Effects of Dobutamine Open Heart Surgery -...
10
DOBUTAMINE AFTER OPEN HEART SURGERY/Sakamoto, Yamada Consultants and Associates Jack M. Becktel James A. Hagans, M.D., Ph.D. C. Morton Hawkins, Sc.D. Sibley W. Hoobler, M.D. Arthur F. Johnson, Ph.D. H. M. Perry, M.D. Harold W. Schnaper, M.D. Lawrence W. Shaw William M. Smith, M.D. References 1. Page IH, Hurley RE, Dustan HP: The prolonged treatment of hyperten- sion with guanethidine. JAMA 175: 543, 1961 2. Kelly JJ Jr, Housel EL, Daly JW: Clinical experience with guanethidine in the treatment of hypertension. JAMA 176: 577, 1961 3. Maronde RF, Haywood LJ, Barbour B: Comparison of guanethidine and guanethidine plus a thiazide diuretic. Am J Med Sci 242: 228, 1961 4. Editorial: Today's drugs: Bethanidine sulfate. Br Med J 2: 865, 1964 5. Gibb WE, Malpos JS, Turner P, White RJ: Comparison of bethanidine, alpha methyldopa and reserpine in essential hypertension. Lancet 2: 275, 1970 6. Prichard BNC, Johnston AW, Hill ID, Rosenheim ML: Bethanidine, guanethidine and alpha methyldopa in treatment of hypertension. A within patient comparison. Br Med J 1: 135, 1968 7. Gifford RW Jr: Bethanidine sulphate - a new antihypertensive agent. JAMA 193: 901, 1965 8. Editorial: Today's drugs: Bethanidine. Br Med J 1: 285, 1967 9. Swinyard EA, Harvey SC: Adrenergic blocking drugs. In Remington's Pharmaceutical Series, edited by Martin EW. Easton, Mack Publishing Co., 1965, pp 988-989 10. Page LB, Sidd JJ: Medical Management of Primary Hypertension. Boston, Little, Brown, 1973, pp 42-46 11. Veterans Administration Cooperative Study Group on Antihypertensive Agents: Effects of treatment on morbidity in hypertension. Results in patients with diastolic blood pressures averaging 115 through 129 mm Hg. JAMA 202: 116, 1967 12. Veterans Administration Cooperative Study Group on Antihypertensive Agents: Effects of treatment on morbidity in hypertension. II. Results in patients with diastolic blood pressures averaging 90 through 114 mm Hg. JAMA 213: 1143, 1970 Hemodynamic Effects of Dobutamine in Patients Following Open Heart Surgery TOHRU SAKAMOTO, M.D., AND TAKASHI YAMADA, M.D. SUMMARY Dobutamine, a new synthetic inotropic agent, was ad- ministered by intravenous infusion to 22 patients following open heart surgery. The dosage of dobutamine started from 2Ag/kg/min and was increased stepwise to 4, 6, and 8 ,ug/kg/min. Cardiac index in- creased from 2.54 ± 0.13 to 3.11 ± 0.19 and 3.50 ± 0.22 L/min/m2 with 4 and 8 ,tg/kg/min, respectively. Heart rate increased from 87.6 ± 2.9 to 96.4 ± 2.3 and 108.9 ± 3.2 beats/min with 4 and 8 ,gg/kg/min, respectively. Systolic and mean aortic pressure and systolic pulmonary arterial pressure were elevated from 126.0 ± 3.8 to 144.6 ± 6.0 mm Hg, from 91.8 ± 2.7 to 96.2 ± 3.2 mm Hg, and ISOPROTERENOL, a potent beta-adrenergic stimulator, has been widely used for the treatment of cardiac failure, cardiogenic shock, or low output syndrome following open heart surgery.1-3 Although infusion of isoproterenol improves myocardial performance, occurrence of adverse side effects such as tachycardia, ventricular arrhythmia, and reduced perfusion pressure, often necessitates the discontinuation of this drug. Furthermore, isoproterenol has been shown experimentally to intensify myocardial ischemia and to extend infarct size after coronary narrowing or occlusion resulting in acute myocardial failure.4 An agent with inotropic effect as potent as isoproterenol but without significant effects on vasomotor tone, heart rate, or rhythm would be desirable for the treatment of myocar- From the Division of Cardiovascular Surgery, First Department of Surgery, School of Medicine, Tokyo Medical and Dental University, Tokyo, Japan. Address for reprints: Tohru Sakamoto, M.D., Division of Cardiovascular Surgery, First Department of Surgery, School of Medicine, Tokyo Medical and Dental University, No. 1-5-45, Yushima, Bunkyo-Ku, Tokyo, Japan. Received June 23, 1976; revision accepted September 30, 1976. from 33.4 ± 2.3 to 37.1 ± 2.5 mm Hg with 8 Ag/kg/min, while other pressures were unchanged. Mean left atrial pressure fell significantly from 15.9 ± 0.6 to 14.8 ± 0.7 mm Hg. Stroke volume index, stroke work index, and left ventricular work also increased. Premature ven- tricular beats were observed in only one patient during dobutamine in- fusion, but no other side effect was observed. We conclude that dobutamine is a potent inotropic agent which in- creases cardiac output without causing significant tachycardia or arrhythmias, and is useful for the treatment of patients following open heart surgery. dial pump failure. Recently, Tuttle and Millis synthesized a new beta-adrenergic stimulator.6 This new beta-adrenergic stimulator, dobutamine, which is synthesized by modifying the side-chain of dopamine, is reported to have a strong in- otropic action with a weak chronotropic action and little effect on peripheral vessels.7-14 In this study, we examined the acute hemodynamic effects of dobutamine on patients following open heart surgery and compared the hemodynamic responses with isoproterenol infusion. Method and Materials The study group (table I) consisted of 22 patients hospitalized at the Tokyo Medical and Dental University Hospital for open heart surgery. Their ages ranged from 19 to 54 years with a mean of 32.5 years. The surgical procedure for aortic valve replacement with the Starr- Edwards ball prosthesis was performed during either cor- onary perfusion or a period of anoxic arrest. For other sur- gical procedures which included mitral valve replacement with the Starr-Edwards disc prosthesis, an anoxic arrest was 525 by guest on May 23, 2018 http://circ.ahajournals.org/ Downloaded from
Transcript of Effects of Dobutamine Open Heart Surgery -...

DOBUTAMINE AFTER OPEN HEART SURGERY/Sakamoto, Yamada
Consultants and Associates
Jack M. BecktelJames A. Hagans, M.D., Ph.D.C. Morton Hawkins, Sc.D.Sibley W. Hoobler, M.D.Arthur F. Johnson, Ph.D.H. M. Perry, M.D.Harold W. Schnaper, M.D.Lawrence W. ShawWilliam M. Smith, M.D.
References
1. Page IH, Hurley RE, Dustan HP: The prolonged treatment of hyperten-sion with guanethidine. JAMA 175: 543, 1961
2. Kelly JJ Jr, Housel EL, Daly JW: Clinical experience with guanethidinein the treatment of hypertension. JAMA 176: 577, 1961
3. Maronde RF, Haywood LJ, Barbour B: Comparison of guanethidine and
guanethidine plus a thiazide diuretic. Am J Med Sci 242: 228, 19614. Editorial: Today's drugs: Bethanidine sulfate. Br Med J 2: 865, 19645. Gibb WE, Malpos JS, Turner P, White RJ: Comparison of bethanidine,
alpha methyldopa and reserpine in essential hypertension. Lancet 2: 275,1970
6. Prichard BNC, Johnston AW, Hill ID, Rosenheim ML: Bethanidine,guanethidine and alpha methyldopa in treatment of hypertension. Awithin patient comparison. Br Med J 1: 135, 1968
7. Gifford RW Jr: Bethanidine sulphate - a new antihypertensive agent.JAMA 193: 901, 1965
8. Editorial: Today's drugs: Bethanidine. Br Med J 1: 285, 19679. Swinyard EA, Harvey SC: Adrenergic blocking drugs. In Remington's
Pharmaceutical Series, edited by Martin EW. Easton, Mack PublishingCo., 1965, pp 988-989
10. Page LB, Sidd JJ: Medical Management of Primary Hypertension.Boston, Little, Brown, 1973, pp 42-46
11. Veterans Administration Cooperative Study Group on AntihypertensiveAgents: Effects of treatment on morbidity in hypertension. Results inpatients with diastolic blood pressures averaging 115 through 129 mmHg. JAMA 202: 116, 1967
12. Veterans Administration Cooperative Study Group on AntihypertensiveAgents: Effects of treatment on morbidity in hypertension. II. Results inpatients with diastolic blood pressures averaging 90 through 114 mm Hg.JAMA 213: 1143, 1970
Hemodynamic Effects of Dobutaminein Patients Following Open Heart Surgery
TOHRU SAKAMOTO, M.D., AND TAKASHI YAMADA, M.D.
SUMMARY Dobutamine, a new synthetic inotropic agent, was ad-ministered by intravenous infusion to 22 patients following open heartsurgery. The dosage of dobutamine started from 2Ag/kg/min andwas increased stepwise to 4, 6, and 8 ,ug/kg/min. Cardiac index in-creased from 2.54 ± 0.13 to 3.11 ± 0.19 and 3.50 ± 0.22 L/min/m2with 4 and 8 ,tg/kg/min, respectively. Heart rate increased from87.6 ± 2.9 to 96.4 ± 2.3 and 108.9 ± 3.2 beats/min with 4 and 8,gg/kg/min, respectively. Systolic and mean aortic pressure andsystolic pulmonary arterial pressure were elevated from 126.0 ± 3.8to 144.6 ± 6.0 mm Hg, from 91.8 ± 2.7 to 96.2 ± 3.2 mm Hg, and
ISOPROTERENOL, a potent beta-adrenergic stimulator,has been widely used for the treatment of cardiac failure,cardiogenic shock, or low output syndrome following openheart surgery.1-3
Although infusion of isoproterenol improves myocardialperformance, occurrence of adverse side effects such astachycardia, ventricular arrhythmia, and reduced perfusionpressure, often necessitates the discontinuation of this drug.Furthermore, isoproterenol has been shown experimentallyto intensify myocardial ischemia and to extend infarct sizeafter coronary narrowing or occlusion resulting in acutemyocardial failure.4An agent with inotropic effect as potent as isoproterenol
but without significant effects on vasomotor tone, heart rate,or rhythm would be desirable for the treatment of myocar-
From the Division of Cardiovascular Surgery, First Department ofSurgery, School of Medicine, Tokyo Medical and Dental University, Tokyo,Japan.
Address for reprints: Tohru Sakamoto, M.D., Division of CardiovascularSurgery, First Department of Surgery, School of Medicine, Tokyo Medicaland Dental University, No. 1-5-45, Yushima, Bunkyo-Ku, Tokyo, Japan.
Received June 23, 1976; revision accepted September 30, 1976.
from 33.4 ± 2.3 to 37.1 ± 2.5 mm Hg with 8 Ag/kg/min, while otherpressures were unchanged. Mean left atrial pressure fell significantlyfrom 15.9 ± 0.6 to 14.8 ± 0.7 mm Hg. Stroke volume index, strokework index, and left ventricular work also increased. Premature ven-tricular beats were observed in only one patient during dobutamine in-fusion, but no other side effect was observed.We conclude that dobutamine is a potent inotropic agent which in-
creases cardiac output without causing significant tachycardia orarrhythmias, and is useful for the treatment of patients followingopen heart surgery.
dial pump failure. Recently, Tuttle and Millis synthesized anew beta-adrenergic stimulator.6 This new beta-adrenergicstimulator, dobutamine, which is synthesized by modifyingthe side-chain of dopamine, is reported to have a strong in-otropic action with a weak chronotropic action and littleeffect on peripheral vessels.7-14
In this study, we examined the acute hemodynamic effectsof dobutamine on patients following open heart surgery andcompared the hemodynamic responses with isoproterenolinfusion.
Method and Materials
The study group (table I) consisted of 22 patientshospitalized at the Tokyo Medical and Dental UniversityHospital for open heart surgery. Their ages ranged from 19to 54 years with a mean of 32.5 years. The surgicalprocedure for aortic valve replacement with the Starr-Edwards ball prosthesis was performed during either cor-onary perfusion or a period of anoxic arrest. For other sur-gical procedures which included mitral valve replacementwith the Starr-Edwards disc prosthesis, an anoxic arrest was
525
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 55, No 3, MARCH 1977
TABLE 1. Study GroupNYHA
Pt/Age/Sex Diagnosis class Operation
N.T. /22/M MI III MAPS.N. /48/F MS II OMCA.Y. /32/M Marfan's syndrome III AVR + MVRA.S. /39/F ASD II ASD closureH.S. /21/M VSD + Al III VSD closure
+ AVPK.S. /54/M AI III AVRY.S. /34/F MS III OMCM.T. /21/M ASD + PS II ASD closure
+ PCE.O. /19/F ASD I ASD closureT.S. /34/M AI + MI III AVR + MVRN.S. /19/F ASD I ASD closureE.K. /27/F MI III MAPY.O. /35/F AI III AVRY.O. /33/F Al III AVRK.Y. /22/M ASD I ASD closureH.Y. /37/F ASD II ASD closureT.I. /23/M VSD I VSD closureH.K. /37/M MS + PH IV OMCN.S. /48/F MS III OMCY.H. /29/M MS + PH IV OMCT.O. /29/F MS II OMCT.M. /47/M MI IV MVR
Abbreviations: AI = aortic insufficiency; ASD = atrial septal defect;AVP = aortic valvuloplasty; AVR = aortic valve replacement; MAP =mitral annuloplasty; MI = mitral insufficiency; MS = mitral stenosis;MVR = mitral valve replacement; OMC = open mitral commissurotomy;PC = pulmonary commissurotomy; PH = pulmonary hypertension;PS = pulmonary valvular stenosis; VSD = ventricular septal defect.
used. The cardiopulmonary bypass technique utilizedhemodilution, the Temptrol Q-100 disposable bubble oxy-genator, and perfusion rates of 3.0 L/min/m2 at nor-mothermia.At operation, 19 gauge Teflon catheters (30 cm in length)
were placed in the main trunk of the pulmonary artery andthe left atrium. They were connected through the operativewound to metal three-cockplates outside of the thorax. Inorder to keep the catheters patent postoperatively, one armof the three-way cock was connected to a continuous micro-infusion pump. The remaining arm was connected to anelectric manometer. A 19 gauge polyethylene catheter (70cm in length) was inserted into the left radial artery andpassed to the aortic arch.
Central aortic pressure was measured through thecatheter, which was used also as the cuvette circuit for dye-dilution method to determine the cardiac output. Pulmonaryarterial pressure, left atrial pressure, and aortic pressurewere simultaneously obtained from the Statham P-23Dbpressure transducers using the midchest as the zero referencepoint and recorded at various paper speeds on multichannelrecorder. Mean values of these pressures were also obtainedusing an electronic integrating circuit. Cardiac output wasdetermined by duplicated dye-dilution technique. After se-quential injections of indocyanine green (5 mg) into the maintrunk of the pulmonary artery and the left atrium, arterialblood was sampled by continuous withdrawal pump at aspeed of 34.5 ml/min. Dye-dilution curves were recordedand the cardiac output was computed by an -Erma BloodFlow Computer (Erma Optical Company). The arithmeticmean of cardiac output was derived from the average of thetwo curves which were obtained from the injections into thetrunk of the pulmonary artery and the left atrium. Left ven-
tricular stroke work index (LVSWI) in g-m/beat/m' andsystemic vascular resistance (SVR) in units were calculatedas follows:
LVSWI =SVI X (MAP - MLAP)X 13.6
1000
SVR = MAPCO
Where SVI = stroke volume index (ml/beat/m2), MAP =mean aortic pressure (mm Hg) and CO = cardiac output(L/min).
Studies were carried out within six hours following openheart surgery. Dobutamine was infused with a Harvard infu-sion pump and its dose was increased stepwise from 2 to 4, 6,and 8 Atg/kg/min at a 15 min interval. Various hemody-namic parameters mentioned above were determined beforethe start of infusion, during the infusion at a rate of 2, 4, 6and 8 Mg/kg/min, and at 5 and 10 minutes after stopping theinfusion. In three of the 22 patients studied, the response todobutamine was tested in a similar manner 12 to 24 hoursafter the original test. Thus, the final statistical analysis ofthe effects of dobutamine on hemodynamics was made witha total number of 25.
In nine out of the 22 patients, isoproterenol was infusedwith a Harvard infusion pump at 30 min after the dobuta-mine study and its dose was increased from 0.005 to 0.01 and0.02 ,ug/kg/min at 15 min intervals. Hemodynamic resultsobtained with dobutamine and isoproterenol in the samenine patients were compared with each other.
All patients received blood transfusion to maintain leftatrial pressure above 12 mm Hg and 21 patients had anuneventful recovery and did not require pharmacologicalsupport therapeutically during the postoperative period.Statistical analysis utilized the Student's t-test on a paired orunpaired basis as appropriate. A P value of less than 0.05was considered to indicate a significant difference betweencompared group of data.
Results
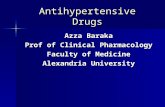
Table 2 shows changes in various hemodynamic param-eters obtained from dobutamine infusion. With infusion ofdobutamine, systolic aortic pressure showed a significantand constant increase by 17.1 mm Hg (13.6%) from anaverage of 126.0 ± 3.8 to 144.6 ±: 6.0 mm Hg, but on dis-continuation of infusion, it immediately decreased to a levellower than the control value by 2 mm Hg (fig. 1). No signifi-cant change was observed in diastolic aortic pressure butmean aortic pressure showed a significant increase by 4.4mm Hg (4.8%) from an average of 91.8 ± 2.7 to 96.2 ± 3.2mm Hg. Pulmonary arterial pressure showed changessimilar to aortic pressure. Systolic pulmonary arterial pres-sure showed a significant increase by 3.7 mm Hg (11.1%)from an average of 33.4 ± 2.3 to 37.1 ± 2.5 mm Hg withdobutamine but it showed a significantly lower value thanthe control after its termination. No significant change wasobserved either in diastolic or mean pulmonary arterialpressure with dobutamine infusion. However, meanpulmonary arterial pressure showed a significant decreaseafter discontinuation of dobutamine. Mean left atrialpressure showed a slight but significant decrease from an
526 CIRCULATION
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

DOBUTAMINE AFTER OPEN HEART SURGERY/Sakamoto, Yamada
150 r
3- 140-rE 130ELH 120
in 110"Inn*U)rr
. _
L-0
.d4A\.EcE-J%._O
40$--
L-(.
V80 FI70 -
At Ie I I,. I .
control 2 4 6 8Dobutamine
(mcg/Kg/min)
5 .10 .mirt min.
FIGURE 1. Changes in aortic pressure with dobutamine. Systolicand mean aortic pressures showed a significant increase. Values aremean + standard error of mean.
average of 15.9 ± 0.6 to 14.8 + 0.7 mm Hg (7.2%). Afterdiscontinuation of dobutamine, mean left atrial pressureremained at the decreased level.
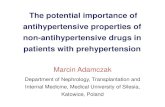
Cardiac index showed a significant stepwise increase withgraded doses of dobutamine (fig. 2). The increase in cardiacindex with each increase of dobutamine dose was 13.4, 22.4,31.4, and 37.7%, respectively, and the overall increase wasfrom an average of 2.54 + 0.13 to 3.50 + 0.22 L/min/m2.With cessation of dobutamine, cardiac index showed adecrease and was at the control level after 10 min. Heart rateincreased significantly from an average of 87.6 ± 2.9 to108.9 ± 3.2 beats/min (24.3%) but returned to the controlvalue 10 min after the stop of infusion.The only arrhythmia that developed in these cases during
dobutamine infusion was premature ventricular beats ob-served in a patient (E.K.). In a 39-year-old female patient(A.S.) with atrial septal defect, multiple premature ventric-ular beats were observed before infusion of dobutamine, butthey disappeared during dobutamine infusion. With discon-tinuation of dobutamine, the arrhythmia reappeared.
Left ventricular stroke work index showed a significant in-crease of 11.8%, from an average of 32.1 ± 2.9 to 35.9 ± 3.2g-m/beats/m2, immediately after the onset of dobutamineinfusion, and reached a plateau and returned to the controllevel upon the cessation of dobutamine.
Calculated systemic vascular resistance showed a signifi-cant decrease, from an average of 24.7 + 1.3 to 19.3 ± 1.2units (21.8%), but returned to the control value afterdobutamine infusion. The decrease in systemic vascularresistance was due to marked increase of cardiac output bydobutamine but not to a direct vasoactive effect of the drug.During hemodynamic studies, an interesting finding wasobserved in a 21-year-old patient (H.S.). His urinary outputwas between 40 and 50 ml/hour before infusion ofdobutamine but during dobutamine infusion urine volumewas markedly increased to 450 ml/hour and after the infu-sion urine volume returned to 42 ml/hour.Hemodynamic effects of isoproterenol infusion were com-
4.0 r
3.01F
2.0 -
control 2 4 6 8 5 .10 .Dobutamine min. min.
(mcg/Kg/min)FIGURE 2. Changes in cardiac index. With increased doses ofdobutamine, cardiac index showed a significant increase and at arate of 8 pg/kg/min, it was 37.7% higher than the control value.Values are mean + standard error of mean.
pared to dobutamine in the same nine patients out of thestudy group (table 3, fig. 3). With 0.02 ,ug/kg/min of isopro-terenol, aortic pressure changed from an average of 124/80(95) to 132/76 (93) mm Hg. But in dobutamine infusion,aortic pressure increased constantly from an average of123/76 (94) to 143/82 (101) mm Hg. At a comparable heartrate, 96.3 beats/min after 4 gg/kg/min of dobutamine vs96.6 beats/min after 0.005 pg/kg/min of isoproterenol, theincrease of cardiac index from control value was larger in
4.0
3.5 dobutamine
E
x 3.0c 2.5 1- FTi W isoproterenol(0 1192(5
80 90 100 110 120 130 140Heart Rate (beat/min)
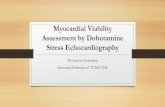
FIGURE 3. Changes in cardiac index and heart rate withdobutamine and isoproterenol. At comparable effects on cardiac in-dex, the increase in heart rate is less with dobutamine than withisoproterenol.
a a I II I
527
, r
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 55, No 3, MARCH 1977
TABLE 2. Hemodynamic Effects of DobutamineA B C D E F G
APs (mm Hg)N.T. 144 150 168 160 160 150 140S.N. 124 120 128 122 132 121 120S.N.* 140 146 148 144 152 136 130Y.A. 112 116 124 127 123 116 119A.S. 153 160 178 192 204 142 146H.S. 160 166 175 189 186 159 157K.S. 121 115 113 118 126 101 100K.S.* 95 106 108 116 110 105 104Y.S. 115 113 115 119 121 113 113M.T. 132 151 166 162 152 124 125E.O. 142 156 168 178 178 155 151T.S. 92 98 98 97 96 90 88T.S.* 98 98 105 102 105 98 98N.S. 126 137 123 130 148 128 129E.K. 156 149 150 166 149 147 151Y.O. 127 138 143 141 140 125 124Y.O. 142 145 150 158 151 141 133K.Y. 132 155 176 183 186 136 132H.Y. 141 160 170 178 175 145 151T.I. 132 148 170 166 189 137 132H.K. 103 108 105 109 107 102 112N.S. 123 138 143 143 150 138 135Y.H. 120 118 118 143 142 109 111T.O. 102 114 110 110 110 101 100T.M. 119 124 125 124 122 107 103Mean 126.0 133.2 139.1 143.1 144.6 125.0 124.2SE 3.8 4.2 5.4 5.7 6.0 4.0 3.8P 0.001 0.001 0.001 0.001 NS NS
APm (mm Hg)N.T. 102 103 110 104 99 103 97S.N. 91 85 92 86 92 87 88S.N.* 100 102 102 101 104 96 91Y.A. 79 86 86 90 87 87 88A.S. 113 120 118 131 128 104 105H.S. 111 110 115 115 110 106 108K.S. 91 84 80 81 84 77 80K.S.* 73 76 81 81 77 76 77Y.S. 85 82 84 90 91 88 93M.T. 91 96 97 90 92 83 86E.O. 96 98 98 95 96 92 95T.S. 73 73 71 72 76 71 71T.S.* 75 71 73 71 73 71 72N.S. 77 86 85 82 83 85 82E.K. 82 83 82 84 89 84 83Y.O. 89 97 99 94 93 89 91Y.O. 118 119 108 108 110 106 114K.Y. 99 115 123 124 123 103 101H.Y. 109 117 125 131 125 117 117T.I. 111 115 116 117 118 113 111H.K. 72 75 78 78 78 78 77N.S. 98 101 105 105 108 106 106Y.H. 86 92 91 92 92 91 89T.O. 88 86 87 87 90 87 87T.M. 85 89 89 86 86 78 76Mean 91.8 94.4 95.8 95.8 96.2 91.1 91.4SE 2.7 3.0 3.2 3.4 3.2 2.6 2.6P 0.05 0.01 0.05 0.01 NS NS
PAPd (mm Hg)N.T. 12S.N. 19S.N.* 37
Y.A. 24A.S. 13H.S. 17K.S. 18K.S.* 13
Y.S. 20M.T. 11
12194023141417132112
12204424131215132012
12204124131115132111
12214724131015122112
1320352591014142010
12193626101213142011
A B
APd (mm Hg)80 8075 6880 8070 7288 8593 9276 6963 6175 6473 7669 7266 6666 5861 6461 6072 78109 10477 8989 9194 9352 6078 8468 6574 7566 7375.0 75.22.5 2.5
NS
PAPs (mm Hg)27 3045 4737 4061 6126 2829 2529 2822 2432 3225 2822 2630 3027 2826 2829 2930 2835 3425 3029 2529 2756 5233 3966 6838 3526 2833.4 34.02.3 2.3
NS
PAPm (mm Hg)17 1818 2824 2540 4017 1921 1822 2116 1724 2516 17
C D E F G
84 7674 6879 8075 7495 9391 8566 7067 6466 7881 7174 7164 6655 6364 6459 6676 8090 8994 97102 101100 9755 5887 8776 7475 7571 7176.8 76.72.7 2.4NS NS
787280739180686078727166666462751009410093608974757076.42.4NS
8070767377866661687265616567657988829798608274776574.22.1NS
76727275848370647771706365676481101839686638676795675.22.2NS
33 35 35 26 2653 53 54 45 4044 41 47 35 3661 63 63 59 5929 29 30 21 2027 27 28 22 2228 26 26 24 2324 26 28 25 2632 34 34 33 3330 32 32 25 2531 32 35 24 2230 30 28 28 2829 27 27 27 2728 28 26 22 2129 29 28 30 2930 31 31 27 2637 42 42 31 3036 37 35 24 2325 27 26 21 2228 27 28 23 2252 54 58 53 4941 47 49 38 4065 64 70 65 6036 36 37 35 3830 29 30 29 2935.5 36.2 37.1 31.7 31.02.2 2.3 2.5 2.4 2.20.05 0.01 0.01 0.05 0.01
19282541181719172418
19282440181619172518
19322740191619172519
17282240131417182415
17262140131516182415
528CIRCULATION
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

DOBUTAMINE AFTER OPEN HEART SURGERY/Sakamoto, Yamada
TABLE 2.A B
E.O.T.S.T.S.*N.S.E.K.Y.O.Y.O.K.Y.H.Y.T.I.H.K.N.S.Y.H.T.O.T.M.MeanSEp
12 1118 1815 1313 1315 1615 1523 2013 1413 1212 1226 2814 1536 3618 1817 1817.8 17.81.4 1.5
NS
C D
10 1017 1713 1712 1215 1515 1520 2017 1612 1212 1229 3017 1834 3218 1820 1917.8 17.81.6 1.5NS NS
E F G A B C D E F G
10 1016 1513 1411 1115 1615 1520 1615 1111 1212 1230 2819 1734 3120 2021 2018.0 16.71.7 1.4NS NS
10181411151519121114281735211917.31.5NS
15221817222326182020362146262023.01.5
16221818232324211919362347252123.31.5NS
17211817232326241919372644242323.51.5NS
17212017232427232019382743262223.61.5NS
18201816222426211820392946272424.01.6NS
15211815212221171818362642262321.91.50.05
14211814202222171817352643282221.71.60.05
LAPm (mm Hg)N.T. 12 12S.N. 18 18S.N.* 16 15Y.A. 18 19A.S. 16 16H.S. 17 14K.S. 18 17E.S.* 13 13Y.S. 24 24M.T. 11 12E.O. 12 11T.S. 18 18T.S.* 15 13N.S. 13 12E.K. 16 16Y.O. 16 15Y.O. 18 15K.Y. 13 15H.Y. 15 13T.I. 11 11H.K. 18 19N.S. 17 17Y.H. 21 19T.O. 16 13T.M. 16 16Mean 15.9 15.3SE 0.6 0.6p 0.0r
1218151915121513231210171310151517161310191919111614.90.7
121814191511151324111017178151617141310201917111514.80.7
12 1317 1814 1419 2014 1210 1015 1412 1424 2312 1010 1016 1513 1412 1116 1516 1616 1513 1313 1310 1020 2220 1918 1812 1615 1514.8 14.80.7 0.7
1217142013121314241110181411151615141312181919151615.00.7
5 0.05 0.05 0.05 0.05 0.05
CI (L/min/m2)2.50 2.86 3.19 3.40 3.673.17 3.72 4.03 4.27 4.062.28 2.54 3.11 3.18 3.791.79 2.07 2.24 2.33 2.523.74 3.82 3.54 3.89 3.712.78 3.22 3.57 4.27 4.132.26 2.61 2.67 2.95 3.111.83 2.02 1.95 2.10 2.292.10 2.10 2.06 2.37 2.132.56 2.75 2.85 2.97 3.192.99 3.94 4.46 5.17 5.442.23 2.32 2.33 2.59 2.552.18 2.43 2.63 2.77 2.803.84 4.76 5.21 5.30 5.381.85 1.96 2.01 2.30 2.071.94 2.10 2.16 2.22 2.392.66 3.15 3.10 3.37 3.393.73 4.09 4.66 5.16 5.822.15 2.79 2.50 2.64 3.333.25 3.29 4.60 4.90 5.303.09 3.19 3.24 3.34 4.022.01 2.43 2.66 2.93 2.981.89 2.45 2.92 2.76 3.042.86 3.42 3.93 4.10 4.171.85 1.99 2.13 2.23 2.192.54 2.88 3.11 3.34 3.500.13 0.15 0.19 0.20 0.22
0.001 0.001 0.001 0.001
HR (beats/mmn)N.T. 81S.N. 96S.N.* 70Y.A. 96A.S. 78H.S. 94K.S. 113K.S.* 106Y.S. 106M.T. 89E.O. 57T.S. 80T.S.* 88N.S. 76E.K. 105Y.O. 112Y.O. 95K.Y. 82H.Y. 64T.I. 85
9310471998695
1091031038969809186106113100926595
10810084
10086
10411010810296788097100871201109877102
121110851028912011210610210886839511211012412011080105
1301141021059712711510910213096901001388713012212086110
1051088610485107108105969172798999961091039964105
9410972102849610310198926579899096110102966087
SVI (ml/beat/M2)31 31 3033 36 4033 36 3719 21 2248 44 4130 34 3420 24 2417 20 1820 20 2029 31 3053 57 5728 29 2925 27 2750 55 5218 18 2317 19 1828 32 2845 45 4834 43 3238 35 45
3.05 2.853.66 3.202.55 2.422.20 2.043.21 3.063.32 2.852.30 1.911.96 1.802.26 1.942.40 2.573.99 3.582.22 2.092.35 2.183.80 3.602.07 2.142.00 1.892.64 2.593.65 2.822.38 1.994.60 3.763.76 2.682.22 2.212.74 2.242.49 2.422.08 1.892.80 2.510.15 0.120.01 NS
2839372344362620232860312947211828473347
2836372438332721212557282839241828493948
2934302138312119242655282638221826373744
3029342036301918202855262540221725293443
529
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 55, No 3, MARCH 1977
TABLE 2. (Continued)A B C D E F G A B C D E F G
H.K. 86 86 90 97 95 93 80 36 37 36 34 42 40 34N.S. 81 86 91 94 105 84 82 25 28 29 31 28 26 27Y.H. 95 96 90 94 98 88 92 20 26 32 29 31 31 24T.O. 75 94 109 120 130 85 81 38 36 36 34 32 29 30T.M. 80 80 82 82 85 80 77 23 25 26 27 26 26 25Mean 87.6 91.6 96.4 102.7 108.9 93.6 89.5 33.3 32.4 32.6 32.8 32.3 30.2 28.8SE 2.9 2.5 2.3 2.7 3.2 2.4 2.6 2.1 2.1 2.1 2.0 1.9 1.7 1.7P 0.01 0.001 0.001 0.001 0.01 NS 0.01 0.01 0.01 NS NS NS
LVSWI (gm-nm/beat/M2) SVR (unit)N.T. 38 38 40 35 33 36 35 24.8 21.8 20.9 18.5 16.3 20.5 20.6S.N. 33 33 40 36 37 32 28 19.8 15.8 15.8 13.9 15.6 16.4 19.0S.N.* 38 42 43 44 45 33 36 30.3 27.7 22.5 21.9 18.9 25.9 25.9Y.A. 16 19 20 22 22 19 18 26.2 24.8 22.9 23.0 20.5 23.6 25.7A.S. 63 62 58 69 59 47 45 22.9 23.8 25.3 25.5 26.1 24.5 26.0H.S. 38 44 48 51 45 41 39 25.8 22.0 20.8 17.4 17.2 20.6 24.4K.S. 20 22 21 23 25 18 17 30.5 24.4 22.7 20.8 20.4 25.3 31.7K.S.* 14 17 17 19 19 16 15 30.3 28.5 31.4 29.2 25.5 29.3 32.4Y.S. 17 16 17 21 19 21 19 28.5 27.5 28.8 26.7 30.1 27.4 33.7M.T. 32 35 35 30 27 26 29 20.3 20.0 19.5 17.3 16.5 19.8 19.2E.O. 61 67 68 69 67 61 64 23.1 17.9 15.8 13.2 12.7 16.6 19.1T.S. 21 22 21 23 23 21 19 17.8 17.1 16.6 15.1 16.2 17.4 18.4T.S.* 20 21 22 21 23 20 20 18.7 15.8 15.1 13.9 14.2 16.4 17.9N.S. 43 56 53 47 38 38 38 13.2 11.9 10.7 10.2 10.1 14.7 15.0E.K. 16 17 21 20 24 21 20 32.8 31.4 30.3 27.1 31.8 30.0 28.7Y.O. 17 21 21 19 19 18 17 28.6 28.9 28.7 26.5 24.3 27.8 30.1Y.O. 38 45 35 35 36 32 34 27.2 23.2 21.4 19.6 19.9 24.7 27.0K.Y. 53 61 70 70 73 45 35 15.6 16.5 15.5 14.2 12.4 16.6 21.1H.Y. 43 61 49 53 59 52 48 34.0 28.1 33.6 33.2 25.2 33.0 39.4T.I. 52 50 65 68 71 62 58 17.3 17.7 12.8 12.1 11.3 14.1 15.0H.K. 26 28 29 27 33 31 27 15.5 15.6 15.9 15.5 12.9 13.7 19.0N.S. 28 32 34 37 33 31 32 36.4 31.1 29.5 26.8 27.1 35.6 35.8Y.H. 18 26 32 30 31 31 23 29.8 24.5 20.4 21.8 19.8 21.7 25.9T.O. 37 36 37 35 34 28 30 21.1 17.2 15.2 14.6 14.8 24.0 24.6T.M. 22 25 26 26 25 22 20 27.3 26.6 24.9 22.9 23.4 22.3 23.9Mean 32.1 35.9 36.8 37.2 36.8 32.1 30.6 24.7 22.4 21.5 20.0 19.3 22.5 24.8SE 2.9 3.2 3.3 3.5 3.3 2.6 2.6 1.3 1.1 1.3 1.2 1.2 1.2 1.3P 0.001 0.001 0.001 0.001 NS NS 0.001 0.001 0.001 0.001 0.05 NS
Abbreviations: A = control; B = 2mcg/kg/min; C = 4mcg/kg/min; D = 6mcg/kg/min; E = 8mcg/kg/min; F = 5 min after dobutamine; G = 10min after dobutamine; APd = diastolic aortic pressure; APm = mean aortic pressure; APs = systolic aortic pressure; CI = cardiac index; HR = heartrate; MLAP = mean left atrial pressure; PAPd = diastolic pulmonary arterial pressure; PAPm = mean pulmonary arterial pressure; PAPs = systolic pul-monary arterial pressure; SVI = stroke volume index; SVR = systemic vascular resistance; SWI = stroke work index.sIB = standard error of mean.P values derived from paired t-test comparing A vs B, C, D, E, F, G.*indicates the second test of dobutamine infusion.
the former (0.57 L/min/m2) than the latter (0.41L/min/m2), but this difference was not significantstatistically. Moreover, comparison in stroke volume indexwas not significantly different in these dosage of both drugs.But the increase in heart rate was considerably greater withisoproterenol than that with dobutamine. It appears that in-otropically, 2 and 8 ,sg/kg/min of dobutamine were com-parable to 0.005 and 0.01 Ag/kg/min of isoproterenol,respectively (fig. 3).A representative case (Y.O.) is presented below (fig. 4).
Aortic valve replacement by the Starr-Edwards ball pros-thesis was performed for aortic insufficiency. Immediatelypostop, the patient was in a stable condition and aorticpressure was 123/71 (90) mm Hg; pulmonary arterial pres-sure, 31/16 (23) mm Hg; mean left atrial pressure, 15.5 mmHg, and cardiac index 1.92 L/min/m2. Fourteen hours aftersurgery, aortic pressure fell to 90/65 (74) mm Hg, cardiacindex decreased to 1.06 L/min/m2, and pulmonary arterialpressure and mean left atrial pressure increased. A diagnosis
of severe left ventricular failure was made and the infusionof dobutamine at a rate of 6 Ag/kg/min was started. Afteraortic pressure had been elevated to a safe level, the infusionof phenoxybenzamine at a dose of I mg/kg was added forthe purpose of reducing the afterload of the left ventricle.Subsequently cardiac index increased to over 2.0 L/min/m2and systolic aortic pressure stabilized at 120 mm Hg. The in-fusion of dobutamine was stopped at 8 hours after initi-ation, but there was no change in hemodynamics and thepatient remained in a satisfactory condition. Sufficienturinary output was also maintained.
Discussion
With the administration of isoproterenol, tachycardia orarrhythmia often develops and necessitates the cessation ofinfusion before a sufficient increase in cardiac output canbe obtained. Myocardial oxygen consumption (MVO2) in-creases markedly as both myocardial contractile force and
530 CIRCULATION
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

DOBUTAMINE AFTER OPEN HEART SURGERY/Sakamoto, Yamada
heart rate increase with isoproterenol, thus shifting themyocardial metabolism to anaerobic."5
In an attempt to develop a new beta-adrenergic stimulatorwithout these adverse effects on cardiac rhythm or myocar-dial metabolism, dobutamine has been synthesized bymodifying the side-chain of dopamine.6 It has been reportedthat dobutamine increases myocardial contractile forceselectively.8 12 In the present study, dobutamine increasedsystolic and mean aortic pressure and systolic pulmonaryarterial pressure significantly but diastolic aortic pressureand diastolic pulmonary arterial pressure remained un-altered. These changes demonstrate that dobutamine pro-duced relatively little change in peripheral vascular resis-tance at doses less than 8 ,Ag/kg/min. Dobutamine has beenshown to possess both vasoconstricting and vasodilatingeffects on peripheral vessels."6' 17 At low doses, a mildperipheral alpha-adrenergic action predominates, while withhigher doses, beta-adrenergic effect is predominant.Holloway et al. observed this biphasic response clinicallywith dobutamine, with 10 gg/kg/min being the cut-offpoint,'3 and Robie et al. reported that as the dose ofdobutamine was increased to higher than 16 gg/kg/minperipheral vasodilation became predominant and aorticpressure and total peripheral resistance began to lower.",
Since dobutamine does not lower aortic pressure, it is ex-pected that the inflow pressure of the coronary arteries is notlowered, thus acting favorably on coronary perfusion. Thisadvantage makes an interesting contrast to isoproterenolwhich reduces diastolic aortic pressure because of its potentvasodilating action on peripheral vessels.'8 Tuttle et al.reported that in experimental dogs P02 in coronary sinus in-creased by 35% after infusion of dobutamine, but decreasedby 11% after isoproterenol.7 They considered that dobuta-mine increased myocardial oxygen supply more signifi-cantly than myocardial oxygen consumption. The fact ob-tained from our study that the diastolic aortic pressure wasunchanged during dobutamine infusion may also have beenresponsible for the finding by Tuttle et al.7 Vatner et al."'reported that in the presence of experimental moderateglobal ischemia, dobutamine is not as deleterious as isopro-terenol. In their experiment, left ventricular function wasmaintained during dobutamine infusion but acute depressionof cardiac function occurred when isoproterenol was sub-stituted for dobutamine.
In the present study, mean left atrial pressure showed asignificant, gradual decrease after the start of dobutamineinfusion because of the improvement of left ventricular func-tion. These changes in pressure were very similar to thosereported by Jewitt et al." As far as clinical investigations areconcerned, cardiac index was found to be increased withdobutamine by 82% (Akhtar et al.8), 82% (Beregovich etal.9" 10), and 43% (Jewitt et al."). Loeb et al."2 reported on 36patients of whom 17 patients had impaired left ventricularperformance. Dobutamine augmented cardiac index by 48%(7.5 ,g/kg/min) in patients with normal left ventricularfunction and 82% (10.7 Ag/kg/min) in patients withdepressed left ventricular function. Discrepancies of thedegree of increase in cardiac index is thought to be related tothe differences in myocardial contractility reserve before theadministration of dobutamine. This is supported by the fact
ZQ'
S-(
0
000.
0
.0
0
rS
0,-"
V
0
0
c-i
eDC so
in 0000,- ooo
c es0-H H -H e 1 -H -H -H u1 N
f
NMO 00_d 4 CS 00CN 0 00 0CD41
10 0r-c 0 0 00 )0011
o ctsino D0 oC o O oit4
00 0 6 c-~ 00 4 00 in 1
- -
fl fl i CZI I 0i 00It 0i ini00 c01011 NcmC o in 01
00 1 0tl _ O 0 0C 0001t m o
00 c 0 in inc0 0 i -O--
. .. * * *. . . .6 .C
0 0 t- CSn(o o _
if 00 fl fl N i i 000 00fl
CYD Cq CO Cli N
OC) coeC) LoCcqXOC)
0041-i 00000
L6 X6 L dq, CN CQ O c-iCqCS
000 in 00 i 00 i N 00icli cl
C) O <U-. OC5 o MCS20 oqcs ; 16 e C~ c6 _ oo cys Lo ca
--Hl-H-H-H-H-HH-H~00
O1 001000 in 00 N) O O N
00
06 i L6 4 ci cli C-o ' X<
it- CD r4 ci cz i i00
CS00NC C- 1000000 C00
r--l
CS oq Ci ol- o0<X
t-(D 000 qmC l
- N-- N0001i 0m 0
00 o o tN co - 000 0o
6 C6Cs tz_;(Xb crz X6 C; 1 cooo t < CYD C~OO- oo CS ce C
017:
000i Nfl '-0 01i - -ini
0 oo 00 N 0 > _ C' in0 -
0001000
A44X
531
co
0
.0
44
0
co44
.0
co
0
00
CD
01
9
as-d
00
6
010
- %..-aCIS 0C
A
0.
E-40
n0
0O0001:-Of.0 0
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 55, No 3, MARCH 1977
Y.O.(F.35yrs) AI-'AVRCedilanidO.4mg O4 0.2
Dobutamime6rKg/mignin
FIGURE 4. This patient sufferedfrom severe leftventricular failure following aortic valve replace-ment. With 6 ,ug/kg/min ofdobutamine infusion,aortic pressure and cardiac index increased andthe patient's hemodynamics remained satisfactoryafter the cessation of dobutamine infusion. Ab-breviations: HR = heart rate; AP = aortic pres-sure; PAP = pulmonary arterial pressure;LAMP = left atrial mean pressure; CI = cardiacindex; and UV = urinary output.
I I II
6pm Oam 6am Opm 6pm OamFeb.s. Feb.5.
that the dose-response curves of cardiac index duringdobutamine infusion are more steep in congenital heart dis-eases than in acquired heart diseases. Heart rate is reportedto increase with dobutamine by 28% (Gunnar et al.'4), 7.3%(Akhtar et al.8), 31% (Beregovich et al.9 10), and 8.5% (Jewittet al."1). The increase by 24% in the present study is ratherlarge as compared with the results by other investigators.
Premature ventricular beats were observed in one patientduring dobutamine infusion. This patient, who developedarrhythmia (premature ventricular beat) with dobutamine,developed it during isoproterenol administration as well.Some patients who developed arrhythmia with isoproterenoldid not develop any with dobutamine. Thus, the occurrenceof premature ventricular contraction is definitely less fre-quent with dobutamine than with isoproterenol. This is themost useful feature of dobutamine in the postoperativemanagement of patients after open heart surgery. When thehemodynamic responses with dobutamine and isoproterenolwere compared in the same nine patients, no significantdifferences were observed, but dobutamine had less effecton heart rate. For comparable effect on cardiac index, 8 ,ug/kg/min of dobutamine was equivalent to 0.01 ,ug/kg/min of isoproterenol. A dose of dobutamine of 4-10 gg/kg/min was sufficient to improve cardiac performance withoutany undesirable side effects. Beregovich et al.'0 also foundthat 5-10 Ag/kg/min was preferable for clinical use. Sincethe increase in cardiac index was lower in acquired heart dis-ease than in congenital disease, further increase in the dosein acquired heart diseases seemed feasible.We observed a marked increase in urinary output in one
patient. The mechanism of this phenomenon is unknownbecause the hemodynamic response of this patient did notdiffer from others. But previous investigators reported thatthe renal vascular bed showed the least response todobutamine infusion.'7 20
In conclusion, dobutamine, a new beta-stimulator, showsconsiderable promise therapeutically. This agent is usefulfor the treatment of patients following open heart surgery.Undesirable side effects such as tachycardia, arrhythmias,hypotension, and peripheral vasoconstriction do not occur.Moreover, with dobutamine a comparable effect on cardiacindex could be attained with less change in heart rate thanthat caused by isoproterenol, and 8 ,ug/kg/min of dobuta-mine had an inotropic effect comparable to that of 0.01,ug/kg/min of isoproterenol.
AcknowledgmentThe authors wish to thank Dr. T. Murakami, Dr. R. Hatano, Dr. T.
Tsukuura, Dr. M. Sunamori, and Mr. S. Heima for their invaluableassistance.
References1. Dodge HT, Lord JD, Sandier H: Cardiovascular effects of isoproterenol
in normal subjects and subjects with congestive heart failure. Am Heart J60: 94, 1960
2. Elliot WC, Gorlin R: Isoproterenol in treatment of heart disease.Hemodynamic effects on circulatory failure. JAMA 197: 315, 1966
3. Beregovich J, Reicher-Reiss H, Kunstadt D, Grisman A: Hemodynamiceffects of isoproterenol in cardiac surgery. J Thorac Cardiovasc Surg 62:957, 1971
4. Sarnoff J, Wexler BC: Isoproterenol-induced myocardial infarction inrats. Circ Res 27: 1101, 1970
5. Gunnar RM, Loeb HS, Pietras RJ, Tobin JR: Ineffectiveness of
532 CIRCULATION
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

PRAZOSIN HCI AND HYPERTENSION/Koshy et al.
isoproterenol in shock due to acute myocardial infarction. JAMA 202:1124, 1967
6. Tuttle RR, Millis J: Dobutamine, development of a new catecholamine toselectively increase cardiac contractility. Circ Res 36: 185, 1975
7. Tuttle RR, Pollock GD, Todd G, Tust R: Dobutamine: Containment ofmyocardial infarction size by a new inotropic agent. Circulation 48 (supplIV): IV-132, 1973
8. Akhtar N, Mikulic E, Cohn J, Chaudry MH: Hemodynamic effect ofdobutamine in patients with severe heart failure. Am J Cardiol 36: 202,1975
9. Beregovich J, Bianchi C, D'Angelo R, Rubler S: Hemodynamic studieswith dobutamine, a new inotropic agent. Circulation 48 (suppl IV): IV-144, 1973
10. Beregovich J, Bianchi C, D'Angelo R, Diaz R, Rubler S: Hemodynamiceffects of a new inotropic agent (dobutamine) in chronic cardiac failure.Br Heart J 37: 629, 1975
11. Jewitt D, Birkhead J, Mitchell A, Dollery C: Clinical cardiovascularpharmacology of dobutamine. A selective inotropic catecholamine.Lancet 2: 363, 1974
12. Loeb HS, Kahn M, Klodnycky ML, Sinno MZ, Towne WD, GunnarRM: Hemodynamic effects of dobutamine in man. Circ Shock 2: 29,1975
13. Holloway GA, Frederikson EL: Dobutamine, a new beta agonist. AnesthAnalg 53: 616, 1974
14. Gunnar RM, Loeb HS, Klodnycky M, Sinno MZ, Towne W:Hemodynamic effects of dobutamine in man. Circulation 48 (suppl IV):IV-132, 1973
15. Mueller H, Giannelli S, Ayres SM, Conklin EF, Gregory JJ: Effect ofisoproterenol on ventricular work and myocardial metabolism in thepost-operative heart. Circulation 37 (suppl II): 11-146, 1968
16. Robie NW, Nutter DO, Moody C, McNay JL: In vivo analysis ofadrenergic receptor activity of dobutamine. Circ Res 34: 663, 1974
17. Vatner SF, McRitchie RJ, Braunwald E: Effects of dobutamine on leftventricular performance, coronary dynamics, and distribution of cardiacoutput in conscious dogs. J Clin Invest 53: 1265, 1974
18. Hinds JE, Hawthorne EW: Comparative cardiac dynamic effects ofdobutamine and isoproterenol in conscious instrumented dogs. Am JCardiol 36: 894, 1975
19. Vatner SF, McRitchie RJ, Maroko PR, Patrick TA, Braunwald E:Effects of catecholamine, exercise, and nitroglycerin on the normal andischemic myocardium in conscious dogs. J Clin Invest 54: 563, 1974
20. Robie NW, Goldberg LI: Comparative systemic and regionalhemodynamic effects of dopamine and dobutamine. Am Heart J 90: 340,1975
Physiologic Evaluationof a New Antihypertensive Agent:
Prazosin HClM. C. KOSHY, M.D., DIANE MICKLEY, M.D.,
JACQUES BOURGOIGNIE, M.D., AND M. DONALD BLAUFOX, M.D.
SUMMARY The mechanism of action of prazosin hydrochloride,a new antihypertensive agent was studied in 14 patients with essentialhypertension. Mean supine blood pressure for the group fell from148/102 ± 3/2 (SE) mm Hg at baseline to 139/91 ± 5/4 after eightweeks of therapy (P < 0.05). No significant postural hypotension wasnoted in the patients who responded to therapy. Glomerular filtrationrate (endogenous creatinine or inulin clearance) and effective renalplasma flow (PAH clearance) remained unchanged during therapy asdid supine and stimulated peripheral plasma renin activity. Cardiacoutput did not change significantly although plasma volume increasedin ten out of 12 patients in whom it was measured (P < 0.025).
PRAZOSIN HYDROCHLORIDE* is a new type of anti-hypertensive agent (fig. 1) which effectively lowers the bloodpressure in hypertensive subjects. It is relatively free ofserious side effects.14 Although it has been studied exten-sively in animal modelsg' 10 there are few physiologic studiesreported in humans. The mechanism of action of prazosin isnot fully understood. It does not appear to be relatedchemically or pharmacologically to any of the antihyper-tensive agents in general clinical use. Animal data suggest
*Prazosin hydrochloride - Minipress, C. P. 122991 (Pfizer).
From the Albert Einstein College of Medicine of Yeshiva University,Bronx, New York.
Supported in part by NIH grant 11984 and USPHS Training Grant STOIHL05928, The New York State Kidney Disease Institute, and a researchgrant from Pfizer, Inc., New York, New York. Dr. Bourgoignie was recipientof USPHS Career Development Award NO K04 HL40977.
Address for reprints: M. Donald Blaufox, M.D., Ph.D., Albert EinsteinCollege of Medicine, 1300 Morris Park Avenue, Bronx, New York 10461.
Received July 27, 1976; revision accepted October 21, 1976.
Among the patients whose mean blood pressure fell 10 mm Hg ormore, peripheral vascular resistance fell significantly (P < 0.025),and the change in plasma volume was not statistically significant.Among the patients whose mean blood pressure changed less than 10mm Hg with therapy, there was no significant change in peripheralvascular resistance and plasma volume increased significantly(P < 0.025).
Prazosin hydrochloride appears to be an effective antihypertensiveagent which acts by peripheral vasodilatation. It may cause fluidretention. The drug does not appear to affect renal function or reninsecretion.
that its antihypertensive action is associated with peripheralvasodilation. The present study was designed to evaluatesome physiologic parameters of importance in the therapyof moderate essential hypertension with prazosin HCI.
Methods
Fourteen patients with essential hypertension were studiedon an outpatient basis. Criteria for participation in the studyincluded sustained diastolic blood pressure between 90 and130 mm Hg in patients who had received no antihyper-tensive therapy in the last four weeks. Diabetes, coronaryheart disease, cerebrovascular disease or renal insufficiencywere criteria for exclusion from the study. Renal and reno-vascular causes of hypertension were ruled out with tripleisotope renal studies using 197Hg chlormerodrin, "mTc per-technetate and "'1I orthoiodohippuratell and by rapid se-quence intravenous urography. Pheochromocytoma wasexcluded with urinary VMA. All patients were offered par-
533
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

T Sakamoto and T YamadaHemodynamic effects of dobutamine in patients following open heart surgery.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1977 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.55.3.525
1977;55:525-533Circulation.
http://circ.ahajournals.org/content/55/3/525the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from