
lationship of Advance Directives to Physician-Patient...
5
Reprinted from the Archives of Internal Medicine April 25, 1994 Volume 154 Copyright 1994, American Medical Association ORIGINAL INVESTIGATION Relationship of Advance Directives to Physician-Patient Communication Jaya Virmani; Lawrence J. Schneiderman, MD; Robert M. Kaplan, PhD Background: Although advance medical directives, such Results: Physicians were frequenflyunaware oftheir patients' as living wills and durable powers of attorney for health advance directives. Although patients with advance direc- care, are by themselves imperfect instruments for ex- rives were marginally more likely than patients without ad- pressing patients' treatment preferences, a possible ben- vance directives toreportdiscussionsabout end-of-lifetreat- efit of these documents is that they will enhance patient- ment decisions, only 34 (30%) out of the total of 115 patients physician communication, especially when end-of-life claimedthattheyhadanydiscussionoftreatmentdecisions treatment decisions have to be made. with their physicians. Such discussions tended to be about general life attitudes and feelings rather than specific treat- Method: Structured interviews were completed for 115 ments, such as use of artificial nutrition or ventilation. seriously ill cancer patients and 22 of their physicians. The questions dealt with various aspects of advance di- Conclusion: Despite public enthusiasm for the use of rectives, including communications between the two par- advance directives and great efforts to promote them, we ties regarding general and specific treatment wishes. Re- found little evidence that these documents are associ- sponses were compared in 37 physician-patient pairs for ated with enhanced communication between patients and patients who had executed advance directives and in 31 physicians about end-of-life treatment decisions. physician-patient pairs for patients who had not ex- ecuted advance directives. (Arch Intern Med. 1994;154:909-913) p ATIENTS' RIGHTStO partici- thermore, they have been shown to be ira- pate in medical decisions perfect vehicles for conveying patients' and, in particular, to refuse wishes.l° Without specific guidance, how- unwanted treatments are ever, physicians apparently have poor in- now well grounded in eth- sights into their patients' wishes and may ics and the law. Advance directives, in- even project their own values when it cluding instruction directives, such as liv- comes to medical treatment decisions.1149 ing wills, and proxy directives, such as In the face of these observations, an argu- durable powers of attorney for health care, ment has been made that, although they have been developed as means of extend- may be flawed instruments for conveying ing patients' decision-making powers be- information, advance directives will en- yond their loss of mental competence, t-5 hance communication between patients The federally legislated Patient Self- and their physicians about these matters Determination Act now requires all medi- through the process of formulating and re- cal facilities certified by Medicaid or Medi- cording critical end-of-life medical treat- care to advise patients of their rights to ment wishes, n The purpose of this study accept or refuse medical treatment and to provide information regarding state- provided advance directives. Surveys and From the Divisionof Health studies show, however, that despite wide- Care Sciences,Departmentof spread support and promotion, 6,7written Familyand Preventive Medicine,Universityof advance directives are infrequently ex- California, San Diego. ecuted even by seriously ill patients, s,9Fur- ARCH INTERN MED/VOL 154, APR 25, 1994 9O9
Transcript of lationship of Advance Directives to Physician-Patient...

Reprinted from the Archives of Internal MedicineApril 25, 1994 Volume 154
Copyright 1994, American Medical Association
ORIGINAL INVESTIGATION
Relationship of Advance Directives toPhysician-Patient CommunicationJaya Virmani; Lawrence J. Schneiderman, MD; Robert M. Kaplan, PhD
Background: Although advance medical directives, such Results:Physicians were frequenflyunaware oftheir patients'as living wills and durable powers of attorney for health advance directives. Although patients with advance direc-care, are by themselves imperfect instruments for ex- rives were marginally more likely than patients without ad-pressing patients' treatment preferences, a possible ben- vance directives toreportdiscussionsabout end-of-lifetreat-efit of these documents is that they will enhance patient- ment decisions, only 34 (30%) out of the total of 115 patientsphysician communication, especially when end-of-life claimedthattheyhadanydiscussionoftreatmentdecisionstreatment decisions have to be made. with their physicians. Such discussions tended to be about
general life attitudes and feelings rather than specific treat-Method: Structured interviews were completed for 115 ments, such as use of artificial nutrition or ventilation.seriously ill cancer patients and 22 of their physicians.The questions dealt with various aspects of advance di- Conclusion: Despite public enthusiasm for the use ofrectives, including communications between the two par- advance directives and great efforts to promote them, weties regarding general and specific treatment wishes. Re- found little evidence that these documents are associ-sponses were compared in 37 physician-patient pairs for ated with enhanced communication between patients andpatients who had executed advance directives and in 31 physicians about end-of-life treatment decisions.physician-patient pairs for patients who had not ex-ecuted advance directives. (Arch Intern Med. 1994;154:909-913)
p ATIENTS' RIGHTStO partici- thermore, they have been shown to be ira-
pate in medical decisions perfect vehicles for conveying patients'and, in particular, to refuse wishes.l° Without specific guidance, how-unwanted treatments are ever, physicians apparently have poor in-now well grounded in eth- sights into their patients' wishes and may
ics and the law. Advance directives, in- even project their own values when itcluding instruction directives, such as liv- comes to medical treatment decisions.1149ing wills, and proxy directives, such as In the face of these observations, an argu-durable powers of attorney for health care, ment has been made that, although theyhave been developed as means of extend- may be flawed instruments for conveyinging patients' decision-making powers be- information, advance directives will en-yond their loss of mental competence, t-5 hance communication between patientsThe federally legislated Patient Self- and their physicians about these mattersDetermination Act now requires all medi- through the process of formulating and re-cal facilities certified by Medicaid or Medi- cording critical end-of-life medical treat-care to advise patients of their rights to ment wishes, n The purpose of this studyaccept or refuse medical treatment and toprovide information regarding state-provided advance directives. Surveys and
From theDivisionof Health studies show, however, that despite wide-
CareSciences,Departmentof spread support and promotion, 6,7writtenFamilyand PreventiveMedicine,Universityof advance directives are infrequently ex-California, San Diego. ecuted even by seriously ill patients, s,9Fur-
ARCH INTERN MED/VOL 154, APR 25, 19949O9

METHODS INTERVIEW QUESTIONNAIRE
The structured format was designed to obtain the followingSUBJECTS information:Doesthepatienthavean advancedirective?If
the patient has an advance directive, what type is it (living will
Physicians in the Cancer Center of the University of Cali- or durable power of attorney for health care) ? How did thefornia, San Diego, Medical Center, the Veterans Affairs Medi- patient find out about advance directives? What does the pa-cal Center in San Diego, and the offices of two oncologists tient see as the purpose of the advance directive? Did the pa-in private practice in San Diego were asked to provide the tient discuss the advance directive with his or her physician,names of cancer patients who were estimated to have less and if so, what was discussed? If the patient does not have anthan a 50% chance of S-year survival. No other criteria, such advance directive, does the patient know what it is? What isas age, gender, type of cancer, or advance directive status, the reason for not having one? Did the patient discuss futurewere imposed. A total of 150 patients were referred, and at- health carewishes with the physician, includinglife-sustainingtempts were made to contact and administer a structured treatment decisions, regardless of any advance directive dis-interview to all of them by phone. Of these 150 patients, 33 cussion? Does the patient believe that the physician wouldcould not be entered into the study: 16 had died by the time know what kind of health care the patient would want in thecontact was attempted, nine refused the interview, five were event the patient lost decision-making capacity? Does the pa-too sick to speak over the phone, and three did not speak tient believe that the physician will comply with the patient's
English. A total of 115 patients (77%) (62 patients from the wishes for medical treatments? Is the patient satisfied that theCancer Center, 14 from the Veterans Affairs Medical Cen- advance directive document clearly states the patient's medi-ter, and 39 from the offices of the two oncologists in private cal treatment wishes?
practice) of the original sample of 150 patients formed the Patients were interviewed and questionnaires were ad-subject of this study. The referring physicians were asked ministered to physicians between June 24 and Septemberto return a written questionnaire that was designed to match 4, 1992. The project was approved by the University of Cali-the formatadministeredbytelephoneto thepatients.Twenty- fornia Human Subjects Committee.two (76%) of 29 physicians returned completed question-naires, which resulted in 37 physician-patient pairs for those DATA ANALYSIS
patients who had executed advance directives and 31physician-patient pairs for those patients who had not ex- Thedatawereanalyzedusingdescriptivetechniques. Compari-ecuted advance directives. Fifteen (52%) of 29 physicians sonsweremadeusingxatests fordichotomousvariables.Ninety -had more than one patient in the study (range, two to 18 pa- five percent confidence intervals (CIs) were calculated usingtients; median, four patients). SEsfor proportions and the standard normal distribution.
is to examine this argument and to determine whether highest category was patients who reported that it was
executing advance directives is indeed associated with "my own idea." Other responses were lawyer, friend, ram-
enhanced communication between patients and their phy- ily, and counselor (Table i). The majority of the pa-sicians on these issues, tients who had executed advance directives (53 of [83%]
of 64) stated that the document clearly expressed theirwishes for future medical treatments.RESULTS
Of those patients who had not executed an advance
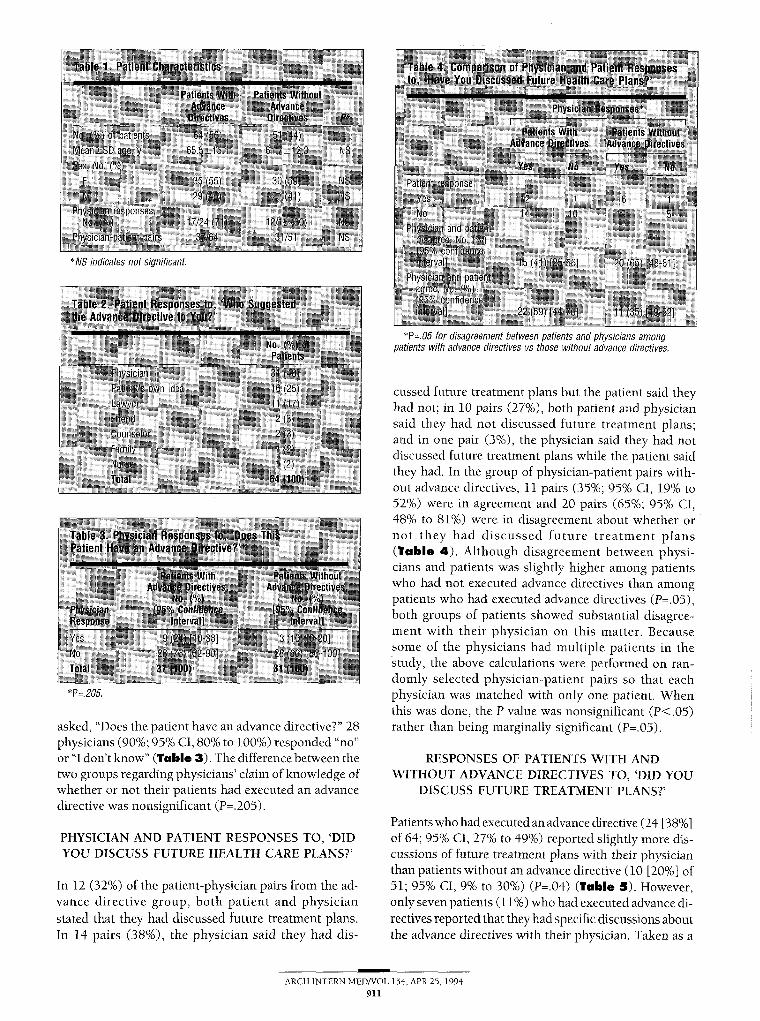
Of the 115 patients contacted and interviewed, 64 (55.7%) directive, 36 (71%) of 51 claimed knowledge about what
had executed some type of advance directive; 51 (44.3%) these documents are and gave various reasons for not hav-
had not. Of those patients with advance directives, 52 ing executed one.had executed a California Durable Power of Attorney for
Health Care (which contains both a proxy and an in- PHYSICIAN RESPONSES TO, 'DOES THE
struction component), seven had executed a living will PATIENT HAVE AN ADVANCE DIRECTIVE?'
(which provides an instruction component only), and five
had executed living wills and durable powers of attor- Within the group of 64 patients with advance directives,
ney for health care as two separate documents. There were there were 37 cases in which a physician interview was
no significant differences between the two groups with also available. When the physicians of these patients were
respect to age, sex, physician response, or number ofphy- asked, "Does the patient have an advance directive?" 28
sician-patient pairs (Table 1 ). physicians (76%; 95% CI, 62% to 90%) responded "no"
Half the patients who had executed an advance di- or "I don't know" to the question. In the group of 51 pa-
rective stated that the documents were suggested to them tients without advance directives, there were 31 physician-
by their physician or another health care worker. The next patient pairs. When the physicians of these patients were
ARCH INTERN MED/VOL 154, APR 25, 1994910
*NSindicatesnotsignificant.
*P=.05 for disagreement between patients and physicians amongpatients with advance directives vs those without advance directives.
cussed future treatment plans but the patient said theyhad not; in 10 pairs (27%), both patient and physiciansaid they had not discussed future treatment plans;and in one pair (3%), the physician said they had notdiscussed future treatment plans while the patient saidthey had. In the group of physician-patient pairs with-out advance directives, 11 pairs (35%; 95% CI, 19% to52%) were in agreement and 20 pairs (65%; 95% CI,
................................ 48% to 81%) were in disagreement about whether or_?!_'VS!g_ not they had discussed future treatment plans
{}|_!i_ntN :_ (Table 4). Although disagreement between physi-........................ clans and patients was slightlyhigher among patients
whohad not executedadvancedirectivesthanamongpatients who had executed advance directives (P=.05),
}f _w|_|an_ie.................... both groups of patients showed substantial disagree-.......... ment with their physicianon this matter. Because
;;_, some of the physicians had multiple patients in theStudy,theabovecalculationswereperformedon ran-
{{{................................. domly selected physician-patient pairs so that each*p=.2os. physician was matched with only one patient. When
this was done, the P value was nonsignificant (P<.05)asked, "Does the patient have an advance directive?" 28 rather than being marginally significant (P=.05).physicians (90%; 95% CI, 80% to 100%) responded "no"or "I don't know" (Table 3). The difference between the RESPONSES OF PATIENTS WITH AND
two groups regarding physicians' claim of knowledge of WITHOUT ADVANCE DIRECTIVES TO, 'DID YOUwhether or not their patients had executed an advance DISCUSS FUTURE TREATMENT PLANS?'directive was nonsignificant (P=.205).
Patients who had execu ted an advance directive ( 24 [38%]
PHYSICIAN AND PATIENT RESPONSES TO, 'DID of 64; 95% CI, 27% to 49%) reported slightly more dis-YOU DISCUSS FUTURE HEALTH CARE PLANS?' cussions of future treatment plans with their physician
than patients without an advance directive (10 [20%] ofIn 12 (32%) of the patient-physician pairs from the ad- 51; 95% CI, 9% to 30%) (P=.04) (Table S). However,vance directive group, both patient and physician only seven patients (l l%) who had executed advance di-stated that they had discussed future treatment plans, rectives reported that they had specific discussions aboutIn 14 pairs (38%), the physician said they had dis- the advance directives with their physician. Taken as a
ARCH INTERN MED/VOL 154-, APR 25, 1994911
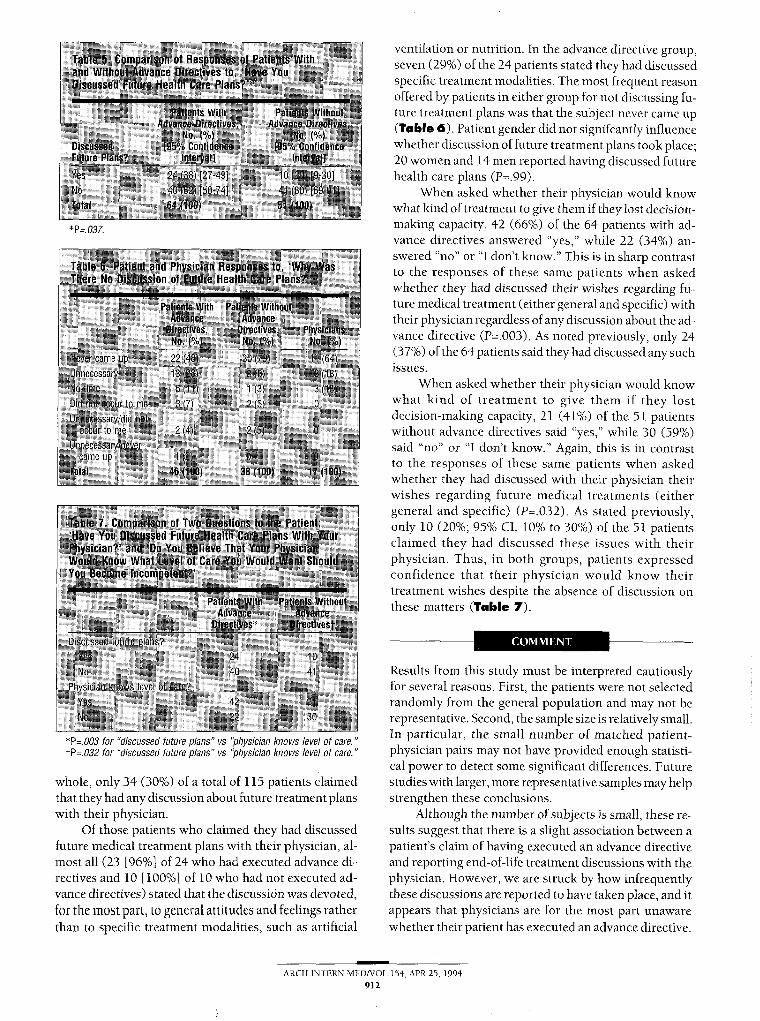
ventilation or nutrition. In the advance directive group,seven (29%) of the 24 patients stated they had discussedspecific treatment modalities. The most frequent reason
offered by patients in either group for not discussing fu-th.tiut;_{ ture treatment plans was that the subject never came up¢_v_;,_: (Table 6). Patient gender did not signifcantly influence
_n_e_-_ whether discussion of future treatment plans took place;.................. 20 women and !4 men reported having discussed futurela!_>;i_ health care plans (P=.99).g!qa_!<_ When asked whether their physician would know
what kind of treatment to give them if they lost decision-
*P=.037. .......... making capacity, 42 (66%) of the 64 patients with ad-vance directives answered "yes," while 22 (34%) an-swered "no" or "I don't know." This is in sharp contrastto the responses of these same patients when askedwhether they had discussed their wishes regarding fu-ture medical treatment (either general and specific) withtheir physician regardless of any discussion about the ad-vance directive (P=.003). As noted previously, only 24(37%) of the 64 patients said they had discussed any suchissues.
When asked whether their physician would knowwhat kind of treatment to give them if they lostdecision-making capacity, 21 (41%) of the 51 patientswithout advance directives said "yes," while 30 (59%)said "no" or "I don't know." Again, this is in contrastto the responses of these same patients when askedwhether they had discussed with their physician theirwishes regarding future medical treatments (eithergeneral and specific) (P=.032). As stated previously,only 10 (20%; 95% CI, 10% to 30%) of the 51 patientsclaimed they had discussed these issues with theirphysician. Thus, in both groups, patients expressedconfidence that their physician would know theirtreatment wishes despite the absence of discussion onthese matters (Table 7).
COMMENT
Results from this study must be interpreted cautiouslyfor several reasons. First, the patients were not selectedrandomly from the general population and may not berepresentative. Second, the sample size is relatively small.In particular, the small number of matched patient-*P=.O03for"discussedfutureplans"vs"physicianknowslevelofcare."
tP=.032for"discussedfutureplans"vs"physicianknowslevelofcare." physician pairs may not have provided enough statisti-cal power to detect some significant differences. Future
whole, only 34 (30%) of a total of 115 patients Claimed studies with larger, more representative samples may helpthat they had any discussion about future treatment plans strengthen these conclusions.
with their physician. Althoughthe number ofsubjects issmall, thesere-Of those patients who claimed they had discussed sults suggest that there is a slight association between a
future medical treatment plans with their physician, al- patient's claim of having executed an advance directivemost all (23 [96%] of 24 who had executed advance di- and reporting end-of-life treatment discussions with therectives and 10 [100%1 of 10 who had not executed ad- physician. However, we are struck by how infrequentlyvance directives) stated that the discussion was devoted, these discussions are reported to have taken place, and itfor the most part, to general attitudes and feelings rather appears that physicians are for the most part unawarethan to specific treatment modalities, such as artificial whether their patient has executed an advance directive.
ARCH INTERN MED/VOL 154, APR 25, 1994912

Indeed, overall communication on these matters be- vance directive document, there still appears to be a lacktween physicians and patients seems to be low. This is of detailed discussion dealing with specific medical treat-all the more surprising since, if any patients would be ments. It is clear, therefore, that there is more to be learned
likely to seek discussions about future end-of-life medi- about the role of advance directives in physician-patientcal treatments, it would seem to be this group of pa- communication and, in particular, about the apparentlack
dents, all of whom were aware that they were seriously of engagement in this process, despite public enthusi-ill with cancer. Also, it is apparent that discussions that asm to promote these instruments.took place did not usually concern specifics of treat-
ment, such as artificial ventilation or cardiopulmonary Accepted for publication August 16, 1993.resuscitation, but rather tended to deal with generalities This study was supported by grant HS 06912-03fromand avoided details, the Agency of Health Care Policy Research and by grant
The most frequent reason claimed by both patients HL07491 from the National Heart, Lung, and Blood In-and physicians for not having discussions about end-of-
stitute, National Institutes of Health, Bethesda, Md.life medical treatments was that "the subject never came Reprint requests to Family & Preventive Medicine,up." It would seem, therefore, that physicians are not tak- 0622, University of California, San Diego, 9500 Gilmaning the responsibility for initiating such discussions. Dr, La Jolla, CA 92093-0622 (Dr Schneiderman).
Because there was slightly more agreement be-tween physicians and patients in the advance directive
REFERENCESgroup about whether or not future medical treatment planshad been discussed, it seems that the presence of the docu-ment did stimulate communication between the two par- t. Schneidermank,ArrasJ. Counselingpatientstocounselphysiciansonfutureties. Nevertheless, even in the absence of such discus- careintheeventofpatientincompetence.AnnInternMeal.1985;102:693-698.sions, patients appeared to have great confidence that their 2. Oavids0nKW,HacklerC,CaradineDR,McC0rdRS.Physicians'attitudesonadvancedirectives.JAMA.1989;262:2415-2419.physicians would know what kind of treatments they 3. BuchananAE,BrockDW. Decidingfor Others:TheEthicsof SurrogateDeci-would want. Unfortunately, empirical studies provide little sion Making.Cambridge, England:Cambridge UniversityPress; 1989.
ground for this confidence in physicians' knowledge of 4. OrentlicherD.Advancemedicaldirectives.JAMA.1990;263:2365-2367.their patients' treatment wishes. ]1-19 5. CurrentOpinionsoftheCouncilonEthicalanddudicialAffairsoftheAmericanMedicalAssociation.Chicago,II1:AmericanMedicalAssociation;1989:§2.20,
The evidence of infrequent discussion between phy- §2.21.sician and patient about matters contained in advance di- 6. DanisM, SoutherlandL, GarrettJ, et el. A prospectivestudy of advancedi-
rectives may indicate physician discomfort with the sub- rectivesfor life-sustainingcare.N Engld Med.1991;324:882-888.
ject. It is worth noting that all the patients in this study 7. EmanuelL,BarryM.St0eckleJ,Ettels0nL,EmanuelE.Advancedirectivesformedicalcare:a casefor greateruse.NEnglJ Med.1991;324:889-895.discussed their disease and personal wishes openly on 8. Steiber SR. Rightto die: public balks at deciding for others. Hospitals.March
the telephone with an unseen and unfamiliar inter- 6,1987;61:72.viewer. This leads us to believe that patients themselves 9. SchneidermanLJ, PearlmanR,KaplanR,AndersonJ, R0senberg E.Relation-ship of general advance directive instructions to specific life-sustaining treat-want to talk about their end-of-life medical treatment needs mentpreferencesin patientswithseriousiltnesses.ArchInternMeal.1992;and wishes; therefore, there is little justification for phy- 152:2114-2122.sicians not initiating discussions on these subjects based 10. Schneiderman LJ, Kr0nickR, KaplanRM,Anderson dP, Lancer RD.Effects of
on the idea that such discussions might make patients feel offeringadvancedirectivesonmedicaltreatmentsandcosts:a prospectivestudy.Ann Intern MoO.1992;117:599-606.
uncomfortable. Indeed, five of the patients who had not 11. 8choeiderman LJ, Kaplan RM, Pearlman RA, Teetzel H. Do physicians' ownexecuted advance directives asked the interviewer dur- preferencesfor life-sustainingtreatmentinfluencetheirperceptionsof patients'
ing the telephone interview how they could obtain such preferences?d ClioEthics.1993;4:28-33.a document. Although it has been suggested that women 12. Uhlmann RF, Peadman RA. Perceived quality of life and preferences for life-
sustainingtreatmentin olderadults.Arch InternMed.1991;151:495-497.are more willing than men to discuss their medical con- 13. DanisM, Gerrity MS, SoutherlandLI, PatrickDL. A comparisonof patient,cerns with their physician, in this study there was no sig- family, and physician assessments of the value of medical intensive care. Crit
nificant difference in the likelihood of discussing future CareMed.1988;16:594-600.medical treatment plans. Neither men nor women, how- 14. StarrTJ, PearlmanRA,UhlmannRF.Qualityof life andresuscitationdecisionsin elderlypatients.J GenIntern Med.1986;1:373-375.ever, reported discussing these issues much with their 15. BedellSE,DelbancoKL.Choicesaboutcardiopulmonaryresuscitationin thephysician, hospital:when do physicianstalk with patients?N Engl J Med. 1984;310:
This study provides further disquieting evidence of 1089-1093.poor communication between patients and physicians re- 16. UhlmannRF,PearlmanRA,CainKC.Understandingofelderly patients'resus-
citationpreferencesby physiciansandnurses.WestJ Med.1989;50:705-707.carding important medical treatment decisions in the pres- 17. Uhlmann RF, Pearlman RA,CainKD.Physicians' and spouses' predictions ofence of serious illness, despite the many efforts that have elderlypatients'resuscitationpreferences,JGerontol.1988;43:M115-M121.
been made to promote advance directives. (This study 18, Seckler AS, Meier DE, MulvihillM, Paris BE. Substituted judgement: how ac-was carried out after the enactment of the Patient Self- curateareproxypredictions?AnnInternMed.1991;115:92-98,
19. Zweibel NR, Cassel CK. Treatment choices at the end of life: a comparison ofDetermination Act.) Although there is evidence that com- decisionsbyolderpatientsandtheirphysician-selectedproxies.Gerontologist.munication is slightly improved in the presence of an ad- 1989;29:615-621.
ARCH INTERN MED/VOL 154,APR 25, 1994-913
Printed and Published in the United States of America





![Health Status: Types of Validity and by Robert M Kaplan ...rmkaplan.bol.ucla.edu/Robert_M._Kaplan/1976_Publications_files/00… · by Robert M. Kaplan, ].W. Bush, and Charles C. Berry](https://static.fdocuments.net/doc/165x107/60246b910d793f42e26bcfc7/health-status-types-of-validity-and-by-robert-m-kaplan-by-robert-m-kaplan.jpg)












