
Effects of a Preventive Cardiology Curriculum on...
13
PatientEducationand Counseling, 21 (1993) 15-27 15 Elsevier Scientific Publishers Ireland Ltd. Effects of a Preventive Cardiology Curriculum on Behavioral Cardiovascular Risk Factors and Knowledge of Medical Students Iraj A. Kashani, MD, Robert M. Kaplan, PhD, Joan W. Rupp, MS, RD, Robert D. Langer, MD, MPH, Theresa J. McCann, MPH, James F. Sallis, PhD, Mark Bracker, MD, Philip Nader, MD, Joel Dimsdale, MD, Deirdre Browner, MPH, Cheryl A. Holiday, BA, and Michael H, Criqui, MD, MPH University of California, San Diego School of Medicine, Departments of Pediatrics, Community and Family Medicine. Medicine and Psychiatry, La Jolla, California 92093 (USA) (Received June 7th, 1992) (Accepted August 17th, 1992) Abstract significant for women in comparison to the control class women. Additional analyses showed no sys- We evaluated a Preventive Cardiology Aca- tematic secular trends in dietary or other variables demic Award (PCAA) program designed to in- in classes entering from 1986 to 1990. We conclude tegrate preventive cardiology concepts into the that the PCAA curriculum changes have favorably medical school curriculum. Diet, preventive car- affected the preventive cardiology knowledge, atti- diology knowledge, preventive cardiology atti- tudes and diet of medical students. tudes, exercise behavior, and body mass index were compared at entrance to medical school and Key words: Preventive cardiology; Car- during the graduation year. Complete data were diovascular risk factors; Medical students; available on 94 students (65 men and 29 women). Medical education. Similar data from students who graduated in 1987, prior to the introduction of the PCAA curriculum, Introduction served as a control. Women showed a significant enhancement in attitude towards cardiovascular Some information on the prevention of disease (CVD) prevention, while both men and heart disease is now included in most medical women significantly increased their knowledge school curricula. However, many physicians about CVD prevention. The frequency of planned still lack the skills and confidence necessary to physical activity decreased significantly in both provide preventive cardiology services. Pre- sexes and men showed a significant increase in vious studies have shown that medical body mass index. Men significantly reduced total students are not knowledgeable about dietary calories, percent of calories from fat and saturated intervention [1-3]. More favorable attitudes fat and dietary cholesterol and increased fiber in- towards prevention appeared to be related to take. In women, the only significant reduction was healthier personal eating habits among in total calories. In comparison to the control class medical students [1]. These attitudes may af- ' that did not have the program, men receiving the fect not only the students but the patients they PCAA curriculum reduced dietary cholesterol, will advise when they practice. The Preventive dietary fat, saturated fat and monounsaturated fat. Cardiology Academic Award (PCAA) at the Changes in these dietary parameters were non- University of California, San Diego (UCSD) 0738-3991/93/$06.00@ 1993ElsevierScientificPublishersIrelandLtd.
Transcript of Effects of a Preventive Cardiology Curriculum on...

PatientEducationand Counseling,21 (1993)15-27 15Elsevier Scientific Publishers Ireland Ltd.
Effects of a Preventive Cardiology Curriculum on BehavioralCardiovascular Risk Factors and Knowledge of Medical Students
Iraj A. Kashani, MD, Robert M. Kaplan, PhD, Joan W. Rupp, MS, RD, Robert D.
Langer, MD, MPH, Theresa J. McCann, MPH, James F. Sallis, PhD, Mark Bracker,
MD, Philip Nader, MD, Joel Dimsdale, MD, Deirdre Browner, MPH, Cheryl A.
Holiday, BA, and Michael H, Criqui, MD, MPH
University of California, San Diego School of Medicine, Departments of Pediatrics, Community and Family Medicine. Medicine andPsychiatry, La Jolla, California 92093 (USA)
(Received June 7th, 1992)(Accepted August 17th, 1992)
Abstract significant for women in comparison to the controlclass women. Additional analyses showed no sys-
We evaluated a Preventive Cardiology Aca- tematic secular trends in dietary or other variablesdemic Award (PCAA) program designed to in- in classes entering from 1986 to 1990. We concludetegrate preventive cardiology concepts into the that the PCAA curriculum changes have favorablymedical school curriculum. Diet, preventive car- affected the preventive cardiology knowledge, atti-diology knowledge, preventive cardiology atti- tudes and diet of medical students.tudes, exercise behavior, and body mass indexwere compared at entrance to medical school and Key words: Preventive cardiology; Car-during the graduation year. Complete data were diovascular risk factors; Medical students;available on 94 students (65 men and 29 women). Medical education.Similar data from students who graduated in 1987,prior to the introduction of the PCAA curriculum, Introductionserved as a control. Women showed a significantenhancement in attitude towards cardiovascular Some information on the prevention of
disease (CVD) prevention, while both men and heart disease is now included in most medicalwomen significantly increased their knowledge school curricula. However, many physiciansabout CVD prevention. The frequency of planned still lack the skills and confidence necessary tophysical activity decreased significantly in both provide preventive cardiology services. Pre-sexes and men showed a significant increase in vious studies have shown that medicalbody mass index. Men significantly reduced total students are not knowledgeable about dietarycalories, percent of calories from fat and saturated intervention [1-3]. More favorable attitudesfat and dietary cholesterol and increased fiber in- towards prevention appeared to be related totake. In women, the only significant reduction was healthier personal eating habits amongin total calories. In comparison to the control class medical students [1]. These attitudes may af-
' that did not have the program, men receiving the fect not only the students but the patients theyPCAA curriculum reduced dietary cholesterol, will advise when they practice. The Preventive
dietary fat, saturated fat and monounsaturated fat. Cardiology Academic Award (PCAA) at theChanges in these dietary parameters were non- University of California, San Diego (UCSD)
0738-3991/93/$06.00@ 1993ElsevierScientificPublishersIreland Ltd.

'2

17
questions on cardiovascular risk factors, student received his/her individual risk factorKnowledge items were sampled from a pool profile, class means and handouts on theof items that had been analyzed and evaluated significance of CVD risk factors, includingfor content validity. The attitude and diet. During the sessions PCAA facultyknowledge scales were developed as part of reviewed the significance of CVD risk factorscooperative efforts in the PCAA program; (e) and described the prudent diet recommendeda physical activity assessment, based on the by the American Heart Association and othertype and frequency of the student's physical behaviors to limit CVD risk. In addition,activity; (f) an optically scanned semi- psychological test scores were reviewed andquantitative food frequency questionnaire, discussed in terms of the complex literaturedeveloped by Willett and colleagues, used to pertaining to CVD risk and Type A behavior,assess usual diet [8-11]; and (g) pulmonary anger, and depression. Packets for studentshistory questionnaire, added during the third not in attendance were placed in theiryear of the program when a Preventive mailboxes.Pulmonary Academic Award became active.
3. High risk session: This session was
In addition to the questionnaires, the asses- scheduled to accommodate students withsment included blood pressure, blood elevated lipids or blood pressure, defined aspressure reactivity, five-minute exercise step- LDL cholesterol _>150 mg/dl, triglyceridetest, lipids and lipoproteins, height, weight _>200 mg/dl, systolic blood pressure _>140and, during years three through five, a tuber- mmHg, or diastolic blood pressure _ 90culin skin test and pulmonary function tests, mmHg. Cardiovascular risk factors including
lipids and blood pressure were reviewed andThe examinations were performed by senior discussed in detail. The dietitian reviewed
medical students, physical education and practical dietary guidelines and othernutrition students and preventive medicine members of the faculty also contributed.residents. Spirometry was performed by Where necessary, clinical referrals were ar-trained pulmonary function technicians. The ranged.
supervising group consisted of eight faculty 4. Data from the risk factor assessmentphysicians, a dietitian and two psychologists.
were also used in a core epidemiology lectureEach year the entire group of students com-
to illustrate certain principles of epidemi-pleted the risk factor assessment in less than ologic research.four hours.
Student feedback. Data from the risk factor Graduating students comparison groupsassessment were used in the following four To evaluate the program, a limited self-ways: report cardiovascularrisk factor assessment
was carried out during the last year of medical1. During the risk factor assessment, any school. All graduating students in 1990 and
student with an abnormal resting pulse rate; 1991 were mailed the same risk factor and dieti.e. < 60 per min or _ 120 per min, or a resting questionnaires they completed the first year.systolic blood pressure of >__140 mmHg, or a In view of the logistic difficulties of gatheringdiastolic blood pressure of >_90 mmHg, was all the graduating students at one time, theapproached by a qualified faculty member blood sample, exercise step test and bloodand after a thorough investigation, was advis- pressure reactivity tests were not carried out.ed or referred as appropriate. Data from students who completed the asses-
sment at entry and graduation from medical2. General feedback sessions: Two one- school were compared to assess within subject
hour sessions were held one day apart. Each changes.

_,_ .,,...a2___ r ._=_,.,._ _ . i.a ,,._._ ._., e-_._ "..a,
_ 0 _ _ ''. c_,.._ _ _ , _ _ _ i_ _ _ _
0 _ _ ¢1._.._",. 0 C:l,_'_ _--.,_ _ 0 _ ,_'_ ¢_"_"_.0 .._o _ _ _ _ _-,,-, _ _ _ ,'-_._ _ _ _ ,.., _ " _. _- _.
o _ -_ o Ca. _ _ _ _'_.-_ _'_ ,-._ C__ _,_'_ O_'c:_ '-_ _C_ _ _-__--] O- O. c_ o_ _ _. .__ _ oo _ 0"c_ =_'_'_ -_ c_'_ c_ o _ O_ c_ 0"_'__ _ _ _" _c__._._" ...._ o _O_ _ _ _ _ _,.__ c_ _" _ C:__-.-__ c_0"_ _" c_ _ 0 _ c_c__n,_
"_ __ _o,_. E _ _ _ _. ___'_ _E -= -_ _ _ _ _-_._ = o o ,-, o _ _
"-'"_ "" o _-_ _::4° ''" _ _"'-'_ "_"_ _"_ _ _ -'="_"_' _ _ _ _ _'_-_ r__ ,--___ l=sro .--,.,__
0 0 c_ _ _ _. _.,0 _.
,.% _'._ _ _ ,_,-t _ _:::i,ca _.,,_-,¢:I,_ i_l . ,-.-,_ ,-* _, _ 0 0.., , _ _::s"O'c_'T'"
_.. _ c_ ',,_ _ _.._ __.]_" _ _ _ ,_., ...... _ .., _,,C_..oo _._._ _ ._ ,_,.'.,_ r_ _ _ o _ c_ _.
_-_ C:l. _-, _ ,-._._ m I=1 _'C: _ m__._=_ _ ',o c_
I::I I_ _'I:t _ _-_ _ _'_ _ 1_ 0._ 0 _ , _ _ _ . _ ,
0 0 _ ?'_ _,._ _ _ _ _;_ _ r-z,_ c_ _ _ _ _o_ _/ _ "
0"_ _i,, 0 ee ._. _ _, _'_b._ I_ _ t,,a,.._oo _ _=, o
19
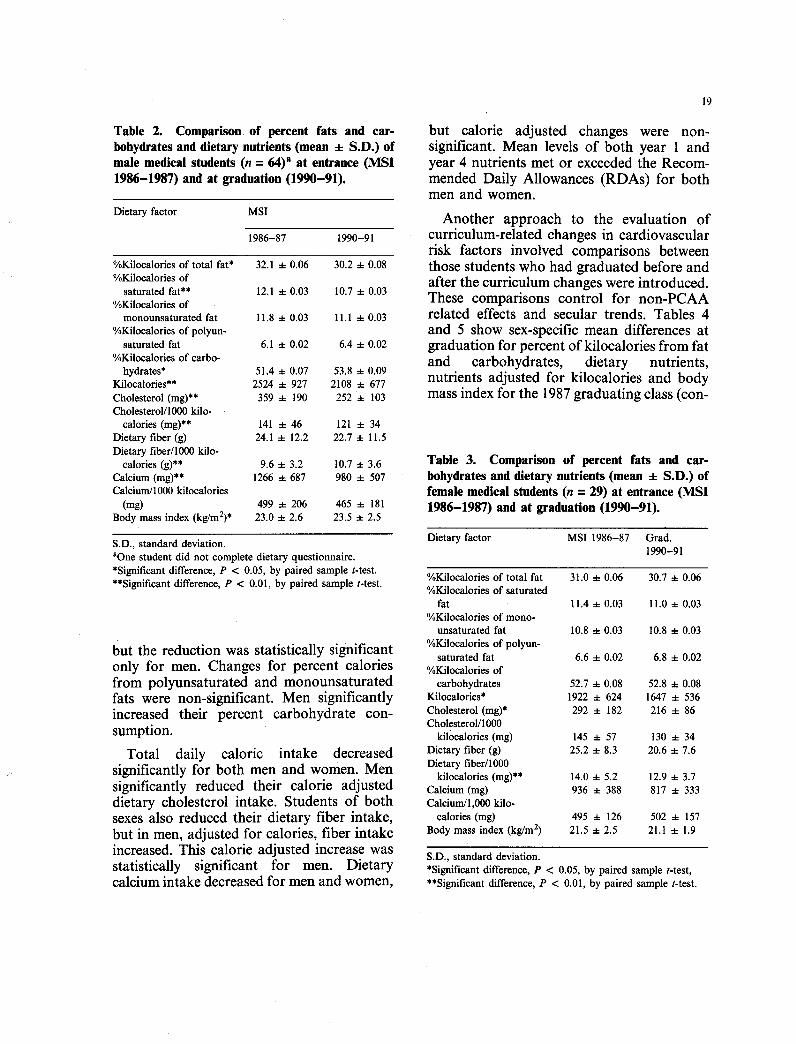
Table 2. Comparison of percent fats and car- but calorie adjusted changes were non-bobydratesanddietary nutrients (mean 4- S.D.) of significant. Mean levels of both year 1 andmale medical students (n = 64)a at entrance (MSI year 4 nutrients met or exceeded the Recom-1986-1987) and at graduation(1990-91). mended Daily Allowances (RDAs) for both
men and women.
Dietaryfactor MSI Another approach to the evaluation of1986-87 1990-91 curriculum-related changes in cardiovascular
risk factors involved comparisons between%Kilocaloriesof totalfat* 32.1-*-0.06 30.2_-0.08 those students who had graduated before and%Kilocalories of after the curriculum changes were introduced.
saturatedfat** 12.1q-0.03 10.7_-0.03 These comparisons control for non-PCAm%Kilocalories ofmonounsaturated fat 11.8 a-0.03 11.1_-0.03 related effects and secular trends. Tables 4
%Kilocaloriesof polyun- and 5 show sex-specific mean differences atsaturated fat 6.1q- 0.02 6.4_-0.02 graduation for percent of kilocalories from fat
%Kiiocaloriesofcarbo- and carbohydrates, dietary nutrients,hydrates* 51.4_-0.07 53.8+ 0.09 nutrients adjusted for kilocalories and bodyKilocalories** 2524 ± 927 2108 a- 677
Cholesterol (mg)** 359 ± 190 252 4- 103 mass index for the 1987 graduating class (con-Cholesterol/1000 kilo-
calories(mg)** 141± 46 121q- 34Dietaryfiber (g) 24.1± 12.2 22.7 ± I1.5Dietary fiber/1000 kilo-
calories (g)** 9.6 ± 3.2 10.7 ± 3.6 Table 3. Comparison of percent fats and car-Calcium (mg)** 1266 ± 687 980 ± 507 bohydrates and dietary nutrients (mean ± S.D.) ofCalcium/lO00 kilocalories female medical students (n = 29) at entrance (MSI
(mg) 499 ± 206 465 ± 181 1986-1987) and at graduation (1990-91).Body mass index (kg/m2)* 23.0 ± 2.6 23.5 ± 2.5
S.D.,standarddeviation. Dietaryfactor MSI1986-87 Grad.nOnestudentdidnotcompletedietaryquestionnaire. 1990-91• Significant difference, P < 0.05, by paired sample t-test. %Kilocalories of total fat 31.0 ± 0.06 30.7 ± 0.06• *Significant difference, P < 0.01, by paired sample t-test. %Kilocalories of saturated
fat 11.4± 0.03 11.0± 0.03%Kilocalories of mono-
unsaturated fat 10.8 ± 0.03 10.8 a- 0.03
but the reduction was statistically significant %Kilocalories of polyun-saturatedfat 6.6± 0.02 6.8± 0.02only for men. Changes for percent calories %Kilocalories of
from polyunsaturated and monounsaturated carbohydrates 52.7 ± 0.08 52.8 q- 0.08fats were non-significant. Men significantly Kilocalories* 1922 ± 624 1647 ± 536
increased their percent carbohydrate con- Cholesterol(mg)* 292 ± 182 216 ± 86
sumption. Cholesterol/1000kil0calories(mg) 145± 57 130± 34
Total daily caloric intake decreased Dietary fiber (g) 25.2 ± 8.3 20.6 ± 7.6
significantly for both men and women. Men Dietary fiber/1000kilocalories(mg)** 14.0± 5.2 12.9± 3.7significantly reduced their calorie adjusted Calcium (mg) 936 ± 388 817 ± 333dietary cholesterol intake. Students of both Calcium/l,000 kilo-sexes also reduced their dietary fiber intake, calories (mg) 495 ± 126 502 ± 157
but in men, adjusted for calories, fiber intake Body mass index (kg/m2) 21.5 q- 2.5 21.1 ± 1.9increased. This calorie adjusted increase was S.D., standard deviation.statistically significant for men. Dietary *Significant difference, P < 0.05, by paired sample t-test,calcium intake decreased for men and women, **Significant difference, P < 0.01, by paired sample t-test.

=r,'= ...... , p.: / _ _ - _1 '_1 _- @_ Br.ll-0 _ (:l'Cl _ I_ _ _ _ _" -- _ _ _-_,-_ _"0"
_a_ O _ . :_ ,_._.,e_I:::1_ _--":__-_ _ _ _ _,_m::_ _^ / • It-H- _-r_ - _ _1 _'1 _ I_.._ ,_,
{ira o_ ,._ _ _ =1 •m:3 e-,. ,.... o M::,
.. o, -_, ,_ ,.,_-_,,-]-,, _,,,_ _ , _ _ ....
-1. .I. [/_
-- _:_ I "-'/ l I .. -_ L _ 1_ o_ _._. ,-_ _ _ ,._ _ _- _ _
H- II- I _ r| _I !_., ._,:. _ A. , _ _ .-- , •
_ * _ _0 t_/ _ ,-_ I,a _ _:_ - "_] --a | I'_ ,l_ _ ,. ell
l I _=.__ o ,I_ -- oo- ° ,, :1 =I _'-_.-.=_-._._._ ._ -_ _ _ _ _ _1 .. _-_- _-_-_ _- _ "- _1 _/ E_• _ _'"

21
take for men or women between the two tudes significantly. Preventive cardiologygroups of graduating classes, knowledge increased in both men and women.
Body mass index Table 7 shows sex-specific comparisons ofmean scores on preventive cardiologyThere was a significant increase in mean knowledge and preventive cardiology atti-
body mass index from year 1 to year 4 of tudes for the control 1987 graduating classmedical school for men (Table 2) but not for and the subsample of medical students whowomen (Table 3). In men, body mass index were graduated in 1990-91. No significantdecreased in 23.4% of the students, did not differences were observed in average preven-change more than 1% in 26.6% and increased tive cardiology knowledge or preventive car-in 50.0%. In women, body mass index diology attitudes in the two graduating classesdecreased for 27.6%. Body mass index was not and there were no significant-differences insignificantly different between the two groups the frequency of physical activity for eitherof graduating classes for men and women, sex.
Physical activity, attitudes and knowledge An alternative explanation for the changesTable 6 presents sex-specific mean change observed during the program years is that
in the frequency of physical activity, preven- secular trends rather than the curriculum ac-tive cardiology knowledge and preventive car- count for the differences. In an attempt todiology attitudes. Physical activity decreased discern whether the observed Changes mightin both men and women. Male students reflect secular trends, comparisons were made
preventive cardiology attitudes were not between each entering class from 1986 tosignificantly different but female students 1990. Figure 1 shows class-specific meanenhanced their preventive cardiology atti- values for frequency of physical activity, body
mass index, preventive cardiology knowledgeand preventive cardiology attitudes. Class-specific mean percent of calories fromsaturated fat, total fat and carbohydrates areTable 7. Comparison of physical activity preven-
tivecardiologyknowledgeandpreventivecardiology shown in Fig. 2. Figure 3 presents class-attitudes (mean -4-S.D.) of male MSIV graduating specific mean levels of dietary fiber,medical students 1987 versus 1990-91. cholesterol and calcium adjusted for calories.
These data show no evidence of linear trends
Students Activity Attitudes Knowledge over time for any of the assessed variables.(no./week) Thus, the changes do not appear to represent
a systematic secular trend.Men
Graduated Discussion1987 3.1 -4-2.6 47.5 -4-3.9 15.3 4. 2.5
Graduated
1990-91 2.94. 2.0 46.94- 4.7 15.44.2.6 The principal goal of our PCAA has beenWomen the introduction and integration of preventive
Graduated cardiology concepts into the medical school1987 3.2 4. 2.6 48.8 4. 4.8 15.6 4- 2.1Graduated curriculum. Through an intensive commit-
1990 2.8 4. 1.7 48.8 4. 4.0 16.1 4.2.8 ment emphasizing education in preventivecardiology, UCSD medical students who had
Independent sample t-tests were non-significant at P=0.05. entered since 1986 have had consistent ex-
S.D., standard deviation posure to preventive cardiology conceptsNote: 1987 "Control MSIV" (men = 54), 1990-91 MSIV (men throughout their training. Exposure to= 65), 1987 "Control" MSIV (women = 21), 1990-91 MSIV(women= 29). preventive cardiology concepts begins during


23
PCAA faculty, have generated a great deal of Students participating in the preventive car-student interest. Students with elevated risk diology elective received extensive exposure tofactors are given further counseling and treat- adult and pediatric preventive cardiology.ment. During the four years of medicalschool, students receive numerous lectures on The annual CVD risk factor assessment was
preventive cardiology in the core curriculum, designed as a teaching tool [12]. The par-
Fig. 2. Percent of saturatedfat, total fat and carbohydratesamong enteringmedical students, 1986-1990.The changes do not show a linear trend, thus renderingthe influenceof secular trends unlikely.
Percent of Calories MEN6O55 ...................................................................................................................................................................................................................................................................50 .........454 0 :!$i:i:i:i:i:_:i:i::........................................
35
30252015
10
01986 1987 1988 1989 1990
Year of Entry to Medical School
I Saturated Fat _ Total Fat _ Carbohydrates
Percent of Calories WOMEN60
455055 ............ _ .........-ll,40 ....i35 ......i3O ....2520
105 i0
1986 1987 1988 1989 1990
Year of Entry to Medical School
1 Saturated Fat _ Total Fat _ Carbohydrates

0 0 0 0 0 0 0 0 0 0 0 0 _m"0 0 0 0 0 0 0 0 0 0 0 0 0 0
I I I
"tl _ m
o_. o _. o _:._" _ _" •-, _. _-'.
-- _ --
o --- g _"0 :.: 0
_ -- " l _ l _ _
:=l 0 :::l 0 "

25
ticipation of senior students as technicians in We recognize that this is not a formalthe annual risk factor assessment has pro- experiment and that there are many sources ofvided an additional educational opportunity bias. One possible source of bias is the limitedin preventive cardiology. Moreover, the op- response rate among fourth year students.portunity to reassess part of the risk factorprofile in the year of graduation has provided Despite their apparent representativeness, it isan opportunity for an evaluation of our possible that respondents over represented theeducational efforts, more preventive cardiology oriented students.
However, this selection bias applies to bothWhile the risk factor assessment upon en- the "control" and exposed groups and thus
trance to medical school is fairly comprehen- should not explain differences on dietarysive, repeating the physical examination measures between the 1987 and 1991
component for the graduating students has graduating classes.not been possible, due to the logistics of
fourth year of medical school schedules. Both men and women reported significantDespite reminders and incentives, a low ques- decreases in leisure time physical activity overtionnaire response rate was obtained from the course of medical school, so the preven-fourth year students who also had first year tive cardiology curriculum appeared to havedata. Comparing the graduating class with the little effect on this variable. This question-"control group" (graduating students before naire does not obtain information on whythe PCAA curriculum changes) showed ap- students reduced activity. It is likely that fin-parently curriculum related changes for ding time to exercise is difficult during theirmales; i.e. lower consumption of fats, clinical rotations. However, some clinicalcholesterol and higher consumption of car- rotations require mild physical exertion. Morebohydrates for the PCAA exposed group, research is needed to evaluate these problems.There are several explanations for the failure Perhaps some attention should be paid toto find these effects for women. For example, helping students maintain an exercise pro-the baseline diet for women contained less gram while in medical school.saturated fat to begin with. For both groupshowever, the comparison of the diet and per- Several previous studies have demonstratedcent of calories from macronutrients were the value of assessing of CVD risk factorssimilar to the current National Cholesterol among medical students. In one study, focus-Education program recommendation. This is ing on exercise, students at St. Louis Universi-encouraging since it reflects the favorable ty who participated in a special exercisedietary habits in this select group of students program increased their maximum oxygenwho will be future physicians. Knowledge, consumption 15% over the four years ofattitudes, and exercise were comparable for medical school [13]. Several studies havethe two graduating classes. Although these evaluated blood pressure in medical students.data suggest that the program produced Pearson and colleagues evaluated coronarylimited change, there may have been ceiling heart disease and hypertension among formereffects for both the knowledge and attitude graduates of the Johns Hopkins Medicaltests. For attitudes, the distribution was skew- School. Significant prospective predictors ofed toward the top scores. For knowledge, the hypertension included age, systolic blooddifficulty of the questions made scores above pressure _during medical school, parental17 difficult for even the best of students. The history of hypertension and quetelet index.comparison of means from 1986 through 1990 Thus, information obtained during medicalsuggested that the observed results were not school can be a significant prospective predic-due to secular trends, tor of later hypertension and CVD [14] and

r_-_ -_ _ _ _"O" _a
_ O_ ¢_ _ _-__ _-__ _ _ _ .'_ _" _ _-_
_°' _ _'_'* "_ _" _ o x=._-_*__o_=.= _.. i:_ 0 ¢_ _
• _ <o _ _.._ O__ oo (,_ ca .• _'_ 0 ¢:_" I:= ""
-" -- *_ _ _ _ 0 r_ _" 0 _.
•. 7_ _n.>_ ._ _*_ '* _ _".... ¢_ , ¢:__
_'_" _ o.° _ ,-._ = _ =
o'" o _ oo _B ._ _,'_ o" "_I
a_ ,_ _. __ e oT_. _ _ ._ r,'= _-=<" =_ ? ,*,o
_-. _ _.-. _ = ._'._ _-_ _ _-_-_.._ ,_ ___
,_ _ E_ -.o° _o_- _o_ _
_- _ _ _. _= __ _ _ =.o _ _ Eo_ o_ _ _ o
27
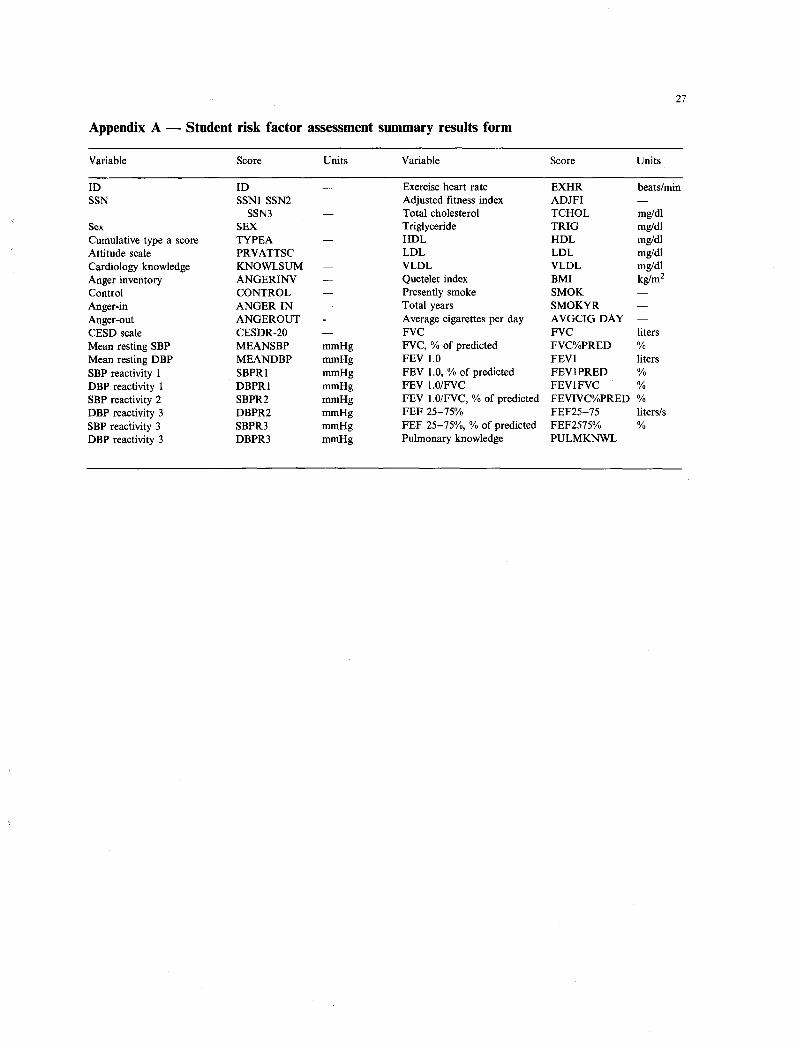
Appendix A -- Student risk factor assessment summary results form
Variable Score Units Variable Score Units
ID ID -- Exercise heart rate EXHR beats/min
SSN SSN1 SSN2 Adjusted fitness index ADJFI --
SSN3 -- Total cholesterol TCHOL mg/dl
Sex SEX Triglyceride TRIG mg/dl
Cumulative type a score TYPEA -- HDL HDL mg/dlAttitude scale PRVATTSC -- LDL LDL mg/dl
Cardiology knowledge KNOWLSUM -- VLDL VLDL mg/dl
Anger inventory ANGERINV -- Quetelet index BMI kg/m 2Control CONTROL -- Presentlysmoke SMOK --
Anger-in ANGERIN -- Totalyears SMOKYR --
Anger-out ANGEROUT Average cigarettesper day AVGCIG DAY --CESDscale CESDR-20 -- FVC FVC liters
Mean resting SBP MEANSBP mmHg FVC, % of predicted FVC%PRED %
MeanrestingDBP MEANDBP mmHg FEV 1.0 FEV1 liters
SBP reactivity 1 SBPR1 mmHg FEV 1.0,% of predicted FEV1PRED %DBP reactivity 1 DBPR1 mmHg FEV 1.0/FVC FEV1FVC %
SBP reactivity 2 SBPR2 mmHg FEV 1.0/FVC, % of predicted FEVIVC% PRED %DBP reactivity 3 DBPR2 mmHg FEF 25-75% FEF25-75 liters/s
SBP reactivity 3 SBPR3 mmHg FEF 25-75%, % of predicted FEF2575% %
DBP reactivity 3 DBPR3 mmHg Pulmonary knowledge PULMKNWL




![Health Status: Types of Validity and by Robert M Kaplan ...rmkaplan.bol.ucla.edu/Robert_M._Kaplan/1976_Publications_files/00… · by Robert M. Kaplan, ].W. Bush, and Charles C. Berry](https://static.fdocuments.net/doc/165x107/60246b910d793f42e26bcfc7/health-status-types-of-validity-and-by-robert-m-kaplan-by-robert-m-kaplan.jpg)













