exudative pleural effusions.

Evidence Anyone ?• Pleural Effusions in Febrile Medical ICU Patients Chest
Ultrasound Study• Same Group Of Annoying China Men• From the Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, China Medical University Hospital,
Taichung, Taiwan.• Study objectives: To assess the necessity of thoracentesis in febrile medical ICU (MICU) patients, and to evaluate the efficiency and
reliability of sonographic effusion patterns for diagnosing empyema.• Design and setting: A prospective, 1-year, tertiary-care hospital study of febrile MICU patients with physical, radiographic, and
ultrasonographic evidence of pleural effusion.• Patients: During this study period, we screened 1,640 patients who had been admitted to the MICU; of these, 94 patients had a
temperature > 38°C for > 8 h with evidence of pleural effusion proven by chest radiography and ultrasound.• Intervention: Routine thoracentesis and pleural effusion cultures were performed in 94 febrile patients under portable chest
ultrasound guidance. Three days later, if the first pleural effusion culture was inconclusive and the patient still had persistent fever of > 38°C, we repeated the diagnostic thoracentesis and pleural effusion culture. In total, 118 procedures were performed in those 94 febrile patients.
• Measurements and results: In all, 58 patients (62%) had infectious exudates (parapneumonic, n = 36; empyema, n = 15; urosepsis, n = 3; liver abscess, n = 2; deep neck infection, n = 1; and wound infection, n = 1), 28 patients (30%) had transudates, and 8 patients (8%) had noninfectious exudates. The prevalence of empyema in febrile patients admitted to the MICU was 16% (15 of 94 patients). Analyses of the sonographic patterns of the 15 patients with empyema out of the 118 thoracenteses performed showed the following: anechoic pattern, 0% (0 of 47 procedures); complex nonseptated and relatively nonhyperechoic pattern, 0% (0 of 36 procedures); complex nonseptated and relatively hyperechoic pattern, 100% (2 of 2 procedures); complex septated pattern, 35% (11 of 31 procedures); and homogenously echogenic pattern, 100% (2 of 2 procedures). Hemothorax was the only complication, and it occurred in two patients (2%). Both patients had a favorable outcome after drainage.
• Conclusion: Portable chest ultrasound examination and ultrasound-guided thoracentesis in febrile MICU patients are safe, feasible, and useful methods for diagnosing thoracic empyema. Our results suggest that only some sonographic patterns of pleural effusion (homogenously echogenic, complex nonseptated and relatively hyperechoic, and complex septated) deserve aggressive assessment and rapid management.

Thank You
Lets Watch This Video