Calculous Cholecystitis
193
Calculous Cholecystitis A Case Study Presented to the Faculty, Ateneo de Davao Universi ty College of Nursing Submitted to: Daphny Grace Peneza, R.N., R.M., M.N. Clinical Instructor – Panelist for the Case Study Submitted by: Gino Gregor Palaca Marvin Rey Andrew Pepino Rio Remonde Kevin Melvin Roa Krystle Rustia BSN-3H-4a May 25, 2010
Transcript of Calculous Cholecystitis

Calculous Cholecystitis
A Case StudyPresented to the Faculty,
Ateneo de Davao Universi tyCollege of Nursing
Submitted to:
Daphny Grace Peneza, R.N., R.M., M.N.Clinical Instructor – Panelist for the Case Study
Submitted by:Gino Gregor Palaca
Marvin Rey Andrew PepinoRio Remonde
Kevin Melvin RoaKrystle Rustia
BSN-3H-4a
May 25, 2010

TABLE OF CONTENTS
I. Introduction........................................................................................1
II. Objectives (General & Specific)........................................................3
III. Patient’s Data......................................................................................6
IV. Family Background and Health History..........................................7
V. Definition of Complete Diagnosis......................................................14
VI. Developmental Data............................................................................17
VII. Physical Assessment............................................................................26
VIII. Anatomy and Physiology....................................................................34
IX. Etiology and Symptomatology...........................................................37
X. Pathophysiology..................................................................................47
XI. Doctor’s Order....................................................................................50
XII. Diagnostic Exam.................................................................................62
XIII. Drug Study..........................................................................................72
XIV. Procedural Report..............................................................................87
XV. Nursing Theories.................................................................................94
XVI. Nursing Care Plan..............................................................................100
XVII. Discharge Plan (M. E. T. H. O. D.) & Prognosis..............................123
XVIII. Recommendation................................................................................130
XIX. References............................................................................................133

ACKNOWLEDGMENT
The Group 4-1 of section 3H, would like to acknowledge the contributions of the
following groups and individuals to the development of this case presentation.
To the Almighty God for blessing them with wisdom, competence and genuine
passion and giving them the strength to finish this presentation. The group dedicates to
Him the fruits of their hard-earned achievement.
To the staff of the Davao Medical School Foundation Hospital-3C for being
accommodating to the students and for giving them additional teachings during their
exposure in the said hospital. They have also been very willing to allow the students to
obtain records necessary for this presentation.
To their respected clinical instructor for this rotation, Daphny Grace Peneza,
R.N., R.M., M.N., for her support and guidance to the group. She has imparted
knowledge that would furthermore enhance the student’s understanding of their patient’s
case, thus making them ready to present this case presentation.
To their client, Meg, and her family, for being open and generous enough to
disclose personal information that would be helpful for this study. The group would also
like to thank them for their patience throughout the duration of the study and for giving
the group the opportunity to care for Selecta and apply what they have learned.
To the proponents’ respective family and friends for their prayers as well as their
financial support. They have also been a source of inspiration of the students.
To the members of this group for working hard and giving their efforts, time and
resources in conducting the study and for the completion of the written output.

INTRODUCTION
One of the body organs that we can live without is the gallbladder.
However, does this mean it is of no use to the body? The gallbladder is a pear-
shaped organ situated underneath the liver. Its function is to store bile and
release it as needed for digestion. Bile emulsifies the fats in food, breaking them
to small fragments so they can be further digested and absorbed in the small
intestine. If the gallbladder is not working as it should, the digestion of fats can be
seriously impaired.
One of the common gallbladder diseases is calculous cholecystitis.
Calculous cholecystitis is a condition wherein gallstones obstruct the gallbladder
outlet leading to poor drainage of bile. Trapped bile can irritate and inflame the
walls of the bladder, thus leading to inflammation. Calculous cholecystitis is the
cause of more than 90% of cases of acute cholecystitis (Feldman, Friedman &
Brandt, 2006). It affects women more often than men and is more likely to occur
at the age of 20-50 or over 60. Asians are also more prone to develop pigment
stones. Moreover, people who are obese and those who had had low fat diet are
at an increased risk for developing cholelithiasis. In the United States, it is
estimated that 6.3 million men and 14.2 million women aged 20 to74 had
gallbladder disease (Everhart, Khare, Hill, Maurer, 1999). In the Philippines, an
extrapolated prevalence of 5, 073, 040 people are affected by the disease
(http://digestive.niddk.nih.gov/statistics). Gallstones that do not cause symptoms
do not require treatment. However, if gallstones cause, disruptive, recurring
episodes of pain, surgical removal of the gallbladder is recommended.
Recently, the Group 3H-4a had a patient who was diagnosed with
symptomatic calculous cholecystitis and underwent laparoscopic
cholecystectomy. The group chose this case for they see it fit for their
perioperative concept. Rarely do they interact with patients who had minimally
invasive surgery. The proponents are hoping that through this case study, they
will be more knowledgeable and aware about such gallbladder disorder and the
surgical procedure done for the said disease. They are also interested to know
Page | 1

the proper and necessary nursing management that will be given to a patient
affected by the disease. Moreover, they would also like to impart their learning to
their families and their community regarding the prevention and care if ever such
condition will arise in the scenario.
As nursing students, they are hoping that this study will help them become
more efficient and better nurses in the future. The student nurses also hope to
apply their learning in taking care not only of their patients but of themselves as
well.
Page | 2

OBJECTIVES
General objective: Within 2 weeks exposure to various clinical areas, the group
should have been able to present a comprehensive case study which explains
the pathology, the treatment and the appropriate medical and nursing
management regarding the condition of their chosen client. The group also aims
to perform the necessary nursing interventions to help alleviate the patient’s
condition and improve her health.
Specific Objectives: The proponents also created certain aims that will help
them in achieving their general objectives. Within 2 weeks of exposure, the
proponents aim to:
Cognitive:
Gather pertinent data regarding the past and present health history of the
patient through interview and assessment;
Draw the family genogram of the patient;
Define the complete diagnosis of the patient by directly citing it from three
different sources;
Ascertain the patient’s developmental status using the theories of Robert
Havighurst, Erik Erikson and Lawrence Kohlberg;
Conduct a thorough cephalocaudal assessment obtained from the client;
Review the anatomy and physiology of the organs affected in the patient’s
disease;
Present the etiology and symptomatology of the disease;
Trace the pathophysiology of the patient’s disease;
Obtain the doctor’s orders and make rationales for each order;
Page | 3

Obtain, analyze and interpret laboratory and diagnostic procedures done
on the patient and include the normal and abnormal values and findings
for comparison, and the specific nursing responsibilities associated with
each diagnostic procedure;
Make drug studies on each drug given to the client, correlate them with
the disease process, explain why such drugs were ordered, and present
important interventions in administering the drug;
Identify three nursing theories that can be applied to the patient’s
condition;
Present specific, measurable, attainable, realistic, and time-bounded
nursing care plans for the patient;
Correlate the different nursing theories with the nursing care plans that are
presented in this case study;
Make a discharge plan for the patient with the use of M.E.T.H.O.D.;
Validate patient’s prognosis according to the following categories: onset of
illness, duration of illness, precipitating factors, willingness to take
medications and treatment, age, environmental factors and family support;
Broaden our scope of knowledge about the disease and the appropriate
Nursing Care for the patient with the disease;
Psychomotor:
Find a patient who will be the subject of their case presentation;
Render health teachings to the patient and her significant others to
promote health;
Provide care based on the various nursing care plans formulated by the
researchers and the patient herself;
Page | 4

Share information about calculous cholecystitis and the factors that cause
the development of such disease and its complications;
Share how the disease affects those affected by it and the systems
involved in its occurrence;
Affective:
Establish rapport with the patient and significant others;
Show genuine concern and willingness in serving the client;
Be aware of the client’s progress on the succeeding interactions;
Appropriately state the bibliography of all resources used in order to
prevent plagiarism and promote honesty.
Page | 5

PATIENT’S DATA
Client’s Code Name: Meg
Age: 38 years old
Gender: Female
Birth date: November 6, 1971
Address: Upper Sirib, Calinan Davao City
Nationality: Filipino
Religion (Denomination): Christian (Roman Catholic)
Civil Status: Married
Spouse: Bobong
Educational Attainment: 4th year high School
Occupation: House keeper
Height: 5ft 2inches
Weight: 62 kgs.
Health Insurance: Phil Care
Hospital: Davao Medical School Foundation (DMSF)
Vital Signs on Admission: BP: 130/80 mmHg PR: 79 bpm RR: 19 cpm
T: 37 ºC
Unit: 3C- 324-5
Chief Complaint: Pain at right upper quadrant
Admitting Physician: Dr. Walter Batucan
Admitting Diagnosis: Acute Cholelithiasis
Final diagnosis Calculous Cholecystitis
Surgical procedure Laparoscopic cholecystectomy
FAMILY BACKGROUND AND HEALTH HISTORY
Page | 6

A. Family Background
Meg is the second child among Mamang and Papang’s four
children. All children of Mamang were born through Normal Spontaneous
Vaginal Delivery without any complications. She delivered all her children
at their house with the help of “mananabang”. The family has been
residing in Sirib, Calinan Davao City since the marriage of Papang and
Mamang. Their home is near their farm.
The client, Meg has 3 siblings namely: Kenny (Male, deceased),
Luigi (Male, 30, married), and Dora (Female, 28, married). Meg graduated
high school and didn’t to proceed to college because she helped her
family tend their farm.
According to the patient, her father and mother are still alive and
they suffer from hypertension and diabetes. She said that the family
lineage of her mother also suffers from heart problems as well as kidney
problems. Two of her uncles on father’s side underwent surgery,
cholecystectomy, and had the same condition as Meg. Her older brother
died due to motorcycle accident. Luigi was diagnosed with hypertension
and Dora had a history of UTI. There was no one else in her immediate
family that suffered cholecystitis aside from Meg herself.
Meg got married to Bobong in the 1998. They were blessed with 3
children. Her 3 children were delivered through Normal Spontaneous
Vaginal Delivery, all were born in the Maternity clinic in Calinan. Her eldest
child is now studying in 4th grade. So far, none of her children suffer a
serious illness.
In terms of their expenses, Bobong is the one that provides money
for their daily expenses. Bobong is a Supervisor at DABCO and has a
wage of approximately 10,000 a month. Meg said that they budget the
money well for them to have food and to provide the necessary daily
needs and expenses. By helping tend to the 2 hectare farm of the patient’s
Page | 7

parents, they also get their share. They plant coconut trees, bananas, and
pineapples in their farm.
Lifestyle
The patient has sedentary lifestyle. When Meg stopped going to
school, she helped her mother with household chores. Right now, she is
busy taking care of Bobong and their 3 children. She is the one who
cooks, cleans the house, and does the laundry of the whole family.
Sometimes, she does gardening in their backyard. According to her, she
only works in the house, but still, she experiences fatigue from doing
household chores especially since she is the only one who does the
laundry.
She reported that she doesn’t smoke, but her husband does; he
smokes almost one pack a day. Meg said that she drinks liquor very
seldom; she only consumes a half of glass or a glass of liquor
occasionally.
The family has good relationship. At night, they watch television
together and this serves as their bonding time. Occasionally, they gather
together with her relatives when there are fiestas, birthday celebrations
and other special occasions.
She is not so active in terms of social organizations such as GKK
(Gagmay’ng Kristohanong Katilingban), but she sometimes joins in the
events in their community like the fiesta. She sometimes goes to church
on Sundays together with her children.
Meg sleeps around 9:00 o’clock at night and wakes up around 5:00
o’clock in the morning to prepare things needed of her husband. She is
the one who cooks the “baon” of her husband for work.
Page | 8

Meg said that she eats at least two times a day in small meals. She
said “naga-diet diet man ko kay tabaan nako sa akoang lawas, nagsugod
ko katong 36 years old pako, pero karong tuiga giundangan na nako ang
pagdiet-diet”. For breakfast she usually eats, “bulad”, “bagoong”,
“ginamos” and bread. Every morning, she always drinks coffee. In a day,
she can consume at least 3 cups of coffee. Her lunch and supper are
sometimes vegetables that are found in their backyard such as
“kamunggay”, “upo”, “okra”, “talong” and “tinangkong”. She is not fond of
eating pork and beef. She said that before, she limits herself from eating
fatty foods since she aimed to lose weight because she was afraid of
becoming obese. Also, she is so fond of drinking soft drinks. In a day she
can consume 4 glasses of coke. But she also drinks approximately 5-6
glasses of water. She also loves to eat salty foods, especially junk foods.
According to her, she has no allergy from any form of food.
B. Past Health History
Meg and her husband preferred to have artificial family planning than
natural family planning. She started using birth control pills since she was
36 years old.
She said that she is not sure if she completed her immunizations.
Her mother forgot already and the records were lost. They only avail of the
services of the health center very seldom. She said that their house was
far from the health center so they weren’t able to avail of all of the
services. She also experienced common illnesses such as cough, colds,
fever, measles and even chickenpox. They only treated it at home, since
her mother knows how to make use of different herbal medicines such as
kalabo, mayana, buyo, gabon, and tawa-tawa. Also, they sometimes
bought over-the-counter drugs such as paracetamol, Neozep, and
Medicol. With regards to how long she experienced those usual illnesses,
Page | 9

she said “dili man jud ko maabtan ug simana sa akoang kalintura ug bisan
ubo”.
She experienced measles when she was a 1-year old and had
chickenpox when she was 10-year old. Meg had her menarche when she
was 11 years old.
Meg reported that she got pregnant with her 1st child at the age of 28;
unfortunately, she had miscarriage on the 1st week of pregnancy. She
was hospitalized at Robillo Hospital, Calinan Davao City. Completion
curettage was performed to her. Again, on her 3rd pregnancy, she had a
miscarriage and was hospitalized on the maternity clinic and underwent
completion curettage. She reported that in almost all her pregnancies, she
experienced an increased blood pressure, usually 140/90. After delivering
her third child at the age of 36, Bobong and Meg decided to make use of
family planning. Meg started to take birth control pills until now to prevent
unexpected pregnancy.
C. History of Present Illness
On the second week of December 2009, Meg felt mild pain at the right
upper quadrant of her abdomen. She neglected it thinking that it’s nothing
serious and might be just an episode of indigestion. After three days, the
pain went away. But after two weeks, pain recurred at a higher scale
(5/10). Because of this, she was forced to seek medical advice. She went
to Isaac T. Robillo Memorial Hospital Calinan, Davao City and was asked
to have ultrasound of the whole abdomen. After 2 days, the result was
released and they found out that there were stones in her gallbladder. She
was advised by the doctor to undergo surgery, cholecystectomy. However,
the patient resisted the doctor’s advice due to fear of surgery. She was
given medications as an alternative (the patient already forgot the name of
medications prescribed). She was instructed by the doctor to increase
Page | 10

water intake and have a low fat diet, unfortunately, she wasn’t able to
follow the doctor’s order and still continued with her usual lifestyle.
Meg said that she still felt the pain after the check-up but she could still
tolerate it. She just took medications that were prescribed by the doctors
to alleviate the pain she felt.
Last May 5 this year, three days prior to admission, the patient again
experienced right upper quadrant pain which lasted until the present
condition. This was characterized to be progressive pain with a pain scale
of 8 out of 10. There was no radiation noted and no associated symptoms.
Two days prior to admission, pain recurred with a pain scale of 10 out of
10. This prompted Meg to seek consultation, hence, admission.
On May 8, 2010, the patient was admitted at Davao Medical School
Foundation at Surgical Ward, room 324 bed 5 under the service of Dr.
Batucan, with admitting diagnosis of Acute Cholelithiasis.
D. Effects/Expectations of Illness to Self/Family
Biological:
When Meg knew about her condition that she needs to undergo
surgery, she didn’t know what to do. She was very worried about herself
because she has fear of not waking up after surgery. She feared having
complications of not having a gall bladder anymore.
Psychosocial:
Page | 11

Also, she is worried about her 3 children, who still need care and
guidance from their mother. This made her decide not to go through with
the surgery before.
Meg wants to overcome her illness so that she can still spend time
with her family and friends. Furthermore, she said that she wants to be in
good condition as much as possible so that she can do her daily task in
everyday life for her family. The client is worried about her condition
because she has many plans in life together with her family.
Spiritual:
Still, Meg is still hopeful to overcome her challenges in life. The
client still has faith in the Creator, and she continues to pray to Him. She
believes that everything will be alright with the help of the creator.
Also, her children were worried about their mother, who’s suffering
from such condition. Her husband, Bobong is trying his best to support his
wife. Bobong was worried about Meg because for him, it makes him suffer
seeing his wife suffering. In addition, their relatives are also extending
their care and prayers for Meg because they are worried and concerned
for her.
The client is also very thankful because her family, relatives and
friends are still there giving support to her for her fast recovery. They are
always there and look after her in the hospital and to aid her physically,
mentally, emotionally, and spiritually.
Page | 12

Genogram
Maternal Side Paternal Side
Page | 13
Ana, , 70 Lala, K, 67
Lolo, K ,†
Jose, c, , D, 64
Mamita, †,
Lola, †, o
Papito, †
Papang, 62Po, c, 67Mamang, 60, DSis, , 64
Dora, 28, K
Kenny, a, †
- Female
-Male
#- age
- Heart problems
†-deceased
D- diabetic
K- Kidney problem
o- old age
c- cholelithiasis
a- accident
Meg, , c, 38
Bobong, 45,
Luigi, 30,
Bebe two, 7Bebe three, 2 Bebe one, 10

DEFINITION OF COMPLETE DIAGNOSIS
Complete Diagnosis: Calculous Cholecystitis
Calculous
Calculi, or gallstones, usually form in the gallbladder from the solid
constituents of bile; they vary greatly in size, shape and composition.
Source: Boyer, M. (2006). Brunner and Suddarth’s Textbook of Medical-
Surgical Nursing, 11th ed., p. 1347. Lippincott Williams & Wilkins.
Calculus (pl. calculi) is also called stone; an abnormal stone formed in
body tissues by accumulation of mineral salts. Calculi are usually found in
the biliary and urinary tracts.
Source: http://medical-dictionary.thefreedictionary.com/calculi. Retrieved
May 15, 2010.
Calculi (stones) can be divided into two groups—renal calculi and
gallstones. The majority of gallstones are composed principally of
cholesterol and other calcium salts.
Source: Iyengar, V. Elemental Analysis of Biological Systems: Biomedical,
Environmental, Compositional and Methodological Aspects of Trace
Elements, Vol. 1, p. 49.
Cholecystitis
Cholecystitis is the inflammation of the gallbladder. In more than 90% of
the cases, gallstones are present.
Page | 14

Source: White, L. Foundations of Nursing: Caring for the Whole Person, p.
832.
Inflammation of the gallbladder is called cholecystitis (chole = bile +cyst =
bladder + itis = inflammation)
Source: Crowley, L. (2010). An Introduction to Human Disease: Pathology
and Pathophysiology Correlations, 8th ed., p. 563. USA: Jones and Bartlett
Publishers.
Inflammation of the bladder which may be either acute or chronic. In an
acute cholecystitis, the blood flow to the gallbladder may become
compromised which in turn will cause problems with the filling and
emptying of the gallbladder. A stone may block the cystic duct which will
result in bile becoming trapped within the bladder due to inflammation
around the stone within the duct. Chronic cholecystitis occurs when there
have been recurrent episodes of blockage of cystic duct.
Source: Digiulio, M. & Jackson, D.(2007). Medical-Surgical Nursing
Demystified, p. 288. USA: McGraw-Hill.
Calculous Cholecystitis
Acute cholecystitis is inflammation of the gallbladder. There are two major
types of acute cholecystitis— calculous and acalculous. In calculous
cholecystitis, gallstones obstruct the gallbladder outlet leading to poor
drainage of bile. In physical exam, patients may exhibit Murphy’s sign—
right upper quadrant pain elicited by palpation under the right costal
margin when the patient inspires.
Page | 15

Source: Ginsber, G. & Ahmad, N. (2006) The Clinician’s Guide to
Pancreaticobiliary Disorders, p. 121-123. USA: SLACK Incorporated.
Page | 16

DEVELOPMENTAL DATA
According to Taylor, Lillis, LeMone and Lynn (2008), growth and development are orderly and sequential as well as
continuous and complex. All humans experience the same growth patterns and developmental levels, but, because these
patterns and levels are individualized, a wide variation in biologic and behavioral changes is considered normal. Within
each developmental level, certain milestones can be identified; for example, the time the infant rolls over, crawls, walks, or
says his or her first words. Although growth and development occur in individual ways for different people, certain
generalizations can be made about the nature of human development for everyone.
Robert Havighurst’s Developmental Task Theory
Robert Havighurst believed that living and growing are based on learning, and that a person must continuously learn to
adjust to changing societal conditions. He described learned behaviors as developmental tasks that occur at certain
periods in life. Successful achievement leads to happiness and success in late tasks, whereas unsuccessful achievement
leads to unhappiness, societal disapproval, and difficulty in later tasks. The developmental tasks arise from maturation,
personal motives, and values that determine occupational and family choices, and civic responsibility. (Taylor, et al. 2008)
Stage Description Result Justification
Middle
Age(30-40)
In the middle years, men and women reach
the peak of their influence upon society, and
at the same time the society makes its
Page | 17

maximum demands upon them for social and
civic responsibility. It is the period of life to
which they have looked forward during their
adolescence and early adulthood. And the
time passes so quickly during these full and
active middle years that most people arrive
at the end of middle age and the beginning of
later maturity with surprise and a sense of
having finished the journey while they were
still preparing to commence it.
Selecting a mate
Learning to live with a partner
Starting family
Rearing children
Achieved
The patient married and started a
family last 1998. She is happy with her
husband since she receives care and
unconditional love from him. She works
together with her husband in taking
care of and rearing their children by
providing their physiological,
psychological, and emotional needs.
Page | 18

Managing home
Getting started in occupation
Taking on civic responsibility
Achieved
Achieved
The patient has no job, however, she is
the one managing the house, by
cleaning, washing clothes, doing other
household chores and being a
peacemaker when trouble happens
among her children. She is the one
managing the house to have a
peaceful and organized home. Meg is
also responsible for budgeting their
money needed to sustain them in their
everyday living. She sees to it that her
husband’s salary is well budgeted and
not put into waste.
The patient is doing her responsibilities
as a Filipino citizen by following laws in
our country such as not throwing
garbage anywhere, and following traffic
rules. She is also a registered voter.
Patient verbalized that if she were not
Page | 19

admitted in the hospital, she would
really vote in the 2010 Presidential
elections. She also pays taxes
(property tax and cedula) as part of her
responsibility as a citizen.
Erik Erikson’s Psychosocial Development Theory
Erikson emphasized developmental change throughout the human life span. In Erikson’s theory, eight stages of
development unfold as we go through the life span. Each stage consists of a crisis that must be faced. According to
Erikson, this crisis is not a catastrophe but a turning point of increased vulnerability and enhanced potential. The more an
individual resolves the crises successfully, the healthier development will be. It is patterned to the Psychosexual
Development of Sigmund Freud but more concentrated on what task and conflict should a person be able to manage in a
certain age group. That is termed psychosocial development. He described eight stage of development:
1. Infancy
2. Early childhood
3. Late childhood
4. School age
5. Adolescence
6. Young adulthood
7. Adulthood
8. Maturity
Page | 20

Each stage signals a task that must be accomplished. The resolution of the task can be complete, partial, or
unsuccessful.
Stage Description Result Justification
Middle
Adulthood:
25-65 years
Ego
Development
Outcome:
Generativity
vs. Self
absorption or
Stagnation
Basic
Strengths:
The significant task is to perpetuate
culture and transmit values of the
culture through the family (taming the
kids) and working to establish a stable
environment. Strength comes through
care of others and production of
something that contributes to the
betterment of society, which Erikson
calls generativity, so when a person is
in this stage, she often fear inactivity
and meaninglessness.
As the children leave home, or the
person’s relationships or goals
changes, she may be faced with major
Working
towards
achieving
goal
As a wife and a mother of three children, she is
the one who inculcates values in the family
whom she acquired from her parents. She
makes sure that her children will be raised with
good attitude and as good Filipino Citizens.
As of now, her children are dependent and still
with them, she still doesn’t know what her
feelings will be when her children will leave
home someday. Today, she is busy taking care
of her children and her husband as those are the
responsibilities of a mother and wife.
Page | 21

Production
and Care
life changes—the mid-life crisis—and
struggle with finding new meanings
and purposes. If a person doesn't get
through this stage successfully, she
can becomes self-absorbed and
stagnate.
Significant relationships are within the
workplace, the community and the
family.
Creativity, productivity, concern for
others or self-indulgence, self-
concern, lack of interests and
commitments
Kozier and Erbs, Fundamentals of
Nursing, Chap. 20, page 352
http://www.learningplaceonline.com/
stages/organize/Erikson.htm
Page | 22

Lawrence Kohlberg’s Levels of Moral Development
Lawrence Kohlberg outlined the different planes of moral adequacy, based on his continued interest in how
children would react to varying moral dilemmas. Kohlberg stated that ethical behavior was based on moral reasoning,
which in turn could be broken down into six specific developmental stages. The stages are progressive, in that it is highly
improbable for someone to regress backwards. Once a person acquires the functionalities of higher stages of moral
development, it will be difficult for him to lose these abilities and revert to lower levels of growth. Every stage follows
another, making it difficult for a person to jump forward and virtually skip an entire stage.
The levels and stages are as follows:
Level 1: Preconventional
Stage1: Punishment/obedience
Stage2: Instrumental/relativist
Level 2: Conventional
Stage3: Approval Seeking
Stage4: Law and order
Level 3: Postconventional
Stage5: Social Contract
Stage6: Universal-ethical
Page | 23

Stage Description Result Justification
Post-
conventional
Level
Stage 5:
Social
Contract
Stage6:
Universal-
ethical
At stage 5 social contract and
utilitarian orientation, correct
behavior is defined in terms of
society’s law. Laws can be
changed, however, to meet
society’s needs, while
maintaining respect for self and
others.
Stage 6, universal ethical
principle orientation, represents
the person’s concern for
equality for all human beings,
guided by personal values and
standards regardless of those
Achieved
Working
towards
achieving
goal
She sees that most of the laws are correct and worth to
be followed. She said that she follows the rules of the
country and the city she lives in. She doesn’t want
nuisance in the society because she believes that to be
able to live in a serene place, people must maintain and
establish respect with themselves and then to others.
She knows about universal laws, specifically about
justice. She is concerning about justice, “malooy gyud ko
sa mga tao nga dili matagaan ug hustisya, labaw na ng
mga kabus” , as verbalized by the patient.
Page | 24

set by society or laws. Justice
might be internalized at an
even higher level than society.
Few adults ever reach this
stage of development.
(Taylor et. al, 2008)
Page | 25

PHYSICAL ASSESSMENT
Patient’s Name: Meg
Age: 38 yrs. old
Sex: Female
Admitting Diagnosis: Acute Cholelithiasis
Final Diagnosis: Calculous Cholecystitis
Chief Complaint: right upper quadrant pain
Date of Assessment: May 12, 2010
Time of Assessment: 4:00 pm
Location of Assessment: DMSF Hospital, 3C, Room 324-5
Vital Signs upon physical assessment:
I. General Survey
The patient was received lying on bed, awake, conscious, coherent,
afebrile and without IVF. She has three 0.5-cm long incisions at her epigastric
and right lower rib cage areas and a 1-cm incision under her umbilicus. Incision
site is dry and intact. Each incision is covered with dry and intact dressing.
Patient complains of pain on the incision site and rated this pain as 6 out of 10 in
the pain scale. She is oriented to time (verbalized it was late in the afternoon),
person (identified watcher correctly), place (verbalized she’s in the hospital) and
Page | 26
Temperature : 36.6 °C
Pulse Rate: 82 bpm
Respiratory Rate: 18 cpm
Blood Pressure: 130/80 mmHg

reason for admission (stated that she was admitted due to right upper quadrant
abdominal pain). Patient is not in respiratory distress.
Patient appears appropriate for her stated age. She stands 5 feet and 2
inches tall and weighs 62 kg. Her body mass index (BMI) is 24.9 which is normal.
She has an endomorphic body type. Patient is in fair grooming as evidenced by
unsoiled t-shirt she is wearing, well-kept hair and clean linens and pillows.
However, it was noted that patient has halitosis. Nails were long but clean.
Through the course of the physical assessment, it was observed that the
patient is cooperative and has an accommodating attitude towards the student.
The patient is calm. Patient’s speech was audible, comprehensible and in
moderate pace.
II. Skin
Skin is fair in color, intact and with hairs, except in the palms, soles and
dorsa of the distal phalanges. Skin is dry and slightly warm upon palpation. It
returns quickly to its normal state when picked up between two fingers and
released. Skin texture is soft and fine while extensor surfaces such as the elbows
have coarser skin. The palms and the soles are calloused. No skin breaks
present aside from the incision sites on her abdomen. No edema present.
III. Hairs and Nails
Upon inspection, hair was noted to be black. It is thick, oily, straight, long
and well-kept. Hair is also evenly distributed as evidenced by absence of bald
spots. Dandruff or flaking was not present. Other infestations, such as lice, were
not noted. The color of scalp is lighter than the color of skin.
Nails on both hands and feet are long but clean. Nail polish was removed.
Client has a capillary refill time of 2 seconds. No clubbing of the nailbeds noted.
Page | 27

IV. Head
Patient’s head is round and normocephalic in configuration with smooth
skull contour. There were no palpated masses, nodules, deformities or fractures.
Facial features are symmetric as evidenced by palpebral fissures being equal in
size and symmetric nasolabial folds. Facial movements are symmetrical and
patient is able to perform different kinds of expression effortlessly and without
any obstructions. Patient can move her head up and down and side to side. No
lesions noted on the face.
V. Eyes
Hairs of eyebrows are thick and evenly distributed. Eyebrows are
symmetrically aligned and there’s equal movement as evidenced by the patient’s
ability to elevate and lower the eyebrows. No edema, lesions, puffiness or
tenderness noted upon inspection and palpation of the periorbital area.
Eyelashes are equally distributed and curled slightly outward with no ectropion or
entropion. Eyelids’ surface is intact with no discharges and no discoloration but
with noted eye bags on the lower surface. No lid lag noted. Blink reflex is
present. Palpebral fissure is equal in both eyes. Bulbar conjunctiva is pale pink.
Cornea is transparent and without cloudiness. Sclera is anicteric. Eyeballs are
symmetrical with no bulging observed. Pupils were black in color, equally round,
3mm in size and reactive to light and accommodation. Pupils quickly constrict
when a penlight is shone towards the pupil from a lateral position. Iris is dark
brown in color.
Client has central and peripheral vision. She can see things on the side
of her eye, like the adjacent bed, even when looking straight ahead. Moreover,
pupils constrict when looking at near objects and dilate when looking at far
objects. During ocular motility testing, patient was asked to follow the examiner’s
Page | 28

finger in the six cardinal fields of gaze. There was smooth, parallel movement of
eyes in all direction. Both eyes move in unison. No nystagmus noted. To test her
visual acuity, the students asked her to read their nameplates placed about 1 ½
feet away from her. She was able to correctly read the names without any
difficulty. Patient verbalized she doesn’t use any corrective aids. She also did not
report any vision difficulty or eye pain.
VI. Ears
The color of the patient’s ears is the same as her facial skin. The skin
behind the ear in the crevice is smooth and without breaks. The left and right
pinna are symmetrical and aligned with the inner canthus of the eye. Pinna
recoils after it is folded. Auricle is nontender upon palpation. Mastoid process is
smooth and hard and no tenderness or swelling noted. External canals have
minimal cerumen. No sanguinous discharges noted on the meatus. Patient was
able to hear a soft whisper equally in both ears. She can also hear normal voice
tones as evidenced by prompt responses to questions asked.
VII. Nose
It was noted that the nostrils were symmetrical and the nasal septum is
midline. There were no observed discharges draining from the client’s nose. Hair
is noted on the nares. Nares are patent since patient is able to breathe normally
on both nostrils without difficulty when one nose is closed with digital
compression and patient inhaled with mouth closed. No lesions on the external
nose structure were seen. There was no tenderness over the maxillary and
frontal sinuses upon palpation of the cheeks and supraorbital ridges. Client’s
gross smell was functional as she could identify the scent of alcohol.
Page | 29

VIII. Mouth
Mouth is proportional and symmetrical. Lips are cracked, dry, pink in
color and with no masses or congenital defect. Buccal mucosa was uniform pale
pink in color and moist. The patient’s gum was, moist, firm and pinkish in color.
No gum retraction or bleeding was noted. Teeth are of complete set. There are
no spaces in between teeth. Dental carries are evident in lower right and left
molar. Teeth are yellow in color. Patient has no dentures. Tongue is pink, moist,
slightly rough and has thin whitish color on the surface. It is also in central
position and moves freely. The base of tongue is smooth with prominent veins.
No tenderness, lesions or any unusualness noted. Soft palate is light pink in
color. On the other hand, hard palate is much lighter and more irregular in
texture. Uvula is positioned in midline of soft palate and rises when the patient
says “ah”. Tonsils are not inflamed. No ulcerations and exudates present. Patient
has no difficulty of masticating and swallowing. Halitosis was noted. Patient has
no speech disorders.
IX. Neck
Neck is symmetrical with no masses or unusual swelling upon
palpation. No jugular vein distention noted. Pulsation at carotid arteries is strong
and regular in rhythm. Range of motion is normal and no pain elicited upon
flexion, extension, and rotation of head. Thyroid is not enlarged upon palpation
with no nodules, masses or irregularities upon palpation. Thyroid also rises when
patient was asked to swallow. Trachea is symmetrical and in midline without
deviation. No lymph adenopathies appreciated. No torticollis present.
Page | 30

X. Breast
Breast is conical, symmetrical and skin color is lighter than exposed areas.
No lesions, redness, or edema and texture is even. No dimpling or retraction.
Nipples are in midline and everted pointing in the same direction. Areola and
nipples are dark brown in color and has no discharges, crusting and masses.
XI. Chest/Lungs
Chest skin integrity is good and intact. Patient has symmetrical chest wall
movement. Point of maximal impulse is at 5th intercostal space left midclavicular
line. Apical pulse is 84bpm. Patient has distinct heart sounds, with S1 louder than
S2; negative for murmurs. There were no noted deformities in the client’s
thoracic area. There are no bulges or retraction of the intercostal spaces.
Client’s respiratory rate is 18 cycles per minute. Patient did not complain of
chest pain or chest tightness. Guarding of the chest noted upon respiration due
to the proximity of the incision site to the diaphragm. Patient is not in respiratory
distress. Coughing episodes were also not observed. Vesicular breath sounds
are soft and low pitched. Her breathing is deep, regular and slow with a long
inspiratory phase and a short expiratory phase. With no adventitious sounds,
lungs are clear to auscultation and no crackles, wheezes or rubs. It was
observed that vocal fremitus is present both at the back and front of the chest
when the patient says “ninety-nine”.
XII. Abdomen
Abdomen is round. Color of skin in abdomen is slightly lighter than the
rest of the body. A 0.5-cm incision was noted at the subxyphoid area. Another
two 0.5-cm incisions are seen at her right lower rib cage. A 1-cm incision is also
present just below her umbilicus. All four incisions are covered with dry and intact
dressing. Patient complains of pain on the surgical site and verbalized,
Page | 31

“Nagangulngol tong gioperhan. Pwede makahingi ug tambal para sa sakit?”
Patient reported a pain scale of 6 out of 10. Aortic pulsations are not visible.
Umbilicus is midline and inverted. Symmetrical movement of abdomen upon
respiration was noted. Upon auscultation of the abdomen, it was noted that
patient has normal bowel sounds—high-pitched and occurred 16 times per
minute. Abdomen is soft and there is no point tenderness. Patient was on DAT
as ordered.
XIII. Back and Extremities
Peripheral pulse of the patient was symmetrical and regular in rhythm;
radial pulse is 82bpm. Patient has normal capillary refill of 2 seconds. The nails
were pinkish in color without cyanosis and clubbing. Patient is able to ambulate
freely. She was able to sit up on bed and perform range of motion on both upper
and lower extremities. However, it was noted that patient has guarded and slow
movement for she feels pain on her abdomen. Client’s grasping ability was
moderately strong on both hands. No edema or cyanosis was noted on both
upper and lower extremities. There is no swelling, tenderness or nodules
palpated on each joint. The shoulders, arms, elbows and forearms are free of
nodules, swelling, deformities and atrophy.
The skin at the back of the patient is uniform in color. Symmetrical
chest expansion with respirations noted. No spinal tenderness noted. There are
no skin breaks present. The back is also symmetrical with the spinal cord
aligning from the neck down to the buttocks. There were no deformities or
abnormalities on the bone such as scoliosis, osteoporosis and alike to be noted.
XIV. Genito-urinary
Pubic hair is present, thick in each strand, curly and equally distributed
on the mons pubis. No vaginal bleeding or any other unusual discharges noted.
Page | 32

Patient voids freely. She has no difficulty urinating and did not report dysuria.
She verbalized her urine is amber in color.
XV. Neurological
Patient was received lying on bed, awake, conscious, coherent and
afebrile. Reflexes are normal and symmetrical bilaterally in both extremities.
Patient is oriented to person, place and time. She has a Glasgow coma scale of
15: 4 from eye opening, 5 for verbal resoponse and 6 for motor response. She is
also alert and attentive.
Page | 33

ANATOMY AND PHYSIOLOGY
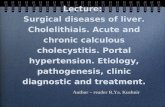
GALLBLADDER
The gallbladder is a hollow organ that sits just beneath the liver. In adults,
the gallbladder measures approximately
8 cm in length and 4 cm in diameter when
fully distended. It is divided into three
sections: fundus, body, and neck. The neck
tapers and connects to the biliary tree via
the cystic duct, which then joins the common
hepatic duct to become the common bile
duct. Its function is to store and release bile,
a fluid made by the liver.
Page | 34

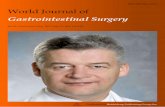
CYSTIC DUCT
The cystic duct is the
short duct that joins the gall bladder to
the common bile duct. The cystic duct
varies from 2 to 3 cm in length and
terminates in the gallbladder.
Throughout its length, the cystic duct is
lined by a spiral mucosal elevation,
called the valvula spiralis (valve of
Heister) which is
a series of crescentic folds of mucous
membrane in the upper part of the cystic duct, arranged in a
somewhat spiral manner. Its length is variable and usually ranges from 2 to 4 cm.
The cystic duct is usually 2-3 mm wide. It can dilate in the presence of pathology
(stones or passed stones).
The duct and spiral folds contain muscle fibers responsive to
pharmacologic, hormonal, and neural stimuli. There is, however, no convincing
evidence of a discrete muscular sphincter within the duct. Although the cystic
duct is unlikely to play a major role in gallbladder filling and emptying, it appears
to function as more than a passive conduit. Coordinated, graded muscular
activity in the cystic duct in response to hormonal and neural stimuli may facilitate
gallbladder emptying. The principal function of the internal spiral folds that are
found in man may be to preserve patency of this narrow, tortuous tube rather
than to regulate bile flow.
BILE
The main components of bile include contains water, cholesterol, fats, bile
salts, proteins, and bilirubin.
Page | 35

Bile, is produced by hepatocytes in the liver and and then flows into
the common hepatic duct, which joins with the cystic duct from the gallbladder to
form the common bile duct. The common bile duct in turn joins with the
pancreatic duct to empty into the duodenum. If the sphincter of Oddi, a muscular
valve that controls the flow of digestive juices (bile and pancreatic juice) through
the ampulla of Vater into the second part of the duodenum, is closed, bile is
prevented from draining into the intestine and instead flows into the gallbladder,
where it is stored and concentrated to up to five times its original potency
between meals. This concentration occurs through the absorption of water and
small electrolytes, while retaining all the original organic molecules.
When food is released by the stomach into the duodenum in the form of
chyme, the duodenum releases cholecystokinin, which causes the gallbladder to
release the concentrated bile to complete digestion.
Bile helps to emulsify the fats in the food. Besides its digestive function,
bile serves also as the route of excretion for bilirubin, a byproduct of red blood
cells recycled by the liver.
The alkaline bile also has the function of neutralizing any excess stomach
acid before it enters the ileum, the final section of the small intestine. Bile salts
also act as bactericides, destroying many of the microbes that may be present in
the food.
In the absence of bile, fats become indigestible and are instead excreted
in feces, a condition called steatorrhea.
Page | 36

ETIOLOGY AND SYMPTOMATOLOGY
Etiology
Predisposing Factors
Present/ Absent
Rationale Justification
Female PRESENT Women between 20 and 60 years of
age are twice as likely to develop
gallstones as men.
Estrogen increases cholesterol
levels in bile and decrease
gallbladder movement, both of
which can lead to gallstones.
Sources:
Harrison’s Principles of Internal Medicine,
Tenth Edition 1983 page 1822
Lippincott Williams and Wilkins Handbook
of Diseases Third Edition, page 184
http://www.diabetesmonitor.com/learning-
center/gallstones.htm
The patient
is female.
Diabetes
mellitus
ABSENT People with diabetes generally have
high levels of fatty acids called
triglycerides. These fatty acids
increase the risk of gallstones.
Sources:
Harrison’s Principles of Internal Medicine,
Tenth Edition 1983 page 1823
The patient
is not
diabetic.
Page | 37

Lippincott Williams and Wilkins Handbook
of Diseases Third Edition, page 184
Age
(20-50; over
age 60)
PRESENT Many of the body’s systems and
protective mechanisms become less
efficient with age. Body systems and
processes become sluggish.
Sources:
Harrison’s Principles of Internal Medicine,
Tenth Edition 1983 page 1823
Lippincott Williams and Wilkins Handbook
of Diseases Third Edition, page 184
The patient
is 38 years
old.
Ethnicity
(Native
American,
Mexican
American)
(Asian)
PRESENT Native Americans have a genetic
predisposition to secrete high levels
of cholesterol in bile. In fact, they
have the highest rate of gallstones
in the United States. A majority of
Native American men have
gallstones by age 60. Mexican
American men and women of all
ages also have high rates of
gallstones.
Asians are more genetically
predisposed to having pigment
stones as compared to those living
in the Western countries
The patient
is Filipino.
She is
predisposed
to having
pigment
stones.
Page | 38

Sources:
Lippincott Williams and Wilkins Handbook
of Diseases Third Edition, page 184
http://www.diabetesmonitor.com/learning-
center/gallstones.htm
Precipitating Factors
Present/ Absent
Rationale Justification
PregnancyABSENT Excess estrogen from pregnancy,
hormone replacement therapy, or birth control pills appears to
increase cholesterol levels in bile and decrease gallbladder
movement, both of which can lead to gallstones.
Source: http://www.fbhc.org/Patients/Modul
es/gallstns.cfm
The patient is not pregnant.
Rapid weight loss ABSENT As the body metabolizes fat during
rapid weight loss, it causes the liver to secrete extra cholesterol into
bile, which can cause gallstones.
Sources:
Lippincott Williams and Wilkins Handbook of Diseases Third
Edition, page 184
http://www.fbhc.org/Patients/Modules/gallstns.cfm
No rapid weight loss
was noted by the patient.
Page | 39

Obesity ABSENT The most likely reason is that obesity tends to reduce the amount of bile salts in bile, resulting in more cholesterol. Obesity also decreases
gallbladder emptying.
Sources:
Harrison’s Principles of Internal Medicine, Tenth Edition 1983 page
1823
Lippincott Williams and Wilkins Handbook of Diseases Third
Edition, page 184
http://www.fbhc.org/Patients/Modules/gallstns.cfm
The patient is not obese.
Fasting ABSENT Fasting decreases gallbladder movement, causing the bile to become overconcentrated with cholesterol, which can lead to
gallstones.
Source:
http://www.diabetesmonitor.com/learning-center/gallstones.htm
The patient doesn’t fast.
Hormone replacement therapy, or
birth control pills
PRESENT Excess estrogen from pregnancy, hormone replacement therapy, or
birth control pills appears to increase cholesterol levels in bile
and decrease gallbladder movement, both of which can lead
to gallstones.
Source:
Lippincott Williams and Wilkins
The patient has been on birth control pills since
she was 36 years old.
Page | 40

Handbook of Diseases Third Edition, page 184
http://www.diabetesmonitor.com/learning-center/gallstones.htm
Low Fat Diet PRESENT Before dietary fat can be digested, it has to be emulsified. Bile is used for this purpose. The liver makes
bile continuously and stores it in the gall bladder until such time as it is
needed. However, if a low-fat diet is eaten, that bile remains in the gall
bladder.
Gallstones are formed when the gall bladder is not emptied on a
regular basis. In people who continually resort to low-fat diets,
bile is stored for long periods in the gall bladder — and it stagnates. In time — and it is really quite a short time — a 'sludge' begins to form.
Source:
http://www.second-opinions.co.uk/gallstones.html
The patient avoids fatty
foods.
Symptomatology
Signs and Present/ Rationale Justification
Page | 41

Symptoms Absent
Right upper
quadrant pain
(may radiate
to right
scapula,
shoulder, or
interscapular
area)
“biliary colic”
PRESENT Obstruction of ducts
connected to the gallbladder
will cause inflammation
produced by increased
intraluminal pressure and
distension of the
gallbladder.
Sources:
Harrison’s Principles of
Internal Medicine, Tenth
Edition 1983 page 1825
The patient
came into
DMSF
complaining
of RUQ pain.
Fever (low
grade)
ABSENT Fever is a nonspecific
response that is mediated
by endogenous pyrogens
released from host cells in
response to infectious or
non-infections disorders. It
may be brought about by
prostaglandins released
during inflammation.
Source: Carol Mattson
Porth (2005.
Pathophysiology, Seventh
The patient
was not
febrile.
Page | 42

edition page 205)
Murphy's sign
(abrupt
interruption of
deep
inspiration)
PRESENT Classically Murphy's sign is
tested for during
an abdominal examination;
it is performed by asking the
patient to breathe out and
then gently placing the hand
below the costal margin on
the right side at the mid-
clavicular line (the
approximate location of
the gallbladder). The patient
is then instructed to inspire
(breathe in). Normally,
during inspiration,
the abdominal contents are
pushed downward as
the diaphragm moves down
(and lungs expand). If the
patient stops breathing in
(as the gallbladder
is tender and, in moving
downward, comes in
contact with the examiner's
fingers) and winces with a
'catch' in breath, the test is
considered positive. A
positive test also requires
no pain on performing the
The patient
was positive
for the
Murphy’s
Sign.
Page | 43

maneuver on the patient's
left hand side.
Source:
http://www.turner-
white.com/pdf/
hp_nov00_murphy.pdf
Nausea and
vomiting
ABSENT Nausea and vomiting
sometimes occur with biliary
colic. The inflammation of
the gallbladder causes pain
and spasms of the
abdominal muscles which
may make one feel
nauseated.
Source:
Understanding Medical
Surgical Nursing by
Williams and Hopper page
742
The patient
didn’t
complain of
nausea or
vomiting.
Mildly
elevated
serum
bilirubin
ABSENT Biliary obstruction causes
suppression of bile flow,
and regurgitation of
conjugated bilirubin into the
The patient’s
bilirubin was
not increased.
Page | 44

bloodstream.
Sources:
Harrison’s Principles of
Internal Medicine, Tenth
Edition 1983 page 1829
Elevated
SGPT and
SGOT
enzymes
PRESENT SGOT (AST) and (ALT) is
an enzyme found mostly in
the liver but also in the
heart, the muscles, the
kidneys, the pancreas and
in red blood cells. High
elevations may be
associated with liver
disease or muscle trauma.
Elevations may also be
associated with a variety of
conditions including
myocardial infarction (heart
attack), pancreatitis, bile
duct obstruction and more.
Abnormalities of liver
enzymes including
AST/SGOT and ALT/SGPT
are indicative of problems
such as Mirrizi syndrome, or
The patient’s
lab tests
reveal an
elevated level
of SGPT and
SGOT
enzymes.
Page | 45

a stone in the bile duct
causing infection/liver
inflammation.
Sources
http://
my.diabetovalens.com/
apollo/sgot.asp
Page | 46

Page | 47
PATHOPHYSIOLOGY
Predisposing Factors:
Female Age 38 Ethnicity Diabetes Mellitus
Precipitating Factors:
Birth control pills Low Fat Diet Pregnancy Rapid weight loss Obesity fasting
Bile stagnates in the gallbladder
Pigment solute precipitate as solid crystals
Crystals clump together and form stones
Gallstones
Upon contraction, a stone is moved and becomes impacted on the cystic duct
Bile stasis
Gallbladder contracts after intake of fat to release bile
CHOLELITHIASIS
Lumen is obstructed by stones

Page | 48
If treated with:
If not treated
Good prognosis
Chemical reaction inside gallbladder triggers the release of inflammatory
enzymes
(Prostaglandins)
ACUTE CHOLECYSTITIS
Increased intraluminal pressure and distention
of the gallbladder
Inflammation of the gallbladder
Biliary Colic
(RUQ pain)
Murphy’s Sign
Fluids leak into gallbladder
Edema
Constriction of blood vessels
Continued increase in intraluminal pressure of gallbladder
Rupture of gallbladder
Spread of bile and indigenous microorganisms into peritoneal cavity
Continued lack of blood supply to gallbladder
Necrosis
Gangrene and empyema
Perforation of gallbladder
Surgery, proper diet (low fat, high fiber), compliance
to medications

Page | 49
Sepsis
Death

DOCTOR’S ORDER
Date Order Rationale Remarks
5/8/10
@ 11pm
Admit under the care
of Dr. Batucan
Admitted under the care of
Dr. Batucan, a surgeon, for
his specialties on surgical
procedures (Laparoscopic
cholecystectomy)
Done.
Patient was
placed in
ward 324
bed 5
Secure consent to
care
Consent is an agreement
between client and health
care provider to give proper
quality care. It is also to
protect the client from harmful
procedures and the institution
from law suits
Done
Low fat diet Doctors were not sure
whether the gallstones are
either cholesterol or pigment
stones. Thus, this is done to
prevent any further damage
to the gallbladder.
Done
Monitor VSqShift and
record
Monitoring vital signs is
important in order to note any
unusualities and to refer
these as follows.
Done
Labs:
CBC A complete blood count
(CBC) is a series of tests
used to evaluate the
composition and
concentration of the cellular
Done
Page | 50

Platelet
Urinalysis
components of blood. It
consists of the following tests:
red blood cell (RBC) count,
white blood cell (WBC) count,
and platelet count;
measurement of hemoglobin
and mean red cell volume;
classification of white blood
cells (WBC differential); and
calculation of hematocrit and
red blood cell
Platelet count is to determine
the number of platelets; If the
number of platelets is too low,
excessive bleeding can occur.
However, if the number of
platelets is too high, blood
clots can form (thrombosis),
which may obstruct blood
vessels.
It is done to detect urinary
tract infection. It also
measures the level of
ketones, sugar, protein, blood
components and many other
substances
Done
Done
Venoclysis: PNSS 1L
@ 100cc/hr
PNSS is an isotonic solution
to provide hydration since it
was found out that the
Done. IVF
infusing well
at right
Page | 51

specific gravity for urine is in
the borderline (1.010). It is
also to provide electrolytes,
and as a medium for IVTT
meds
metacarpal
vein.
Meds:
Demerol 50mg IVTT
now then prn for
abdominal pain
HNBB (Hyoscine N-
Butyl Bromide) 20mg
1amp IVTT now
Acts as agonist at specific
opioid receptors in the CNS to
produce analgesia, euphoria,
sedation for relief of moderate
to severe pain
It's a competitive antagonist
of the actions of acetylcholine
and other muscarinic agonists
causing smooth muscle
relaxation indicated for her
abdominal pain
Given
Given
MHBR Moderate high back rest is to
elevate the upper portion of
the body to increase lung
expansion thus promoting gas
exchange. This is also to
prevent ascending infection
that could be caused by
possible rupture of the
gallbladder.
Done
Refer any
unusualities: severe
In order for the patient to be
assessed and evaluated
Done
Page | 52

abdominal pain,
vomiting
properly and be managed
accordingly.
5/9/10
8:10am
Start Cefoxitin
(Monowel) 1g IVTT
q8 ANST
Cefoxitin inhibits synthesis of
bacterial cell wall causing cell
death which acts as a
perioperative prophylaxis for
surgical procedures. ANST or
after negative skin test is to
check whether the client is
not allergic to the antibiotic.
Done. Result
for skin test
is negative.
Cefoxitin
may be
given to the
patient.
For ultrasound
tomorrow morning
This is done to visualize
internal organs, to capture
their size, structure and any
pathological lesions with real
time tomographic images.
This is also to know the
condition of the gallbladder
whether it ruptured or not.
Not able to
comply.
Patient had
her
ultrasound
on May 11,
2010.
For total bilirubin,
Direct bilirubin,
Indirect bilirubin
Bilirubin is elvated if
hepatocytes are injured and
cannot metabolize or excrete
bilirubin
Increases in conjugated
bilirubin are highly specific for
disease of the liver or bile
ducts
Increase in unconjugated
bilirubin may be caused by
hepatic disease, cholestasis,
Done.
Results are
normal
Page | 53

Alkaline phosphatise
and hemolysis
High levels of alkaline
phosphatise indicates liver
disease
SGPT
(Serum glutamic
pyruvic
transaminase)
SGOT
(Serum glutamic
oxaloacetic
transaminase)
SGPT is released into blood
when the liver or heart is
damaged; thus, this is to
determine liver function.
Elevation of this may possibly
mean liver problems
AST (aspartate
aminotransferase) or SGOT is
an enzyme found in high
amounts in heart muscle and
liver and skeletal muscle
cells. It is also found in lesser
amounts in other tissues.
Elevated levels may be
caused by liver or heart
disease
Done.
Patients
SGPT
results are
high
Done. SGOT
results are
also high
Schedule for
laparoscopic
cholecystectomy on
Tuesday (4/11/10)
2pm
Lap Chole was to surgically
remove the gallbladder with
only a small incision.
Done.
Surgery was
done on
4/11/10 @
4pm
Secure consent/AC Patient has the right to be
consented in all procedures to
be done, and for legal
Done.
Page | 54

purposes. Anesthesia
clearance is for the patient to
be evaluated whether he/she
is fit to undergo the operation.
It is also for the
anaesthesiologist to predict
the operative risk and the
appropriateness of the
anaesthesia to be induced
during operation.
Inform OR For the OR to know that such
case will be performed and to
prepare the necessary
instruments and room. This is
also to coordinate availability
of staff and surgeon
Done
Refer In order for the patient to be
assessed and evaluated
properly and be managed
accordingly.
Done
5/9/10
5:00pm
May have ultrasound
on Tuesday 5/11/10
This was to visualize internal
organs, to capture their size,
structure and any pathological
lesions with real time
tomographic images. It is also
to know whether the
gallbladder has ruptured or
not.
Done.
Ultrasound
result
retrieved on
5/11/10.
Impression:
Cholelithiasi
s;
Sonographic
ally normal
liver and
Page | 55

pancreas
5/10/10
1:00pm
To reschedule OR
tomorrow from 2pm
to 4pm
To inform the OR that the
procedure will be moved from
2pm to 4pm
Done.
Patient had
her surgery
at 4pm of
May 11,
2010.
IVF TF: PNSS 1L @
KVO
PNSS is an isotonic solution
for hydration and as a
medium for IVTT meds; KVO
was done since patient’s
hydration was good.
Done
9:15pm Please facilitate AC AC is to assess patient’s rate
of survival and check for what
anesthetics is right for the
patient, making sure that the
patient isn’t allergic to the
anesthetic
Done
For Lap Chole tom
4pm
This was to surgically remove
the gallbladder with only a
small incision. Patient can
undergo laparoscopic
cholecystectomy since
gallbladder has not ruptured
yet as seen on the ultrasound
result.
Done.
For blood chem. and
Ultrasound tom
Blood tests are used to
determine physiological and
biochemical states, such as
disease, mineral content,
drug effectiveness, and organ
Done.
Page | 56

function.
9:30pm Pre-op orders:
NPO after light
breakfast (8am)
Assess VS prior to
OR
General oral hygiene
IVF: D5NSS 1L @
120cc/hr
Meds:
Diazepam 10mg 1
tab 2am
NPO is to prevent peristalsis,
aspiration and injury during
surgery
as baseline data and to detect
any unusualities
Oral hygiene is the practice of
keeping the mouth clean and
healthy by brushing and
flossing to prevent tooth
decay and gum disease.
Intravenous solutions with
reduced saline concentrations
typically have dextrose added
to maintain a safe osmolality
while providing less sodium
chloride; to hydrate before
surgery in preparation for
disruption of homeostasis
Potentiates the effects of
GABA; Act in spinal cord and
at supraspinal sites to
Done
Done
Done
Done
Given
Page | 57

Ranitidine 150mg
1tab 2am
Vitamin K
produce skeletal muscle
relaxation; it is also used as
adjunct to General anesthesia
Inhibits basal gastric acid
secretion and gastric acid
secretion; patient was placed
on NPO
For the liver to activate
clotting factors such as
prothrombin, proconvertin,
thromboplasstin, and stuart
factor.
Given
Given
5/11/10
1:30pm
NPO NPO is to prevent peristalsis,
aspiration and injury to the GI
tract during surgery.
Done
Post op orders:
To PACU then to
room
NPO for 4 hrs then
may have SD
Patient must first be stabilized
before transfer to the ward;
PACU is a place with
complete gadgets and staff
for emergency purposes after
post op.
Patient not yet fully conscious
due to anesthetics, thus this
is to prevent aspiration.
Done
Done
Page | 58

Monitor VS q15 until
stable then q30 for
2hrs then q2
Meds:
Etoricoxib 120mg PO
12mn
Tramadol 100mg
1tab 12mn
Demerol 50mg IVTT
Sultamicillin 375mg
PO TID
Monitoring vital signs is to
detect any unusualities after
the operation.
Half life is 22hrs. Etoricoxib
blocks COX2 thus relieving
pain and inflammation.
Half life is 5-7hrs
Inhibits the reuptake of
norepinephrine and serotonin;
causes many effects similar
to opioids – analgesic
Half life is 3-5hrs
Causes analgesia, euphoria,
sedation; thus reducing pain
Inhibits synthesis of bacterial
cell wall causing cell death;
this was indicated due to
possible intra – abdominal
infections
Done
Given
Given
Given
Given
O2 inhalation @ 4pm
until fully awake
This ensures optimum
oxygenation of cells gearing
towards achieving balance or
homeostasis. Also this was
for optimum respiratory level;
prevents lung collapse.
Done
Page | 59

MHBR Moderate high back rest is to
elevate the upper portion of
the body to increase lung
expansion thus promoting gas
exchange.
Done
Deep breathing
exercises for 15mins
TID
Post op exercise is indicated
To prevent lung collapse and
to eliminate anesthetic gases
introduced to the body
Done
5/12/10
11:15am
May have DAT Patient may eat anything as
long as it can’t harm her
current condition
Done.
Continue meds For the patient to complete
the medication regimen and
for continuity of care
Done
Wound care Daily routine wound care is
indicated in order to promote
healing and/or prevent
infection
Done
5/13/10
9:00am
MGH Patient may go home after
the doctor decides if
unusualities are absent
Done
Home meds:
Etoricoxib 90mg PO
BID
Tramadol 100mg ½
tab PO BID
Half life is 22hrs. Etoricoxib
blocks COX2 thus relieving
pain and inflammation.
Half life is 5-7hrs
Inhibits the reuptake of
Done.
Patient was
informed
Page | 60

Sultamicillin 375mg
PO BID
norepinephrine and serotonin;
causes many effects similar
to opioids – analgesic
Inhibits synthesis of bacterial
cell wall causing cell death
C/D IVF Terminate IVF when IVF is
about 50cc
IVF
discontinued
ff. up check at
5/18/10
Follow up check up is for the
patient to be assessed and
evaluated properly and be
managed accordingly.
Patient to
come back
at 5/18/10
Page | 61

DIAGNOSTIC EXAM
CBC – a determination of red and white blood cells per cubic millimeter of blood. It helps health professional check any
symptoms such as weakness, fatigue, or bruising. It also helps diagnose conditions such as anemia, infection and other
disorders
May 8, 2010
Test Normal Values
Result Remark Rationale Interpretation Nursing Responsibilities
Hemoglobin 115.0-
155.0
137.0 Normal Hemoglobin carries
oxygen to and removes
carbon dioxide from red
blood cells. It measures
total amount of
hemoglobin in the blood
Within normal
range
There is very little risk
associated with taking
blood from a vein in the
arm, although there is a
slight risk of infection
anytime the skin is
broken. Strict asepsis
should be observed
The patient may feel
discomfort when blood is
drawn from a vein.
Hematocrit 0.36-
0.52
0.42 Normal Hematocrit measures the
percentage of red blood
cells in the total blood
volume
Within normal
range
RBC 4.2-6.1 4.47 Normal Measures the number o
RBCs per cubic millimeter
of the whole blood.
Within normal
range
Page | 62

Bruising may occur at
the puncture site, or the
person may feel dizzy or
faint. Pressure should be
applied to the puncture
site until the bleeding
stops to reduce bruising.
Warm packs can also be
placed over the puncture
site to relieve discomfort
Instruct patient in dietary
sources of iron such as
red meat, organ meats,
clean green vegetable
and fortified grains
Protect the patient from
potential sources of
infection, monitor for
WBC 5.0-
10.0
14.1 High Determines the number of
circulating WBCs per cubic
millimeter of the whole
blood.
Elevated levels
may be caused by
acute infections –
tuberculosis,
pneumonia,
meningitis,
tonsillitis,
appendicitis,
colitis, etc.
Neutrophil 55-75 74 Normal Phagocytes engulfing
bacteria and cellular
debris. It prevents or limits
bacterial infections.
Within normal
levels.
Lymphocyte
s
20-35 21 Normal Cells present in the blood
and lymphatic tissue that
provide the main means of
immunity for the body.
There are three types of
lymphocytes: the natural
killer (NK), thymus-derived
lymphocytes (T cells), and
Within normal
range
Page | 63

bone marrow-derived
lymphocytes (B cells). NK
cells are found in the
blood, red bone marrow,
lymph nodes and spleen
and are able to destroy
many kinds of infected
body cells and tumor cells.
The T cells and B cells are
involved in specific
immune responses.
signs of infection.
Provide soft, bland diet
high in protein, vitamins,
and calories. Meticulous
hand washing and strict
asepsis are mandatory
Institute protective
isolation measures
immediately if there is
neutrophil disorder. Also
instruct the patient to
observe aseptic
technique and to take
caution most especially
if immunocompromised.
Inflammatory responses
involve more than one
body system. Monitor
the patient for worsening
Monocytes 2-10 4 Normal This type of granular
leukocyte functions in the
ingestion of bacteria and
other foreign particles
Within normal
range
Eosinophil 1-8 1 Normal Functions in allergic
responses and in resisting
infections. Eosinophils
mount on attack against
parasitic invaders by
attacking to their bodies
Within normal
range
Page | 64

and discharging toxic
molecules from their
cytoplasmic granules.
of the inflammatory
condition, particularly
respiratory
compromised.
Encourage patient to
rest between activities.
Encourage patient to
plan ahead and save
energy for the most
important activities.
Encourage patient to
void or stop activities
that make short of
breath or make heart
beat faster.
Encourage patient to Eat
a diet with adequate
protein and vitamins.
Drink plenty of non-
caffeinated and non-
Platelet 150.0-
400.0
278 Normal A test that direct count of
platelets in whole blood.
Platelets number from
100,000-500,000 per cubic
millimeter and are
important in triggering the
sequence of events that
leads to the formation of
blood clots.
Within normal
range
Page | 65

alcoholic fluids.
Urinalysis - Urinalysis is a physical, microscopic, or chemical examination of the urine. It is done to detect urinary tract
infection. It also measures the level of ketones, sugar, protein, blood components and many other substances
May 8, 2010
TEST RESULT NORMAL CLINICAL SIGNIFICANCE NURSING RESPONSIBILITIES
Glucose Negative <50mg/dL Glucose is the type of sugar found in blood.
Normally there is very little or no glucose in urine.
When the blood sugar level is very high, as in
uncontrolled diabetes. Glucose can also be found in
urine when the kidneys are damaged or diseased.
Advise Patient to:
Wash hands to make
sure they are clean
before collecting the
urine.
If the collection cup
has a lid, remove it
carefully and set it
down with the inner
surface up. Do not
Protein Negative <30mg/dL Protein is normally not found in the urine. Fever,
hard exercise, pregnancy, and some diseases,
especially kidney disease, may cause protein to be
in the urine.
Bilirubin Negative <1mg/dL This is a substance formed by the breakdown of red
blood cells. If it is present, it often means the liver is
Page | 66

damaged or that the flow of bile from the gallbladder
is blocked.touch the inside of the
cup with your fingers.
Clean the area around
your genitals.
Begin urinating into
the toilet or urinal.
Finish urinating into
the toilet or urinal.
Carefully replace and
tighten the lid on the
cup then return it to
the lab.
After the urine has
flowed for several
seconds, place the
collection cup into the
urine stream and
collect "midstream"
urine without stopping
your flow of urine.
Urobilinogen Normal <2mg/dL This is a substance formed by the breakdown of
bilirubin. Urobilinogen in urine can be a sign of liver
disease (cirrhosis, hepatitis) that the flow of bile
from the gallbladder is blocked.
pH 6 4.5-8 Urine pH is used to classify urine as either a dilute
acid or base solution. The lower the pH, the greater
the acidity of a solution; the higher the pH, the
greater the alkalinity. The glomerular filtrate of blood
is usually acidified by the kidneys from a pH of
approximately 7.4 to a pH of about 6 in the urine
Blood Negative <5-
10RBC/mL
Red blood cells in the urine may be caused by
kidney or bladder injury, kidney stones, a urinary
tract infection (UTI), inflammation of the kidneys
(glomerulonephritis), a kidney or bladder tumor, or
systemic lupus erythematosus (SLE).
Ketone Negative <5 mg/dL Ketones in the urine may mean a very serious
condition, diabetic ketoacidosis, is present. A diet
low in sugars and starches (carbohydrates),
starvation, or severe vomiting may also cause
Page | 67

ketones to be in the urine.Do not touch the rim
of the cup to your
genital area. Do not
get toilet paper, pubic
hair, stool (feces),
menstrual blood, or
anything else in the
urine sample.
Nitrite Negative Negative Bacteria that cause a urinary tract infection (UTI)
make an enzyme that changes urinary nitrates to
nitrites. Nitrites in urine show a UTI is present.
Leukocytes 25 <25WBC/
mL
Leukocyte esterase shows leukocytes in the urine.
WBCs in the urine may mean a UTI is present.
Clarity Clear Clear Urine is normally clear. Bacteria, blood, sperm,
crystals, or mucus can make urine look cloudy.
Specific
gravity
1.010 1.010-1.030 This checks the amount of substances in the urine.
It also shows how well the kidneys balance the
amount of water in urine. The higher the specific
gravity, the more solid material is in the urine.
Color Yellow Pale to dark
yellow
Many things affect urine color, including fluid
balance, diet, medicines, and diseases. How dark
or light the color is tells you how much water is in it.
Vitamin B supplements can turn urine bright yellow.
Some medicines, blackberries, beets, rhubarb, or
blood in the urine can turn urine red-brown.
Page | 68

Blood Chemistry - A number of tests performed on blood serum (liquid portion of the blood). It determines certain
enzymes that may be present (including lactic dehydrogenase [LDH], certain kinase [CK], aspartate aminotransferase
[AST], and alanine aminotransferas [ALT]), serum glucose, hormones such as thyroid hormone and other substances
such as cholesterol and triglycerides. These tests provide valuable diagnostic cues.
May 9, 2010
TEST RESULT REFERENCE REMARK RATIONALE
Total Bilirubin 8.3 2.0 – 21.0 Normal It occurs when bilirubin production exceeds the liver's
excretory capacity. This may occur because (1) too
much bilirubin is being produced, (2) hepatocytes are
injured and cannot metabolize or excrete bilirubin, or
(3) the biliary tract is obstructed blocking the flow of
conjugated bilirubin into the intestine
Direct Bilirubin 0.9 0.0 – 3.4 Normal Increases in conjugated bilirubin are highly specific for
disease of the liver or bile ducts
Inderct Bilirubin 7.4 2.0 – 17.0 Normal Increase in unconjugated bilirubin may be caused by
hepatic disease, cholestasis, and hemolysis
SGPT 60.2 0.0 – 34.0 High SGPT is released into blood when the liver or heart is
Page | 69

damaged; thus, this is to determine liver function.
SGOT 55.6 0.0 – 31.0 High SGOT is an enzyme found in high amounts in heart
muscle and liver and skeletal muscle cells. Elevated
levels may be caused by liver or heart disease
Alkaline
Phosphate
191 64 – 306 Normal When a person has evidence of liver disease , very
high ALP levels can tell the doctor that the person’s
bile ducts are somehow blocked
Medical sonography (ultrasonography) is an ultrasound-based diagnostic medical imaging technique used to visualize
muscles, tendons, and many internal organs, to capture their size, structure and any pathological lesions with real time
tomographic images. Ultrasound has been used by sonographers to image the human body for at least 50 years and has
become one of the most widely used diagnostic tools in modern medicine.
Page | 70

12/28/10 Isaac T. Robillo Memorial Hospital
Impression:
Non-obstructive cholelithiasis
Ultrasonically normal liver, intrahepatic ducts,
pancreas, spleen, aorta, paraaortic areas, kidneys
and urinary bladder
05/11/10 Davao Medical School Foundation
Impression:
Cholelithiasis
Sonographically normal liver and pancreas
Nursing Responsibilities:
Explain the procedure and purpose of the test
Provide a gown without snaps, and ask the patient to remove all jewelry
Take ultrasound if the patient’s bladder is fluid filled for better results
Page | 71

DRUG STUDY
Generic Name: Meperidine Hydrochloride
Brand Name: DemerolClassification: Opioid agonist analgesicOrdered Dose: 50mg IVTT now then prn for abdominal pain Mode Of Action: Acts as agonist at specific opioid receptors in the CNS to
produce analgesia, euphoria, sedation; the receptors mediating these effects are thought to be the same with endorphins
Indications: Relief of moderate to severe acute pain.
Pre-op: Support for of anesthesia
Contraindications: Hypersensitivity to narcotics, diarrhea, asthma, COPD, respiratory depression, pregnancy, seizure, renal dysfunction
Drug Interactions: Potentiation of effects with barbiturate anesthetics Severe/fatal reactions with MAOIs Increased chances of respiratory depression,
hypotension, sedation, and coma with phenothiazinesSide Effect: Nausea, vomiting, loss of appetite, constipation, dizziness,
sedation, drowsiness, impaired visual acuityAdverse Effects: CNS: light-headedness, dizziness, sedation, euphoria,
dysphoria, delirium, insomnia, agitation, anxiety, fear, hallucinations, disorientation, mood changes, lethargy, weakness, headache, tremor
CV: peripheral circulatory collapse, tachycardia, bradycardia, arrhythmia, palpitations, hypertension, hypotension
Page | 72

Dermatologic: pruritus, urticaria, bronchospasm, edema GI: nausea, vomiting, dry mouth, anorexia, constipation, GU: ureteral spasm, urinary retention, oliguria,
decreased libido MAJOR: respiratory depression, apnea, circulatory
depression, respiratory arrest, shock, cardiac arrest
Nursing Responsibilities:
Keep opioid antagonist and facilities readily available during parenteral administration
Use caution when injecting to patients with hypotension Reduce dosage of Demerol in patients receiving
phenothiazines or other tranquilizers Reassure that addiction is unlikely to occur Use Demerol with extreme caution in patient with renal
dysfunction Give only prescribed dosage Avoid alcohol, antihistamines, sedatives, tranquilizers Do not take left over medications for other disorders Keep out the reach of children Take Demerol with food, small frequent meals May use laxative if constipation occurs Avoid driving or doing activities that require alertness
because it could cause drowsiness and impaired visual activity.
Bibliography: 2005 Lippincott’s Nursing Drug Guidewww.drugs.com/demerol.htmlwww.rxlist.com/demerol-drug.htm
Generic Name: Hyoscine N-butyl Bromide
Page | 73

Brand Name: Buscopan
Classification: Gastro-intestinal antispasmodicOrdered Dose: 20mg 1amp IVTT nowMode Of Action: It's a competitive antagonist of the actions of acetylcholine
and other muscarinic agonists. Hyoscine works by relaxing the muscle that is found in the walls of the stomach, intestines and bile duct (gastrointestinal tract) and the reproductive organs and urinary tract (genitourinary tract)
Indications: This medication is used to relieve bladder or intestinal spasms.
Contraindications: Hypersensitivity to hyoscine butylbromide, Patients with prostatic enlargement, paralytic ileus or pyloric stenosis, ulcerative colitis, closed angle glaucoma
Drug Interactions: Anticholinergic agents Antihistamines Monoamine oxidase inhibitors Tricyclic antidepressants Competitively blocks prokinetic agents
Side Effect: Nausea, vomiting, loss of appetite, constipation, dry mouth, rash, itching, swelling of the hands or feet, trouble breathing, increased pulse, dizziness, diarrhea, vision problems, eye pain
Adverse Effects: CNS: light-headedness, dizziness, sedation, euphoria, dysphoria, delirium, insomnia, agitation, anxiety, fear, hallucinations, disorientation, mood changes, lethargy, weakness, headache, tremor
CV: peripheral circulatory collapse, tachycardia, bradycardia, arrhythmia, palpitations, hypertension, hypotension
Dermatologic: pruritus, urticaria, bronchospasm, edema GI: nausea, vomiting, dry mouth, anorexia, constipation, GU: ureteral spasm, urinary retention, oliguria,
decreased libido MAJOR: respiratory depression, apnea, circulatory
depression, respiratory arrest, shock, cardiac arrest
Nursing Responsibilities:
Inform patient that drug may cause blurred vision. Instruct patient to report if she experiences such symptom.
Page | 74

Assess for parkinsonism and Extra-pyramidal symptoms.
Assess for urinary hesitancy Assess for constipation. Caution patient to avoid alcohol because it may
increase CNS depression. As appropriate, review all other significant adverse
reactions and interactions Give only prescribed dosage Do not take left over medications for other disorders Keep out the reach of children
Bibliography: MIMS 113th edition 2007http://home.intekom.com/pharm/quatrom/q-hyosc.html http://www.medicinenet.com/hyoscine_butylbromide-oral/page2.htmhttp://www.netdoctor.co.uk/medicines/100000395.html
Generic Name: Cefoxitin Sodium
Brand Name: Monowel
Classification: Antibiotic, Cephalosphorin (2nd gen)Ordered Dose: 1g IVTT q8 ANSTMode Of Action: Inhibits synthesis of bacterial cell wall causing cell death
Indications: Perioperative prophylaxis
Contraindications: Hypersensitivity to cephalosphorins and/or penicillinsDrug Interactions: Increased nephrotoxicity with aminoglycosides
Increased bleeding effects with anticoagulants
Side Effect: Stomach upset, nausea, vomiting, diarrheaAdverse Effects: CNS:, dizziness, lethargy, headache
CV: peripheral circulatory collapse, tachycardia, bradycardia, arrhythmia, palpitations, hypertension,
Page | 75

hypotension GI: nausea, vomiting, diarrhea, anorexia, abdominal
pain, psuedomembranous colitis GU: Nephrotoxicity Hematologic: bone marrow depression,
thrombocytopeniaNursing Responsibilities:
Culture infection before starting therapy Have vitamin K available in case of
hypoprothrombinemia Discontinue if hypersensitivity occurs Avoid alcohol while taking drug Take only prescribed dosage Complete antibiotic therapy, don’t skip doses Do not use extra medicine to make up the missed dose Do not use drug if you are allergic to penicillins and
cephalosporins Antibiotic medicines can cause diarrhea, which may be
a sign of a new infection. If you have diarrhea that is watery or has blood in it, call your doctor.
Store at room temperature away from moisture, heat, and light
If you get a skin rash, do not treat yourself.Bibliography: 2005 Lippincott’s Nursing Drug Guide
MIMS 113th edition 2007www.drugs.com/cdi/cefoxitin.htmlwww.revolutionhealth.com/drugs-treatments/cefoxitin
Generic Name: Diazepam
Brand Name: Valium
Classification: Benzodiazepine, skeletal muscle relaxantOrdered Dose: 10mg 1 tab 2am
Page | 76

Mode Of Action: Potentiates the effects of GABA; Act in spinal cord and at supraspinal sites to produce skeletal muscle relaxation
Indications: Relief of anxiety and tension; to lessen recall in patients prior to surgical procedures
Contraindications: Hypersensitivity to benzodiazepines, psychosis, shock, coma, alcoholic intoxication, pregnancy
Drug Interactions: Increased CNS depression with omperazole Increased effects of diazepam with cimetidine,
hormononal contraceptives Decreased effects with ranitidine
Side Effect: Drowsiness, dizziness, GI upset, difficulty concentrating, fatigue, nervousness, crying
Adverse Effects: CNS: drowsiness, sedation, depression, lethargy, fatigue, light headedness, disorientation, restlessness, tremor, stupor, psychomotor retardation, EPS, hallucinations, nasal congestion
CV: bradycardia, tachycardia, hypotension, hypertension, edema
Dependence: drug dependence Dermatologic: uticaria, pruritus, dermatitis GI: constipation, diarrhea, dry mouth, salivation,
nausea, anorexia, vomiting, hepatic dysfunction, jaundice
GU: incontinence, retention, change in libido, menstrual irregularities
Other: phlebitis and thrombosis at injection site, hiccups, fever, diaphoresis, pain at injection site
Nursing Responsibilities:
Carefully monitor pulse, respiration rate and blood pressure during administration
Keep addiction – prone patients under careful surveillance
Ensure ready access to bathroom if GI effects occur Provide small, frequent meals to prevent GI upset Establish safety precautions if CNS changes occur Monitor liver and kidney function, CBC during long term
therapy Taper dose gradually after long term therapy Discuss risk of fetal abnormalities with patients desiring
to become pregnant
Page | 77

Take drug exactly as prescribed Do not stop drug abruptly during long term therapy Caregiver should learn to assess seizures and monitor
patient Use of barrier contraceptive is advised while on this
drug Avoid alcohol, sleep inducing drugs
Bibliography: 2005 Lippincott’s Nursing Drug GuideMIMS 113th edition 2007www.drugs.com/valium.html www.medicinenet.com/diazepam/article.htm
Generic Name: Ranitidine Hydrochloride
Brand Name: Zantac
Classification: Histamine2 antagonistOrdered Dose: 150mg 1tab
Mode Of Action: Competitively inhibits action of histamine at histamine2 receptors of the parietal cells of the stomach, inhibiting basal gastric acid secretion and gastric acid secretion that is stimulated by food, insulin, histamine, cholinergic agonists, gastrin, and pentagastrin
Indications: Against ulcer brought about by NPO due to surgical procedure
Contraindications: Hypersensitivity to ranitidine, lactationDrug Interactions: Increased effects of warfarinSide Effect: Constipation, nausea, vomiting, breast enlargement,
impotence, headacheAdverse Effects: CNS: headache, malaise, dizziness, somnolence,
insomnia, vertigo CV: bradycardia, tachycardia, Dermatologic: rash, alopecia
Page | 78

GI: constipation, diarrhea, nausea, anorexia, vomiting, abdominal pain, hepatic dysfunction, jaundice
GU: gynecomastia, impotence Hematologic: leucopenia, granulocytopenia,
thrombocytopenia, pancytopenia Local: pain at IM site, local burning pain at injection site
Nursing Responsibilities:
Administer oral drug with meals and hs Decrease doses in renal and liver failure Provide concurrent antacid therapy to relieve pain Avoid cigarette smoking as it decreases
effectiveness Have regular medical follow-up to evaluate
response Adjust environment (lights, temp, noise) to prevent
headache Using ranitidine may increase your risk of
developing pneumonia Avoid drinking alcohol. It can increase the risk of
damage to your stomach If you think you have taken too much of this
medicine contact a poison control center or emergency room at once.
If you need to take an antacid you should take it at least 1 hour before or 1 hour after this medicine. This medicine will not be as effective if taken at the same time as an antacid.
If you get black, tarry stools or vomit up what looks like coffee grounds, call your doctor or health care professional at once. You may have a bleeding ulcer.
Bibliography: 2005 Lippincott’s Nursing Drug GuideMIMS 113th edition 2007www.rxlist.com/zantac- www.medicinenet.com/ranitidine/article.htmhttp://www.healthline.com/goldcontent/ranitidine
Page | 79

Generic Name: Phytonadione
Brand Name: Hema K
Classification: Fat soluble vitamin; antifibrinolytic agent Ordered Dose: 1amp now
Mode Of Action: Vitamin K is required for the liver to make factors that are necessary for blood to properly clot (coagulate), including factor II (prothrombin), factor VII (proconvertin), factor IX (thromboplastin component), and factor X (Stuart factor).
Indications: Preoperatively: to activate clotting factors to decrease chances of bleeding during surgical procedure
Contraindications: Hypersensitivity to benzyl alcohol, Drug Interactions: Coumarin and indanedione derivatives
Side Effect: No known side effects for this drug; bruising and bleeding are less likely to happen.
Adverse Effects: No known adverse effects reported
Nursing Responsibilities:
Instruct patient to take only prescribed order If a dose is missed, take as soon as remembered
unless almost time for the next dose Cooking does not destroy substantial amounts of
Vitamin K Caution patient to avoid IM injection and activities
leading to injury Patient should not drastically alter diet while taking
Vitamin K Use a soft toothbrush until coagulation effect is
corrected Advise patient to report any signs of
bleeding/bruising Patient should be advised not to take OTC drugs
Page | 80

without advice of health care provider Advise patient to inform health care provider of
medication regimen prior to treatment or surgery Emphasize importance of frequent lab test to
monitor coagulation factors Source MIMS 113th edition 2007
http://www.nlm.nih.gov/medlineplus/druginfo/natural/patient-vitamink.htmlhttp://www.drugs.com/enc/vitamin-k.html
Generic Name: Etoricoxib
Brand Name: Arcoxia
Classification: COX-2 Selective Inhibitor
Ordered Dose: 120mg PO 12mn
Mode Of Action: Arcoxia reduces pain and inflammation by blocking COX-2, an enzyme in the body.Arcoxia does not block COX-1, the enzyme involved in protecting the stomach from ulcers.Other anti-inflammatory medicines (NSAIDS) block both COX-1 and COX-2.Arcoxia relieves pain and inflammation with less risk of stomach ulcers compared to NSAID
Indications: relief of acute pain
Contraindications: Hypersensitivity to arcoxia and it’s ingredients such as etoricoxib
Drug Interactions: warfarin, a medicine used to prevent blood clots rifampicin, an antibiotic used to treat tuberculosis and
other infections water pills (diuretics) ACE inhibitors and angiotensin receptor blockers,
medicines used to lower high blood pressure or treat
Page | 81

heart failure lithium, a medicine used to treat a certain type of
depression birth control pills hormone replacement therapy methotrexate, a medicine used to suppress the immune
system
Side Effect: Nausea, vomiting, diarrhea, Headache, Rash, Blurred vision, Difficulty in sleeping, Muscle cramps, Fatigue
Adverse Effects: CNS: headache, malaise, dizziness, hallucinations, insomnia, vertigo, anxiety, drowsiness, confusion
CV: bradycardia, tachycardia, hypertension Dermatologic: rash, urticaria GI: constipation, diarrhea, nausea, anorexia, vomiting,
abdominal pain, hepatic dysfunction, jaundice GU: gynecomastia, impotence Hematologic: leucopenia, granulocytopenia,
thrombocytopenia, pancytopenia Local: pain at IM site, local burning pain at injection site
Nursing Responsibilities:
Take Arcoxia only when prescribed by your doctor.
For the relief of chronic musculoskeletal pain the recommended dose is 60 mg once a day.
If you have mild liver disease, you should not take more than 60 mg a day. If you have moderate liver disease, you should not take more than 60 mg every other day.
When taking the tablets, swallow them with a glass of water. Do not halve the tablet.
Take your Arcoxia at about the same time each day.
Taking Arcoxia at the same time each day will have the best effect. It will also help you remember when to take the dose.
It does not matter if you take Arcoxia before or after food.
Page | 82

Do not use Arcoxia for longer than your doctor says. Do not take a double dose to make up for the dose that
you missed. If you get an infection while taking Arcoxia, tell your
doctor. Arcoxia may hide fever and may make you think, mistakenly, that you are better or that your infection is less serious than it might be.
Bibliography: MIMS 113th edition 2007http://www.drugs.com/arcoxia.htmlhttp://arcoxia-side-effects.com/
Generic Name: Tramadol hydrochloride
Brand Name: Ultram
Classification: Central acting analgesicOrdered Dose: 100mg 1tab PO Mode Of Action: Binds to mu-opioid receptors and inhibits the reuptake of
norepinephrine and serotonin; causes many effects similar to opioids but doesn’t cause respiratory depression
Indications: Relief of moderate to severe pain.
Contraindications: Hypersensitivity to tramadol or opioids or intoxication with alcohol, opioids, or psychoactive drugs
Drug Interactions: Decreased effectiveness with carbamezapine Increased risk of tramadol toxicity with MAOIs
Side Effect: Dizziness, sedation, drowsiness, impaired visual acuity, nausea, loss of appetite
Adverse Effects: CNS: sedation, dizziness, headache, confusion, dreaming, anxiety, seizures
CV: hypotension, tachycardia, bradycardia, Dermatologic: pruritus, urticaria, sweating, pallor GI: nausea, vomiting, dry mouth, flatulence,
constipation,
Page | 83

Other: potential for abuse, anaphylactoid reactionsNursing Responsibilities:
Control environment ( temp, light, noise) Limit use in patients with past or present history of
addiction or dependence to opioids Caution patient not to chew or crush tablet Keep opioid antagonist readily available in case of
emergency Instruct post-op patients that drug suppress cough
reflex Monitor bowel function and arrange laxatives for
constipation Institute safety precautions (side rails, assistive
device) Provide frequent, small meals if GI upset occurs Provide back rubs, positioning, and other non
pharmacological measures to alleviate pain Take drug exactly as prescribed Avoid alcohol, antihistamines, sedatives,
tranquilizers while taking this drug
Bibliography: 2005 Lippincott’s Nursing Drug Guidehttp://www.webmd.com/drugs/drug-11276-Ultram+Oral.aspxhttp://www.drugs.com/ultram.htmlhttp://www.medicinenet.com/tramadol/article.htm
Generic Name: Sultamicillin (ampicillin and sulbactam)
Brand Name: Unasyn
Classification: AntibioticOrdered Dose: 375mg tab PO TID
Mode Of Action: It acts through the inhibition of cell wall mucopeptide
Page | 84

biosynthesis. Ampicillin has a broad spectrum of bactericidal activity against many gram-positiveand gram-negative aerobic and anaerobic bacteria. sulbactam in the UNASYN formulation effectively extends the antibioticspectrum of ampicillin to include many bacteria normally resistant to it and to other beta-lactamantibiotics.
Indications: Intra-Abdominal Infections caused by beta-lactamase producing strains of Escherichia coli, Klebsiella spp. (including K. pneumoniae*), Bacteroides spp. (including B. fragilis), and Enterobacter spp.
Contraindications: contraindicated in individuals with a history of hypersensitivity reactions to any of the penicillins.
Drug Interactions: allopurinol (Zyloprim); probenecid (Benemid); or an antibiotic such as amikacin (Amikin), gentamicin
(Garamycin), kanamycin (Kantrex), neomycin (Mycifradin, Neo-Fradin, Neo-Tab), netilmicin (Netromycin), streptomycin, tobramycin (Nebcin, Tobi).
Side Effect: Nausea, vomiting, stomach pain, bloating, gas, vaginal itching or discharge, headache, itching, swollen, black, or "hairy" tongue, thrush ;pain, swelling, or other irritation where the needle is placed.
Adverse Effects: CNS: lethargy, hallucinations, seizures GI: stomatitis, gastritis, nausea, vomiting, diarrhea,
abdominal pain, pseudomembranous colitis, nonspecific hepatitis
GU: proteinuria, oliguria, hematuria, pyuria Hematologic: anemia, thrombocytopenia, leukopenia,
neutropenia, prolonged bleeding time Hypersensitivity: rash, fever, wheezing, anaphylaxis Local: pain, phlebitis, thrombosis at injection site Other: superinfection, sodium overload, CHF
Nursing Responsibilities:
Culture infected area before beginning treatment Monitor serum electrolytes and cardiac status Do not use this medication if you are allergic to
ampicillin and sulbactam or to any other penicillin
Page | 85

antibiotic Antibiotic medicines can cause diarrhea, which may be
a sign of a new infection. If you have diarrhea that is watery or has blood in it, call your doctor. Do not use any medicine to stop the diarrhea unless your doctor has told you to.
Use this medication for the entire length of time prescribed by your doctor. Your symptoms may get better before the infection is completely treated.
This medication can cause you to have unusual results with certain medical tests. Tell any doctor who treats you that you are using ampicillin and sulbactam.
Store ampicillin and sulbactam at room temperature away from moisture, heat, and light.
Provide small, frequent meals if GI upset occurs Do not use extra medicine to make up the missed dose. Seek emergency medical attention if you think you have
used too much of this medicine. If you get a skin rash, do not treat yourself.
Bibliography: http://www.rxlist.com/unasyn-drug.htmhttp://www.pfizer.com/files/products/uspi_unasyn.pdfhttp://www.drugs.com/mtm/ampicillin-and-sulbactam.html
Page | 86

PROCEDURAL REPORT
Date of operation: May 11, 2010
Time of Operation: 4:48 pm
Time Ended: 6:25 pm
Age: 38 years old
Diagnosis: Calculous Cholecystitis
Operation Performed: Laparoscopic Cholecystectomy
Type of Anesthesia: General Endotracheal Anesthesia
Name of Surgeon: Dr. Walter Batucan
Anesthesiologist: Dr. Lamanosa
Scrub Nurse: J. Dabon, R.N.
Circulating nurse: R. Napoles, R.N.
Procedural Report
A. Definition of Laparoscopic Cholecystectomy
The surgery to remove the gallbladder is called a cholecystectomy. The
gallbladder is removed through a 5 to 8 inch long incision, or cut, in the
abdomen. The cut is made just below the ribs on the right side and goes to just
below the waist. This is called open cholecystectomy.
A less invasive way to remove the gallbladder is called laparoscopic
cholecystectomy. This surgery uses a laparoscope (an instrument used to see
the inside of your body) to remove the gallbladder. It is performed through
several small incisions rather than through one large incision.
A laparoscope is a small, thin tube that is put into your body through a tiny
cut made just below the navel. The surgeon can then see the gallbladder on a
television screen and do the surgery with tools inserted in three other small cuts
Page | 87

made in the right upper part of the abdomen. The gallbladder is then taken out
through one of the incisions.
B. Instrumentations
(4) folded towels(1) oral gastric tube(1) foley catheter(1) Veress needle(1) 5mm trocar/port(1) 10mm trocar/port(1)10mm right angle laparoscopic dissector(1) 5mm right angle dissector(1) Dolphin Nose Dissecting forceps(1) scoop
(1) Merlin dissector(1) suction irrigator(1) Bovie with spatula tip(1) endoscissors(1) cholangiogram catheter unit(1) aspirating needle(1) Laparoscope(4) metallic surgical clips(1) camera(1) light source cord(1) Bovie cord
C. Procedure
1. Placed on supine position, reverse trendelenburg
2. Administration of General Endotracheal Anesthesia (GETA)
3. Skin over surgical site is cleansed with antiseptic solution
4. Placement of drapes.
5. Three to four small
incisions is made in
the abdomen.
Carbon dioxide gas
is introduced into
the abdomen to
inflate the
abdominal cavity so
that the gallbladder
and surrounding
organs can be more easily visualized.
Page | 88

6. The laparoscope is inserted through one of the incisions (usually at the
incision below the umbilicus) and instruments will be inserted through
the other incisions to remove the gallbladder.
7. When the procedure is completed, the laparoscope is removed.
8. The gallbladder is sent to the lab for examination
9. The skin incisions are closed with stitches or surgical staples.
10.A sterile bandage/dressing or adhesive strips is applied.
D. Nursing Responsibilities
Preoperative Phase
o Secure the informed consent for legal purposes and take note of
the following things:
1. The surgeon must provide a clear and simple explanation of
the surgical procedure.
2. The nurse may witness the patient’s signature.
4. If the patient needs additional information about the procedure,
nurse notifies the surgeon.
5. The nurse ascertains that the consent form has been signed
before administering psychoactive drugs.
6. No patient should be urged or coerced to sign an operative
permit.
7. Refusing to undergo a surgical procedure is a person’s legal
right and privilege.
o Assess for drug and alcohol abuse. Persons with history of
chronic alcoholism often suffer from malnutrition and other
systemic problems that increase the surgical risk.
o Assess the respiratory status. The goal for potential surgical
patients is optimal respiratory function.
Page | 89

o Assess the cardiovascular status. The goal in preparing any
patient for surgery is to ensure a well functioning cardiovascular
system to meet the oxygen, fluid and nutritional needs.
o Assess the hepatic and renal functioning. Presurgical goal is
optimal function of the liver and urinary system to enhance
removal of medications.
o Assess the immune functioning. An important function of the
preoperative assessment is to determine the existence of
allergies.
o Assess for the previous medication use. A medication history is
obtained from each patient because of the possibility of drug
interactions
o Make nursing diagnoses, and prepare nursing care plans to
address patient’s needs
o Teach deep-breathing, coughing and incentive Spiro meter to aid
the patient post operatively
o Encourage mobility and active body movement to avoid
complications
o Teach cognitive coping strategies such as imagery, distraction
and optimistic self-recitation to reduce fear and anxiety
o Explain the activities that may occur inside the operating room to
reduce anxiety
o Inform the patient on the following to impart knowledge on the
part of the patient and to avoid delay in surgery due to
noncompliance:
Scheduled date and time of the surgery and where to
report
What to bring such as insurance card, list of medications
and allergies
What to leave at home such as jewelry, watch, medications
and contact lenses
Page | 90

What to wear which is loose-fitting, comfortable clothes
and flat shoes
take nothing by mouth for six to 12 hours before the
surgery.
o Acquire and document patient’s vital signs for baseline data and
maintain the preoperative record
o Transport the patient to the presurgical area to prepare the patient
for surgery
o Attend to the family needs to reduce the anxiety felt by the family
o Make sure that preoperative checklist which contains the following
is accomplished:
Lab exam results in
OR services form accomplished
Patient is scheduled in OR
Anesthesiologist informed
Medicines in
Blood Typed and Matched
Field of Operation prepared
Sponged or bathed
Diet instruction given
Enema given
Make-up and nail polish removed
Jewelry removed
Oral hygiene given
Patient changed into patient’s gown
Indwelling catheter inserted
Pre-op meds given
Medicine for OR in
Intraoperative phase
Page | 91

o Position the patient:
The patient is in a supine position reverse trendelenburg.
o Skin preparation
o Circulating nurse:
Manages the operating room
Protects patient’s safety and health by monitoring the
activities of the surgical team
Checks and verifies the consent form
Ensures fire safety precautions, cleanliness, proper
temperature, humidity and lighting of the operating room
Monitors safe functioning of the equipments
Coordinates with the surgical/ perioperative team and
monitors aseptic practices
Documents operating room surgical activities
Count all needles, sponges and instruments together with
the scrub nurse
o For the scrub nurse:
Setting up sterile tables
Assisting the surgeon and assistant surgeon, taking
care of tissue specimens
Count all needles, sponges and instruments together
with the circulating nurse
Postoperative Phase
o Assess patient : appraise air exchanges status & note skin color;
verify & identify operative status & surgeon performed; assess
neurological status (LOC)
o Perform safety checks – good body alignment, side rails and
maintain patent airway and cardiovascular stability
Page | 92

o Medication
Analgesics are administered as prescribed for pain.
Antibiotics are administered to prevent infection.
o Surgical dressing is assessed periodically and reinforced when
necessary.
o HEALTH TEACHINGS
Inform the patient about the importance of complying with
the prescribed medication.
Emphasize the proper dosage of the medications taken.
Educate the client about the importance of proper
nutrition.
Encourage the client to have the prescribed diet for her
condition.
Encourage to have early ambulation in order to promote
circulation and wound healing.
Instruct to do splinting while performing deep breathing
exercises to minimize pain.
Page | 93

NURSING THEORIES
VIRGINIA HENDERSON’S DEFINITION OF NURSING
Virginia Henderson sees the nurse as concerned with both healthy and ill
individuals, acknowledges that nurses interact with clients even when recovery
may not be feasible, and mentions the teaching and advocacy roles of the
nurses. In 1955, Virginia Henderson devised her own definition as to create a
proper standard of what nursing should be, to ensure safe and competent care
for patients. Her famous definition of nursing states "The unique function of the
nurse is to assist the individual, sick or well, in the performance of those activities
contributing to health or its recovery (or to peaceful death) that he would perform
unaided if he had the necessary strength, will or knowledge, and to do this in
such a way as to help him gain independence as rapidly as possible". In this
definition of hers, she recognized the need to be clear about the functions of the
nurse and described the nurse's role as substitutive (doing for the person),
supplementary (helping the person), or complementary (working with the
person), with the goal of helping the person become as independent as possible.
Henderson conceptualizes the nurse’s role as assisting sick or
healthy individuals to gain independence in meeting 14 fundamental
needs which is: (1) breathing normally; (2) eating and drinking adequately;
(3) eliminating body wastes; (4) moving and maintaining a desirable
position; (5) sleeping and resting; (6) selecting suitable clothes; (7)
maintaining body temperature within normal range; (8) keeping the body
clean and well-groomed to protect the integument; (9) avoiding dangers in
the environment and avoiding injuring others; (10) communicating with
others in expressing emotions, needs, fears, or opinions; (11) worshipping
according to one’s faith; (12) working in such a way that one feels a sense
of accomplishment; (13) playing or participating in various forms of
recreation; and (14) learning, discovering, or satisfying the curiosity that
leads to normal development and health, and using available health
Page | 94

facilities. When the patient was able to perform all the functions by him or
herself then the patient could be considered independent and no longer
required the aid of a nurse.
Virginia Henderson also believed that it was important that nursing
be based on evidence, and that research was a critical component of
improving nursing practice. She believed all nurses should have access to
literature on nursing and current nursing research to help better their
practices, and to this end, she worked to develop an index of nursing.
Virginia Henderson’s theory is one of the most valuable theories
that a student nurse has in his or her arsenal in providing care for the
clients. It provides student nurses a guide on what to focus on and on
giving priority on the care being provided to the client. The client was
admitted to Davao Medical School Foundation Hospital due to right upper
quadrant abdominal pain and was later diagnosed with Calculous
Cholecystitis. Employing this theory the student nurses noted that among
the 14 Fundamental Needs that Henderson laid out, eating and drinking
adequately and getting enough sleep and rest are given most priority.
Since the ability of the body to handle fat and other fat soluble substances
is impaired, following a diet which is specified for patients with Calculous
Cholecystitis is essential to improve the patient’s wellbeing. The diet
promoted by the student nurses to the client should be moderate in
calories and low in fat. This diet included High fiber foods (fresh fruits and
vegetables), Whole grains (such as whole wheat bread and oats) and lean
meat (such as chicken and fish). Supervising the client in her diet was
done by the student nurses in order for the client to improve her current
condition. Having enough rest and sleep is also important for the client in
order for her to reach optimum wellbeing. Having enough sleep periods
was encouraged to the client by the group. The client was made
comfortable and was placed in a stress free environment to minimize
stressors that might further compromise the client’s health.
Page | 95

ORLANDO’S THEORY
Ida Jean Orlando's theory was developed in the late 1950s from
observations she recorded between a nurse and patient. Her nursing process is
based on the manner in which all individuals act and that this process is used by
a nurse to meet a patient’s need for help; meeting this need improves the
patient’s behavior. The components of Orlando’s Nursing Process Theory are
(1.) patient behavior, (2.) nurse reaction, and (3.) nurse action. The nursing
process is set in motion by the patient’s behavior and all patient behavior, no
matter how significant, may represent a cry for help because the patient who
cannot resolve a need feels helpless, and the person’s behavior reflects this
feeling. Nurse reaction to a patient’s behavior forms the basis for determining
how a nurse acts; it consists of perception, thought, and feeling. The nurse’s first
experience with the patient’s behavior is through the senses; this perception
leads to thought, which evokes a feeling, and because these three parts occur
automatically and almost simultaneously a nurse must identify each part of the
reaction to help the patient. Nurse action is whatever the nurse says or does to
benefit the patient and when performing an action, the nurse is influenced by
stimuli related to the patient’s needs.
Orlando’s theory states that the function of the nurse is to find out and
meet the patient's immediate need for help and to use the nursing process
(nurse-patient interaction) to relieve a patient’s feelings of helplessness or
suffering.
Given the client’s current medical status, the group utilized
Orlando’s theory as they provided care and did their work. Focusing on
the client’s verbal and non-verbal cues as focusing on the immediate
people surrounding her is essential in any medical situation for it may
indicate distress or danger in one form or another. The patient may have
concerns that she will not communicate with the people around her. These
concerns may be hazardous to the client’s wellbeing and may further
compromise her health. Orlando’s theory keeps the student nurses focus
Page | 96

on the needs and concerns of the patient whether the client or her
significant others stated it or not. Learning how to interpret and validate
both verbal cues and non verbal cues is essential in any hospital situation
for not all cues is presented as it is. Therefore, the student nurses applied
Orlando’s theory to aid them in interpreting the actions and behaviors of
the patient. They also made sure to verify first what they’ve observed
before planning anything. The student nurses paid close attention to any
signs that may lead to distress that might threaten the patient’s life.
Application of the theory also helps the student nurse prepare and plan
the course of action towards the situation. This preparation leads to an
appropriate intervention by the nurse that might relieve the patient of her
distress or might even save the patient’s life.
ROY’S ADAPTATION THEORY
Roy’s Adaptation theory views the client as an adaptive system
where the goal of nursing is to help the person adapt to changes in
physiological needs, self-concept, role function & interdependent relations
during health & illness. Roy believed that the need for nursing care arises
when the client cannot adapt to internal & external environmental
demands.
Callista Roy noted different stimuli that would affect a client’s adaptive
response, namely the focal stimuli, which constitute the greatest degree of
change impacting upon the person and is the stimulus most immediately
confronting the person, the contextual stimuli which are all other stimuli of the
person’s internal & external world that can be identified as having a positive or
negative influence on the situation, and the residual stimuli which are those
internal or external factors whose current effects are unclear. With that said,
Callista Roy theorized that there are four adaptive modes: (1.) Physiological
mode which represents physical response to environmental stimuli & primarily
Page | 97

involves the regulator subsystem. The basic need is the physiologic integrity,
associated with oxygenation, nutrition, elimination, activity & rest and protection.
(2.) Self-concept mode which relates to the basic need for psychic integrity
(psychological & spiritual aspect)
a. Physical self – has components of body image & body sensation
b. Personal self – has components of self-consistency, self-ideal &
moral-ethical-spiritual self. (3.) Role function mode which identifies the patterns
of social interaction of the person in relation to others reflected by; (a.) primary
role which determines the majority of a person’s behavior & is defined by age,
sex and developmental stage. (b.) Secondary role - assumed to carry out the
tasks required by the stage of development & primary role.(c.) Tertiary role – are
temporary, freely chosen & may include activities related to hobby. (4.)
Interdependence mode – identifies patterns of human value, affection, love &
affirmation.
The proponents conceptualized that the patient’s well being
depends upon her ability to adapt to her current condition. Being able to
adapt to her illness may lead to a faster recovery. However failure to adapt
and cope up may lead to a decline in her health status. Therefore it is the
role of the student nurses to help the patient cope up with her ailment. Use
of Roy’s Adaptation Theory guided the student nurses that the goal of
nursing in this theory is the promotion of adaptive responses in relation to
the four adaptive modes. Nursing seeks to reduce ineffective responses &
promote adaptive responses as output behavior of the person. With that,
the proponents first identified the stressors, either in the client’s
environment or within the client herself, that cause distress to the patient’s
mental and emotional status. Having identified the said stressors, the
student nurses planned the action to be done and implemented it. One of
which is providing vital information about the patient’s current condition.
By providing the patient information, her false beliefs towards her ailments
may be reduced. Anxiety, which is the fear of the unknown, may also be
alleviated through giving the patient information. Aside from giving
Page | 98

information, the proponents also listened and took notice of the patient’s
concerns about her admission to the hospital. By doing so, the student
nurses hope that any mental and emotional stress may be reduced. This
decrease in stressors hopefully will lead the patient to a faster recovery.
Page | 99

NURSING CARE PLAN
1. Acute pain related to presence of surgical incision secondary to status post laparoscopic
cholecystectomy.
2. Impaired skin integrity related to surgical procedure: laparoscopic cholecystectomy secondary to
calculous cholecystitis
3. Deficient knowledge regarding illness and treatment course related to lack of information presented.
4. Risk for infection related to presence of surgical incision.
5. Risk for imbalanced body temperature related to exposure to anesthesia secondary to status post
laparoscopic cholecystectomy.
Page | 100

NURSING CARE PLAN
Patient’s Name: Meg Age: 38 years old
Chief Complaint: pain at the right upper quadrant of the abdomen Ward: 3C
Diagnosis: Calculous Cholecystitis
1. Acute pain related to presence of surgical incision secondary to status post laparoscopic cholecystectomy.
Date Cues Need Nursing Diagnosis Objective/Goal Nursing Interventions Evaluation
5/12/
10
4:30
pm
Subjective Cues:
Verbalized “Sakit
pa akong opera,
ngul-ngul pa.”
Objective Cues:
pain scale of 6 out
of 10 noted.
Grimaced face
noted.
Guarding
behavior noted.
C
O
G
N
I
T
I
V
Acute pain related to
presence of surgical
incision secondary to
status post laparoscopic
cholecystectomy.
R: Pain is a common
aftermath for every
surgery after the
anesthesia wore down.
Pain is recognized in two
different forms:
physiologic pain and
At the end of 3
hours nursing
intervention, the
patient will be able
to:
1. Report a
decrease in pain
intensity to a
scale of 3 out of
10.
2. Demonstrate
non–
1. Monitor and assess
vital signs every 2 hours.
R: Vital signs are usually
altered in acute pain.
2. Administer analgesics
(e.g Tramadol) as
ordered.
R: Tramadol is an
analgesic. It binds to
mu-opioid receptors and
inhibits the reuptake of
GOAL MET
At the end of
rendering 3 hours
nursing
intervention, the
patient was able
to:
1. Report pain as
relieved and
controlled as
evidenced by
verbalization
Page | 101

Slow and limited
movement of the
upper extremities
Patient is 1 day
post operative
0.5 mm incision
noted on the right
lower rib cage and
the subxyphoid
area; 10mm
incision below the
umbilicus.
Incisions are
covered with dry
and intact
dressing.
Vital Signs: T-
36.6°C; BP-
130/90; RR-18;
PR- 81.
E
P
E
R
C
E
P
T
U
A
L
P
clinical pain. Physiologic
pain comes and goes,
and is the result of
experiencing a high-
intensity sensation. It
often acts as a safety
mechanism to warn
individuals of danger
(e.g., a burn, animal
scratch, or broken
glass). Clinical pain, in
contrast, is marked by
hypersensitivity to
painful stimuli around a
localized site, and also is
felt in non-injured areas
nearby. When a patient
undergoes surgery,
tissues and nerve
endings are traumatized,
resulting in incision pain.
pharmacological
methods and/or
use of relaxation
skills and
diversional
activities, as
indicated, for
individual
situation.
norepinephrine and
serotonin; causes many
effects similar to opioids
but doesn’t cause
respiratory depression. It
is for moderate to severe
pain.
3. Evaluate the
effectiveness of
analgesic at regular
intervals after each
administration, also
observing for any
signs and symptoms
of untoward effects
(e.g. respiratory
depression, nausea
and vomiting)
R: The analgesic dose
of client, “Dili
na man kaayo
siya sakit,
makaya na
man.” And
reported a
pain scale of 3
out of 10
2. Demonstrate
non–
pharmacologic
al methods
and/or use of
relaxation
skills and
diversional
activities (e.g.
patient
maintained
moderate high
back rest
Page | 102

A
T
T
E
R
N
This trauma overloads
the pain receptors that
send messages to the
spinal cord, which
becomes
overstimulated. The
resultant central
sensitization is a type of
posttraumatic stress to
the spinal cord, which
interprets any
stimulation—painful or
otherwise—as
unpleasant. That is why
a patient may feel pain
in movement or physical
touch in locations far
from the surgical site.
http://
may not be adequate to
raise the client’s
pain threshold or may be
causing intolerable or
dangerous side
effects or both. Ongoing
evaluation will assist in
making necessary
adjustments for effective
pain management.
4. Monitor patient’s pain
at least every hour
while awake by the
use of the pain scale.
R: Allows evaluation of
the severity of the pain
felt by the patient. Pain
is a subjective
experience and only the
position; she
also
performed
diversional
activities such
as talking with
her watcher)
Vital Signs: T-
36.4°C; BP-
120/90; RR-19;
PR- 84.
Page | 103

www.surgeryencyclopedi
a.com/Pa-St/Post-
Surgical-Pain.html
patient can describe the
pain she’s feeling.
5. Instruct and
demonstrate use of
deep breathing
exercise. Also
instruct patient to do
splinting while doing
deep breathing
exercises.
R: Deep breathing
increases oxygen in the
body and prevents
atelectasis. Deep
breathing exercise also
provides
comfort.Splinting while
doing deep breathing is
to lessen the pain upon
Page | 104

respiration.
6. Position the patient
properly in bed.
Elevate head of bed.
Maintain anatomic
alignment
R: Alignment helps
prevent pain from
malposition and it
enhances comfort
7. Encourage
diversional activities
(TV/radio,
socialization with
others, mental
imaging).
R: These highten ones
concentration upon
nonpainful stimuli to
Page | 105

decrease one's
awareness and
experience of pain.
8. Provide rest periods
to facilitate comfort,
sleep, and relaxation
R: The patient's
experiences of pain may
become exaggerated as
the result of fatigue.
Adequate rest helps
provide comfort
9. Assist patient in
doing her activities of
daily living
R: Helps reduce pain
brought about by the
exertion of force
necessary to perform
Page | 106

activities
10.Encourage patient to
report pain as soon
as it starts and allow
her to verbalize pain
experienced or
describe the pain
she’s feeling.
R: Severe pain is more
difficult to control and
increases the client’s
anxiety and fatigue.
2. Impaired skin integrity related to surgery: laparoscopic cholecystectomy secondary to calculous cholecystitis.
Date Cues Need Nursing Diagnosis Objectives/Goals Nursing Interventions Evaluation
5/11/10
Subjective: N Impaired skin integrity related to surgery:
At the end of 2 days nursing intervention
1. Assess dressings/ wound every shift.
Goal Met
Page | 107

@
9:00 pm
“Gioperahan ko diri sa tiyan,” as verbalized by the patient
Objective:
-post laparoscopic cholecystectomy (2 hrs)
-disruption of the dermis, epidermis, and subcutaneous tissues.
-with 0.5 to 1 cm incisions at the epigastrium, right lower rib cage and below the umbilicus
U
T
R
I
T
I
O
N
A
L
-
M
E
T
A
B
laparoscopic cholecystectomy secondary to calculous cholecystitis.
Rationale:
Laparoscopic cholecystectomy is a less invasive way to remove the bladder. It is performed through inserting a laparoscope just below the navel. Three additional ports are inserted by making three other incisions in the epigastrium and in the right upper quadrant of the abdomen.
Source:
Talamini, M. (2006). Advanced Therapy in
the patient will be able to:
1. Display improvement in wound healing as evidenced by intact incision site.
2. Remain free from infection as evidenced by normal vital signs and absence of purulent discharge.
3. Demonstrate behaviors/techniques to promote healing or prevent complications
Describe wounds and observe for changes.
®: Establishes comparative baseline providing opportunity for timely intervention.
2. Keep the incision site clean and dry, carefully dress wounds.
®: Keeping incision site clean and dry prevents infection; it also aids in the process of wound healing.
3. Encourage early ambulation. Assist patient in doing active and passive range of motion exercises.
®: Movement stimulates circulation and assists in the body’s natural process of repair.
5/12/10 @
11:00pm
At the end of 2 days nursing intervention, the patient was able to:
1. Maintain incision site and dressing intact and dry.
2. Remain free from infection as evidenced by normal vital signs (BP= 120/70; RR=18; PR=85; Temp=36.6) and absence of purulent discharge.
3.Demonstrate
Page | 108

-incisions covered with dry and intact dressing
-skin slightly warm to touch. Temperature: 36.8°C
O
L
I
C
P
A
T
T
E
R
N
Minimally Invasive Surgery, p. 179. USA: Decker Inc.
4. Monitor temperature every 4 hours.
®: Early recognition of developing infection enables rapid institution of treatment and prevention of further complications.
5. Place in semi-Fowler’s position or moderate high back rest.
®:Proper positioning decreases tension in the operative site and promotes healing.
6. Instruct to wear clean, dry, loose-fitting clothes, preferably cotton fabric
®: Skin friction caused by stiff or rough clothes leads to irritation of fragile skin and increases risk for
behaviors/techniques to promote healing or prevent complications (e.g patient washes hands after using the comfort room, eats a balanced diet, and takes antibiotic medication (sultamicillin) as ordered)
Page | 109

infection. Loose clothing reduces pressure on compromised tissues, which may improve circulation/healing
7. Emphasize importance of adequate nutrition and fluid intake. Encourage patient to eat foods rich in protein, iron and vit. C.
®: Improved nutrition and hydration will improve skin condition. Protein and iron helps in repair of tissues. Vitamin C is important for immune system function and increases resistance to some pathogens.
8. Instruct the client in proper postoperative skin care. Teach client and her significant
Page | 110

others the importance of proper hand washing.
®: This is to involve the patient in caring for skin, promoting comfort, and preventing infection or other complications. Proper washing of hands deter the spread of microorganisms.
9. Instruct the client to observe for signs and symptoms of complications such as elevated temperature, redness, warmth, swelling near the surgical incision, purulent discharge, or breakdown of sutures around the incision, and report to the physician.
®: Provides for prompt recognition of complications and facilitates prompt
Page | 111

treatment.
10. Administer antibiotics as indicated (sultamicillin)
®: May be given prophylactically or to treat specific infection and enhance healing.
3.Deficient knowledge regarding illness and treatment course related to lack of information presented.
Date
&
Cues Need Nursing Diagnosis Objective/Goal Nursing Interventions Evaluation
Page | 112

Time
05/12/
10
@
6:00
pm
Subjective
cues:
Verbalized:
“Para asa
diay ni siya
(holds
sultamicillin
tablet)?”
Objective
cues:
Frequent
questioning
Incorrect
verbal
feedback
regarding
understandin
g of
C
O
G
N
I
T
I
V
E
-
P
E
R
Knowledge deficit
regarding illness
and treatment
course related to
lack of information
presented.
R: Knowledge is
important especially
in health matters.
Deficiency in
knowledge might
affect the patient’s
health status. If
ever health issues
are taken for
granted, it may
result to
disorders/diseases
that could have
At the end of 2
hours nursing
intervention, the
patient will be
able to:
1. Verbalize
understanding of
disease process
and treatment.
2. Initiate
necessary
lifestyle changes
and participate in
treatment
regimen.
1. Assess the patient’s
current knowledge of the
medications and other
doctor’s instructions and
nursing procedures and its
implications, the likelihood
of complications if these are
not followed, and the
likelihood of cure or disease
control. Specifically ask
about the physician’s
explanations and the
patient’s past experiences.
R: Adults learn best when
teaching builds on previous
knowledge or experience.
Assessing recall of the
physician’s explanations as
well as the patient’s past
Goal Met
At the end of 2
hours nursing
intervention, the
patient was able to:
1. Verbalize
kasabot nako karon
ngano ginahatagan
ko ug mga ing
aning tambal, para
pud malabanan ang
inpeksyon nako.”
2. Initiate necessary lifestyle changes and participate in treatment regimen and verbalized “ Sa sunod mag-iwas na gyud ko ug mga taba kayo nga
Page | 113

treatment
regimen.
C
E
P
T
U
A
L
P
A
T
T
E
R
been prevented if
the patient had
enough knowledge
regarding her
current health
status. Lack of
knowledge about
health may also
contribute to
occurrence of
anxiety.
Source:
Berman, A. et. al.
(2008) Kozier &
Erb’s Fundamental
of Nursing
Concepts, Process
and Practice 8th
Edition. Pearson
Prentice Hall,
experiences and exposure
to health information
provides an opportunity for
evaluating attitudes and the
accuracy and completeness
of knowledge.
2. Ask how much the
patient wants to know.
Consider patient’s
preference for information in
planning and teaching.
R: People vary in the
degree of detail they find
helpful. Those who cope
with a threatening
experience by avoiding it
generally want to know
relatively little about
impending experiences,
whereas those who cope by
pagkaon.”
Page | 114

N volume Two,
Chapter 42, stress
and coping
learning as much as
possible about the
threatening experience want
to know a great deal.When
possible, supporting the
patient’s preferred learning
style shows respect for
individual differences.
3. Determine learning
needs. Consider needs
expressed by the patient
and family.
R: Learning needs
determine appropriate
content. Learning occurs
most rapidly when it’s
relevant to current needs.
Responding to expressed
needs displays sensitivity to
the patient’s and family’s
Page | 115

concern. Identifying
predictable concerns and
responses and necessary
self-care activities helps the
nurse fulfill learning needs
of which the patient and
family may be unaware.
4. Present manageable
amounts of information at
any one time.
R: Too much information at
one time causes confusion.
They patient may lose sight
of key points.
5. Inform the patient about
indication of medication,
drug interaction and its side
effects
R: Allows patient to be
Page | 116

knowledgeable about
medication and avoid
misconceptions.
6. Inform the patient about
the diet specific for her
condition (low fat, high fiber
foods; avoid spicy foods,
alcohol and caffeine)
R: A patient who has
recently had
a gallbladder removed may
suffer from diarrhea and
bloating after consuming
foods high in fat. Diarrhea
and bloating occur because
of two reasons. One reason
is that fat inside the
intestine absorbs more
water, causing stomach
upset. A second reason is
Page | 117

that bacteria begins to
digest the fat within the
intestine and ultimately
produces gas. When a
person
with gallbladder problems
consumes spicy foods, ,
unpleasant side
effects such as gas
and heartburn can occur.
7. Provide simple
explanations, using easy-to-
understand terminology.
R: Medical and nursing
jargon distances the patient
and family members.
Intricate explanations may
Page | 118

confuse or overwhelm them.
8. Discuss to the patient
and to the family the
importance of complying
with the medications and
other doctor’s orders.
R: This lets the patient be
aware of the significance of
the doctor’s instructions. It
also lets the patient know
the consequences which
might occur if instructions
weren’t followed. Knowing
the benefits of complying
with the instructions
encourages participation.
9. Ask for feedback.
R: The patient may initially
feel overwhelmed and
Page | 119

insecure about learning
because of the magnitude,
urgency or unfamiliarity of
necessary adaptations to
illness.
10. Use review and
repetition judiciously,
considering individual
factors.
R: The unit environment
and the patient’s age may
contribute to a short
attention span and poor
retention.
11. During and after
teaching, determine what
learning has occurred.
R: Determining learning
accomplishment permits
Page | 120

resolution of some learning
needs and provides
guidance for meeting
others.
12. Provide information
about additional learning
resources, like the nearest
baranggay health center in
their area.
R: Patients should be
informed that there are
health services in the health
centers which are for free,
so as to persuade them to
avail it.
Page | 121

DISCHARGE PLAN (M.E.T.H.O.D.)
I. MEDICATION
1. Take medications as ordered.
2. Inform the patient to take medications on time or as directed for the full
course of therapy even if feeling better.
3. Inform the client about the adverse effects and possible side effects of
the medications.
4. Inform the client about the importance of taking prescribed medications
and the consequences of not following the treatment regimen.
5. Encourage the patient to report or inform the health team if any of these
side effects occur. Inform and explain to the client that other drugs that
he is taking will probably have effects with the medication given.
Moreover, emphasize the right time interval of these drugs to maximize
its effects and avoid further complications.
6. Provide information for better understanding regarding therapeutic
regimen.
II. EXERCISE
1. Promote regular light exercise and exercise as tolerated.
2. Encourage exercise in lower and upper extremities to promote good
circulation.
3. Inform patient about proper exercise regimen to avoid injury.
4. Alternate rest periods with activity.
5. Encourage walking exercise.
III. TREATMENT
1. Instruct the patient to continue drug therapy as ordered.
2. Inform the patient as well as family the dangers of non compliance to
treatment regimen.
Page | 122

3. Discuss to the patient the complications and other problems that might
arise from the condition.
4. Inform the patient to exercise and do breathing exercises.
5. Instruct the patient to report to the health team promptly about any
changes on health condition.
6. Encourage patient to strictly comply with the doctor’s orders, especially
in taking prescribed medications.
7. Encourage the patient to have followed up visitations to the physician
after discharge.
IV. HEALTH TEACHINGS
1. Encourage patient to avoid strenuous activities.
2. Improving nutritional intake; meal planning is implemented with High
fiber moderate calorie, low fat and low salt as the primary goal.
3. Encourage to balance diet and intake of nutritious food such as
vegetables and lean meat, avoiding high fat foods.
4. Check with healthcare provider to evaluate progress of the condition.
5. Encourage to have adequate hydration. Water is the best source of fluid
that is needed by the body to maintain its function.
6. Instruct to avoid alcoholic beverages due to a compromised hepatic
system.
7. Encourage to have a restful and quiet atmosphere at home.
8. Encourage patient to use relaxation skills when in pain.
9. Encourage patient to seek emotional and social support especially to
family and friends to promote strength and comfort.
10.Check the condition with a healthcare provider to evaluate progress of
the condition.
V. OUTPATIENT
1. Remind patient on the arrangements to be made with the physician for
follow-up checkups.
Page | 123

2. Follow-up check up regularly in order to monitor and properly manage
patient’s illness.
3. Inform to continue medication as ordered.
4. Instruct to have a follow-up check up or refer to the physician if the
patient is uncomfortable.
5. Instruct the patient and significant others to report for any irregularities.
VI. DIET
1. The diet recommended for the client is High fiber moderate calorie, low
fat and low salt
2. Encourage patient to increase nutritious foods intake by eating fresh
fruits and vegetables, whole grain products, and lean meat.
3. Recommend to eat 5 or more servings of vegetables and fruits each day.
4. Encourage to choose whole grain foods instead of white flour and
sugars.
5. Advise to try to limit meats that are high in fat and cut back on processed
meats like hot dogs and bacon.
6. Inform patient to avoid food such as salted, cured, smoked, or canned
meat.
7. Increase oral fluid intake. Hydration is needed by the body to transport
nutrients needed by the body.
8. Instruct to avoid drinking of alcoholic beverages as much as possible.
9. Encourage not to forget to get some type of light exercise because the
combination of good diet and regular exercise will help in the
maintenance of healthy weight and the feeling of more energetic.
Page | 124

PROGNOSIS
Good Fair Poor Justification
Onset of the
illnesses
♠
Signs and symptoms of her current illness
first appeared on the second week of
December 2009. After three days, the
pain disappeared. But after two weeks,
pain recurred in a higher scale of pain
(5/10). Because of this, she was forced to
seek medical advice and consult at
Robillo Memorial Hospital. On May 5,
2010, three days prior to admission, the
patient again experienced right upper
quadrant pain. This was characterized to
be progressive pain with a pain scale of 8
out of 10. There was no radiation noted
and no associated symptoms. Two days
prior to admission, pain recurred with a
pain scale of 10 out of 10. This prompted
Meg to seek consultation, hence,
admission. On May 8, 2010, the patient
was admitted at Davao Medical School
Foundation at Surgical Ward, room 324
bed 5 under the service of Dr. Batucan,
with admitting diagnosis of Acute
Cholelithiasis. Based on the data, the
onset of illness of the client first started
on December of 2009. Patient did not
comply with her doctor’s order to modify
her diet (low fat, high fiber) and this led to
Page | 125

exacerbation of her illness. Because of
the patient’s onset of illness, the
proponents rated the area as fair.
Duration of
illnesses♠
The client’s hepatic system has been
compromised since December 2009, 5
months before admission to DMSF
Hospital. Because of the span of the
illness of the client, the proponents rated
the Duration of Illness as fair.
Precipitating
factors
♠
The precipitating factors of Calculous
Cholecystitis present in the client were (1)
Hormone replacement therapy, or birth
control pills and (2) a Low Fat Diet. Given
that the client has a few of the
precipitating factors present and has
none of the much more serious
precipitating factors, the proponents rated
the Precipitating factors as good.
Willingness
to take
medications
and
treatment
♠
Before she was brought to DMSF, she
had a consult first at the Robillo Hospital.
There, she was instructed to revise her
diet into a low fat, high fiber diet. She was
also instructed to drink lots of fluids.
However, patient was not able to comply
with this treatment plan and this later on
led to worsening of her condition. On the
positive note, she was later on able to
follow instructions about her treatment
regimen and cooperate with the health
care team when she was admitted at
Page | 126

DMSF. Because of these reasons, the
proponents rated the Willingness to take
medications and treatment as fair.
Age ♠
Most of the body’s protective
mechanisms become less efficient with
age. Since the patient is 38 years old, the
proponents rated the age factor as fair.
Environment
al factors
♠
The proponents rated the Environmental
factor as good for the reason that there is
nothing in her environment at home or at
work that can decrease her health status
and further compromise her wellbeing.
Family
support♠
The client’s family is very supportive and
willing to comply with the therapy in order
for the patient to get well, even with their
financial problems. The patient also
stated that her family provides her with all
the emotional support she needs.
Members of her family frequently visit her
in the hospital and she is able to verbalize
any concern to them. Her husband is also
present and is able to provide her support
as she undergoes her current condition.
TOTAL
3 4 0
Computation:
Poor:(0*1)/7 = 0/7
Fair: (4*2)/7= 8/7
Good: (3*3)/7= 9/7
Total: 17/7 or 2.42 (Good Prognosis)
*Scoring for General Prognosis: 1-1.6 = Poor Prognosis; 1.7-2.3 = Fair Prognosis; 2.4-3.0 = Good Prognosis
Page | 127

Rationale for a Good Prognosis
The patient has a good chance of recuperating from her current ailment as
evidenced by the study done. The onset and duration of the illness, the
absence of the much more serious precipitating factors, her willingness to take
medication and treatment, and the support of the patient’s family made the
prognosis better, increasing the chance of her recovery from her current
ailment. The current status of her condition is very manageable and there is a
good chance that she can recover as long as she is determined enough to
achieve optimum well being. Therefore, according to the research and the
calculations done by the proponents, the patient has a very good chance of
recovering from her ailment.
Page | 128

RECOMMENDATION
This case study about Calculous Cholecystitis gave the group more
information and knowledge in making an actual management for this kind of
problem. Thus, the members of the group have realized the need of promoting
and maintaining optimal health to both the patient and her significant others. With
these, the group would like to recommend the following.
To the client:
The patient’s participation and willingness to be assessed and comply with
the therapeutic regimen is needed for an effective management and prevention
of complications. The patient is encouraged to always reach for wellness, and be
cautious enough to know what her body needs and to recognize her limitations in
complying therapeutic regimen. Also, the patient is encouraged to follow the
discharge plan for the betterment of her condition while at home. She is also
recommended to have her regular follow-up checkups to evaluate her condition.
The patient is enlightened to be more open with her feelings regarding her
current condition, family problems and concerns about her health
To the client’s family:
The patient’s family plays an important role in the improvement of patient’s
condition because they are source of strength and inspiration to deal with the
disease. The family is encouraged to be sensitive enough to know the patient’s
need and weaknesses that they may be able to render their support and care. Just
with their presence and affection can help the patient feel that she is being loved
and that she can successfully surpass the challenges that are brought by her
illness. The feeling of being secured and accepted is what also the patient needs
to achieve optimal state of well being.
Page | 129

To the community:
The community should also be sensitive with the client’s condition, not
treating her like she is incapable of doing her daily activities. They must still
respect the client even with the illness. They must also be understanding enough
and let the client feel security and acceptance. They should be more aware about
this kind of condition. More knowledge should be acquired by the community to
be able to know how to manage this kind of illness and how to prevent the
occurrence of the illness within the community.
To the government:
Budget for health must be increased so that patients would be able to
receive adequate amount of health services from government hospitals. They
should also disseminate vital information regarding illnesses that may affect the
body’s hepatic system. They should also make sure that people from far flung
areas have access to medical services. Being able to access even basic medical
attention may lead to a decrease in certain ailments of the genitourinary system.
To professional health workers:
Health care providers should be passionate about their job, giving proper
care and support to their clients. Health workers should be sensitive to the
client’s feelings and emotions. They should be open for conversation to know
what the client is feeling at the moment. They should also continue their work
even though they receive little or sometimes no salary at all, thinking that what
they’re doing is for humanitarian reasons.
To the College of Nursing:
They should provide more exposure to the students on a consistent area
to further increase their experience regarding the concept. They should also do
proper scheduling of duties so that students wouldn’t be stressed out with their
case presentations, clearing any scheduling matters with the students. They
should also make sure that the student nurses are respected and treated well by
Page | 130

their superiors. Also, they should make sure that their students are safe while on
their duty, and if able, provide prophylactic treatment to avoid endangering the
lives of the students. The College of Nursing should be more sensitive to the
needs of the students and should be open to any comments or suggestions.
To the Student Nurses:
Give appropriate nursing care and follow out doctor’s order properly to
avoid any errors and give better care to the clients. Cooperation with the
healthcare team is also essential to provide better quality care. They should also
be honest in the data collecting done to the patient, putting in mind that they are
dealing lives. They should treat the client as a fellow human being giving quality
care and service. They must also research about the disease to enhance their
knowledge about it. They must also be updated with current updates that could
be beneficial to the nurse, the client and the rest of the healthcare team.
Page | 131

REFERENCES
Berman, A. et. al. (2008) Kozier & Erb’s Fundamental of Nursing Concepts,
Process and Practice 8th Edition. Pearson Prentice Hall, volume Two, Chapter
42, stress and coping
Boyer, M. (2006). Brunner and Suddarth’s Textbook of Medical-Surgical
Nursing, 11th ed.
Carol Mattson Porth (2005). Pathophysiology, Seventh edition.
Crowley, L. (2010). An Introduction to Human Disease: Pathology and
Pathophysiology Correlations, 8th ed., p. 563. USA: Jones and Bartlett
Publishers.
Digiulio, M. & Jackson, D.(2007). Medical-Surgical Nursing Demystified, p.
288. USA: McGraw-Hill.
Everhart, JE, Khare, M, Hill, M, Maurer, KR. Prevalence and ethnic
differences in gallbladder disease in the United States. Gastroenterology
1999; 117:632.
Ginsber, G. & Ahmad, N. (2006) The Clinician’s Guide to Pancreaticobiliary
Disorders, p. 121-123. USA: SLACK Incorporated.
Harrison’s Principles of Internal Medicine, Tenth Edition 1983.
Iyengar, V. Elemental Analysis of Biological Systems: Biomedical,
Environmental, Compositional and Methodological Aspects of Trace
Elements, Vol. 1, p. 49.
Kozier and Erbs, Fundamentals of Nursing, Chap. 20, page 352
Lippincott Williams and Wilkins Handbook of Diseases Third Edition, page
184
MIMS 113th edition 2007
Talamini, M. (2006). Advanced Therapy in Minimally Invasive Surgery, p. 179.
USA: Decker Inc.
Taylor, Lillis, LeMone and Lynn (2008),Fundamentals of Nursing: The Art and
Science of Nursing Care, 6th edition.
Understanding Medical Surgical Nursing by Williams and Hopper page 742
White, L. Foundations of Nursing: Caring for the Whole Person, p. 832.
Page | 132

http://arcoxia-side-effects.com/
http://digestive.niddk.nih.gov/statistics
http://home.intekom.com/pharm/quatrom/q-hyosc.html
http://medical-dictionary.thefreedictionary.com/calculi
http://www.diabetesmonitor.com/learning-center/gallstones.htm
http://www.drugs.com/arcoxia.html
http://www.drugs.com/enc/vitamin-k.html
http://www.drugs.com/mtm/ampicillin-and-sulbactam.html
http://www.drugs.com/ultram.html
http://www.healthline.com/goldcontent/ranitidine
http://www.learningplaceonline.com/stages/organize/Erikson.htm
http://www.medicinenet.com/hyoscine_butylbromide-oral/page2.htm
http://www.medicinenet.com/tramadol/article.htm
http://www.netdoctor.co.uk/medicines/100000395.html
http://www.nlm.nih.gov/medlineplus/druginfo/natural/patient-vitamink.html
http://www.pfizer.com/files/products/uspi_unasyn.pdf
http://www.rxlist.com/unasyn-drug.htm
http://www.turner-white.com/pdf/hp_nov00_murphy.pdf
http://www.webmd.com/drugs/drug-11276-Ultram+Oral.aspx
www.drugs.com/valium.html
www.medicinenet.com/diazepam/article.htm
www.medicinenet.com/ranitidine/article.htm
www.revolutionhealth.com/drugs-treatments/cefoxitin
www.rxlist.com/zantac-
Page | 133