
Electrocardiograma o essencial nos SCA - … · Electrocardiograma –o essencial nos SCA Pedro...
97
Electrocardiograma – o essencial nos SCA Pedro Silva Cunha Hospital de Santa Marta, Hospital Lusíadas Lisboa Pós-Graduação em Medicina de Emergência Abordagem urgente das Síndromes Coronárias Agudas (António Fiarresga, João Abecassis, Pedro Silva Cunha, Sílvio Leal)
-
Upload
trinhhuong -
Category
Documents
-
view
231 -
download
0
Transcript of Electrocardiograma o essencial nos SCA - … · Electrocardiograma –o essencial nos SCA Pedro...

Electrocardiograma – o essencial nos SCA
Pedro Silva Cunha
Hospital de Santa Marta, Hospital Lusíadas Lisboa
Pós-Graduação em Medicina de Emergência
Abordagem urgente das Síndromes Coronárias Agudas(António Fiarresga, João Abecassis, Pedro Silva Cunha, Sílvio Leal)
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas
ECG in STEMI•Definition of STEMI
–New ST elevation at the J point in two contiguous leads of >0.1 mV in all leads other than leads V2-V3
–For leads V2-V3 the following cut points apply: ≥0.2 mV in men ≥40 years, ≥0.25 mV in men <40 years, or ≥0.15 mV in women
•Other conditions which are treated as a STEMI
–New or presumed new LBBB
–Isolated Posterior MI
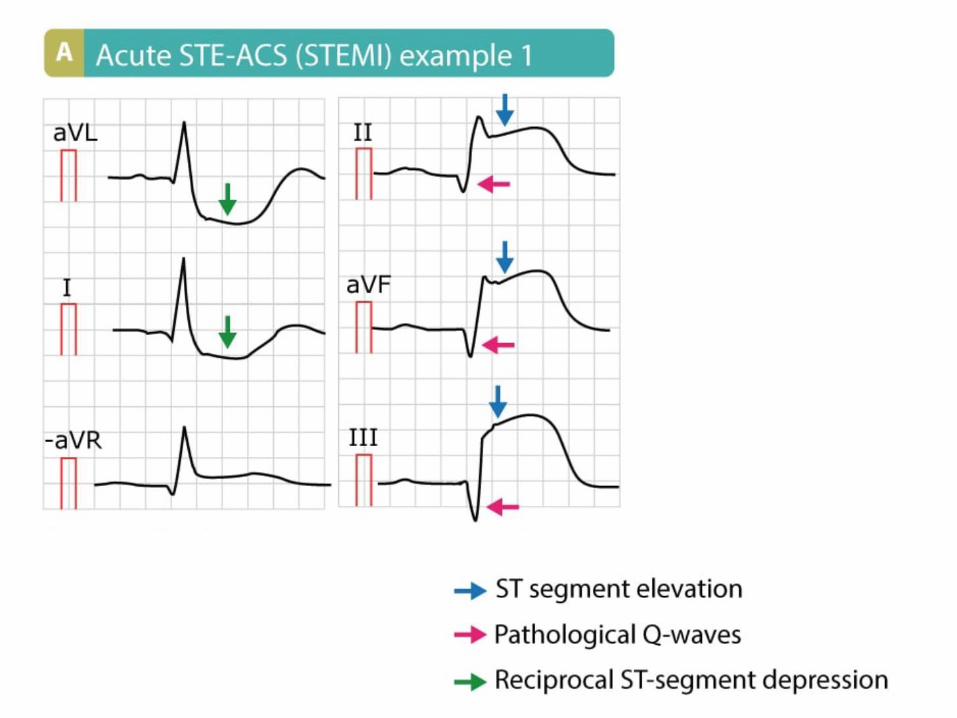
•The presence of reciprocal ST depression helps confirm the diagnosis
Bases Teóricas do ECG
O ECG Normal: Ondas e Intervalos
Determinação do Eixo Eléctrico
ECG Patológico
• Alterações das Aurículas
• Hipertrofia Ventricular
• Alterações da Condução Intraventricular
• Isquemia e Enfarte do Miocárdio
• Outros
INTERPRETAÇÃO DO ELECTROCARDIOGRAMA
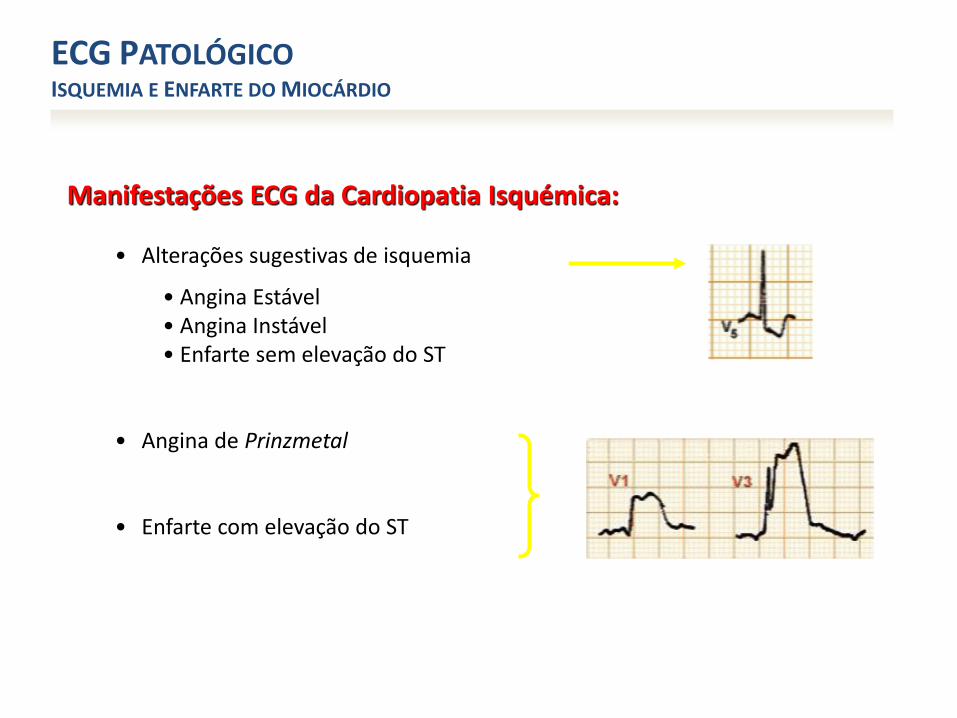
Manifestações ECG da Cardiopatia Isquémica:
• Alterações sugestivas de isquemia
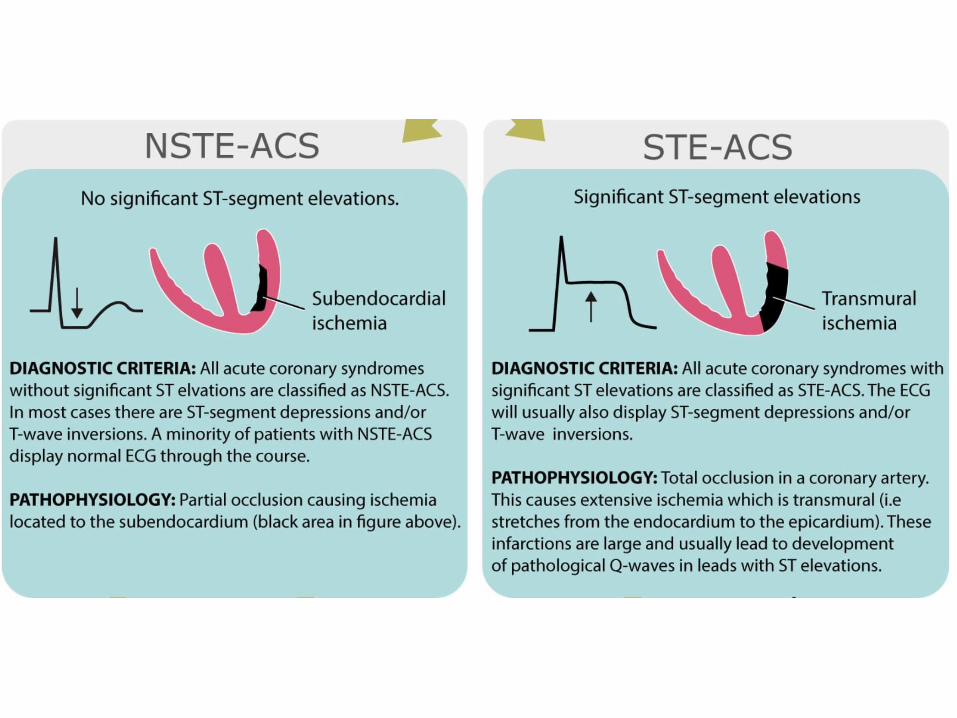
• Angina Estável • Angina Instável• Enfarte sem elevação do ST
• Angina de Prinzmetal
• Enfarte com elevação do ST
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
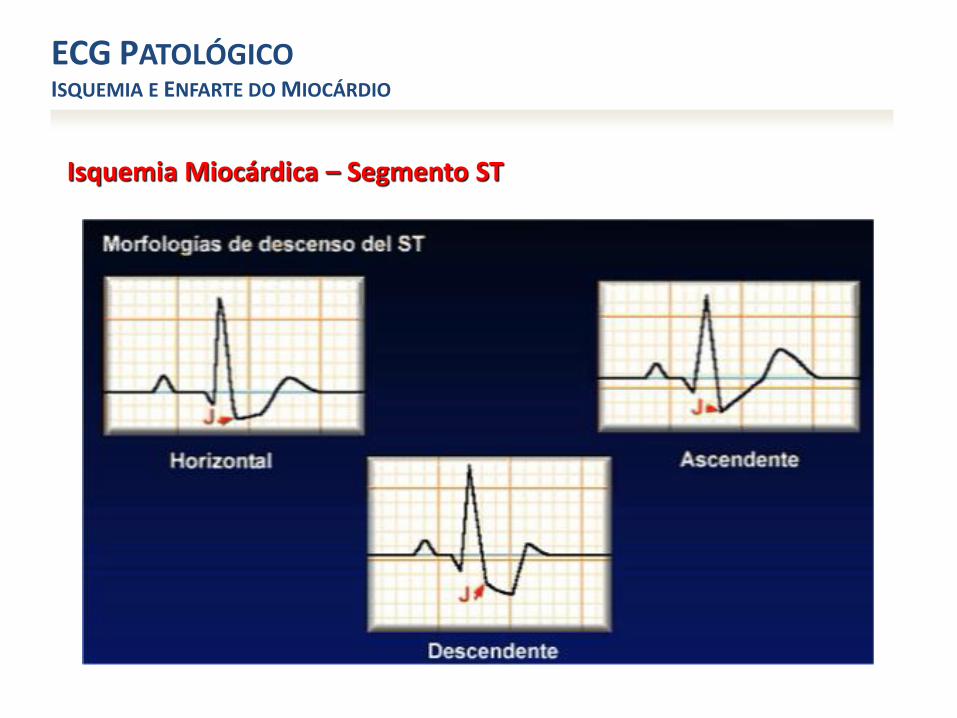
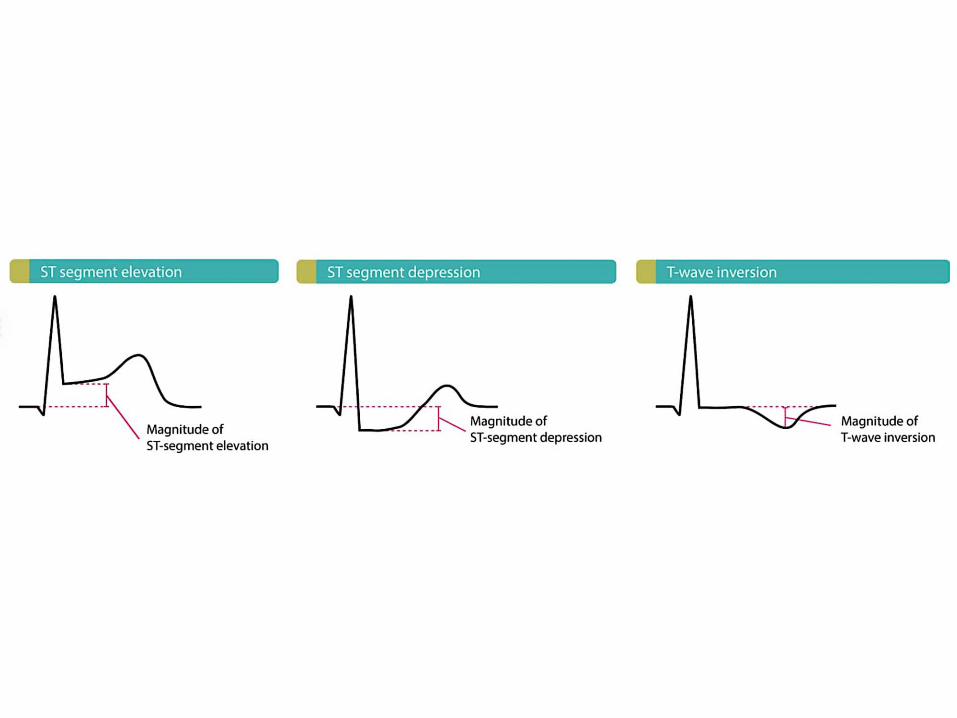
Isquemia Miocárdica – Segmento ST
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
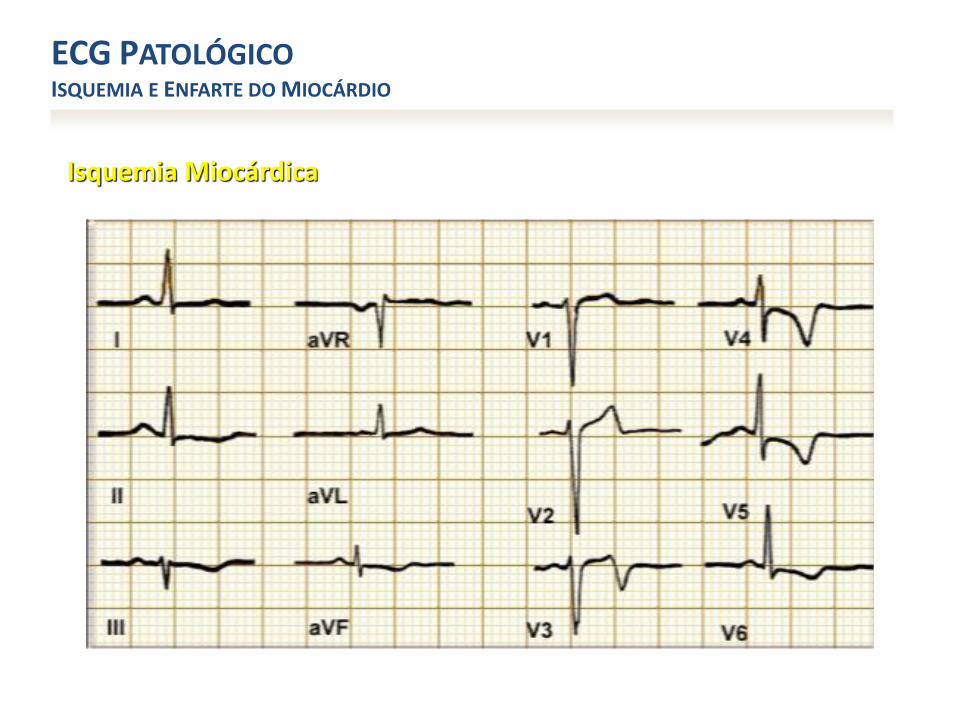
Isquemia Miocárdica
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
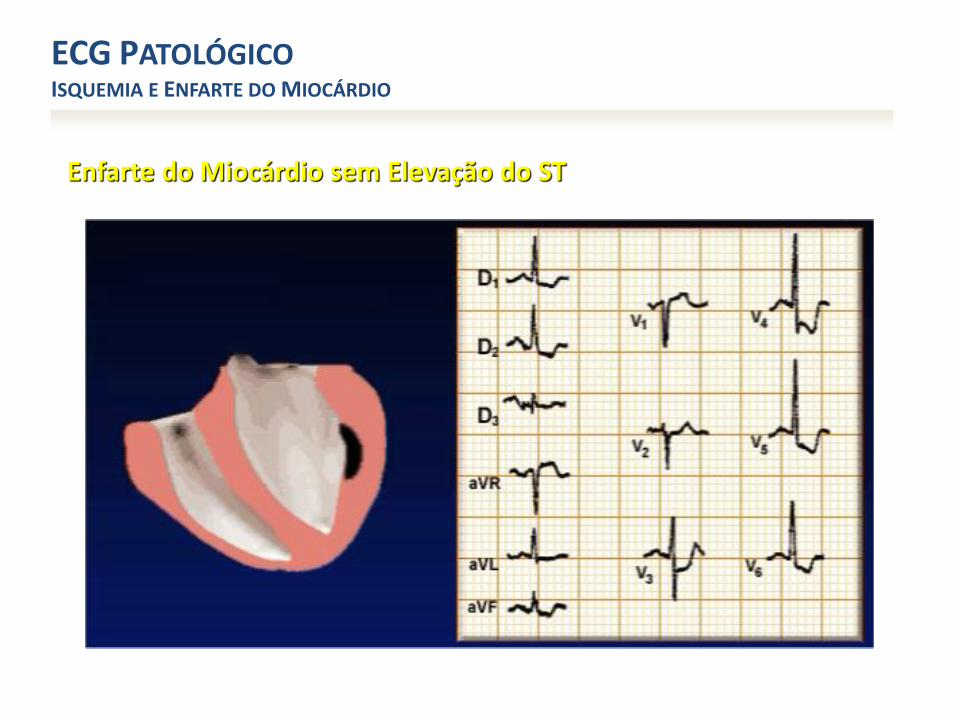
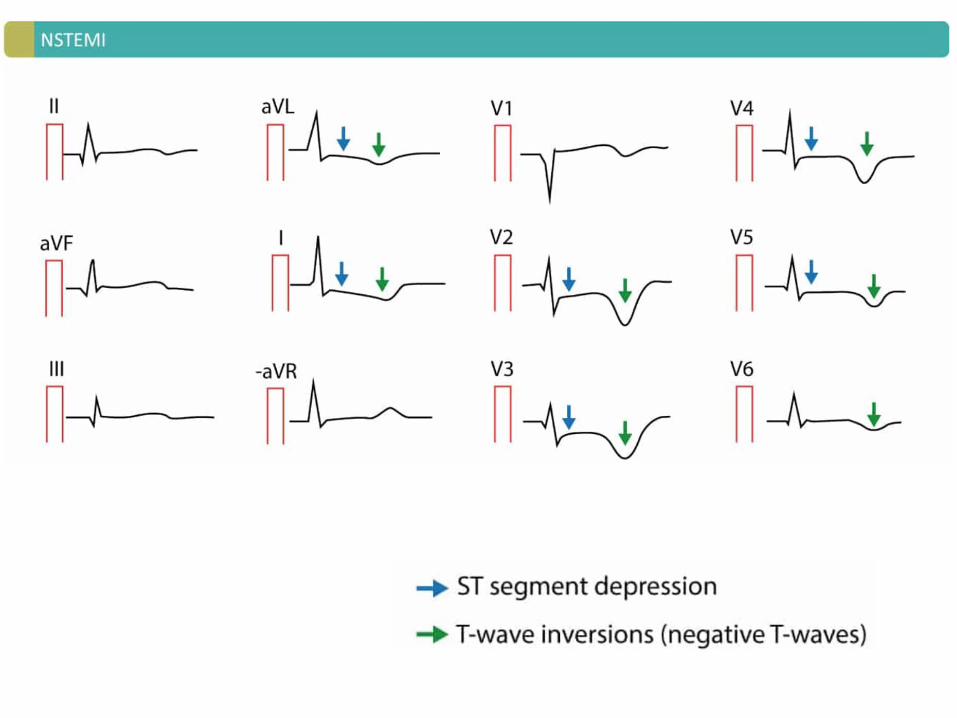
Enfarte do Miocárdio sem Elevação do ST
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO

Angina de Prinzmetal (Vasoespástica)
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
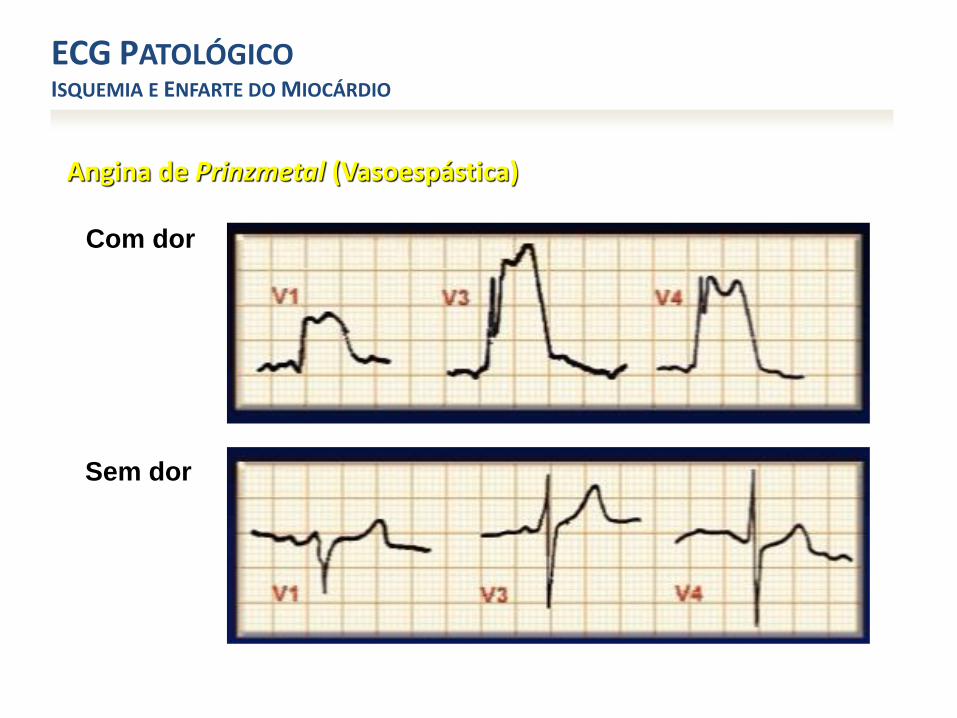
Angina de Prinzmetal (Vasoespástica)
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
Com dor
Sem dor

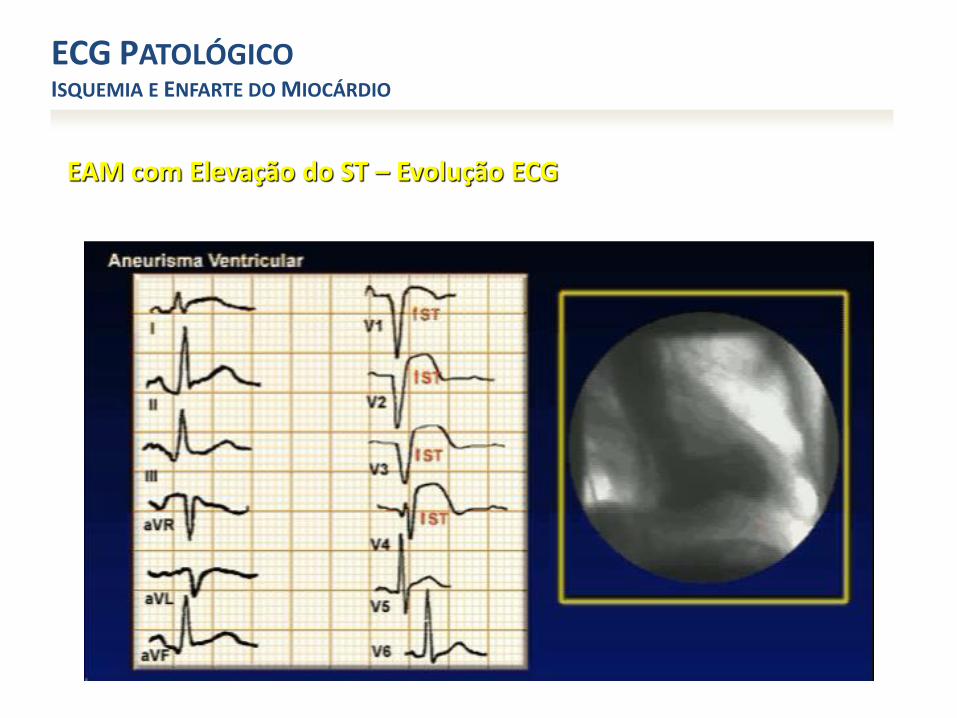
EAM com Elevação do ST – Evolução ECG
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO

EAM com Elevação do ST – Evolução ECG
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO

EAM com Elevação do ST – Evolução ECG
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
Risk Stratification by ECG
• Simple, quick, noninvasive tool
• Universally available, cheap
• Correlates with risk and prognosis
• Guides treatment decisions
• Can identify alternative causes
Risk Stratification by ECG
• ECG Findings and Associated LR for AMI
– New ST-E > 1mm LR 5.7-53.9
– New Q waves LR 5.3-24.8
– Any ST-E LR 11.2 (7.1-17.8)
– New Conduction Defect LR 6.3 ( 2.5-15.7)
– New ST-D LR 3.0-5.2
– NORMAL ECG LR 0.1-0.4
Panju AA. JAMA. 1998;280:1256.
Risk Stratification by ECG
CAVEATS
• 1-8% AMI have a normal ECG
• Only Approx 50% of AMI patients have diagnostic changes on their initial ECG
Peter J. Zimetbaum, M.D., N Engl J Med 2003;348:933-40.
Risk Stratification by ECG
CAVEATS cont.
• 1 ECG cannot exclude AMI
– Brief sample of a dynamic process
• Small regions of ischemia or infarction may be missed
Peter J. Zimetbaum, M.D., N Engl J Med 2003;348:933-40.
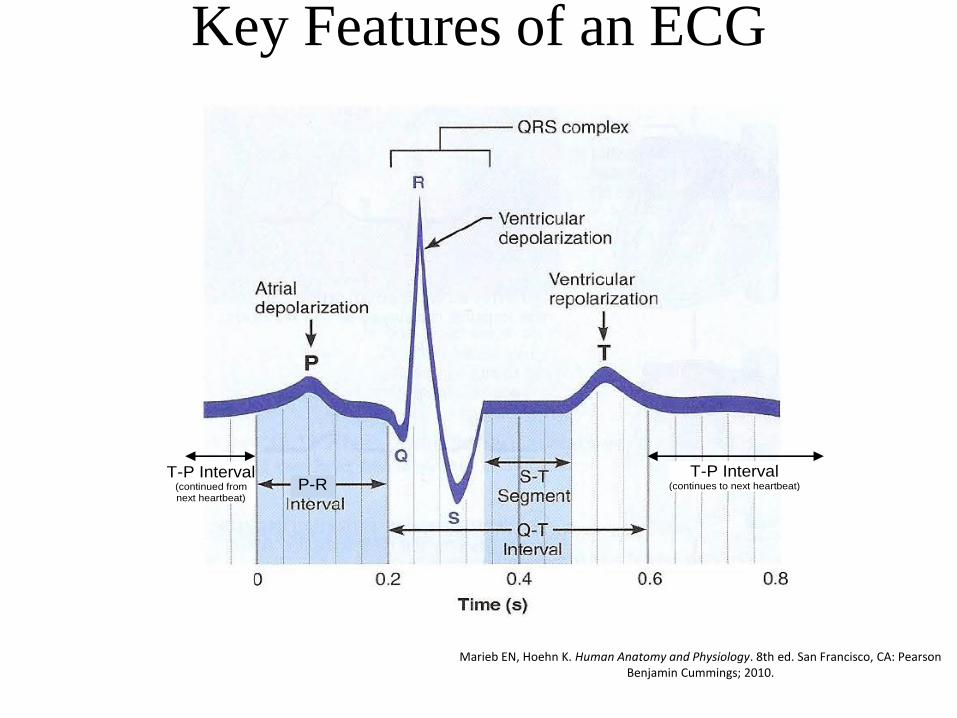
Key Features of an ECG
P-R T-P Interval
(continues to next heartbeat)
T-P Interval (continued from next heartbeat)
Marieb EN, Hoehn K. Human Anatomy and Physiology. 8th ed. San Francisco, CA: Pearson Benjamin Cummings; 2010.
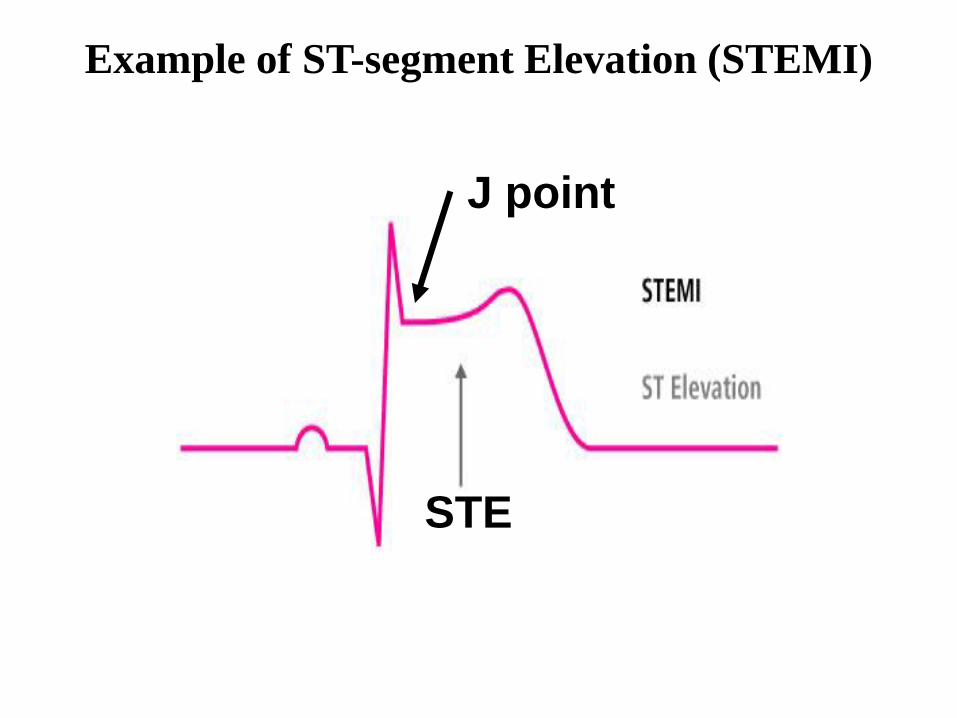
Example of ST-segment Elevation (STEMI)
J point
STE
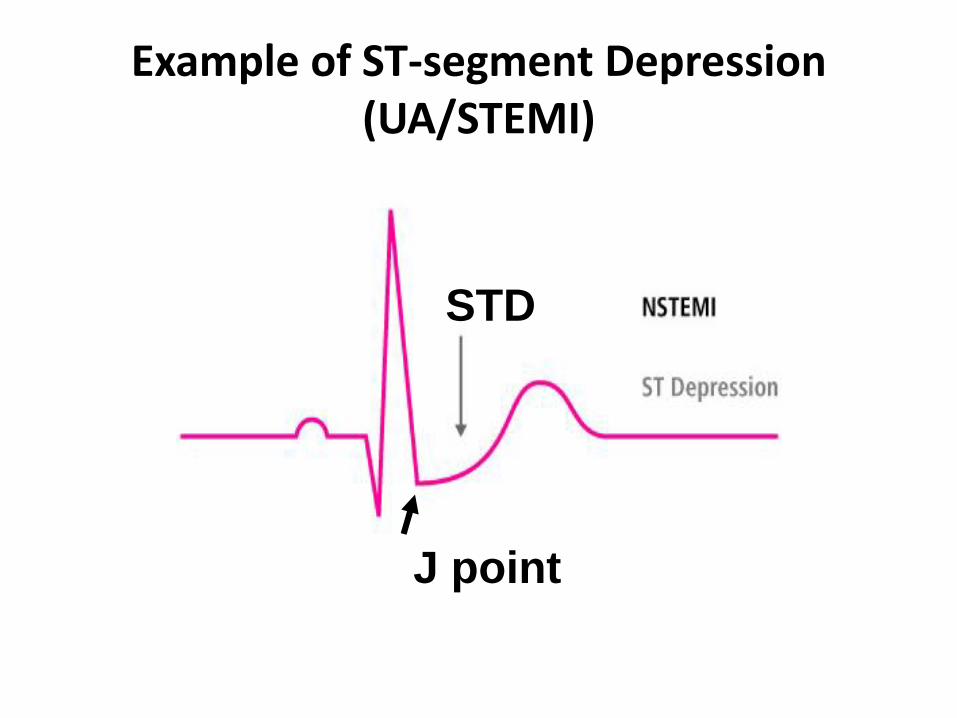
Example of ST-segment Depression (UA/STEMI)
J point
STD
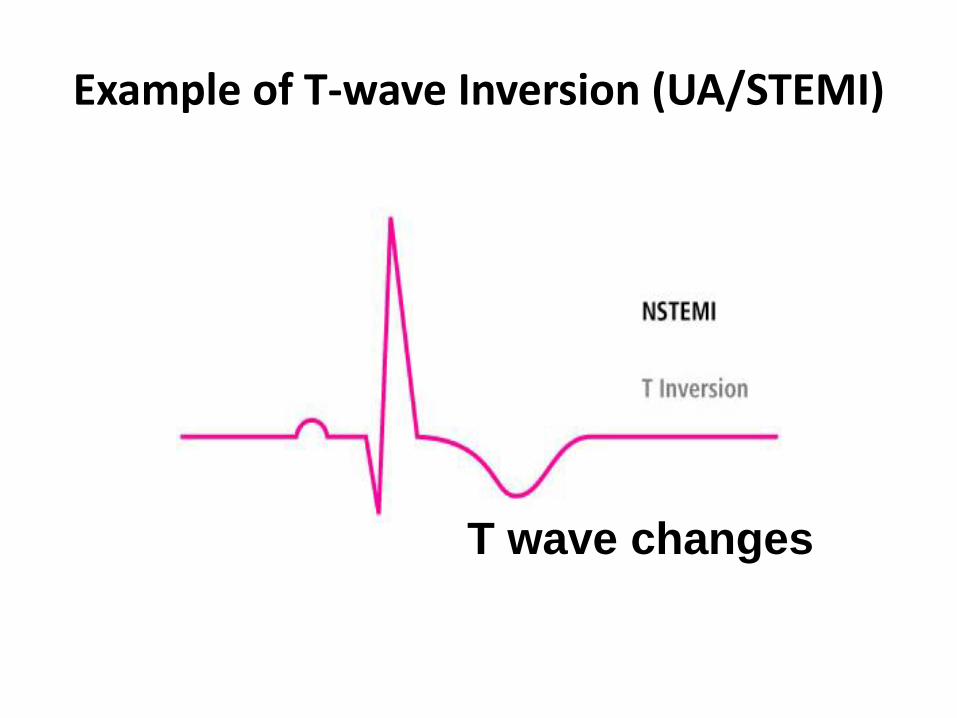
Example of T-wave Inversion (UA/STEMI)
T wave changes
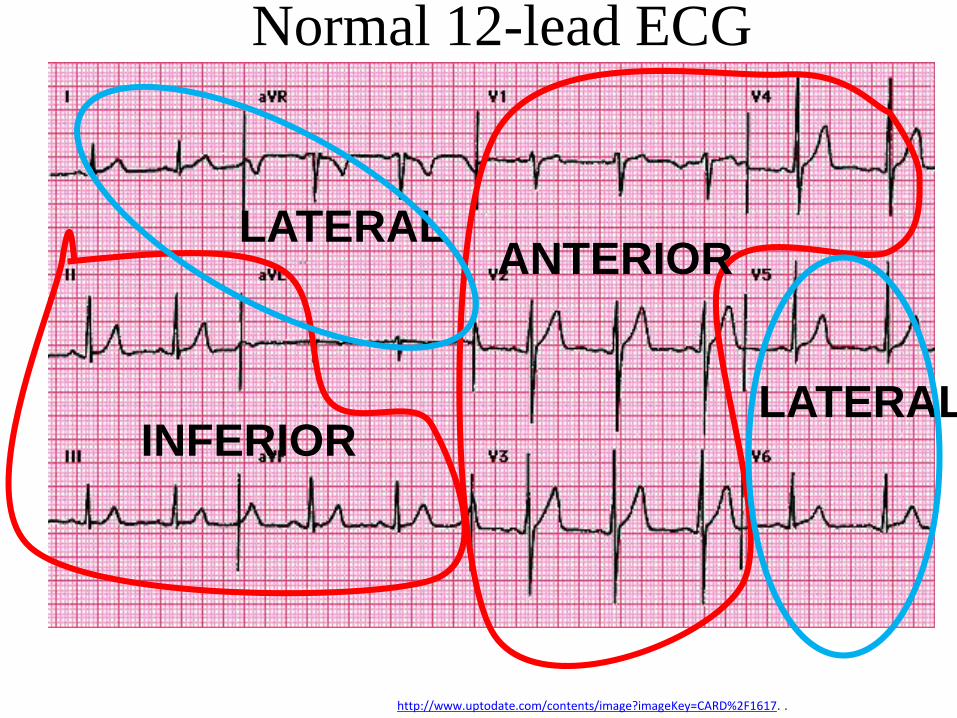
Normal 12-lead ECG
http://www.uptodate.com/contents/image?imageKey=CARD%2F1617. .
INFERIOR
ANTERIORLATERAL
LATERAL
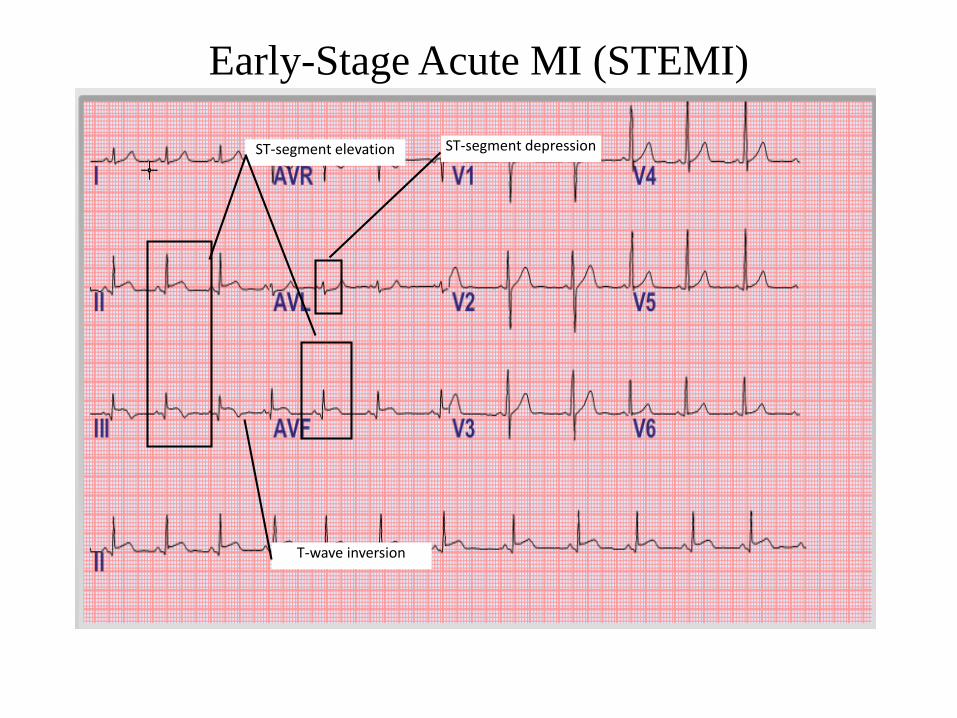
Early-Stage Acute MI (STEMI)
ST-segment elevation ST-segment depression
T-wave inversion
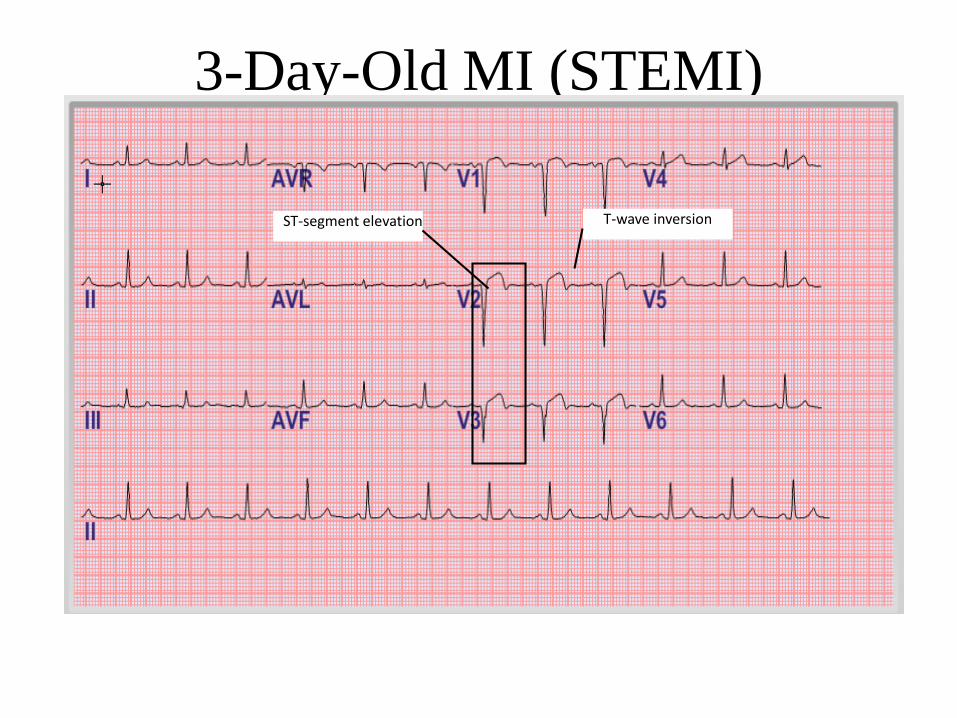
3-Day-Old MI (STEMI)
ST-segment elevation T-wave inversion
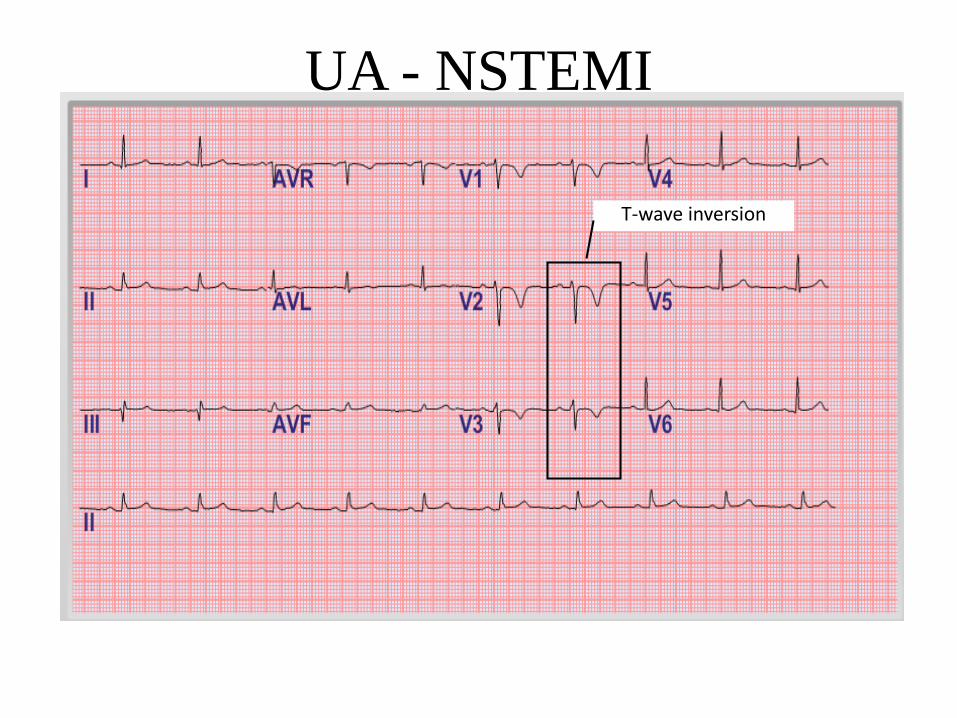
UA - NSTEMI
T-wave inversion
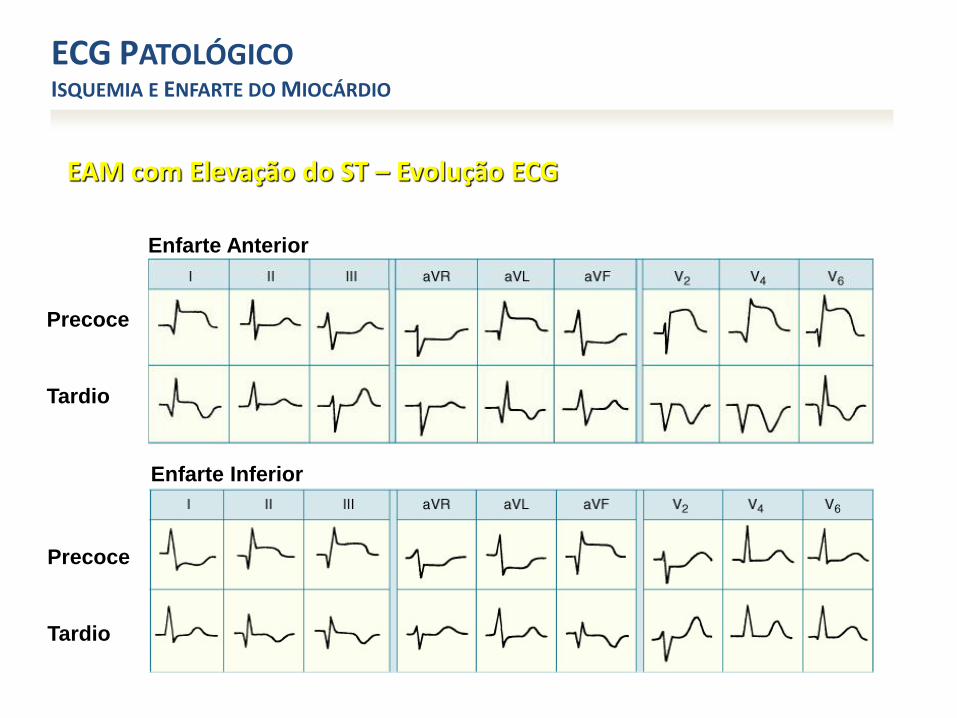
EAM com Elevação do ST – Evolução ECG
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
Precoce
Tardio
Enfarte Inferior
Enfarte Anterior
Precoce
Tardio
EAM com Elevação do ST – Evolução ECG
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
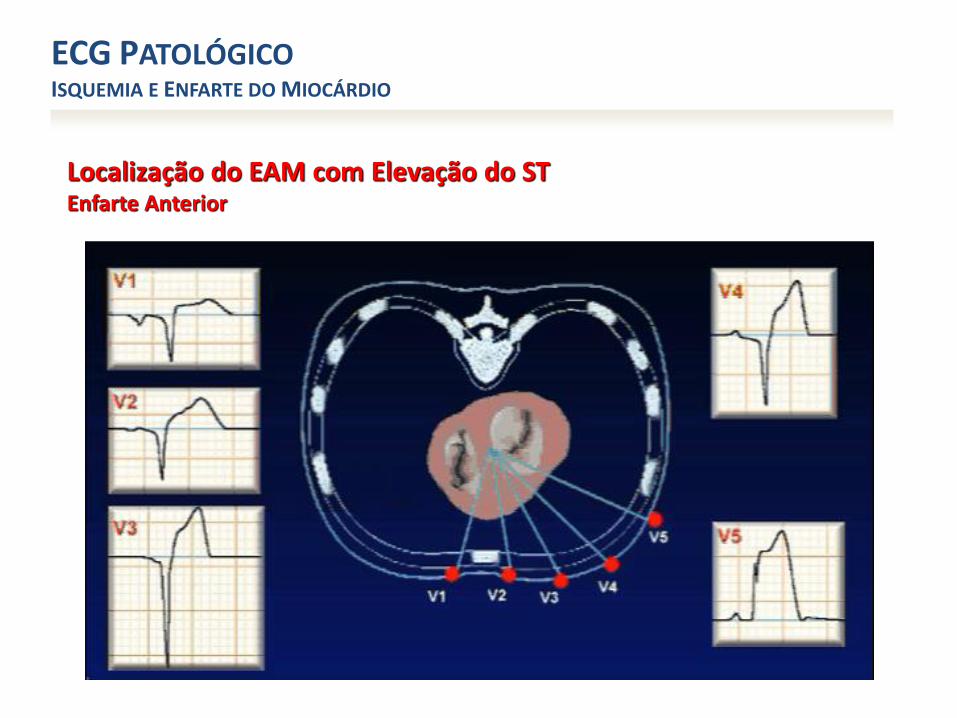
Localização do EAM com Elevação do STEnfarte Anterior
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
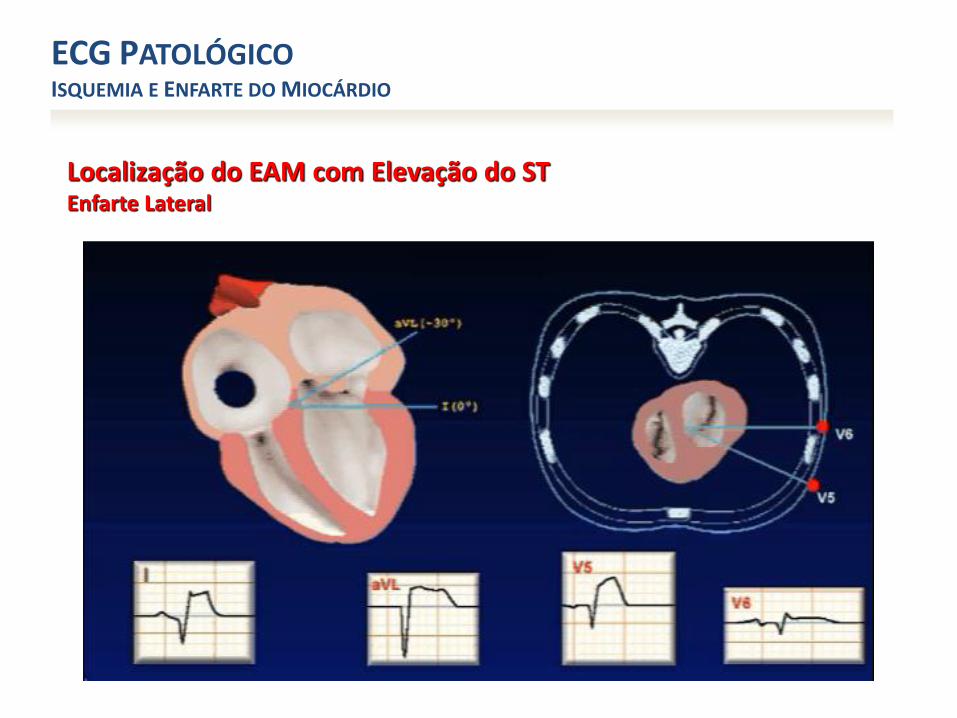
Localização do EAM com Elevação do STEnfarte Lateral
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
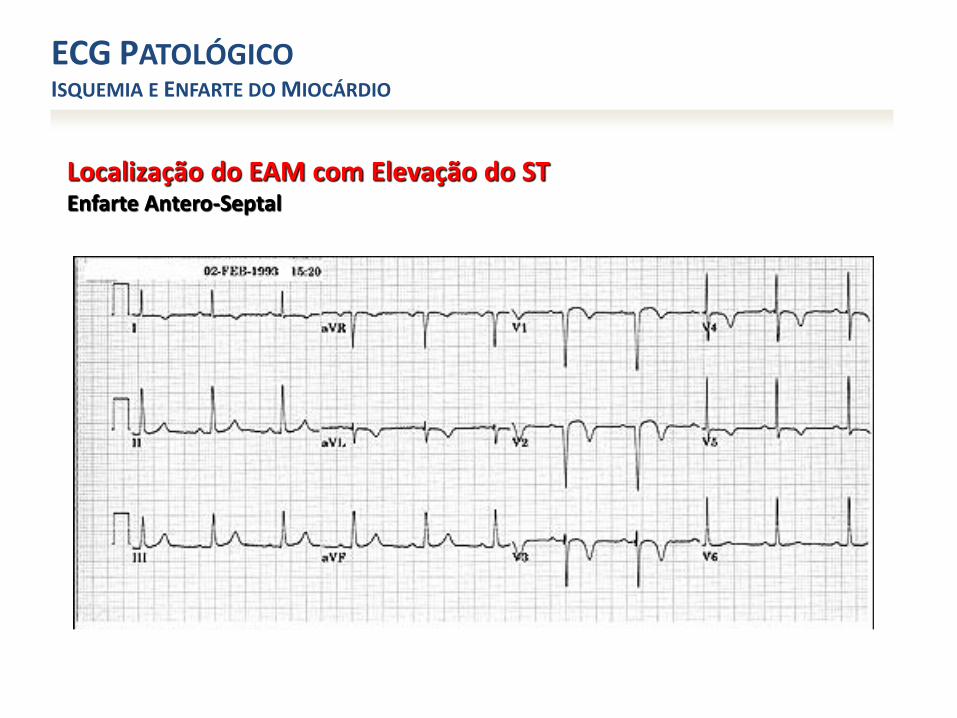
Localização do EAM com Elevação do STEnfarte Antero-Septal
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
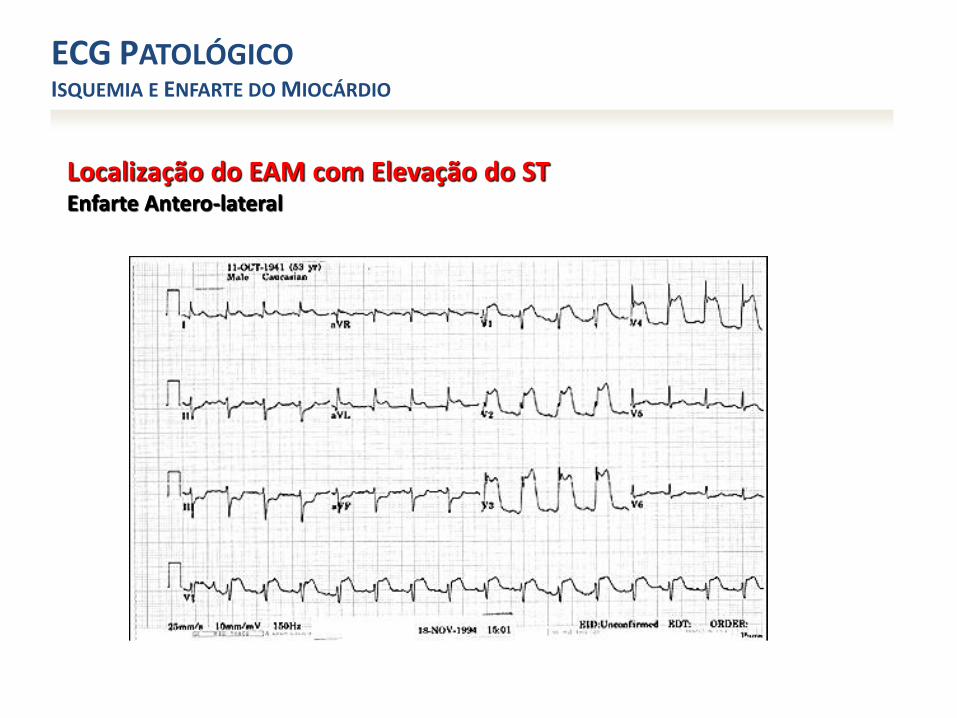
Localização do EAM com Elevação do STEnfarte Antero-lateral
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
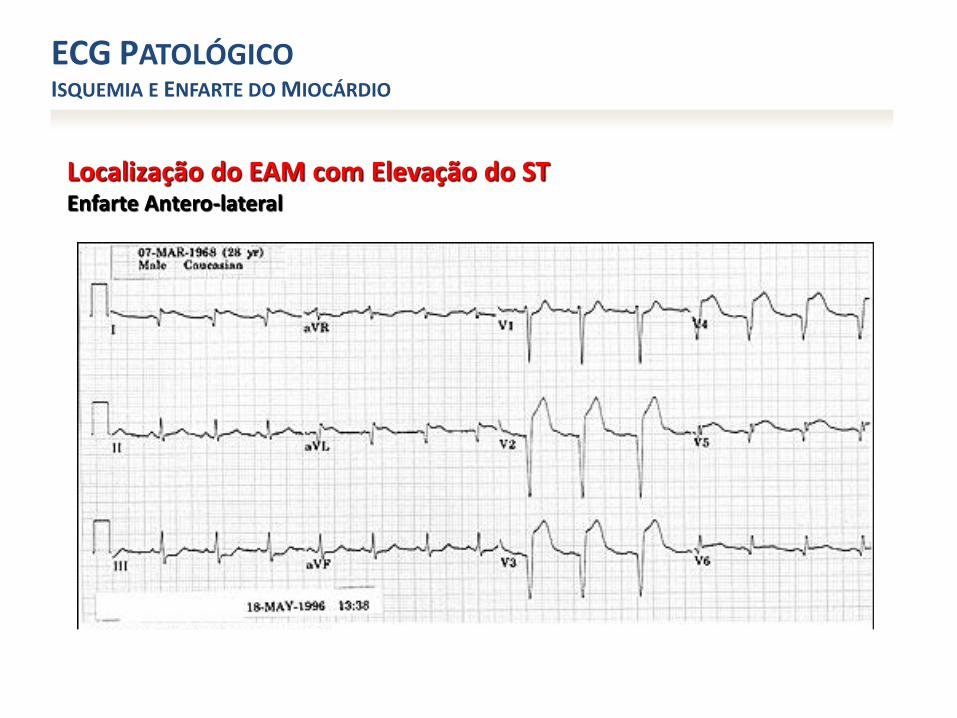
Localização do EAM com Elevação do STEnfarte Antero-lateral
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
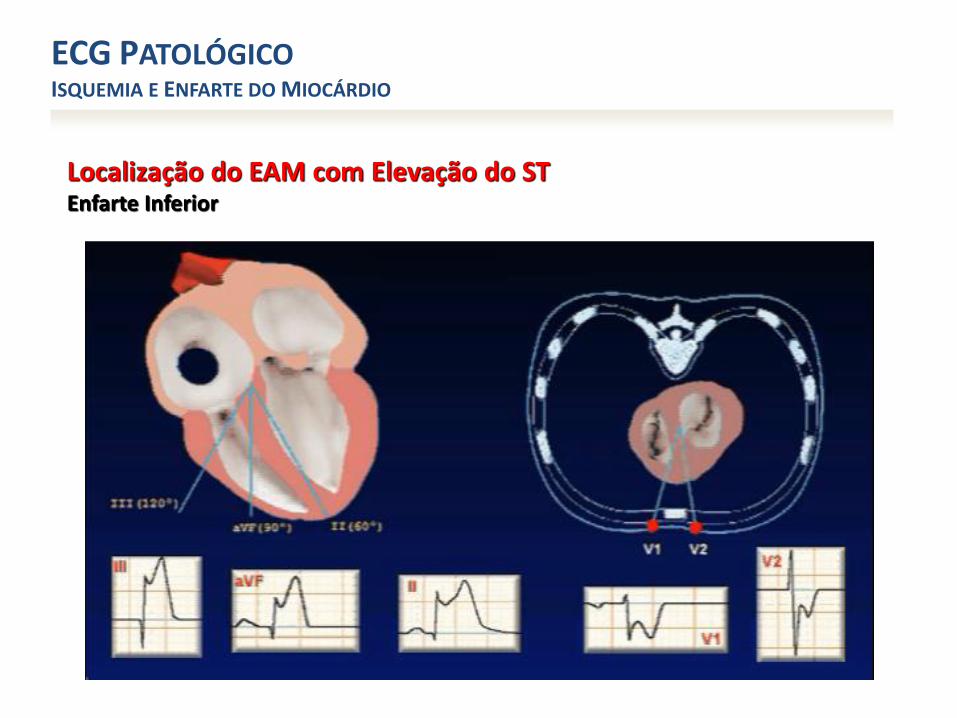
Localização do EAM com Elevação do STEnfarte Inferior
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
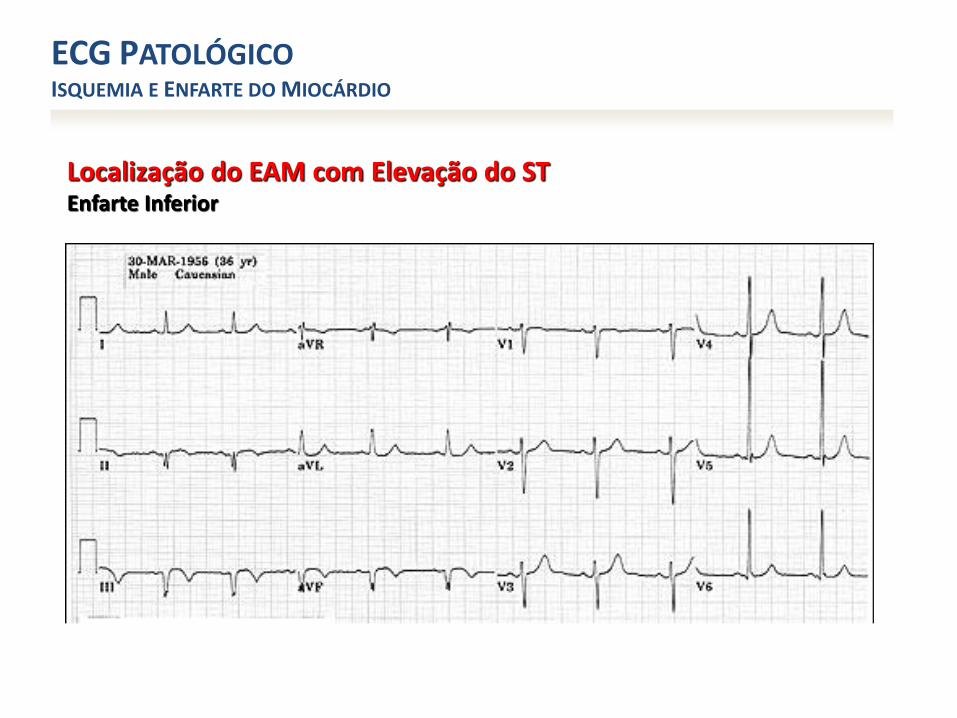
Localização do EAM com Elevação do STEnfarte Inferior
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
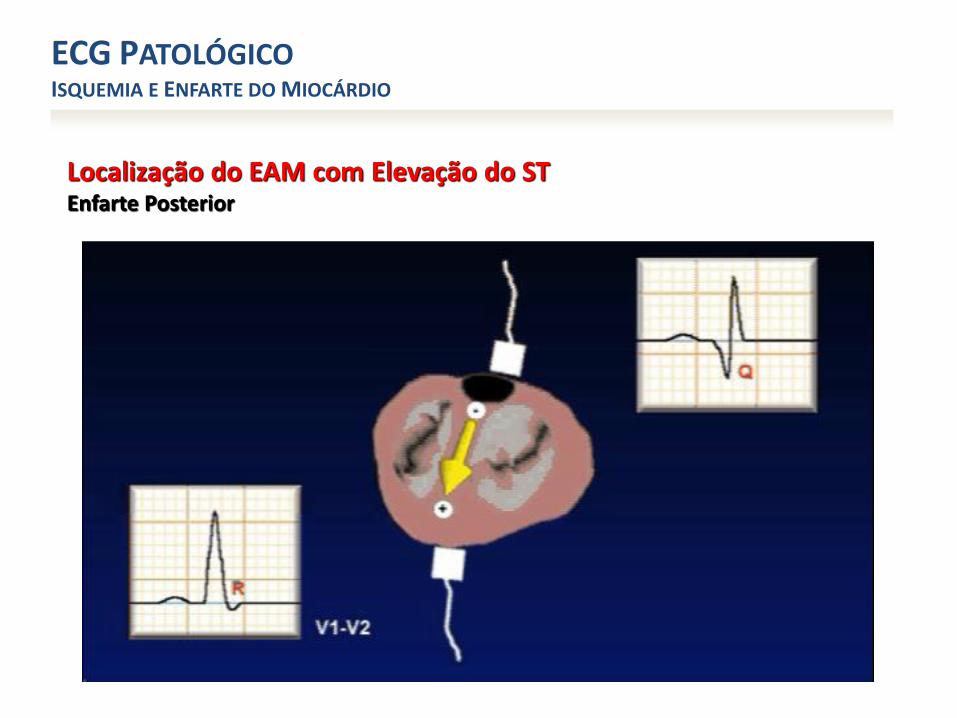
Localização do EAM com Elevação do STEnfarte Posterior
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
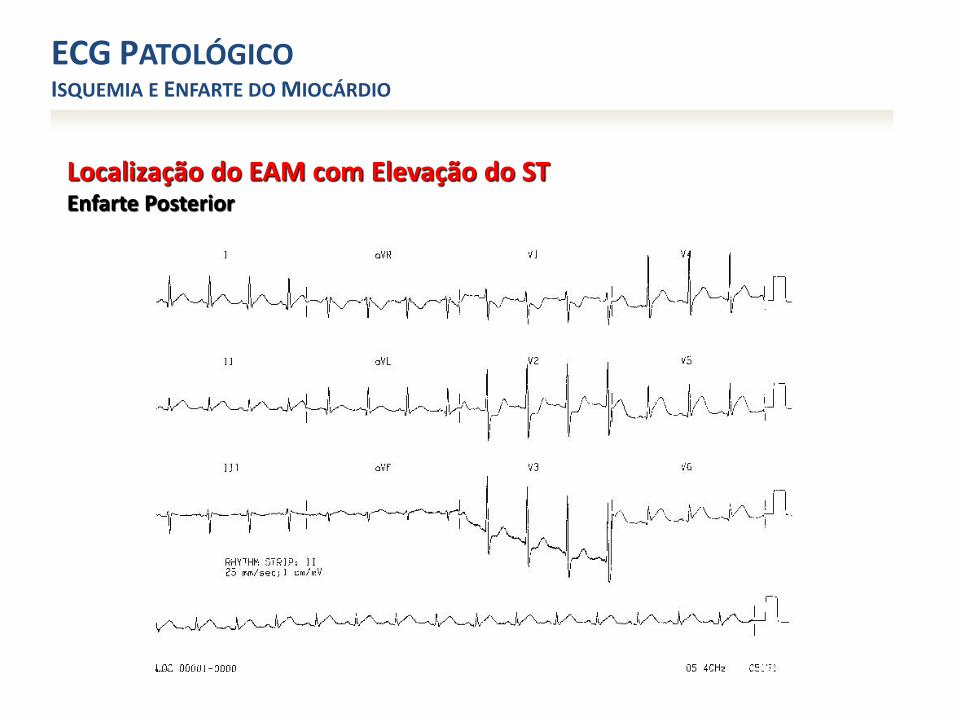
Localização do EAM com Elevação do STEnfarte Posterior
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
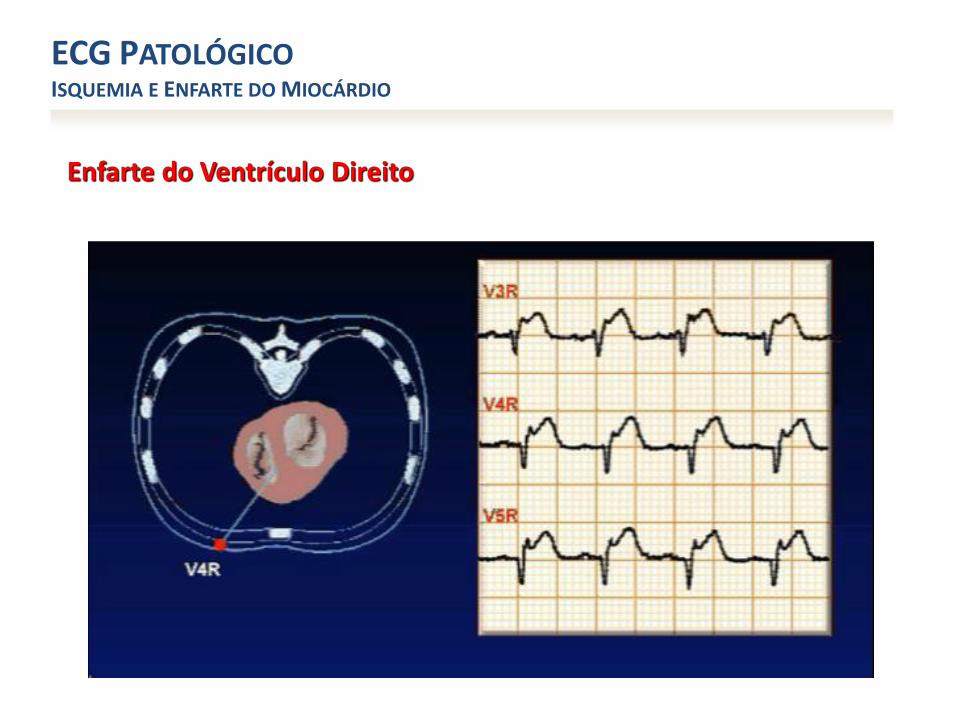
Enfarte do Ventrículo Direito
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
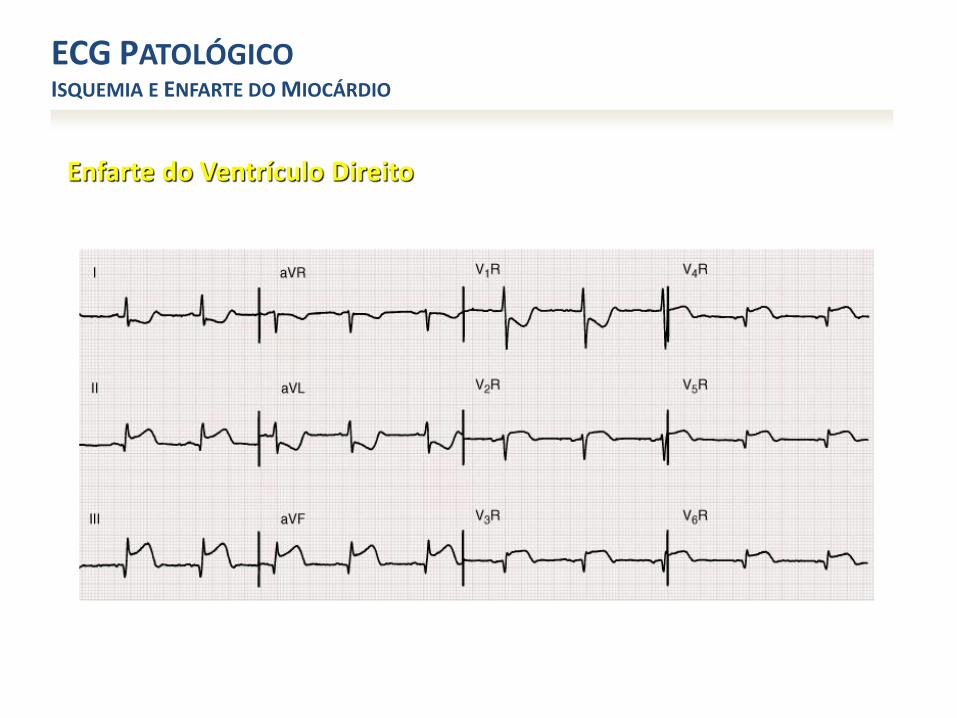
Enfarte do Ventrículo Direito
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
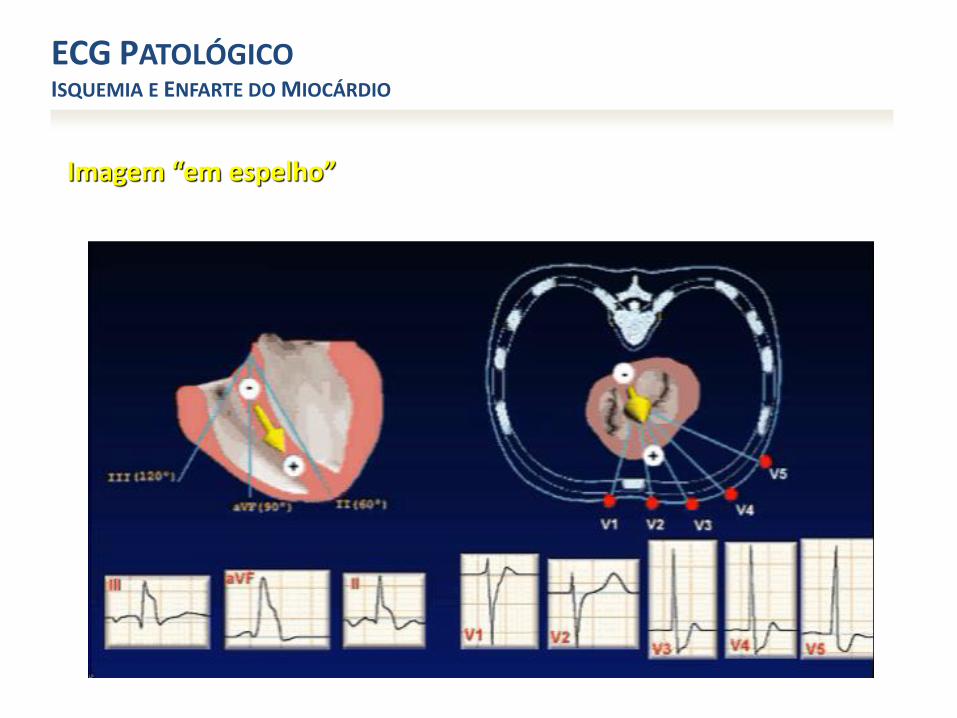
Imagem “em espelho”
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
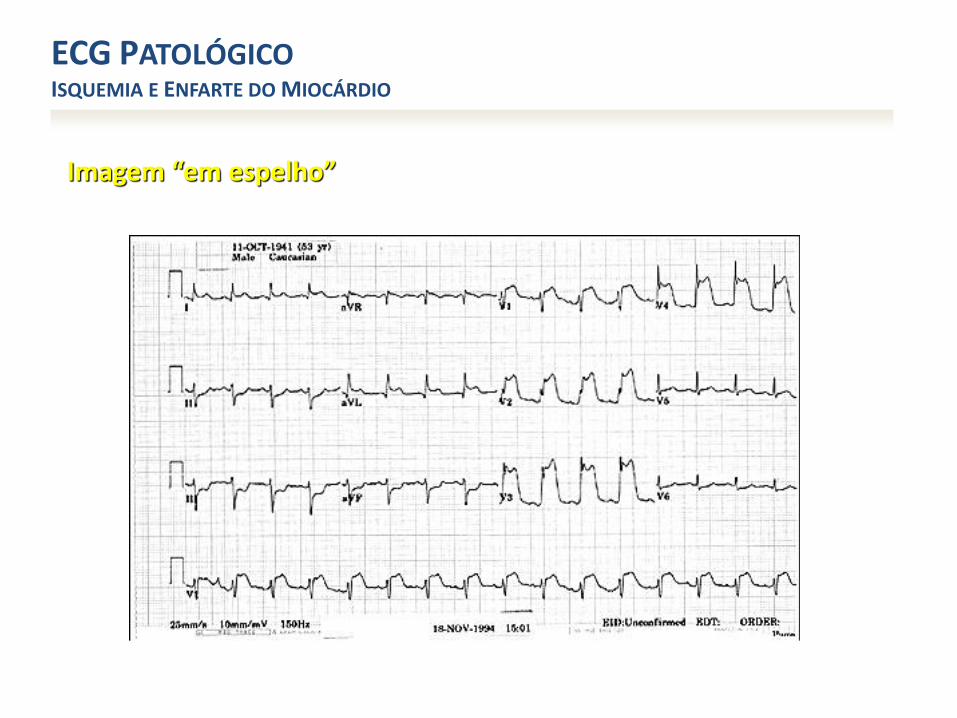
Imagem “em espelho”
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
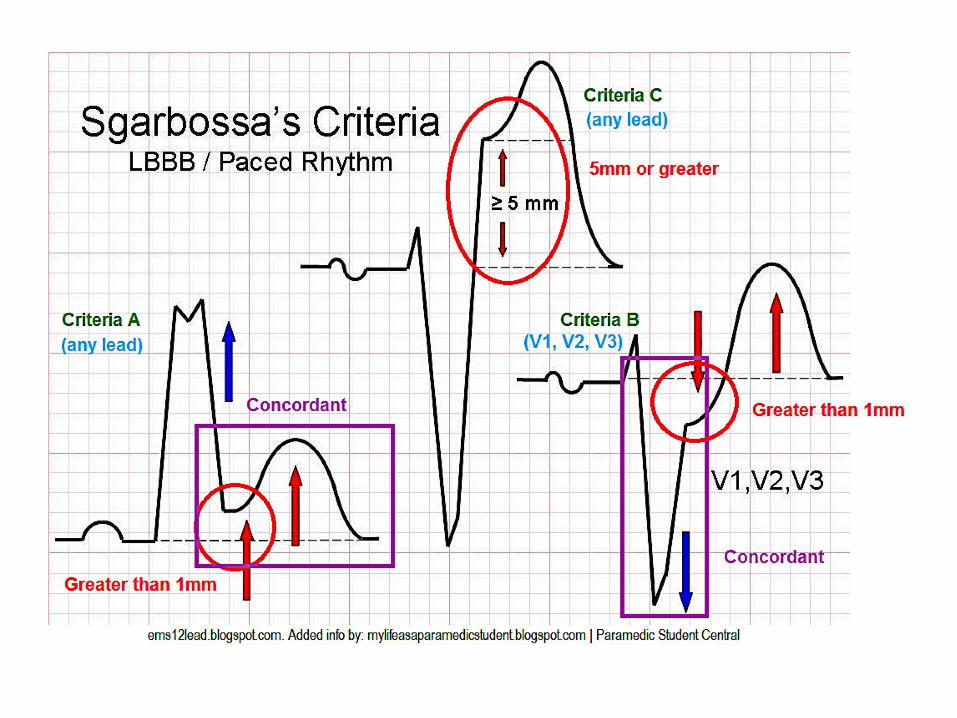
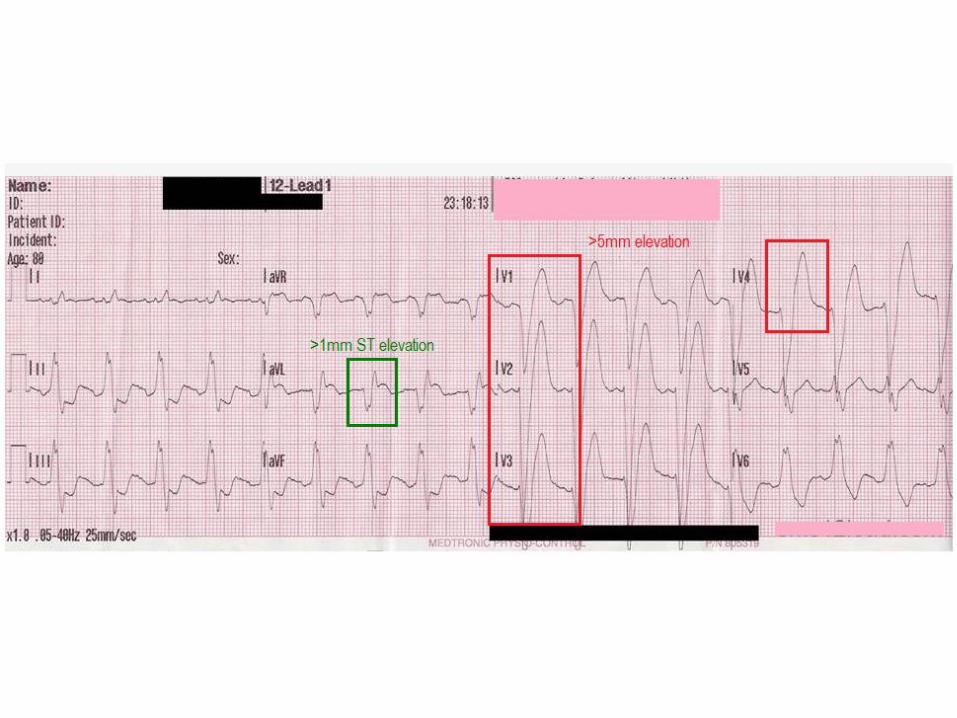
LBBB
• LBBB occurs when normal electrical activity in the His-Purkinje system is interrupted
• Most often occurs in patients with underlying heart disease
• Can be functional (rate related) and can be seen in asymptomatic individuals without structural heart disease
• Obscures ischemic changes on the ECG
LBBB
• A new LBBB in a patient with symptoms consistent with MI should be treated like a STEMI
• LBBB is associated with ST changes as part of the ECG pattern (discordant changes)
• Concordant changes
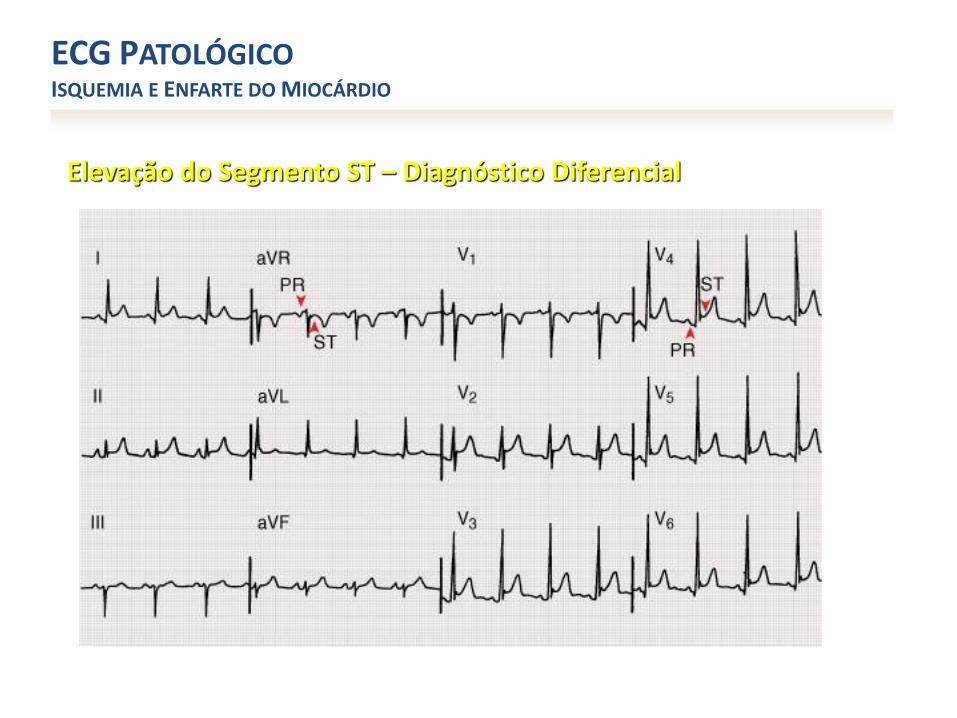
Elevação do Segmento ST – Diagnóstico Diferencial
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
• Doença coronária:✓ Enfarte agudo do miocárdio
✓ Angina de Prinzemtal
✓ Aneurisma pós-enfarte
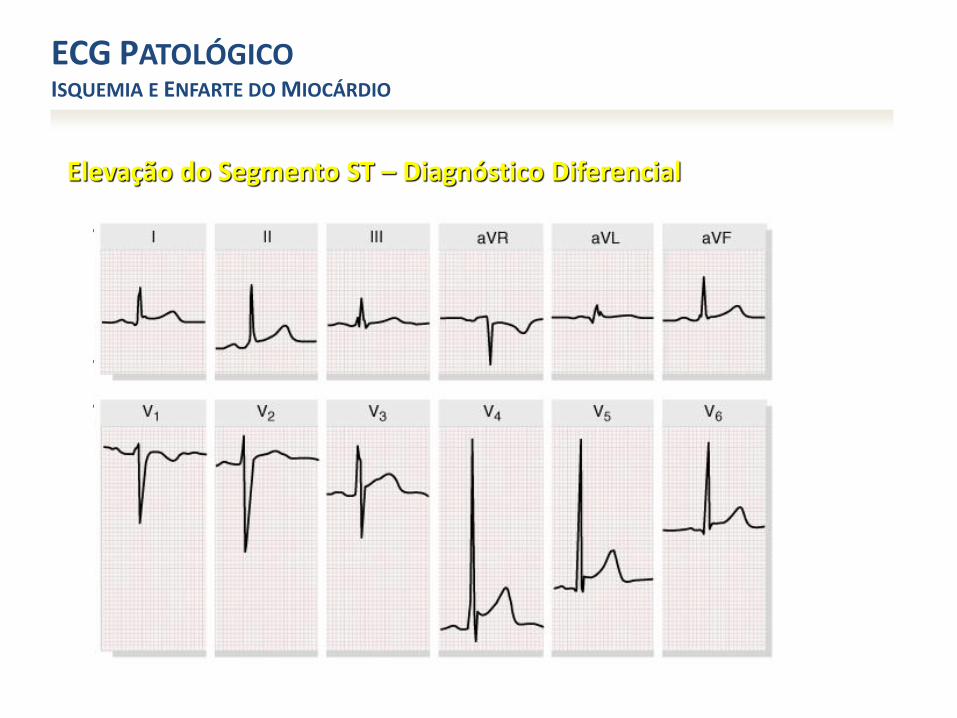
Elevação do Segmento ST – Diagnóstico Diferencial
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
• Doença coronária:✓ Enfarte agudo do miocárdio
✓ Angina de Prinzemtal
✓ Aneurisma pós-enfarte
• Pericardite a Miopericardite agudas
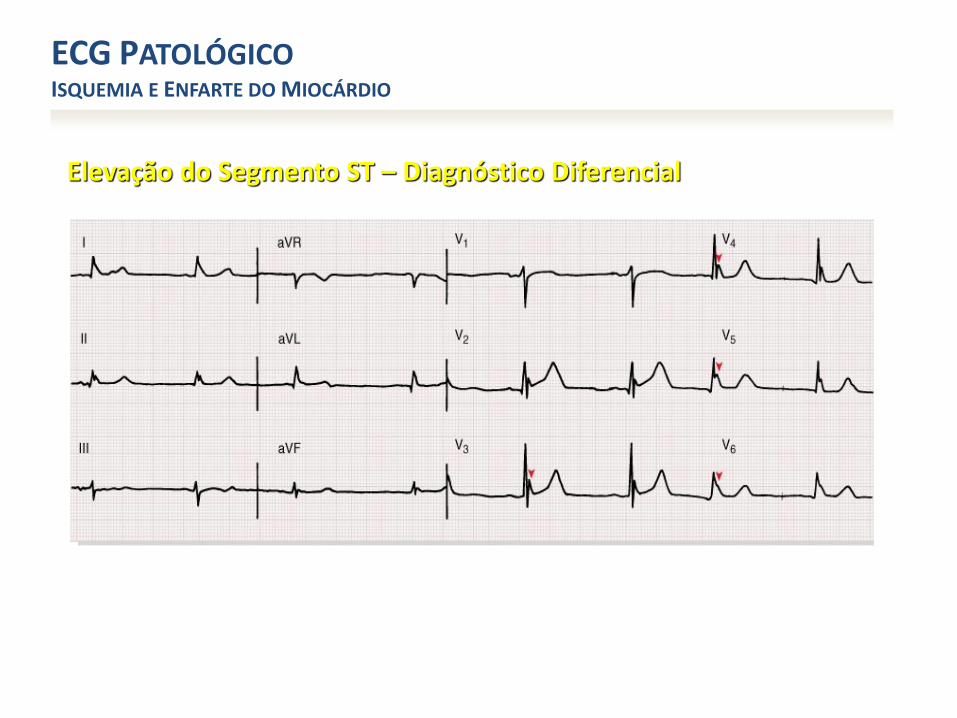
Elevação do Segmento ST – Diagnóstico Diferencial
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
• Doença coronária:✓ Enfarte agudo do miocárdio
✓ Angina de Prinzemtal
✓ Aneurisma pós-enfarte
• Pericardite a Miopericardite agudas
• Padrão de repolarização precoce (variante do normal)
Elevação do Segmento ST – Diagnóstico Diferencial
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
• Doença coronária:✓ Enfarte agudo do miocárdio
✓ Angina de Prinzemtal
✓ Aneurisma pós-enfarte
• Pericardite a Miopericardite agudas
• Padrão de repolarização precoce (variante do normal)
• Hipotermina (ondas de Osborn)

Elevação do Segmento ST – Diagnóstico Diferencial
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
• Doença coronária:✓ Enfarte agudo do miocárdio
✓ Angina de Prinzemtal
✓ Aneurisma pós-enfarte
• Pericardite a Miopericardite agudas
• Padrão de repolarização precoce (variante do normal)
• Hipotermina (ondas de Osborn)
• Padrão de Brugrada (com BCRD)
Elevação do Segmento ST – Diagnóstico Diferencial
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
• Doença coronária:✓ Enfarte agudo do miocárdio
✓ Angina de Prinzemtal
✓ Aneurisma pós-enfarte
• Pericardite a Miopericardite agudas
• Padrão de repolarização precoce (variante do normal)
• Hipotermina (ondas de Osborn)
• Padrão de Brugada (com BCRD)
• Outros• Lesão traumática do miocárdio
• Tumor com invasão do ventrículo esquerdo
• Após cardioversão eléctrica
• BCRE
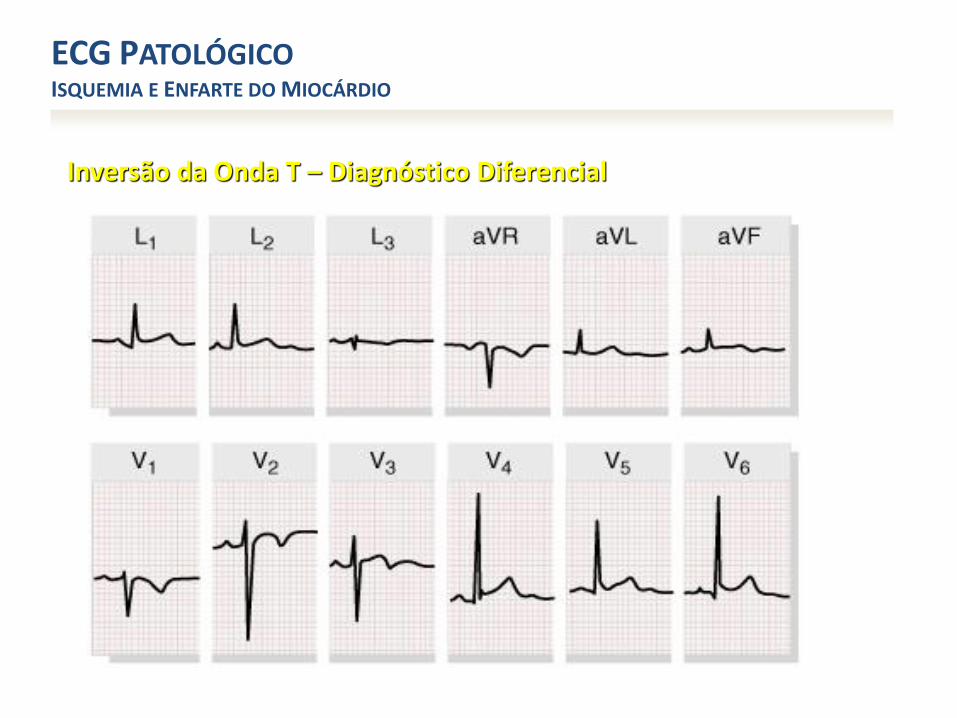
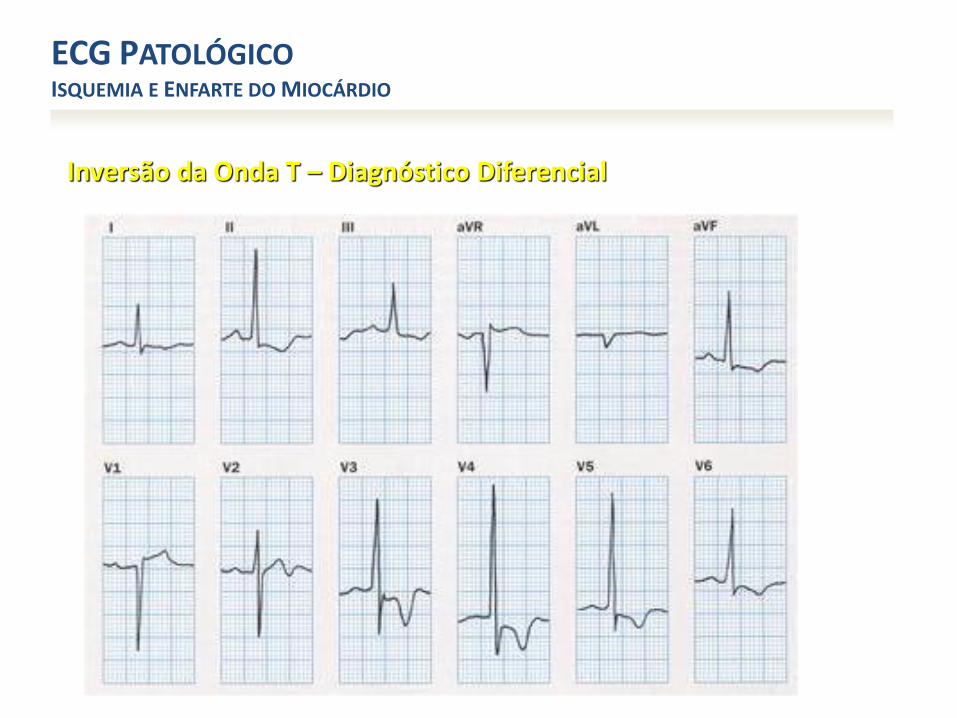
Inversão da Onda T – Diagnóstico Diferencial
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
• Doença coronária – Isquemia
• Padrão juvenil (variante do normal)
Inversão da Onda T – Diagnóstico Diferencial
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
• Doença coronária – Isquemia
• Padrão juvenil (variante do normal)
• Padrão de repolarização precoce (variante do normal)
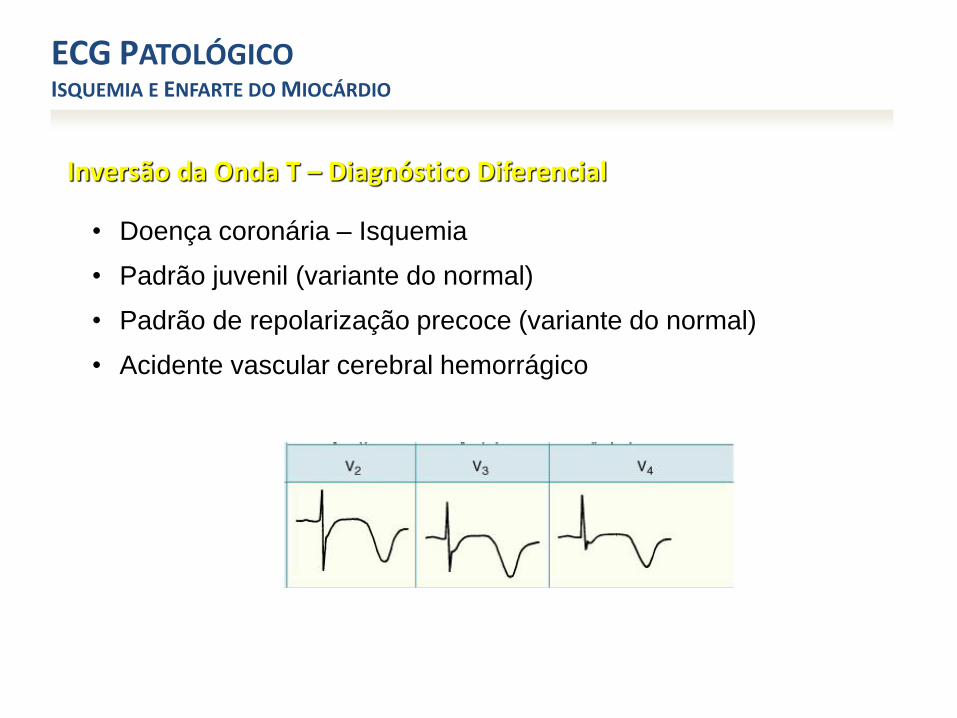
Inversão da Onda T – Diagnóstico Diferencial
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
• Doença coronária – Isquemia
• Padrão juvenil (variante do normal)
• Padrão de repolarização precoce (variante do normal)
• Acidente vascular cerebral hemorrágico
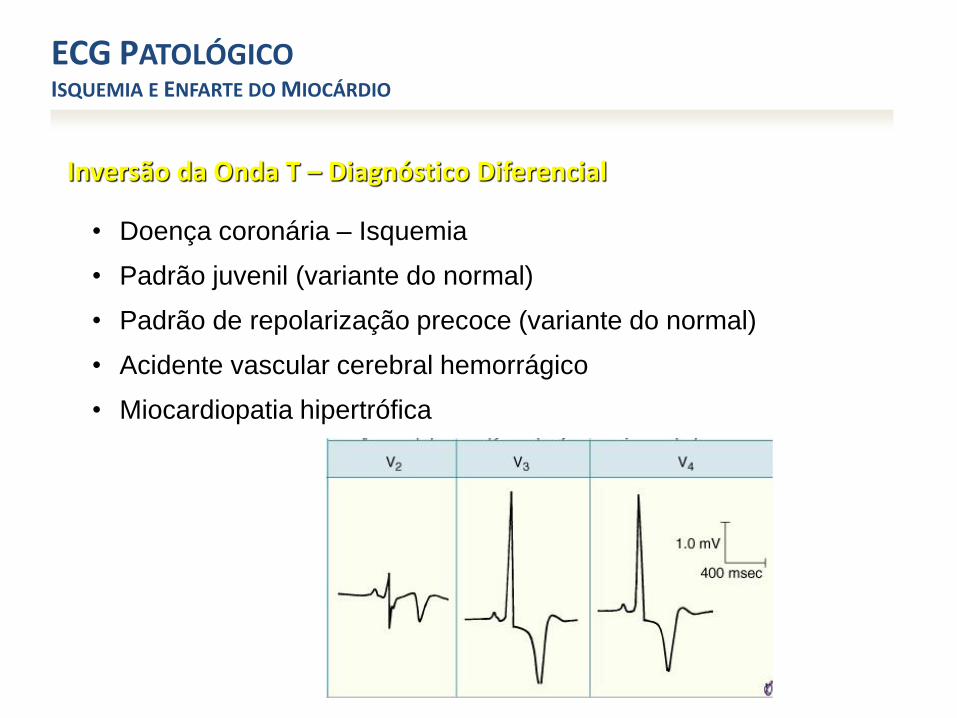
Inversão da Onda T – Diagnóstico Diferencial
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
• Doença coronária – Isquemia
• Padrão juvenil (variante do normal)
• Padrão de repolarização precoce (variante do normal)
• Acidente vascular cerebral hemorrágico
• Miocardiopatia hipertrófica
Inversão da Onda T – Diagnóstico Diferencial
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
• Doença coronária – Isquemia
• Padrão juvenil (variante do normal)
• Padrão de repolarização precoce (variante do normal)
• Acidente vascular cerebral hemorrágico
• Miocardiopatia hipertrófica
• Padrão de “sobrecarga” VE
Inversão da Onda T – Diagnóstico Diferencial
ECG PATOLÓGICOISQUEMIA E ENFARTE DO MIOCÁRDIO
• Doença coronária – Isquemia
• Padrão juvenil (variante do normal)
• Padrão de repolarização precoce (variante do normal)
• Acidente vascular cerebral hemorrágico
• Miocardiopatia hipertrófica
• Padrão de “sobrecarga” VE
• Bloqueio completo do ramo esquerdo ou direito
• Pré-excitação – Wolf-parkinson-White

OBRIGADO ....
COMPLICATIONS OF ACUTE CORONARY SYNDROMES
• cardiac failure• post-infarction ischaemia• ventricular free wall rupture
– therapy: pericardiocentesis and repair
• ventricular septal rupture– therapy: IABP, inotropes, surgery
• acute mitral regurgitation– therapy: afterload reduction, IABP, inotropes, surgery ASAP
• right ventricular infarction– therapy: IV fluids, inotropes, AV synchrony, IABP, reperfusion
• arrhythmias– therapy: correct hypoxia, acidosis, hypovolaemia, K+, Mg2+ (controversial)
• cardiogenic shock– therapy: must get revascularisation (PCI or CABG) within 24 hours
• thromboembolism– therapy: mural thrombus -> anticoagulate
• pericarditis and Dressler’s syndrome• complications of therapy, e.g. haemorrhage, coronary artery dissection, stent thrombosis, surgical
complications


Complicações arrítmicas e mecânicas
Pedro Silva Cunha
Hospital de Santa Marta, Hospital Lusíadas Lisboa
Pós-Graduação em Medicina de Emergência
Abordagem urgente das Síndromes Coronárias Agudas(António Fiarresga, João Abecassis, Pedro Silva Cunha, Sílvio Leal)
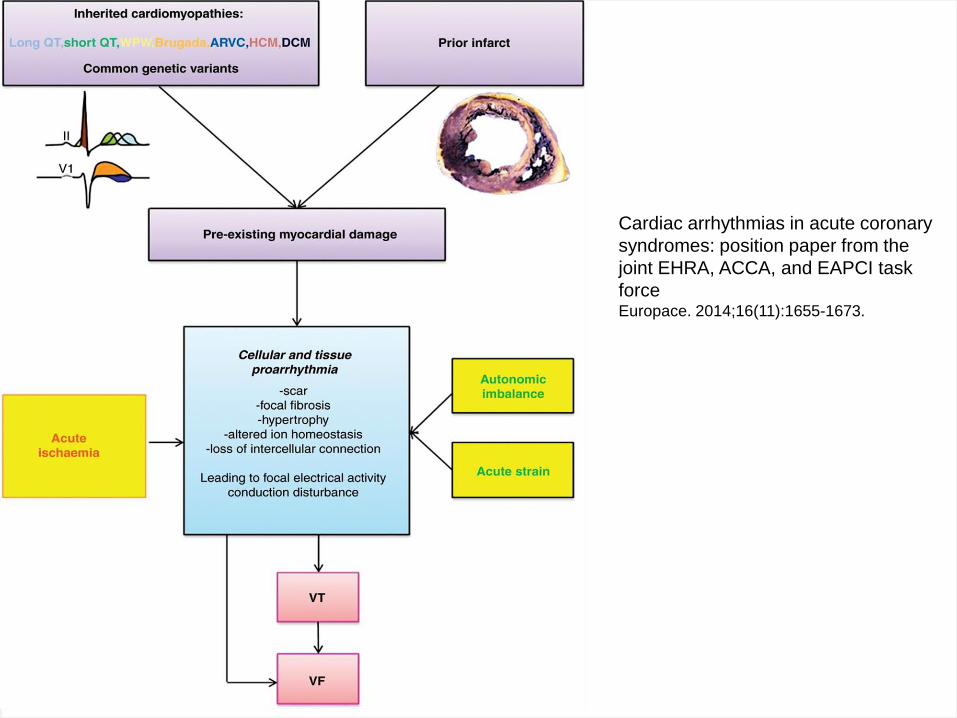
Mechanisms of ischaemia-relatedventricular arrhythmias
• Generation of the ventricular action potential by voltage and substrate dependent ion currents is the basis for the contraction of each individual myocardial cell.
• This ionic balance can be disturbed by insults, such as ischaemia/reperfusion.
Acute myocardial ischaemia leads to:
• Adenosine tri-phosphate deficiency, anaerobic glycolysis causing acidosis, elevation of extracellular potassium (K+), and lysophosphatidylcholineaccumulation.
• Multifactorial sequence of events results electrophysiologically in(i) ionic imbalance: (a) shorter duration of the action potential by activationof the substrate related potassium current: IKatp and (b) less
• reduced resting membrane potential through inhibition of the inward• rectifying potassium current: IK1; (ii) less contractile force by events• that culminate in the mishandling of intracellular calcium (Ca2+);• and (iii) a reduced conduction velocity because of less functional• gap junctions.
Janse MJ, Wit AL. Electrophysiological mechanisms of ventricular arrhythmiasresulting from myocardial ischemia and infarction. Physiol Rev 1989;69:1049–69.
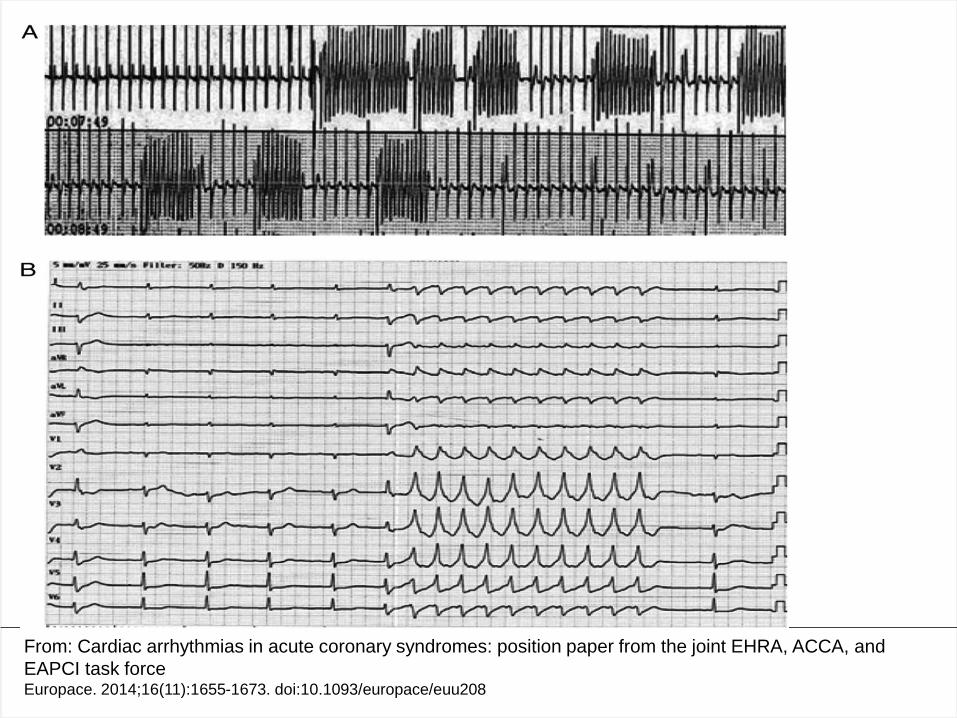
From: Cardiac arrhythmias in acute coronary syndromes: position paper from the joint EHRA, ACCA, and
EAPCI task forceEuropace. 2014;16(11):1655-1673. doi:10.1093/europace/euu208
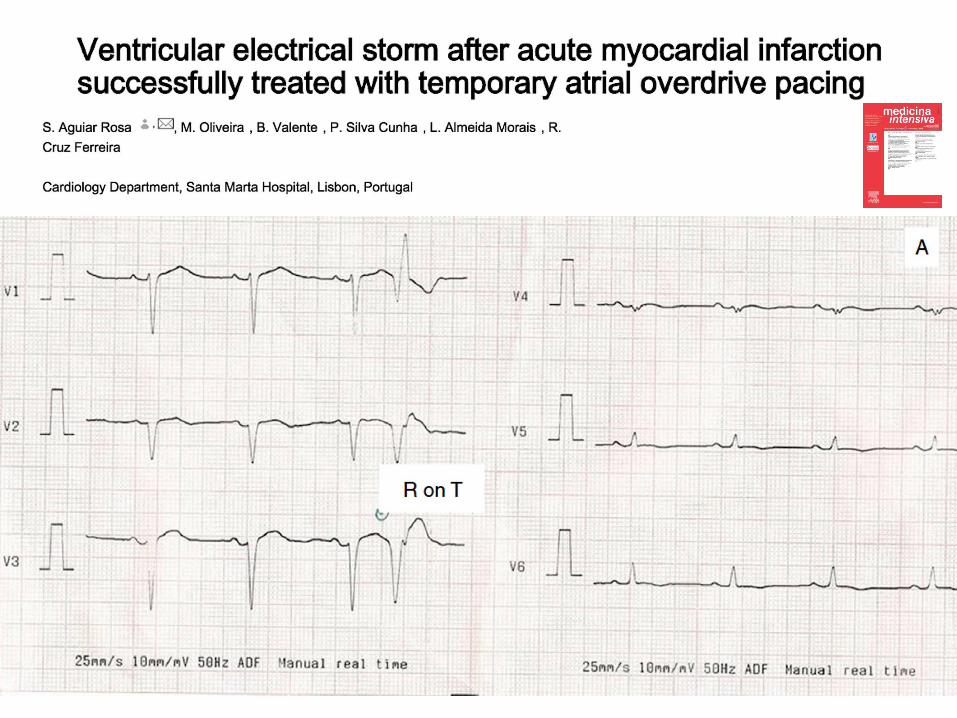
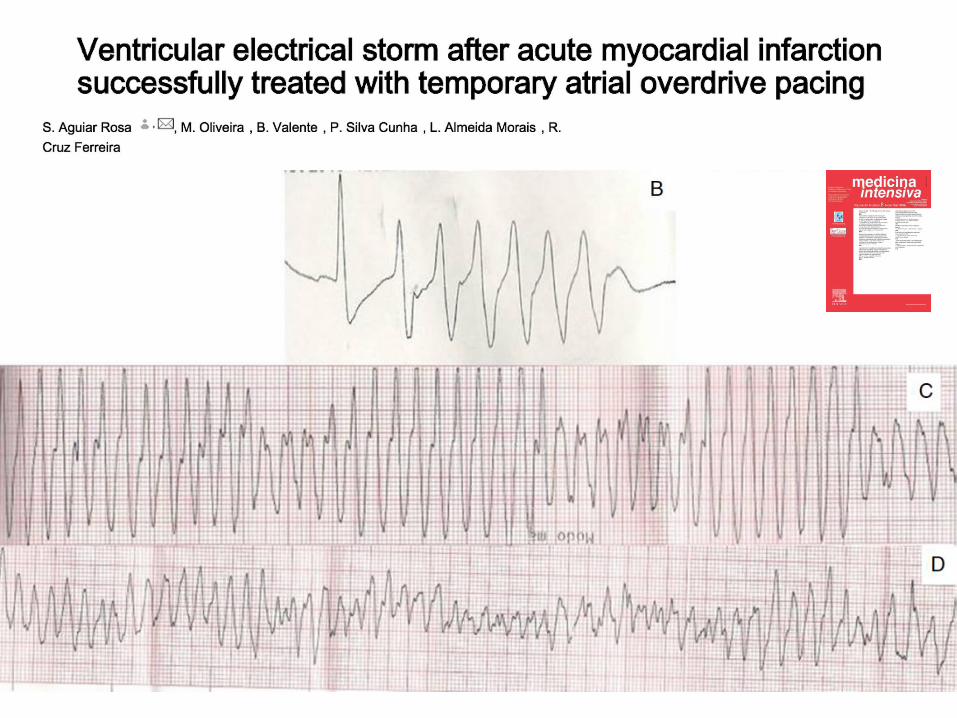
Ventricular Arrythmias
• Recent evidence supports the assumption that sustained VA in the setting of an ACS is also dependent on an individual genetic predisposition to such events.
• This is most obvious in patients with inherited cardiomyopathies that confer electrical instability but may also be mediated by common genetic variants.
Cardiac arrhythmias in acute coronary
syndromes: position paper from the
joint EHRA, ACCA, and EAPCI task
forceEuropace. 2014;16(11):1655-1673.
From: Cardiac arrhythmias in acute coronary syndromes: position paper from the joint EHRA, ACCA, and
EAPCI task forceEuropace. 2014;16(11):1655-1673. doi:10.1093/europace/euu208
Sistema Nervoso Autónomo
• Supervisão do status e
actuação de todo o
sistema cardiovascular
• Componentes Simpático
e Parassimpático:
• Jogadores chave no
controlo cardiovascular
Mechanical complications of acute myocardial infarction
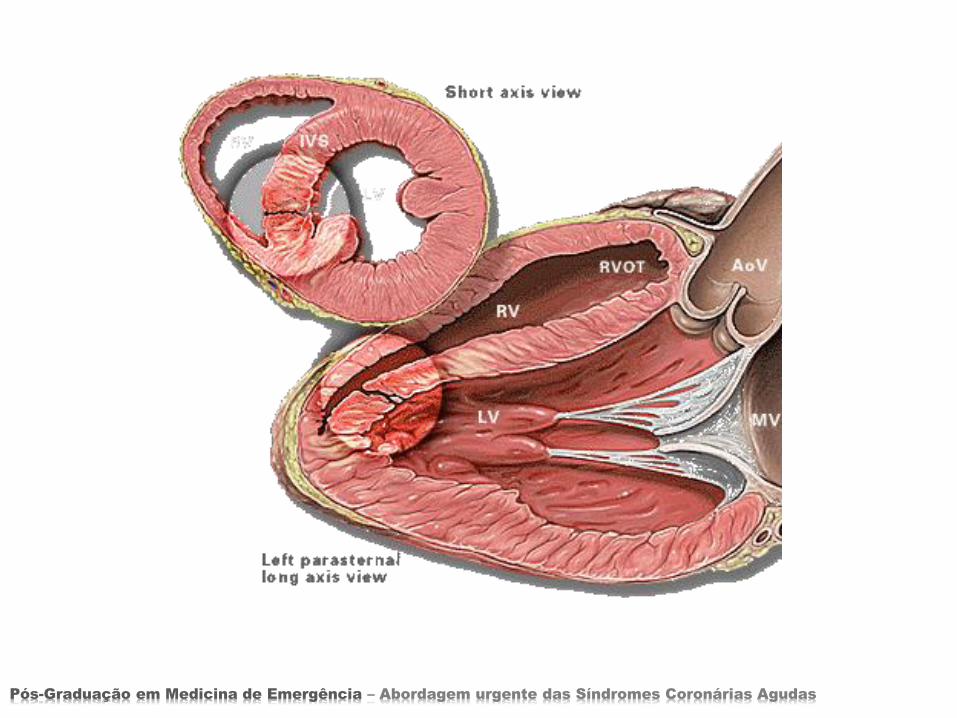
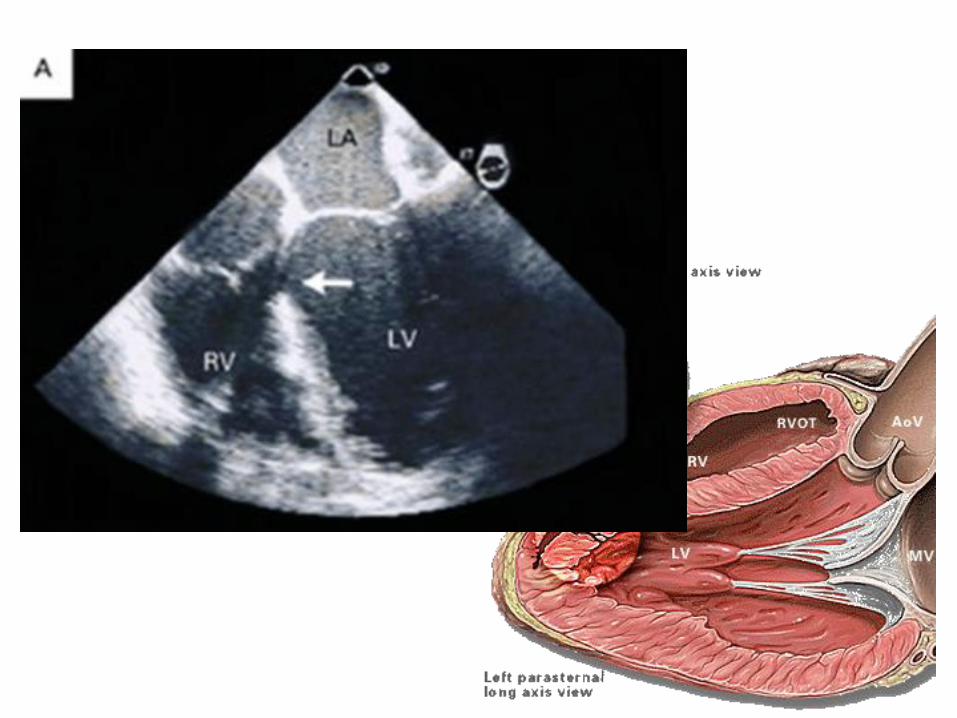
• The main mechanical complications (MC) of acute myocardial infarction are ventricular septal rupture(VSR), free wall rupture(FWR), and ischemic mitral regurgitation (IMR).
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas
VENTRICULAR SEPTAL RUPTURE
• The incidence of VSR in the pre-thrombolytic era was between 1-3 percent, and has declined with the use of fibrinolytic agents to 0.2 percent
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas
• The time of occurrence has changed from 3-5 days from the onset of the AMI in the pre-thrombolytic era to less than 24 hours with thrombolysis
VENTRICULAR SEPTAL RUPTURE
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas
• The known risk determinants for this complication are:
• Advanced age, female sex, no previous smoking, anterior MI, worse killip class and, increased heart rate on admission
VENTRICULAR SEPTAL RUPTURE
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas
• On angiography, there is a higher occurance of total occlusion of the IRA (57%), usually the LAD, less collaterals with low TIMI flow and low ejection fraction
VENTRICULAR SEPTAL RUPTURE
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas
• Outcome and treatment
• Mortality at 30 days is higher in patients with VSR than in those without this complication (73.8% versus 6.8%, P<0.001).
• Patients with VSDs selected for surgical repair have better outcomes than patients treated medically (30-day mortality, 47% versus 94%) (7).
• When the clinical presentation is cardiogenic shock with RV dysfunction in the setting of inferior wall MI, the prognosis is grave.
VENTRICULAR SEPTAL RUPTURE
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas
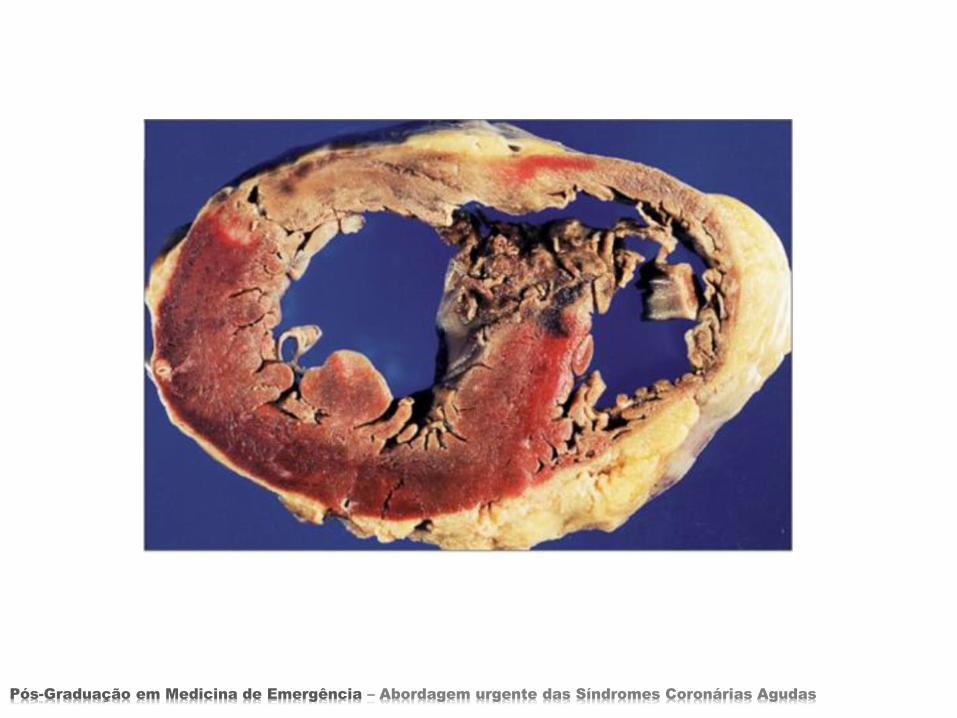
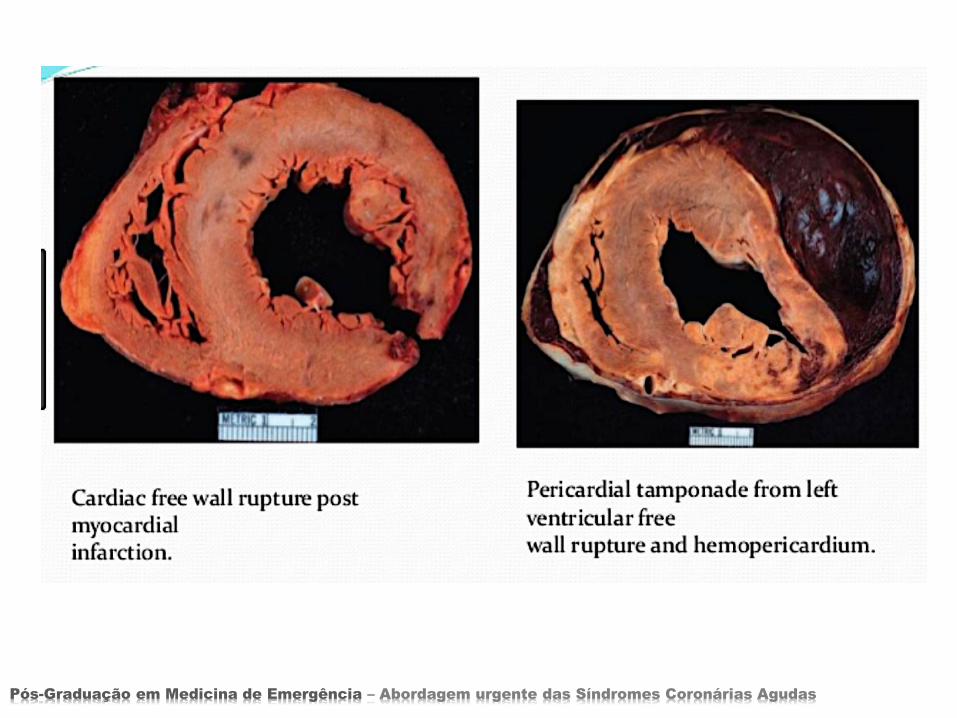
FREE WALL RUPTURE
• develops with large transmural anterior wall MI, that involves more than 20 percent of the LV.
• It is usually preceded by infarct expansion, it appears in the junction of the infarct and the normal muscle and it rarely occurs in the thickened ventricule with good collaterals
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas
FREE WALL RUPTURE
• It can present as an acute tear with immediate death or subacute allowing opportunity for intervention.
• Rupture can occur as early as the first day after infarction, although it most often occurs later in the first week in the setting of myocardial necrosis and neutrophilicinfiltration
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas
FREE WALL RUPTURE
• It is a fatal compliction that contributes to 10 percent of AMI mortality and it is the second cause of death after pump failure
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas
FREE WALL RUPTURE
• The incidence of FWR can probably be reduced by reducing infarct size with immediate reperfusion, avoiding agents that interfere with the healing process like steroids and NSAID, and attenuating wall stress.
• Survival depends on immediate diagnosis, hemodynami stabilisation and prompt surgical repair. Delayed thrombolysis increases the risk and primary PCI reduces it.
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas

ISCHEMIC MITRAL REGURGITATION
• In the acute stage of AMI, the etiology of mitral regurgitation is either papillary muscle dysfunction/ rupture or rupture of chordae.
• In the chronic stage, mitral annulus dilation, tethering of mitral leaflets and localised wall motion abnormalities are the mechanisms underlying MR.
• In the acute setting the volume of regurgitation, LV function and LA compliance determine the clinical presentation and the prognosis.
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas
ISCHEMIC MITRAL REGURGITATION
• Patients with chronic ischemic MR have a higher cardiovascular mortality rate compaired to no MR (29 % vs 12%, p<0.001, 3.5 y follow up ),
• higher rate of persistently occluded IRA (27.3% vs 15.2%, p=0, 001),
• larger LV volume and they develop more often severe heart failure
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas
ISCHEMIC MITRAL REGURGITATION
• A MR increase significantly the 5 year cardiac and total mortality of patients with reduced LV function with a relative risk of 1.83 and 1.88 respectively.
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas
ISCHEMIC MITRAL REGURGITATION
• Mitral valve replacement is the procedure of choice for acute MR, yet mitral valve repair may be feasible
Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas

Pós-Graduação em Medicina de Emergência – Abordagem urgente das Síndromes Coronárias Agudas
Prevention
Prevention of all these severe complications can be achieved by/with :
1-Early and efficient reperfusion and surgical repair
2-Preventing reperfusion injury3-Preventing breakdown of extracellular collagen,
necrosis and apoptosis.4-Preserving the microcirculation
5-Modulation of tissue repair like hypertrophy and fibrosis


















