Early Versus Delayed Cholecystectomy for Acute Calculous Cholecystitis
181
Early Versus Delayed Cholecystectomy for Acute Calculous Cholecystitis by Charles William Armand de Mestral A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy Graduate Department of the Institute of Medical Science University of Toronto © Copyright by Charles William Armand de Mestral 2013
Transcript of Early Versus Delayed Cholecystectomy for Acute Calculous Cholecystitis
Early Versus Delayed Cholecystectomy for Acute Calculous Cholecystitis
by
Charles William Armand de Mestral
A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy Graduate Department of the Institute of Medical Science
University of Toronto
© Copyright by Charles William Armand de Mestral 2013

ii
Early Versus Delayed Cholecystectomy for
Acute Calculous Cholecystitis
Charles de Mestral
Doctor of Philosophy
The Institute of Medical Science University of Toronto
2013
ABSTRACT
Introduction: Despite evidence in favour of cholecystectomy early during first presenting
admission for most patients with acute calculous cholecystitis, variation in the timing of
cholecystectomy remains evident worldwide. This dissertation characterizes the extent of
variation within a large regional healthcare system, as well as addresses gaps in our current
understanding of the clinical consequences and costs associated with early versus delayed
cholecystectomy for acute cholecystitis.
Methods: A population-based retrospective cohort of patients admitted emergently with acute
cholecystitis was identified from administrative databases for the province of Ontario, Canada.
First, the extent of variation across hospitals in the performance of early cholecystectomy (within
7 days of emergency department presentation) was characterized. Second, among patients
discharged without cholecystectomy following index admission, the risk of recurrent gallstone
symptoms over time was quantified. Third, operative outcomes of early cholecystectomy were
compared to those of delayed cholecystectomy. Finally, a cost-utility analysis compared
healthcare costs and quality-adjusted life-year gains associated with three management strategies

iii
for acute cholecystitis: early cholecystectomy, delayed cholecystectomy and watchful waiting,
where cholecystectomy is performed urgently if recurrent gallstone symptoms arise.
Results: The rate of early cholecystectomy varied widely across hospitals in Ontario (median
rate 51%, interquartile range 25-71%), even after adjusting for patient characteristics (median
odds ratio 3.7). Among patients discharged without cholecystectomy following an index
cholecystitis admission, the probability of a gallstone-related emergency department visit or
hospital admission was 19% by 12 weeks following discharge. Early cholecystectomy was
associated with a lower risk of major bile duct injury (0.28% vs. 0.53%, RR=0.53, 95% CI 0.31–
0.90, p=0.025). No significant differences were observed in terms of open cholecystectomy (15%
vs. 14%, RR=1.07, 95% CI 0.99–1.16, p=0.10) or in conversion among laparoscopic cases (11%
vs. 10%, RR=1.02, 95% CI 0.93–1.13, p=0.68). Early cholecystectomy was on average less
costly ($6,905 per person) and more effective (4.20 QALYs per person) than delayed
cholecystectomy ($8,511; 4.18 QALYs per person) or watchful waiting ($7,274; 3.99 QALYs
per person).
Conclusions: Early cholecystectomy offers a benefit over delayed cholecystectomy in terms of
major bile duct injury, mitigates the risk of recurrent symptoms, and is associated with the
greatest QALY gains at the least cost.
iv
Acknowledgments
I wish to thank the following people and organizations who generously provided invaluable
support for my thesis work:
My supervisor Dr. Avery Nathens, for consistently using his experience, enthusiasm and
resources to support my success over the last 3 years.
My thesis committee members, Dr. Jeffrey Hoch, Dr. Andreas Laupacis and Dr. Ori Rotstein, for
their steadfast support and sound advice.
Brandon Zagorksi, for helping me navigate the complexities of accessing and analyzing ICES
data.
My fellow graduate students Barbara Haas, David Gomez, Marvin Hsiao, Sunjay Sharma, Aziz
Alali, Chethan Sathya and Debbie Li as well as our lab’s research manager Jennifer Bridge, for
the insightful input on my work and for creating a great work environment.
Harindra Wijeysundera and Murray Krahn, for their help with my Markov model.
The University of Toronto Department of Surgery, Division of General Surgery, Dr. George
Hiraki and the Clinician Investigator Program, for supporting my training in the Surgeon-
Scientist Training Program.
The Canadian Association of General Surgeons, Physician Services Inc. Foundation and the
Institute for Clinical Evaluative Sciences for financially supporting this thesis work.
v
Funding
This graduate work was financially supported by an Ontario Doctoral Award, the Chikai
and Sawa Hiraki Surgeon-Scientist fellowship, a Clinician-Investigator Program Award from the
Ontario Ministry of Health as well as funds from the Division of General Surgery and
Department of Surgery of the University of Toronto.
Operating costs were covered by a grant from the Canadian Surgical Research Fund and a
Resident Research Grant from Physician Services Inc. Foundation. In addition, this work was
supported by the Institute for Clinical Evaluative Sciences, which is funded by an annual grant
from the Ontario Ministry of Health and Long-Term Care. The opinions, results and conclusions
reported in this thesis are those of the author and are independent from the funding sources. No
endorsement by the Canadian Institutes of Health Research, the Institute for Clinical Evaluative
Sciences or the Ontario Ministry of Health and Long-Term Care is intended or should be
inferred.
The author has no other financial disclosures or any conflict of interest to declare.
vi
Table of Contents
Abstract ............................................................................................................................................ ii
Acknowledgments........................................................................................................................... iv
Funding ............................................................................................................................................ v
Table of Contents ............................................................................................................................ vi
List of Tables ................................................................................................................................... x
List of Figures ................................................................................................................................ xii
List of Abbreviations .....................................................................................................................xiii
Chapter 1 - Thesis Overview, Hypotheses and Specific Aims ........................................................1
1.1 Thesis Overview ..................................................................................................................2
1.2 Rationale ..............................................................................................................................2
1.3 Hypotheses ...........................................................................................................................3
1.4 Research Aims .....................................................................................................................4
1.4 Contributions........................................................................................................................5
Chapter 2 - Background ...................................................................................................................6
2.1 Epidemiology of Gallstone Disease and Acute Cholecystitis..............................................7
2.2 Pathogensis of Gallstones and Acute Calculous Cholecystitis ............................................8
2.3 Diagnosis and Severity.......................................................................................................10
2.4 Surgical Management of Acute Cholecystitis....................................................................11
2.4.1 Rationale for Surgical Management of Acute Cholecystitis..................................11
2.4.2 Surgical Approach..................................................................................................12
2.4.3 Complications of Cholecystectomy .......................................................................13
2.4.4 Laparoscopic Cholecystectomy in the Setting of Acute Cholecystitis ..................15
2.4.5 Timing of Cholecystectomyfor Acute Cholecystitis..............................................16
vii
2.4.6 Timing of Cholecystectomy and Clinical Outcomes...........................................17
2.4.7 Timing of Cholecystectomy and Economic Outcomes .........................................18
2.5 Management Guidelines for Acute Cholecystitis ..............................................................20
2.6 Variation in Practice Worldwide........................................................................................21
2.7 Summary of Gaps in Current Knowledge..........................................................................22
2.7 Tables for Chapter 2...........................................................................................................24
2.8 Figures for Chapter 2 .........................................................................................................27
Chapter 3 - General Methods .........................................................................................................29
3.1 Strengths of Ontario's Administrative Health Data ...........................................................30
3.2 Description of Data Sources ..............................................................................................31
3.3 Data Validity ......................................................................................................................33
3.4 Approach to Costing with Ontario's Administrative Data .................................................35
3.5 Analytic Considerations .....................................................................................................36
Chapter 4 - Variation in Early Cholecystectomy for Acute Cholecystitis in Ontario ...................42
4.1 Summary ............................................................................................................................43
4.2 Background ........................................................................................................................44
4.3 Methods..............................................................................................................................45
4.4 Results ................................................................................................................................50
4.5 Discussion ..........................................................................................................................52
4.6 Tables for Chapter 4...........................................................................................................56
4.7 Figures for Chapter 4 .........................................................................................................59
Chapter 5 - The Risk of Recurrent Symptoms if Cholecystectomy is Delayed .............................62
5.1 Summary ............................................................................................................................63
5.2 Background ........................................................................................................................64
5.3 Methods..............................................................................................................................65
5.4 Results ................................................................................................................................68
viii
5.5 Discussion ..........................................................................................................................70
5.6 Tables for Chapter 4...........................................................................................................73
5.7 Figures for Chapter 4 .........................................................................................................77
Chapter 6 - Comparative Operative Outcomes of Early and Delayed Cholecystectomy ..............78
6.1 Summary ............................................................................................................................79
6.2 Background ........................................................................................................................80
6.3 Methods..............................................................................................................................82
6.4 Results ................................................................................................................................87
6.5 Discussion ..........................................................................................................................89
6.6 Tables for Chapter 4...........................................................................................................93
6.7 Figures for Chapter 4 .......................................................................................................100
Chapter 7 - Cost-utility Analysis of Alternative Timeframes of Cholecystectomy for Acute Cholecystitis ............................................................................................................................101
7.1 Summary ..........................................................................................................................102
7.2 Background ......................................................................................................................103
7.3 Methods............................................................................................................................104
7.4 Results ..............................................................................................................................112
7.5 Discussion ........................................................................................................................114
7.6 Tables for Chapter 7.........................................................................................................117
7.7 Figures for Chapter 7 .......................................................................................................120
7.8 Supplemental data for Chapter 7......................................................................................128
Chapter 8 - General Discussion ...................................................................................................136
8.1 Thesis summary ...............................................................................................................137
8.2 Implications......................................................................................................................139
8.3 Thesis Limitations............................................................................................................141
Chapter 9 - Future Directions.......................................................................................................144
ix
9.1 Understanding the Context-Specific Determinants of Management ...............................145
9.2 Knowledge Translation Plan ............................................................................................146
9.3 Ongoing Evaluation of Patient Outcomes and Preference...............................................147
References ....................................................................................................................................149
x
List of Tables
Table 2.1 - Acute cholecystitis severity classification from the Tokyo Guidelines......................24
Table 2.2 . Major sources of morbidity and resource utilization to consider when comparing
early to delayed cholecystectomy………………………………………………………………..25
Table 2.3 - Summary of randomized controlled trials comparing early to delayed
cholecystectomy for acute cholecystitis……………………………………………………….....26
Table 4.1 - Distribution of patient characteristics……………………………………………….56
Table 4.2 - Distribution of hospital characteristics……………………………………………...57
Table 4.3 - Multilevel multivariable logistic regression results showing association of patient and
hospital characteristics with early cholecystectomy ………………………………………….....58
Table 5.1 - Probability of a gallstone-related event by time from discharge……………………73
Table 5.2 - Multivariable time to event analysis showing adjusted risk of gallstone-related event
across patient characteristics………………………………….………………………………….74
Table 5.3 - Probability of a gallstone-related event by time from discharge in competing risk
time-to-event analysis……………………………………………………………………………75
Table 5.4- Probability of a gallstone-related event by 12 weeks across age groups in competing
risk time-to-event analysis ………………………………………………………………………76
Table 6.1 - Baseline characteristics of patients and their surgeon before matching…………….93
Table 6.2 - Baseline characteristics of patients and their surgeon after matching………………94
Table 6.3 - Outcome frequency and relative risk before and after matching ……………….......95
Table 6.4 - Baseline characteristics of patients and their surgeon in synthetic cohort after
weighting on the inverse probability of treatment received………………………………...........96
Table 6.5 - Relative risk of outcome after weighting on inverse probability of treatment……...97
xi
Table 6.6 - Relative risk of outcomes when defining early cholecystectomy as occurring within 3
days of emergency department presentation……………………………………………………..98
Table 6.7 - Relative risk of outcome when excluding delayed cholecystectomy later than 1 year
after discharge……………………………………………………………………………………99
Table 7.1 - Model parameter inputs with sources and threshold analysis results……………...117
Table 7.2 - Average costs and quality-adjusted life-year gains and associated increments..…..119
Table 7.S1 - Baseline characteristics of patients and their surgeon before matching………….130
Table 7.S2 - Baseline characteristics of patients and their surgeon after matching……………131
Table 7.S3 - Baseline characteristics of patients before matching……………………………..132
Table 7.S4 - Baseline characteristics of patients after matching……………………………….133
xii
List of Figures
Figure 2.1 - Depiction of anatomy of gallbladder, cystic duct and common bile duct………….27
Figure 2.2 - Depiction of laparoscopic and open cholecystectomy………………….………….28
Figure 4.1 - Patient eligibility flowchart………………………………………………………...59
Figure 4.3 - Variation in the rate of early cholecystectomy across hospitals (N=24,437 patients,
106 hospitals)…………………………………………………………………………………….60
Figure 4.4 - Variation in the rate of early cholecystectomy rate across hospitals among young
(<50 years) healthy patients without concurrent biliary tract obstruction or pancreatitis (N=2,894
patients, 102 hospitals)…………………………………………………………………………...61
Figure 5.1 - Unadjusted probability of a gallstone-related event across age groups in the first
year following discharge…………………………………………………………………….…...77
Figure 6.1 - Patient eligibility flowchart……………………………………………………….100
Figure 7.1 - Simplified representation of model state transition diagram……………………...120
Figure 7.2 - Cost-effectiveness plane of Monte-Carlo probabilistic analysis results (10,000
iterations)……………………………………………………………………………………….122
Figure 7.3 - Incremental cost-effectiveness plane comparing early to delayed
cholecystectomy………………………………………………………………………………...124
Figure 7.4 - Cost-effectiveness acceptability curve derived from Monte-Carlo probabilistic
sensitivity analysis……………………………………………………………………………...126
Figure 7.S1 - Example of two-way sensitivity analysis results …………………………….....134
xiii
List of Abbreviations
ADG - Aggregated Diagnosis Group
QALY - Quality-Adjusted Life-Year
CBD - Common Bile Duct
CI - Confidence Interval
CIHI - Canadian Institute for Health Information
CPWC - Cost Per Weighted Case
DAD - Discharge Abstract Database
ED - Emergency Department
ICES - Institute for Clinical Evaluative Sciences
IQR - Interquartile Range
ISPOR - International Society for Pharmacoeconomics and Outcomes Research
KM - Kaplan Meier
MOR - Median Odds Ratio
NACRS - National Ambulatory Care Reporting System
NMB - Net Monetary Benefit
OHIP - Ontario Health Insurance Plan

xiv
OR - Odds Ratio
PSA - Probabilistic Sensitivity Analysis
RIW - Resource Intensity Weight
RPDB - Registered Person Database
RR - Relative Risk
SD - Standard Deviation
SMDM - Society for Medical Decision Making
WTP - Willingness-To-Pay

1
Chapter 1
Thesis Overview, Hypotheses, and Specific Aims
The purpose of this chapter is to:
I. Provide an overview of the thesis structure
II. Describe the rationale for the thesis focus
III. Provide the research hypotheses
IV. List the overarching objective and specific aims
V. Detail all contributions to this thesis work
2
1.1 Thesis Overview
In Chapter 1, I outline the structure of this dissertation as well as present the rationale,
hypotheses and specific aims of the thesis. In Chapter 2, I detail the relevant epidemiology,
pathophysiology and severity classification of acute cholecystitis. I then review the rationale for
surgical management of acute cholecystitis as well as the historical and clinical context of the
controversy concerning the optimal timing of cholecystectomy for acute cholecystitis. Existing
evidence comparing the clinical and economic outcomes of early and delayed cholecystectomy
are then described followed by a description of practice worldwide. Chapter 3 is a discussion of
general methods applicable to all specific aims. First, details on the contents and validity of
administrative databases utilized are provided. Second, major analytic concepts relevant to each
specific aim are discussed. Chapters 4, 5, 6 and 7 reflect the four specific aims of this thesis in
manuscript format. The final two chapters summarize the thesis results, place the implications in
the context of general limitations, and proposes ideas for future directions.
Chapter 4 has been accepted for publication by the Canadian Medical Association Journal
Open and Chapter 5 has been published in the Journal of Trauma and Acute Care Surgery.
Chapter 6 is currently under review by Annals of Surgery.
1.2 Rationale
As detailed in Chapter 2, cholecystectomy early on first admission is recommended over
delayed elective cholecystectomy for most patients with acute cholecystitis, based on
randomized trials and meta-analyses. However, recent reports reveal inconsistency in following
3
this recommendation internationally, suggesting that the timing of cholecystectomy remains
controversial.
In order to generate local solutions for quality improvement, a setting-specific
understanding of the extent and potential underlying etiology for the inconsistent application of
early cholecystectomy is required. In addition, important limitations of current knowledge should
be addressed in order to better inform best practice with regards to the surgical care of acute
cholecystitis. In fact, randomized trials comparing early to delayed surgery suffer from limited
contemporary external validity and no study to date has been large enough to compare rare but
serious operative complications such as bile duct injury or death. Large population-based
analyses undertaken in this thesis offer the unique opportunity to address these limitations.
Finally, given the constrained nature of healthcare budgets, costs should be considered alongside
the clinical consequences of alternative management strategies being considered. Setting-specific
economic evaluations incorporating contemporary data will provide critical supplemental
evidence with which to inform decision making.
1.3 Hypotheses
We first hypothesize that there is considerable variation in the rate of early
cholecystectomy for acute cholecystitis across hospitals in Ontario. Second, we hypothesize that
early cholecystectomy is associated with similar operative outcomes as delayed cholecystectomy
but confers less morbidity by mitigating the risk of recurrent gallstone-related symptoms.
Finally, we hypothesize that in Ontario, early cholecystectomy is cost saving and is associated
with greater quality-adjusted life year gains compared to delayed laparoscopic cholecystectomy.
4
1.4 Research Aims
The overarching research objective of this thesis is to investigate the clinical outcomes
and costs associated with early and delayed cholecystectomy for acute cholecystitis, using a
population-based approach.
Given our overarching objective and hypotheses, this thesis is structured around the
following four specific aims:
Specific Aim #1: To characterize the extent and potential sources of variation in the
performance of early cholecystectomy for acute cholecystitis in Ontario.
Specific Aim #2: To determine the probability of gallstone-related complications in patients
discharged home without cholecystectomy on first admission.
Specific Aim #3: To compare the frequency of operative outcomes between early and
delayed cholecystectomy.
Specific Aim #4: To conduct an economic evaluation comparing different timeframes of
cholecystectomy for acute cholecystitis.
5
1.5 Contributions
My contributions
I was involved in every stage of this thesis work with the support and guidance of my
program advisory committee. I developed the specific research aims with my supervisor and
program advisory committee. I was responsible for creating the population-based cohorts with
assistance from an analyst at the Institute for Clinical Evaluative Sciences (ICES). Based on the
previous work and input of ICES scientists, I performed and take responsibility for all statistical
analyses and the accuracy of the reports. I created the Markov model used in the economic
evaluation with input from experts in medical decision modeling and my program advisory
committee members. I am the first author of all four manuscripts resulting from this thesis.
Specific contribution of others to each specific aim
Avery Nathens, Ori Rotstein, Andrea Laupacis, Jeffrey Hoch contributed to the design of
all four specific aims. Brandon Zagorski was involved in helping me create the cohorts for each
specific aim. Input on statistical analysis was provided by Barbara Haas (specific aim 1), David
Gomez (specific aim 1), Aziz Alali (specific aim 3), Jeffrey Hoch (specific aims 1,3,4), Brandon
Zagorki (specific aims 1,2,3) and Avery Nathens (all specific aims). Harindra Wijeysundera and
Murray Krahn provided input in the development of the Markov model for specific aim 4. All
co-authors provided critical revisions on manuscripts.
6
Chapter 2
Background
The purpose of this chapter is to:
I. Describe the epidemiology, pathogenesis and severity classification of acute cholecystitis
II. Review the role of surgery for acute cholecystitis
III. Review current knowledge with respect to the impact of timing of cholecystectomy on
clinical outcomes and healthcare costs.
IV. Describe the extent of variation in the timing of cholecystectomy worldwide.
V. Provide a summary of gaps in current knowledge

7
2.1 Epidemiology of gallstone disease and acute cholecystitis
Large screening ultrasound studies have shown that gallstones are present in 5% to 20%
of adults1-3. The prevalence ranges widely across ethnicities1,3 and is approximately twice as high
in women as in men 4-6. In addition to the important influence of ethnicity and sex on prevalence,
other non-modifiable risk factors for gallstones include older age, family history and genetic
predisposition2. Modifiable risk factors include obesity, rapid weight loss and a high calorie diet.
Furthermore, certain drugs (e.g. estrogen replacement therapy, thiazide diuretics) promote
gallstone formation2 whereas others such as statins, inhibitors of HMG-CoA reductase, have
been shown to reduce the risk of gallstone disease 7-9.
The previously mentioned risk factors are most applicable to the formation of cholesterol
gallstones, which account for 90% of gallstones in Western nations10. Pigment stones are more
common in eastern Asia and more frequently present as stones in the bile duct
(choledocholithiasis) as opposed to in the gallbladder (cholelithiasis)2,10. Pigment stones are
associated with states of increased bilirubin excretion (e.g. hemolysis, cirrhosis, bile salt
malabsorption) in the case of black pigment stones, or with biliary tract infection and
inflammation (cholangitis) in the case of brown pigment stones2,10.
The large majority of patients with gallstones will remain asymptomatic. However, 1% to
3% of patients per year will develop symptoms of gallstone disease11,12. Symptomatic gallstone
disease can present as biliary colic, a short-lived episode of right upper quadrant abdominal pain
due to temporary obstruction of outflow from the gallbladder by a gallstone. Acute cholecystitis
is a more severe manifestation of cholelithiasis and results from prolonged gallbladder outflow
obstruction giving rise to an inflammatory reaction described in the next section. Patients present

8
with pain of longer duration than biliary colic and with local and system signs of inflammation.
Stones can also escape the gallbladder into the biliary tract (choledocholithiasis) leading to
obstruction of the common bile duct with or without infection (cholangitis) or to an
inflammatory process in the pancreas (gallstone pancreatitis).
The incidence of acute cholecystitis decreased by 18% in Canada in the 1990s as elective
laparoscopic cholecystectomy was increasingly performed for symptomatic gallstones13.
However, acute cholecystitis remains prevalent and is in fact the most common reason for
hospitalization among all digestive diseases in the United States14.
Between 90% and 95% of cases of acute cholecystitis are due to gallstones, more
accurately referred to as acute calculous cholecystitis10,15. Gallbladder outflow obstruction may
however also occur due to malignancy, gallbladder polyps and parasites16. More commonly,
acalculous cholecystitis arises in association with predisposition to gallbladder ischemia or
instances of reduced gallbladder motility (e.g. critical illness, sepsis, burns, major surgery, total
parenteral nutrition)10,16. This thesis work focuses on the management of acute cholecystitis due
to gallstones.
2.2 Pathogenesis of gallstones and acute calculous cholecystitis
Gallstones form from the precipitation of bile solutes. Bile is produced in the liver by
hepatocytes and is stored in the gallbladder (Figure 2.1). After ingestion of a meal, neuro-
hormonal signals lead to contraction of the gallbladder and excretion of bile into the
gastrointestinal tract where it functions to facilitate the digestion of fats by emulsifying lipids
9
into micelles. In its role as a reservoir for bile, the gallbladder is the primary site of gallstone
formation.
The major solutes of bile include cholesterol, water-soluble bile salts and water-insoluble
phospholipids (lecithins)10. The formation of cholesterol gallstones is promoted by a number of
processes. First, cholesterol precipitates into crystals when its concentration in bile exceeds the
solubilizing capacity of bile salts and phospholipids. Bile stasis with gallbladder hypomotility
supports the nucleation of cholesterol crystals and mucous hypersecretion by the gallbladder
epithelium facilitates the formation of stones10,17,18.
Acute calculus cholecystitis develops as a result of gallstone obstruction of the cystic
duct leading to impaired bile outflow from the gallbladder and increased pressure within the
gallbladder. Gallbladder wall inflammation results from progressive mucosal ischemia
exacerbated by the release of inflammatory prostaglandins, leading to the compromise of the
glycoprotein mucous layer protecting the gallbladder epithelium10. While infection is not present
at the onset of acute cholecystitis, secondary superinfection is identified on biliary or gallbladder
cultures in 29% to 54% of cases of acute cholecystitis19. Gram negative organisms (E. coli,
Klebsiella spp., Pseudomonas spp., Enterobacter spp.) are most frequently involved as well as
anaerobes (Bacteroides, Clostridium) and gram positive cocci (Enterococcus, Streptococcus)
16,19.
Acute cholecystitis therefore includes a pathologic spectrum ranging from mild
inflammation with sterile bile to gangrenous cholecystitis with necrosis, empyema of the
gallbladder or emphysematous cholecystitis from gas-forming organisms. Untreated acute
cholecystitis can also progress to perforation of the gallbladder leading to bile peritonitis or a

10
pericholecystic abscess15. The formation of a biliary fistula between the gallbladder and
duodenum is also a well-documented complication15.
2.3 Diagnosis and severity
In an effort to standardize nomenclature, inform best practices and facilitate research
efforts, an international consensus conference focusing on the topics of acute cholecystitis and
cholangitis was organized in Toyko, Japan, in 2006. A panel of international experts in surgery,
internal medicine (including infectious diseases and gastroenterology), critical care and
radiology participated in performing systematic reviews and discussions ultimately leading to a
guidelines on the diagnosis and management of acute cholecystitis in 2007. This series of
publications, known as the Tokyo guidelines, were updated in January 2013, and lay out
diagnostic criteria and a clinical severity classification system for acute cholecystitis20.
As per the 2013 Toyko guidelines, the diagnosis of acute cholecystitis can be ‘suspected’
given one local sign of gallbladder inflammation (either Murphy’s sign on physical exam or right
upper quadrant mass/pain/tenderness) and one systemic sign of inflammation (either fever, an
elevated C reactive protein or a white blood cell count >12,000/mm3)20. A ‘definite’ diagnosis is
achieved when, in addition to the two previous criteria, imaging findings characteristic of acute
cholecystitis are present20. In a retrospective validation study, these criteria had a 91% sensitivity
and 97% specificity for a definite diagnosis of acute cholecystitis20.
The pathologic spectrum of acute cholecystitis mentioned previously is reflected by a
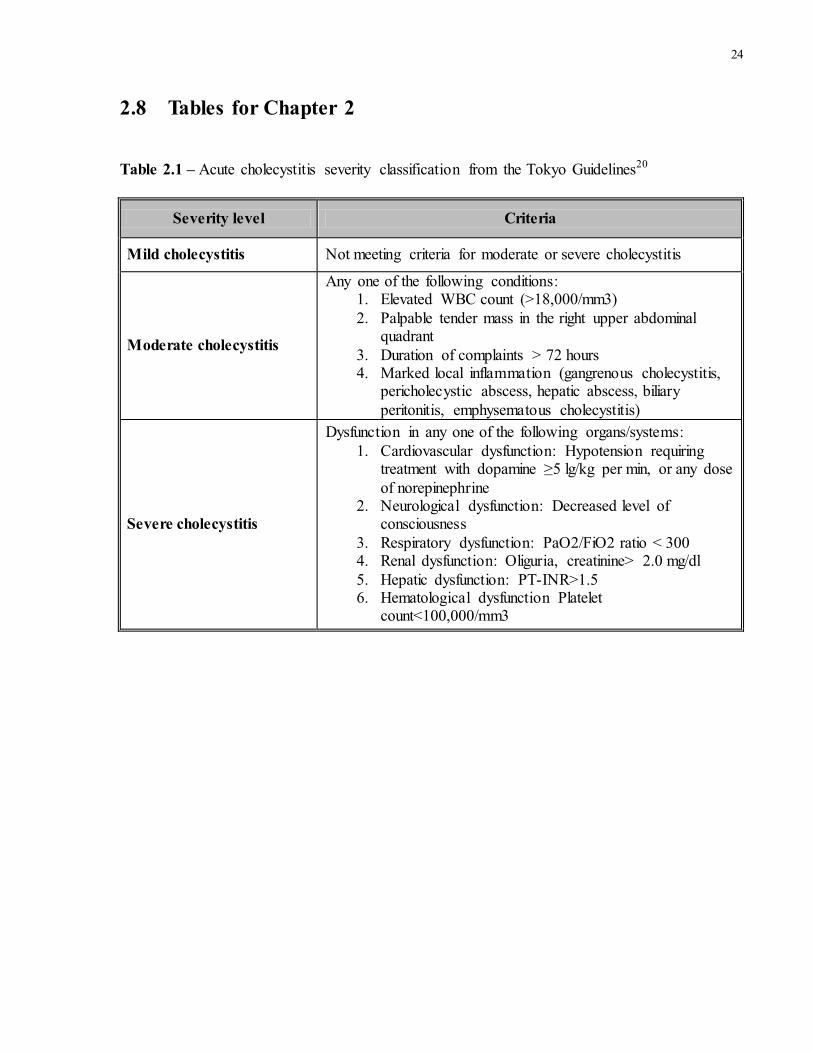
range in severity of clinical presentation. In patients with acute cholecystitis, the Tokyo
guidelines describe three levels of severity (Table 2.1). Mild cholecystitis involves meeting the
11
cholecystitis diagnostic criteria without any markers of greater severity. Moderate cholecystitis
reflects a greater degree of inflammation as suggested by a patient’s history, physical exam or
investigations. Finally, the definition of severe cholecystitis mirrors that of severe sepsis in so far
as the criteria are all markers of organ dysfunction. Approximately 95% of patients with acute
cholecystitis have mild or moderate cholecystitis21.
Several patient characteristics are frequently cited as associated with more severe
cholecystitis. However, no published studies have identified predictors of greater cholecystitis
severity in the context of the Toyko guidelines severity classification system. Furthermore, the
conclusion of an association between a patient characteristic and “more severe cholecystitis” has
been based on a range of metrics including clinical presentation, pre-operative imaging findings,
intraoperative findings, pathology or operative outcomes. With these caveats in mind, the
characteristics most consistently associated with more severe cholecystitis include older age,
male sex and diabetes22-27.
2.4 Surgical Management of Acute Cholecystitis
2.4.1 Rationale for surgical management of acute cholecystitis
Current management of acute cholecystitis is predominantly surgical for two main
reasons. First, cholecystectomy is the only definitive management of acute cholecystitis since it
manages the inflamed organ and, by removing the site of gallstone formation, prevents recurrent
symptoms. Second, the advent of laparoscopic cholecystectomy in 1990 has reduced the
12
morbidity associated with surgery thereby increasing the proportion of patients to whom
definitive surgery can be offered13.
The majority of cases of acute cholecystitis, if managed non-operatively, will settle.
In these patients, the need for definitive management is justified based on the risk of recurrent
gallstone-related symptoms. In the era when open cholecystectomy was the only surgical
approach, alternatives to cholecystectomy such as gallstone lithotripsy and pharmacologic
dissolution were extensively investigated for patients with symptomatic gallstones, outside of the
acute setting28. A high rate of recurrent or residual stones, high cost, applicability to only a small
proportion of patients and, ultimately, the advent of laparoscopic technique limited the uptake of
these nonsurgical treatments29-31. Laparoscopic cholecystectomy therefore became the
predominant treatment of symptomatic gallstone disease and the number of cholecystectomies
performed annually rose significantly in the 1990s13.
In a small proportion of cases of acute cholecystitis initially managed non-
operatively, symptoms will fail to settle and worsening sepsis, gangrenous cholecystitis, or
gallbladder perforation may ensue. Urgent surgical intervention is justified in these cases. An
alternative to surgery in the acute phase for patients with severe or worsening cholecystitis is
gallbladder decompression, generally via placement of a percutaneous drain known as a
cholecystostomy drain. Cholecystostomy placement is very effective in settling the acute
inflammation however, unlike surgery, does not prevent recurrence of symptom in the future32,33.
2.4.2 Surgical approach
Historically, cholecystectomy was performed via a subcostal incision (open
approach). Since the advent of laparoscopy in the late 1980s, laparoscopic cholecystectomy,
13
performed through 5-10mm incisions, has become the standard surgical approach (Figure 2.2). In
the non-emergent setting, the benefits of laparoscopic over open cholecystectomy include a
shorter hospital stay, faster return to work as well as better cosmesis, less post-operative pain and
a reduced incidence of surgical site infection34-36. As a result, by year 2000, over 90% of elective
cholecystectomies were started via a laparoscopic approach in Ontario13. However, in the event
of technical difficulty, conversion from laparoscopic to standard open technique is safe practice.
2.4.3 Complications of cholecystectomy
Removing the gallbladder first involves entering the abdominal cavity, either through an
open subcostal incision or laparoscopic instrument port placement (Figure 2.2), and dissecting
off omentum or bowel that is adherent to the gallbladder due to the inflammatory process. The
cystic duct, which connects the gallbladder to the common bile duct, and the cystic artery, which
supplies blood to the gallbladder, are then carefully identified, ligated and then divided (Figure
2.1). The gallbladder is then free to be dissected off the liver bed.
As with any invasive surgery, cholecystectomy carries certain risks. Operation-specific
complications include surgical site infection, bile leak, bile duct injury, bowel injury, vascular
injury and vasculo-biliary injuries. Medical complications include myocardial infarction,
pneumonia, urinary tract infection and venous thromboembolism. While rare, death may result
from any of these or other rarer complications.
The frequency of surgical site infection ranges from 1% to 10% and the risk is related to
surgical approach (laparoscopic or open cholecystectomy) and the degree of contamination (e.g.
gangrenous cholecystitis, leakage of infected bile, occurrence of a bile duct or bowel injury)37.
More specifically, when characterized according to the Center for Disease Control’s levels of
14
surgical site infection, the frequency of infection is 1% - 5%, 0.1% - 1% and 0.3% - 2.5% for
superficial incisional surgical site infection, deep incisional surgical site infection and organ
space surgical site infection respectively37,38. Appropriate management is usually based on the
nature and severity of infection. Antibiotics or simply opening the surgical wound will treat a
superficial surgical site infection. Percutaneous drainage or re-operation and washout are
required for more extensive or deep organ-space infections.
Bile leaks and bile duct injuries represent a spectrum of injury to the biliary tract.
Strasberg et al. proposed a classification system most applicable to the laparosopic era that
classifies injuries based on the length, circumference and level of the injury involved and
whether the main duct (common hepatic and common bile duct) versus an accessory or the cystic
duct are injured39. With respect to associated morbidity and impact on quality of life, injury to
the biliary tract can be considered in two broad categories: bile leaks and bile duct injuries
requiring operative intervention. Leaks may result from injury to a side branch of the biliary tree,
the cystic duct stump or a non-circumferential injury to the main ductal system. These may be
managed with endoscopic cholangiopancreatography and stent placement, possibly in association
with percutaneous drainage40. Major bile duct injuries require operative repair or reconstruction
of the biliary tract and are therefore associated with the greatest morbidity40. In fact bile duct
injuries are associated with reduced long term survival and are a major cause of litigation against
general surgeons40-43. Leaks occur in approximately 1-3% of laparoscopic cholecystectomies
whereas injuries complicate only 0.3-0.5% of cholecystectomies41,44-48. In addition, vasculo-
biliary injuries have recently received greater attention and refer to an extreme case of major bile
duct injury that occurs in conjunction with injury to a hepatic artery and/or portal vein 49,50. This
devastating injury accounts for only 2% of major bile duct injuries51.
15
The frequency of bowel injuries is not well characterized but results from dissection of
the colon, small bowel or duodenum adhered to an inflamed gallbladder or from inadvertent
cautery burn. Primary repair is generally possible if recognized early; otherwise, patients will
present later with peritonitis necessitating a return visit to the operating room.
A small proportion of cholecystectomies for symptomatic gallstones lead to medical
complications. Based on data from the National Surgery Quality Improvement Program (NSQIP)
of the American College of Surgeons, a procedure-specific registry, medical complications such
as myocardial infarction, pneumonia, urinary tract infection and venous thromboembolism
respectively occur in 0.2%-1%, 0.4%-4%, 0.7%-2% and 0.2%-1% patients respectively37. The
frequency of such complications might reasonably be expected to be higher in patients operated
on for acute cholecystitis.
Finally, mortality for patients with acute cholecystitis is under 1%15 and mortality
attributable to cholecystectomy (within 30 days or same admission) ranges between 0.3% and
3%15,37,52,53.
2.4.4 Laparoscopic cholecystectomy in the setting of acute cholecystitis
The initial experience with laparoscopic cholecystectomy was in the elective setting for
patients suffering from biliary colic, where transient gallbladder outflow obstruction occurs
without gallbladder inflammation. In fact, acute cholecystitis was initially considered a
contraindication to laparoscopic surgery based on the argument that laparoscopy in the setting of
acute inflammation would translate into high rates of operative complications54. High common
bile duct injury rates (5.5%) and high rates of conversion to open approach (15%-33%) were
indeed initially seen with laparoscopic cholecystectomy in the setting of acute cholecystitis54-56.
16
However, in a randomized trial comparing laparoscopic to open cholecystectomy in the setting of
acute cholecystitis, laparoscopy was associated with less morbidity, shorter hospital stay and
more rapid return to work57. More recent evidence suggests an improvement in rates of bile duct
injury as surgeons’ experience and comfort with laparoscopy has grown. In fact, large scale
analyses of laparoscopic cholecystectomy in patients with prior acute cholecystitis showed a
0.3% common bile duct injury rate with conversion rates remaining high in the order of 15%58.
Given the benefits of laparoscopy over an open approach, as well as evidence of improvement in
outcomes with experience, laparoscopic cholecystectomy has become the standard initial
surgical approach for acute cholecystitis.
As mentioned previously, in the event of operative difficulty, conversion from
laparoscopic to an open approach should be undertaken to prevent complications such as bile
duct injury. A number of preoperative factors have been associated with an increased probability
of conversion from laparoscopic to open surgery. These include male sex, older age, the presence
or history of obstructive jaundice, an elevated white blood cell count and a longer duration of
symptoms 22,49. Nevertheless, the degree of inflammation encountered intra-operatively
(particularly in the area known as Calot’s triangle, where the cystic duct, cystic artery and
common hepatic duct are found) remains challenging to predict preoperatively. Furthermore, the
surgeon’s comfort with difficult laparoscopic cholecystetomy is also a critical determinant of the
probability of conversion.
2.4.5 Timing of cholecystectomy for acute cholecystitis
While laparoscopic cholecystectomy was established as superior to open
cholecystectomy for patients with acute cholecystitis, the timing of operative intervention in the
laparoscopic era remained controversial in the late 1990s. Two broad strategies exist: urgent
17
early cholecystectomy and delayed elective cholecystectomy. Early cholecystectomy, while
variably defined throughout the surgical literature, most generally refers to cholecystectomy
performed on the initial admission within up to 7 days from symptom onset 22,59,60. With delayed
intervention, acute inflammation is allowed to settle before proceeding with cholecystectomy
some 6 to 12 weeks after the initial admission.
In the pre-laparoscopy era, early open cholecystectomy for acute cholecystitis was
supported by randomized prospective trials59,61,62. However with laparoscopy, it was not initially
known how conversion rates and operative complications would compare between early and
delayed cholecystectomy. Performing a delayed cholecystectomy when the gallbladder is no
longer acutely inflamed and friable might reasonably be safer. Conversely, if delayed
cholecystectomy allows for the formation of fibrosis in and around Calot’s triangle, the operation
may prove more difficult resulting in a higher rate of conversion and complications. Also,
patients managed with the intention of delayed cholecystectomy, who are discharged home once
their acute symptoms improve, remain at risk of recurrent gallstone-related symptoms until their
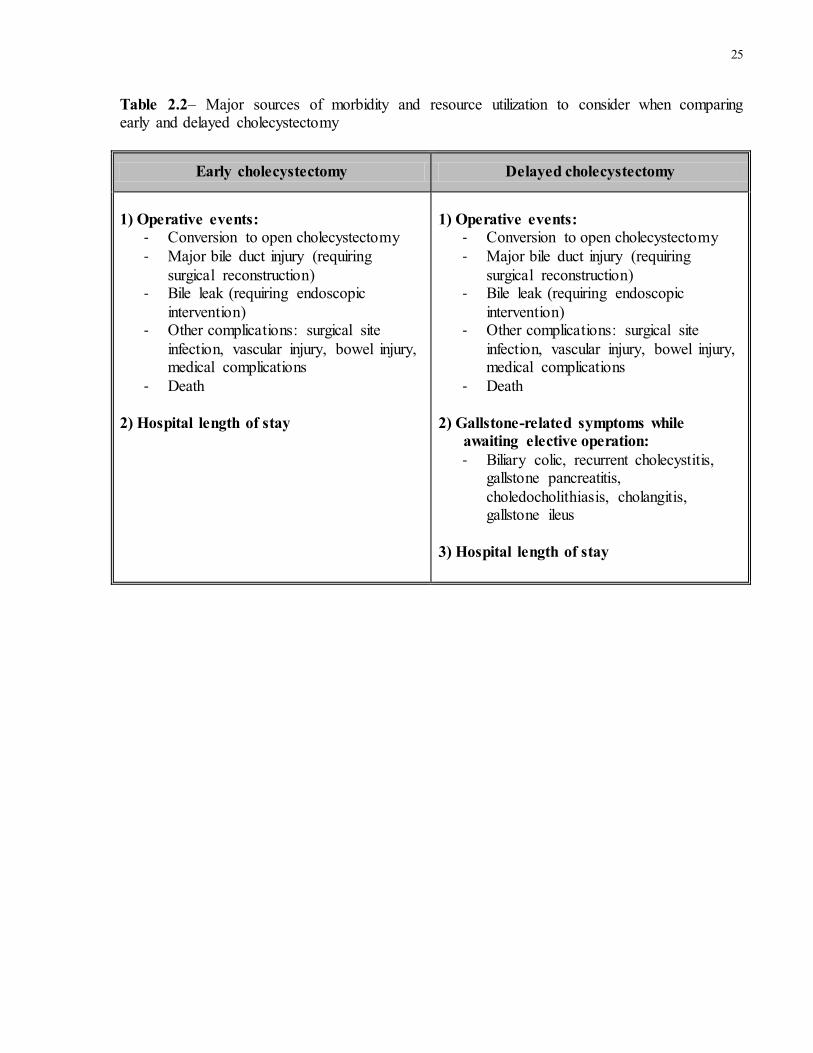
scheduled elective cholecystectomy. Table 2.2 lists the major sources of morbidity and resource
use to consider when comparing early to delayed cholecystectomy.
2.4.6 Timing of cholecystectomy and clinical outcomes
Starting in the late 1990s multiple studies prospectively examined the timing of
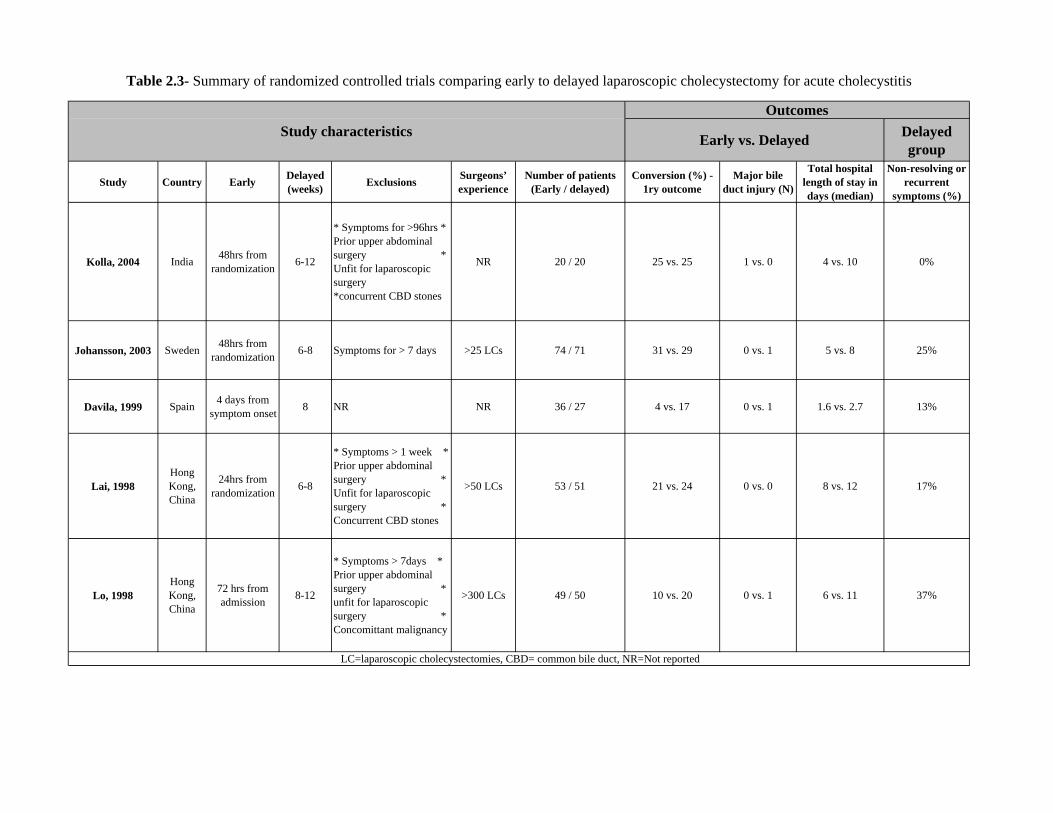
laparoscopic cholecystectomy in acute cholecystitis. Five randomized prospective trials compare
the outcomes of laparoscopic cholecystectomy performed on first presentation compared to a
delayed procedure and are synthesized in Table 2.3. The results of these trials show that
laparoscopic cholecystectomy within 7 days of symptom onset or diagnosis is associated with a
significantly reduced total hospital stay and a similar conversion rate as delayed cholecystectomy
18
46,63-67. Furthermore, with respect to the clinical course of patients managed with delayed
cholecystectomy, trial data and retrospective studies of selected patient samples suggest that
delayed management is associated with a 0% to 38% readmission rate for gallstone related
complications 46,63-70. This range of estimates also provides insight into our contemporary
understanding of the natural history of untreated acute cholecystitis.
As such, early cholecystectomy for most patients with acute cholecystitis has been
promoted based on the findings of a similar conversion rate, shorter hospital length of stay and
avoidance of recurrent gallstone symptoms. However, the randomized trials suffer from many
limitations. First, they were published from 1998 to 2004 and certain exclusion criteria such as
suitability for laparoscopy are unlikely to apply today as experience with difficult laparoscopic
cholecystectomy has grown. Second, the trials were powered to compare conversion rates in the
order of 20% but were too small to compare rare but devastating complications such as bile duct
injury or mortality. A recent meta-analysis of the trials’ data remains underpowered to offer a
conclusive comparison of the frequency of bile duct injury (1 in 232 early cases versus 3 in 219
delayed cases)71. Finally, the studies originate from single academic centers and therefore may
not provide estimates of outcomes and recurrent gallstone symptoms that can be generalized to a
broader sphere of practice. The only published population-based data on recurrent gallstone
complication rates, in patients discharged home without cholecystectomy, is limited to capturing
admissions in patients over the age of 6569.
2.4.7 Timing of cholecystectomy and economic outcomes
The timing of laparoscopic cholecystectomy for acute cholecystitis has important
ramifications in terms of resource utilization and associated costs. Clinical studies suggest lower
healthcare costs with early cholecystectomy based on a reduction in total hospital length of
19
stay46,69. However, only two formal economic evaluations have focused on the timing of
cholecystectomy in acute cholecystitis. A complete economic evaluation requires consideration
of both the costs and clinical consequences of alternative management strategies72. The results of
an economic evaluation can help a decision maker, such as a third party payer, decide whether
the clinical benefit of one treatment over the other is worth any additional cost. Furthermore,
quantifying the amount of uncertainty around the results is an integral component of economic
evaluations and remains relevant even in situations where a treatment is more effective and less
costly than its alternative.
In the first published economic evaluation on this topic, Wilson et al. undertook a cost-
utility analysis using a decision tree framework to compared early cholecystectomy, performed
within up to 7 days symptom onset, to delayed elective cholecystectomy73. Costs were calculated
from the perspective of the United Kingdom Ministry of Health and the metric of clinical
effectiveness was the quality-adjusted life-year (QALY). Their analysis showed that early
laparoscopic cholecystectomy was less costly (−£820 per patient) and associated with greater
QALY gains (+0.05QALYs per patient) for patients with acute cholecystitis. On probabilistic
sensitivity analysis, they reported an 80% probability that early laparoscopic cholecystectomy
was cost-effective given a Ministry of Health willingness-to-pay £20,000 per additional quality-
adjusted life-year. In a similar cost-utility analysis, Johner and colleagues reached the same
conclusion, but included only costs from the perspective of a single academic hospital in British
Columbia, Canada74. However, the outcomes probabilities that informed both group’s decision
tree models input parameters were derived from the existing randomized trials comparing early
to delayed cholecystectomy. As a result, both studies are hindered by the previously mentioned
limited contemporary external validity and constraints related to the small sample size of the
trials.
20
In addition to these two similar model-based studies, a person-level cost-utility analysis
was also published by MaCafee et al. that compared early to delayed cholecystectomy for
patients with biliary or acute cholecystitis75. They performed a small randomized trial capturing
patients’ quality of life 30-35 days after surgery as well as costs from a National Health Service
and societal perspective. Although no significant differences in costs or quality of life were
observed, the marginally higher quality of life 30 days after delayed surgery (vs. early surgery)
was associated with minimal additional cost. Since the risk of operative complications and
recurrent symptoms is lower with biliary colic than acute cholecystitis, the lack of a subgroup
analysis focused on patients with acute cholecystitis limits direct application of these results to
the central question of this thesis. Furthermore, temporary reductions in quality of life while
awaiting delayed elective cholecystectomy were not captured in Macafee’s analysis and are a
critical consideration.
2.5 Management guidelines for acute cholecystitis
The previously described Tokyo consensus guidelines represent the most detailed
guidelines for the management of acute cholecystitis 49. Based on existing evidence and
consensus among the expert panel members, the 2013 Tokyo guidelines support early surgery on
first presenting admission as the optimal management strategy for patients with non-severe acute
cholecystitis. This recommendation is also consistent with the Society of American
Gastrointestinal and Endoscopic Surgeon’s (SAGES) guidelines for the clinical application of
laparoscopic biliary surgery76. While much less detailed, SAGES endorses early laparoscopic
cholecystectomy within 24 to 72 hours of diagnosis for patients with acute cholecystitis.
21
The Tokyo guidelines also provide recommendations specific to the grade of cholecystitis
severity. Since the severity classification system was published relatively recently, grade-specific
recommendations do not have a strong evidence base. However, the recommendations are
informed by consensus of international experts that participated in the development of these
guidelines. Patients with mild (grade I) acute cholecystitis should be managed with
cholecystectomy early on first presenting admission. For patients with moderate cholecystitis
(grade II), early cholecystectomy is also recommended as the preferred management strategy.
However, the 2013 version of the guidelines, more so than the 2007 version, stresses the point
that, at the surgeon-level, delaying surgery may be reasonable if the surgeon is not comfortable
with difficult laparoscopic cholecystectomy where severe local inflammation is encountered.
Conversely, the point is also made that a minority of cases of moderate cholecystitis involving
gallbladder perforation, grangrenous cholecystitis or emphysematous cholecystitis may require
urgent early surgery or gallbladder drainage. Finally, for patients with severe cholecystitis,
intervention is required given the organ dysfunction resulting from the acute cholecystitis.
Percutaneous cholecystostomy followed by delayed cholecystectomy is recommended as the
optimal management for these patients.
2.6 Variation in practice
As described, best available evidence can be interpreted as supportive of early
cholecystectomy for most patients with acute cholecystitis based on a similar conversion rate,
shorter total hospital length of stay and elimination of the risk of recurrent gallstone symptoms
associated with delayed cholecystectomy. While the clinical trials were published between 1998

22
and 2004, practice patterns have not universally followed suit. In studies published between 2004
and 2007, only 11% to 55% of surgeons surveyed in the UK, Japan and Australia reported
having a preference for early laparoscopic cholecystectomy77-80. Further support in the literature
for early cholecystectomy was provided in 2006-2007 when a Cochrane Collaborative meta-
analysis of the randomized trial data was published as well as the Tokyo consensus guidelines
for the management of acute cholecystitis. However, studies published between 2006 and 2012
in the USA, UK and Japan have shown that 36-88% of patients with acute cholecystitis actually
undergo early cholecystectomy69,70,80-83. Clearly practice patterns remain variable across
hospitals worldwide. However, because of differences in the setting and cohort characteristics
across published studies, our understanding of the extent and underlying etiology of the
inconsistent application of early cholecystectomy remains circumstantial.
2.7 Summary of gaps in knowledge
In summary, important gaps remain in the clinical evidence comparing early to delayed
cholecystectomy for acute cholecystitis. The main gaps include:
(1) The need for a contemporary comparison of the rate of conversion from
laparoscopic to open cholecystectomy in real world practice.
(2) The lack of an accurate comparison of rare but devastating operative
complications including bile duct injury and death.
(3) The need for estimates of the risk of recurrent symptoms if cholecystectomy is
delayed, that can be generalized to a broad range of patients.
23
Furthermore, published reports suggest variation in the application of early
cholecystectomy across different contexts of care. Therefore, in order to effectively translate
clinical evidence into practice within a given healthcare system such as Ontario’s, a detailed
understanding of the local context of practice is required.
Finally, given the constrained nature of healthcare budgets, economic evaluations can
provide useful information for decision making by explicitly presenting the costs of alternative
treatments relative to the associated clinical consequences. Setting-specific cost estimates as well
as clinical outcome estimates addressing previously mentioned knowledge gaps will best inform
decision making.
24
2.8 Tables for Chapter 2
Table 2.1 – Acute cholecystitis severity classification from the Tokyo Guidelines20
Severity level Criteria
Mild cholecystitis Not meeting criteria for moderate or severe cholecystitis
Moderate cholecystitis
Any one of the following conditions: 1. Elevated WBC count (>18,000/mm3) 2. Palpable tender mass in the right upper abdominal
quadrant 3. Duration of complaints > 72 hours 4. Marked local inflammation (gangrenous cholecystitis,
pericholecystic abscess, hepatic abscess, biliary peritonitis, emphysematous cholecystitis)
Severe cholecystitis
Dysfunction in any one of the following organs/systems: 1. Cardiovascular dysfunction: Hypotension requiring
treatment with dopamine ≥5 lg/kg per min, or any dose of norepinephrine
2. Neurological dysfunction: Decreased level of consciousness
3. Respiratory dysfunction: PaO2/FiO2 ratio < 300 4. Renal dysfunction: Oliguria, creatinine> 2.0 mg/dl 5. Hepatic dysfunction: PT-INR>1.5 6. Hematological dysfunction Platelet
count<100,000/mm3
25
Table 2.2– Major sources of morbidity and resource utilization to consider when comparing early and delayed cholecystectomy
Early cholecystectomy Delayed cholecystectomy
1) Operative events:
- Conversion to open cholecystectomy - Major bile duct injury (requiring
surgical reconstruction) - Bile leak (requiring endoscopic
intervention) - Other complications: surgical site
infection, vascular injury, bowel injury, medical complications
- Death 2) Hospital length of stay
1) Operative events:
- Conversion to open cholecystectomy - Major bile duct injury (requiring
surgical reconstruction) - Bile leak (requiring endoscopic
intervention) - Other complications: surgical site
infection, vascular injury, bowel injury, medical complications
- Death 2) Gallstone-related symptoms while
awaiting elective operation: - Biliary colic, recurrent cholecystitis,
gallstone pancreatitis, choledocholithiasis, cholangitis, gallstone ileus
3) Hospital length of stay
Delayed group
Study Country Early Delayed (weeks) Exclusions Surgeons’
experienceNumber of patients
(Early / delayed)Conversion (%) -
1ry outcomeMajor bile
duct injury (N)
Total hospital length of stay in days (median)
Non-resolving or recurrent
symptoms (%)
Kolla, 2004 India 48hrs from randomization 6-12
* Symptoms for >96hrs * Prior upper abdominal surgery * Unfit for laparoscopic surgery *concurrent CBD stones
NR 20 / 20 25 vs. 25 1 vs. 0 4 vs. 10 0%
Johansson, 2003 Sweden 48hrs from randomization 6-8 Symptoms for > 7 days >25 LCs 74 / 71 31 vs. 29 0 vs. 1 5 vs. 8 25%
Davila, 1999 Spain 4 days from symptom onset 8 NR NR 36 / 27 4 vs. 17 0 vs. 1 1.6 vs. 2.7 13%
Lai, 1998Hong Kong, China
24hrs from randomization 6-8
* Symptoms > 1 week * Prior upper abdominal surgery * Unfit for laparoscopic surgery * Concurrent CBD stones
>50 LCs 53 / 51 21 vs. 24 0 vs. 0 8 vs. 12 17%
Lo, 1998Hong Kong, China
72 hrs from admission 8-12
* Symptoms > 7days * Prior upper abdominal surgery * unfit for laparoscopic surgery * Concomittant malignancy
>300 LCs 49 / 50 10 vs. 20 0 vs. 1 6 vs. 11 37%
LC=laparoscopic cholecystectomies, CBD= common bile duct, NR=Not reported
Outcomes
Early vs. Delayed Study characteristics
Table 2.3- Summary of randomized controlled trials comparing early to delayed laparoscopic cholecystectomy for acute cholecystitis
Charles
Text Box
26

27
2.9 Figures for Chapter 2
Figure 2.1 - Depiction of anatomy of gallbladder, cystic duct and common bile duct (copyright
A.D.A.M)

28
Figure 2.2 - Depiction of laparoscopic and open cholecystectomy

29
Chapter 3
General Methods
The purpose of this chapter is to:
I. Describe the strengths of using Ontario’s population-based administrative databases for
this thesis work
II. Present details on the data sources and data validity
III. Provide an overview of the major analytic considerations for each chapter

30
There is no large population-based study to date that compares early to delayed
cholecystectomy for acute cholecystitis. As detailed previously, trials comparing these
management strategies suffer from limited sample size and limited contemporary external
validity. Analysis of a large population-based cohort of patients with acute cholecystitis is
uniquely suited to address these limitations and offer added value to decision making. The need
for such studies has in fact been echoed in a number of published reports 84-86.
While retrospective analysis of population-based administrative databases offers several
unique strengths, important methodological considerations are necessary. In view of this fact,
this chapter discussed the major strengths associated with the use of Ontario’s administrative
data to address the specific aims of this thesis. I then provide details on each of the databases
utilized as well as their validity for the purposes of this thesis. Finally, major analytic concepts
relevant to each specific aim are presented.
31
3.1 Strengths of Ontario’s Administrative Health Data
Administrative health data for the province of Ontario are housed and consolidated at
the Institute for Clinical Evaluative Sciences (ICES), Toronto. The strengths of Ontario’s
administrative health data for the purposes of this thesis include the provision of a large study
sample, its population-based nature, the broad scope of services captured, the longitudinal span
of the data supported by deterministic linkage and a data collection framework supporting data
validity.
3.1.1 Large sample size
Canada’s most populous province, Ontario has a population of over 13 million persons
contributing to the administrative data sources utilized for this thesis87. Studying a large sample
of patients with acute cholecystitis drawn from this population allows the detection of rare
operative complications such as bile duct injury or death as well as rare gallstone-related
complications such as gallstone ileus.
3.1.2 Unselected population-based sample
A number of large databases worldwide have been utilized for the purpose of studying
gallstone disease. Procedure-specific registries exists such as the U.S. National Surgical Quality
Improvement Program37, the Swiss Association of Laparoscopic and Thoracoscopic Surgery
Database53 or the population-based Swedish Gallrisk registry42. These registries do not support
the disease-specific analysis required for the specific aims of this thesis since episodes of care
not involving surgery are not captured. Disease-specific cohorts of patient with acute
cholecystitis can be defined from many large administrative databases, however most are
32
restricted to a selected patient group (e.g. patients over 65 years of age in U.S. Medicare data69)
or a selection of hospitals (e.g. U.S. Nationwide Inpatient Sample88, the Health Episode Statistics
database in the U.K.89). In part due to the fact that there are no private general hospitals in
Ontario, the data sources utilized in this thesis offer the important advantage of including all
residents within the province with a valid health card. Therefore, a population-based disease-
specific cohort of all patients with acute cholecystitis can be studied and generate results
generalizable to a wide range of patients and settings.
3.1.3 Longitudinal span supported by deterministic data linkage
Administrative records held at ICES data back as far as the late 1980s in some cases and
new records are added on an annual basis. These databases are linkable across episodes of care
and fiscal year using an encrypted unique patient identifier based on a patient’s Ontario Health
Card Number. This deterministic linkage supports longitudinal follow-up with loss of follow-up
occurring only in the case where patients lose their status as residents of Ontario.
3.1.4 Broad scope of services captured
As can be appreciated below in the descriptions of the individual databases, the scope of
services and information captured in Ontario’s administrative data is broad. Records cover all
hospitalizations, day surgeries, emergency rooms visits, physician billing as well as information
on hospitals and physicians. The scope of health services captured and deterministic linkage of
individual records at the patient-level allows a detailed understanding of patients’ clinical course.
33
3.2 Description of Data Sources
3.2.1 Discharge Abstract Database
The Discharge Abstract Database (DAD) at ICES includes data on all hospital admissions
and same day surgeries in Ontario. Each record of a hospital stay includes patient demographics,
diagnostic and procedural data as well as disposition. Prior to processing at ICES, the data is
collected as part of a national DAD by the Canadian Institute for Health Information (CIHI) and,
with the exception of Québec, is submitted directly to CIHI by individual hospitals. A DAD
abstraction manual, describing province-specific mandatory fields, as well as required testing of
abstraction software supports a standardized abstraction process90. When data errors at an
individual hospital are identified during initial processing, CIHI is able to request that corrected
data be resubmitted. DAD was used to capture the index acute cholecystitis admission as well as
day surgeries for cholecystectomy and gallstone-related admissions.
3.2.2 National Ambulatory Care Reporting System
Records from the National Ambulatory Care Reporting System (NACRS) also originate
from a national database collected and maintained by CIHI that includes all emergency
department visits. NACRS records are processed at ICES to allow direct linkage to an associated
DAD record. For the purposes of this thesis, entry via the emergency department prior to the
index cholecystitis admission was confirmed through linkage with NACRS. In addition,
gallstone-related emergency department visits were identified in NACRS.
34
3.2.3 Registered Person Database
The registered person database (RPDB) is provided to ICES by the Ontario Ministry of
Health and includes basic demographic information (age, sex) and vital statistics (date of birth,
date of death) on residents of Ontario with a valid health card. Date of death and patient
demographic information are preferentially identified from RPDB as is standard with ICES
projects.
3.2.4 Ontario Health Insurance Plan Billing Database
The Ontario Health Insurance Plan (OHIP) Billing Database contains records of all
physician billing claims paid by the Ontario Ministry of Health and Long Term Care. Each
record contains a fee code, a fee suffix reflecting the type of physician service (e.g. performing a
surgical procedure vs. assisting with a surgical procedure) as well as an encrypted physician
number and the ICES patient key number for linkage to other databases. A diagnosis code is also
included. However, this field is of uncertainty validity and may reflect broad disease categories
rather than specific diseases. The OHIP Billing Database was used to derive a comorbidity index
as well as identify cholecystectomies and biliary tract repair for major bile duct injury.
3.2.5 ICES Physicians Database
The ICES Physician Database contains information on physicians in Ontario that is
linkable to the encrypted physician billing number included in the OHIP Billing Database. From
this database year of medical school graduation was obtained and used as a reflection of a
surgeon’s number of years in practice.
35
3.3 Data validity
The validity of the above-mentioned databases can be an important strength or a serious
limitation depending on the research question. The data held at ICES has been validated for the
identification of a variety of diagnoses including congestive heart failure91, acute myocardial
infarction91, chronic obstructive pulmonary disease92, hypertension93, diabetes94 and infection
with human immunodeficiency virus95. In addition to these specific diagnoses, referencing a
patient’s inpatient and outpatients records in DAD, NACRS and the OHIP billing database
support the derivation of a comorbidity index predictive of 1 year mortality in a general cohort of
adult Ontarians96,97. Finally, the accuracy of DAD coding for a broader range of diagnoses as
well as procedures was examined in an ICES-funded multicenter re-abstraction study98. This
study was the largest of its kind in Canada, including over 14,000 records across 18 hospitals in
Ontario. Juurlink and coauthors reported consistently high sensitivity and specificity of
procedure coding in administrative records. While variation across disease areas was observed,
coding of the diagnosis most responsible for hospitalization was generally accurate.
Of specific relevance to this thesis, almost perfect agreement (kappa= 0.83 (0.76 to 0.90))
and high sensitivity (0.85 (0.74 to 0.92)) was found for gallstone disease as the most responsible
diagnosis98. However, it should be noted that the accuracy of coding of specific types of
gallstone disease (e.g. cholelithiasis with cholecystitis versus cholelithiasis without cholecystitis
versus cholecystitis with choledocholithiasis) was not examined. With respect to the accuracy of
cholecystectomy coding, almost perfect agreement (kappa= 0.97 (0.95 to 0.99)) and very high
sensitivity (0.98 (0.93 to 1.00)) were found in Ontario’s DAD98.
36
3.4 Approach to costing with Ontario’s administrative data
Methods of cost estimation using administrative data in Canada are becoming
increasingly refined and were outlined in a 2009 report by the Canadian Agency for Drugs and
Technologies in Health99. Based on this methodology, an ICES-specific person-level costing
approach has been described in a recent report that includes database-specific considerations100.
Hospital costs are estimated using the Resource Intensity Weight (RIW) method 18. Each
ED visit, hospital admission and day surgery is assigned an RIW value, which when multiplied
by the provincial average cost per weighted case (CPWC), estimates the cost of the given patient
visit. The RIW value for a given admission for example reflects a patient`s level of resource
utilization during that admission and is based on the patient`s major diagnosis, age, comorbidity
burden, interventions received and length of stay. The CPWC values are year and visit type
specific (e.g. inpatient stay in fiscal year 2009), and they are derived from the allocation of
global hospital budgets across all patients (total annual budget of inpatient care divided by sum
of all inpatients’ RIWs). Both direct medical and overhead hospital costs associated with relevant
ED visits, inpatient stays and day surgery are captured within this costing approach.
The cost of physician services relevant to this thesis work fall outside the scope of the
RIW method since general surgery physician services in Ontario are largely directly paid by the
Ministry of Health on a fee-for-service basis. The costs specific to physician claims can therefore
be derived based on the fee schedule known as the Ontario Health Insurance Plan schedule of
benefits for physician services101.
37
3.5 Analytic consideration
3.5.1 Clustered data
Data and variables included in large administrative databases generally reflect
patients treated within given structures of care (e.g. patients cared for by specific physicians,
working within specific hospitals). In other words patients can be considered clustered within
structures of healthcare delivery. Furthermore, when studying a large cohort, it is reasonable in
many cases to expect that patients within the same cluster (e.g. cared for at the same hospital) are
more similar to one another than to patients within a distinct cluster (e.g. cared for at another
hospital). However, standard multivariable regression techniques (i.e. generalized linear models)
to account for confounding assume that all observations are independent102. The impact of this
assumption is most important when interpreting the association of cluster-level characteristics
(e.g. hospital teaching status) with a given outcome 103. For example, when considering the
association between patient and hospital level characteristics with the receipt of early
cholecystectomy as we do in Specific Aim 1, standard regression will tend increase the precision
of the association between hospital-level characteristics and the outcome. This occurs because
instead of comparing for example 25 teaching hospitals to 127 non-teaching hospitals, teaching
status is attributed to the person-level such that the comparison of teaching status now involves
comparing approximately 13,000 patients at teaching hospitals to approximately 10,000 patients
at non-teaching hospitals104. Multilevel regression overcomes this analytic fallacy by attributing
an additional measure of effect in the regression equation for each higher-level unit and also
supports further understanding of outcome variation across high-level units. While the magnitude
of change in the direction and significance of effects when accounting for clustering cannot
always be predicted, the impact is generally greatest on higher-level characteristics. In other
38
words, the estimate (e.g. odds ratio) and the confidence limits around this estimate are more
likely to change for hospital teaching status or a hospital volume metric than for patient age or
sex104.
3.5.2 Standard versus competing risks in time-to-event analysis
Specific Aim 2 focuses on quantifying the risk of recurrent gallstone-related
symptoms among patients discharged without cholecystectomy following an index cholecystitis
admission. The outcome of interest is occurrence of the first gallstone-related emergency
department visit or hospital admission. In calculating the probability of this outcome at clinically
meaningful time intervals after discharge, time-to-event (survival analysis) is appropriate in
order to account for the different individual periods of follow-up as well as considering the fact
that patients’ follow-up may be censored. Censoring means that follow-up is cut short before the
outcome is observed. Reasons a patient’s follow-up may be censored include end of the
observation window, death or end of the period where the patient is at risk of the outcome (e.g. a
patient has their gallbladder removed so is no longer at risk of recurrent acute cholecystitis). The
reasons patients are censored as well as the clinical question are important considerations when
deciding on an appropriate analytic approach.
Standard univariable time-to-event analysis using the Kaplan-Meier method considers
that censoring is non-informative105.The assumption of non-informative censoring means that
patients who undergo a censoring event (e.g. cholecystectomy) should not be at greater or lesser
risk of a subsequent outcome event (e.g. gallstone-related complication) as compared to the
remaining patients with a similar event-free (“survival”) time. When censoring is an informative
competing risk (e.g. a large proportion of deaths at home are due to gallstone disease), the
Kaplan-Meier method will overestimate the probability of the outcome 106,107. The cumulative

39
incidence approach has been developed as an alternative analytic approach that accounts for the
competing nature of a censoring event107,108.
However, both approaches can be interpreted as presenting valid information, even in
the context of informative censoring by a competing risk. On one hand, the Kaplan-Meier results
reflect the probability of the outcome over time among patients who would not be affected by the
competing risk. Alternatively, the cumulative incidence approach describes the probability of the
outcome as actually observed in the study cohort. Therefore it is important to consider to whom
the results are meant to apply. Ultimately, the magnitude of the difference between the two
approaches will be minimal in cases where the competing risk is rare, as is the case for death
among patients being offered delayed elective cholecystectomy. Given these considerations, as
detailed in Chapter 5, we performed standard time-to-event analysis as our primary approach.
The cumulative incidence function of a gallstone-related event was also calculated as a
secondary approach.
3.5.3 Accounting for selection bias in comparative effectiveness studies
By the very nature of non-experimental studies, treatment selection bias is a critical
consideration when comparing two treatment alternatives using administrative data. Standard
regression techniques are most often used and are an accessible tool to non-statisticians given the
ease of implementation in most statistical software and rapidly increasing processing power.
Nevertheless, regression techniques also offer the opportunity to perform an analysis without
seeing explicit evidence that the results reflect a less biased estimate of an exposure-outcome
association. Propensity score methods were first developed by Rosenbaum and Rubin as an
alternative to regression methods109. The propensity value is the probability of exposure based on
observed covariates109. When conditioning on the propensity score, a comparison of similar
40
patients is possible. Four methods of using the propensity score to reduce bias have been
described: direct adjustment, stratification, matching and inverse probability of treatment
weighting110. The first involves including the propensity score value as a continuous independent
variable in a regression model. The second involves creating strata based on the propensity score
within which a less biased outcome comparison can be made. The third involves matching
patients in exposure groups based on the propensity score and the fourth methods weighs each
patient based on the inverse of the probability of treatment received. The third and fourth
methods have been shown to most effectively reduce bias given a binary outcome measure 111.
Matching has the added benefit of a being more transparent approach since balance before and
after matching of exposure groups is presented and, similarly to the first table of baseline
characteristics in a randomized trial, requires minimal statistical training to appreciate. Matching
on the propensity score was therefore employed as the primary analytic technique to minimize
bias related to observed covariates when comparing the operative outcomes of early and delayed
cholecystectomy for acute cholecystitis in Specific Aim 3. Inverse probability of treatment
weighting was also undertaken as a secondary approach.
3.5.4 Best modeling practices in economic evaluation
The final paper of this thesis is a model-based cost-utility analysis comparing
alternative timeframes of cholecystectomy for acute cholecystitis. Economic evaluation such as
cost-utility or cost-effectiveness analyses can either be person-level or model-based72. Since
simultaneous collection of all relevant clinical outcomes probabilities, health-related quality of
life and costs relevant to a decision is rare, modeling is most often required. Based on decision
analysis methods, a model-based economic evaluation can support the comparison of many
alternative treatment strategies and should be informed by best available evidence, often drawn

41
from multiple difference sources. Given the complexity of many economic models as well as the
subjective nature of model construction, the Society for Medical Decision Making (SMDM) and
International Society for Pharmacoeconomics and Outcomes Research (ISPOR) created a Task
Force on best modeling practices112. Recommendations were made with respect to model
structure, integration of outcomes, model evaluation as well as sensitivity analyses. The
recommendations stress the role of decision/economic models as a means to support decision
making by explicitly considering all clinical consequences (and costs for economic evaluations)
of alternative management strategies. Another critical recommendation is that model structure be
based on the relevant clinical and economic consequences as opposed to available data (e.g. from
the newest randomized controlled trial) and that best available data consistent with principles of
evidence-based medicine should inform the model. Finally, sensitivity analyses, including
probabilistic sensitivity analysis, are considered essential to evaluate model input parameter
uncertainty. These and other recommendations of the SMDM-ISPOR Task Force were
considered in completing Specific Aim 4.
42
Chapter 4
Variation in early cholecystectomy for acute cholecystitis in Ontario
The purpose of this chapter is to:
I. Characterize the extent of variation in early cholecystectomy across hospitals in Ontario.
II. Identify patient and hospital characteristics associated with performing early
cholecystectomy
Preamble
The contents of this chapter have been accepted for publication in CMAJOpen:
De Mestral C, Laupacis A, Rotstein OD, Hoch JS, Haas B, Gomez D, Zagorski B, Nathens AB.
Early Cholecystectomy for Acute Cholecystitis: A Population-based Retrospective Cohort Study
of Variation in Practice. CMAJ Open. In press. 2013
Copyright for this manuscript in CMAJOpen is retained by the authors for noncommercial use.
43
4.1 Summary
Background
Despite evidence in favour of early cholecystectomy for most patients with acute
cholecystitis, variation in practice has been reported across hospitals worldwide. We sought to
characterize the extent and potential sources of variation in the performance of early
cholecystectomy for acute cholecystitis, within a large regional healthcare system.
Methods
We used a population-based retrospective cohort design. The cohort was limited to adults
with a first episode of acute cholecystitis, admitted through the emergency department. Patients
were identified using administrative databases comprising all emergency department visits and
hospital admissions in Ontario, Canada, from 2004 to 2010. Patient and hospital-level
characteristics associated with early cholecystectomy (within 7 days of emergency department
presentation) were identified using multilevel logistic regression.
Results
We identified 24,437 patients admitted to 106 hospitals with a first episode of acute
cholecystitis. A majority (58%, N=14,286) underwent early cholecystectomy. Rates of early
cholecystectomy varied widely across hospitals (median 51%, IQR 25%-72%), even among 18-
49 year old healthy patients with uncomplicated cholecystitis (median 74%, IQR 41%-88%). On
multivariable multilevel analysis, hospitals in the top quartile for acute cholecystitis admission
44
volume had the highest adjusted odds of early cholecystectomy and hospital effects accounted
for half of the explained variation in early cholecystectomy.
Conclusion
Across a large regional healthcare system’s hospitals, similar patients with acute
cholecystitis did not receive comparable care. Hospital-level factors, independent of patient
characteristics, appear strongly related to practice.
4.2 Background
Acute cholecystitis is a ubiquitous cause of hospitalization for gastrointestinal disease
and is definitively managed with cholecystectomy14,113.Randomized controlled trials, meta-
analyses and expert consensus support a practice of early laparoscopic cholecystectomy on first
hospital admission for most patients with acute cholecystitis, without severe sepsis49,60,76,84,114. In
fact, when compared to delaying cholecystectomy, early laparoscopic cholecystectomy within up
to 7 days of symptom onset is associated with a shorter total hospital length of stay and a similar
risk of conversion to open cholecystectomy60. Further support for early intervention can be
drawn from reports showing an approximately 20% risk of recurrent gallstone-related symptoms,
if delaying cholecystectomy15,60.
In spite of this evidence favouring early intervention, inconsistency in delivering what
many consider best practice has been reported worldwide. In fact, reports out of the United
Kingdom, Japan and the United States show rates of early cholecystectomy ranging from 36% to
88%69,70,81,82,88. However, because of differences in the setting and patient sample characteristics
across published studies, our understanding of the extent and underlying etiology of the
45
inconsistent application of early cholecystectomy remains circumstantial. We postulated that a
better understanding of the factors associated with the performance of early cholecystectomy
would provide opportunities to address the gap between evidence and practice. Our objective
was therefore to evaluate the extent of variation across hospitals in a large regional healthcare
system and, to identify patient and hospital characteristics associated with performing early
cholecystectomy.
4.3 Methods
Study design
This is a population-based retrospective cohort study of all adults with a first episode of
acute cholecystitis emergently admitted to an acute care hospital between April 1, 2004 and
March 31, 2010, in the province of Ontario, Canada. We compared rates of early
cholecystectomy across hospitals and used multivariable multilevel logistic regression to identify
patient and hospital characteristics associated with performing early cholecystectomy. This study
was approved by the Research Ethics Board of Sunnybrook Health Sciences Center.
Setting
This study used data from Ontario, Canada’s most populous province with over 13
million persons across 918,000 square kilometres. All hospital and physician services for Ontario
residents are paid by the provincial Ministry of Health. There are no private general hospitals in
Ontario.
Data sources
46
Patients were identified from the Canadian Institute for Health Information Discharge
Abstract Database, which contains demographic, diagnostic and procedural information on all
hospitalizations in Ontario. Admission via the emergency department was confirmed through
linkage to the National Ambulatory Care Reporting System database, which captures all
emergency department visits. To derive certain covariates (patient comorbidities and hospital
after-hours procedure volume), the Discharge Abstract Database was supplemented with data
from the Ontario Health Insurance Plan billing database that contains all physician claims. These
datasets were deterministically linked through a unique encrypted patient identifier and have
been validated for a variety of exposures and comorbidities91-94,98. In a multicenter validation
study, almost perfect agreement was found between Ontario’s Discharge Abstract Database and
reabstracted data for cholecystectomy coding and coding of gallstone disease as the most
responsible diagnosis98.
Study cohort
The cohort included residents of Ontario, 18 years of age or older, who were admitted to
hospital via the emergency department with a most responsible diagnosis of acute cholecystitis
(ICD-10-CA codes K80.0, K80.1, K80.4, K81.0, K81.8, K81.9). We restricted our analysis to
those with a first episode of acute cholecystitis and without other prior gallstone-related
admissions or emergency department visits in the two years preceding their index admission. We
also excluded patients directly admitted to an intensive care unit. Intensive care unit admission
was considered a surrogate for cholecystitis with severe sepsis, consistent with the Tokyo
guidelines definition of severe cholecystitis20. Patients who underwent cholecystostomy tube
placement were also excluded since this may suggest either severe cholecystitis, acalculous
47
cholecystitis or significant comorbidity that might preclude operative intervention at any time.
Less than 0.5% of patients were excluded due to missing covariate information.
There were two exclusions at the hospital level. First, we wished to exclude hospitals
where there was no general surgeon, because patients presenting to these hospitals could not
have had an early cholecystectomy. Since data on the availability of physicians at specific
hospitals were not directly available, we excluded hospitals where no appendectomy was
recorded over the six year study period. Appendectomy was chosen as the surrogate for surgeon
availability since appendicitis is common and is managed in the vast majority of cases with
urgent appendectomy if surgical expertise is available. Finally, to provide more robust estimates
of rates, we also excluded hospitals with fewer than 5 patients meeting entry criteria per study
year. These two criteria resulted in the exclusion of 52 of 158 hospitals.
Outcome measure
The primary outcome of interest was early cholecystectomy, defined as cholecystectomy
within 7 days of emergency department presentation.
Patient and hospital-level characteristics
Several patient and hospital-level characteristics were considered as potential explanatory
variables influencing the performance of early cholecystectomy. Patient-level characteristics
included age, sex, income level, comorbidity level, concomitant common bile duct obstruction
and pancreatitis. Income quintile was used as crude surrogate for socioeconomic status and was
derived from the median household income of the patient’s postal code of residence based on
2001 and 2006 census data115. Comorbidity level was captured using the John Hopkins
Aggregated Diagnosis Group scoring system116.Using inpatient and outpatient records in the two
48
years preceding the index admission, an Aggregate Diagnosis Group-based comorbidity index
was calculated according to an algorithm validated for the prediction of 1 year mortality in a
large cohort of adult Ontarians96,97.
The hospital-level characteristics we considered included teaching status (academic
teaching / non-teaching) as recognized by the Ontario Ministry of Health117, annual volume of
acute cholecystitis admissions (quartiles) and, annual volume of elective cholecystectomies
(quartiles). We also considered the possibility that a hospital’s policy regarding the use of
operating room resources after hours (evenings, nights and weekends) or operating room
availability might influence the likelihood of early cholecystectomy. Therefore, as a standardized
measure of operating room utilization after hours, we derived a variable corresponding to the
ratio of total after-hours operative cases (for all surgical specialties) divided by the number of
all-cause emergency department visits. Lower values are indicative of lesser after-hours
operating room utilization.
Statistical analysis
Exploration of variation across hospitals
We first calculated the crude rate of early cholecystectomy at each hospital for all
patients. To better understand the source of variation, we also explored rates across hospitals for
young healthy patients (<50 years old in lowest comorbidity quartile) with uncomplicated
disease (without common bile duct obstruction or pancreatitis). Variation across hospitals is
presented using funnel plots in which each hospital’s early cholecystectomy rate is plotted
against their volume of acute cholecystitis admissions. The funnel plots graphically show
whether the variation in the rate of early cholecystectomy across hospitals is in excess or within
49
the range expected based on chance alone. Ninety-nine percent control limits frame the range of
random variation around the overall cholecystectomy rate and are defined as exact binomial
confidence intervals that vary as a function of the volume of acute cholecystitis admissions118. A
hospital outside the control limits is therefore interpreted as having an early cholecystectomy rate
outside the range of random variation that would be expect based on chance alone.
Exploration of factors associated with early cholecystectomy
We then evaluated the association of patient and hospital characteristics with early
cholecystectomy using multilevel (two-level) logistic regression, which accounted for the non-
independence of patients admitted to the same hospital104. Model calibration was examined
through observed versus predicted outcome plots and discrimination was quantified with the c-
statistic.
To evaluate the relative importance of hospital characteristics and patient case-mix, we
compared the proportion of explained outcome variation in the multilevel logistic model with
patient and hospital-level characteristics to a standard logistic model containing only the patient-
level covariates. Each model’s respective proportion of explained outcome variation was
calculated as the squared Pearson correlation coefficient between the probabilities of early
cholecystectomy predicted by the model and the observed outcomes119,120.
In addition, the multilevel model was used to quantify the extent of variation between
hospitals, adjusted for differences in patient case-mix, by calculating the median odds ratio121.
The median odds ratio is the median value of all possible ratios of the odds of cholecystectomy
in two patients with the same covariates admitted to two randomly selected, distinct hospitals. By
convention, the odds of the patient at the hospital with the highest propensity for
50
cholecystectomy is used as the numerator of the ratio, such that the median odds ratio is always
greater or equal to 1. As an example, a median odds ratio of 3.0 suggests a threefold median
difference in the odds of early cholecystectomy for two similar patients admitted to distinct
randomly selected hospitals. The median odds ratio can also be directly compared to the fixed
effects in the study (e.g. patient age, sex, etc.) thereby informing a meaningful interpretation of
its magnitude.
All analyses were performed using SAS 9.2. Given the large sample size, a two-tailed α
<0.01 was considered statistically significant.
4.4 Results
Study cohort
We identified 24,437 patients admitted to 106 hospitals with a first episode of acute
cholecystitis who met inclusion criteria (figure 4.1). The median number of patients per hospital
was 196 (IQR 71 – 357). Teaching hospitals comprised 13% of all hospitals and cared for 21%
of all patients. The cohort was evenly distributed across study years. Over half of patients were
female (59%) and the mean age was 56±18 years. Concurrent common bile duct obstruction and
pancreatitis were present in 11% and 5% of patients, respectively. Overall, 14,286 (58%)
patients underwent early cholecystectomy.
Variation in the rate of early cholecystectomy across hospitals
There was marked variation in the rate of early cholecystectomy across hospitals: median
51%, IQR 25% to 72%. This variation remained evident even when limited to young (<50 years)
51
healthy (lowest comorbidity quartile) patients with uncomplicated disease (without CBD
obstruction or pancreatitis): median early cholecystectomy rate 74%, IQR 41%-88%. In the full
cohort and in the younger healthy subgroup, the variation in early cholecystectomy was in excess
of that expected by chance alone as evidenced by the large number of hospitals lying outside the
ninety-nine percent control limits shown in the funnel plots (figures 4.2 and 4.3). In other words,
the funnel plots suggest that factors other than chance explain the extent of variation. As expect,
there was less variation within the more homogeneous younger subgroup as evidenced by a
smaller proportion of hospitals lying outside the control limits (figure 4.3).
A broad range in early cholecystectomy rates was also seen across hospitals with similar
characteristics: teaching hospitals (median 47%, IQR 27%-54%), hospitals in the top volume
quartile of elective cholecystectomies (median 54%, IQR 35%-79%) and, hospitals in the top
quartile of OR utilization after hours (median 60%, IQR 46%-77%).
Association of patient and hospital-level characteristics with early cholecystectomy
On univariable analysis, patients who were younger, female, with a lower comorbidity
burden and without common bile duct obstruction were more likely to undergo early operative
intervention (Table 4.1). As well, patients admitted to non-teaching hospitals, hospitals that had
high operating room utilization after hours and, hospitals that had a high institutional volume of
acute cholecystitis admissions and elective cholecystectomies, were more likely to undergo early
cholecystectomy (Table 4.2).
On multivariable multilevel analysis, the same patient-level associations with early
cholecystectomy remained and, at the hospital level, a high volume of acute cholecystitis
admissions was associated with increased odds of early cholecystectomy (Table 4.3). Albeit

52
significant, the level of OR utilization after hours showed an inconsistent association with
performance of early cholecystectomy. The model showed good discrimination (c-statistic=0.80)
and calibration.
We then used the multilevel model to quantify the extent of variability between hospitals,
adjusted for differences in patient case-mix, by calculating the Median Odds Ratio (MOR). The
MOR for the model was 3.7, which can be interpreted as a nearly 4-fold median difference in the
odds of early cholecystectomy for two similar patients admitted to randomly selected hospitals.
Finally, we apportioned the explained outcome variation between patient and hospital
level effects as described in the methods section. Our multilevel model explained 53% of the
variation in the frequency of early cholecystectomy. Of this explained variation, about half
(27%) could be attributed to hospital-level effects, and half (26%) to patient-level effects.
4.5 Discussion
In this population-based study evaluating the practice of early cholecystectomy for acute
cholecystitis, we demonstrated significant variation across hospitals, even when considering only
young, healthy patients with uncomplicated disease. Our analysis suggests that two similar
patients presenting to randomly selected hospitals have an almost 4-fold median difference in
their respective odds of early cholecystectomy. Furthermore, hospital effects, as opposed to
patient effects, accounted for half of the explained variation in early cholecystectomy. Admission
to a hospital with a high acute cholecystitis admission volume was associated with the highest
rate of early intervention.

53
Best available evidence supports early over delayed laparoscopic cholecystectomy for
most patients with acute cholecystitis, based on findings of a shortened total hospital stay, a
similar conversion rate and the elimination of the risk of recurrent gallstone symptoms associated
with delayed elective cholecystectomy60.While trials comparing early to delayed
cholecystectomy were published between 1998 and 2005, inconsistency in the practice of early
cholecystectomy remains evident across different practice environments internationally, with
reported early cholecystectomy rates ranging from 36% to 88%69,70,81,82,88. Previous studies have
also shown that, in those 66 years of age or older, early cholecystectomy is less likely in patients
of greater age and comorbidity level and that early cholecystectomy is less likely with limited
insurance status in the United States69,88.Other determinants of management identified in surveys
of physicians include the surgeon’s competing elective clinical obligations, the surgeon’s
comfort with laparoscopy, as well as the availability of hospital resources for emergency
surgery77,78,122.While we found patient characteristics associated with management that are
consistent with the prior literature, our study also described the wide extent of variation across
hospitals within a large regional healthcare system and quantified the importance of hospital-
level effects as a source of variation in practice.
While many hospitals are providing early cholecystectomy for most patients in Ontario,
we have shown that similar patients managed at different hospitals did not receive comparable
care. We postulate that these results may in part be related to logistic barriers to early
cholecystectomy at certain institutions. Variation across hospitals in the management of acute
cholecystitis may be reduced in the future because of a recent focus on the efficient delivery of
emergency surgical care. This focus includes the American College of Surgeons’ support for the
emerging field of acute care surgery as well as the Royal College of Surgeons of England’s
promotion of the separation of emergency and elective surgery practice123,124. Initiatives targeting
54
better delivery of emergency surgical care, including a dedicated service for emergency surgery
referrals, a surgeon-of-the-week practice model, and operating room time during the day
dedicated to emergency cases, are likely to facilitate early cholecystectomy. In fact, recent
evidence supports a dedicated emergency surgery team as the catalyst for more efficient
management of gallstone disease125-129.
In addition, variation in practice may in part reflect the need to address remaining gaps in
the evidence comparing the outcomes of early and delayed cholecystectomy. In fact, one of the
factors hindering the uptake of early cholecystectomy may be concern that early intervention is
associated with a higher rate of major bile duct injury, a rare but devastating operative
complication. Adequately powered studies assessing whether this is true, as well as a comparison
of real world rates of conversion from laparoscopic to open cholecystectomy are required.
Strengths and limitations
The main strengths of this study include its population-based scope, the quality of the
data sources, as well as the study setting - a health care system where emergency surgical care is
only accessed through single-payer funded public hospitals. However, the study also has
limitations. The first is potential residual confounding related to the severity of cholecystitis. We
attempted to reduce this potential bias by excluding patients with severe cholecystitis and prior
gallstone disease. While a gradient of severity (captured by duration of symptoms, white blood
cell count, gallbladder wall thickness on ultrasound) is likely present in our study cohort, it is
reasonable to expect that this gradient be similarly distributed across hospitals, particularly after
adjusting for age, sex, socioeconomic status and comorbidity level. Furthermore, we believe the
extent of variation across hospital is too large to be fully explained by unmeasured differences in
cholecystitis severity. The second limitation is that we are unable to identify the decision-making
55
surgeon in our data sources. Nevertheless, many surgeon characteristics such as physician
practice type and cholecystectomy volumes would be expected to overlap with the hospital
characteristics we included. As such, the measured hospital effects are likely partly attributable
to the hospital’s surgeons and characterizing the relative importance of surgeon-level variation in
practice merits further investigation. Despite this limitation, understanding variation at the
hospital-level remains a constructive starting point to generate solutions for quality
improvement. Finally, definitions of the timeframe for early cholecystectomy range in the
literature between 24 hours and 7 days from symptom onset or diagnosis. While we chose a
broad timeframe definition (within 7 days from emergency department presentation), when we
defined early cholecystectomy as occurring within 3 days of emergency department presentation,
we found the same extent of variation and similar associations on multivariable analysis.
In conclusion, we have presented a population-based analysis of the management of acute
cholecystitis within a geographic region where all emergency surgical care is accessed from a
single public payer. We have found considerable variation in the rate of early cholecystectomy
across hospitals and also shown that, across these hospitals, similar patients with acute
cholecystitis did not receive comparable care. Hospital-level factors, independent of patient
characteristics, appear strongly related to practice.
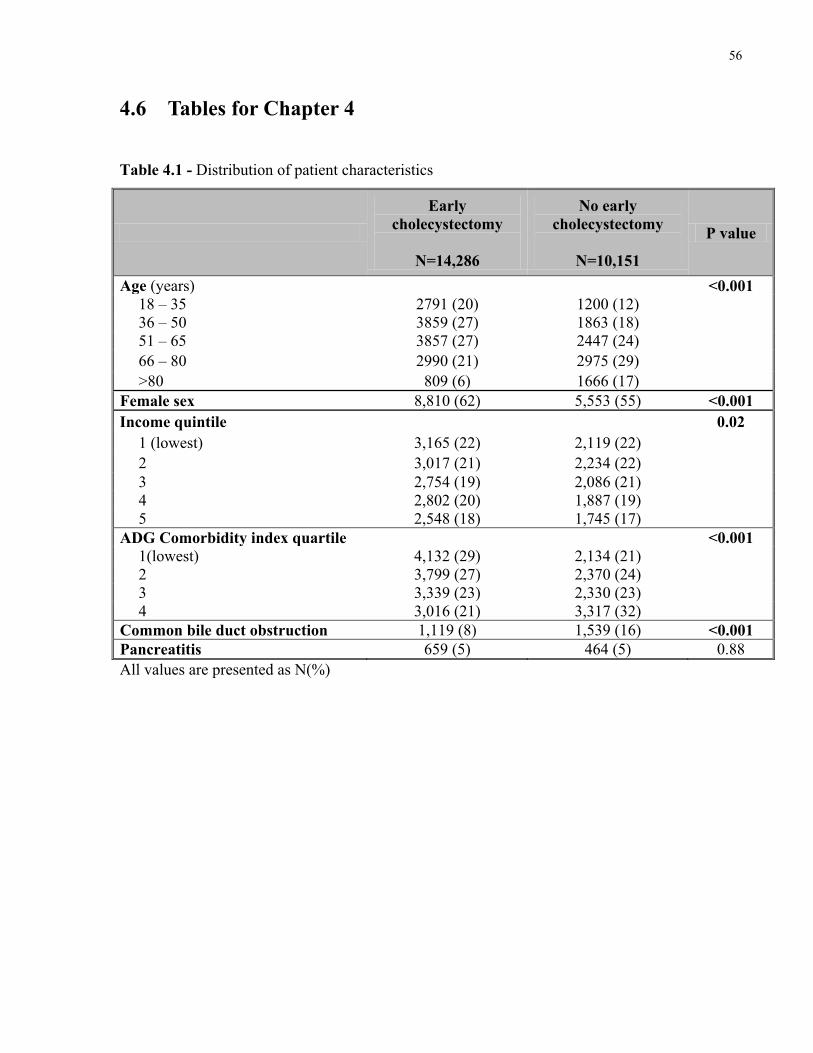
56
4.6 Tables for Chapter 4
Table 4.1 - Distribution of patient characteristics
Early cholecystectomy
N=14,286
No early cholecystectomy
N=10,151
P value
Age (years) <0.001 18 – 35 2791 (20) 1200 (12) 36 – 50 3859 (27) 1863 (18) 51 – 65 3857 (27) 2447 (24) 66 – 80 2990 (21) 2975 (29) >80 809 (6) 1666 (17)
Female sex 8,810 (62) 5,553 (55) <0.001 Income quintile 0.02
1 (lowest) 3,165 (22) 2,119 (22) 2 3,017 (21) 2,234 (22) 3 2,754 (19) 2,086 (21) 4 2,802 (20) 1,887 (19) 5 2,548 (18) 1,745 (17)
ADG Comorbidity index quartile <0.001 1(lowest) 4,132 (29) 2,134 (21) 2 3,799 (27) 2,370 (24) 3 3,339 (23) 2,330 (23) 4 3,016 (21) 3,317 (32)
Common bile duct obstruction 1,119 (8) 1,539 (16) <0.001 Pancreatitis 659 (5) 464 (5) 0.88 All values are presented as N(%)
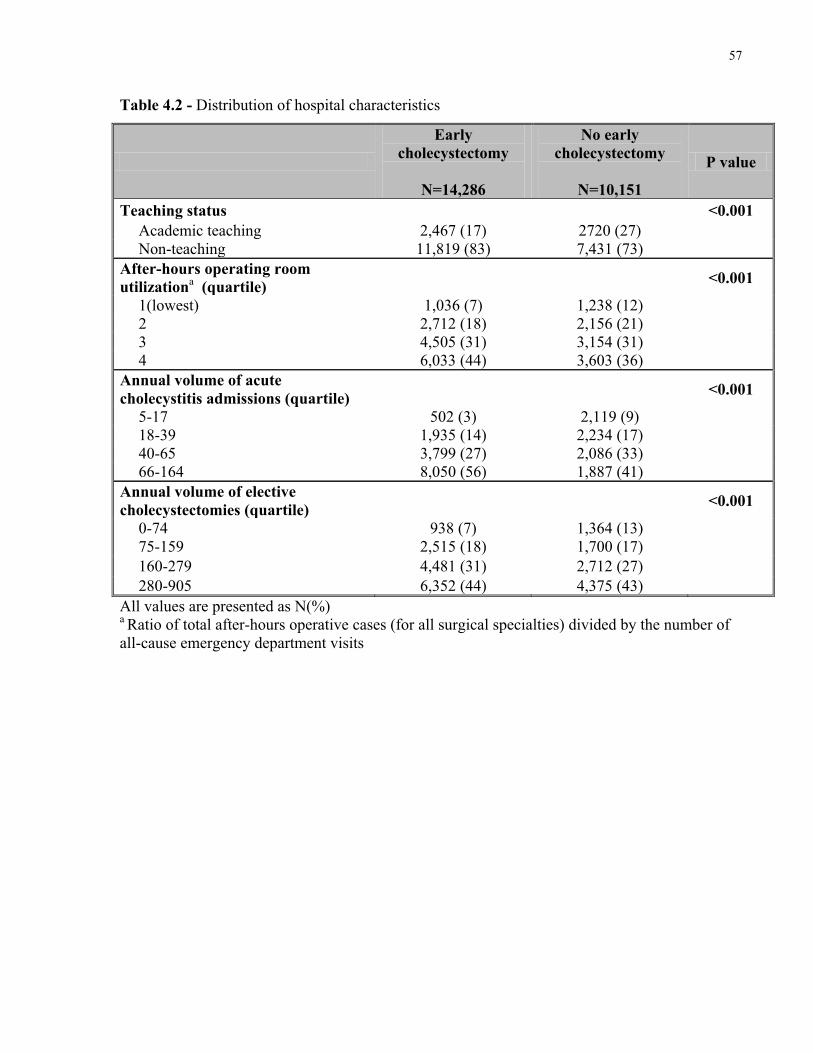
57
Table 4.2 - Distribution of hospital characteristics
Early cholecystectomy
N=14,286
No early cholecystectomy
N=10,151
P value
Teaching status <0.001 Academic teaching 2,467 (17) 2720 (27) Non-teaching 11,819 (83) 7,431 (73)
After-hours operating room utilizationa (quartile) <0.001
1(lowest) 1,036 (7) 1,238 (12) 2 2,712 (18) 2,156 (21) 3 4,505 (31) 3,154 (31) 4 6,033 (44) 3,603 (36)
Annual volume of acute cholecystitis admissions (quartile)
<0.001
5-17 502 (3) 2,119 (9) 18-39 1,935 (14) 2,234 (17) 40-65 3,799 (27) 2,086 (33) 66-164 8,050 (56) 1,887 (41)
Annual volume of elective cholecystectomies (quartile) <0.001
0-74 938 (7) 1,364 (13) 75-159 2,515 (18) 1,700 (17) 160-279 4,481 (31) 2,712 (27) 280-905 6,352 (44) 4,375 (43)
All values are presented as N(%) a Ratio of total after-hours operative cases (for all surgical specialties) divided by the number of all-cause emergency department visits

58
Table 4.3 - Multilevel multivariable logistic regression results showing association of patient and hospital characteristics with early cholecystectomy
Characteristic Adjusted Odds Ratio (99% CI)
Patient Age (years)
18 – 35 Reference 36 – 50 0.92 (0.81 – 1.05) 51 – 65 0.69 (0.61 – 0.79) 66 – 80 0.46 (0.40 – 0.53) >80 0.21 (0.18 – 0.25)
Male sex 0.87 (0.80 – 0.95) Income quintile
1(lowest) Reference 2 0.98 (0.87 – 1.10) 3 0.93 (0.82 – 1.05) 4 1.06 (0.94 – 1.21) 5 1.12 (0.98 – 1.27)
ADG Comorbidity index quartile 1(lowest) Reference 2 0.90 (0.80 – 1.01) 3 0.89 (0.79 – 1.00) 4 0.67 (0.60 – 0.75)
Common bile duct obstruction 0.41 (0.36 – 0.47) Pancreatitis 1.14 (0.94 – 1.37) Hospital Annual volume of acute cholecystitis admissions (quartile)
5-17 0.53 (0.35 – 0.78) 18-39 0.67 (0.52 – 0.87) 40-65 0.84 (0.72 – 0.97) 66-164 Reference
After-hours operating room utilizationa (quartile) 1(lowest) 0.97 (0.72 – 1.30) 2 0.84 (0.66 – 1.07) 3 0.79 (0.64 – 0.97) 4 Reference
Annual volume of elective cholecystectomies (quartile) 0-74 1.02 (0.63 – 1.63) 75-159 1.15 (0.82 – 1.60) 160-279 1.11 (0.91 – 1.35) 280-905 Reference
Academic teaching hospital 0.71 (0.27 – 1.85) aRatio of total after-hours operative cases (for all surgical specialties) divided by the number of all-cause emergency department visits
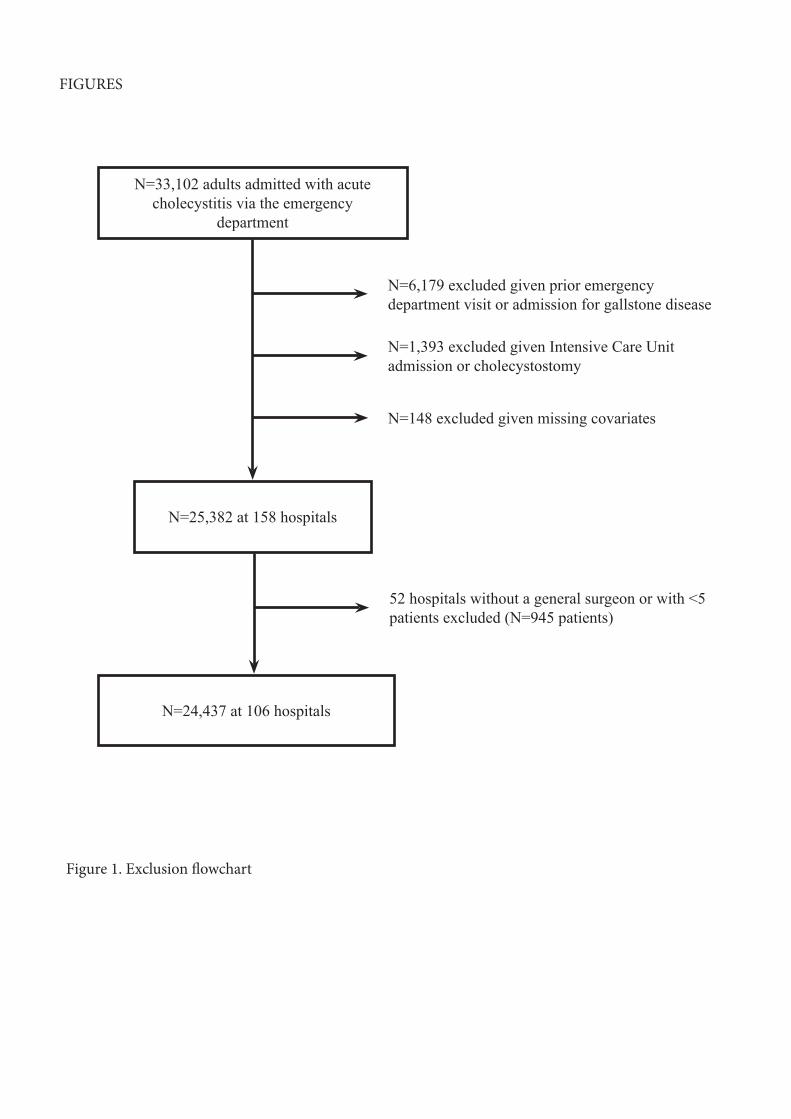
N=33,102 adults admitted with acute cholecystitis via the emergency
department
N=25,382 at 158 hospitals
N=24,437 at 106 hospitals
N=6,179 excluded given prior emergency department visit or admission for gallstone disease
N=1,393 excluded given Intensive Care Unit admission or cholecystostomy
N=148 excluded given missing covariates
52 hospitals without a general surgeon or with <5 patients excluded (N=945 patients)
FIGURES
Figure 1. Exclusion flowchart
Charles
Rectangle
Charles
Text Box
4.7 Figures for Chapter 4
Charles
Text Box
Figure 4.1 - Patient eligibility flowchart
Charles
Text Box
59
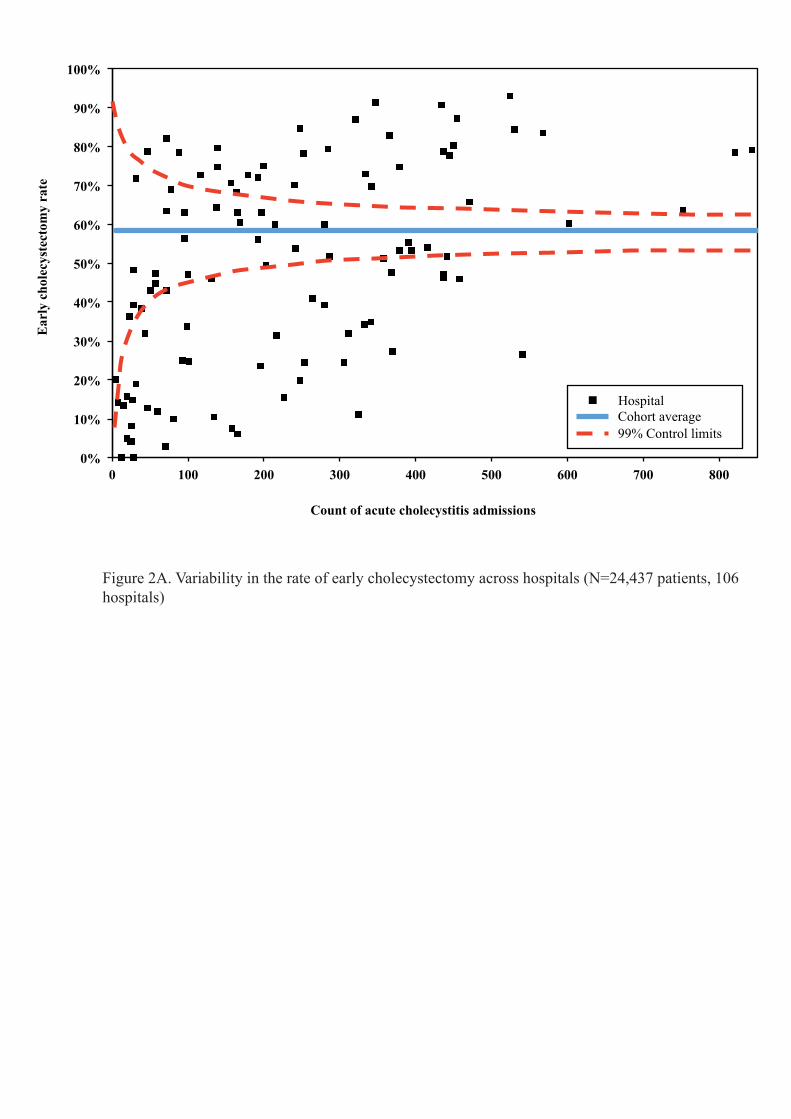
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 100 200 300 400 500 600 700 800
Ear
ly c
hole
cyst
ecto
my
rate
Count of acute cholecystitis admissions
Hospital Cohort average 99% Control limits
Figure 2A. Variability in the rate of early cholecystectomy across hospitals (N=24,437 patients, 106 hospitals)
Charles
Rectangle
Charles
Text Box
60
Charles
Text Box
Figure 4.2 - Variation in the rate of early cholecystectomy across hospitals (N=24,437 patients, 106 hospitals)

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 20 40 60 80 100 120 140 160
Ear
ly c
hole
cyst
ecto
my
rate
Count of acute cholecystitis admissions
Hospital Cohort average 99% Control limits
Figure 2B. Variability in the rate of early cholecystectomy rate across hospitals among young (<50 years) healthy patients without concurrent biliary tract obstruction or pancreatitis (N=2,894 patients, 102 hospitals)
Charles
Rectangle
Charles
Text Box
61
Charles
Text Box
Figure 4.3 - Variation in the rate of early cholecystectomy rate across hospitals among young (<50 years) healthy patients without concurrent biliary tract obstruction or pancreatitis (N=2,894 patients, 102 hospitals)
62
Chapter 5
Risk of Recurrent Symptoms if Cholecystectomy is Delayed
The purpose of this chapter is to:
I. Present the frequency of recurrent gallstone-related symptoms if discharged without
cholecystectomy.
II. Identify patient subgroups at highest risk of recurrent symptoms.
Preamble
The contents of this chapter have been published in the Journal of Trauma and Acute Care
Surgery:
de Mestral C, Rotstein OD, Laupacis A, Hoch JS, Zagorksi B, Nathens AB. The clinical course
of 10,304 patients with acute cholecystitis discharged without cholecystectomy. Journal of
Trauma and Acute Care Surgery. 2013; 74: 26-31
© Wolters Kluwer. The use of the manuscript is by permission of the copyright holder.
63
5.1 Summary
Background
Randomized trials and expert opinion support early laparoscopic cholecystectomy for
most patients with acute cholecystitis; however, practice patterns are variable worldwide and
delayed cholecystectomy remains a common practice. We therefore present a population-based
analysis of the risk of recurrent gallstone-related symptoms in patients with acute cholecystitis
discharged without cholecystectomy.
Methods
Using administrative databases capturing all ED visits and hospital admissions within a
geographic region encompassing 13 million persons, we identified adults with a first emergency
admission for uncomplicated acute cholecystitis over the period of 2004-2011. In those
discharged without cholecystectomy, the probability of a subsequent gallstone-related event
(gallstone-related ED visit or hospital admission) was evaluated using the Kaplan-Meier method.
The association of patient characteristics with time to first gallstone related event after discharge
was explored through multivariable time-to-event analysis.
Results
10,304 of 25,397 patients with acute cholecystitis (41%) did not undergo
cholecystectomy on first admission. The probability of a gallstone-related event by 6 weeks, 12
weeks and 1 year after discharge was 14%, 19% and 29% respectively. Of these events, 30%
were for biliary tract obstruction or pancreatitis. When controlling for sex, income and
comorbidity level, the risk of a gallstone-related event was highest in patients 18 to 34 years old.
64
Conclusions
In patients who do not undergo cholecystectomy on first admission for acute
cholecystitis, the probability of a gallstone-related ED visit or hospital admission within 12
weeks of discharge is 19%. The increased risk in younger patients reinforces the value of early
cholecystectomy in the non-elderly.
5.2 Background
Randomized trials and expert opinion support early laparoscopic cholecystectomy within
up to 7 days of symptom onset for most patients with acute cholecystitis22,60,65-67,114,130.
Nevertheless, early cholecystectomy rates reported worldwide vary from 36% to 88%,
suggesting that delayed cholecystectomy remains a common practice at many
institutions69,70,81,82,88. One of the strongest arguments against delayed cholecystectomy is that, in
the interval between discharge and delayed elective cholecystectomy, patients are at risk of
recurrent gallstone-related symptoms. Existing data suggest that the frequency of recurrent
symptoms post discharge is in the range of 0% to 38% 65-67,69,130,131. Small study samples, single
centre analyses and data sources limited to specific patient subgroups are limitations of these
studies65-67,69,130,131. Accurate estimates that can be generalized to a broad population of adults are
needed to inform clinical and resource allocation decisions about the management of acute
cholecystitis. Therefore, the objectives of this study were to determine the frequency of recurrent
gallstone-related symptoms using population-based data, as well as to identify patient subgroups
at highest risk of recurrent symptoms.

65
5.3 Methods
Study design and setting
This is a population-based retrospective cohort study of the clinical course of adults
admitted with a first episode of acute cholecystitis and discharged without undergoing
cholecystectomy. We used data from Ontario, Canada’s most populous province with over 13
million residents. Funding for all medically necessary hospital and physician services accessed
by Ontario residents is solely provided by the provincial Ministry of Health. This study was
approved by the Research Ethics Board of Sunnybrook Health Sciences Center.
Data sources
The cohort was identified from administrative datasets housed and consolidated at the
Institute for Clinical Evaluative Sciences, Toronto, Canada. Diagnostic and procedural
information was obtained from the Discharge Abstract Database (DAD) that contains data about
all hospital admissions in Ontario, and the National Ambulatory Care Reporting System
(NACRS) that includes data about all Emergency Department (ED) visits and same day
surgeries. Demographic data and date of death were obtained from the Registered Person
Database (RPDB). An encrypted unique patient identifier allows these datasets to be
deterministically linked, thereby providing an accurate record of patients’ clinical trajectories.
Cohort
66
All Ontario residents, admitted via the ED from April 2004 to March 2011 with a most
responsible diagnosis of acute cholecystitis (ICD-10-CA codes K80.00, K80.01, K80.10,
K80.11, K81.0, K81.8, K81.9) were considered for inclusion in the cohort. We identified patients
with a first episode of AC by excluding those with an ED visit or hospital admission for
gallstone disease in the 2 years preceding the index admission. We also excluded patients with
complicated cholecystitis, namely: those with a concurrent diagnosis of pancreatitis or common
bile duct obstruction, those with severe cholecystitis as evidence by direct admission to an
intensive care unit and those who underwent cholecystostomy tube placement. The remaining
patients that survived to hospital discharge and did not undergo cholecystectomy on their index
admission comprised the final cohort.
Outcome
The outcome of interest was time to first gallstone-related event. A gallstone-related
event was defined as any ED visit or hospital admission for biliary colic, recurrent acute
cholecystitis, choledocholithiasis, cholangitis, biliary pancreatitis or gallstone ileus. All ED visits
and hospital admissions between the date of hospital discharge and date of maximum follow-up
were searched. Identification of gallstone-related events was limited to the main diagnosis field
for ED visits and to the most responsible and post-admission comorbidity fields for hospital
admissions. If a hospital admission included two or more gallstone diagnoses (e.g. cholecystitis
and pancreatitis), the gallstone-related event was classified based on the diagnosis with greatest
potential morbidity (i.e. pancreatitis).
67
Patient characteristics
Risk of recurrent gallstone-related symptoms across patient subgroups was examined
based on the following patient characteristics: age, sex, comorbidity level and income quintile.
Used as a crude proxy for socioeconomic status, income quintile reflects the median household
income in a patient’s postal code of residence based on 2001 or 2006 Canada census data 115.
The John Hopkins Aggregate Diagnosis Groups (ADG) system was used to quantify the level of
comorbidity based on inpatient and outpatient records in the 2 years preceding the index
cholecystitis admission116. From this grouping system, an ADG-based comorbidity index was
calculated according to an algorithm validated for the prediction of 1 year mortality in a large
cohort of adult Ontarians96,97.
Statistical Analysis
First, the probability of a gallstone-related event by clinically meaningful time points
following discharge was calculated using the Kaplan-Meier method (1 minus the product limit
value). Patients who underwent elective cholecystectomy, who died or who reached the maximal
follow-up date prior to any gallstone-related event were censored. Cholecystectomy was
considered elective if performed as same day surgery, or on an inpatient admission without an
associated ED visit. Any admission for gallstone disease involving a cholecystectomy but with
an associated ED visit was considered an admission for a recurrent gallstone-related event.
Second, in order to understand which patient subgroups might be at greater risk of
recurrent gallstone symptoms, we performed univariable comparisons with the log-rank test as
well as developed a Cox proportional-hazard model. This multivariable time to event analysis
68
was used to describe the association of all the previously listed patient characteristics with time
to first gallstone-related event. The proportional hazards assumption was evaluated graphically
by plotting logarithm-minus-logarithm survival curves105. Given the large sample size, alpha was
set at 0.01.
As a secondary analytic approach, competing risk time-to-event analysis was undertaken.
In doing so the cumulative incidence method was used to derive the probability of a gallstone-
related event over time. As discussed in Chapter 3, unlike the Kaplan-Meier method, the
cumulative incidence approach accounts for the competing nature of a censoring event107,108. In
this secondary analysis, death and elective cholecystectomy were treated as informative
competing risks.
5.4 Results
Study cohort
Of 25,397 patients admitted with a first episode of uncomplicated acute cholecystitis
meeting inclusion criteria, 10,304 (41%) were discharged without undergoing cholecystectomy.
The majority (54%, N=5,550) were female and the median age was 62 years (IQR 47-76 years).
The cohort was evenly distributed across study years.
Median follow-up was 3.4 years (IQR 1.7-5.1). Over the interval of follow-up, 2,479
(24%) patients had an observed gallstone-related ED visit or admission. Median time to first
event was 78 days with 88% (N=2,177) of events occurring within 1 year of discharge. A total of
4,617(45%) underwent elective cholecystectomy and an additional 733 (7%) patients died prior
69
to any gallstone-related event. Median times to elective cholecystectomy and death were 8 weeks
(IQR 5-13 weeks) and 14 months (IQR 4-30 months) respectively.
Frequency of gallstone-related ED visit or admission
The probability of a gallstone-related event by 6 and 12 weeks following discharge was
14% and 19% respectively (Table 5.1). Of the patients with a gallstone-related event within 12
weeks of discharge, over two thirds presented with recurrent cholecystitis or biliary colic (70%)
with the remaining patients presenting with biliary tract obstruction (24%) or pancreatitis (6%).
A similar distribution of event type was found by 1 year, with an additional small proportion of
first gallstone-related ED visits or admissions (<1%) due to gallstone ileus. In those patients
readmitted for AC or biliary colic and in those with pancreatitis, biliary obstruction or gallstone
ileus, in-hospital mortality was 1.6% and 1.4% respectively (p=0.77).
Risk of gallstone-related ED visit or admission
Differences in the risk of a gallstone-related event were found across age groups (Figure
5.1). For example, the probability of a first gallstone-related event by 12 weeks following
discharge was 30% in patients between the ages of 18 and 35, compared to only 14% in those 80
years of age or older (p<0.001). No difference in the type of gallstone-related event was seen
across age groups. On multivariable analysis, when controlling for sex, comorbidity level and
income, younger patients remained at greatest risk throughout the first year following discharge
from hospital (Table 5.2). No difference in the probability of recurrent gallstone symptoms was
seen between sexes or across comorbidity and income levels.
70
Secondary analysis
When treating death and elective cholecystectomy as competing risks, the probability of a
gallstone-related event over time was not meaningfully different from the primary analysis
(Table 5.3) and a higher risk of a gallstone-related event was also observed in younger patients
(Table 5.4).
5.5 Discussion
This study of the clinical course of patients with acute cholecystitis discharged without
cholecystectomy demonstrates three main findings. First, by 12 weeks from discharge, the time
interval conventionally used for delayed elective cholecystectomy after an episode of acute
cholecystistis, the risk of a gallstone-related ED visit or hospital admission was 19%. Second, in
those who had recurrent symptoms, nearly 30% presented with biliary tract obstruction or
pancreatitis, diseases with greater morbidity potential than the initial cholecystitis episode. Third,
the risk of recurrent gallstone-related ED visit or hospital admission decreased with age.
In randomized trials comparing early to delayed intervention, 0% to 37% of patients
randomized to delayed treatment had non-resolving or recurrent gallstone symptoms65-67,130,131.
In a large cohort study of patients with acute cholecystitis aged 65 and older, Riall and
colleagues reported a 38% probability of gallstone-related readmission by 2 years after
discharge69. The same study also demonstrated a higher risk of recurrent symptoms in the
youngest patients of the cohort.
71
Our results are consistent with the existing literature, but provide estimates of the risk of
recurrent symptoms that were derived from a broad population of adults with acute cholecystitis.
Furthermore, this analysis demonstrates that a relatively large proportion of patients return with
biliary tract obstruction or pancreatitis, which carry significant potential for added morbidity.
These data are critical for informed decision-making with patients, concerning delayed
cholecystectomy as a management strategy. That an age-related gradient in risk of recurrent
symptoms was also found by Riall reinforces the validity of our similar finding, although our
data cannot explain the underlying reasons for such differences in risk across ages. It may be that
diet, genetics and anatomy contribute to the development of acute cholecystitis early in life in
these younger patients, who then remain at increased risk of recurrent symptoms. Another
possible explanation is that younger patients were more prone to seek medical attention. The
higher risk of symptomatic disease in younger patients, and the lower risk in those older than 80
years of age, can inform decision making about the benefits and risks of early cholecystectomy
in these patients. Most clearly, these results reinforce the value of early cholecystectomy in the
non-elderly.
Strengths of this study are its population-based scope, large sample size and the capture
of emergency department visits in addition to admissions. However, its limitations must be
recognized. First, the increased risk of recurrent gallstone disease in younger patients may be
partially attributable to unmeasured characteristics such as dietary intake, body mass index,
genetic factors, biliary anatomy or differences in cholecystitis severity. Second, our results may
slightly overestimate the probability of recurrent gallstone disease if pre-admission cholecystitis
was erroneously coded as a post-admission comorbidity on a subsequent visit. However, when
we restricted the outcome definition to only the most-responsible diagnosis field for subsequent
emergency department visits and admissions, the estimates of recurrent symptoms were not

72
meaningfully lower from those in table 5.1 and adjusted risks across patient characteristics were
similar to those presented in table 5.2. Finally, while we were able to capture all emergency
department visits and hospitals admissions in Ontario, we did not capture outpatient clinic visits
to a family physician for gallstone-related symptoms and therefore may slightly underestimate
the probability of recurrent symptoms.
In conclusion, this population-based analysis characterizes the risk of recurrent gallstone
symptoms in a large cohort of patients who presented with a first episode of acute cholecystitis
and were discharged without cholecystectomy. The probability of a gallstone-related emergency
department visit or hospital admission within 12 weeks of discharge was 19%. The increased risk
in younger patients reinforces the value of early cholecystectomy in the non-elderly.
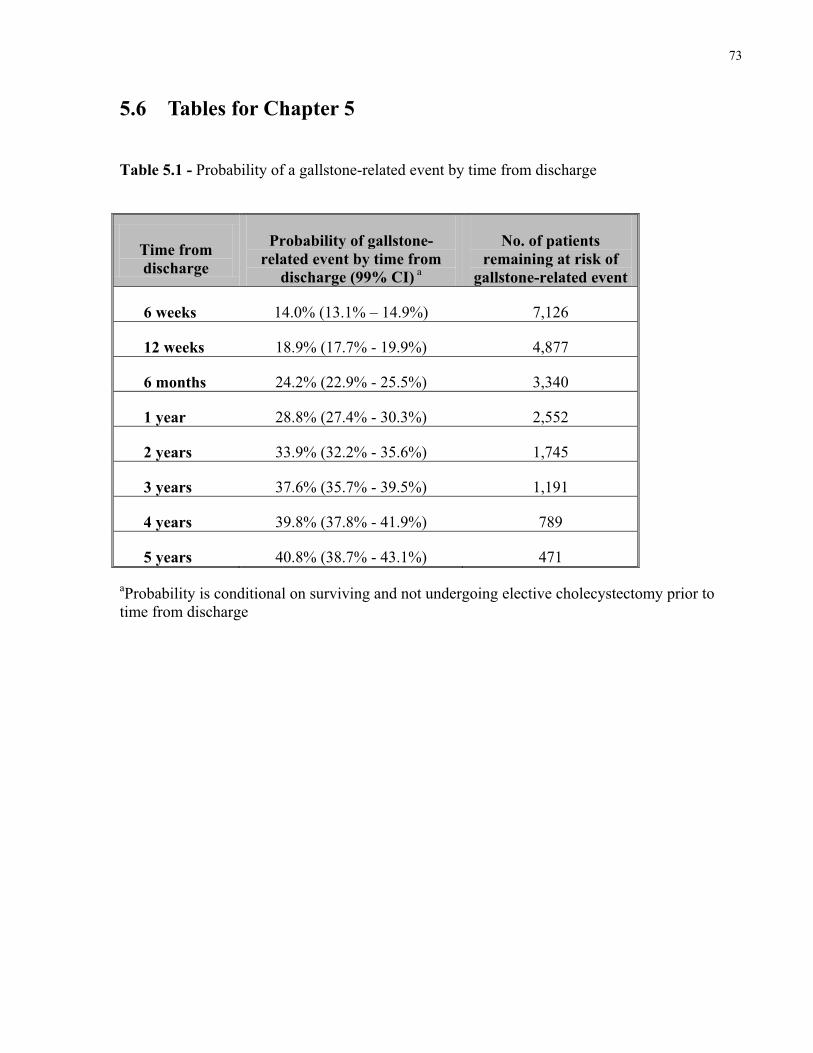
73
5.6 Tables for Chapter 5
Table 5.1 - Probability of a gallstone-related event by time from discharge
Time from discharge
Probability of gallstone-related event by time from
discharge (99% CI) a
No. of patients remaining at risk of
gallstone-related event
6 weeks 14.0% (13.1% – 14.9%) 7,126
12 weeks 18.9% (17.7% - 19.9%) 4,877
6 months 24.2% (22.9% - 25.5%) 3,340
1 year 28.8% (27.4% - 30.3%) 2,552
2 years 33.9% (32.2% - 35.6%) 1,745
3 years 37.6% (35.7% - 39.5%) 1,191
4 years 39.8% (37.8% - 41.9%) 789
5 years 40.8% (38.7% - 43.1%) 471
aProbability is conditional on surviving and not undergoing elective cholecystectomy prior to time from discharge
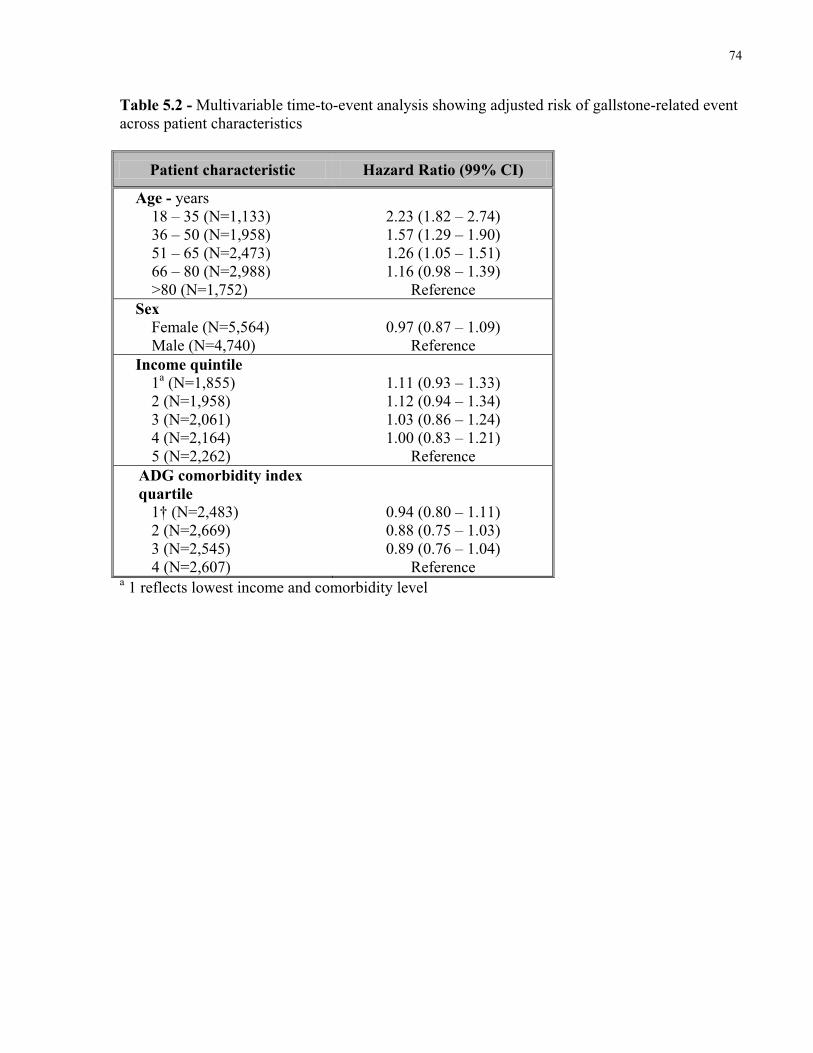
74
Table 5.2 - Multivariable time-to-event analysis showing adjusted risk of gallstone-related event across patient characteristics
Patient characteristic Hazard Ratio (99% CI)
Age - years 18 – 35 (N=1,133) 36 – 50 (N=1,958) 51 – 65 (N=2,473) 66 – 80 (N=2,988) >80 (N=1,752)
2.23 (1.82 – 2.74) 1.57 (1.29 – 1.90) 1.26 (1.05 – 1.51) 1.16 (0.98 – 1.39)
Reference Sex
Female (N=5,564) Male (N=4,740)
0.97 (0.87 – 1.09)
Reference Income quintile
1a (N=1,855) 2 (N=1,958) 3 (N=2,061) 4 (N=2,164) 5 (N=2,262)
1.11 (0.93 – 1.33) 1.12 (0.94 – 1.34) 1.03 (0.86 – 1.24) 1.00 (0.83 – 1.21)
Reference ADG comorbidity index quartile
1† (N=2,483) 2 (N=2,669) 3 (N=2,545) 4 (N=2,607)
0.94 (0.80 – 1.11) 0.88 (0.75 – 1.03) 0.89 (0.76 – 1.04)
Reference a 1 reflects lowest income and comorbidity level
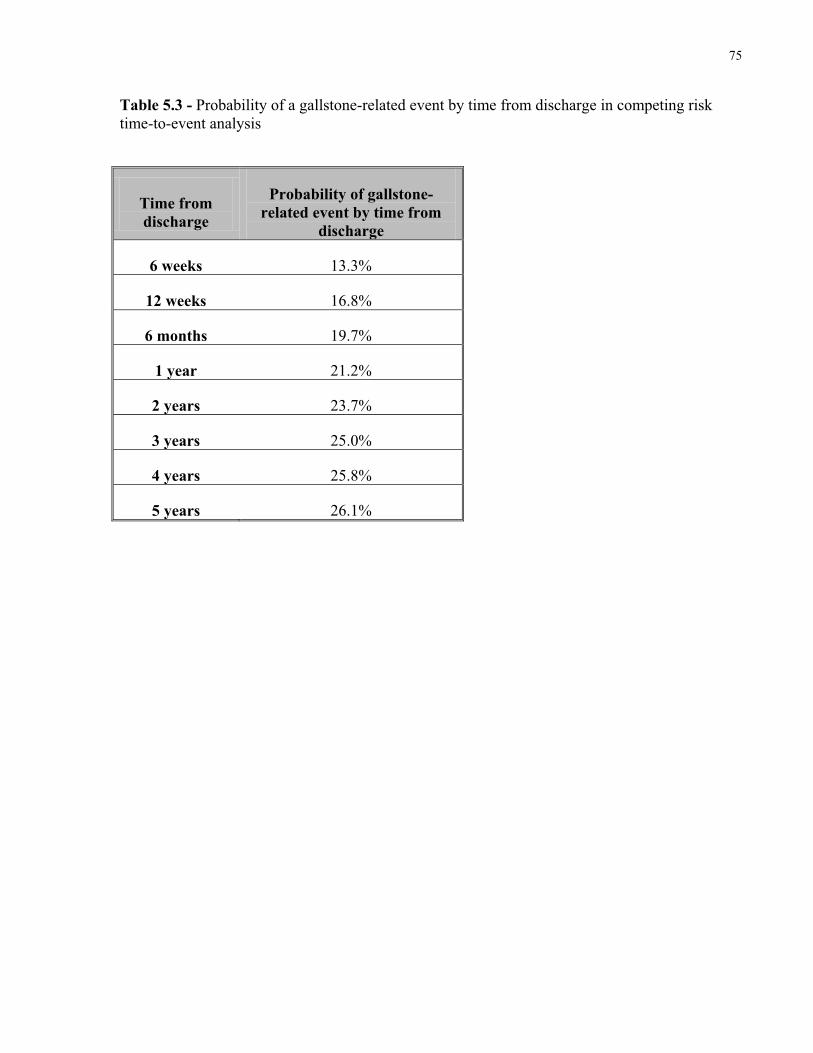
75
Table 5.3 - Probability of a gallstone-related event by time from discharge in competing risk time-to-event analysis
Time from discharge
Probability of gallstone-related event by time from
discharge
6 weeks 13.3%
12 weeks 16.8%
6 months 19.7%
1 year 21.2%
2 years 23.7%
3 years 25.0%
4 years 25.8%
5 years 26.1%
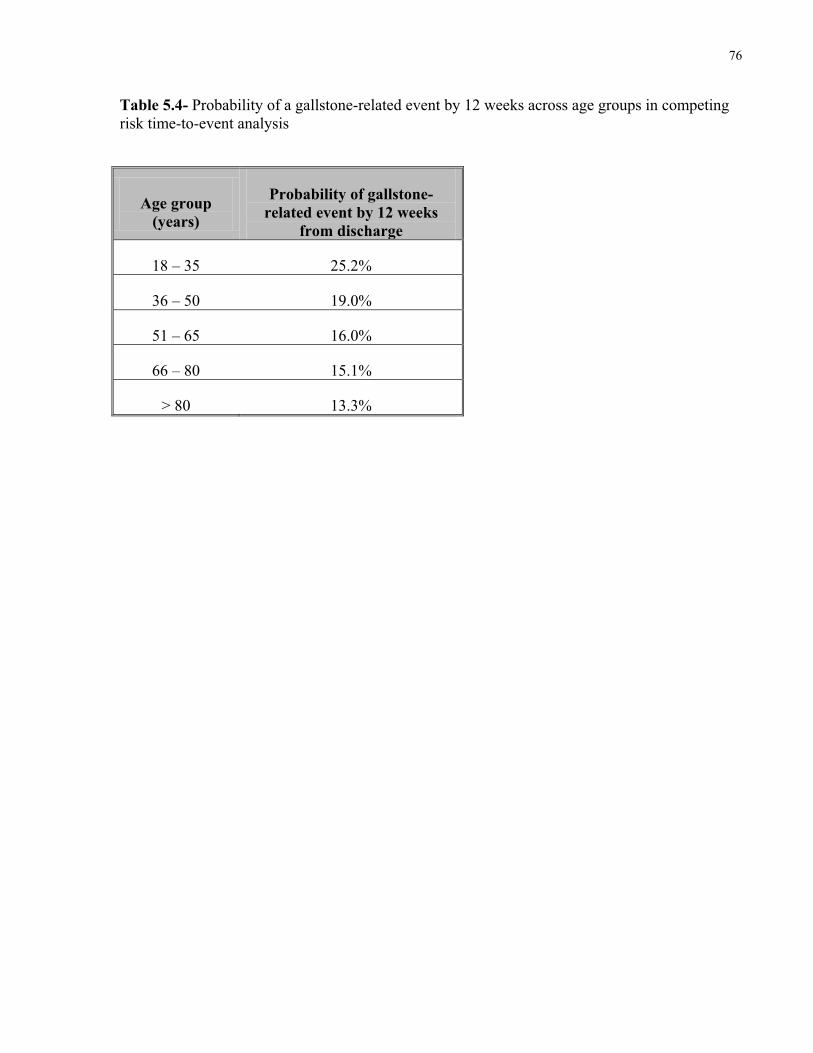
76
Table 5.4- Probability of a gallstone-related event by 12 weeks across age groups in competing risk time-to-event analysis
Age group (years)
Probability of gallstone-related event by 12 weeks
from discharge
18 – 35 25.2%
36 – 50 19.0%
51 – 65 16.0%
66 – 80 15.1%
> 80 13.3%
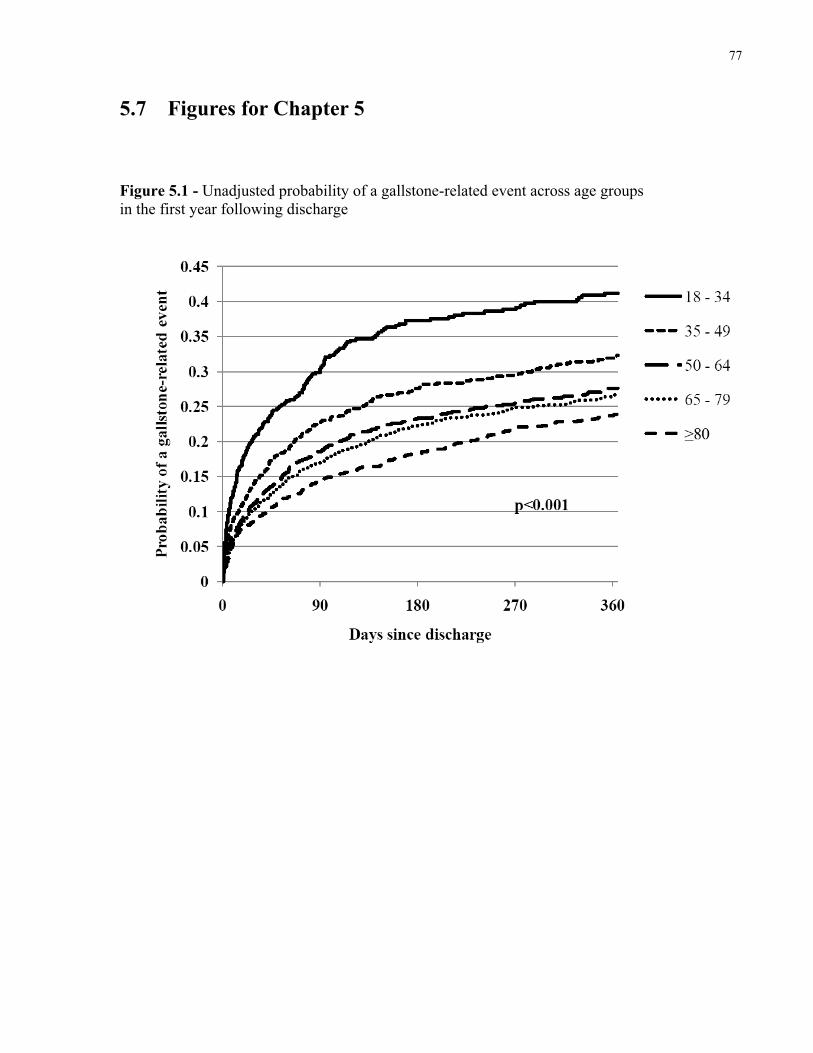
77
5.7 Figures for Chapter 5
Figure 5.1 - Unadjusted probability of a gallstone-related event across age groups in the first year following discharge
78
Chapter 6
Comparative Operative Outcomes of Early and Delayed
Cholecystectomy for Acute Cholecystitis
The purpose of this chapter is to:
I. Present the comparative frequency of rare operative complications between early and
delayed cholecystectomy in a large population-based cohort.
II. Present the comparative frequency of open cholecystectomy and conversion among
laparoscopic cases between early and delayed cholecystectomy in a large population-
based cohort.
Preamble
The contents of this chapter are currently under review with Annals of Surgery:
De Mestral C, Rotstein OD, Laupacis A, Hoch JS, Zagorksi B, Alali A, Nathens AB.
Comparative operative outcomes of early and delayed cholecystectomy for acute
cholecystitis: A population-based propensity score analysis.

79
6.1 Summary
Background
Randomized trials comparing early to delayed cholecystectomy for acute cholecystitis
have limited contemporary external validity. Furthermore, no study to date has been large
enough to assess the impact of timing of cholecystectomy on the frequency of serious rare
complications including bile duct injury and death. We sought to compare the operative
outcomes of early and delayed cholecystectomy for acute cholecystitis in a large population-
based cohort.
Methods
This is a retrospective cohort study of patients emergently admitted to hospital with acute
cholecystitis and managed with cholecystectomy over the period of April 1, 2004 to March 31,
2011. We used administrative records for the province of Ontario, Canada. Patients were divided
into two exposure groups: those who underwent cholecystectomy within 7 days of emergency
department presentation on index admission (early cholecystectomy) and those whose
cholecystectomy was delayed. The primary outcome was major bile duct injury requiring
operative repair within 6 months of cholecystectomy. Secondary outcomes included major bile
duct injury or death, 30-day post-cholecystectomy mortality, completion of cholecystectomy
with an open approach and, among laparoscopic cases, conversion from a laparoscopic to an
open approach. Propensity score methods were used to address confounding by indication.
Results
80
From 22,202 patients, a well-balanced matched cohort of 14,220 patients was defined.
Early cholecystectomy was associated with a lower risk of major bile duct injury (0.28% vs.
0.53%, RR=0.53, 95% CI 0.31–0.90, p=0.025), of major bile duct injury or death (1.36% vs.
1.88%, RR=0.72, 95% CI 0.56–0.94, p=0.016) and, albeit not significant, of 30-day post-
operative mortality (0.46% vs. 0.64%, RR=0.73, 95% CI 0.47–1.15, p=0.21). No significant
differences were observed in terms of open cholecystectomy (15% vs. 14%, RR=1.07, 95% CI
0.99–1.16, p=0.10) or in conversion among laparoscopic cases (11% vs. 10%, RR=1.02, 95% CI
0.93–1.13, p=0.68).
Conclusion
These results support the benefit of early over delayed cholecystectomy for patients with
acute cholecystitis.
6.2 Background
Acute cholecystitis is the most common cause of hospitalization for gastrointestinal
disease14. While cholecystectomy is the definitive management, the timing of surgery in relation
to the first episode of acute cholecystitis remains an area of considerable practice variation.
Operative intervention is either undertaken early on first presenting admission or, may be
delayed 6 to 12 weeks after initial non-operative management to allow the acute inflammation to
resolve. Several randomized controlled trials have shown that early laparoscopic
cholecystectomy (within up to 7 days of symptom onset) is associated with a shorter total
hospital length of stay and a similar rate of conversion to an open procedure, when compared to
delayed cholecystectomy60. Furthermore, early surgery precludes the risk of recurrent gallstone-
81
related symptoms, estimated to affect approximately 20% of patients15,60,132. However, despite
this evidence as well as expert consensus supporting early laparoscopic cholecystectomy, rates of
early surgery remain variable.
Practice patterns may not be consistent with best available evidence because concern
remains that rare but serious complications such as major bile duct injury or death may occur
more frequently in the setting of emergency surgery on an acutely inflamed gallbladder22. Major
bile duct injury occurs in 0.3-0.5%41,53of cholecystectomies and is a serious complication
associated with reduced long term survival41,42 and high litigation rates43. No study to date has
been large enough to compare major bile duct injury or mortality rates between early and
delayed cholecystectomy.
Furthermore, the trials comparing early to delayed surgery were derived from single
specialized centres and included patients recruited between 1993 and 200265-67,130,131.
Consequently, these data may not be generalizable to a broader range of hospitals or to current
practice characterized by greater expertise with laparoscopic surgery. Understanding
comparative rates of open cholecystectomy and conversion in the laparoscopic era is important
since, while conversion to an open approach is safe practice in the face of operative difficulty,
open cholecystectomy is associated with greater post-operative pain, an increased incidence of
surgical site infection and a longer hospital stay34-36.
To address these evidence gaps, we compared the operative outcomes of early and
delayed cholecystectomy in a contemporary, population-based cohort of patients with acute
cholecystitis.
82
6.3 Methods
Design
This is a retrospective cohort study of patients emergently admitted to hospital with acute
cholecystitis who were subsequently managed with cholecystectomy over the period of April 1,
2004 to March 31, 2011. Operative outcomes were compared between patients who underwent
cholecystectomy within 7 days of emergency department (ED) presentation on index admission
(early cholecystectomy) and patients whose cholecystectomy was delayed. The research ethics
board of Sunnybrook Health Sciences Centre, Toronto, Canada, approved this study.
Setting
We used administrative records for the province of Ontario, Canada. Medically necessary
hospital and physicians services for Ontario’s over 13 million residents are universally accessible
and funded by the provincial Ministry of Health and Long Term Care.
Data sources
Population-based datasets that include all ED visits, hospital admissions, outpatient
surgeries and physician billing claims in Ontario were deterministically linked using an
encrypted unique patient identifier. The index cholecystitis admission was identified in the
Discharge Abstract Database (DAD) and, linkage to the National Ambulatory Care Reporting
System confirmed entry via the ED. Patient characteristics were derived from DAD
83
supplemented with data from the Ontario Health Insurance Plan (OHIP) physician claims
database. Surgical procedure data and surgeon characteristics were also available through linkage
of DAD and the OHIP claims database. Date of death was obtained from the Registered Persons
Database. These datasets have been validated for a variety of diagnoses91-94,98 and, a multicenter
validation study showed almost perfect agreement on the most responsible diagnosis between
DAD and re-abstracted records for gallstone-related admissions98.
Cohort
Adults admitted through the ED with a most responsible diagnosis of acute cholecystitis
(ICD-10-CA: K80.0, K80.1, K80.4, K81.0, K81.8, K81.9) and without prior symptomatic
gallstone disease – no ED visit or hospital admission for gallstone disease in the two preceding
years – were considered for inclusion in the cohort. Patients admitted directly to the intensive
care unit or managed with a cholecystostomy drain (ICD-10-CA: 1.OD.52) were excluded
because they were considered to have cholecystitis with severe sepsis or significant comorbidity
precluding operation. Patients who underwent cholecystectomy were identified based on having
an inpatient or outpatient record of cholecystectomy (ICD-10-CA: 1.OD.57, 1.OD.89) and an
associated OHIP claim for cholecystectomy (S287). Finally, given the primary outcome
definition described below, we excluded patients without at least 6 months of post-operative
follow-up, as well as patients with a diagnosis of biliary tract malignancy or cyst (ICD-10-
CA:C23, C22.1, C24, Q44.4) within 6 months of cholecystectomy (figure 1).
Exposure
84
The main exposure was early cholecystectomy, defined as cholecystectomy within 7 days
of ED presentation on index admission.
Outcomes
The primary outcome was major bile duct injury. Patients who underwent operative
repair of the biliary tract (OHIP billing claim: S281, S285 – choledochoenterostomy; S292 –
repair of common duct) within 6 months of cholecystectomy were considered to have suffered a
major bile duct injury. There were four secondary outcomes: (1) a composite outcome of major
bile duct injury or death – included because of potential for censoring of the primary outcome by
death before biliary tract repair within 6 months; (2) 30-day post-cholecystectomy mortality; (3)
completion of cholecystectomy through an open approach – whether started open or via
laparoscopy; (4) conversion to open cholecystectomy among laparoscopic cases.
Identification of major bile duct injury in administrative data through physician billing
claims for surgical repair of the biliary tract has been previously utilized41 with injury rates
consistent with prospective cholecystectomy and gallstone registries42,53. It is also unlikely that
differences exist between exposure groups in the sensitivity and specificity of OHIP repair
claims for the identification of major bile duct injury. ICD-10 procedure coding was used to
differentiate open from laparoscopic cases and an attribute status code was used to identify
conversion among laparoscopic cases. A multicentre validation study found almost perfect
agreement on surgical approach (open vs. laparoscopic) between administrative and re-abstracted
records across a range of abdominal surgical procedures98. Substantial agreement was also
85
reported regarding conversion during laparoscopic appendectomy, indirectly supporting the
validity of conversion in this study98.
Covariates
Several characteristics of the patient and surgeon might confound the relationship
between the timing of cholecystectomy and operative outcomes. We considered patient age, sex,
income level, comorbidity burden, and pancreatitis or biliary tract obstruction on index
admission as potential confounders. A crude proxy for socioeconomic status, income quintiles
were based on the median income of a patient’s postal code of residence115. Comorbidity level
was calculated using the John Hopkins Aggregated Diagnostic Groups (ADG) system116 with a
2-year look-back at inpatient and outpatient records. The ADG system was used to derive a
comorbidity index validated for the prediction of 1-year mortality in a general cohort of adult
Ontarians96,97. At the physician level, we considered the number of cholecystectomies a surgeon
had performed in the year prior to the index cholecystectomy, as well as the number of years
since medical school graduation.
Analytic approach
We used propensity score methods to account for selection bias. Matching on the
propensity score was the primary analytic approach employed111.
First, each patient’s probability of receiving early cholecystectomy (propensity score)
was derived from a logistic regression model where all of the previously mentioned potential
86
confounders were regressed onto the binary outcome of early or delayed cholecystectomy.
Continuous variables (age, comorbidity index, surgeon’s number of cholecystectomies and years
since medical school graduation) were modeled using smoothing cubic splines to allow for
departures from linearity133.
Propensity score matching was then performed using a nearest-neighbour, 1-to-1 pair
match within 0.2 standard deviations (caliper) of the logit of the propensity score and without
replacement111,134. Thus, in random sequence, a patient in the early group was selected and then
matched to a patient in the delayed group with the closest propensity score, within the defined
caliper range. Covariate balance after matching was quantified by calculating the standardized
difference of the mean or proportion for each covariate, with a standardized difference of <10%
indicative of good balance between groups135,136. The distributions of continuous variables were
also compared graphically through cumulative density and quantile-quantile plots136. In addition
to matching on the propensity score, given that older age and male sex have been associated with
greater severity of cholecystitis22-24, matched pairs were required to be of the same sex and have
an age difference of at most 5 years. Within the matched sample, outcome frequency differences
were tested with the McNemar chi-square. A relative risk and 95% confidence interval was also
calculated for each outcome, taking account of the sample’s matched nature137.
A variety of sensitivity analyses were undertaken. First, we employed an alternate
propensity score approach that used the entire study cohort: inverse probability of treatment
weighting. Weighting each patient on the inverse probability of treatment received produces a
synthetic study sample balanced on observed covariates111,138. The relative risk for each outcome
was calculated from a weighted log binomial regression model with robust variance
estimation110. Second, given the variable definition of timing of early cholecystectomy across the
87
literature, we reanalyzed the data using cholecystectomy within 3 days of ED presentation as the
exposure. Finally, we examined the results after excluding patients who underwent
cholecystectomy later than 1 year after discharge from index admission, considering that they
were less likely to have been discharged with the intention of delayed cholecystectomy.
6.4 Results
A total of 22,202 patients were emergently admitted across 154 hospitals with a first
episode of acute cholecystitis and ultimately managed with cholecystectomy from 2004 to 2011.
The mean age was 54±18 years and most were women (60%, n=13,376). Common bile duct
obstruction and pancreatitis were present on admission in 10% (n=2,243) and 5% (n=1,058) of
patients, respectively. The majority of cholecystectomies (67%, n=14,948) were early. The
median time to delayed cholecystectomy was 8 weeks (IQR 4-12 weeks) from ED presentation.
Overall, there were 77 (0.35%) major bile duct injuries and 100 (0.45%) deaths within 30 days of
cholecystectomy. A total of 2,861 of the 22,202 cholecystectomies (13%) were completed open
(started open or converted). Among the 21,280 cases started via laparoscopy, 1,939 (9%) were
converted to an open approach.
Patients undergoing early cholecystectomy were younger, more frequently female, less
likely to have biliary tract obstruction and had a lower comorbidity burden (table 6.1). These
patients were also operated on by surgeons earlier in their career and with a larger recent
cholecystectomy experience when compared to patients receiving delayed cholecystectomy.
Matching on the propensity score, sex and age created 7,110 distinct pairs. After matching, all
patient and surgeon characteristics were well balanced (Table 6.2).
88
Within the matched sample, early cholecystectomy was associated with half the risk of
major bile duct injury and a lower risk of the composite outcome of major bile duct injury or
death (Table 6.3). While 30-day post-cholecystectomy mortality was lower in the early group,
this observation did not reach statistical significance (Table 6.3). The frequencies of open
cholecystectomy or conversion among laparoscopic cases were similar between the two groups
(table 6.3).
While 98% of patients managed with delayed cholecystectomy were included in the
matched sample, a majority (52%) of patients managed with early cholecystectomy were not
matched. Among the early cholecystectomy group, unmatched patients reflect those with a
higher propensity for early cholecystectomy than matched patients (mean propensity score 0.73
vs. 0.64, p<0.001) as well as similar or better outcomes (major bile duct injury 0.28% vs. 0.23%,
p=0.53; major bile duct injury or death 0.85% vs. 1.36%, p=0.002; cholecystectomy completed
open 9% vs. 15%, p<0.001).
Sensitivity analyses included an alternate analytic approach (inverse probability of
treatment weighting), a change in the exposure definition (early surgery within 3 days of ED
presentation) and a restricted timeframe for delayed cholecystectomy (within 12 months of
discharge). First, with inverse probability of treatment weighting, the probability of treatment
received for each patient is calculated and corresponds to the propensity score for early group or,
1 minus the propensity score for the delayed group. Weighting on the inverse of the probability
of treatment received created a synthetic study sample that was well-balanced with respect to
observed covariates (Table 6.4). The outcome results from the weighted analysis were similar to
the matched analysis (Table 6.5).
89
Second, when narrowing the timeframe for early cholecystectomy to 3 days from ED
presentation, 13,087 (59% of 22,202) were considered to have undergone early cholecystectomy.
Using the same propensity score model and matching algorithm as the primary analysis, 7,865
well-balanced matched pairs were formed. The results with the new exposure definition
remained consistent with the primary analysis (Table 6.6).
Third, when excluding patients who underwent delayed cholecystectomy later than 1 year
after discharge, the cohort was reduced to 21,937 patients. Applying the same propensity score
model and matching algorithm as the primary analysis resulted in 6,864 well-balanced matched
pairs. The results for this cohort were similar to the primary analysis (Table 6.7).
6.5 Discussion
In this population-based analysis of over 20,000 patients with acute cholecystitis, early
cholecystectomy was associated with half the risk of major bile duct injury, a lower risk of major
bile duct injury or death, and a reduction, albeit non-significant, in 30-day post-cholecystectomy
mortality. Furthermore, no significant differences between management strategies were observed
in terms of open cholecystectomy or conversion. That early cholecystectomy is associated with
improved operative outcomes substantiates the need for a paradigm shift in the management of
acute cholecystitis.
Based on best available evidence, early cholecystectomy is supported by many expert
groups49,76 but practice patterns remain variable. Given the limited external validity and small
sample size of existing trials, concern remained that a higher frequency of rare but serious
operative complications might result from early surgery in the setting of acute inflammation22,49.
90
Meta-analysis of randomized trials failed to show a difference in rates of bile duct injury (1/222
in early group vs. 3/216 in delayed group)71. Our study is the first comparison of these strategies
with the power to detect a benefit associated with early surgery in terms of major bile duct
injury. The development of fibrosis in and around Calot’s triangle following resolution of the
initial bout of acute cholecystitis is a reasonable pathologic explanation supporting a causal
association between delayed surgery and a higher risk of major bile duct injury130,131.
Furthermore, recurrent acute cholecystitis which may occur prior to the delayed cholecystectomy
may also contribute to the increased average risk of major bile duct injury. With respect to post-
cholecystectomy mortality, the trials provide little insight since no deaths occurred71. Our
analysis showed a lower 30-day mortality following early surgery, although it is very possible
that this observation occurred due to chance. It is also plausible that patients deemed unfit for
surgery because of a perceived mortality risk were less likely to undergo early cholecystectomy.
To examine the possibility of residual confounding of mortality, we compared the proportion of
patients who underwent elective hip and knee replacement surgery within two years of
cholecystectomy. The rates of these elective procedures, performed to improve quality of life,
were not significantly different between early and delayed groups (hip: 0.38% vs. 0.42%,
p=0.79; knee: 0.72% vs. 0.82%, p=0.57), suggesting that residual confounding is an unlikely
explanation for the observed lower mortality.
This study is consistent with trial data in showing a similar frequency of conversion to an
open procedure between early and delayed cholecystectomy. By addressing this comparison
across a population-based cohort of patients and general surgeons, our analysis alleviates the
concern of limited external validity of the randomized trials. While the trials showed conversion
rates in the order of 20%, the conversion rate in this contemporary cohort approximated 10%.
Given that these trials recruited patients between 1993 and 2002, the observed decrease has face
91
validity and is consistent with increased training and experience with laparoscopic
cholecystectomy over time.
In addition to the benefit of early surgery in terms of major bile duct injury, early surgery
is also favoured based on the considerable risk of recurrent gallstone symptoms if
cholecystectomy is delayed. In a meta-analysis of existing trials, 17.5% of patients randomized
to delayed cholecystectomy suffered non-resolving or recurrent symptoms71. In the work
described in Chapter 4 of this thesis, 19% of patients with acute cholecystitis who were
discharged without cholecystectomy, either returned to the ED or were readmitted to hospital for
gallstone disease within 12 weeks of discharge132. These results and the present study therefore
both support early over delayed surgery for most patients.
Strengths of this study include the large sample size, the use of a validated 1-year
mortality risk index and a sophisticated analytic approach to address confounding by indication.
However, several limitations exist. First, propensity score methods only account for confounding
related to observed covariates. Thus residual confounding due to differences in cholecystitis
severity or surgeon characteristics may partially explain the observed difference in major bile
duct injury. For a number of reasons we feel that differences in cholecystitis severity between
exposure groups is unlikely. First, we excluded patients likely to have severe cholecystitis or
severe comorbidity. Second, although information about time delay between symptom onset and
hospital presentation (a widely cited marker of greater cholecystitis severity20) was not available,
because all emergency care is universally accessible without copayment in Ontario, prolonged
delay in seeking medical attention for cholecystitis symptoms is unlikely. Furthermore,
controlling for age, sex and comorbidity can reasonably be expected to minimize differences
between exposure groups with respect to cholecystitis severity22-24. Finally, the performance of
92
an intraoperative cholangiogram may be indicative of severe inflammation or fibrosis in Calot’s
triangle and was identified in 3% (n=604) of cholecystectomies. We did not include this
characteristic in deriving the propensity score since it could also reflect the consequence of a bile
duct injury. However, before and after matching, the frequency of cholangiogram was similar in
the early and delayed groups, offering further support for the premise that cholecystitis severity
was not meaningfully different. With respect to surgeon characteristics, two potentially
important unmeasured factors are whether the surgeon had subspecialty training in hepato-biliary
or minimally invasive surgery, and whether a trainee was involved in the operation. However,
even if residual confounding exists related to surgeon characteristics, these results suggest that
early cholecystectomy can confer improved operative outcomes. Thus, surgeons uncomfortable
with offering early laparoscopic surgery should consider seeking the expertise of colleagues with
more experience in difficult laparoscopic cholecystectomy before recommending initial non-
operative management and delayed cholecystectomy. Second, we were unable to capture bile
leaks managed with percutaneous or endoscopic intervention since the date of these procedures,
undertaken outside the operating room, was inconsistently available. However, major bile duct
injuries requiring operative repair remain most clinically important given high associated
morbidity. Finally, the cause of death was unavailable, precluding an understanding of the
proportion of post-operative deaths that could be attributed to cholecystectomy.
In conclusion, these data are consistent with randomized controlled trials but also provide
considerable added value for decision making. The results offer strong support for a practice of
early over delayed cholecystectomy for most patients with acute cholecystitis.
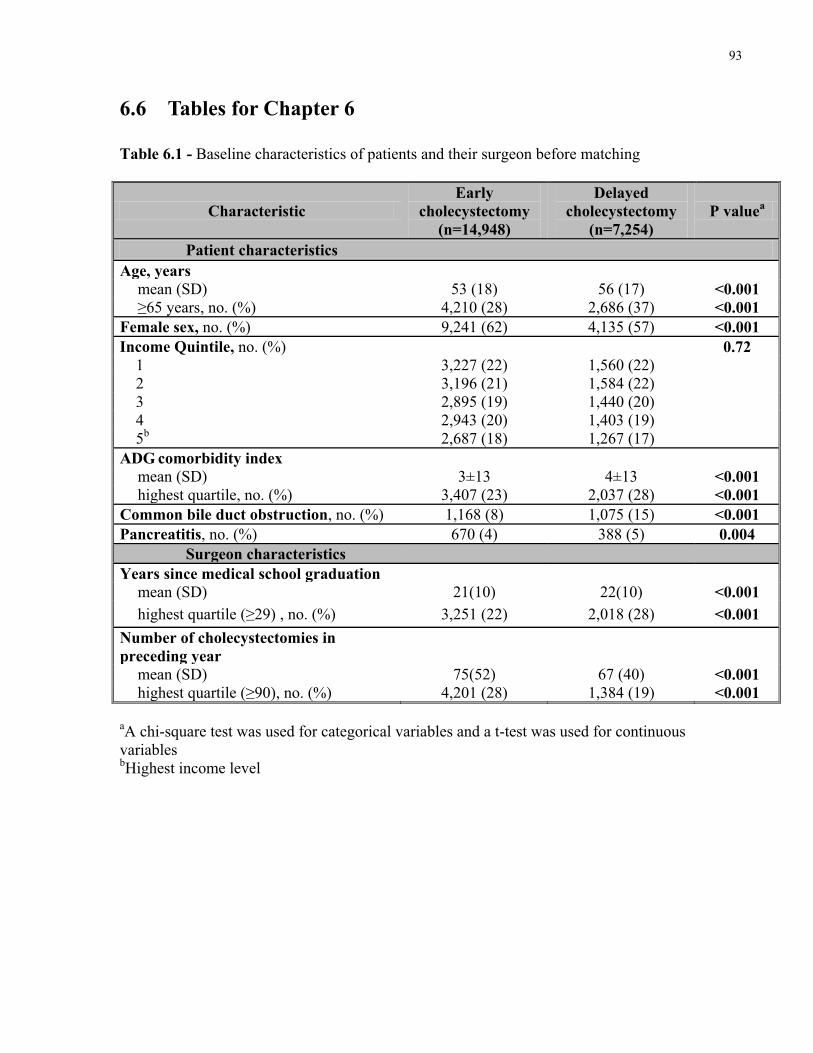
93
6.6 Tables for Chapter 6
Table 6.1 - Baseline characteristics of patients and their surgeon before matching
Characteristic Early
cholecystectomy (n=14,948)
Delayed cholecystectomy
(n=7,254) P valuea
Patient characteristics Age, years
mean (SD) 53 (18) 56 (17) <0.001 ≥65 years, no. (%) 4,210 (28) 2,686 (37) <0.001
Female sex, no. (%) 9,241 (62) 4,135 (57) <0.001 Income Quintile, no. (%) 0.72
1 3,227 (22) 1,560 (22) 2 3,196 (21) 1,584 (22) 3 2,895 (19) 1,440 (20) 4 2,943 (20) 1,403 (19) 5b 2,687 (18) 1,267 (17)
ADG comorbidity index mean (SD) 3±13 4±13 <0.001 highest quartile, no. (%) 3,407 (23) 2,037 (28) <0.001
Common bile duct obstruction, no. (%) 1,168 (8) 1,075 (15) <0.001 Pancreatitis, no. (%) 670 (4) 388 (5) 0.004
Surgeon characteristics Years since medical school graduation
mean (SD) 21(10) 22(10) <0.001 highest quartile (≥29) , no. (%) 3,251 (22) 2,018 (28) <0.001
Number of cholecystectomies in preceding year
mean (SD) 75(52) 67 (40) <0.001 highest quartile (≥90), no. (%) 4,201 (28) 1,384 (19) <0.001
aA chi-square test was used for categorical variables and a t-test was used for continuous variables bHighest income level
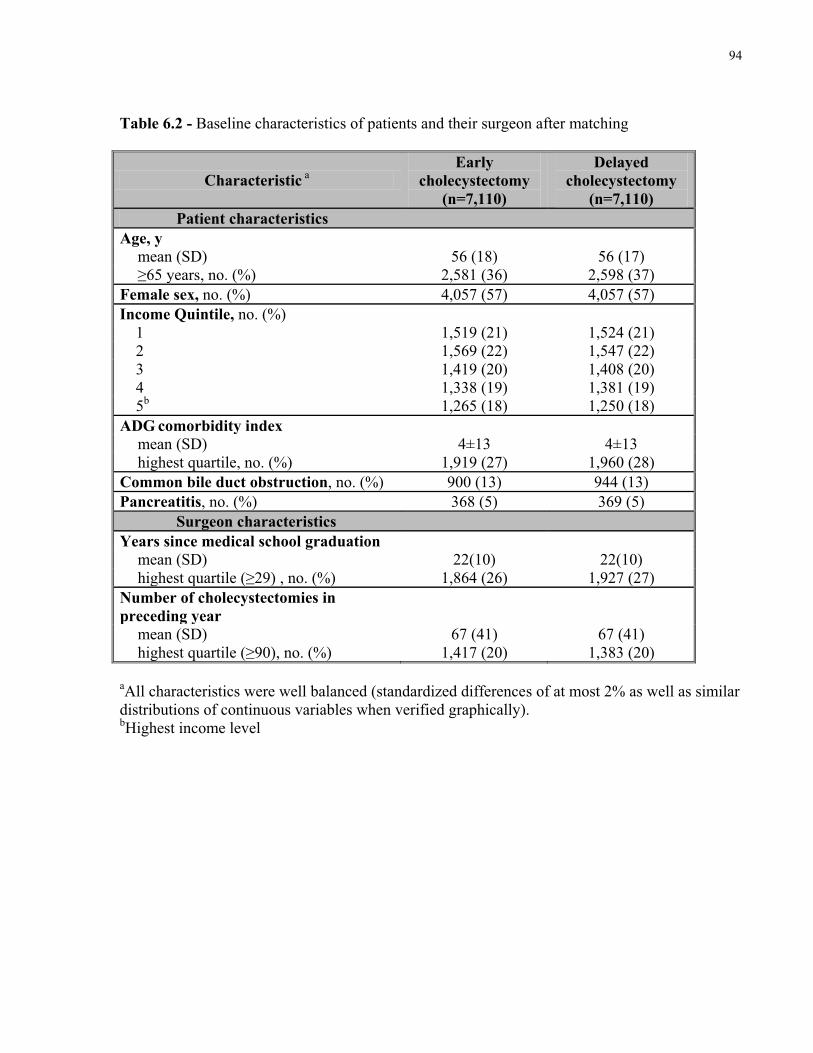
94
Table 6.2 - Baseline characteristics of patients and their surgeon after matching
Characteristic a Early
cholecystectomy (n=7,110)
Delayed cholecystectomy
(n=7,110) Patient characteristics
Age, y mean (SD) 56 (18) 56 (17) ≥65 years, no. (%) 2,581 (36) 2,598 (37)
Female sex, no. (%) 4,057 (57) 4,057 (57) Income Quintile, no. (%)
1 1,519 (21) 1,524 (21) 2 1,569 (22) 1,547 (22) 3 1,419 (20) 1,408 (20) 4 1,338 (19) 1,381 (19) 5b 1,265 (18) 1,250 (18)
ADG comorbidity index mean (SD) 4±13 4±13 highest quartile, no. (%) 1,919 (27) 1,960 (28)
Common bile duct obstruction, no. (%) 900 (13) 944 (13) Pancreatitis, no. (%) 368 (5) 369 (5)
Surgeon characteristics Years since medical school graduation
mean (SD) 22(10) 22(10) highest quartile (≥29) , no. (%) 1,864 (26) 1,927 (27)
Number of cholecystectomies in preceding year
mean (SD) 67 (41) 67 (41) highest quartile (≥90), no. (%) 1,417 (20) 1,383 (20)
aAll characteristics were well balanced (standardized differences of at most 2% as well as similar distributions of continuous variables when verified graphically). bHighest income level
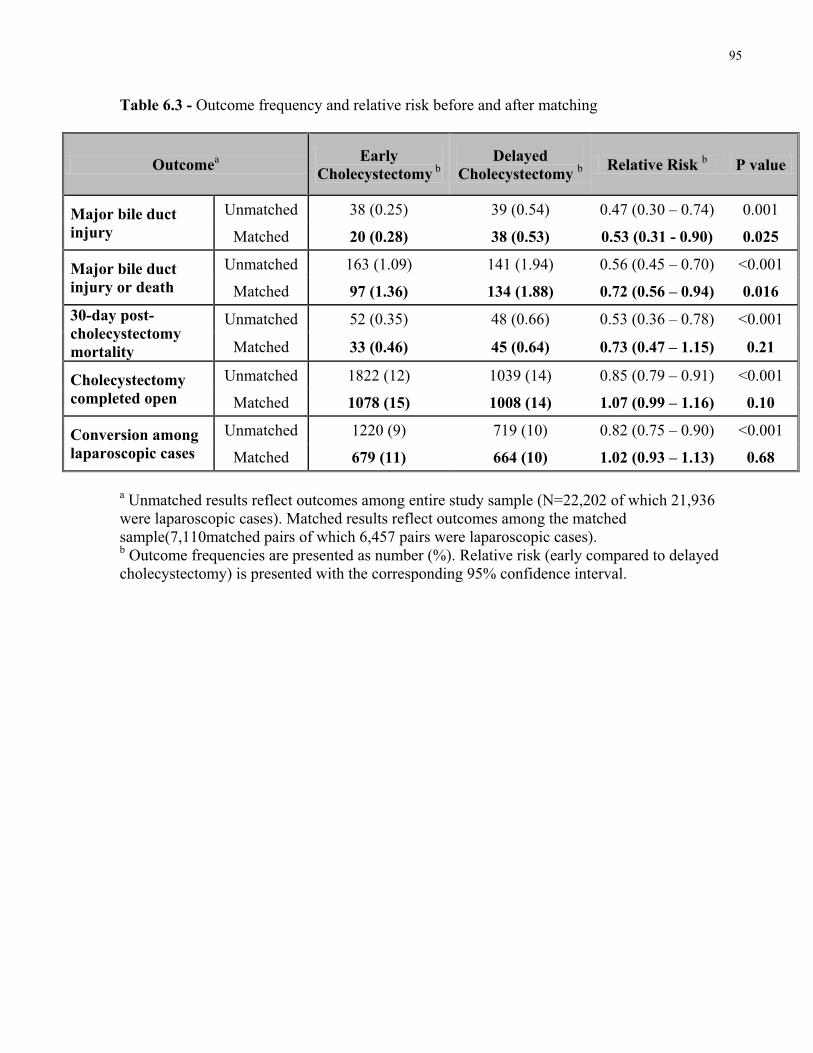
95
Table 6.3 - Outcome frequency and relative risk before and after matching
Outcomea Early Cholecystectomy b
Delayed Cholecystectomy b Relative Risk b P value
Major bile duct injury
Unmatched 38 (0.25) 39 (0.54) 0.47 (0.30 – 0.74) 0.001
Matched 20 (0.28) 38 (0.53) 0.53 (0.31 - 0.90) 0.025
Major bile duct injury or death
Unmatched 163 (1.09) 141 (1.94) 0.56 (0.45 – 0.70) <0.001
Matched 97 (1.36) 134 (1.88) 0.72 (0.56 – 0.94) 0.016 30-day post-cholecystectomy mortality
Unmatched 52 (0.35) 48 (0.66) 0.53 (0.36 – 0.78) <0.001
Matched 33 (0.46) 45 (0.64) 0.73 (0.47 – 1.15) 0.21
Cholecystectomy completed open
Unmatched 1822 (12) 1039 (14) 0.85 (0.79 – 0.91) <0.001
Matched 1078 (15) 1008 (14) 1.07 (0.99 – 1.16) 0.10
Conversion among laparoscopic cases
Unmatched 1220 (9) 719 (10) 0.82 (0.75 – 0.90) <0.001
Matched 679 (11) 664 (10) 1.02 (0.93 – 1.13) 0.68
a Unmatched results reflect outcomes among entire study sample (N=22,202 of which 21,936 were laparoscopic cases). Matched results reflect outcomes among the matched sample(7,110matched pairs of which 6,457 pairs were laparoscopic cases). b Outcome frequencies are presented as number (%). Relative risk (early compared to delayed cholecystectomy) is presented with the corresponding 95% confidence interval.
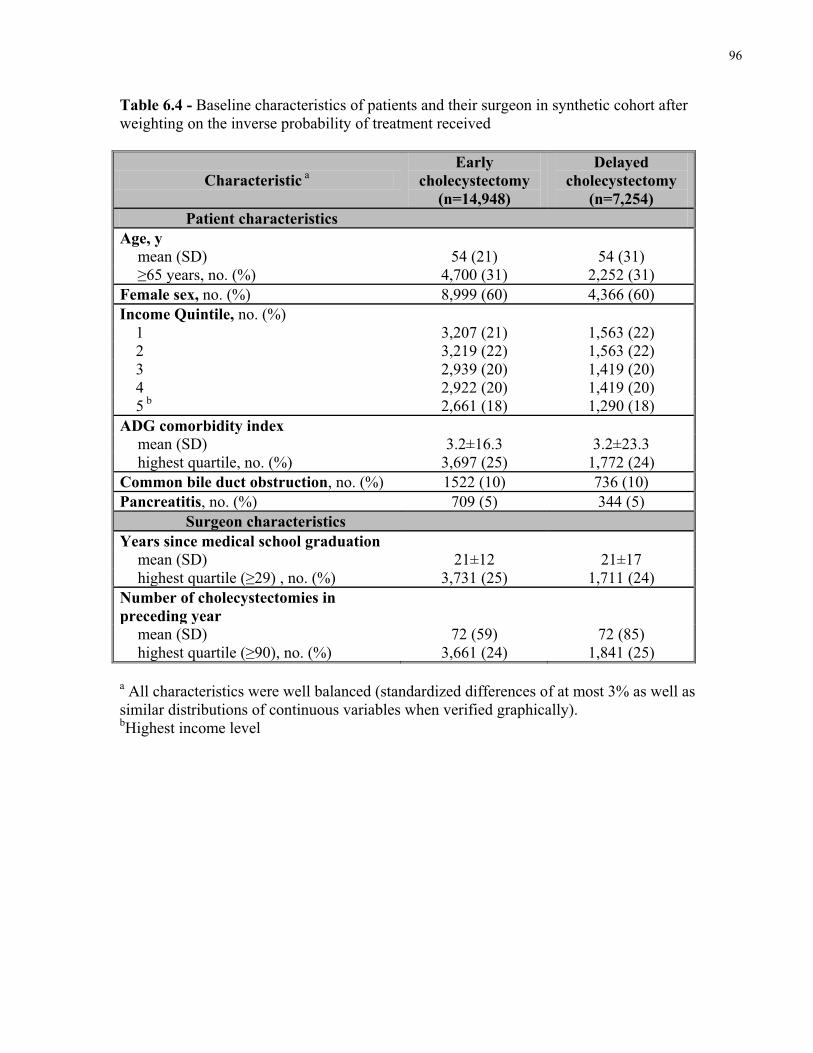
96
Table 6.4 - Baseline characteristics of patients and their surgeon in synthetic cohort after weighting on the inverse probability of treatment received
Characteristic a Early
cholecystectomy (n=14,948)
Delayed cholecystectomy
(n=7,254) Patient characteristics
Age, y mean (SD) 54 (21) 54 (31) ≥65 years, no. (%) 4,700 (31) 2,252 (31)
Female sex, no. (%) 8,999 (60) 4,366 (60) Income Quintile, no. (%)
1 3,207 (21) 1,563 (22) 2 3,219 (22) 1,563 (22) 3 2,939 (20) 1,419 (20) 4 2,922 (20) 1,419 (20) 5 b 2,661 (18) 1,290 (18)
ADG comorbidity index mean (SD) 3.2±16.3 3.2±23.3 highest quartile, no. (%) 3,697 (25) 1,772 (24)
Common bile duct obstruction, no. (%) 1522 (10) 736 (10) Pancreatitis, no. (%) 709 (5) 344 (5)
Surgeon characteristics Years since medical school graduation
mean (SD) 21±12 21±17 highest quartile (≥29) , no. (%) 3,731 (25) 1,711 (24)
Number of cholecystectomies in preceding year
mean (SD) 72 (59) 72 (85) highest quartile (≥90), no. (%) 3,661 (24) 1,841 (25)
a All characteristics were well balanced (standardized differences of at most 3% as well as similar distributions of continuous variables when verified graphically). bHighest income level
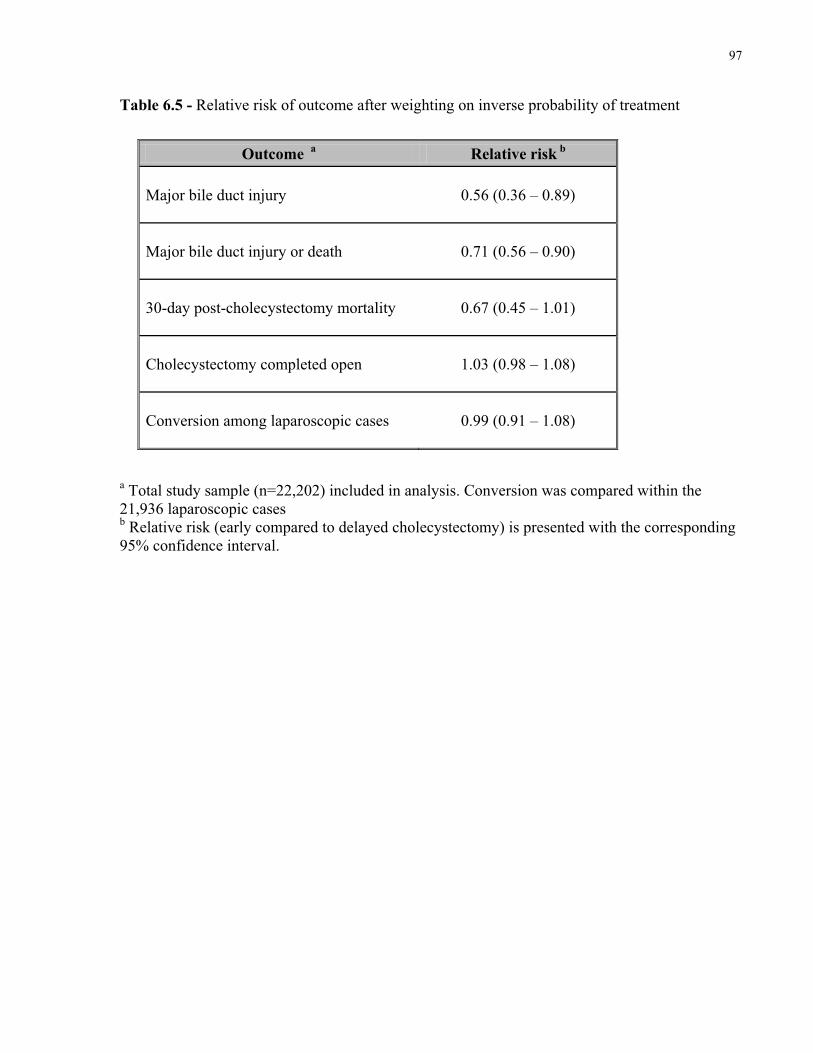
97
Table 6.5 - Relative risk of outcome after weighting on inverse probability of treatment
a Total study sample (n=22,202) included in analysis. Conversion was compared within the 21,936 laparoscopic cases b Relative risk (early compared to delayed cholecystectomy) is presented with the corresponding 95% confidence interval.
Outcome a Relative risk b
Major bile duct injury 0.56 (0.36 – 0.89)
Major bile duct injury or death 0.71 (0.56 – 0.90)
30-day post-cholecystectomy mortality 0.67 (0.45 – 1.01)
Cholecystectomy completed open 1.03 (0.98 – 1.08)
Conversion among laparoscopic cases 0.99 (0.91 – 1.08)
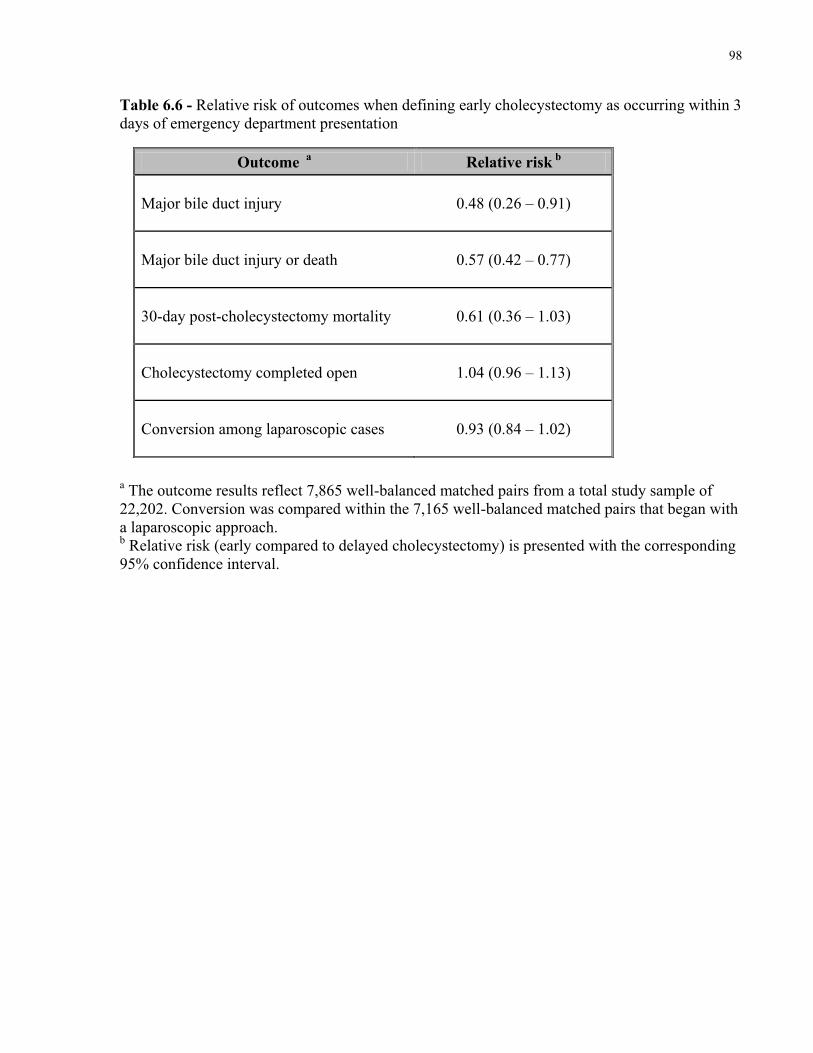
98
Table 6.6 - Relative risk of outcomes when defining early cholecystectomy as occurring within 3 days of emergency department presentation
a The outcome results reflect 7,865 well-balanced matched pairs from a total study sample of 22,202. Conversion was compared within the 7,165 well-balanced matched pairs that began with a laparoscopic approach. b Relative risk (early compared to delayed cholecystectomy) is presented with the corresponding 95% confidence interval.
Outcome a Relative risk b
Major bile duct injury 0.48 (0.26 – 0.91)
Major bile duct injury or death 0.57 (0.42 – 0.77)
30-day post-cholecystectomy mortality 0.61 (0.36 – 1.03)
Cholecystectomy completed open 1.04 (0.96 – 1.13)
Conversion among laparoscopic cases 0.93 (0.84 – 1.02)
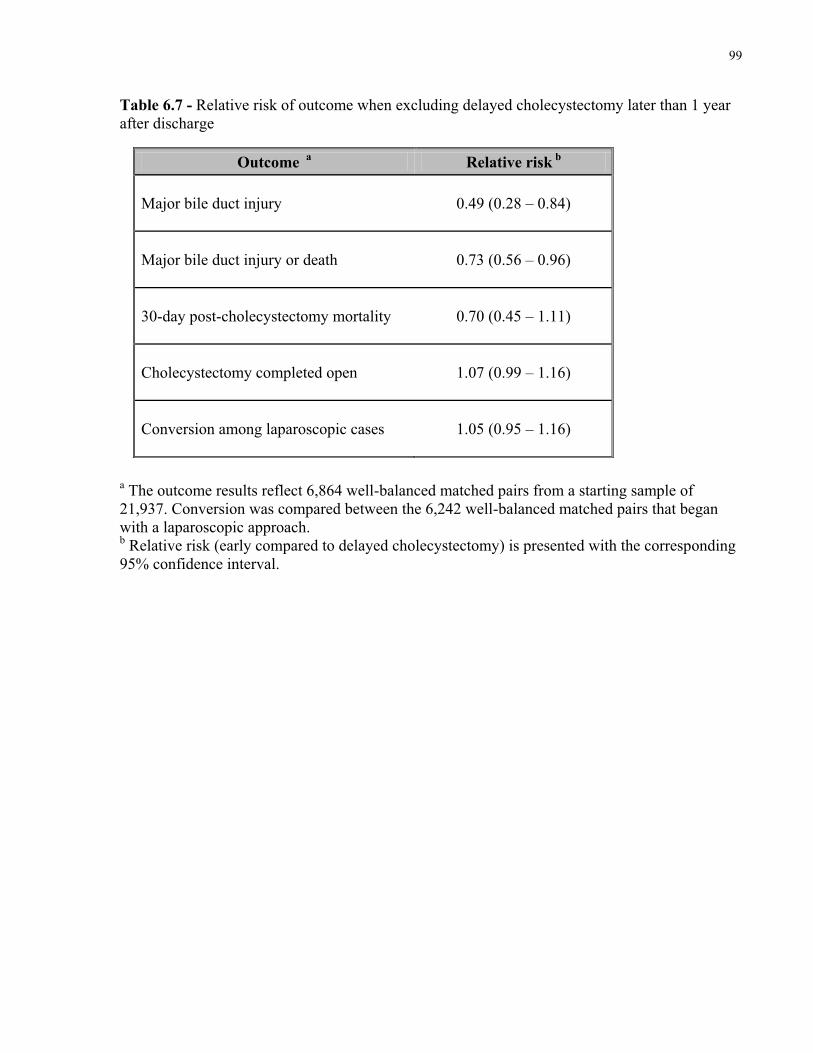
99
Table 6.7 - Relative risk of outcome when excluding delayed cholecystectomy later than 1 year after discharge
a The outcome results reflect 6,864 well-balanced matched pairs from a starting sample of 21,937. Conversion was compared between the 6,242 well-balanced matched pairs that began with a laparoscopic approach. b Relative risk (early compared to delayed cholecystectomy) is presented with the corresponding 95% confidence interval.
Outcome a Relative risk b
Major bile duct injury 0.49 (0.28 – 0.84)
Major bile duct injury or death 0.73 (0.56 – 0.96)
30-day post-cholecystectomy mortality 0.70 (0.45 – 1.11)
Cholecystectomy completed open 1.07 (0.99 – 1.16)
Conversion among laparoscopic cases 1.05 (0.95 – 1.16)
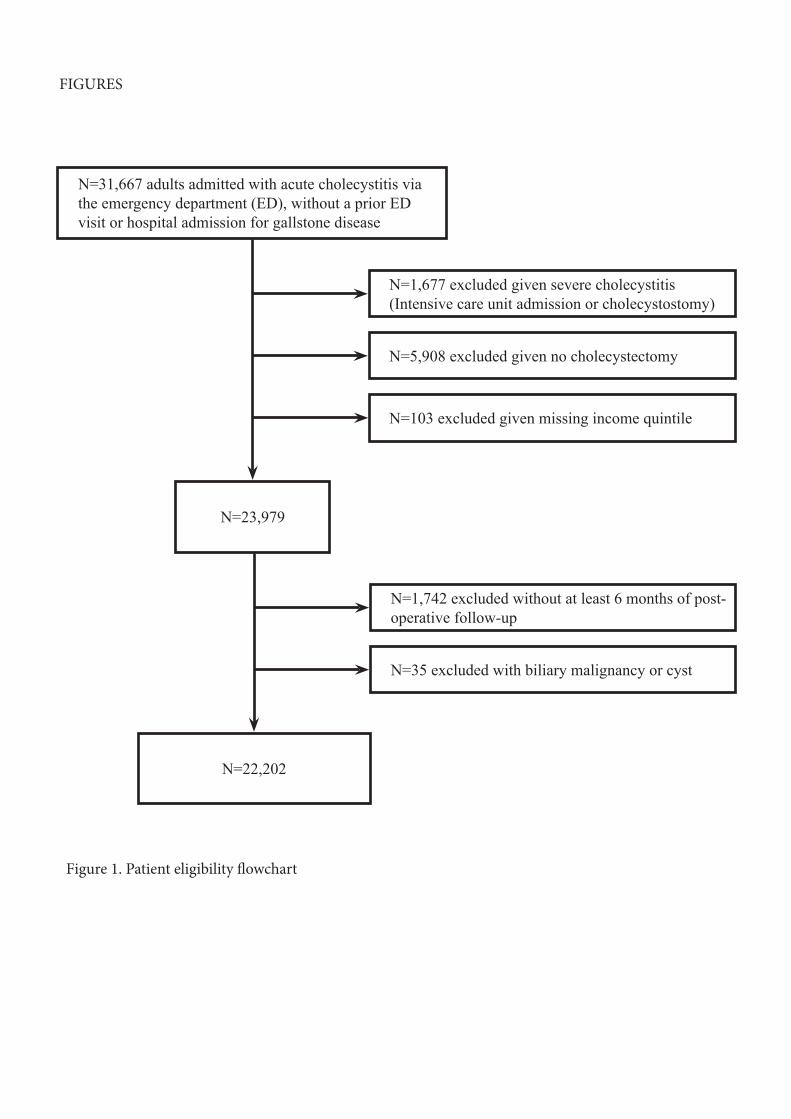
N=31,667 adults admitted with acute cholecystitis via the emergency department (ED), without a prior ED visit or hospital admission for gallstone disease
N=23,979
N=22,202
N=1,677 excluded given severe cholecystitis (Intensive care unit admission or cholecystostomy)
N=5,908 excluded given no cholecystectomy
N=103 excluded given missing income quintile
N=1,742 excluded without at least 6 months of post-operative follow-up
N=35 excluded with biliary malignancy or cyst
FIGURES
Figure 1. Patient eligibility flowchart
Charles
Text Box
6.7 Figures for Chapter 4
Charles
Text Box
Figure 6.1 - Patient eligibility flowchart
Charles
Rectangle
Charles
Text Box
100
101
Chapter 7
Cost-utility Analysis Comparing Alternative Timeframes of
Cholecystectomy for Acute Cholecystitis
The purpose of this chapter is to:
I. Compare the clinical effectiveness and costs associated with three alternative timeframes
of cholecystectomy for acute cholecystitis
II. Characterize the level of uncertainty around these estimates through probabilistic
sensitivity analysis
102
7.1 Summary
Background
The constrained nature of healthcare budgets mandates careful consideration of costs,
relative to the clinical consequences of alternative treatments. We performed a cost-utility
analysis comparing alternative timeframes of cholecystectomy for acute cholecystitis.
Methods
A Markov decision analytic model with a 5 year time horizon was developed to compare
costs and quality-adjusted life-years (QALY) gained from three alternative management
strategies: early cholecystectomy (within 7 days of presentation), delayed elective
cholecystectomy (8 to 12 weeks from presentation) and watchful waiting, where
cholecystectomy is performed urgently if recurrent symptoms arise. Model inputs were selected
to reflect patients with uncomplicated acute cholecystitis – without concurrent common bile duct
obstruction, pancreatitis or severe sepsis. Outcome probabilities and costs from the perspective
of a third party payer were derived from analysis of population-based administrative databases
for the province of Ontario, Canada. QALY values were based on directly elicited utilities
identified in the literature. Parameter uncertainty was evaluated through probabilistic sensitivity
analyses.
Results
Early cholecystectomy was less costly ($6,905 per person) and more effective (4.20
QALYs per person) than delayed cholecystectomy ($8,511; 4.18 QALYs per person) or watchful
waiting ($7,274; 3.99 QALYs per person), and therefore was the dominant alternative. In
103
probabilistic analysis, early cholecystectomy was most likely to be the optimal management
strategy, regardless of the decision maker’s willingness-to-pay for one additional QALY.
Conclusion
This cost-utility analysis provides further support for early cholecystectomy as the
optimal management of uncomplicated acute cholecystitis since early surgery offered the best
outcomes at the least cost.
7.2 Background
Gallstone disease affects as many as 20% of adults and is associated with an estimated
cost of over 6 billion dollars annually in the United States1. Furthermore, among all diseases of
the gastrointestinal tract, acute calculous cholecystitis is the leading cause of hospitalization14.
The only definitive management of acute cholecystitis remains cholecystectomy since surgery
manages the inflamed organ and, by removing the site of gallstone formation, prevents recurrent
symptoms. However, the timing of cholecystectomy remains contentious. Randomized
controlled trials and analyses in the previous chapters suggest a benefit to early urgent
cholecystectomy (within up to 7 days of symptom onset) over delaying cholecystectomy.
Specifically, early surgery is associated with a lower risk of major bile duct injury, a similar risk
of conversion from laparoscopic to open cholecystectomy, a shorter total hospital length of stay
and, unlike delayed surgery, does not leave the patient at risk of recurrent gallstone
symptoms22,71,114,132.
Despite the publication of the trials starting in the late 1990s, the application of early
cholecystectomy remains inconsistent across hospitals worldwide, with contemporary early
104
cholecystectomy rates ranging from 36% to 88%69,82,88,139,140. While clinical evidence continues
to grow in support of early surgery, very few formal economic evaluations have been published
comparing alternative timeframes of cholecystectomy in acute cholecystitis. A formal economic
evaluation involves estimating the relative costs and clinical consequences of alternative
treatments as well as characterizing uncertainty around the joint distribution of both outcomes72.
Furthermore, the economic evaluations that exist are based on data from small randomized trials
of limited contemporary external validity73,74. Given the constrained nature of healthcare
budgets, such analyses can provide important supplemental data for decision makers to consider
alongside clinical efficacy and effectiveness studies. We therefore performed an economic
evaluation comparing different timeframes of cholecystectomy for acute cholecystitis.
7.3 Methods
Study design
This is a model-based cost-utility analysis that compared three treatment strategies for
patients admitted to hospital with a first presentation of acute cholecystitis. The strategies were:
(1) early cholecystectomy, performed within 7 days of presentation, (2) delayed
cholecystectomy, performed electively 8 to 12 weeks following presentation, and (3) watchful
waiting, with cholecystectomy performed urgently, should recurrent symptoms arise.
Outcomes, time horizon and perspective
105
The outcomes of interest were quality-adjusted life-years (QALYs) and costs. Not
infrequently used in surgical literature141-143, QALYs combine the quality of life associated with
a particular health state and the duration of that health state into a single measure72. All costs
were converted to 2011 Canadian dollars using the consumer price index for health care in
Ontario144.
Outcomes were quantified over a 5 year time horizon starting at the time of first
presentation. A 5 year horizon was chosen over a lifetime horizon since acute cholecystitis and
cholecystectomy on average only have a short term impact on quality of life and mortality.
Furthermore, based on the analysis from Chapter 5, 95% of emergency department visits or
readmissions for recurrent gallstone symptoms occur within 2 years of discharge132. Therefore,
nearly all the impact of the modeled decision on quality of life and mortality would reasonably
be expected to occur within a 5 year time period.
Costs were considered from the perspective of a third party payer, the Ontario Ministry of
Health and Long Term Care. Therefore, patients’ out of pocket costs were not included in the
analysis. As per Canadian cost-effectiveness guidelines, costs and QALYs were discounted at a
rate of 5% per year145.
Model Structure
The underlying framework of the analysis was a Markov cohort decision analytic model,
used to derive the average cost and QALY gains of each management strategy, for a hypothetical
cohort of patients. Decision analysis provides an explicit framework to inform decision making
based on best available evidence. While defining a model structure necessarily involves a

106
simplification of reality, the model should reflect all important clinical consequences and costs
associated with the disease process and management strategies72. Thus, the initial cholecystitis
admission, recurrent gallstone-related symptoms if discharged without cholecystectomy and
complications resulting from cholecystectomy were modeled. Patients’ clinical course was
represented through a Markov process involving a series of mutually exclusive health states
(Figure 7.1). Over the 5 year time horizon of the analysis, patients transition from one health
state (e.g. acute cholecystitis) to another (e.g. asymptomatic awaiting elective cholecystectomy)
according to defined transition probabilities and at time intervals dictated by the defined cycle
length (1 month in our model).
As modeled, cholecystectomy could be undertaken via a laparoscopic or open (either
started open or converted to open) approach and cholecystectomy-related outcomes were
incorporated as: major bile duct injury requiring operative reconstruction, bile leak requiring
endoscopic intervention, other complications and no complication. In the base case analysis,
major bile duct injury, bile leak and other complications were modeled as impacting on quality
of life for 6, 2, and 1 month, respectively. Finally, gallstone-related symptoms were modeled as
biliary colic or recurrent cholecystitis, choledocholithiasis with or without cholangitis, and
pancreatitis. In both the delayed cholecystectomy and watchful waiting strategies, if a patient
suffered a gallstone-related symptom after their initial cholecystitis admission, they were
admitted and cholecystectomy was performed urgently on the same admission. Mortality was
incorporated in all stages of the model.
Model Inputs

107
The required model inputs include transition probabilities, costs, and utilities associated
with each health state or trajectory between health states. The input values were selected to be
representative of a hypothetical cohort of adult patients, emergently admitted with a first episode
of uncomplicated acute cholecystitis – without concurrent severe sepsis, common bile duct
obstruction or pancreatitis.
Probabilities
The analyses detailed in Chapters 5 and 6 provided the foundation for deriving most of
the model probabilities (Table 7.1).
Briefly, a cohort of patients with acute cholecystitis was first defined from
deterministically-linked population-based databases including all ED visits, hospitals admissions
and day surgeries in Ontario, Canada. All adults admitted to hospital from April, 2004 to March
2011, with a most responsible diagnosis of acute cholecystitis were identified. The cohort was
restricted to patients admitted through the ED and without prior gallstone disease – no gallstone-
related ED visit or hospital admission in the preceding 2 years. We excluded patients with biliary
tract obstruction or pancreatitis on the index admission in addition to patients considered to have
severe cholecystitis, defined as those directly admitted to an intensive care unit or whose disease
was treated with a cholecystostomy tube.
From this cohort, outcome probabilities specific to each of the three modeled
management strategies were derived. To do so, three propensity-score matched groups were
defined: (1) patients managed with early cholecystectomy – within 7 days of ED presentation,
(2) patients managed with delayed cholecystectomy – between 7 days from ED presentation and
108
1 year following discharge, and (3) patients discharged from the initial cholecystitis admission
without cholecystectomy. The first and second matched groups were used to determine the
frequency of operative outcomes and mortality for all three strategies. The third matched group
was used to calculate the risk of recurrent gallstone-related symptoms, relevant only to the
delayed and watchful waiting strategies.
As per the approach described in Chapter 6, patients managed with early and delayed
cholecystectomy were matched on propensity of treatment (early or delayed cholecystectomy),
age (within 5 years) and sex in order to control for factors that might have confounded the
relationship between timing of cholecystectomy and operative outcomes. The confounders
contributing to the propensity score included patient (age, sex, comorbidity level, income level)
and surgeon (years since medical school graduation and cholecystectomy experience)
characteristics as previously described in chapter 6 (see 7.8 - Supplemental data). The relevant
operative outcomes included the frequency of open cholecystectomy, major bile duct injury and
other complications. When calculating operative outcome probabilities, distinction was made
between delayed urgent cholecystectomy, occurring because of a recurrent gallstone-related
event, and delayed elective cholecystectomy. A cholecystectomy was considered elective if the
operation took place in day surgery or the hospital admission was elective.
Major bile duct injury was identified based on the presence of a billing code for biliary
tract repair or reconstruction within 6 months of cholecystectomy (OHIP billing claim: S281,
S285 – choledochoenterostomy; S292 – repair of common duct) as previously described. Other
cholecystectomy-related complications were identified based on ICD-10-CA diagnosis codes
identified on the same visit as the index cholecystectomy or within 30 days of cholecystectomy
The diagnosis codes considered complications of cholecystectomy included – T81.0
109
Haemorrhage and haematoma complicating a procedure, T81.3 Disruption of operation wound
(dehiscence), T81.4 Infection following a procedure, including post-procedural intra-abdominal
abscess, post-procedural wound infection and post-procedural sepsis.
Finally, patients discharged from hospital without cholecystectomy were matched to the
early cholecystectomy group on age (within 5 years), sex and propensity for group membership,
based on patient characteristics only (see 7.8 - Supplemental data). As per the approach
described in Chapter 5, this third matched group provided the probability of recurrent gallstone-
related symptoms (ED visit or hospital admission for gallstone disease)132.
These inputs were supplemented with data from a Cochrane meta-analysis of randomized
trials comparing early to delayed cholecystectomy for acute cholecystitis71. Due to difficulty
ascertaining bile leaks in our administrative data, the relative frequency of this complication was
taken from the meta-analysis. The meta-analysis included five single-center trials and was not
used as the primary data source since the trials have limited contemporary external validity and
lacked power to compare costly major bile duct injuries and death. However, all meta-analysis
outcome estimates were incorporated into one-way sensitivity analysis ranges detailed below.
Costs
Hospital costs were estimated using the Resource Intensity Weight (RIW) method100.
Each ED visit, hospital admission and day surgery is assigned an RIW value, which when
multiplied by the provincial average cost per weighted case (CPWC), estimates the cost of a
patient`s visit. The RIW value for a given admission reflects a patient`s level of resource
utilization during that admission and is based on the patient`s major diagnosis, age, comorbidity
110
burden, interventions received and length of stay. The CPWC values are year and visit type
specific (e.g. inpatient stay in fiscal year 2009), and they are derived from the allocation of
global hospital budgets across all patients (total annual budget divided by sum of all patients’
RIWs). Both direct medical and overhead hospital costs associated with relevant ED visits,
inpatient stays and day surgery were thus included in our model. Furthermore, since surgeons’
services are largely reimbursed on a fee-for-service basis in Ontario, hospital costs were
supplemented with the cost of specific physician claims, priced according to the Ontario Health
Insurance Plan schedule of benefits for physician services101 (Table 7.1).
Quality-adjusted life-years
QALY gains over the 5 year time horizon were derived from utility values. A utility is a
numerical measure of preference for a particular health state under conditions of uncertainty, and
is expressed on a scale from 0 (reflecting death) to 1.0 (representing perfect health)72. The
quantity of QALYs associated with an outcome is calculated by multiplying the utility value of
the relevant health state by the duration of time spent in that health state. For example, 6 months
of life with a major bile duct injury requiring operative repair would have a value of 0.32
QALYs (utility value of 0.64 multiplied by 0.5 years). Utilities for our model were obtained from
review of the literature and the Cost-Effectiveness Analysis Registry of the Institute for Clinical
Research and Health Policy Studies, Tufts Medical Center146. When multiple utility values were
identified, those directly elicited under conditions of uncertainty (standard gamble) were used
with the remaining values incorporated in sensitivity analysis. The majority of the utility values
were obtained from a cohort of general medical patients without prior gallstone disease, with

111
similar age and sex distributions to the population-based cohort used to derive the outcome
transition probabilities 147(Table 7.1).
Analysis
The model was first evaluated using cohort simulation. Cohort simulation refers to the
process of running a hypothetical cohort of patients from the starting health state (i.e. acute
cholecystitis) through to the end of the time horizon. At each cycle during the cohort simulation,
costs and QALY gains are added to a running total based on the distribution of the cohort across
health states. Changes in the distribution of patients across health states, from one cycle to the
next, are dictated by the defined transition probability point estimates (Table 7.1). The cohort
simulation was run three times, once for each treatment strategy. The final result is an average
per patient total cost and QALY gains over 5 years for each strategy.
We evaluated the robustness of the results through a number of sensitivity analyses.
Parameter uncertainty was first evaluated through one-way and two-way sensitivity analyses.
One-way sensitivity analysis offers an understanding of the sensitivity of the results to individual
input parameters by varying each parameter value one at a time while keeping the others fixed.
For each parameter, the threshold at which the study conclusions changed was reported if one
existed. Two-way sensitivity analysis was also undertaken. Both these analyses confirmed that
changes of input parameters had predictable effects on model outcomes (internal consistency).
Next, in order to evaluate uncertainty of all parameters simultaneously, probabilistic sensitivity
analysis (PSA) was undertaken and involved second-order Monte Carlo simulation (10,000
iterations of the previously described cohort simulation). For every iteration, a new value for
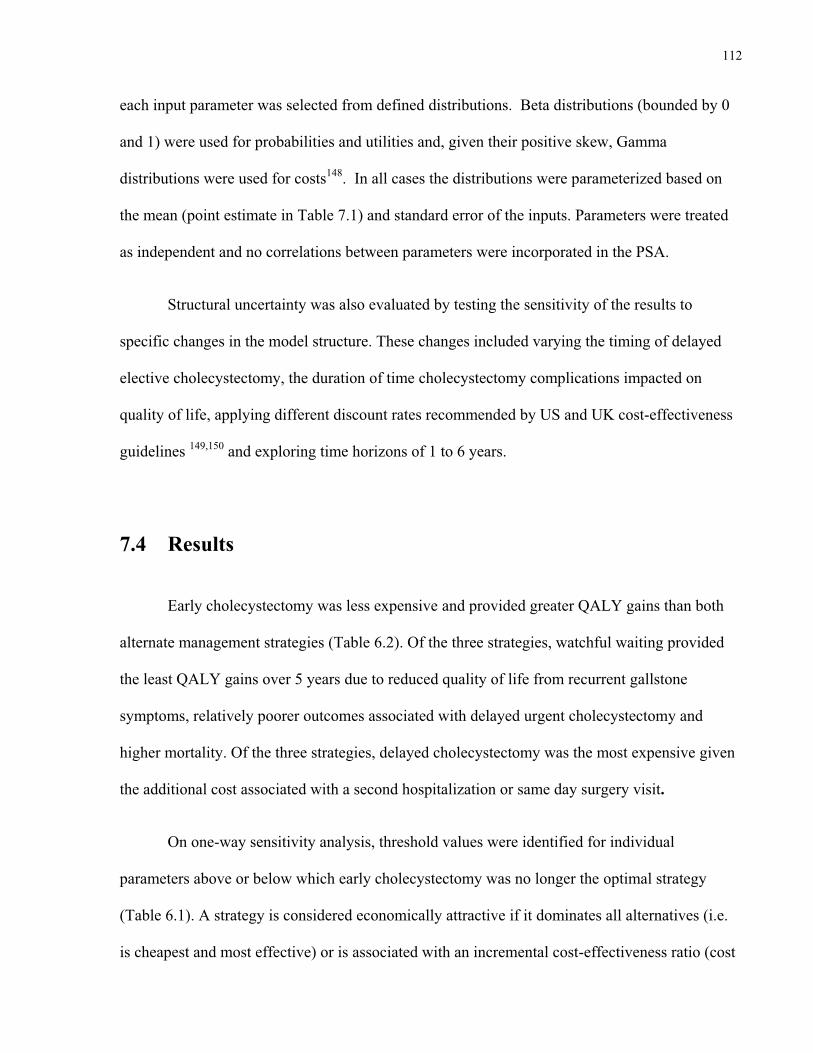
112
each input parameter was selected from defined distributions. Beta distributions (bounded by 0
and 1) were used for probabilities and utilities and, given their positive skew, Gamma
distributions were used for costs148. In all cases the distributions were parameterized based on
the mean (point estimate in Table 7.1) and standard error of the inputs. Parameters were treated
as independent and no correlations between parameters were incorporated in the PSA.
Structural uncertainty was also evaluated by testing the sensitivity of the results to
specific changes in the model structure. These changes included varying the timing of delayed
elective cholecystectomy, the duration of time cholecystectomy complications impacted on
quality of life, applying different discount rates recommended by US and UK cost-effectiveness
guidelines 149,150 and exploring time horizons of 1 to 6 years.
7.4 Results
Early cholecystectomy was less expensive and provided greater QALY gains than both
alternate management strategies (Table 6.2). Of the three strategies, watchful waiting provided
the least QALY gains over 5 years due to reduced quality of life from recurrent gallstone
symptoms, relatively poorer outcomes associated with delayed urgent cholecystectomy and
higher mortality. Of the three strategies, delayed cholecystectomy was the most expensive given
the additional cost associated with a second hospitalization or same day surgery visit.
On one-way sensitivity analysis, threshold values were identified for individual
parameters above or below which early cholecystectomy was no longer the optimal strategy
(Table 6.1). A strategy is considered economically attractive if it dominates all alternatives (i.e.
is cheapest and most effective) or is associated with an incremental cost-effectiveness ratio (cost
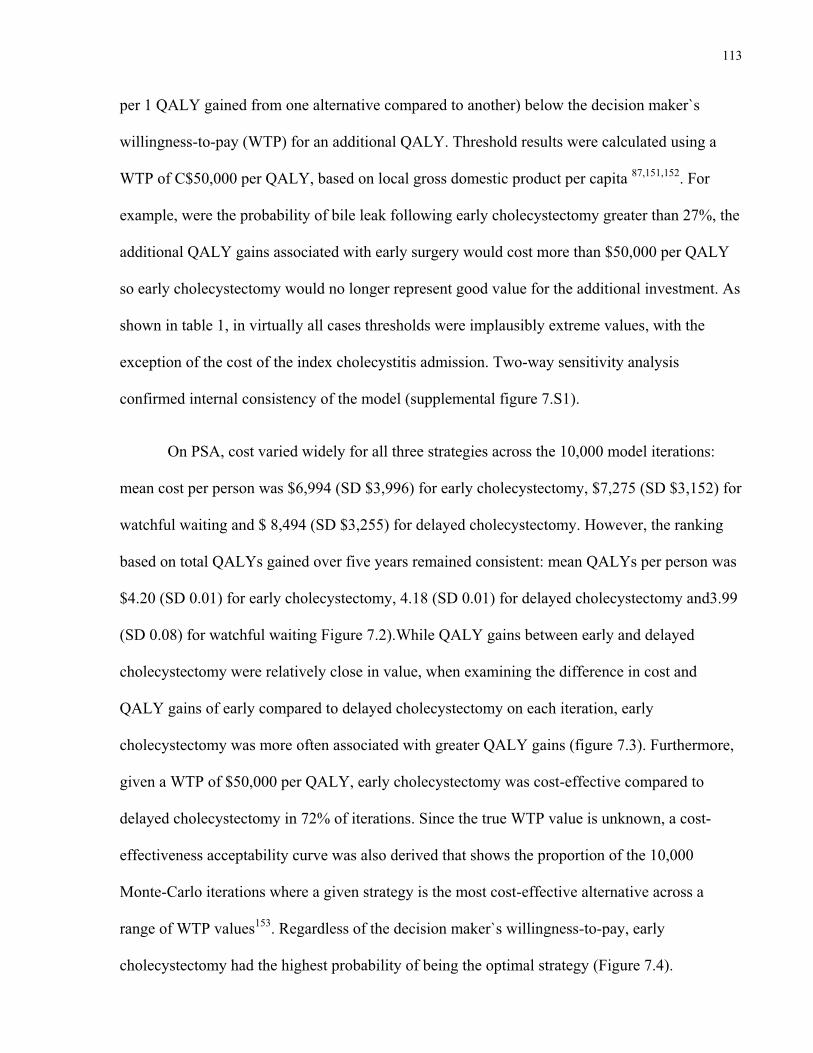
113
per 1 QALY gained from one alternative compared to another) below the decision maker`s
willingness-to-pay (WTP) for an additional QALY. Threshold results were calculated using a
WTP of C$50,000 per QALY, based on local gross domestic product per capita 87,151,152. For
example, were the probability of bile leak following early cholecystectomy greater than 27%, the
additional QALY gains associated with early surgery would cost more than $50,000 per QALY
so early cholecystectomy would no longer represent good value for the additional investment. As
shown in table 1, in virtually all cases thresholds were implausibly extreme values, with the
exception of the cost of the index cholecystitis admission. Two-way sensitivity analysis
confirmed internal consistency of the model (supplemental figure 7.S1).
On PSA, cost varied widely for all three strategies across the 10,000 model iterations:
mean cost per person was $6,994 (SD $3,996) for early cholecystectomy, $7,275 (SD $3,152) for
watchful waiting and $ 8,494 (SD $3,255) for delayed cholecystectomy. However, the ranking
based on total QALYs gained over five years remained consistent: mean QALYs per person was
$4.20 (SD 0.01) for early cholecystectomy, 4.18 (SD 0.01) for delayed cholecystectomy and3.99
(SD 0.08) for watchful waiting Figure 7.2).While QALY gains between early and delayed
cholecystectomy were relatively close in value, when examining the difference in cost and
QALY gains of early compared to delayed cholecystectomy on each iteration, early
cholecystectomy was more often associated with greater QALY gains (figure 7.3). Furthermore,
given a WTP of $50,000 per QALY, early cholecystectomy was cost-effective compared to
delayed cholecystectomy in 72% of iterations. Since the true WTP value is unknown, a cost-
effectiveness acceptability curve was also derived that shows the proportion of the 10,000
Monte-Carlo iterations where a given strategy is the most cost-effective alternative across a
range of WTP values153. Regardless of the decision maker`s willingness-to-pay, early
cholecystectomy had the highest probability of being the optimal strategy (Figure 7.4).
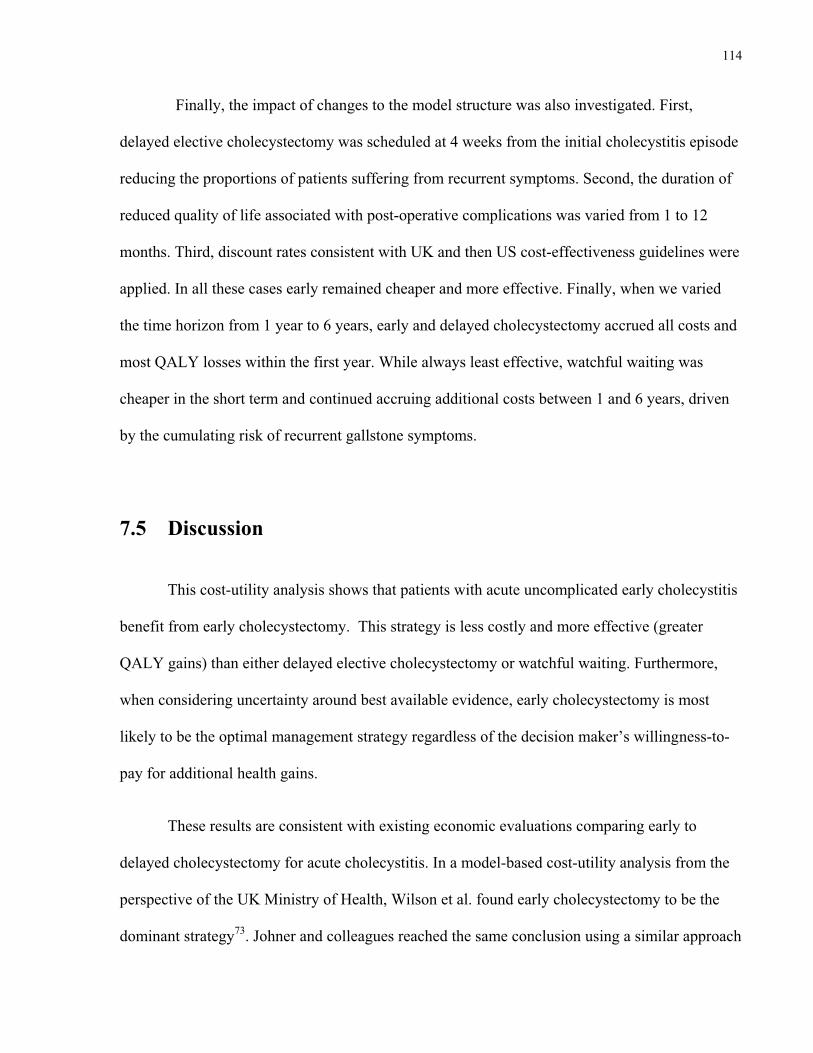
114
Finally, the impact of changes to the model structure was also investigated. First,
delayed elective cholecystectomy was scheduled at 4 weeks from the initial cholecystitis episode
reducing the proportions of patients suffering from recurrent symptoms. Second, the duration of
reduced quality of life associated with post-operative complications was varied from 1 to 12
months. Third, discount rates consistent with UK and then US cost-effectiveness guidelines were
applied. In all these cases early remained cheaper and more effective. Finally, when we varied
the time horizon from 1 year to 6 years, early and delayed cholecystectomy accrued all costs and
most QALY losses within the first year. While always least effective, watchful waiting was
cheaper in the short term and continued accruing additional costs between 1 and 6 years, driven
by the cumulating risk of recurrent gallstone symptoms.
7.5 Discussion
This cost-utility analysis shows that patients with acute uncomplicated early cholecystitis
benefit from early cholecystectomy. This strategy is less costly and more effective (greater
QALY gains) than either delayed elective cholecystectomy or watchful waiting. Furthermore,
when considering uncertainty around best available evidence, early cholecystectomy is most
likely to be the optimal management strategy regardless of the decision maker’s willingness-to-
pay for additional health gains.
These results are consistent with existing economic evaluations comparing early to
delayed cholecystectomy for acute cholecystitis. In a model-based cost-utility analysis from the
perspective of the UK Ministry of Health, Wilson et al. found early cholecystectomy to be the
dominant strategy73. Johner and colleagues reached the same conclusion using a similar approach
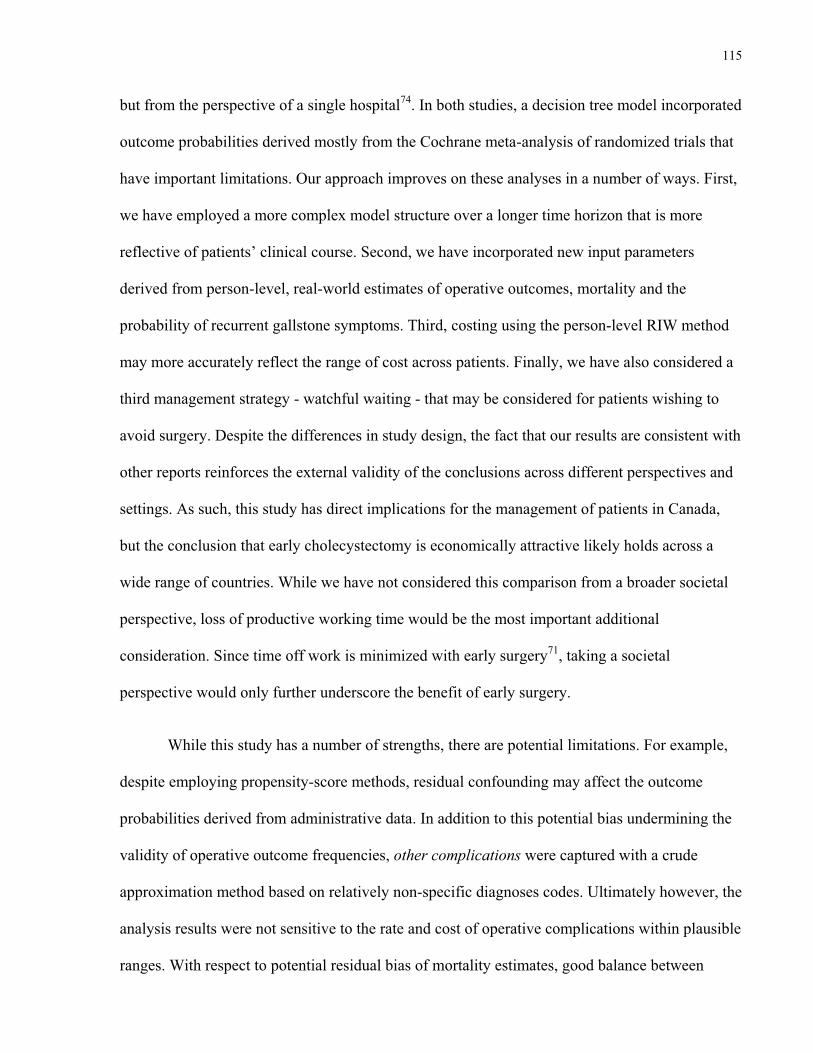
115
but from the perspective of a single hospital74. In both studies, a decision tree model incorporated
outcome probabilities derived mostly from the Cochrane meta-analysis of randomized trials that
have important limitations. Our approach improves on these analyses in a number of ways. First,
we have employed a more complex model structure over a longer time horizon that is more
reflective of patients’ clinical course. Second, we have incorporated new input parameters
derived from person-level, real-world estimates of operative outcomes, mortality and the
probability of recurrent gallstone symptoms. Third, costing using the person-level RIW method
may more accurately reflect the range of cost across patients. Finally, we have also considered a
third management strategy - watchful waiting - that may be considered for patients wishing to
avoid surgery. Despite the differences in study design, the fact that our results are consistent with
other reports reinforces the external validity of the conclusions across different perspectives and
settings. As such, this study has direct implications for the management of patients in Canada,
but the conclusion that early cholecystectomy is economically attractive likely holds across a
wide range of countries. While we have not considered this comparison from a broader societal
perspective, loss of productive working time would be the most important additional
consideration. Since time off work is minimized with early surgery71, taking a societal
perspective would only further underscore the benefit of early surgery.
While this study has a number of strengths, there are potential limitations. For example,
despite employing propensity-score methods, residual confounding may affect the outcome
probabilities derived from administrative data. In addition to this potential bias undermining the
validity of operative outcome frequencies, other complications were captured with a crude
approximation method based on relatively non-specific diagnoses codes. Ultimately however, the
analysis results were not sensitive to the rate and cost of operative complications within plausible
ranges. With respect to potential residual bias of mortality estimates, good balance between
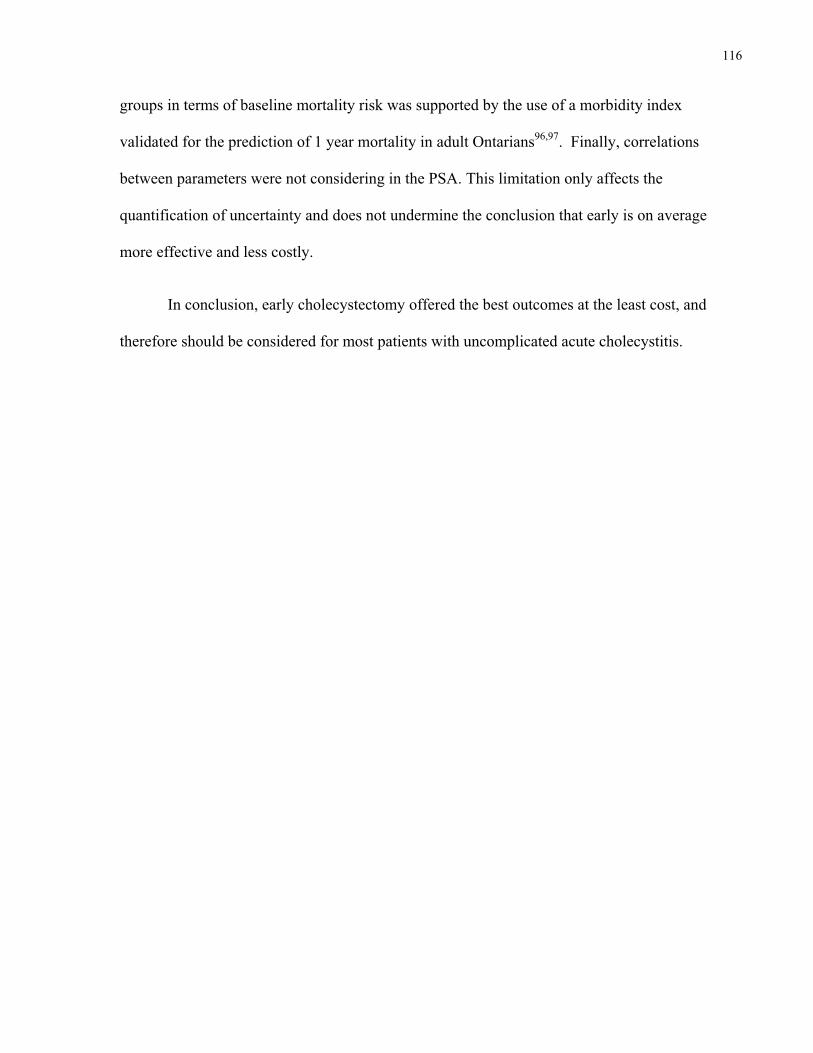
116
groups in terms of baseline mortality risk was supported by the use of a morbidity index
validated for the prediction of 1 year mortality in adult Ontarians96,97. Finally, correlations
between parameters were not considering in the PSA. This limitation only affects the
quantification of uncertainty and does not undermine the conclusion that early is on average
more effective and less costly.
In conclusion, early cholecystectomy offered the best outcomes at the least cost, and
therefore should be considered for most patients with uncomplicated acute cholecystitis.

117
7.6 Tables for Chapter 7
Table 7.1 - Model parameter inputs with sources and threshold analysis results
Point estimate Sourcea Thresholdb
PROBABILITIES
Early cholecystectomy Open cholecystectomy 15% - >53% Major bile duct injury 0.2% - >8.9% Bile leak 3.1% 71 >27% Other complication 4.1% - >73%
Mortality KM c - >30% increase
Delayed cholecystectomy Open cholecystectomy – elective cholecystectomy 12% - None Major bile duct injury – elective cholecystectomy 0.5% - None Bile leak – elective cholecystectomy 0% 71 None Other complication – elective cholecystectomy 4.4% - None Open cholecystectomy – urgent cholecystectomy 24% - None Major bile duct injury – urgent cholecystectomy 0.5% - None Bile leak – urgent cholecystectomy 0% 71 None Other complication – urgent cholecystectomy 5.2% - None Risk of recurrent gallstone-related symptoms KM c - None
Biliary colic or cholecystitis as recurrent eventd 68% - None Choledocholithiasis as recurrent eventd 25% - None Acute pancreatitis as recurrent eventd 7% - None
Mortality KM c - >30% decrease
Watchful waiting Open cholecystectomy – urgent cholecystectomy 24% - None Major bile duct injury – urgent cholecystectomy 0.5% - None Bile leak – urgent cholecystectomy 0% 71 None Other complication – urgent cholecystectomy 5.2% - None Gallstone-related recurrent symptoms KM c - None
Biliary colic or cholecystitis as recurrent eventd 68% - None Choledocholithiasis as recurrent eventd 25% - None Acute pancreatitis as recurrent eventd 7% - None
Mortality KM c - >85% decrease
UTILITY VALUES Acute cholecystitis admission 0.77 147 None
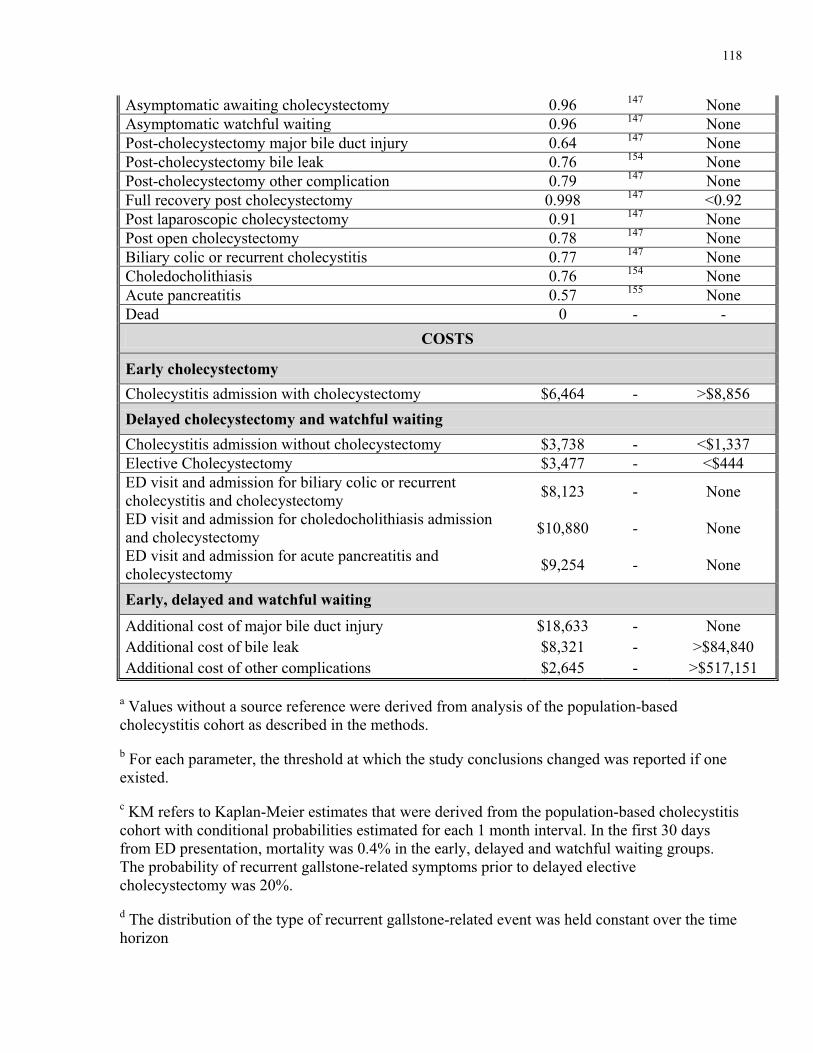
118
Asymptomatic awaiting cholecystectomy 0.96 147 None Asymptomatic watchful waiting 0.96 147 None Post-cholecystectomy major bile duct injury 0.64 147 None Post-cholecystectomy bile leak 0.76 154 None Post-cholecystectomy other complication 0.79 147 None Full recovery post cholecystectomy 0.998 147 <0.92 Post laparoscopic cholecystectomy 0.91 147 None Post open cholecystectomy 0.78 147 None Biliary colic or recurrent cholecystitis 0.77 147 None Choledocholithiasis 0.76 154 None Acute pancreatitis 0.57 155 None Dead 0 - -
COSTS
Early cholecystectomy Cholecystitis admission with cholecystectomy $6,464 - >$8,856 Delayed cholecystectomy and watchful waiting Cholecystitis admission without cholecystectomy $3,738 - <$1,337 Elective Cholecystectomy $3,477 - <$444 ED visit and admission for biliary colic or recurrent cholecystitis and cholecystectomy $8,123 - None
ED visit and admission for choledocholithiasis admission and cholecystectomy $10,880 - None
ED visit and admission for acute pancreatitis and cholecystectomy $9,254 - None
Early, delayed and watchful waiting
Additional cost of major bile duct injury $18,633 - None Additional cost of bile leak $8,321 - >$84,840 Additional cost of other complications $2,645 - >$517,151
a Values without a source reference were derived from analysis of the population-based cholecystitis cohort as described in the methods.
b For each parameter, the threshold at which the study conclusions changed was reported if one existed.
c KM refers to Kaplan-Meier estimates that were derived from the population-based cholecystitis cohort with conditional probabilities estimated for each 1 month interval. In the first 30 days from ED presentation, mortality was 0.4% in the early, delayed and watchful waiting groups. The probability of recurrent gallstone-related symptoms prior to delayed elective cholecystectomy was 20%.
d The distribution of the type of recurrent gallstone-related event was held constant over the time horizon
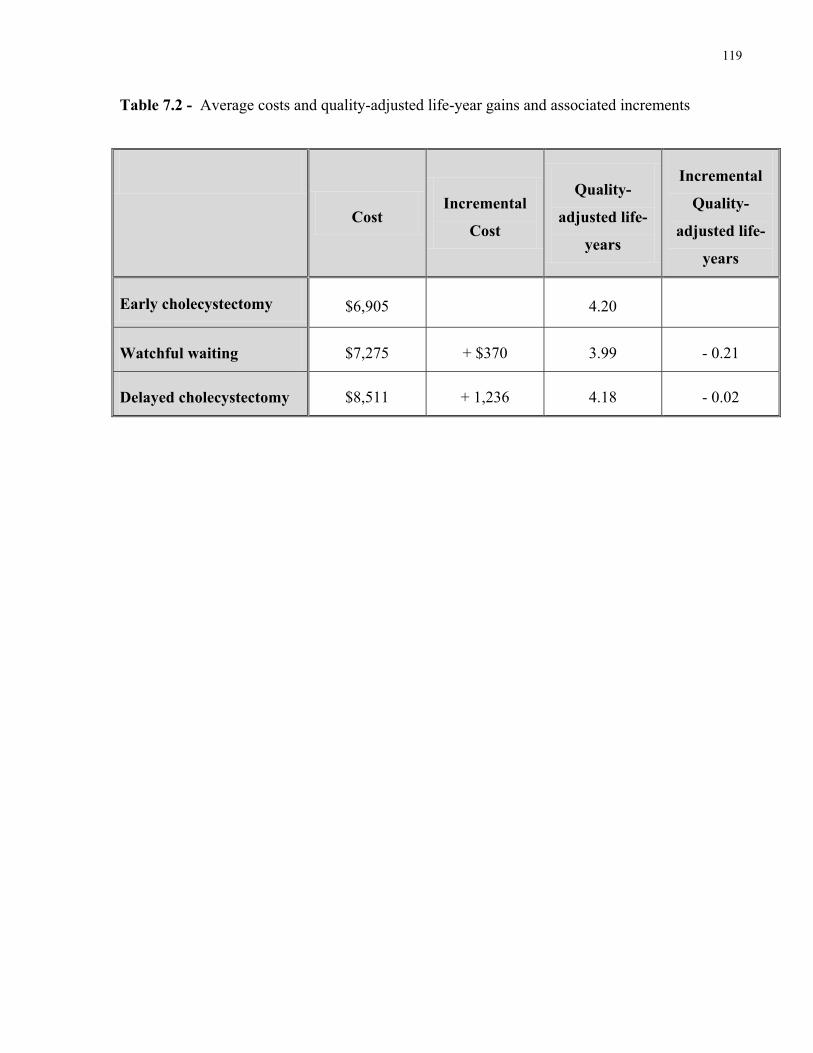
119
Table 7.2 - Average costs and quality-adjusted life-year gains and associated increments
Cost Incremental
Cost
Quality-
adjusted life-
years
Incremental
Quality-
adjusted life-
years
Early cholecystectomy $6,905 4.20
Watchful waiting $7,275 + $370 3.99 - 0.21
Delayed cholecystectomy $8,511 + 1,236 4.18 - 0.02
ACUTE CHOLECYSTITIS
Asymptomatic awaiting cholecystectomy
Asymptomatic - watchful waiting
Recurrent gallstone symptomsand urgent cholecystectomy
Post cholecystectomy states
EARLY CHOLECYSTECTOMY
DELAYED CHOLECYSTECTOMY
WATCHFUL WAITING
Elective cholecystectomy
- Post-cholecystectomy major bile duct injury- Post-cholecystectomy bile leak- Post-cholecystectomy other complication- Full recovery post cholecystectomy
Charles
Text Box
Figure 7.1 Simplified representation of model state transition diagram 120
Charles
Line
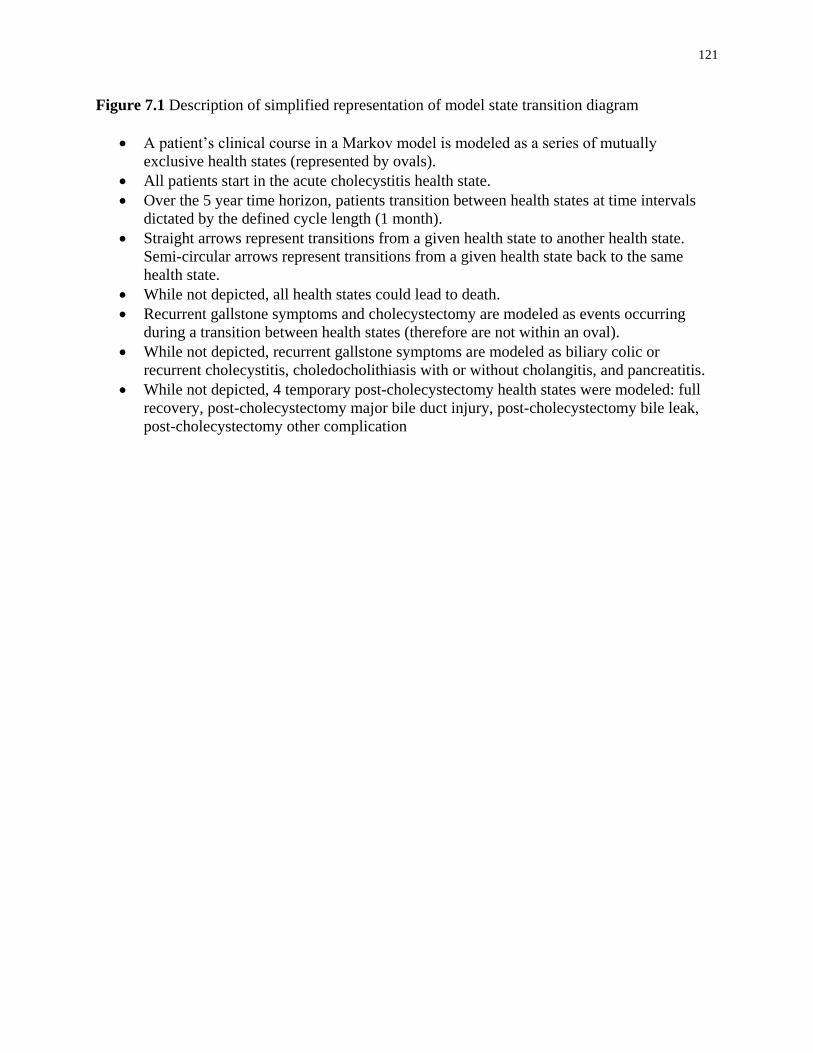
121
Figure 7.1 Description of simplified representation of model state transition diagram
A patient’s clinical course in a Markov model is modeled as a series of mutually
exclusive health states (represented by ovals).
All patients start in the acute cholecystitis health state.
Over the 5 year time horizon, patients transition between health states at time intervals
dictated by the defined cycle length (1 month).
Straight arrows represent transitions from a given health state to another health state.
Semi-circular arrows represent transitions from a given health state back to the same
health state.
While not depicted, all health states could lead to death.
Recurrent gallstone symptoms and cholecystectomy are modeled as events occurring
during a transition between health states (therefore are not within an oval).
While not depicted, recurrent gallstone symptoms are modeled as biliary colic or
recurrent cholecystitis, choledocholithiasis with or without cholangitis, and pancreatitis.
While not depicted, 4 temporary post-cholecystectomy health states were modeled: full
recovery, post-cholecystectomy major bile duct injury, post-cholecystectomy bile leak,
post-cholecystectomy other complication

Charles
Text Box
Figure 7.2 - Cost-effectiveness plane of Monte-Carlo probabilistic analysis results (10,000 iterations) 122
123
Figure 7.2 – Description of the cost-effectiveness plane of Monte-Carlo probabilistic analysis
results (10,000 iterations)
For each iteration of the Monte-Carlo simulation, the model is run three times (once for
each management strategy) and a corresponding average QALY gain (x-axis) per person
and average cost per person (y-axis) is obtained for each strategy.
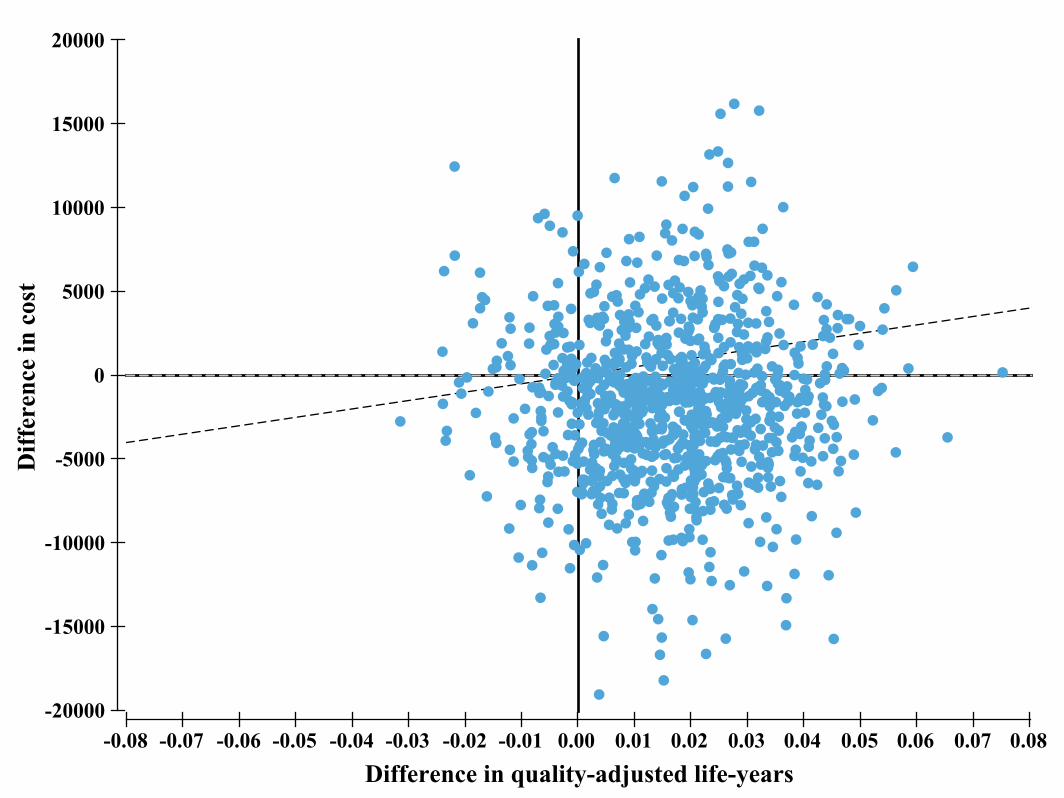
Charles
Text Box
Figure 7.3 - Incremental cost-effectiveness plane comparing early to delayed cholecystectomy 124
Charles
Callout
Willingness-to-pay threshold of $50,000 per QALY
Charles
Text Box
I
Charles
Text Box
II
Charles
Text Box
III
Charles
Text Box
IV
125
Figure 7.3 – Description of incremental cost-effectiveness plane comparing early to delayed
cholecystectomy
Each point represents one iteration of the Monte-Carlo probabilistic analysis.
The X-axis represents the difference between the average cost of early minus delayed
cholecystectomy.
The Y-axis represents the difference between the average QALY gains from early minus
delayed cholecystectomy.
In quadrants I and IV, early is more effective than delayed cholecystectomy, in quadrants
I and II, early is more expensive than delayed cholecystectomy.
Interpretation: In a majority of Monte-Carlo runs, early cholecystectomy is more
effective than delayed. Given a willingness-to-pay of $50,000 (angled broken line), early
cholecystectomy was cost-effective compared to delayed cholecystectomy in 72% of
iterations.
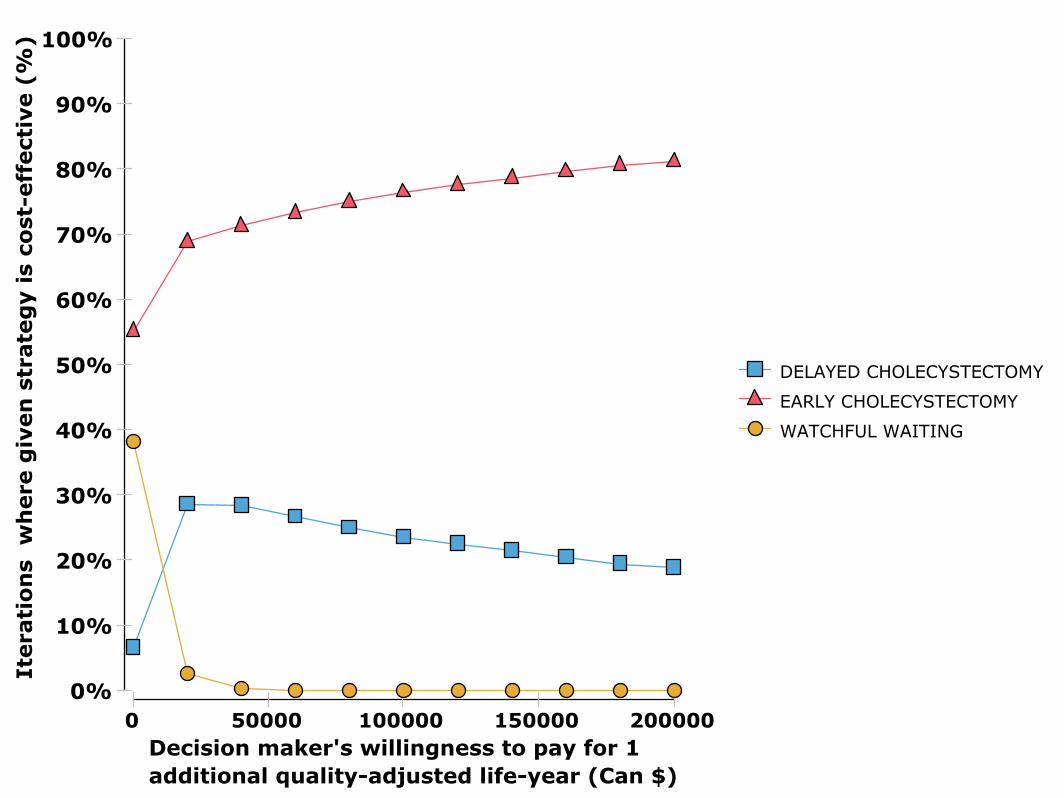
Charles
Text Box
Figure 7.4 - Cost-effectiveness acceptability curve derived from Monte-Carlo probabilistic sensitivity analysis 126

127
Figure 7.4 – Description of cost-effectiveness acceptability curve derived from Monte-Carlo
probabilistic sensitivity analysis.
For every iteration of the Monte-Carlo probabilistic analysis, a net monetary benefit
(NMB) is calculated for each of the three management strategies. The
NMB=WTP*QALYs-Cost. At a given WTP level (x-axis), the proportions of iterations
where a given strategy has the highest NMB is calculated (y-axis)
Interpretation: At a WTP=0, the average QALY gains do not contribute to NMB (since
if WTP=0 then WTP*QALY=0), therefore the least expensive strategy will have the
highest NMB. As the WTP increases, QALY gains increasingly drive the NMB value.
Since early cholecystectomy is the least expensive and the most effective, it remains most
likely to have the highest NMB (i.e. most likely to be the optimal strategy) across all
values of WTP.

128
7.8 Supplemental data for Chapter 7
A total of 31,667 adults were admitted with acute cholecystitis via the emergency
department and did not have a prior ED visit or hospital admission for gallstone disease. Of these
patients, 6,122 were excluded given concurrent severe cholecystitis (i.e. intensive care unit
admission or insertion of a cholecystostomy drain, N=1,677), biliary tract obstruction or
pancreatitis (N=4,313) and missing income level (N=132). Of the remaining 25,545 patients,
19,126 underwent cholecystectomy (either on initial admission of within 1 year of discharge) and
met additional inclusion criteria (at least 6 months of post-cholecystectomy follow-up and no
diagnosis of biliary tract malignancy within 6 months of cholecystectomy).
First and second matched groups: early and delayed cholecystectomy
These 19,126 patients were divided based on having received early (within 7 days of ED
presentation) or delayed cholecystectomy. A propensity score for receipt of early
cholecystectomy was calculated and the two groups were then matched based on the propensity
score, age (within 5 years) and sex. Characteristics of the two groups prior to the match are
presented in Table 7.S1 and characteristics of the matched cohort are presented in Table 7.S2.
Balance in covariates between groups after matching was confirmed by verifying that the
standardized difference was less than 10%. The distributions of continuous variables were also
compared graphically through cumulative density and quantile-quantile plots. All characteristics
were well balanced with standardized differences of at most 3% as well as similar distributions
of continuous variables when verified graphically.
Third matched group: patients discharged without cholecystectomy following initial cholecystitis
admission

129
Starting from 25,545 patients described above, 15,162 underwent cholecystectomy on the
index admission. Another 79 patients died during the index admission leaving 10,304 patients
discharged without cholecystectomy. This group was matched to the 5,676 matched early group
previously. The propensity score and matching process was similar to the first match with the
exception that only patient characteristics were used to derive the propensity score.
Characteristics of the two groups prior to the match are presented in Table S3 and characteristics
of the matched cohort are presented in Table S4. All characteristics were well balanced with
standardized differences of at most 2% as well as similar distributions of continuous variables
when verified graphically.

130
Table 7.S1 - Baseline characteristics of patients and their surgeon before matching
Characteristic Early
cholecystectomy (n=13,212)
Delayed cholecystectomy
(n=5,700) P valuea Patient characteristics
Age, year mean (SD) 52 (18) 56 (17) <0.001 ≥65 years, no. (%) 3,594 (28) 2,020 (35) <0.001
Female sex, no. (%) 5,093 (39) 2,487 (44) <0.001 Income Quintile, no. (%) 0.62
1 2,831 (22) 1,194 (21) 2 2,802 (21) 1,243 (22) 3 2,569 (19) 1,141 (20) 4 2,609 (20) 1,121 (19) 5b 2,401 (18) 1,001 (17)
ADG comorbidity index mean (SD) 2±13 4±13 <0.001 highest quartile, no. (%) 2,899 (22) 1,514 (27) <0.001
Surgeon characteristics Years since medical school graduation
mean (SD) 21(10) 22(10) <0.001 highest quartile (≥29) , no. (%) 2,882 (22) 1,574 (28) <0.001
Number of cholecystectomies in preceding year
mean (SD) 74 (52) 66 (40) <0.001 highest quartile (≥90), no. (%) 3,659 (28) 1,077 (19) <0.001
aA chi-square test was used for categorical variables and a t-test was used for continuous variables bHighest income level
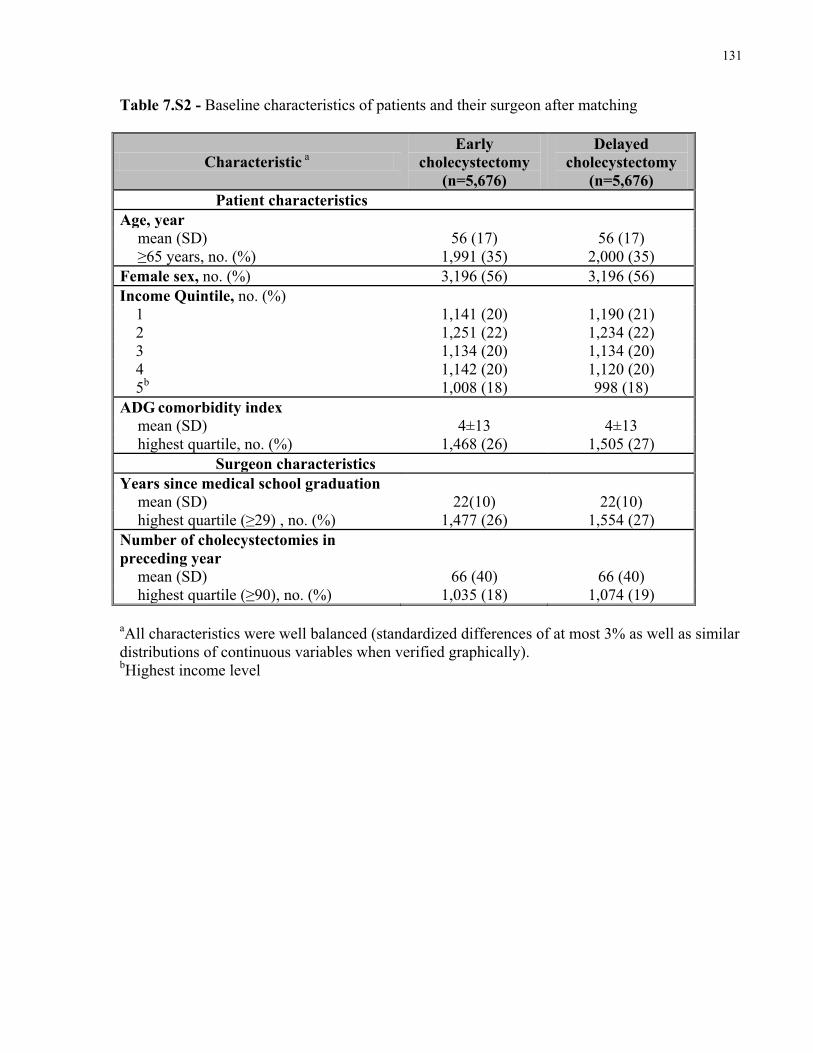
131
Table 7.S2 - Baseline characteristics of patients and their surgeon after matching
Characteristic a Early
cholecystectomy (n=5,676)
Delayed cholecystectomy
(n=5,676) Patient characteristics
Age, year mean (SD) 56 (17) 56 (17) ≥65 years, no. (%) 1,991 (35) 2,000 (35)
Female sex, no. (%) 3,196 (56) 3,196 (56) Income Quintile, no. (%)
1 1,141 (20) 1,190 (21) 2 1,251 (22) 1,234 (22) 3 1,134 (20) 1,134 (20) 4 1,142 (20) 1,120 (20) 5b 1,008 (18) 998 (18)
ADG comorbidity index mean (SD) 4±13 4±13 highest quartile, no. (%) 1,468 (26) 1,505 (27)
Surgeon characteristics Years since medical school graduation
mean (SD) 22(10) 22(10) highest quartile (≥29) , no. (%) 1,477 (26) 1,554 (27)
Number of cholecystectomies in preceding year
mean (SD) 66 (40) 66 (40) highest quartile (≥90), no. (%) 1,035 (18) 1,074 (19)
aAll characteristics were well balanced (standardized differences of at most 3% as well as similar distributions of continuous variables when verified graphically). bHighest income level

132
Table 7.S3 - Baseline characteristics of patients before matching
Characteristic Early
cholecystectomy (n=5,676)
Delayed cholecystectomy
(n=10,304) P valuea
Age, year mean (SD) 56 (17) 60 (19) <0.001 ≥65 years, no. (%) 1,991 (35) 4,539 (44) <0.001
Female sex, no. (%) 3,196 (56) 5,559 (54) 0.004 Income Quintile, no. (%) 0.05
1 1,141 (20) 2,253 (22) 2 1,251 (22) 2,270 (22) 3 1,134 (20) 2,025 (20) 4 1,142 (20) 1,927 (18) 5b 1,008 (18) 1,829 (18)
ADG comorbidity index mean (SD) 4±13 6±14 <0.001 highest quartile, no. (%) 1,157 (20) 2,734 (27) <0.001
aA chi-square test was used for categorical variables and a t-test was used for continuous variables bHighest income level
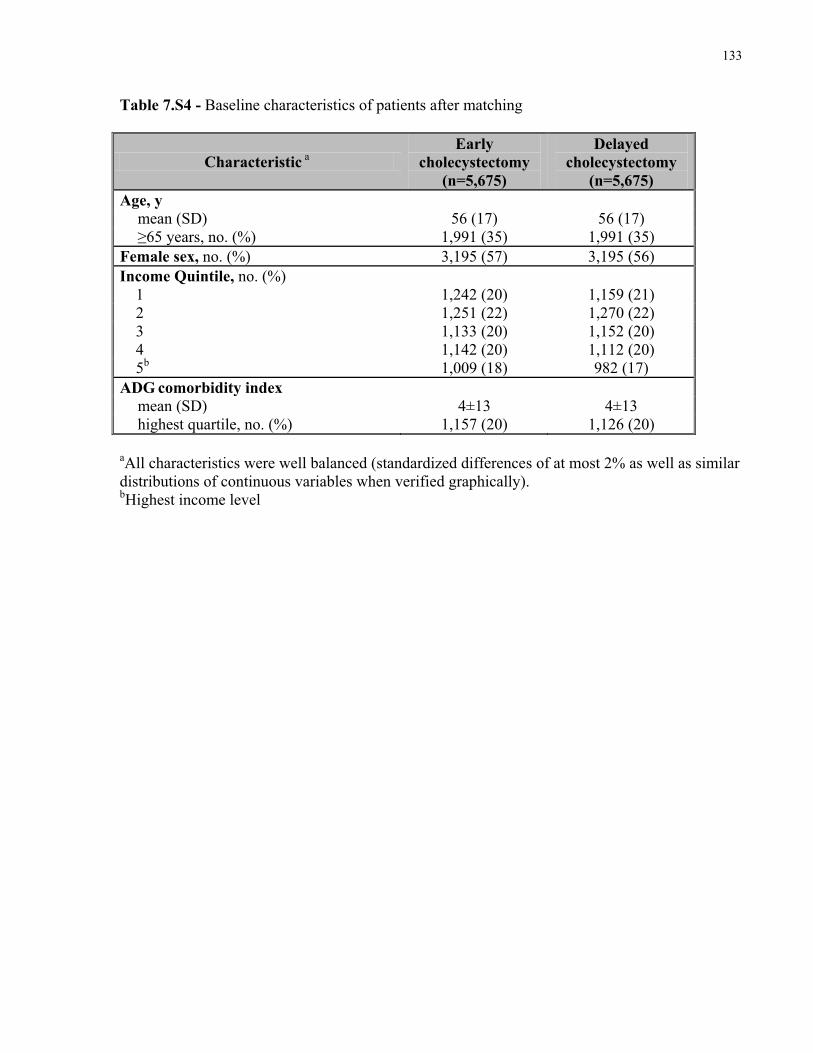
133
Table 7.S4 - Baseline characteristics of patients after matching
Characteristic a Early
cholecystectomy (n=5,675)
Delayed cholecystectomy
(n=5,675) Age, y
mean (SD) 56 (17) 56 (17) ≥65 years, no. (%) 1,991 (35) 1,991 (35)
Female sex, no. (%) 3,195 (57) 3,195 (56) Income Quintile, no. (%)
1 1,242 (20) 1,159 (21) 2 1,251 (22) 1,270 (22) 3 1,133 (20) 1,152 (20) 4 1,142 (20) 1,112 (20) 5b 1,009 (18) 982 (17)
ADG comorbidity index mean (SD) 4±13 4±13 highest quartile, no. (%) 1,157 (20) 1,126 (20)
aAll characteristics were well balanced (standardized differences of at most 2% as well as similar distributions of continuous variables when verified graphically). bHighest income level

Charles
Text Box
Figure 7.S1 - Example two-way sensitivity analysis results 134

135
Figure 7.S1 – Description of example of two-way sensitivity analysis results
The probability of a major bile duct injury(x-axis) was varied simultaneous with the
utility of major bile duct injury (y-axis).
The pink area represents values of both variables where early cholecystectomy is the
optimal strategy given a WTP of $50,000, whereas the blue area represents values for
both variables where delayed cholecystectomy would optimal.
Interpretation: Regardless of the utility of a major bile duct injury, the probability of a
major bile duct injury with early cholecystectomy would need to be unrealistically high
(>6%) to change the conclusion that early cholecystectomy is the optimal management
strategy.

136
Chapter 8
General Discussion
The purpose of this chapter is to:
I. Provide a summary of the thesis results
II. Discuss the implications
III. Review the general limitations
137
8.1 Thesis Summary
This thesis focused on characterizing the clinical outcomes and costs associated with
early and delayed cholecystectomy for acute cholecystitis. The specific aims were defined in
order to address existing gaps in knowledge comparing early to delayed cholecystectomy as well
as to provide insight into the current context of practice in Ontario. We began by characterizing
the extent of variation in early cholecystectomy, then compared early to delayed surgery with
respect to specific clinical outcomes followed by a comparison of both clinical outcomes and
cost within the framework of economic evaluation.
In the Specific Aim 1, the extent of variation in application of early cholecystectomy
(within 7 days of emergency department presentation) across hospitals in Ontario was
characterized. The median early cholecystectomy rate was 51% and wide variation was observed
across hospitals (interquartile range of 25% to 72%), even among 18-49 year old healthy patients
with uncomplicated cholecystitis (median 74%, interquartile range of 41% to 88%). When
accounting for patient characteristics on multivariable analysis, similar patients did not receive
similar care across the province (Median Odds Ratio 3.7). Hospitals seeing higher volumes of
patients with acute cholecystitis were found to confer the highest adjusted odds of early
cholecystectomy and half of the explained variation in early cholecystectomy was related to
hospital-level effects.
In the Specific Aim 2, the risk of recurrent symptoms in patients discharged without
cholecystectomy was derived. In a study sample of 10,304 patients with acute cholecystitis, the
probability of a gallstone-related emergency department visit or hospital admission by 6 weeks,
12 weeks and 1 year after discharge was 14%, 19% and 29% respectively. Of these events, 30%
were for biliary tract obstruction or pancreatitis. A difference in the risk of a gallstone-related
event was also observed across age groups, with the lowest risk observed in the oldest patients.

138
In the Specific Aim 3, we sought to address the limitations of small randomized trials
comparing early to delayed cholecystectomy for acute cholecystitis with respect to operative
outcomes. We performed the same comparison in a sample of over 20,000 patients drawn from
Ontario’s population-based administrative databases. We compared rare outcomes including
major bile duct injury and death as well as the rate of open cholecystectomy (started open or
converted) and, among laparoscopic cases, the rate of conversion to an open approach. Early
cholecystectomy was associated with half the risk of major bile duct injury as well as a lower
risk of major bile duct injury or death within six months. Finally the rate of open
cholecystectomy and conversion were not meaningfully different between exposure groups.
The final Specific Aim 4 was to perform a cost-utility analysis comparing three
management strategies for acute cholecystitis: early cholecystectomy (within 7 days of
emergency department presentation), delayed elective cholecystectomy (8 to 12 weeks from
presentation) and watchful waiting, where cholecystectomy is performed urgently only if
recurrent gallstone symptoms arise. The outcomes were costs from the perspective of the Ontario
Ministry of Health and QALYs gained over 5 years. Early cholecystectomy was on average less
costly ($6,905 per person) and more effective (4.20 QALYs per person) than delayed
cholecystectomy ($8,511; 4.18 QALYs per person) or watchful waiting ($7,274; 3.99 QALYs
per person). In probabilistic sensitivity analysis, early cholecystectomy was most likely to be the
optimal management strategy, regardless of the value a decision maker would be willing to pay
for one additional QALY.
These results represent novel data on variation in practice in Ontario as well as clinical
and economic outcomes associated with early to delayed cholecystectomy for acute cholecystitis.
This thesis work therefore offers significant added value to decision making that is applicable to
the province of Ontario and can also be generalized to a wider context of practice.
139
8.2 Implications
The implications of this thesis work should be considered when placing these results in
the context of existing best available evidence. We now know that early cholecystectomy offers
multiple benefits over delayed cholecystectomy.
First, delaying surgery is associated with a considerable risk of recurrent symptoms. This
risk is approximately 20% by 3 months following discharge based on existing trials and
observational studies 15,46,89 as well as the Chapter 5 results in this thesis. This risk represents one
of the most convincing arguments against delaying surgery,
Second, based on a similar rate of conversion to open cholecystectomy and low rates of
serious complications in both early and delayed groups in randomized trials, early
cholecystectomy was deemed ‘safe’ given appropriate surgical experience. However, valid
concern remained that urgent early surgery in the setting of acute inflammation might confer a
higher risk of rare but devastating complications such as bile duct injury. This analysis has not
only confirmed that the rate of open cholecystectomy and conversion is similar across a broad
group of patients, but it also shows a benefit of early cholecystectomy in terms of major bile duct
injury. These results therefore support a shift in thinking. Early cholecystectomy should no
longer simply be viewed as safe compared to delayed surgery but, in fact, should be considered
superior to delaying intervention in terms of rare operative outcomes. The development of
fibrosis in and around Calot’s triangle following resolution of the initial bout of acute
cholecystitis may explain the increased risk of major bile duct injury when delaying surgery
130,131. Although bile duct injuries are rare, given the serious morbidity, increased mortality and
high litigation rates associated with this injury, a seemingly subtle shift in thinking may in fact
be the catalyst of a further shift in practice towards early cholecystectomy for most patients.
140
Third, randomized controlled trials in both the open and laparoscopic era consistently
showed that early surgery was associated with a shorter total hospital length of stay. Since
hospital stay is the main source of costs associated with the surgical management of acute
cholecystitis, it is reasonable that early surgery would be less costly than delayed surgery. While
the clinical and costs benefits are clear, the formal economic evaluation in this thesis is useful on
multiple grounds. Not only does the cost-utility analysis in this thesis provide economic evidence
most directly relevant to Ontario but the conclusion that early cholecystectomy is the dominant
strategy also hold external validity. This external validity can be based on the fact that the results
are consistent with two other cost-utility analyses using distinct modeling approaches, outcome
probabilities sources, and perspective for costing. In addition, our study as well as that published
by Wilson and colleagues suggests a high probability that early cholecystectomy is the optimal
management strategy when considering uncertainty around clinical outcome and cost estimates.
Overall, the economic evaluation in this thesis should be viewed a suggesting an economic
benefit of early surgery that compliments the evidence of clinical benefit. Such data may be of
particular interest to healthcare administrators striving to support the provision of best clinical
care while containing healthcare spending.
Finally, the variation in practice observed across Ontario suggests inconsistency with best
available evidence at many hospitals. The importance of hospital-level effects in explaining
variation in early cholecystectomy independently of patient-level effects suggests that the
implementation of hospital specific measures to facilitate early cholecystectomy should be
considered.
141
8.3 Limitations
8.3.1 Inability to capture variation at the physician-level
The major limitation associated with Specific Aim 1 is the inability to identify the
decision making physician using the administrative data sources. As a result some of the
unexplained variation in practice may be explained by physician-level effects. However, while a
surgeon’s comfort with difficult laparoscopic cholecystectomy might influence management of
some patients, it is unlikely that it would explain the wide range of variation in early
cholecystectomy observed across the province. Furthermore, as mentioned previously the
characteristics of hospitals included in our analysis are closely related to characteristics of the
surgeons working within them. While, future research should focus on identifying and
distinguishing barriers to early cholecystectomy at the physician and hospital level,
understanding variation at the hospital level remains a constructive starting point to generate
solutions for quality improvement.
8.3.2 Differentiating the type of gallstone-related admission
As mentioned in Chapter 3, while ICD-10 coding clearly permits the differentiation of the
different types of gallstone-related complications (e.g. biliary colic, cholecystits,
choledocholithiasis, gallstone pancreatitis, etc.) the accuracy of this differentiation has not been
validated. This limitation has impact in terms of identifying the proportion of patients with
complicated cholecystitis (i.e. same presentation biliary tract obstruction or pancreatitis) for
Specific Aims 1 and 3. Furthermore, it also affects the accuracy around the type of recurrent
gallstone-related event described in Specific Aims 2 and 4. Nevertheless, unlike many other
medical diagnoses, data coders can generally find documentation (i.e. imaging reports, operative
142
reports, pathology reports) to help differentiate the type of gallstone disease, thereby supporting
the likely accuracy of the most responsible diagnosis code.
8.3.3 Limited scope of operative outcomes
The major limitation that applies to the comparison of operative outcomes in Specific
Aim 3 is that only a limited number of specific outcomes can be reasonably captured within
Ontario’s administrative health data. While the validity of mortality, major bile duct injury, open
cholecystectomy and conversion as outcomes can be justified (seen Chapter 6, section 6.2
Methods), other surgical and medical complications cannot be ascertained with certainty.
Contemporary randomized trials or validated registry studies would be useful to understand the
comparative risk of complications such as bile leak, surgical site infection and other medical
complications.
8.3.4 Potential for residual confounding
Residual confounding is the main limitation affecting the comparison of operative
outcomes between early and delayed cholecystectomy. A gradient of cholecystitis severity is
likely the most important source of residual confounding and, as detailed in the chapter 6
discussion, there are number of reason to suggest that any difference in severity gradient between
groups is minimal. Ultimately however, if residual confounding is present, the results are likely
biased against early intervention. Since the definition of early surgery is a wide timeframe (7
days) patients initially managed with an intention of delaying surgery, but whose symptoms did
not resolve, are likely included in the early group. These patients based on the Tokyo guideline
severity classification have moderate as opposed to mild cholecystitis. Furthermore, a subgroup,

143
albeit small, of patients in the early group were likely healthy patients that required emergency
surgery based on the severity of their presentation.
Finally, a surgeon’s inexperience with difficult laparoscopic cholecystectomy may in
practice be reasonable justification for his or her decision not to perform early surgery. However,
from a patient’s perspective, given the benefit now further demonstrated with early
cholecystectomy, it would seem unreasonable to delay surgery if colleagues with appropriate
expertise are available. This point underscores the utility of considering this topic from the
perspective of the hospital or surgical provider group in order to develop solutions that optimize
the efficient management of acute cholecystitis

144
Chapter 9
Future Directions
The purpose of this chapter is to:
I. Present possible future directions
145
Including the publications stemming from this thesis, a large body of work now supports
early over delayed cholecystectomy for most patients with acute cholecystitis. Future efforts
should focus on understanding the context-specific determinants of management, knowledge
translation and ongoing evaluation of patient outcomes and preference.
9.1 Understanding the context-specific determinants of
management
In Specific Aim 1, we found that in nearly half of hospitals in Ontario, early
cholecystectomy was only provided to a minority of patients with acute cholecystitis. Efficiently
shifting practice at these institutions will require an understanding of the local determinants of
decision making. At the macro-level, specific barriers to early cholecystectomy within a given
practice setting (e.g. an academic health network, a regional health integration network, the
entire province) could be formally clarified through a mixed methods approach involving
interviews or focus groups as well as survey of the general surgeons. Domains of questioning
could include the surgeon’s interpretation of best available evidence and the importance of
specific barriers to offering early cholecystectomy (e.g. competing elective clinical obligations
when on call, limited operating room time, clinical scope of practice not including laparoscopic
surgery). In addition, a respondent’s opinion could also be sought regarding the utility of specific
measures to facilitate early surgery in their practice setting. These results would provide hospital
or regional administrators valuable information on which to act to facilitate early surgery. At the
micro-level, each hospital’s general surgery division members should reassess their local practice
and be well placed to identify ways to offer early surgery to a greater number of patients.
However, a macro-level assessment may be more likely to promote a universal standard of care.
146
9.2 Knowledge translation plan
A second important future direction is the development and implementation of a
knowledge translation plan. While the preliminary knowledge translation plan detailed below
focuses on efforts in Ontario and Canada, a number of the measures described should also
support knowledge translation across other settings.
The goals of the knowledge translation efforts will be twofold: (1) to disseminate the
new research results presented in this thesis and (2) to promote a shift in practice based on the
broader body of evidence supporting early over delayed cholecystectomy. A simple succinct
message will need to be delivered: “Early cholecystectomy offers superior clinical outcomes
over delayed cholecystectomy and is cost saving for the healthcare system”. The message and
the knowledge translation strategy will be tailored to the targeted audience.
Surgeons will be the primary audience but patients, hospital administrators and Ministry
of Health officials will also be targeted. Publications in peer-reviewed journals and presentations
at scientific meetings will form the basis for engaging clinicians. A number of more specific
measures could also be undertaken. For example, the Canadian Association of General Surgeons
and American College of Surgeons supports an email-based journal club that would be an
excellent way to disseminate these research results of across North America. Another local
measure would be to prepare a research brief summarizing the results and mail it to all general
surgery division heads across the province, in order to stimulate discussion at individual
hospitals. Finally, incorporation of the results from Specific Aims 2, 3 and 4 into the next
147
revision of the Tokyo Guidelines in 2018 could help promote knowledge translation
internationally.
In order to reach patients, the media will be engaged as an effective messenger. Press
releases related to publications and communications via social media (e.g. twitter,
www.healthydebate.ca) may help engage a variety of interested members of the public, the
media as well as various members of the healthcare system.
Finally, the Ontario Ministry of Health will be targeted by engaging contacts at the
Ontario Surgical Wait Times Strategy. In face-to-face discussions, the extent of variation in care
will be emphasized as well as the clinical and economic impetus for favouring early
cholecystectomy. The very successful experience of the Wait Times Strategy staff should be
critical in effectively promoting solutions to facilitate the performance of early cholecystectomy.
9.3 Ongoing evaluation of patient outcomes and preference
Ongoing evaluation of patient outcomes will be warranted as the practice of early
cholecystectomy becomes more broadly implemented. It will also be justified if modified
approaches to cholecystectomy (e.g. single port, robotic, natural orifice) become more popular
and if indications for surgical intervention evolve. The role of early cholecystectomy in moderate
to severe cholecystitis is in fact currently being evaluated in the ongoing CHOCOLATE trial
comparing early cholecystectomy to percutaneous cholecystostomy33.
In addition to capturing traditionally reported outcomes such as conversion, surgical site
infection and bile duct injury, future studies should capture health-related quality of life. A focus
on quality of life may be particularly informative for management decisions in elderly patients in
148
whom recurrent gallstone symptoms or post-operative recovery may have a greater or more
prolonged impact on quality of life.
Regular revision every 5 years of the Tokyo Guidelines should support the synthesis and
dissemination of new data as well as the identification of areas where further research is
required.
149
References 1. Shaffer E. Gallstone disease: Epidemiology of gallbladder stone disease. Best Practice
Research Clinical Gastroenterology. 2006;20(6):981-96.
2. Stinton LM, Shaffer EA. Epidemiology of gallbladder disease: Cholelithiasis and cancer. Gut
Liver. 2012;6(2):172-187.
3. Xu Q, Tao L, Wu Q, et al. Prevalences of and risk factors for biliary stones and gallbladder
polyps in a large chinese population. HPB. 2012;14(6):373-381.
4. Everhart JE, Khare M, Hill M, Maurer KR. Prevalence and ethnic differences in gallbladder
disease in the united states. Gastroenterology. 1999;117(3):632-9.
5. Attili AF, Carulli N, Roda E, et al. Epidemiology of gallstone disease in italy: Prevalence data
of the multicenter italian study on cholelithiasis (M.I.COL.). Am J Epidemiol. 1995;141(2):158-
165.
6. Barbara L, Sama C, Labate AMM, et al. A population study on the prevalence of gallstone
disease: The sirmione study. Hepatology. 1987;7(5):913-917.
7. Tsai CJ, Leitzmann MF, Willett WC, Giovannucci EL. Statin use and the risk of
cholecystectomy in women. Gastroenterology. 2009;136(5):1593-1600.
8. Bodmer M, Brauchli YB, Krahenbuhl S, Jick SS, Meier CR. Statin use and risk of gallstone
disease followed by cholecystectomy. JAMA. 2009;302(18):2001-2007.
150
9. Erichsen R, Froslev T, Lash TL, Pedersen L, Sorensen HT. Long-term statin use and the risk
of gallstone disease: A population-based case-control study. Am J Epidemiol. 2011;173(2):162-
170.
10. Kumar V, Abbas AK, Aster JC, Robbins SL. Robbins basic pathology. 9th ed. Philadelphia,
PA: Elsevier/Saunders; 2013:909.
11. Halldestam I, Enell E-, Kullman E, Borch K. Development of symptoms and complications
in individuals with asymptomatic gallstones. Br J Surg. 2004;91(6):734-738.
12. Friedman GD. Natural history of asymptomatic and symptomatic gallstones. The American
Journal of Surgery. 1993;165(4):399-404.
13. Urbach DR, Stukel TA. Rate of elective cholecystectomy and the incidence of severe
gallstone disease. CMAJ Canadian Medical Association Journal. 2005;172(8):1015-1019.
14. Russo MW, Wei JT, Thiny MT, et al. Digestive and liver diseases statistics, 2004.
Gastroenterology. 2004;126(5):1448-1453.
15. Kimura Y, Takada T, Strasberg S, et al. TG13 current terminology, etiology, and
epidemiology of acute cholangitis and cholecystitis. J Hepatobiliary Pancreat Sci. 2013;20(1):8-
23.
16. Elwood D. Cholecystitis. Surg Clin North Am. 2008;88(6):1241-52,viii.
17. Lammert F, Miquel JF. Gallstone disease: From genes to evidence-based therapy. J Hepatol.
2008;48 Suppl 1:S124-35.
151
18. Paumgartner G, Sauerbruch T. Gallstones: Pathogenesis. The Lancet. 1991;338(8775):1117-
1121.
19. Gomi H, Solomkin JS, Takada T, et al. TG13 antimicrobial therapy for acute cholangitis and
cholecystitis. J Hepatobiliary Pancreat Sci. 2013;20(1):60-70.
20. Yokoe M, Takada T, Strasberg S, et al. TG13 diagnostic criteria and severity grading of
acute cholecystitis (with videos). J Hepatobiliary Pancreat Sci. 2013;20(1):35-46.
21. Yokoe M, Takada T, Strasberg SM, et al. New diagnostic criteria and severity assessment of
acute cholecystitis in revised tokyo guidelines. J Hepatobiliary Pancreat Sci. 2012;19(5):578-
585.
22. Strasberg SM. Clinical practice. acute calculous cholecystitis. N Engl J Med.
2008;358(26):2804-2811.
23. McGillicuddy EA, Schuster KM, Barre K, et al. Non-operative management of acute
cholecystitis in the elderly. Br J Surg. 2012;99(9):1254-1261.
24. Lee HK, Han HS, Min SK, Lee JH. Sex-based analysis of the outcome of laparoscopic
cholecystectomy for acute cholecystitis. Br J Surg. 2005;92(4):463-466.
25. Elwood DR. Cholecystitis. Surg Clin North Am. 2008;88(6):1241-1252.
26. Fagan SP, Awad SS, Rahwan K, et al. Prognostic factors for the development of gangrenous
cholecystitis. The American Journal of Surgery. 2003;186(5):481-485.
152
27. Aydin C, Altaca G, Berber I, Tekin K, Kara M, Titiz I. Prognostic parameters for the
prediction of acute gangrenous cholecystitis. J Hepatobiliary Pancreat Surg. 2006;13(2):155-
159.
28. Sauerbruch T, Paumgartner G. Gallbladder stones: Management. The Lancet.
1991;338(8775):1121-1124.
29. Bateson MC. GALLSTONE DISEASE—PRESENT AND FUTURE. The Lancet.
1986;328(8518):1265-1267.
30. Nealon WH, Urrutia F, Fleming D, Thompson JC. The economic burden of gallstone
lithotripsy. will cost determine its fate? Ann Surg. 1991;213(6):645-9; discussion 649-50.
31. Strasberg SM. Cholelithiasis and acute cholecystitis. Baillieres Clin Gastroenterol.
1997;11(4):643-661.
32. Winbladh A, Gullstrand P, Svanvik J, Sandstrom P. Systematic review of cholecystostomy as
a treatment option in acute cholecystitis. HPB (Oxford). 2009;11(3):183-193.
33. Kortram K, van Ramshorst B, Bollen TL, et al. Acute cholecystitis in high risk surgical
patients: Percutaneous cholecystostomy versus laparoscopic cholecystectomy (CHOCOLATE
trial): Study protocol for a randomized controlled trial. Trials. 2012;13:7.
34. Keus F, Gooszen HG, van Laarhoven CJ. Open, small-incision, or laparoscopic
cholecystectomy for patients with symptomatic cholecystolithiasis. an overview of cochrane
hepato-biliary group reviews. Cochrane Database Syst Rev. 2010;(1):CD008318.
doi(1):CD008318.
153
35. Richards C, Edwards J, Culver D, Emori TG, Tolson J, Gaynes R. Does using a laparoscopic
approach to cholecystectomy decrease the risk of surgical site infection? Ann Surg.
2003;237(3):358-62.
36. The Southern Surgeons Club. A prospective analysis of 1518 laparoscopic
cholecystectomies. the southern surgeons club. New England Journal of Medicine, The.
1991;324(16):1073-8.
37. Ingraham AM, Cohen ME, Ko CY, Hall BL. A current profile and assessment of north
american cholecystectomy: Results from the american college of surgeons national surgical
quality improvement program. J Am Coll Surg. 2010;211(2):176-186.
38. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR, The Hospital Infection Control
Practices Advisory Committee. Guideline for prevention of surgical site infection. Infect Control
and Hosp Epidemiol. 1999;20:247-278.
39. Strasberg SM, Hertl M, Soper NJ. An analysis of the problem of biliary injury during
laparoscopic cholecystectomy. J Am Coll Surg. 1995;180(1):101-125.
40. Connor S, Garden OJ. Bile duct injury in the era of laparoscopic cholecystectomy. Br J Surg.
2006;93(2):158-168.
41. Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T. Intraoperative cholangiography and
risk of common bile duct injury during cholecystectomy. JAMA. 2003;289(13):1639-1644.
42. Tornqvist B, Stromberg C, Persson G, Nilsson M. Effect of intended intraoperative
cholangiography and early detection of bile duct injury on survival after cholecystectomy:
Population based cohort study. BMJ. 2012;345:e6457.

154
43. Berney CR. Major common bile duct injury and risk of litigation: A surgeon's perspective.
Am J Surg. 2012;204(5):800-802.
44. Barkun AN, Rezieg M, Mehta SN, et al. Postcholecystectomy biliary leaks in the
laparoscopic era: Risk factors, presentation, and management. Gastrointest Endosc.
1997;45(3):277-282.
45. Eisenstein S, Greenstein AJ, Kim U,Divino CM. Cystic duct stump leaks: After the learning
curve. Archives of Surgery. 2008;143(12):1178-1183.
46. Gurusamy KS, Samraj K. Early versus delayed laparoscopic cholecystectomy for acute
cholecystitis. Cochrane Database of Systematic Reviews. 2006(4):005440.
47. Giger U, Ouaissi M, Schmitz SF, Krahenbuhl S, Krahenbuhl L. Bile duct injury and use of
cholangiography during laparoscopic cholecystectomy. Br J Surg. 2011;98(3):391-396.
48. Enochsson L, Thulin A, Österberg J, Sandblom G,Persson G. The swedish registry of
gallstone surgery and endoscopic retrograde cholangiopancreatography (gallriks): A nationwide
registry for quality assurance of gallstone surgery. JAMA Surgery. 2013:1-8.
49. Yamashita Y, Takada T, Strasberg S, et al. TG13 surgical management of acute cholecystitis.
J Hepatobiliary Pancreat Sci. 2013;20(1):89-96.
50. Strasberg SM, Gouma DJ. 'Extreme' vasculobiliary injuries: Association with fundus-down
cholecystectomy in severely inflamed gallbladders. HPB. 2012;14(1):1-8.
51. Strasberg SM, Helton WS. An analytical review of vasculobiliary injury in laparoscopic and
open cholecystectomy. HPB (Oxford). 2011;13(1):1-14.
155
52. Banz V, Gsponer T, Candinas D, Guller U. Population-based analysis of 4113 patients with
acute cholecystitis: Defining the optimal time-point for laparoscopic cholecystectomy. Ann Surg.
2011;254(6):964-970.
53. Giger U, Michel J, Opitz I, Inderbitzin D, Kocher T, Krhenbhl L. Risk factors for
perioperative complications in patients undergoing laparoscopic cholecystectomy: Analysis of
22,953 consecutive cases from the swiss association of laparoscopic and thoracoscopic surgery
database. J Am Coll Surg. 2006;203(5):723-8.
54. Kum CK, Eypasch E, Lefering R, Paul A, Neugebauer E, Troidl H. Laparoscopic
cholecystectomy for acute cholecystitis: Is it really safe?. World J Surg. 1996;20(1):43-48.
55. Jacobs M, Verdeja JC, Goldstein HS. Laparoscopic cholecystectomy in acute cholecystitis. J
Laparoendosc Surg. 1991;1(3):175-7.
56. Flowers JL, Bailey RW, Scovill WA, Zucker KA. The baltimore experience with
laparoscopic management of acute cholecystitis. The American journal of surgery.
1991;161(3):388-92.
57. Kiviluoto T, Siren J, Luukkonen P, Kivilaakso E. Randomised trial of laparoscopic versus
open cholecystectomy for acute and gangrenous cholecystitis. Lancet. 1998;351(9099):321-325.
58. Giger UF. Michel JM. Opitz I. Th Inderbitzin D. Kocher T. Krahenbuhl L. Swiss Association
of Laparoscopic and Thoracoscopic Surgery (SALTS) Study Group. Risk factors for
perioperative complications in patients undergoing laparoscopic cholecystectomy: Analysis of
22,953 consecutive cases from the swiss association of laparoscopic and thoracoscopic surgery
database. J Am Coll Surg. 2006;203(5):723-728.

156
59. Papi C, Catarci M, D'Ambrosio L, et al. Timing of cholecystectomy for acute calculous
cholecystitis: A meta-analysis. Am J Gastroenterol. 2004;99(1):147-155.
60. Gurusamy K, Samraj K, Gluud C, Wilson E, Davidson BR. Meta-analysis of randomized
controlled trials on the safety and effectiveness of early versus delayed laparoscopic
cholecystectomy for acute cholecystitis. Br J Surg. 2010;97(2):141-50.
61. Jrvinen HJ, Hstbacka J. Early cholecystectomy for acute cholecystitis: A prospective
randomized study. Ann Surg. 1980;191(4):501-5.
62. Norrby S, Herlin P, Holmin T, Sjdahl R, Tagesson C. Early or delayed cholecystectomy in
acute cholecystitis? A clinical trial. Br J Surg. 1983;70(3):163-5.
63. Lo CM, Liu CL, Fan ST, Lai EC, Wong J. Prospective randomized study of early versus
delayed laparoscopic cholecystectomy for acute cholecystitis. Ann Surg. 1998;227(4):461-467.
64. Lai PB, Kwong KH, Leung KL, et al. Randomized trial of early versus delayed laparoscopic
cholecystectomy for acute cholecystitis. Br J Surg. 1998;85(6):764-767.
65. Johansson M, Thune A, Blomqvist A, Nelvin L, Lundell L. Management of acute
cholecystitis in the laparoscopic era: Results of a prospective, randomized clinical trial. Journal
of Gastrointestinal Surgery. 2003;7(5):642-645.
66. Kolla SB, Aggarwal S, Kumar A, et al. Early versus delayed laparoscopic cholecystectomy
for acute cholecystitis: A prospective randomized trial. Surg Endosc. 2004;18(9):1323-7.
67. Davila D, Manzanares C, Picho ML, Albors P, Cardenas F, Fuster E. <br />Experience in the
treatment (earlyvs. delayed) of acute cholecystitis via laparoscopy. Cirugıa Espanola.
1999;66(233).
157
68. Peng WK, Sheikh Z, Nixon SJ, Paterson-Brown S. Role of laparoscopic cholecystectomy in
the early management of acute gallbladder disease. Br J Surg. 2005;92(5):586-91.
69. Riall TS, Zhang D, Townsend CM,Jr, Kuo YF, Goodwin JS. Failure to perform
cholecystectomy for acute cholecystitis in elderly patients is associated with increased morbidity,
mortality, and cost. J Am Coll Surg. 2010;210(5):668-677.
70. Stevens KA, Chi A, Lucas LC, Porter JM, Williams MD. Immediate laparoscopic
cholecystectomy for acute cholecystitis: No need to wait. Am J Surg. 2006;192(6):756-761.
71. Gurusamy K, Samraj K, Gluud C, Wilson E, Davidson BR. Meta-analysis of randomized
controlled trials on the safety and effectiveness of early versus delayed laparoscopic
cholecystectomy for acute cholecystitis. Br J Surg. 2010;97(2):141-150.
72. Drummond MF, Drummond MF. Methods for the economic evaluation of health care
programmes. 3rd ed. Oxford ; New York: Oxford University Press; 2005:379.
73. Wilson E, Gurusamy K, Gluud C, Davidson BR. Cost-utility and value-of-information
analysis of early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Br J Surg.
2010;97(2):210-9.
74. Johner A, Raymakers A, Wiseman SM. Cost utility of early versus delayed laparoscopic
cholecystectomy for acute cholecystitis. Surg Endosc. 2013;27(1):256-262.
75. Macafee DAL, Humes DJ, Bouliotis G, Beckingham IJ, Whynes DK, Lobo DN. Prospective
randomized trial using cost-utility analysis of early versus delayed laparoscopic cholecystectomy
for acute gallbladder disease. Br J Surg. 2009;96(9):1031-40.
158
76. Society of American Gastrointestinal and Endoscopic Surgeons. SAGES guidelines for the
clinical application of laparoscopic biliary tract surgery. http://www.sages.org/publication/id/06/.
Updated 2010.
77. Yamashita Y, Takada T, Hirata K. A survey of the timing and approach to the surgical
management of patients with acute cholecystitis in japanese hospitals. J Hepatobiliary Pancreat
Surg. 2006;13(5):409-415.
78. Cameron IC, Chadwick C, Phillips J, Johnson AG. Management of acute cholecystitis in UK
hospitals: Time for a change. Postgrad Med J. 2004;80(943):292-4.
79. Askew J. A survey of the current surgical treatment of gallstones in queensland. ANZ J Surg.
2005;75(12):1086-9.
80. Sekimoto M, Imanaka Y, Hirose M, Ishizaki T, Murakami G, Fukata Y. Impact of treatment
policies on patient outcomes and resource utilization in acute cholecystitis in japanese hospitals.
BMC health services research. 2006;6:40-40.
81. Lee SW, Yang SS, Chang CS, Yeh HJ. Impact of the tokyo guidelines on the management of
patients with acute calculous cholecystitis. Journal of Gastroenterology & Hepatology.
2009;24(12):1857-1861.
82. Casillas RA, Yegiyants S, Collins JC. Early laparoscopic cholecystectomy is the preferred
management of acute cholecystitis. Arch Surg. 2008;143(6):533-537.
83. Greenstein AJ, Moskowitz A, Gelijns AC, Egorova NN. Payer status and treatment paradigm
for acute cholecystitis. Archives of Surgery. 2012;147(5):453-458.
159
84. Strasberg S. Clinical practice. acute calculous cholecystitis. New England Journal of
Medicine, The. 2008;358(26):2804-11.
85. Skouras C, Jarral O, Deshpande R, Zografos G, Habib N, Zacharakis E. Is early laparoscopic
cholecystectomy for acute cholecystitis preferable to delayed surgery?: Best evidence topic
(BET). International Journal Of Surgery. 2012;10(5):250-258.
86. Gananadha S, Fergusson J. Moderate acute cholecystitis: To cut now or to cut later. Journal
of Gastroenterology & Hepatology. 2009;24(12):1806-1807.
87. Statistics Canada. CANSIM table 051-0001 population by year, by province and territory.
http://www.statcan.gc.ca/tables-tableaux/sum-som/l01/cst01/demo02a-eng.htm. Updated 2013.
88. Greenstein AJ, Moskowitz A, Gelijns AC, Egorova NN. Payer status and treatment paradigm
for acute cholecystitis. Arch Surg. 2012.
89. David GG, Al-Sarira AA, Willmott S, Deakin M, Corless DJ, Slavin JP. Management of
acute gallbladder disease in england. Br J Surg. 2008;95(4):472-476.
90. Canadian Institute for Health Information. Quality assurance processes applied to the
discharge abstract and hospital morbidity databases. ottawa: Canadian institute for health
information. . 2007.
91. Austin PC, Daly PA, Tu JV. A multicenter study of the coding accuracy of hospital discharge
administrative data for patients admitted to cardiac care units in ontario. Am Heart J.
2002;144(2):290-296.

160
92. Gershon AS, Wang C, Guan J, Vasilevska-Ristovska J, Cicutto L, To T. Identifying
individuals with physcian diagnosed COPD in health administrative databases. COPD.
2009;6(5):388-394.
93. Tu K, Chen Z, Lipscombe LL, Canadian Hypertension Education Program Outcomes
Research Taskforce. Prevalence and incidence of hypertension from 1995 to 2005: A population-
based study. CMAJ. 2008;178(11):1429-1435.
94. Hux JE, Ivis F, Flintoft V, Bica A. Diabetes in ontario: Determination of prevalence and
incidence using a validated administrative data algorithm. Diabetes Care. 2002;25(3):512-516.
95. Antoniou T, Zagorski B, Loutfy MR, Strike C, Glazier RH. Validation of case-finding
algorithms derived from administrative data for identifying adults living with human
immunodeficiency virus infection. PLoS One. 2011;6(6):e21748.
96. Austin PC, Walraven C. The mortality risk score and the ADG score: Two points-based
scoring systems for the johns hopkins aggregated diagnosis groups to predict mortality in a
general adult population cohort in ontario, canada. Med Care. 2011;49(10):940-947.
97. Austin PC, van Walraven C, Wodchis WP, Newman A, Anderson GM. Using the johns
hopkins aggregated diagnosis groups (ADGs) to predict mortality in a general adult population
cohort in ontario, canada. Med Care. 2011;49(10):932-939.
98. Juurlink D, Preyra C, Croxford R, et al. Canadian institute for health information discharge
abstract database: A validation study. Toronto: Institute for Clinical Evaluative Sciences. 2006.
99. Jacobs P, Yim R. Using canadian administrative databases to derive economic data for health
technology assessments. Ottawa: Canadian agency for drugs and technologies in health. . 2009.
161
100. Wodchis WP, Bushmeneva K, Nikitovic,M., McKillop,I. Guidelines on person-level costing
using administrative databases in ontario. toronto: Health system performance research network.
. 2011.
101. Ontario Ministry of Health and Long Term Care. Schedule of benefits – physician services
under the health insurance act. . September 1, 2011.
102. Kleinbaum DG, Klein M, Pryor ER. Logistic regression. . 2010:701.
103. Austin PC, Goel V, van Walraven C. An introduction to multilevel regression models. Can
J Public Health. 2001;92(2):150-154.
104. Austin PC, Tu JV, Alter DA. Comparing hierarchical modeling with traditional logistic
regression analysis among patients hospitalized with acute myocardial infarction: Should we be
analyzing cardiovascular outcomes data differently? Am Heart J. 2003;145(1):27-35.
105. Kleinbaum DG, Klein M. Survival analysis. . 2005:590.
106. Southern DA, Faris PD, Brant R, et al. Kaplan-meier methods yielded misleading results in
competing risk scenarios. J Clin Epidemiol. 2006;59(10):1110-1114.
107. Satagopan JM, Ben-Porat L, Berwick M, Robson M, Kutler D, Auerbach AD. A note on
competing risks in survival data analysis. Br J Cancer. 2004;91(7):1229-1235.
108. Tai B, Machin D, White I, Gebski V. Competing risks analysis of patients with
osteosarcoma: A comparison of four different approaches. Statist Med. 2001;20(5):661-684.
109. ROSENBAUM PR, RUBIN DB. The central role of the propensity score in observational
studies for causal effects. Biometrika. 1983;70(1):41-55.
162
110. Austin PC. An introduction to propensity-score methods for reducing confounding in
observational studies. Multivariate Behav Res. 2011;46:399-424.
111. Austin PC. The performance of different propensity-score methods for estimating
differences in proportions (risk differences or absolute risk reductions) in observational studies.
Stat Med. 2010;29(20):2137-2148.
112. Caro J, Briggs A, Siebert U, Kuntz K. Modeling good research Practices—Overview: A
report of the ISPOR-SMDM modeling good research practices task Force–1. Medical Decision
Making. 2012;32(5):667-677.
113. Williams JG, Roberts SE, Ali MF, et al. Gastroenterology services in the UK. the burden of
disease, and the organisation and delivery of services for gastrointestinal and liver disorders: A
review of the evidence. Gut. 2007;56(Suppl 1):1-113.
114. Germanos S, Gourgiotis S, Kocher HM. Clinical update: Early surgery for acute
cholecystitis. The Lancet. 2007;369(9575):1774-1776.
115. Wilkins R. Use of postal codes and addresses in the analysis of health data. Health Rep.
1993;5(2):157-177.
116. Johns Hopkins University. Johns hopkins ACG case-mix adjustment system.
http://www.acg.jhsph.edu.
117. Ontario Ministry of Health and Long Term Care. Classification of hospitals.
http://www.health.gov.on.ca/english/public/contact/hosp/group_a.html. Updated 2009.
118. Spiegelhalter DJ. Funnel plots for comparing institutional performance. Stat Med.
2005;24(8):1185-1202.
163
119. Mittlbock M, Schemper M. Explained variation for logistic regression. Stat Med.
1996;15(19):1987-1997.
120. Mittlbock M, Heinzl H. A note on R2 measures for poisson and logistic regression models
when both models are applicable. J Clin Epidemiol. 2001;54(1):99-103.
121. Larsen K, Merlo J. Appropriate assessment of neighborhood effects on individual health:
Integrating random and fixed effects in multilevel logistic regression. Am J Epidemiol.
2005;161(1):81-88.
122. Campbell EJ, Montgomery DA, Mackay CJ. A national survey of current surgical treatment
of acute gallstone disease. Surg Laparosc Endosc Percutan Tech. 2008;18(3):242-247.
123. Hoyt DB. Looking forward. Bulletin of the American College of Surgeons. 2011;96:6.
124. Royal College of Surgeons of England. Separating emergency and elective surgical care:
Recommendations for practice. http://www.rcseng.ac.uk/. Updated 2007.
125. Lau B, Difronzo LA. An acute care surgery model improves timeliness of care and reduces
hospital stay for patients with acute cholecystitis. Am Surg. 2011;77(10):1318-1321.
126. Agrawal S, Battula N, Barraclough L, Durkin D, Cheruvu CV. Early laparoscopic
cholecystectomy service provision is feasible and safe in the current UK national health service.
Ann R Coll Surg Engl. 2009;91(8):660-664.
127. Simpson DJ, Wood AM, Paterson HM, Nixon SJ, Paterson-Brown S. Improved
management of acute gallstone disease after regional surgical subspecialization. World J Surg.
2008;32(12):2690-2694.
164
128. Lehane CW, Jootun RN, Bennett M, Wong S, Truskett P. Does an acute care surgical model
improve the management and outcome of acute cholecystitis? ANZ J Surg. 2010;80(6):438-442.
129. Britt RC, Bouchard C, Weireter LJ, Britt LD. Impact of acute care surgery on biliary
disease. J Am Coll Surg. 2010;210(5):595-9, 599-601.
130. Lo CM, Liu CL, Fan ST, Lai EC, Wong J. Prospective randomized study of early versus
delayed laparoscopic cholecystectomy for acute cholecystitis. Ann Surg. 1998;227(4):461-7.
131. Lai PB, Kwong KH, Leung KL, et al. Randomized trial of early versus delayed laparoscopic
cholecystectomy for acute cholecystitis. Br J Surg. 1998;85(6):764-7.
132. de Mestral C, Rotstein OD, Laupacis A, Hoch JS, Zagorski B, Nathens AB. A population-
based analysis of the clinical course of 10,304 patients with acute cholecystitis, discharged
without cholecystectomy. J Trauma Acute Care Surg. 2013;74(1):26-30; discussion 30-1.
133. Durrleman S, Simon R. Flexible regression models with cubic splines. Stat Med.
1989;8(5):551-561.
134. Austin PC. Optimal caliper widths for propensity-score matching when estimating
differences in means and differences in proportions in observational studies. Pharm Stat.
2011;10(2):150-161.
135. Flury BK, Riedwyl H. Standard distance in univariate and multivariate analysis. The
American Statistician. 1986;40(3):249-251.
136. Austin PC. Balance diagnostics for comparing the distribution of baseline covariates
between treatment groups in propensity-score matched samples. Stat Med. 2009;28(25):3083-
3107.
165
137. Agresti A, Min Y. Effects and non-effects of paired identical observations in comparing
proportions with binary matched-pairs data. Statist Med. 2004;23(1):65-75.
138. Lunceford JK, Davidian M. Stratification and weighting via the propensity score in
estimation of causal treatment effects: A comparative study. Statist Med. 2004;23(19):2937-
2960.
139. de Mestral C, Laupacis A, Rotstein OD, et al. Early cholecystectomy for acute cholecystitis:
A population-based analysis fo variation in practice. CMAJOpen. 2013;In press.
140. Lee SW, Yang SS, Chang CS, Yeh HJ. Impact of the tokyo guidelines on the management
of patients with acute calculous cholecystitis. J Gastroenterol Hepatol. 2009;24(12):1857-1861.
141. Ramsey SD, Berry K, Etzioni R, et al. Cost effectiveness of lung-volume-reduction surgery
for patients with severe emphysema. N Engl J Med. 2003;348(21):2092-2102.
142. Constantinides VA, Heriot A, Remzi F, et al. Operative strategies for diverticular
peritonitis: A decision analysis between primary resection and anastomosis versus hartmann's
procedures. Ann Surg. 2007;245(1):94-103.
143. Carradice D, Mekako AI, Mazari FA, Samuel N, Hatfield J, Chetter IC. Randomized
clinical trial of endovenous laser ablation compared with conventional surgery for great
saphenous varicose veins. Br J Surg. 2011;98(4):501-510.
144. Statistics Canada. CANSIM Table 326-0021 consumer price index.
http://www.statcan.gc.ca/start-debut-eng.html. Updated 2013.
166
145. Canadian Agency for Drug and Technologies in Health. Guidelines for the economic
evaluation of health technologies. ottawa: Canadian agency for drugs and technologies in health.
. 2006.
146. Center for the Evaluation of Value and Risk in Health, Tufts University. The cost-
effectiveness analysis registry. www.tufts-nemc.org/cearegistry.
147. Bass EB, Steinberg EP, Pitt HA, et al. Comparison of the rating scale and the standard
gamble in measuring patient preferences for outcomes of gallstone disease. Medical Decision
Making. 1994;14(4):307-314.
148. Briggs AH, Claxton K, Sculpher MJ. Decision modelling for health economic evaluation.
Oxford: Oxford University Press; 2006:237.
149. National Institute for Clinical Excellence. Guidance for manufacturers and sponsors.
national institute for clinical excellence. . 2001.
150. Weinstein MC, Siegel JE, Gold MR, Kamlet MS,Russell LB. REcommendations of the
panel on cost-effectiveness in health and medicine. JAMA. 1996;276(15):1253-1258.
151. World Health Organization. Choosing interventions that are cost effective.
http://www.who.int/choice/costs/CER_levels/en/index.html.
152. Statistics Canada. CANSIM table 384-0038 gross domestic product, expenditure-based .
http://www.statcan.gc.ca/start-debut-eng.html. Updated 2013.
153. Fenwick E, Claxton K, Sculpher M. Representing uncertainty: The role of cost-
effectiveness acceptability curves. Health Econ. 2001;10(8):779-787.

167
154. Gregor JC, Ponich TP, Detsky AS. Should ERCP be routine after an episode of ''idiopathic''
pancreatitis? A cost-utility analysis. Gastrointest Endosc. 1996;44(2):118-123.
155. Arseneau KO, Cohn SM, Cominelli F, Connors AF. Cost-utility of initial medical
management for crohn's disease perianal fistulae. Gastroenterology. 2001;120(7):1640-1656.
156. van Baal MC, Besselink MG, Bakker OJ, et al. Timing of cholecystectomy after mild
biliary pancreatitis: A systematic review. Ann Surg. 2012;255(5):860-866.
157. Falor AE, de Virgilio C, Stabile BE, et al. Early laparoscopic cholecystectomy for mild
gallstone pancreatitis: Time for a paradigm shift. Arch Surg. 2012;147(11):1031-1035.
158. Bouwense SA, Besselink MG, van Brunschot S, et al. Pancreatitis of biliary origin, optimal
timing of cholecystectomy (PONCHO trial): Study protocol for a randomized controlled trial.
Trials. 2012;13:225-6215-13-225.