Efficiency improvement of primary care prescription by physicians - pharmacists cooperating in...
1
Efficiency improvement of primary care prescription by physicians - pharmacists cooperating in quality circles Ruggli M. 1 , Nyffeler R. 3 , Duay B. 4 , Repond C. 4 , Buchmann M. 4 , Bugnon O. 1;2 1 Swiss Association of Pharmacists, Liebefeld, Switzerland 2 Community Pharmacy of the University Medical Outpatient Clinic, Lausanne, Switzerland 3 Medical Association of Primary Care Physicians, Fribourg, Switzerland 4 Pharmaceutical Association of Pharmacists, Fribourg, Switzerland Contact address: [email protected] AIMS OF THE STUDY: In 1997 the Medical and Pharmacist's associations of Fribourg, Switzerland, launched a pilot project of cooperation between physicians and pharmacists: 6 pharmacists each coached a quality circle with a total of 27 physicians. The circles worked on 17 therapeutic groups comparing the risk/benefit of drugs, discussing prescribing patterns and trying to agree on treatment options based on two objectives: improving the quality and efficiency of care. After the encouraging results reported in 1999 and 2000 1 , the new assessment is based on the years 1999 to 2002. RESULTS: During these 4 years the overall cost of drugs increased by 39% in the control group (80 comparable general practitioners, but not involved with pharmacists in quality circles) and 30% in the 6 circles (figure 1) CONCLUSIONS: This study confirmed the added value of physicians-pharmacists quality circles as local care managing projects for the improvement of drug prescription efficiency.Quality circles at a local level succeed in promoting the use of evaluated generics and other cost- and outcome-effective activities including evidence-based analyses of new drugs, interdisciplinary continuing education on the rational use of drugs, implementation at a local level of national or international guidelines, continuing and comparative follow-up of the consensus implementation. Community pharmacists can influence physicians’ attitudes and are efficient partners in care management. The project has now disseminated throughout Switzerland and has been acknowledged by politicians and major private insurers. A financial incentive was granted for the pilot project and a national negotiation started in 2004. Fig. 1 cost evolution between 1999 and 2002 for quality circles and control group Fig. 4 : Proportion of prescribed coxibs, A2A and glitazones REFERENCES 1 Increase of generics prescription by physicians involved with pharmacists in quality circles, O. Bugnon, I. Gremaud-Tinguely, C. Repond, J. Carrel, D. Muscionico, R. Nyffeler and M. Buchmann, FIP 2000 1. Prescription data (benchmarking per physician and therapeutic class) 2. Education on guidelines, Evidence-based medecine and pharmacoeconomy. 3. Analysis of prescription attitudes in comparison with scientific and economic data and search for alternatives in drug market 4. Consensus of each quality circle 5. Application of the consensus 6. Check on the impact of the consensus 7. Assessment of the results and improvements Work process Continous quality improvement of prescription CONCEPT OF PHYSICIANS-PHARMACISTS QUALITY CIRCLES: The quality circles are stable groups of 4 to 10 physicians with one (or more) pharmacist as moderator. Based on the physicians’own current prescription data, pharmacists and physicians are involved in the continuous quality improvement of prescribing practices, thanks to education on guidelines, evidence-based medicine and pharmacoeconomy. 121.7 130.6 139.0 115.2 126.7 130.0 100.0 105.0 110.0 115.0 120.0 125.0 130.0 135.0 140.0 145.0 1999 2000 2001 2002 D rugs' costevolution (Index) C ontrol group Quality circles +15.2% +10.0% +2.6% +21.7% +7.3% +6.4% In 2002 this 9% increase difference represents a saving of about 48’000 CHF per physician (circa $ 37’000.- in August 2004) More reasonable influence of marketing and advertising: less coxibs (10.5 vs 17.3%), A2A (23.8 vs 29.4%) or glitazones (3.5 vs 5.2%) (fig 4). 13.0 21.1 17.5 33.5 19.7 38.5 19.3 38.9 25.0 41.4 22.6 46.9 0.0 5.0 10.0 15.0 20.0 25.0 30.0 35.0 40.0 45.0 50.0 control group quality circles control group quality circles Percentageofgenerics'packages 2000 2001 2002 ANTIBIOTICS NSAIDS Fig. 2 Generics prescription for antibiotics and NSAIDS 15.9 13.8 20.9 17.7 16.7 11.3 25.3 20.3 2.5 1.7 17.3 10.5 29.8 23.8 5.2 3.5 0.0 5.0 10.0 15.0 20.0 25.0 30.0 35.0 control group Q uality circles C ontrol group Q uality circles C ontrol group Q uality circles % ofpackagesfrom specific pharm acological classe 2000 2001 2002 GLITAZONES A2A COXIBS Higher rate of generics prescription (42 vs 25% for antibiotics, 47 vs 22% for NSAIDs) (fig 2) The physicians working with pharmacists changed their prescription patterns in a lasting way, as can been seen in 2002: Qualitatively more adapted frequency of prescription: lower for antibiotics (25.2 vs 28.4%) and NSAIDS (37.8 vs 40.1%) (fig3) 28.4 25.2 37.8 40.1 0 5 10 15 20 25 30 35 40 45 C ontrol G roup Q uality circles C ontrol group Q uality circles % ofpatientstreated w ith a specificdrug group 2002 ANTIBIOTICS NSAIDS Fig. 3 Prescription frequency of antibiotics and NSAIDS Schweizerischer Apothekerverband Société Suisse des Pharmaciens Società Svizzera dei Farmacisti
-
Upload
gavin-armstrong -
Category
Documents
-
view
215 -
download
0
Transcript of Efficiency improvement of primary care prescription by physicians - pharmacists cooperating in...

Efficiency improvement of primary care prescription by
physicians - pharmacists cooperating in quality circles
Ruggli M.1, Nyffeler R. 3, Duay B.4, Repond C.4, Buchmann M. 4, Bugnon O.1;2
1 Swiss Association of Pharmacists, Liebefeld, Switzerland2 Community Pharmacy of the University Medical Outpatient Clinic, Lausanne, Switzerland3 Medical Association of Primary Care Physicians, Fribourg, Switzerland4 Pharmaceutical Association of Pharmacists, Fribourg, Switzerland Contact address: [email protected]
AIMS OF THE STUDY:In 1997 the Medical and Pharmacist's associations of Fribourg, Switzerland, launched a pilot project of cooperation between physicians and pharmacists: 6 pharmacists each coached a quality circle with a total of 27 physicians. The circles worked on 17 therapeutic groups comparing the risk/benefit of drugs, discussing prescribing patterns and trying to agree on treatment options based on two objectives: improving the quality and efficiency of care. After the encouraging results reported in 1999 and 2000 1, the new assessment is based on the years 1999 to 2002.
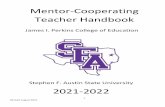
RESULTS: During these 4 years the overall cost of drugs increased by 39% in the control group (80 comparable general practitioners, but not involved with pharmacists in quality circles) and 30% in the 6 circles (figure 1)
CONCLUSIONS: This study confirmed the added value of physicians-pharmacists quality circles as local care managing projects for the improvement of drug prescription efficiency.Quality circles at a local level succeed in promoting the use of evaluated generics and other cost- and outcome-effective activities including evidence-based analyses of new drugs, interdisciplinary continuing education on the rational use of drugs, implementation at a local level of national or international guidelines, continuing and comparative follow-up of the consensus implementation.Community pharmacists can influence physicians’ attitudes and are efficient partners in care management.The project has now disseminated throughout Switzerland and has been acknowledged by politicians and major private insurers. A financial incentive was granted for the pilot project and a national negotiation started in 2004.
Fig. 1 cost evolution between 1999 and 2002
for quality circles and control group
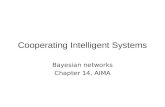
Fig. 4 : Proportion of prescribed coxibs, A2A and glitazones
REFERENCES1 Increase of generics prescription by physicians involved with pharmacists in quality circles, O. Bugnon, I. Gremaud-Tinguely, C. Repond, J. Carrel, D. Muscionico, R. Nyffeler and M. Buchmann, FIP 2000
1. Prescription data (benchmarking per physician
and therapeutic class)
2. Education on guidelines,Evidence-based medecine and pharmacoeconomy.
3. Analysis of prescription attitudes in comparison with scientific and economic data and search for alternatives in drug market
4. Consensus of each quality circle
5. Application of the consensus
6. Check on the impact of the consensus
7. Assessment of the results and improvements
Work processContinous quality improvement of prescription
CONCEPT OF PHYSICIANS-PHARMACISTS QUALITY CIRCLES:The quality circles are stable groups of 4 to 10 physicians with one (or more) pharmacist as moderator. Based on the physicians’own current prescription data, pharmacists and physicians are involved in the continuous quality improvement of prescribing practices, thanks to education on guidelines, evidence-based medicine and pharmacoeconomy.
121.7
130.6
139.0
115.2
126.7130.0
100.0
105.0
110.0
115.0
120.0
125.0
130.0
135.0
140.0
145.0
1999 2000 2001 2002
Dru
gs
' co
st
ev
olu
tio
n (
Ind
ex
)
Control group
Quality circles+15.2%
+10.0%
+2.6%
+21.7%
+7.3%
+6.4%
In 2002 this 9% increase difference represents a saving of about 48’000 CHF per physician (circa $ 37’000.- in August 2004)
More reasonable influence of marketing and advertising: less coxibs (10.5 vs 17.3%), A2A (23.8 vs 29.4%) or glitazones (3.5 vs 5.2%) (fig 4).
13.0
21.1
17.5
33.5
19.7
38.5
19.3
38.9
25.0
41.4
22.6
46.9
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
50.0
control group quality circles control group quality circles
Per
cen
tage
of
gen
eric
s' p
ack
ages
2000 2001 2002
ANTIBIOTICS
NSAIDS
Fig. 2 Generics prescription for antibiotics and NSAIDS
15.9
13.8
20.9
17.7
16.7
11.3
25.3
20.3
2.5
1.7
17.3
10.5
29.8
23.8
5.2
3.5
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
controlgroup
Qualitycircles
Controlgroup
Qualitycircles
Controlgroup
Qualitycircles
% o
f pa
ckag
es f
rom
spe
cifi
c ph
arm
acol
ogic
al c
lass
es
2000
2001
2002
GLITAZONES
A2A
COXIBS
Higher rate of generics prescription (42 vs 25% for antibiotics, 47 vs 22% for NSAIDs) (fig 2)
The physicians working with pharmacists changed their prescription patterns in a lasting way, as can been seen in 2002:
Qualitatively more adapted frequency of prescription: lower for antibiotics (25.2 vs 28.4%) and NSAIDS (37.8 vs 40.1%) (fig3)
28.4
25.2
37.8
40.1
0
5
10
15
20
25
30
35
40
45
Control Group Quality circles Control group Quality circles
% o
f p
atie
nts
tre
ated
wit
h a
sp
ecif
ic d
rug
grou
p
2002ANTIBIOTICS
NSAIDS
Fig. 3 Prescription frequency of antibiotics and NSAIDS
Schweizerischer ApothekerverbandSociété Suisse des PharmaciensSocietà Svizzera dei Farmacisti