
Echocardiographic Stenosis -...
8
Pulsed Doppler Echocardiographic Study of Mitral Stenosis CHRISTIAN THUILLEZ, M.D., PIERRE THEROUX, M.D., MARTIAL G. BOURASSA, M.D., DIDIER BLANCHARD, M.D., PIERRE PERONNEAU, JEAN-LEON GUERMONPREZ, M.D., BENOIT DIEBOLD, M.D., DAVID D. WATERS, M.D., AND PIERRE MAURICE, M.D. SUMMARY The value of pulsed Doppler echocardiography in the assessment of mitral stenosis was studied in a consecutive series of 175 patients before right- and left-heart catheterization. All Doppler recordings were interpreted independently by two observers. Twenty patients had repeat studies to demonstrate the reproducibility of the method. Adequate recordings were obtained in 156 patients. A normal flow pattern was observed in all 41 patients in sinus rhythm without a mitral valve gradient but in none of the 51 patients in sinus rhythm with a mitral gradient. In atrial fibrillation the normal pattern was identified in all three patients with no mitral gradient but in none of the 61 with a gradient. Three patterns of mitral valve flow could be dis- tinguished that corresponded to mild, moderate and severe stenosis. The mitral valve gradient in the 36 pa- tients with pattern I was 6.1 ± 1.7 mm Hg (SD) (range 3-10 mm Hg); in 54 patients with pattern II it was 12.0 ± 2.5 mm Hg (range 8-18 mm Hg) (p < 0.001 vs I); in 22 patients with pattern III it was 22.0 ± 2.6 mm Hg (range 18-27 mm Hg) (p < 0.001 vs II). Overlap was observed in only four patients, all of whom had a gradient between 8-10 mm Hg. Mitral valve area was 2.14 ± 0.58 cm2 in pattern I, 1.17 ± 0.33 cm2 in pattern II and 0.67 ± 0.26 cm2 in pattern III (p < 0.001 between all groups). The presence of associated mitral regurgitation in 39 patients and aortic valve disease in 32 patients did not affect the Doppler assessment of mitral stenosis. Thus, pulsed Doppler echocardiography can accurately detect the presence of mitral stenosis and assess its severity. THE NONINVASIVE STUDY of mitral valvular disease has been greatly enhanced by ultrasound techniques. M-mode echocardiography allows recognition of the stenotic valve' and bidimensional echocardiography permits an estimation of mitral valve area.2 Mitral valve flow can be recorded by Doppler echocardiography3 and preliminary results suggest that this technique can provide an estimate of the severity of mitral stenosis.4 The limitations of standard echocardiography in the quantification of mitral stenosis have been recognized8 and the usefulness of the bidimensional approach is being evaluated.9 Pulsed Doppler techniques theoretically provide an alternative approach to this problem. In this study we extended previous work from our laboratory7 to assess prospectively in a large number of patients undergoing cardiac catheterization the accuracy of Doppler echocardiography in detect- ing and defining the severity of mitral stenosis. Methods Patient Selection A Doppler study of the mitral valve was attempted on the day before right and left cardiac catheterization From the Department of Medicine, Montreal Heart Institute, University of Montreal Medical School, Quebec, Canada, and Clinique Cardiologique and Centre National de Recherches Scien- tifiques, H6pital Broussais, Paris, France. Supported in part by the L.L. Levesque Foundation and a grant from the CNAMTS (France). Mr. Peronneau is Maitre de Recherche at INSERM, France. Address for correspondence: Pierre Theroux, M.D., Montreal Heart Institute, 5000 East, Belanger Street, Montreal, Quebec, HIT 1C8, Canada. Received May 18, 1979; revision accepted July 24, 1979. Circulation 61, No. 2, 1980. in 175 consecutive patients with suspected congenital or valvular heart disease investigated at our institution between September 1977 and August 1978. Nineteen patients in whom a low signal-to-noise ratio precluded the recording of mitral valve flow were excluded from the study. In the remaining 156 patients, a comparison of the Doppler and hemodynamic data was possible. Twelve patients had had mitral valve replacement by a Carpentier-Edwards xenograft. Cardiac catheteriza- tion revealed the presence of a mitral valve gradient in 112 patients. Mitral stenosis was associated with significant mitral regurgitation in 39 and 32 had aortic valvular disease. Among the 44 patients without mitral stenosis six had coronary artery disease, eight aortic valve disease, nine atrial septal defect, four ven- tricular septal defect, six isolated mitral regurgitation, one pulmonary valve stenosis and 10 normal right- and left-heart catheterization. Mean age was 43 years (range 18-65 years). In one patient we obtained simul- taneous Doppler and intracardiac pressure gradient recordings. Doppler Apparatus and Doppler Output The directional range-gated Doppler instrument has been described elsewhere.'0-13 The unit used in this study7' 14 transmits ultrasound at a frequency of 4 MHz, with a pulse repetition rate of 5-10 kHz. The transcutaneous depth of exploration ranges from 3-14 cm. The duration of the emitted pulse is adjusted between 2-4 isec and the crystal is allowed to receive for 100-200 gsec. The size of the sample volume is determined by the delay in the receiver and by the duration of the ultrasound burst. A high-pass filter with a cutoff frequency of 600 Hz eliminates low- frequency signals originating from cardiac wall mo- tion. 381 by guest on June 30, 2018 http://circ.ahajournals.org/ Downloaded from
Transcript of Echocardiographic Stenosis -...

Pulsed Doppler Echocardiographic Studyof Mitral Stenosis
CHRISTIAN THUILLEZ, M.D., PIERRE THEROUX, M.D., MARTIAL G. BOURASSA, M.D.,DIDIER BLANCHARD, M.D., PIERRE PERONNEAU, JEAN-LEON GUERMONPREZ, M.D.,BENOIT DIEBOLD, M.D., DAVID D. WATERS, M.D., AND PIERRE MAURICE, M.D.
SUMMARY The value of pulsed Doppler echocardiography in the assessment of mitral stenosis was studiedin a consecutive series of 175 patients before right- and left-heart catheterization. All Doppler recordings wereinterpreted independently by two observers. Twenty patients had repeat studies to demonstrate thereproducibility of the method. Adequate recordings were obtained in 156 patients. A normal flow pattern wasobserved in all 41 patients in sinus rhythm without a mitral valve gradient but in none of the 51 patients in sinusrhythm with a mitral gradient. In atrial fibrillation the normal pattern was identified in all three patients withno mitral gradient but in none of the 61 with a gradient. Three patterns of mitral valve flow could be dis-tinguished that corresponded to mild, moderate and severe stenosis. The mitral valve gradient in the 36 pa-
tients with pattern I was 6.1 ± 1.7 mm Hg (SD) (range 3-10 mm Hg); in 54 patients with pattern II it was 12.0± 2.5 mm Hg (range 8-18 mm Hg) (p < 0.001 vs I); in 22 patients with pattern III it was 22.0 ± 2.6 mm Hg(range 18-27 mm Hg) (p < 0.001 vs II). Overlap was observed in only four patients, all ofwhom had a gradientbetween 8-10 mm Hg. Mitral valve area was 2.14 ± 0.58 cm2 in pattern I, 1.17 ± 0.33 cm2 in pattern II and0.67 ± 0.26 cm2 in pattern III (p < 0.001 between all groups). The presence of associated mitral regurgitationin 39 patients and aortic valve disease in 32 patients did not affect the Doppler assessment of mitral stenosis.Thus, pulsed Doppler echocardiography can accurately detect the presence of mitral stenosis and assess itsseverity.
THE NONINVASIVE STUDY of mitral valvulardisease has been greatly enhanced by ultrasoundtechniques. M-mode echocardiography allowsrecognition of the stenotic valve' and bidimensionalechocardiography permits an estimation of mitralvalve area.2 Mitral valve flow can be recorded byDoppler echocardiography3 and preliminary resultssuggest that this technique can provide an estimate ofthe severity of mitral stenosis.4The limitations of standard echocardiography in the
quantification of mitral stenosis have been recognized8and the usefulness of the bidimensional approach isbeing evaluated.9 Pulsed Doppler techniquestheoretically provide an alternative approach to thisproblem. In this study we extended previous workfrom our laboratory7 to assess prospectively in a largenumber of patients undergoing cardiac catheterizationthe accuracy of Doppler echocardiography in detect-ing and defining the severity of mitral stenosis.
Methods
Patient Selection
A Doppler study of the mitral valve was attemptedon the day before right and left cardiac catheterization
From the Department of Medicine, Montreal Heart Institute,University of Montreal Medical School, Quebec, Canada, andClinique Cardiologique and Centre National de Recherches Scien-tifiques, H6pital Broussais, Paris, France.
Supported in part by the L.L. Levesque Foundation and a grantfrom the CNAMTS (France).Mr. Peronneau is Maitre de Recherche at INSERM, France.Address for correspondence: Pierre Theroux, M.D., Montreal
Heart Institute, 5000 East, Belanger Street, Montreal, Quebec,HIT 1C8, Canada.
Received May 18, 1979; revision accepted July 24, 1979.Circulation 61, No. 2, 1980.
in 175 consecutive patients with suspected congenitalor valvular heart disease investigated at our institutionbetween September 1977 and August 1978. Nineteenpatients in whom a low signal-to-noise ratio precludedthe recording of mitral valve flow were excluded fromthe study. In the remaining 156 patients, a comparisonof the Doppler and hemodynamic data was possible.Twelve patients had had mitral valve replacement by aCarpentier-Edwards xenograft. Cardiac catheteriza-tion revealed the presence of a mitral valve gradient in112 patients. Mitral stenosis was associated withsignificant mitral regurgitation in 39 and 32 had aorticvalvular disease. Among the 44 patients withoutmitral stenosis six had coronary artery disease, eightaortic valve disease, nine atrial septal defect, four ven-tricular septal defect, six isolated mitral regurgitation,one pulmonary valve stenosis and 10 normal right-and left-heart catheterization. Mean age was 43 years(range 18-65 years). In one patient we obtained simul-taneous Doppler and intracardiac pressure gradientrecordings.
Doppler Apparatus and Doppler Output
The directional range-gated Doppler instrument hasbeen described elsewhere.'0-13 The unit used in thisstudy7' 14 transmits ultrasound at a frequency of 4MHz, with a pulse repetition rate of 5-10 kHz. Thetranscutaneous depth of exploration ranges from 3-14cm. The duration of the emitted pulse is adjustedbetween 2-4 isec and the crystal is allowed to receivefor 100-200 gsec. The size of the sample volume isdetermined by the delay in the receiver and by theduration of the ultrasound burst. A high-pass filterwith a cutoff frequency of 600 Hz eliminates low-frequency signals originating from cardiac wall mo-tion.
381
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
VOL 61, No 2, FEBRUARY 1980
According to the Doppler principle, the unitmeasures the speed of moving structures that reflectultrasound. The frequency shift (AF) between theemitted and reflected ultrasound is proportional to theemitted frequency (F), to the velocity (V) of movingstructures within the sample volume and to the angle(0) between the ultrasound beam and the movingstructures according to the formula
2 V.F. cos 0,AF-=
where C is a constant representing the speed of ul-trasound in the medium.The range-gating system allows deflnition of a sam-
ple volume with known size and depth displayed onthe A- and M-mode echocardiogram. The Dopplershift of frequency within this sample volume isanalyzed through a zero-crossing detector. Thederived analog velocity signal is visualized on the os-cilloscope and transcribed on a Gould Brush model2400 forced-ink recorder.The derived velocity flow curve represents the
average of all velocities of blood cells within the sam-ple volume. The tracing indicates flow direction(toward or away from the transducer) and thepresence or absence of turbulence. The Doppler shiftis audible and the audio signal provides useful infor-mation about the quality of blood flow. For example,a laminar flow sounds soft and regular and its velocityprofile is neat and fine on the recorded tracings. A tur-bulent flow has a rough, more intense pitch withsounds of irregular intensity. The tracing is notsmooth and has indentations corresponding to suddenvariations in the velocity of moving elements. Thevelocity profile tracing omits important informationabout the width of the spectrum of reflected ul-trasound; however, its graphic representation providesobjective data about the pattern of flow. Mitralstenosis was evaluated in this study using only the in-formation contained on the tracings, which wererecorded at a paper speed of 50 cm/sec.
Doppler StudiesPatients were examined in the supine left lateral
position. After careful palpation of the apical impulse,the transducer was placed in the intercostal space atthe cardiac apex and oriented posteriorly, superiorlyand to the right along the axis of the left ventricular in-flow tract. A- and M-mode echocardiography per-mitted rapid recognition of the anterior mitral leafletand location of the sample volume in the left atrium atthe level of the mitral annulus, just behind the valveleaflets in their systolic position. A 5-kHz pulse repeti-tion rate was used. By slightly changing the angle ofthe transducer and the depth of the sample volume theoperator could avoid recording the motion of the valveleaflets that could cause errors in the interpretation ofthe tracings. The valvular motion is readily apparenton the audio signal, and one can avoid recording itwith a little experience. Selection of the highest
amplitude flow curves facilitated the interpretation ofthe tracings. By convention, a flow running toward thetransducer inscribed a curve above the electronic zerobaseline, and a flow running in the opposite directionwas recorded below the baseline. The systolic anddiastolic flow timing was recognized on the tracing bysimultaneously recording lead II of the ECG.The interpretation of tracings was based on our ex-
perience from a preliminary study in which three dis-tinctly abnormal flow curves correlated with differentdegrees of mitral stenosis.7 All Doppler flow patternswere analyzed before cardiac catheterization. Thetracings were then reviewed and interpreted blindly byan independent observer. The reproducibility of theflow pattern in the same patient was also studied byperforming a Doppler study on three different days in20 patients. Half of these 60 studies were performedby one examiner and the other half by a second.
Cardiac Catheterization Studies
Cardiac catheterization was performed in a fastingstate after premedication with 10 mg oral diazepam.Pulmonary wedge, left ventricular and aortic pres-sures were recorded with #8F catheters connected toP23Db Statham strain gauges on an Honeywellfiberoptic recorder at a paper speed of 100 cm/sec anda scale of 4 mm Hg/cm. Mitral valve gradient wasplanimetered over 10 consecutive cardiac cycles and amean gradient was calculated. Cardiac output was ob-tained by the Fick or dye-dilution method. Mitralvalve area was calculated by the formula of Gorlin andGorlinl5 when significant mitral valve regurgitationwas absent. Mitral regurgitation was assessed by leftventriculography and graded as mild when a smallregurgitant flow with incomplete opacification of theleft atrium was present and as significant when com-plete opacification of the left atrium occurred.16 Heartrate at the time of cardiac catheterization was similarto heart rate at the time of the Doppler study, with amaximal variation of 10 beats/min between the twoexaminations. Blood pressure was also comparable ineach patient at the time of the two studies. Statisticalanalyses were done using the t test. Values are ex-pressed as mean ± SD.
ResultsMitral Flow PatternsThe mitral flow patterns are illustrated in figure 1.
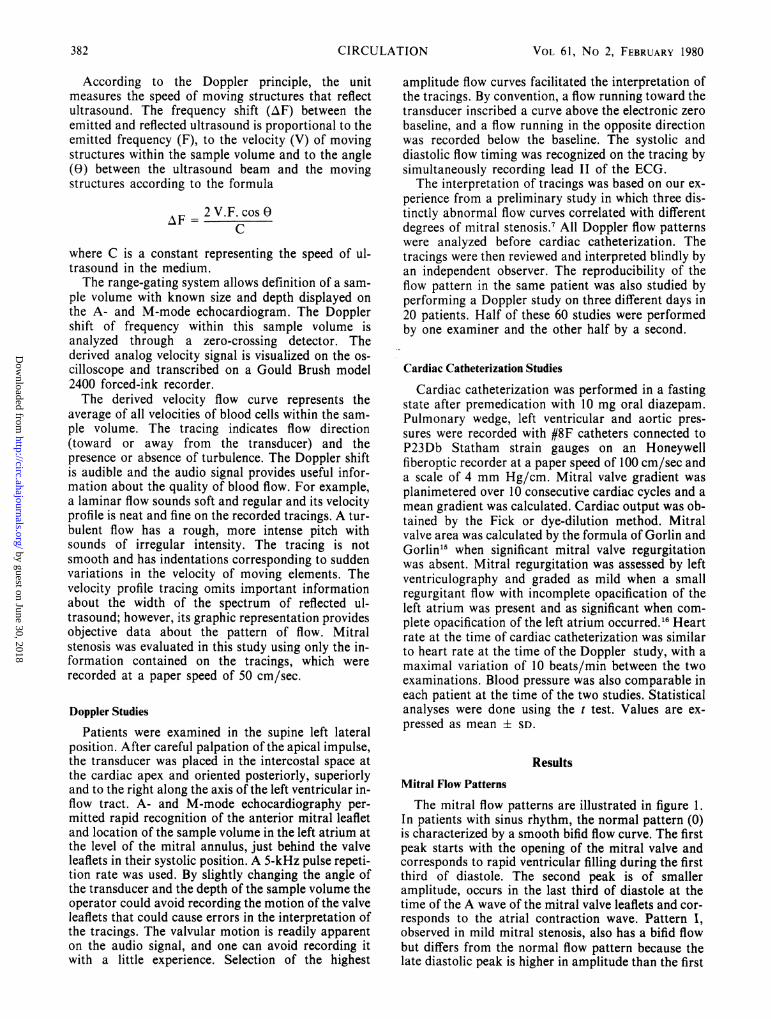
In patients with sinus rhythm, the normal pattern (0)is characterized by a smooth bifid flow curve. The firstpeak starts with the opening of the mitral valve andcorresponds to rapid ventricular filling during the firstthird of diastole. The second peak is of smalleramplitude, occurs in the last third of diastole at thetime of the A wave of the mitral valve leaflets and cor-responds to the atrial contraction wave. Pattern I,observed in mild mitral stenosis, also has a bifid flowbut differs from the normal flow pattern because thelate diastolic peak is higher in amplitude than the first
382 CIRCULATION
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
DOPPLER ECHOC IN MITRAL STENOSIS/Thuillez et al.
v-.-.-4-
4. 4-.-.
-I?.A-- 1
FIGURE 1. Doppler mitral valve flowpatterns in sinus rhythm. The normal flowobserved in sinus rhythm is illustrated in theleft upper panel (0). It is smooth andbiphasic. The initial peak occurs during thefirst third of diastole. The second peak issmaller and coincides with atrial contrac-tion. Pattern I, in the right upper panel, isobserved in mild mitral stenosis and ischaracterized by a biphasic flow whichdiffers from the normal flow (0) by thepresence of small indentations correspond-ing to flow turbulence and by a relative in-crease in the late diastolic peak, whichbecomes taller than the early diastolic wave.Pattern II, in moderate stenosis, is also tur-bulent and is characterized by a monophasicflow curve peaking in mid- or late diastole.It appears irregular and dome-shaped.Pattern III, observed in severe stenosis, isvery turbulent, with a slow, steadily ascend-ing flow; at end-diastole, a sharp descentoccurs. V = velocity; 0 = zero flow, elec-
EGG~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
II
peak. Pattern II, in moderate mitral stenosis, is tur-bulent and characterized by a monophasic flow curvepeaking in mid or late diastole. It is irregular anddome-shaped in appearance. Pattern III, observed insevere stenosis, is very turbulent with a slow, steadilyascending flow. At end-diastole, at the time of theQRS complex, a sharp descent occurs.
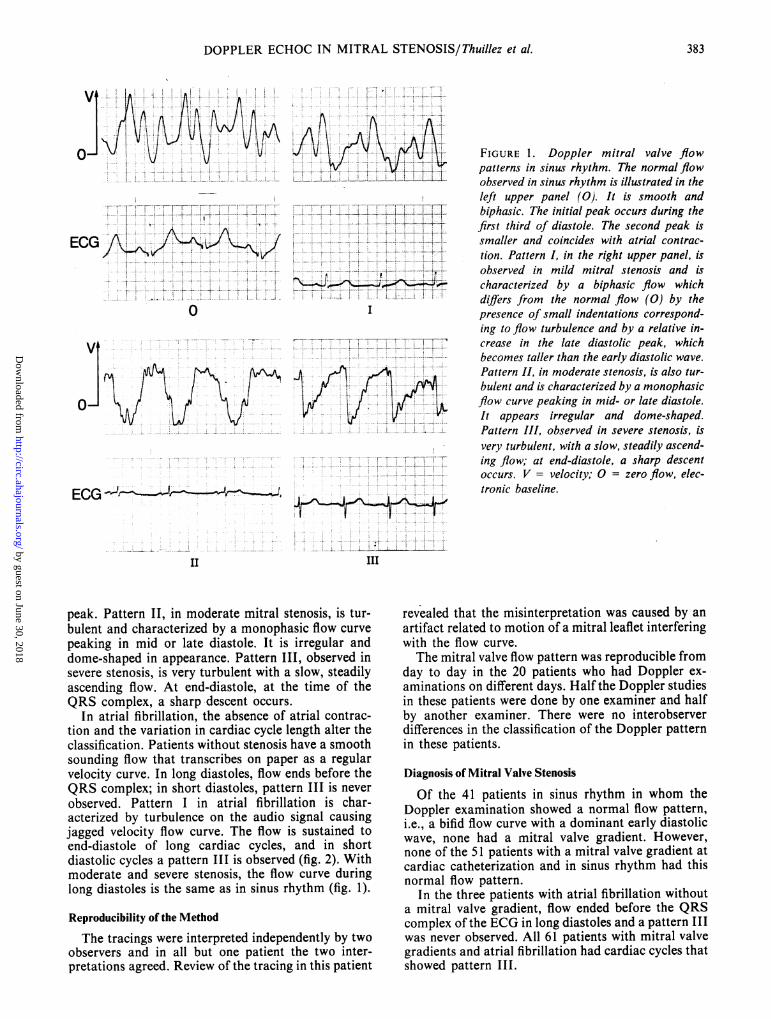
In atrial fibrillation, the absence of atrial contrac-tion and the variation in cardiac cycle length alter theclassification. Patients without stenosis have a smoothsounding flow that transcribes on paper as a regularvelocity curve. In long diastoles, flow ends before theQRS complex; in short diastoles, pattern III is neverobserved. Pattern I in atrial fibrillation is char-acterized by turbulence on the audio signal causingjagged velocity flow curve. The flow is sustained toend-diastole of long cardiac cycles, and in shortdiastolic cycles a pattern III is observed (fig. 2). Withmoderate and severe stenosis, the flow curve duringlong diastoles is the same as in sinus rhythm (fig. 1).
Reproducibility of the Method
The tracings were interpreted independently by twoobservers and in all but one patient the two inter-pretations agreed. Review of the tracing in this patient
tronic baseline.
III
revealed that the misinterpretation was caused by anartifact related to motion of a mitral leaflet interferingwith the flow curve.The mitral valve flow pattern was reproducible from
day to day in the 20 patients who had Doppler ex-aminations on different days. Half the Doppler studiesin these patients were done by one examiner and halfby another examiner. There were no interobserverdifferences in the classification of the Doppler patternin these patients.
Diagnosis of Mitral Valve Stenosis
Of the 41 patients in sinus rhythm in whom theDoppler examination showed a normal flow pattern,i.e., a bifid flow curve with a dominant early diastolicwave, none had a mitral valve gradient. However,none of the 51 patients with a mitral valve gradient atcardiac catheterization and in sinus rhythm had thisnormal flow pattern.
In the three patients with atrial fibrillation withouta mitral valve gradient, flow ended before the QRScomplex of the ECG in long diastoles and a pattern IIIwas never observed. All 61 patients with mitral valvegradients and atrial fibrillation had cardiac cycles thatshowed pattern III.
0* * . . t *- _j -n _ oI. ... +... .. . .. ... . . . w ... ..
A:0:: :::/:1'-0::0:<::::'::::.:':wt / J 1 wVb '; ,; ,,- iV-W-,08 +-SvT - - 1 - T ' 2 --- - ---i-_ S _ + _s +__ 4 i* - f i- l,, . , , : S , . .... .. _ i .= + . ...... v 1 ___ _ .:, f t I + _+ .
383
...... by guest on June 30, 2018
http://circ.ahajournals.org/D
ownloaded from
VOL 61, No 2, FEBRUARY 1980
v t
FIGURE 2. Mitral valveflowpattern in thepresence ofatrialfibrillation and mild mitralstenosis. Pattern III is observed after a shortcardiac cycle (fifth RR interval), and duringlong cardiac cycles (third RR interval) flowends at end-diastole or earlier. This patternis characteristic of mild stenosis in atrialfibrillation. With no stenosis, flow endsbefore end-diastole of the long cardiac cycleand a pattern III is not observed in shortdiastolic cycles. Patterns II and III are thesame as in sinus rhythm (fig. 1). V =velocity; 0 zeroflow, electronic baseline.
Assessment of the Severity of the Mitral Stenosis
Figures 3 and 4 illustrate the correlation betweenthe Doppler flow pattern and the hemodynamic data.
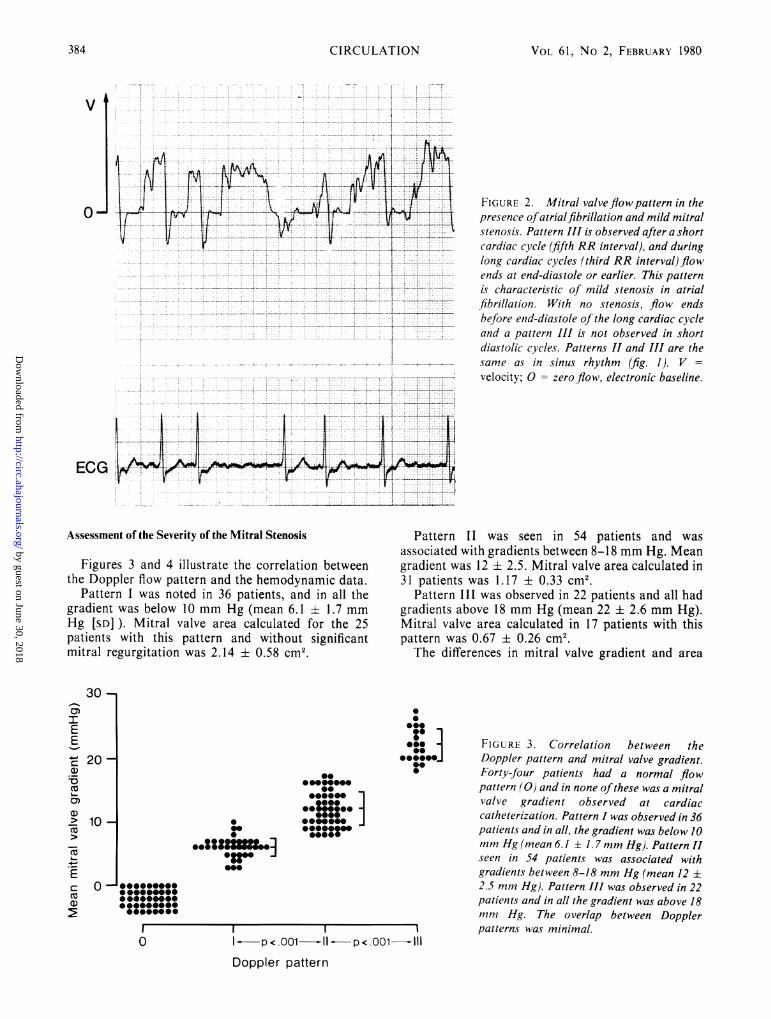
Pattern I was noted in 36 patients, and in all thegradient was below 10 mm Hg (mean 6.1 ± 1.7 mmHg [SD] ). Mitral valve area calculated for the 25patients with this pattern and without significantmitral regurgitation was 2.14 ± 0.58 cm2.
Pattern II was seen in 54 patients and wasassociated with gradients between 8-18 mm Hg. Meangradient was 12 ± 2.5. Mitral valve area calculated in31 patients was 1.17 ± 0.33 cm2.
Pattern III was observed in 22 patients and all hadgradients above 18 mm Hg (mean 22 ± 2.6 mm Hg).Mitral valve area calculated in 17 patients with thispattern was 0.67 ± 0.26 cm2.The differences in mitral valve gradient and area
0*@0
*e@e~~000000
@00~~~0*0 ****r0 *::::..sssr
0
0@
00
..P.*-i-
opp< p001a-11--p<eoorn- Il
Doppler pattern
FIGURE 3. Correlation between theDoppler pattern and mitral valve gradient.Forty-four patients had a normal flowpattern (0) and in none ofthese was a mitralvalve gradient observed at cardiaccatheterization. Pattern I was observed in 36patients and in all, the gradient was below 10mm Hg (mean 6.1 ± 1.7 mm Hg). Pattern IIseen in 54 patients was associated withgradients between 8-18 mm Hg (mean 12 ±2.5 mm Hg). Pattern III was observed in 22patients and in all the gradient was above 18mm Hg. The overlap between Dopplerpatterns was minimal.
0-
ECG
30 -cr)IEE
c 20-
(U
0)a)> 10-
Ecam)
000000000
@0000..00000"00@0000"00
0
o ...._.._^... s _^ . _ ._..._...._ _'' -.-' -. ^'-- X-'' ' T--2
384 CIRCULATION
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
DOPPLER ECHOC IN MITRAL STENOSIS/Thuillez et al.
pressure recordings went from a Doppler pattern IIduring long cardiac cycles, with a hemodynamicgradient of 13 mm Hg, to a pattern III during shortcardiac cycles, with a gradient of 19 mm Hg. Thepresence of mitral regurgitation did not change therelation between the Doppler pattern and thegradients, which were, respectively, 6.4 ± 1.7, 12.5 ±3.7 and 21.4 ± 2.8 mm Hg with patterns I, II and III.The correlation was also unaffected in the 32 patientswith coexisting aortic valve disease. Mean gradientswere, respectively, 6.2 ± 2.4, 12.5 ± 2.6 and 22.7 ±2.5 mm Hg. These values were not significantlydifferent from those in patients with isolated mitralstenosis (table 1).
Application to the Carpentier-Edwards Porcine Xenograft
Twelve patients in this study had had mitral valvereplacement by a Carpentier-Edwards prosthesis. Sixwere in atrial fibrillation and six in sinus rhythm. Allhad pattern I and all gradients were 4.5-8 mm Hg(mean 5.2 ± 1.6 mm Hg).
I - -P< .001 -11 --p<I.001111Doppler pattern
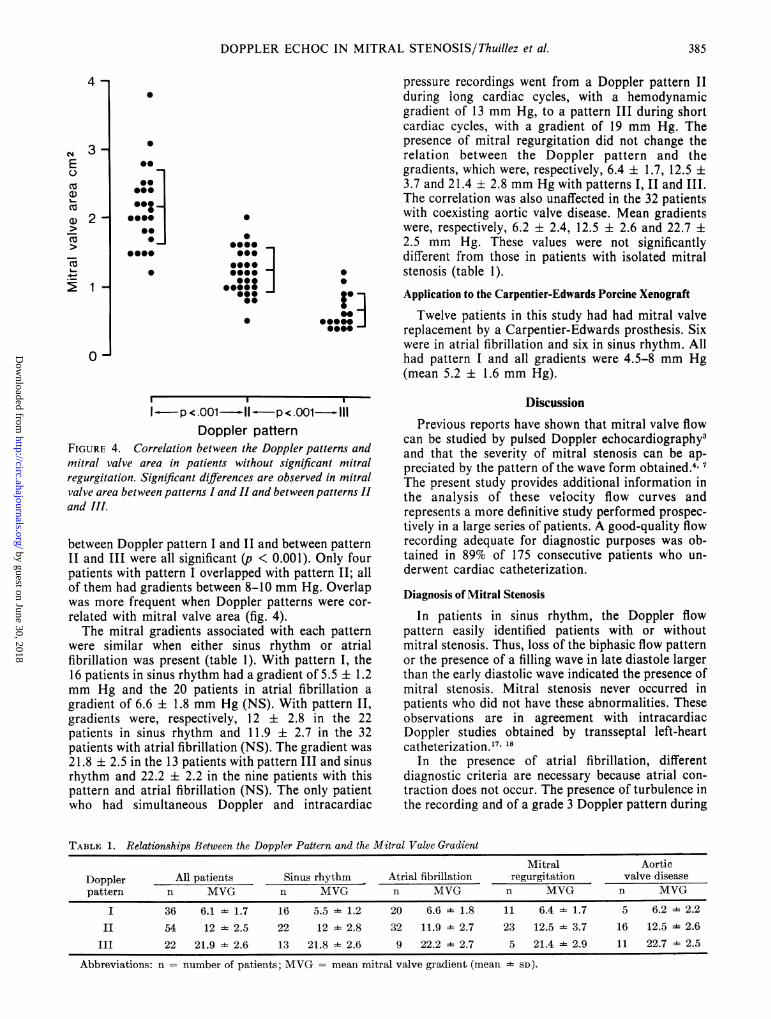
FIGURE 4. Correlation between the Doppler patterns andmitral valve area in patients without significant mitralregurgitation. Significant differences are observed in mitralvalve area between patterns I and II and between patterns IIand lII.
between Doppler pattern I and II and between patternII and III were all significant (p < 0.001). Only fourpatients with pattern I overlapped with pattern II; allof them had gradients between 8-10 mm Hg. Overlapwas more frequent when Doppler patterns were cor-related with mitral valve area (fig. 4).The mitral gradients associated with each pattern
were similar when either sinus rhythm or atrialfibrillation was present (table 1). With pattern I, the16 patients in sinus rhythm had a gradient of 5.5 ± 1.2mm Hg and the 20 patients in atrial fibrillation agradient of 6.6 ± 1.8 mm Hg (NS). With pattern II,gradients were, respectively, 12 ± 2.8 in the 22patients in sinus rhythm and 11.9 + 2.7 in the 32patients with atrial fibrillation (NS). The gradient was21.8 ± 2.5 in the 13 patients with pattern III and sinusrhythm and 22.2 ± 2.2 in the nine patients with thispattern and atrial fibrillation (NS). The only patientwho had simultaneous Doppler and intracardiac
DiscussionPrevious reports have shown that mitral valve flow
can be studied by pulsed Doppler echocardiography3and that the severity of mitral stenosis can be ap-preciated by the pattern of the wave form obtained.'The present study provides additional information inthe analysis of these velocity flow curves andrepresents a more definitive study performed prospec-tively in a large series of patients. A good-quality flowrecording adequate for diagnostic purposes was ob-tained in 89% of 175 consecutive patients who un-derwent cardiac catheterization.
Diagnosis of Mitral Stenosis
In patients in sinus rhythm, the Doppler flowpattern easily identified patients with or withoutmitral stenosis. Thus, loss of the biphasic flow patternor the presence of a filling wave in late diastole largerthan the early diastolic wave indicated the presence ofmitral stenosis. Mitral stenosis never occurred inpatients who did not have these abnormalities. Theseobservations are in agreement with intracardiacDoppler studies obtained by transseptal left-heartcatheterization.'7' 18
In the presence of atrial fibrillation, differentdiagnostic criteria are necessary because atrial con-traction does not occur. The presence of turbulence inthe recording and of a grade 3 Doppler pattern during
TABLE 1. Relationships Between the Doppler Pattern and the Mitral Valve Gradient
Mitral AorticDoppler All patients Sinus rhythm Atrial fibrillation regurgitation valve diseasepattern n MVG n MVG n MVG n MVG n MVG
I 36 6.1 - 1.7 16 5.5 1.2 20 6.6 ==1.8 11 6.4 1.7 5 6.2 2.2
II 54 12 2.5 22 12 * 2.8 32 11.9 2.7 23 12.5 3.7 16 12.5 2.6
III 22 21.9 - 2.6 13 21.8 * 2.6 9 22.2 - 2.7 5 21.4 - 2.9 11 22.7 - 2.5
Abbreviations: n = number of patients; MVG = meani mitral valve gradient (mean - SD).
4 -
cm 3EU
CO
m 2-
2 1
0@]
.0I
@0@
0
*-@000 I
0@00
SS
S..
385
o _
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL 61, No 2, FEBRUARY 1980
short diastoles or after several short cardiac cycles wasindicative of mitral stenosis. Pattern III was not foundwith atrial fibrillation in the absence of a mitralgradient. The behavior of Doppler flow curves in atrialfibrillation is consistent with the hemodynamic obser-vation in mitral stenosis that the mitral valve gradientincreases with shorter diastolic filling periods.
Using the above criteria, all patients with mitralstenosis were detected and all patients without stenosiswere correctly identified even when associated mitralregurgitation or aortic valvular disease was present.These criteria might have been less specific if a largenumber of patients with a wide spectrum of heart dis-ease had been studied; however, none of the 34patients with other types of heart disease or the 10normals studied were misdiagnosed. In addition, all ofthe data acquired by Doppler echocardiography werenot used in this study. We did not use the audiblesignal of the Doppler shift of frequency and based ourdiagnosis only on the recorded signal, which omitsmuch of the data in the audio signal. Turbulence withmitral stenosis is well perceived by the ear as high-frequency sounds and spectral analysis of the audiosignal using a rapid Fourier transformation could im-prove the diagnostic capabilities of Doppler echocar-diography.
Assessment of Severity of Mitral Stenosis
The study of flow patterns provided an accurate,semiquantitative assessment of the severity of mitralstenosis. The overlap in gradient among the threepatterns observed was always between 8-10 mm Hgand thus did not appear important enough to impairthe clinical utility of the test.The correlation between Doppler patterns was
better with mitral valve gradient than with mitralvalve area. This is expected since flow velocity (V) ismore directly related to gradient (MVG) than to area(MVA) according to the formulas V = MVF/MVA,MVA = MVF/VMVG,"5 and V = VMVG With asteady flow through an orifice Torricelli's law predictsthat the pressure gradient is closely related to thevelocity through the orifice when the Reynoldsnumber is large enough and the viscous losses ofenergy negligible compared with the losses of kyneticenergy: /P = 1/2 e V2 max'9 (AP = pressure gradient,= mass density of fluid and V max = maximum fluid
velocity). Holen et al.5 20 and Hatle et al.6 used theDoppler shift to calculate the maximum velocity of themitral flow and showed that indeed this parametercorrelated very well with pressure drop through thestenotic mitral valve.Heart rate influences mitral valve gradient because
tachycardia shortens filling time, compromising ven-tricular flow across the mitral valve. Atrial fibrillationallows study of the dynamic beat-to-beat variation inmean gradient and in Doppler pattern. Thus, theDoppler pattern changes to a higher grade when shortcardiac cycles are selected. This was clearly evident inthe one patient that had Doppler recordings at thetime of cardiac catheterization.
The Doppler flow patterns observed in this studycan be related directly to the hemodynamic abnor-malities that occur in mitral stenosis. Thus, in mildstenosis initial filling of the left ventricle is reducedand left atrial volume is increased. Since the force ofcontraction of the left atrium is related to left atrialpressure at the onset of contraction,21 this will lead toan increased driving pressure during atrial systole, andthus an increased blood flow velocity. Therefore, theDoppler study will show a relatively tall end-diastolicwave in sinus rhythm, indicating that mitral bloodflow velocity is higher during atrial contraction thanduring passive left ventricular filling.With more severe degrees of stenosis, the velocity
flow curve is monophasic, dome-shaped in moderatestenosis, and ascending throughout diastole in severestenosis. In the presence of an anatomic obstruction,the rate of flow is reduced and thus volume accelera-tion of blood flow through the mitral valve is expectedto be slow. If the gradient is sustained, accelerationwill also be sustained to end-diastole. Accelerationvaries inversely with the degree of stenosis and can beappreciated as the slope of the Doppler flow curve.Thus, the characteristics of the flow patterns observedin this study can be explained by known hemodynamicprinciples.
Significant mitral regurgitation does not affect thepredictive value of the Doppler pattern. Similarly, thepresence of aortic stenosis or regurgitation did not in-fluence the relation between the Doppler pattern andmitral valve gradient. This represents an advantage ofthe Doppler approach compared with standardechocardiography for the noninvasive evaluation ofmitral stenosis.
Doppler echocardiography may also be superior tostandard echocardiography in patients with mitralbioprostheses. The Doppler echocardiographic studyis facilitated in these patients by the echo-producingstents of the valve; however, quality decreases becauseof difficulty in eliminating valvular noises. The role ofDoppler echocardiography in patients with prostheticmitral valves must be evaluated in a larger series ofpatients, including those with valvular dysfunction.
AcknowledgmentsThe technical assistance of Michel Xhaard and Jean-Pierre Four-
nier and the secretarial work of Diane Roy and Luce Begin aregratefully acknowledged.
References1. Edler I: Ultrasound cardiogram in mitral valvular disease. Acta
Chir Scand 3: 230, 19562. Henry WL, Griffith JM, Michaelis LL, McIntosh CL, Morrow
AG, Epstein SE: Measurement of mitral orifice area in patientswith mitral valve disease by real-time, two-dimensionalechocardiography. Circulation 51: 827, 1975
3. Johnson SL, Baker DW, Lute RA, Dodge HT: Dopplerechocardiography. The localization of cardiac murmurs. Cir-culation 48: 810, 1973
4. Kalmanson D, Veyrat C, Bouchareine F, Degroote A: Non-invasive recording of mitral valve flow velocity patterns usingpulsed Doppler echocardiography. Br Heart J 39: 517, 1977
5. Holen J, Aaslid R, Landmark K, Simonsen S: Determination
386 CIRCULATION
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from

DOPPLER ECHOC IN MITRAL STENOSIS/Thuillez et al.
of pressure gradient in mitral stenosis with a non-invasive ul-trasound Doppler technique. Acta Med Scand 199: 455, 1976
6. Hatle L, Brubakk A, Tromsdal A, Angelsen B: Noninvasiveassessment of pressure drop in mitral stenosis by Doppler ul-trasound. Br Heart J 40: 131, 1978
7. Diebold B, Theroux P, Bourassa MG, Thuillez C, Peronneau P,Guermonprez JL, Xhaard M, Waters DD: Noninvasive pulsedDoppler study of mitral stenosis and mitral regurgitation. Apreliminary study. Br Heart J 42: 168, 1979
8. Cope GD, Kisslo JA, Johnson ML, Behar VS: A reassessmentof the echocardiogram in mitral stenosis. Circulation 52: 664,1975
9. Martin RP, Rakowski H, Kleiman JH, Beaver W, London E,Popp RL: Reliability and reproducibility of two dimensionalechocardiographic measurement of the stenotic mitral valveorifice area. Am J Cardiol 43: 560, 1979
10. Peronneau P, L6ger F: Doppler ultrasonic pulsed bloodflowmeter. In Proceedings of the 8th International Conferenceon Medicine and Biochemical Engineering, IEEE Editions,Chicago, 1969, p 10
11. Baker DW: Pulsed ultrasonic Doppler flow sensing. In IEEETrans Sonic Ultrason SU-17 3: 170, 1970
12. Baker DW, Rubenstein SA, Lorch GS: Pulsed Dopplerechocardiography: principles and applications. Am J Med 63:69, 1977
13. Lorch G, Rubenstein S, Baker D, Dooley T, Dodge H: Dopplerechocardiography. Use of a graphical display system. Circula-tion 56: 576, 1977
14. Diebold B, Theroux P, Bourassa MG, Ptronneau P, Guermon-prez JL: Noninvasive assessment of aortocoronary bypass graftpatency using pulsed Doppler echocardiography. Am J Cardiol43: 10, 1979
15. Gorlin R, Gorlin SG: Hydraulic formula for calculation of thearea of the stenotic mitral valve, other cardiac valves, and cen-tral circulatory shunts. Am Heart J 41: 1, 1951
16. Wexler L, Silverman JF, DeBusk RF, Harrison DC:Angiographic features of rheumatic and nonrheumatic mitralregurgitation. Circulation 44: 1080, 1971
17. Kalmanson D, Bernier A, Veyrat C, Witchitz S, Savier CH,Chiche P: Normal pattern and physiological significance ofmitral valve flow velocity recording using transseptal direc-tional Doppler ultrasound catheterization. Br Heart J 37: 249,1975
18. Kalmanson D, Veyrat C, Bernier A, Savier CH, Chiche P,Witchitz S: Diagnosis and evaluation of mitral valve diseaseusing transseptal Doppler ultrasound catheterization. Br HeartJ 37: 257, 1975
19. Streeter VL: Handbook of Fluid Dynamics. New York,McGraw-Hill, 1961, p 3
20. Holen J, Rune A, Landmark K, Simonsen S, Ostrem T: Deter-mination of effective orifice area in mitral stenosis from nonin-vasive ultrasound Doppler data and mitral flow rate. Acta MedScand 201: 83, 1977
21. Braunwald E, Fahm CJ: Studies on Starling's law of the heart.IV. Observations on the hemodynamic function of the leftatrium in man. Circulation 24: 633, 1961
387
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from

Diebold, D D Waters and P MauriceC Thuillez, P Théroux, M G Bourassa, D Blanchard, P Péronneau, J L Guermonprez, B
Pulsed doppler echocardiographic study of mitral stenosis.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1980 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.61.2.381
1980;61:381-387Circulation.
http://circ.ahajournals.org/content/61/2/381.citationthe World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from


















