Drug Interactions in Dentistry
15
2004;135;298-311 J Am Dent Assoc ELLIOT V. HERSH and PAUL A. MOORE importance of knowing your CYPs Drug interactions in dentistry: The jada.ada.org ( this information is current as of March 20, 2010 ): The following resources related to this article are available online at http://jada.ada.org/cgi/content/full/135/3/298 found in the online version of this article at: including high-resolution figures, can be Updated information and services http://jada.ada.org/cgi/collection/pharmacology Pharmacology : subject collections This article appears in the following http://www.ada.org/prof/resources/pubs/jada/permissions.asp reproduce this article in whole or in part can be found at: of this article or about permission to reprints Information about obtaining © 2010 American Dental Association. The sponsor and its products are not endorsed by the ADA. on March 20, 2010 jada.ada.org Downloaded from
Transcript of Drug Interactions in Dentistry

2004;135;298-311 J Am Dent Assoc
ELLIOT V. HERSH and PAUL A. MOORE importance of knowing your CYPs
Drug interactions in dentistry: The
jada.ada.org ( this information is current as of March 20, 2010 ):The following resources related to this article are available online at
http://jada.ada.org/cgi/content/full/135/3/298found in the online version of this article at:
including high-resolution figures, can beUpdated information and services
http://jada.ada.org/cgi/collection/pharmacologyPharmacology : subject collectionsThis article appears in the following
http://www.ada.org/prof/resources/pubs/jada/permissions.aspreproduce this article in whole or in part can be found at:
of this article or about permission toreprintsInformation about obtaining
© 2010 American Dental Association. The sponsor and its products are not endorsed by the ADA.
on March 20, 2010
jada.ada.orgD
ownloaded from

A B S T R A C T
298 JADA, Vol. 135, March 2004
C L I N I C A L P H A R M A C O L O G Y
Background. The hepatic and intestinalcytochrome, or CY, P450enzyme system is respon-sible for the biotransforma-tion of a multitude ofdrugs. Certain medicationsused in dentistry can actas substrates, inducers orinhibitors of this system. Methods. The authors conducted a MEDLINE search of articlesappearing between 1976 and the presentusing the keywords “drug interactions” and“cytochrome P450,” and reviewed reportsinvolving dental therapeutic agents usingPubMed links from an Indiana UniversityCYP450 drug interaction table on the WorldWide Web.Results. The antibiotics erythromycin andclarithromycin are potent inhibitors ofCYP3A4 and can increase blood levels andtoxicity of CYP3A4 substrates. Likewise,quinolone antibiotics such as ciprofloxacininhibit the metabolism of CYP1A2 sub-strates. Other dental therapeutic agents aresubstrates for CYP2C9 (celecoxib, ibuprofenand naproxen), CYP2D6 (codeine and tra-madol), CYP3A4 (methylprednisolone) andCYP2E1 (acetaminophen). Because codeineand tramadol are prodrugs, inhibition of theirmetabolism can lead to a diminution of theiranalgesic effects. While inducers ofacetaminophen metabolism, includingalcohol, theoretically can increase the propor-tion of it that is biotransformed into a poten-tially hepatotoxic metabolite, recent researchsuggests that concomitant alcohol intake doesnot increase the hepatotoxic potential of ther-apeutic doses of acetaminophen.Conclusions. A number of clinically sig-nificant drug interactions can arise withdental therapeutic agents that act as sub-strates or inhibitors of the CYP450 system.Clinical Implications. As polyphar-macy continues to increase, the likelihood ofadverse drug interactions in dentistry willincrease as well. Ensuring that patients’medical histories are up to date andacquiring knowledge of the various sub-strates, inducers and inhibitors of theCYP450 system will help practitionersavoid potentially serious adverse druginteractions.
Drug interactions in dentistryThe importance of knowingyour CYPs
ELLIOT V. HERSH, D.M.D., M.S., Ph.D.; PAUL A. MOORE, D.M.D., Ph.D., M.P.H.
As new drugs reach the marketplace andpatients take an increasing number andvariety of pharmaceutical agents for a host ofmedical conditions, the potential for seriousdrug interactions continues to grow.1 The
hepatic and intestinal cytochrome, or CY, P450 enzymesystem is responsible for the biotransformation of a mul-titude of drugs. As it is important for children to learn
their ABCs, it is becoming equallyimportant for dentists to learn theirCYPs, to lessen the chances of severedrug interactions’ appearing in theirpatients.
The CYP450 system is a group ofheme-containing enzymes embedded pri-marily in the lipid bilayer of the endo-plasmic recticulum of hepatocyteswithin the liver and enterocytes withinthe small intestine.2 CYP enzymes areinvolved in the oxidative metabolism ofa number of drug classes, as well as of avariety of endogenous substances,including prostaglandins and steroidhormones.
The current nomenclature of these enzymes is three-tiered: CYP followed by a number representing thefamily of enzymes, a letter representing the subfamilyand then another number representing the individualgene (for instance, CYP3A4).2,3 Each enzyme is termedan “isoform” or “isoenzyme.” More than 30 CYP450isoenzymes have been identified to date; the major onesresponsible for drug metabolism are CYP1A2, CYP2C9,CYP2C19, CYP2D6, CYP2E1 and CYP3A4. The humanCYP3A4 isoform is the most abundant cytochrome
JA D
AC
ON
TI
NU
I N G E D UC
AT
IO
N
✷✷
ARTICLE
1
Acquiringknowledge of
the cytochromeP450 system
will help practitioners
avoid potentially
serious adverse drug interactions.
COVER STORY
Copyright ©2004 American Dental Association. All rights reserved.
on March 20, 2010
jada.ada.orgD
ownloaded from

JADA, Vol. 135, March 2004 299
C L I N I C A L P H A R M A C O L O G Y
family expressed in the human liver and intes-tine, and thus is involved in the metabolism of agreater number of drugs and a greater proportionof adverse drug-drug interactions than are otherCYP isoforms.4
A substrate is a drug or endogenous compoundthat is metabolized by a particular CYP450 iso-form. Some substrates for the various CYP450isoforms are illustrated in Table 1.4,5 For example,the HIV protease inhibitors idinavir, nelfinivir,ritonavir and saquinavir—which, when combinedwith reverse transcriptase inhibitors, have
greatly improved the quality and longevity of lifein patients infected with the virus—are sub-strates for CYP3A4.5,6
Inducers of a specific CYP450 isoform (Table 2)increase the amount and subsequent activity ofthat particular enzyme in hepatic and smallintestinal tissue, potentially leading to dimin-ished plasma levels of active drugs that are sub-strates for that enzyme.2,3,5 In patients with HIVwho take protease inhibitors, the concomitantintake of the herbal antidepressant St. John’swort, which is available without a prescription,
TABLE 1
SOME SUBSTRATES FOR CYTOCHROME P450 ISOENZYMES.
CYP1A2
CYP2C9
CYP2C19
CYP2D6
CYP2E1
CYP3A4
Anesthetic agent, local: ropivacaineAnti-Alzheimer agent: tacrineAntiasthmatic agents: theophylline, zileutonAntidepressant agents: amitriptyline, clomipramine, fluvoxamine, imipramineAntipsychotic agents: clozapine, haloperidol
Angiotensin II receptor blockers: irbesartan, losartanAnticoagulant agent: warfarinAnticonvulsant agent: phenytoinCancer chemotherapeutic agent: tamoxifenHypoglycemic agents, oral: glipizide, glyburide, tolbutamideNSAIDs*: celecoxib, diclofenac, ibuprofen, naproxen
Antidepressant agents: amitriptyline, citalopram, clomipramine, imipramineBenzodiazepine: diazepamImmunosuppressant agent: cyclophosphamide (prodrug)Proton pump inhibitors: lansoprazole, omeprazole, pantopropazole
Analgesic agents, narcotic: codeine (prodrug), tramadol (prodrug)Anesthetic agent, local: lidocaineAntidepressant agents: amitriptyline, clomipramine, desipramine, imipramine, paroxetineAntipsychotic agents: haloperidol, perphenazine, risperidoneBeta blockers: carvedilol, metoprolol, propranolol, timolol
Analgesic agent, nonnarcotic: acetaminophenAnesthetic agents, general: enflurane, halothane, isoflurane, sevofluraneMuscle relaxant: chlorzoxazoneRecreational drug: ethanol
Analgesic agent, narcotic: alfentanilAnesthetic agent, local: lidocaineAntibiotic agents: clarithromycin, erythromycinAnticoagulant agent: warfarinAnticonvulsant agent: carbamazepineAntihistamine agents: astemizole,† terfenadine†Antipsychotic agents: haloperidol, pimozideBenzodiazepine agents: alprazolam, diazepam, midazolam, triazolamCalcium channel–blocking agents: amlodipine, diltiazem, felodipine,nifedipine, verapamilCholesterol-lowering drugs: atorvastatin, cerivastatin,† lovastatin (prodrug),simvastatin (prodrug)Corticosteroids: hydrocortisone, methylprednisolone HIV protease inhibitors: idinavir, nelfinivir, ritonavir, saquinavirHormonal agents: estradiol, progesteroneImmunosuppressant agents: cyclosporine, tacrolimusProkinetic agent: cisapride†
* NSAIDs: Nonsteroidal anti-inflammatory drugs.† No longer available in the United States.
ISOENZYME SUBSTRATE
Copyright ©2004 American Dental Association. All rights reserved.
on March 20, 2010
jada.ada.orgD
ownloaded from

300 JADA, Vol. 135, March 2004
C L I N I C A L P H A R M A C O L O G Y
significantly decreases blood levels and theantiviral efficacy of these drugs because St.John’s wort is a potent inducer of CYP3A4.7
On the other hand, enzymeinhibitors (Table 3) reduce theactivity of a specific CYP450 iso-form, resulting in an accumulationof the substrate drug.2,3,5 The toxicitytypically encountered is identical towhat would be seen from an over-dose of the substrate drug. WithCYP3A4, it is not only drugs thatcan inhibit this isoform, but alsograpefruit juice, a seeminglyinnocuous food product.5,8-10 Itappears that bergamottin, a furan-coumarin, and possibly some other related com-pounds found in grapefruit juice both inhibit theaction of and reduce hepatic and intestinal con-centrations of CYP3A4,11,12 causing the accumula-tion of a number of CYP3A4 substrates. Theability of grapefruit to lead to excessive plasmaconcentrations of CYP3A4 substrates first wasdescribed for calcium channel antagonists, whereexcessive blood levels can lead to hypotension andperipheral edema.9,13 This was a serendipitousfinding (as so many scientific discoveries are);grapefruit juice was being used in the study only
to mask the taste ofethanol.9
The purpose of thisarticle is to introducereaders to some of themore clinically relevantadverse drug interac-tions involving theCYP450 system thatcould appear in dentalpractice. An excellentand continuallyupdated table ofCYP450 substrates,inducers and inhibitors,with links to key arti-cles and PubMed, canbe found on the WorldWide Web.5
METHODS
We conducted a searchon MEDLINE of arti-cles appearing between1976 and the present
employing the keywords “drug interactions” and“cytochrome P450” and reviewed reportsinvolving dental therapeutic agents. In addition,
we reviewed PubMed links forinteractions involving dental thera-peutic agents as found on theCytochrome P450 Drug InteractionTable posted on the World WideWeb by the Indiana UniversitySchool of Medicine’s Division ofClinical Pharmacology.5
RESULTS
A number of drugs used in dentalpractice can be involved in adversedrug-drug interactions as sub-
strates, inducers or inhibitors of the CYP450system. This article will discuss the clinical sig-nificance of these interactions.
Interactions involving CYP450 substrates.Benzodiazepines. Alprazolam, diazepam, mida-zolam and triazolam are substrates for CYP3A4,with diazepam being a substrate for CYP2C19 aswell. These drugs possess a wide therapeuticindex, and it is for this reason that they now arethe most widely used oral and injectable anxi-olytic agents in all of dental medicine.14 Whiledrug interactions with benzodiazepines theoreti-
TABLE 2
SOME INDUCERS OF CYTOCHROME P450 ISOENZYMES.
CYP1A2
CYP2C9
CYP2C19
CYP2D6
CYP2E1
CYP3A4
Antibiotic agent: rifampinAnticonvulsant agent: carbamazepineAntidiabetic agent: insulinFoods: chargrilled meatsRecreational drugs: tobacco
Antibiotic agent: rifampinBarbiturates: phenobarbital, secobarbital
Antibiotic agent: rifampinAnticonvulsant agent: carbamazepineHormonal agent: norethindrone
Antibiotic agent: rifampinCorticosteroid: dexamethasone
Antibiotic agent: isoniazidRecreational drugs: ethanol, tobacco
Antibiotic agents: rifabutin, rifampinAnticonvulsant agents: carbamazepine, phenytoinBarbiturates: phenobarbital, secobarbitalCorticosteroids: dexamethasone, hydrocortisone, prednisolone,methylprednisoloneHerbal remedy: St. John’s wortHIV antiviral agents: efavirenz, nevirapineOral hypoglycemic agents: pioglitazone, troglitazone
ISOENZYME INDUCER
Enzyme inhibitorsreduce the activity ofa specific cytochrome
P450 isoform,resulting in an
accumulation of thesubstrate drug.
Copyright ©2004 American Dental Association. All rights reserved.
on March 20, 2010
jada.ada.orgD
ownloaded from

JADA, Vol. 135, March 2004 301
C L I N I C A L P H A R M A C O L O G Y
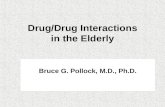
cally can involve inducers and inhibitors of thesespecific CYP450 isoforms, those involvinginhibitors of CYP3A4 are of most concern to theclinician. Like most interactions involving theCYP450 system, interactions involving benzodi-azepines are more likely to occur with the oraladministration of these drugs. These particulardrug interactions have been well-documented; theend result is benzodiazepine accumulation andprolonged and excessive sedation.15,16 Themacrolide antibiotics erythromycin and clar-ithromycin, which are used widely in dentistry,are potent inhibitors of CYP3A4. In one placebo-controlled study,17 erythromycin at 500 mil-ligrams three times per day for six days increasedpeak blood levels of a single dose of oral mida-zolam almost threefold (Figure 1). In addition,drowsiness and other indicators of psychomotorimpairment were far more intense in patientstaking erythromycin for six days than in thosetaking a placebo.17 Even a single dose of eryth-romycin taken concomitantly with oral mida-
zolam has been reported to increase the sedativeeffects of the benzodiazepine.18 By their ability toinhibit CYP3A4, azole antifungal drugs,4,19-21 pro-tease inhibitors (Figure 2),6,16,22 the selective sero-tonin reuptake blocker fluvoxamine and the serotonin-2 receptor antagonist nefezadone (bothantidepressants)23 and grapefruit juice24,25 all havebeen shown to significantly increase blood levels,elimination half-lives and the sedative andpsychomotor impairment effects of diazepam,alprazolam, midazolam and triazolam.
Narcotic analgesics. Codeine and tramadol aresubstrates for CYP2D6. They can be prescribedfor the control of postoperative pain as singleentities or in combination with aspirin (codeine)or acetaminophen (both codeine and tramadol). Inthe outpatient dental setting, combining mini-mally effective doses of these agents (60 mg ofcodeine or 75 mg of tramadol) with optimal ornear-optimal doses of aspirin or acetaminophen(600-1,000 mg) usually will provide better anal-gesia with fewer side effects than will simply
TABLE 3
SOME INHIBITORS OF CYTOCHROME P450 ISOENZYMES.
CYP1A2
CYP2C9
CYP2C19
CYP2D6
CYP2E1
CYP3A4
Antibiotic agents: ciprofloxacin, enoxacin, erythromycin, ofloxacinAntidepressant agent: fluvoxamineAntiplatelet agent: ticlopidineH2 receptor blocker: cimetidine
Antibiotic agents: isoniazid, metronidazole, sulfamethoxazole, trimethoprimAntidepressant agents: fluvoxamine, paroxetine, sertralineAntidysrhythmic agent: amiodaroneAntifungal agents: fluconazole, miconazole
Anticonvulsant agent: felbamateAntidepressant agents: fluoxetine, fluvoxamine, paroxetineAntifungal agent: ketoconazoleAntiplatelet agent: ticlopidineProton pump inhibitors: lansoprazole, omeprazole
Antidepressant agents: fluoxetine, paroxetine, sertralineAntidysrhythmic agents: amiodarone, quinidineH1 receptor blockers: chlorpheniramine, hydroxyzine, promethazineH2 receptor blockers: cimetidine, ranitidineNSAID*: celecoxibRecreational drug: cocaine
Alcoholism rehabilitation drug: disulfiram
Antibiotic agents: ciprofloxacin, clarithromycin, erythromycin, norfloxacinAntidepressant agents: fluvoxamine, nefazodoneAntidysrhythmic agent: amiodaroneAntifungal agents: fluconazole, itraconazole, ketoconazoleCalcium-channel blockers: diltiazem, verapamilFood product: grapefruit juiceH2 receptor blocker: cimetidineHIV protease inhibitors: idinavir, nelfinivir, ritonavir, saquinavir
* NSAID: Nonsteroidal anti-inflammatory drug.
ISOENZYME INHIBITOR
Copyright ©2004 American Dental Association. All rights reserved.
on March 20, 2010
jada.ada.orgD
ownloaded from

302 JADA, Vol. 135, March 2004
C L I N I C A L P H A R M A C O L O G Y
administering a higher dose of the narcoticalone.26,27 Both agents are prodrugs; that is, theparent compound is essentially devoid of anal-gesic activity but the active demethylatedmetabolites—morphine in the case of codeine andO-demethyl tramadol in the case of tramadol—are responsible for the analgesic activity.28,29 TheCYP450 isoform responsible for this conversion isCYP2D6 (Figure 3). It has been demonstratedwith both drugs that the administration of theantidysrhythymic agent quinidine, a knownCYP2D6 inhibitor, essentially abolishes theiranalgesic activity.28,30 Other widely prescribedCYP2D6 inhibitors—including antidepressantagents of the selective serotonin reuptakeinhibitor class (fluoxetine, paroxetine and sertra-line) and the cyclo-oxygenase-, or COX-, 2–selective nonsteroidal anti-inflammatory drug, orNSAID, celecoxib—have the theoretical potentialto diminish the analgesic effects of both codeineand tramadol. The clinical significance of theseinteractions needs to be explored.
One other intriguing discovery with importantclinical implications is that CYP2D6 exhibits a
high degree of genetic polymorphism.28,30 From aclinical perspective, this means that there arepatients in the population who either poorly orextensively metabolize CYP2D6 substrates. Withprodrugs like codeine and tramadol, people whometabolize them poorly exhibit little analgesicactivity with the intake of these drugs becausethey do not form the necessary active metabolites,while people who metabolize them extensivelyreadily form the active metabolites and exhibitsignificant analgesia.28 Up to 10 percent of thewhite population are thought to metabolizeCYP2D6 substrates poorly.5 While this issue isoutside the scope of clinical practice, it is possiblethat in the future, a simple blood test for CYP2D6activity could be used to predict a patient’s likelyresponse to either agent.
Lidocaine. Lidocaine, the most frequently usedlocal anesthetic in all of dentistry, is a substratefor both CYP2D6 and CYP3A4.5 Because twoCYP450 isoforms control the drug’s metabolism,dramatic increases in lidocaine blood levels areunlikely to occur by the inhibition of a single isoform (for example, inhibition of CYP3A4 by
200
180
160
140
120
100
80
60
40
20
0Placebo Erythromycin
DOSE
PEA
K M
IDA
ZO
LA
M C
ON
CEN
TR
AT
ION
(ng/m
L)
N = 12
(P = .003)
Figure 1. Effects of placebo or erythromycin 500 mil-ligrams taken three times per day for six days on peakplasma levels (mean ± standard error) of a single oraldose of midazolam 15 mg. Blood levels of midazolamwere approximately threefold higher in the erythromycingroup (P = .003). Data adapted from Olkkola and col-leagues.17 ng/mL: Nanograms per milliliter.
40
35
30
25
20
15
10
5
0Placebo Ritonavir
DOSE A
LP
RA
ZO
LA
M T
(H
OU
RS)
N = 10
(P < .005)
1 2
Figure 2. Effects of placebo or the protease inhibitorritonavir on the half-life of alprazolam. Alprazolam’shalf-life was 13 hours after taking placebo and 30 hoursafter taking ritonavir (P < .005). Data adapted fromGreenblatt and colleagues.22
Copyright ©2004 American Dental Association. All rights reserved.
on March 20, 2010
jada.ada.orgD
ownloaded from

JADA, Vol. 135, March 2004 303
C L I N I C A L P H A R M A C O L O G Y
erythromycin). Four doses of erythromycin ethyl-succinate 600 mg given over two days modestlyincreased the half-life of an intravenous lidocaineinfusion from 2.2 to 2.8 hours.31 Of interest topediatric dentists, who frequently use antihis-tamines in sedative premedication regimens, theCYP2D6 inhibitors diphenhydramine and chlor-pheniramine impaired lidocaine metabolism inrodent hepatocytes.32 However, the ability of clas-sical antihistamines to increase blood levels of asingle dose of lidocaine after adental injection never has beendemonstrated in humans. In addi-tion, computer-simulated plasmaconcentration curves after theinjection of a single cartridge of 2percent lidocaine plus 1:100,000epinephrine revealed that even adoubling of lidocaine’s half-lifeincreased plasma concentrations byonly 9 percent.16 The most impor-tant ways to avoid local anesthetictoxicity in the outpatient dentalsetting are to use good aspiratingtechniques and to adhere strictly tomaximum recommended dosage guidelines.33,34
NSAIDs. The NSAIDs celecoxib, diclofenac,ibuprofen and naproxen are all substrates ofCYP2C9. As a group, NSAIDs are generally effi-cacious and well-tolerated for the short-termtreatment of postsurgical dental pain.35,36 As pre-viously described for the CYP2D6 substratescodeine and tramadol, there is a growing interestin genetic polymorphisms of CYP2C9.37-39 How-ever, because these NSAIDs are not prodrugs,people who metabolize them poorly would bemore prone to active drug accumulation and toxi-city (renal and gastrointestinal) with chronicdosing than would those who metabolize themextensively.37 Theoretically, drugs that areinhibitors of CYP2C9 (Table 3) also could impairthe metabolism and subsequent elimination ofthese four NSAIDs, leading to drug accumulation
and an increased likelihood of toxicity. However,it appears that other CYP450 isoforms also play arole in NSAID metabolism,38-40 so that inhibitorsof the single CYP2C9 isoform should not causedramatic increases in blood levels or half-lives ofthese NSAIDs, especially after short-term dosingfor acute pain.
Acetaminophen. Acetaminophen is the mostwidely sold over-the-counter, or OTC, analgesic-antipyretic agent in the United States.41 In addi-
tion to OTC sales, the number ofprescriptions dispensed in 2002 foracetaminophen-narcotic combina-tion drugs containing hydrocodone,codeine, propoxyphene and oxy-codone were ranked first, 32nd, 37thand 86th, respectively, of all pre-scribed medications in the UnitedStates.42 When used for the short-term treatment of pain or feveraccording to package insert guide-lines (maximum adult dose of 4grams per day), acetaminophenprobably is the safest of all the non-prescription analgesic agents.36,43
However, acute overdoses of acetaminophen—typically, 15 g or more in an adult—frequentlyresult in hepatotoxicity.36,44 In addition, multipleexcessive dose miscalculations administered tofebrile pediatric patients by their parents alsohave led to severe hepatotoxicity.45 In the case ofoverdose, an electrophilic toxic metabolite N-acetyl-p-benzoquinoneimine, or NAPQI, accumu-lates, resulting in hepatic cell death.44
When therapeutic doses of acetaminophen areconsumed, approximately 96 percent undergoesconjugation in the liver via the addition of a sul-fate or glucuronic acid group leading to the forma-tion of inactive-nontoxic metabolites (Figure 4).Via CYP2E1, the remaining 4 percent is con-verted to the highly reactive hepatotoxic metabo-lite NAPQI.44,46 However, this compound rapidlycombines with glutathione stores in the liver and
N-CH3 N-CH3
CH3O O OHOCodeine Morphine
CYP2D6
Tramadol O-Demethyl TramadolCH3O HO
OHOHCYP2D6
CH3 CH3
CH2
N
CH3 CH3
CH2
N
Figure 3. The demethylation of selected prodrugs to the active metabolites morphine and O-demethyl tramadol byCYP2D6. A. Codeine. B. Tramadol.
The ability of classicalantihistamines to
increase blood levelsof a single dose oflidocaine after adental injection never has beendemonstrated in
humans.
A B
Copyright ©2004 American Dental Association. All rights reserved.
on March 20, 2010
jada.ada.orgD
ownloaded from

essentially is rendered harmless.46 In the case of amassive acetaminophen overdose, the excessiveproduction of NAPQI overwhelms the hepatic glu-tathione stores, resulting in alkylation of hepaticproteins and irreversible cellular damage unlessthe antidote N-acetylcysteine is administeredwithin the first 16 hours (before symptoms of theoverdose become clinically evident).36,44
Since CYP2E1 is an inducible enzyme, therehas been great concern over the possibility thatdrugs that are inducers of this enzyme, particu-larly ethanol, could promote the conversion ofacetaminophen to NAPQI, even in patients takingtherapeutic doses of the analgesic.46 An evengreater concern regarding acetaminophen hepato-toxicity has been voiced for patients with alco-holism. The thought is that not only couldCYP2E1 be induced in these patients, but alsoglutathione, which normally inactivates NAPQI,is known to be depleted in patients with alco-holism, further increasing the likelihood ofserious hepatotoxicity.36,46,47 Current U.S. Foodand Drug Administration-, or FDA-, approvedlabeling of OTC acetaminophen products reflectsthis concern; stating that “patients who consumethree or more alcoholic drinks per day should con-tact their physician before ingestingacetaminophen, because the combination mayincrease the risk of liver damage.”48 In addition,published recommendations limit the maximumdaily dose of acetaminophen to only 2 g inpatients with alcoholism to avoid additional liverdamage that is already present due to alcohol
304 JADA, Vol. 135, March 2004
C L I N I C A L P H A R M A C O L O G Y
abuse.47 Surprisingly, even with the restrictivelabeling and dosing of acetaminophen in combina-tion with alcohol, the interaction is not well-supported by scientific research.
As shown in Tables 1 and 2, ethanol can act asboth a substrate and an inducer of CYP2E1.5,44
Below blood levels of 250 milligrams per deciliter,ethanol preferentially occupies CYP2E1 overother substrates, resulting in the formation ofethanol metabolites while limiting its associa-tion with other substrates, including acetamino-phen.44,46,49 At concentrations greater than 250mg/dL, there also appears to be some de novo syn-thesis of CYP2E1, but experimental and com-puter models have revealed that even when maxi-mally induced, the production of NAPQI fromacetaminophen is increased only twofold.44 It hasbeen estimated that approximately 0.635 g ofNAPQI must be produced in a 150-pound adult toreach the threshold of liver toxicity. This is basedon the facts that approximately 4 percent of agiven acetaminophen dose is converted to NAPQIand an acute intake of 15.9 g of acetaminophen isneeded to reach the threshold of liver toxicity(0.04 × 15.9 g acetaminophen = 0.635 g NAPQI).44,50
If one extrapolates these calculations to a patientconsuming a full 1-g therapeutic dose ofacetaminophen, and having a high blood alcohollevel, the maximum concentration of NAPQIformed would only be 0.080 g (2 × 0.04 × 1 g), orapproximately eightfold less than needed to reachthe threshold of hepatotoxicity.
The simultaneous ingestion of alcohol has been shown to exert a hepatoprotective effect in patients taking massive overdoses ofacetaminophen.44,46,51 In one such case, a patientingested what usually is a lethal dose of 60 g ofacetaminophen after 48 hours of heavy drinkingof alcohol—and survived with little evidence ofhepatotoxicity.52 In this situation, alcohol prob-ably occupied a large proportion of the hepaticCYP2E1, limiting the association ofacetaminophen with the enzyme and the subse-quent production of NAPQI.36,46,49
With regard to patients with alcoholism takingtherapeutic doses of acetaminophen, a review ofmore than 2,000 reports revealed that Class I(controlled, randomized, blinded clinical trials)and Class II (prospective nonrandomized or non-blinded trials or well-designed case-controlstudies) data demonstrated little toxicity with thecombination.44,53 On the other hand, some ClassIII data relying exclusively on patient recall (ret-
Conjugated Metabolite N-acetyl-p-benzoquinoneimine(NAPQI)
Acetaminophen
Glutathione
CYP2E1 (4%)Glucuronidation
or Sulfation(96%)
NHCOCH3
NHCOCH3 NHCOCH3O
HO
RO
Figure 4. Metabolic fate of acetaminophen. The vastmajority of acetaminophen undergoes conjugation toinactive, nontoxic metabolites; “R” represents glucuronicacid or sulfate. Approximately 4 percent of the parentcompound is converted to the hepatotoxic metabolite N-acetyl-p-benzoquinoneimine which at therapeutic dosesof acetaminophen rapidly combines with glutathionestores in the liver and is inactivated.
Copyright ©2004 American Dental Association. All rights reserved.
on March 20, 2010
jada.ada.orgD
ownloaded from

rospective case series, single case studies) sug-gested that “a morbid fate awaits some alcoholicpatients who ingest a therapeutic dose ofacetaminophen.”44 Thus, we are left with con-flicting results: well-designed reports suggestinglittle concern regarding using therapeutic doses ofacetaminophen in these patients, and purely ret-rospective cases suggesting a high likelihood oftoxicity. It appears that some patients with alco-holism who ingest massive overdoses ofacetaminophen (median dose of 54 g) may be atgreater risk of experiencing death than nonalco-holic patients who ingest similar amounts ofacetaminophen. The patient with chronic alco-holism may have decreased synthetic rates of aprotein transporter that moves glutathione fromthe hepatic cytosol into the mito-chondria. Since the mitochondriaare targeted by NAPQI, this mayexplain the increased toxicity of anacetaminophen overdose in thepatient with alcoholism.44 The FDAcontinues to hold hearings on theissue of alcohol and acetaminopheninteractions; it can be hoped thatfuture revisions to its acetamino-phen monograph (and, in fact, themonographs for all OTC analgesicagents with respect to alcohol con-sumption) will be based on evidenceand not solely on the results ofunsubstantiated case reports.54
Corticosteroids. Corticosteroidssuch as dexamethasone and methylprednisoloneare potent anti-inflammatory and immunosup-pressant agents. They frequently are used for ahost of chronic inflammatory and autoimmunediseases, including asthma, ulcerative colitis andlupus erythematosus and, in combination withother immunosuppressant agents, in the preven-tion of organ transplant rejection.55 In dentistry,therapeutic uses of glucocorticoids include thereduction of swelling after oral surgery proce-dures, the treatment of temporomandibular jointsyndrome symptoms (often by localized injection),the topical treatment of various oral-mucosallesions and as “stress steroids” in patients whosehypothalamic-pituitary-adrenal axis is sup-pressed.55 The actions of corticosteroids on theCYP450 system are complex, and various drugs ofthe class can act as both substrates and inducersof CYP3A4 isoform5,56 (Tables 1 and 2). Asinducers of CYP3A4, these agents could be pre-
JADA, Vol. 135, March 2004 305
C L I N I C A L P H A R M A C O L O G Y
dicted to be involved in numerous adverse druginteractions,57 in which their concomitant admin-istration would significantly reduce blood levels ofmany CYP3A4 substrates. However, this predic-tion has not been borne out in clinical studies.56,57
More important from a clinical perspective isthat because corticosteroids are substrates ofCYP3A4, their blood levels could become elevatedand their half-lives significantly increased whenan inhibitor of this enzyme is administered con-comitantly. This, in turn, would lead to anincreased potential for corticosteroid toxicity,including unwanted immunosuppression, sup-pression of the hypothalamic-pituitary-adrenalaxis and hyperglycemia. The corticosteroid thatseems most prone to these interactions is methyl-
prednisolone,58-64 an agent fre-quently administered in a six-day,21-dose regimen (a dose-pack) toreduce postoperative swelling afterdental impaction surgery.CYP3A4-inhibitor drugs that havebeen documented to cause theaccumulation of methylpred-nisolone include the macrolideantibiotic drugs erythromycin andclarithromycin,58,59 the azole anti-fungal drugs itraconazole and keto-conazole,60,61 the calcium-channel–blocking agents diltiazemand mibefradil62,63 and 200 mL ofdouble-strength grapefruit juice.64
It is likely that other CYP3A4inhibitors also could interact adversely withmethylprednisolone. Clinicians should be awareof these potential interactions and advise patientsto avoid the ingestion of grapefruit juice duringtheir course of methylprednisolone therapy andfor at least three days afterward.
Interactions involving CYP450 inducers.Barbiturates. Derivatives of barbituric acid,including phenobarbital and secobarbital, oncewere important drugs in oral sedation techniquesused with anxious dental patients. However,because of their low therapeutic index, high abusepotential, disruptions of rapid-eye-movement–stage sleep and the potential for numerous druginteractions, they have been replaced largely bybenzodiazepines.14,65 Barbiturates are known toinduce various isoforms of the CYP450 systems,including CYP2C9 and CYP3A4, leading to adecrease in blood levels of a number of drugs.This has been documented for the antidys-
Some patients withalcoholism who ingestmassive overdoses ofacetaminophen maybe at greater risk ofexperiencing deaththan nonalcoholic
patients who ingestsimilar amounts of
acetaminophen.
Copyright ©2004 American Dental Association. All rights reserved.
on March 20, 2010
jada.ada.orgD
ownloaded from

rhythmic agent quinidine, azole antifungalagents, nifedipine and other calcium-channelblockers, the cancer chemotherapeutic agentetoposide, oral contraceptive agents containingestradiol and progesterone, the immunosuppres-sant agents cyclosporine and tacrolimus, variousHIV protease inhibitors, methadone and war-farin, among others.2,3,66 Acute (single-dose) barbi-turate therapy that typically was used in dentalsedative techniques probably was only rarelyinvolved in adverse drug interactions involvingthe induction of the CYP450 system, becauseinduction typically takes at least several days ofbarbiturate use.2 Longer-term therapy, such assometimes used for temporomandibular joint dys-function and headache,67 indeedcould cause blood levels of thesedrugs to fall below therapeuticlevels. For example, a patienttaking cyclosporine or tacrolimusbecause of an organ transplant the-oretically could experience acuterejection of that organ. Likewise, apatient taking oral contraceptivescould begin ovulating and becomepregnant while receiving barbitu-rate therapy. To avoid drug inter-actions of this type, clinicians also are cautionedto recognize brand-name drugs with “hidden” bar-biturate components such as the popularmigraine drug Fiorinal (Novartis Pharmaceuti-cals, East Hanover, N.J.), which contains 325 mgof aspirin plus 50 mg of the barbiturate butal-bital.
Interactions involving CYP450 inhibitors.Interestingly, the agents used in dental practicethat can act as inhibitors of various CYP450 iso-forms all are antimicrobial agents. Antimicrobialagents are dosed on a more chronic basis than areother therapeutic agents (such as local anesthetic,analgesic and anxiolytic agents) routinely used indentistry, which enhances the likelihood of clini-cally significant CYP450 inhibition and the asso-ciated drug interactions with CYP450 sub-strates.15 These interactions as a whole can beextremely serious and potentially life-threateningif the substrate drug whose metabolism is beinginhibited has a low margin of safety or whatpharmacologists call a “low therapeutic index.”1,15
Quinolone antibiotic agents. Members of thequinolone class include ciprofloxacin, enoxacin,norfloxacin and ofloxacin. Of these agents, theuse of systemic ciprofloxacin (typically at a dose of
306 JADA, Vol. 135, March 2004
C L I N I C A L P H A R M A C O L O G Y
500 mg twice per day for 10 days) is becomingincreasingly popular in the treatment of refrac-tory periodontal infections that harbor Acti-nobacillus actinomycetemcomitans and othergram-negative, facultatively anaerobic rods.68-70
Ciprofloxacin is a potent inhibitor of CYP1A2 andalso produces some inhibition of CYP3A4. Themost clinically significant interaction involvingciprofloxacin is its ability to inhibit themetabolism of the CYP1A2 substrate theo-phylline.71,72 While increases in theophylline bloodconcentrations and half-life average only about 20to 30 percent, the drug has a rather low thera-peutic index. Cardiac dysrhythmias and convul-sions are the most serious consequence of exces-
sive blood levels of theophylline.It has been reported that a reg-
imen of ciprofloxacin 250 mg takentwice per day for seven daysincreased average plasma concen-trations of the atypical antipsy-chotic agent clozapine (a CYP1A2substrate) by approximately 30 per-cent.73 In one patient, a regimen ofciprofloxacin 500 mg twice per dayincreased plasma concentrations ofclozapine by 80 percent.74 Elevated
plasma clozapine levels increase the risk ofoversedation, urinary retention, constipation andseizures in a patient population in which noncom-pliance with schizophrenic medication regimensalready is the norm because of the nature of thedisease and the unwanted side effects associatedwith this class of drugs.75
Metronidazole. Metronidazole is highly effec-tive against obligate anaerobic bacteria associ-ated with periodontal disease, periapicalabscesses and peri-implantitis.76-79 Because it hasno activity against facultative anaerobic bacteria,which can be part of a mixed flora inhabitingthese infected sites, metronidazole frequently is combined with a penicillin or with ciproflox-acin.76-78 With respect to drug interactions,metronidazole is best known for its interactionwith alcohol. This combination can result in adisulfiram-like reaction, which tends to be morefrightening than serious, with patients experi-encing nausea, vomiting, headache and cardiacpalpitations.15 These symptoms are best explainedby metronidazole’s ability to block a key enzymein alcohol metabolism, namely acetaldehydedehydrogenase, causing acetaldehyde to accumu-late in the bloodstream after alcohol consumption.
Clinicians are cautioned to
recognize brand-name drugs
with ‘hidden’ barbiturate
components.
Copyright ©2004 American Dental Association. All rights reserved.
on March 20, 2010
jada.ada.orgD
ownloaded from

This adverse drug interaction, however, appearsto be unrelated to the inhibition of CYP450enzymes.
Metronidazole also may be involved in otherdrug interactions that relate to its ability toinhibit CYP2C9 (Table 3). While a number of sub-strates are metabolized by this isoenzyme, theinteraction that appears best documented is theability of metronidazole to significantly increasethe blood concentrations, half-life and the associ-ated hemorrhagic potential of the anticoagulantagent warfarin.80,81 In addition, metronidazole’sability to cause the accumulation of theantiepileptic drug and CYP2C9 substrate pheny-toin is supported by at least one well-designedclinical trial.82 Excessive phenytoin levels in theblood increase the risk of drowsi-ness, confusion, diplopia, ataxiaand nystagmus.83 Before pre-scribing metronidazole to a dentalpatient who is receiving chronicwarfarin or phenytoin therapy, den-tists are advised to consult with thepatient’s prescribing physician.
Macrolide antibiotic agents. His-torically, erythromycin was consid-ered to be the antibiotic agent ofchoice for patients with penicillinallergies who had odontogenicinfections.84 However, because of ahigh incidence of gastrointestinal complaints,increasing bacterial resistance problems and onlymoderate activity against anerobic bacteria, itsuse has been decreasing. Clarithromycin isbetter-tolerated than erythromycin; possessesbetter activity against most streptococcal, staphy-lococcal and anaerobic bacterial species; and,while more expensive than erythromycin, mayresult in better patient compliance because it hasto be taken only twice per day.78,84 Like clar-ithromycin, azithromycin has excellent activityagainst anaerobes, possesses an extended half-life(requiring only once-per-day dosing) and is analternative to amoxicillin in patients requiringendocarditis-related prophylaxis who are allergicto penicillins.85 For this indication, both drugs aredosed at 500 mg one hour before the dental procedure.
Erythromycin and clarithromycin are potentinhibitors of CYP3A4 and are associated withnumerous untoward drug interactions,2,3,5,8,15 whileazithromycin is not.5,86-88 This difference betweenthe macrolides probably is structurally related.
JADA, Vol. 135, March 2004 307
C L I N I C A L P H A R M A C O L O G Y
Erythromycin and clarithromycin possess 14carbon atoms surrounding their macrocyclic lac-tone rings, while azithromycin contains 15 ofthese constituents.89 The primary reason for thevast number of potential drug interactions withCYP3A4 inhibitors is the fact that CYP3A4 hasbroad substrate specificity and has been esti-mated to contribute to the metabolism of morethan 50 percent of all available therapeuticagents.57 Since the pharmacokinetic consequencesof all these interactions is an accumulation of thesubstrate drug, side effects of the substrate drug,including relatively rare side effects, become morecommon and more intense. Typically, the morechronic the dosing with the substrate and theinhibitor, the greater the chance for a clinically
significant drug interaction. How-ever, if the substrate undergoes sig-nificant (greater than 60 percent)CYP3A4 metabolism in the gut andthe liver before reaching the sys-temic circulation, the likelihood of asignificant drug interactionincreases, even with just one or twodoses of the substrate drug.8 Exam-ples of CYP3A4 substrates with rel-atively low oral bioavailabilityinclude terfenadine, astemizole,simvastatin, lovastatin, felodipineand midazolam.
The ability of erythromycin and clarithromycinto inhibit the CYP3A4-directed metabolism of cer-tain benzodiazepines15-18 and methylpredniso-lone58,59 already has been discussed. Table 4 sum-marizes some additional interactions betweenCYP3A4 substrates and antimicrobial CYP3A4inhibitors used in dentistry.86,90-138 Some of thesesubstrates—including the nonsedating antihis-tamine agents terfenadine and astemizole, theprokinetic agent (gastroesophageal reflux drug)cisapride and the lipid-lowering drug ceriva-statin—have been removed from the U.S. marketby the FDA, partly because of an unacceptablyhigh incidence of usually rare life-threateningtoxicities (torsades de pointes with terfenadine,astemizole and cisapride and rhabdomyolysiswith cerivastatin) when administered concomi-tantly with CYP3A4 inhibitors.
Azole antifungal drugs. This group of anti-fungal agents blocks the fungal CYP450-directedsynthesis of the cell membrane component ergos-terol in sensitive organisms.139 Unfortunately, thismechanism of action leads to inhibition of human
Metronidazole cansignificantly increase
the blood concentrations,
half-life and the associated
hemorrhagic potentialof the anticoagulant
agent warfarin.
Copyright ©2004 American Dental Association. All rights reserved.
on March 20, 2010
jada.ada.orgD
ownloaded from

308 JADA, Vol. 135, March 2004
C L I N I C A L P H A R M A C O L O G Y
CYP450 isoforms, especially CYP3A4. Of thisgroup, ketoconazole and itraconazole are associ-ated with by far the greatest incidence of adversedrug interactions, resulting in the accumulationand subsequent toxicity of a number of CYP3A4
substrates (Table 4). Fortunately, these drugs arerarely, if ever, used in outpatient dentistry. How-ever, caution still is advised when administeringfluconazole or clotrimazole to treat oral candidi-asis in patients taking CYP3A4 substrates.
TABLE 4
SOME ADVERSE DRUG:DRUG INTERACTIONS INVOLVING ERYTHROMYCIN, CLARITHROMYCIN, KETOCONAZOLE AND ITRACONAZOLE WITH CYP3A4 SUBSTRATES.
Astemizole, Cisapride,Pimozide, Terfenadine
Atorvastatin,Cerivastatin, Lovastatin, Simvastatin
Felodipine,Nifedipine
Cyclosporine,Tacrolimus
Warfarin
Carbamazepine
Theophylline
Substrate accumulation leading tocardiac QT interval prolongationand torsades de pointes ventric-ular tachycardia86, 90-100
Substrate accumulation leading todiffuse myalgias, rhabdomyolysisand renal failure101-106
Substrate accumulation leading to severe hypotension and edema109-111
Substrate accumulation leading toenhanced immunosuppression andnephrotoxicity112-116
Substrate accumulation leading toincreased prothrombin times,international normalized ratiosand increased risk of seriousbleeding119-123
Substrate accumulation leading toincreased risk of ataxia, vertigo,drowsiness and confusion125-130
Substrate accumulation leading toincreased risk of tremors, cardiacdysrhythmias and seizures133-138
Torsades de pointes is a life-threateningventricular dysrhythmia that occurs in thesetting of electrocardiographic QT intervalprolongation. While terfenadine, astemi-zole and cisapride no longer are availablein the United States, pimozide still is usedin the treatment of psychotic disorders andis especially effective in the managementof Gilles de la Tourette’s syndrome.100
The “statin” drugs inhibit the rate-limitingstep (3-hydroxy-3-methyl-glutaryl coen-zyme A, or HMG-CoA, reductase) incholesterol biosynthesis and are usedwidely for this purpose.42 Rhabdomyolysisis a potentially life-threatening breakdownof skeletal muscle, resulting in the releaseof myoglobin into the serum and urine andgiving the urine a brown-rust color. Themyoglobin can cause blockage of the renaltubular system, resulting in kidneydamage and acute renal failure.107
Recently, a single case of a possible fluconazole-simvastatin interaction wasreported.108
This interaction is an extension of theantihypertensive effects of the substrates.Other calcium-channel blockers also maybe predisposed to the interaction.
This interaction has been used therapeuti-cally to reduce the cost of immunosuppres-sant therapy.117 Clotrimazole, in the formof troches—frequently used in the treat-ment of oral candidiasis—also significantlyincreases tacrolimus blood levels.118
Fluconazole also increases warfarin bloodlevels via an inhibition of warfarin’sCYP2C9 metabolism.124
Two cases of a possible fluconazole-carbamazepine interaction have beenreported.131,132
This interaction appears to involve onlyerythromycin, possibly owing to its abilityto inhibit CYP1A2, of which theophyllineis a substrate.2,138
* The use of alternative antibiotics (penicillin, tetracycline, azithromycin or clindamycin) or antifungals (topical nystatin or amphotericin B) that are appropriate for the specific infection is advised when patients are taking these CYP3A4 substrates.
CYP3A4 SUBSTRATES POTENTIAL INTERACTION COMMENTS*
Copyright ©2004 American Dental Association. All rights reserved.
on March 20, 2010
jada.ada.orgD
ownloaded from

JADA, Vol. 135, March 2004 309
C L I N I C A L P H A R M A C O L O G Y
Potentially serious interactions have beenreported when these agents are administered topatients taking simvastatin, tacrolimus, warfarinor carbamazepine.108,118,124,131,132
CONCLUSIONS
The CYP450 system is responsible for themetabolism of a multitude of diverse pharmaco-logical agents. Drugs routinely used in dentistryoften serve as substrates or inhibitors of thissystem. Dentists can avoid untoward drug inter-actions in their practices by gaining an under-standing of the CYP450 substrates, inducers andinhibitors. ■
Dr. Hersh is a professor of oral surgery and pharmacology and asso-ciate dean of clinical research, University of Pennsylvania School ofDental Medicine, Philadelphia, Pa. 19104-6030, e-mail “[email protected]”. Address reprint requests to Dr. Hersh.
Dr. Moore is a professor of pharmacology and dental public health,University of Pittsburgh School of Dental Medicine, Pittsburgh.
1. Moore PA, Gage TW, Hersh EV, Yagiela JA, Haas DA. Adversedrug interactions in dental practice: professional and educationalimplications. JADA 1999;130:47-54.
2. Michalets EL. Update: clinically significant cytochrome P-450 druginteractions. Pharmacotherapy 1998;18:84-112.
3. Cupp MJ, Tracy TS. Cytochrome P450: new nomenclature and clin-ical implications. Am Fam Physician 1998;57:107-16.
4. Venkatakrishnan K, von Moltke LL, Greenblatt DJ. Effects of theantifungal agents on oxidative drug metabolism: clinical relevance.Clin Pharmacokinet 2000;38:111-80.
5. Indiana University, School of Medicine, Division of Clinical Phar-macology. Cytochrome P450 drug interaction table. Available at:“medicine.iupui.edu/flockhart/table.htm”. Accessed Aug. 23, 2003.
6. Antoniou T, Tseng AL. Interactions between recreational drugsand antiretroviral agents. Ann Pharmacother 2002;36:1596-613.
7. Piscitelli SC, Burstein AH, Chaitt D, Alfaro RM, Falloon J. Indi-navir concentrations and St. John’s wort. Lancet 2000;355(9203):547-8.
8. Dresser GK, Spence JD, Bailey DG. Pharmacokinetic-pharmacodynamic consequences and clinical relevance of cytochromeP450 3A4 inhibition. Clin Pharmacokinet 2000;38:41-57.
9. Bailey DG, Malcolm J, Arnold O, Spence JD. Grapefruit juice-druginteractions. Br J Clin Pharmacol 1998;46:101-10.
10. Bjornsson TD, Callaghan JT, Einolf HJ, et al. The conduct of invitro and in vivo drug-drug interaction studies: a PhRMA perspective. JClin Pharmacol 2003;43:443-69.
11. Bailey DG, Dresser GK, Bend JR. Bergamottin, lime juice, andred wine as inhibitors of cytochrome P450 3A4 activity: comparisonwith grapefruit juice. Clin Pharmacol Ther 2003;73:529-37.
12. Bailey DG, Spence JD, Munoz C, Arnold JM. Interaction of citrusjuices with felodipine and nifedipine. Lancet 1991;337(8736):268-9.
13. Lown KS, Bailey DG, Fontana RJ, et al. Grapefruit juiceincreases felodipine oral availability in humans by decreasingintestinal CYP3A protein expression. J Clin Invest 1997;99:2545-53.
14. Jackson DL, Johnson BS. Inhalation and enteral conscious seda-tion for the adult dental patient. Dent Clin North Am 2002;46:781-802.
15. Hersh EV. Adverse drug interactions in dental practice: interac-tions involving antibiotics, part II of a series. JADA 1999;130:236-51.
16. Moore PA. Adverse drug interactions in dental practice: interac-tions associated with local anesthetics, sedatives and anxiolytics, partIV of a series. JADA 1999;130:541-54.
17. Olkkola KT, Aranko K, Luurila H, et al. A potentially hazardousinteraction between erythromycin and midazolam. Clin PharmacolTher 1993;53:298-305.
18. Mattila MJ, Idanpaan-Heikkila JJ, Tornwall M, Vanakoski J.Oral single doses of erythromycin and roxithromycin may increase theeffects of midazolam on human performance. Pharmacol Toxicol1993;73:180-5.
19. Yasui N, Kondo T, Otani K, et al. Effect of itraconazole on thesingle oral dose pharmacokinetics and pharmacodynamics of alpra-zolam. Psychopharmacology (Berl) 1998;139:269-73.
20. Olkkola KT, Backman JT, Neuvonen PJ. Midazolam should beavoided in patients receiving the systemic antimycotics ketoconazole oritraconazole. Clin Pharmacol Ther 1994;55:481-5.
21. Varhe A, Olkkola KT, Neuvonen PJ. Oral triazolam is potentiallyhazardous to patients receiving systemic antimycotics ketoconazole oritraconazole. Clin Pharmacol Ther 1994;56:601-7.
22. Greenblatt DJ, von Moltke LL, Harmatz JS, et al. Alprazolam-ritonavir interaction: implications for product labeling. Clin PharmacolTher 2000; 67;335-41.
23. von Moltke LL, Greenblatt DJ, Harmatz JS, et al. Triazolam bio-transformation by human liver microsomes in vitro: effects of metabolicinhibitors and clinical confirmation of a predicted interaction withketoconazole. J Pharmacol Exp Ther 1996;276:370-9.
24. Goho C. Oral midazolam-grapefruit juice drug interaction.Pediatr Dent 2001;23:365-6.
25. Ozdemir M, Aktan Y, Boydag BS, Cingi MI, Musmul A. Interac-tion between grapefruit juice and diazepam in humans. Eur J DrugMetab Pharmacokinet 1998;23:55-9.
26. Beaver WT. Aspirin and acetaminophen as constituents of anal-gesic combinations. Arch Intern Med 1981;141:293-300.
27. McQuay H, Edwards J. Meta-analysis of single dose oral tramadolplus acetaminophen in acute postoperative pain. Eur J Anaesthesiol2003;20(supplement 28):19-22.
28. Desmeules J, Gascon MP, Dayer P, Magistris M. Impact of envi-ronmental and genetic factors on codeine analgesia. Eur J Clin Phar-macol 1991;41:23-6.
29. Lee CR, McTavish D, Sorkin EM. Tramadol: a preliminary reviewof its pharmacodynamic and pharmacokinetic properties, and thera-peutic potential in acute and chronic pain states. Drugs 1993;46:313-40.
30. Garrido MJ, Sayar O, Segura C, et al. Pharmacokinetic/pharmacodynamic modeling of the antinociceptive effects of (+)-tramadol in the rat: role of cytochrome P450 2D activity. J Phar-macol Exp Ther 2003;305:710-8.
31. Orlando R, Piccoli P, De Martin S, Padrini R, Palatini P. Effect ofthe CYP3A4 inhibitor erythromycin on the pharmacokinetics of ligno-caine and its pharmacologically active metabolites in subjects withnormal and impaired liver function. Br J Clin Pharmacol 2003;55:86-93.
32. Hiroi T, Ohishi N, Imaoka S, Yabusaki Y, Fukui H, Funae Y.Mepyramine, a histamine H1 receptor antagonist, inhibits themetabolic activity of rat and human P450 2D forms. J Pharmacol ExpTher 1995;272:939-44.
33. Hersh EV, Helpin ML, Evans OB. Local anesthetic mortality:report of case. ASDC J Dent Child 1991;58:489-91.
34. Moore PA. Preventing local anesthesia toxicity. JADA1992;123:60-4.
35. Cooper SA. New peripherally-acting analgesic agents. Annu RevPharmacol Toxicol 1983;23:617-37.
36. Hersh EV, Moore PA, Ross GL. Over-the-counter analgesics andantipyretics: a critical assessment. Clin Ther 2000;22:500-48.
37. Kirchheiner J, Meineke I, Freytag G, Meisel C, Roots I, Brock-moller J. Enantiospecific effects of cytochrome P450 2C9 amino acidvariants on ibuprofen pharmacokinetics and on the inhibition ofcyclooxygenases 1 and 2. Clin Pharmacol Ther 2002;72:62-75.
38. Brenner SS, Herrlinger C, Dilger K, et al. Influence of age andcytochrome P450 2C9 genotype on the steady-state disposition ofdiclofenac and celecoxib. Clin Pharmacokinet 2003;42:283-92.
39. Kirchheiner J, Meineke I, Steinbach N, Meisel C, Roots I, Brock-moller J. Pharmacokinetics of diclofenac and inhibition of cyclooxyge-nases 1 and 2: no relationship to the CYP2C9 genetic polymorphism inhumans. Br J Clin Pharmacol 2003;55:51-61.
40. Tracy TS, Marra C, Wrighton SA, Gonzalez FJ, Korzekwa KR.Involvement of multiple cytochrome P450 isoforms in naproxen O-demethylation. Eur J Clin Pharmacol 1997;52:293-8.
41. Jones A. Over-the-counter analgesics: a toxicology perspective.Am J Ther 2002;9:245-57.
42. The top 200 prescriptions for 2002 by number of U.S. prescriptionsdispensed. Available at: “www.rxlist.com/top200.htm”. Accessed July 16,2003.
43. Prescott LF. Current status of issues concerning the safety ofover-the-counter analgesics and nonsteroidal anti-inflammatory drugs.In: Rainsford KD, Powanda MC, eds. Safety and efficacy of non-prescription (OTC) analgesics and NSAIDs. Boston: Kluwer; 1998:1-9.
44. Rumack BH. Acetaminophen hepatotoxicity: the first 35 years. JToxicol Clin Toxicol 2002;40:3-20.
Copyright ©2004 American Dental Association. All rights reserved.
on March 20, 2010
jada.ada.orgD
ownloaded from

310 JADA, Vol. 135, March 2004
C L I N I C A L P H A R M A C O L O G Y
45. Rivera-Penera T, Gugig R, Davis J, et al. Outcome ofacetaminophen overdose in pediatric patients and factors contributingto hepatotoxicity. J Pediatr 1997;130:300-4.
46. Haas DA. Adverse drug interactions in dental practice: interac-tions associated with analgesics, part III in a series. JADA1999;130:397-407.
47. Friedlander AH, Marder SR, Pisegna JR, Yagiela JA. Alcoholabuse and dependence: psychopathology, medical management anddental implications. JADA 2003;134:731-40.
48. Over-the-counter drug products containing analgesic/antipyreticactive ingredients for internal use; required alcohol warning; final rule;compliance date. U.S. Food and Drug Administration, Department ofHealth and Human Services. Fed Regist 1999;64(51):13066-7.
49. Slattery JT, Nelson SD, Thummel KE. The complex interactionbetween ethanol and acetaminophen. Clin Pharmacol Ther 1996;60:241-6.
50. Rumack BH, Peterson RG. Acetaminophen overdose: incidence,diagnosis and management in 416 patients. Pediatrics 1978;62(5 pt 2supplement):898-903.
51. Rumack BH, Peterson RC, Koch GG, Amara IA. Acetaminophenoverdose: 662 cases with evaluation of oral acetylcysteine treatment.Arch Intern Med 1981;141(special issue 3):380-5.
52. Lyons L, Studdiford JS, Sommaripa AM. Treatment ofacetaminophen overdosage with N-acetylcysteine. N Engl J Med1997;296:174-5.
53. Dart RC, Kuffner EK, Rumack BH. Treatment of pain of feverwith paracetamol (acetaminophen) in the alcoholic patient: a systemicreview. Am J Ther 2000;7:123-34.
54. U.S. Food and Drug Administration, Center for Drug Evaluationand Research, Nonprescription Drugs Advisory Committee. Safetyissues related to acetaminophen. Available at: “www.fda.gov/ohrms/dockets/ac/02/transcripts/3882T1.htm”. Accessed July 20, 2003.
55. Trummel CL. Antiinflammatory drugs. In: Yagiela JA, Neidle EA,Dowd FJ, eds. Pharmacology and therapeutics for dentistry. 4th ed. St.Louis: Mosby; 1998:297-319.
56. Villikka K, Varis T, Backman JT, Neuvonen PJ, Kivisto KT.Effect of methylprednisolone on CYP3A4-mediated drug metabolism invivo. Eur J Clin Pharmacol 2001;57:457-60.
57. McCune JS, Hawke RL, LeCluyse EL, et al. In vivo and in vitroinduction of human cytochrome P4503A4 by dexamethasone. ClinPharmacol Ther 2000;68:356-66.
58. LaForce CF, Szefler SJ, Miller MF, Ebling W, Brenner M. Inhibi-tion of methylprednisolone elimination in the presence of erythromycintherapy. J Allergy Clin Immunol 1983;72:34-9.
59. Fost DA, Leung DY, Martin RJ, Brown EE, Szefler SJ, Spahn JD.Inhibition of methylprednisolone elimination in the presence of clar-ithromycin therapy. J Allergy Clin Immunol 1999;103:1031-5.
60. Glynn AM, Slaughter RL, Brass C, D’Ambrosio R, Jusko WJ.Effects of ketoconazole on methylprednisolone pharmacokinetics andcortisol secretion. Clin Pharmacol Ther 1986;39:654-9.
61. Varis T, Kaukonen KM, Kivisto KT, Neuvonen PJ. Plasma con-centrations and effects of oral methylprednisolone are considerablyincreased by itraconazole. Clin Pharmacol Ther 1998;64:363-8.
62. Booker BM, Magee MH, Blum RA, Lates CD, Jusko WJ. Pharma-cokinetic and pharmacodynamic interactions between diltiazem andmethylprednisolone in healthy volunteers. Clin Pharmacol Ther2002;72:370-82.
63. Varis T, Backman JT, Kivisto KT, Neuvonen PJ. Diltiazem andmibefradil increase the plasma concentrations and greatly enhance theadrenal-suppressant effect of oral methylprednisolone. Clin PharmacolTher 2000;67:215-21.
64. Varis T, Kivisto KT, Neuvonen PJ. Grapefruit juice can increasethe plasma concentrations of oral methylprednisolone. Eur J Clin Phar-macol 2000;56:489-93.
65. Loeffler PM. Oral benzodiazepines and conscious sedation: areview. J Oral Maxillofac Surg 1992;50:989-97.
66. Chan E, McLachlan A, O’Reilly R, Rowland M. Stereochemicalaspects of warfarin drug interactions: use of a combined pharmacokinetic-pharmacodynamic model. Clin Pharmacol Ther 1994;56:286-94.
67. Wenzel RG, Sarvis CA. Do butalbital-containing products have arole in the management of migraine? Pharmacotherapy 2002;22:1029-35.
68. Muller HP, Holderrieth S, Burkhardt U, Hoffler U. In vitroantimicrobial susceptibility of oral strains of Actinobacillus actino-mycetemcomitans to seven antibiotics. J Clin Periodontol 2002;29:736-42.
69. Slots J. Selection of antimicrobial agents in periodontal therapy. JPeriodontal Res 2002;37:389-98.
70. Slots J, Feik D, Rams TE. Prevalence and antimicrobial suscepti-bility of Enterobacteriaceae, Pseudomonadaceae and Acinetobacter inhuman periodontitis. Oral Microbiol Immunol 1990;5:149-54.
71. Batty KT, Davis TM, Ilett KF, Dusci LJ, Langton SR. The effectof ciprofloxacin on theophylline pharmacokinetics in healthy subjects.Br J Clin Pharmacol 1995;39:305-11.
72. Wijnands WJ, Vree TB, van Herwaarden CL. The influence ofquinolone derivatives on theophylline clearance. Br J Clin Pharmacol1986;22:677-83.
73. Raaska K, Neuvonen PJ. Ciprofloxacin increases serum clozapineand N-desmethylclozapine: a study in patients with schizophrenia. EurJ Clin Pharmacol 2000;56:585-9.
74. Markowitz JS, Gill HS, Devane CL, Mintzer JE. Fluroquinoloneinhibition of clozapine metabolism. Am J Psychiatry 1997;153:881.
75. Perkins DO. Predictors of noncompliance in patients withschizophrenia. J Clin Psychiatry 2002;63:1121-8.
76. Ciancio SG, van Winkelhoff AJ. Antibiotics in periodontaltherapy. In: Newman MG, van Winkelhoff AJ, eds. Antibiotic andantimicrobial use in dental practice. 2nd ed. Chicago: Quintessence;2001:113-26.
77. Baumgartner JC. Antibiotics in endodontic therapy. In: NewmanMG, van Winkelhoff AJ, eds. Antibiotic and antimicrobial use in dentalpractice. 2nd ed. Chicago: Quintessence; 2001:143-55.
78. Peterson LJ. Antibiotics for oral and maxillofacial infections. In:Newman MG, van Winkelhoff AJ, eds. Antibiotic and antimicrobial usein dental practice. 2nd ed. Chicago: Quintessence; 2001:157-73.
79. Beikler T, Flemmig TF. Antimicrobials in implant dentistry. In:Newman MG, van Winkelhoff AJ, eds. Antibiotic and antimicrobial usein dental practice. 2nd ed. Chicago: Quintessence; 2001:195-211.
80. Kazmier FJ. A significant interaction between metronidazole andwarfarin. Mayo Clin Proc 1976;51:782-4.
81. O’Reilly RA. The stereoselective interaction of warfarin andmetronidazole in man. N Eng J Med 1976;295:354-7.
82. Blyden GT, Scavone JM, Greenblatt DJ. Metronidazole impairsclearance of phenytoin but not of alprazolam or lorazepam. J ClinPharmacol 1988;28:240-5.
83. Kapseals dilantin (extended phenytoin sodium capsules, USP). In: Physicians’ desk reference. 57th ed. Montvale, N.J.: Medical Economics; 2003:2531-3.
84. Montgomery EH. Antibacterial antibiotics. In: Yagiela JA, NeidleEA, Dowd FJ, eds. Pharmacology and therapeutics for dentistry. 4thed. St. Louis: Mosby; 1998:496-533.
85. Montgomery EH. Antimicrobial agents in the prevention andtreatment of infection. In: Yagiela JA, Neidle EA, Dowd FJ, eds. Phar-macology and therapeutics for dentistry. 4th ed. St. Louis: Mosby;1998:634-43.
86. Honig P, Wortham D, Zamani K, Conner D, Cantilena L. Effect oferythromycin, clarithromycin and azithromycin on pharmacokinetics ofterfenadine. Clin Pharmacol Ther 1993;53:161.
87. Matitila MJ, Vanakokski J, Idänpään-Heikkilä JJ. Azithromycindoes not alter the effects of oral midazolam on human performance.Eur J Clin Pharmacol 1994;47:49-52.
88. Harris S, Hilligoss DM, Colangelo PM, Eller M, Okerholm R.Azithromycin and terfenadine: lack of drug interaction. Clin PharmacolTher 1995;58:310-5.
89. Sanz M, Herrera D. Individual drugs. In: Newman MG, vanWinkelhoff AJ, eds. Antibiotic and antimicrobial use in dental practice.2nd ed. Chicago: Quintessence; 2001:33-52.
90. Honig PK, Woosley RL, Zamani K, Conner DP, Cantilena LR Jr.Changes in the pharmacokinetics and electrocardiographic pharmaco-dynamics of terfenadine with concomitant administration of ery-thromycin. Clin Pharmacol Ther 1993;53:231-8.
91. Biglin KE, Faraon MS, Constance TD, Leih-Lai M. Drug-inducedtorsades de pointes: a possible interaction of terfenadine and ery-thromycin. Ann Pharmacother 1994;28:282.
92. Kivisto KT, Neuvonen PJ, Klotz U. Inhibition of terfenadinemetabolism: pharmacokinetic and pharmacodynamic consequences.Clin Pharmacokinet 1994;27:1-5.
93. Honig PK, Wortham DC, Zamani K, Conner DP, Mullin JC, Can-tilena LR. Terfenadine-ketoconazole interaction: pharmacokinetic andelectrocardiographic consequences. JAMA 1993;269:1513-8.
94. Honig PK, Wortham DC, Hull R, et al. Itraconazole affects single-dose terfenadine pharmacokinetics and cardiac repolarization pharma-codynamics. J Clin Pharmacol 1993;33:1201-6.
95. Goss JE, Ramo BW, Blake K. Torsades de pointes associated withastemizole (Hismanal) therapy. Arch Intern Med 1993;153:2705.
96. Lefebvre RA, Van Peer A, Woestenborghs R. Influence of itra-conazole on the pharmacokinetics and electrocardiographic effects ofastemizole. Br J Clin Pharmacol 1997;43:319-22.
Copyright ©2004 American Dental Association. All rights reserved.
on March 20, 2010
jada.ada.orgD
ownloaded from

JADA, Vol. 135, March 2004 311
C L I N I C A L P H A R M A C O L O G Y
97. Kyrmizakis DE, Chimona TS, Kanoupakis EM, Papadakis CE,Velegrakis GA, Helidonis ES. QT prolongation and torsades de pointesassociated with concurrent use of cisapride and erythromycin. Am JOtolaryngol 2002;23:303-7.
98. Piquette RK. Torsades de pointes induced by cisapride/clarithromycin interaction. Ann Pharmacother 1999;33:22-6.
99. van Haarst AD, van ’t Klooster GA, van Gerven JM, et al. Theinfluence of cisapride and clarithromycin on QT intervals in healthyvolunteers. Clin Pharmacol Ther 1998;64:542-6.
100. Desta Z, Kerbusch T, Flockhart DA. Effect of clarithromycin onthe pharmacokinetics and pharmacodynamics of pimozide in healthypoor and extensive metabolizers of cytochrome P450 2D6 (CYP2D6).Clin Pharmacol Ther 1999;65:10-20.
101. Spach DH, Bauwens JE, Clark CD, Burke WG. Rhabdomyolysisassociated with lovastatin and erythromycin use. West J Med1991;154:213-5.
102. Kantola T, Kivisto KT, Neuvonen PJ. Erythromycin and vera-pamil considerably increase serum simvastatin and simvastatin acidconcentrations. Clin Pharmacol Ther 1998;64:177-82.
103. Lees RS, Lees AM. Rhabdomyolysis from the coadminsistrationof lovastatin and the antifungal agent itraconazole. N Engl J Med1995;333:664-5.
104. Neuvonen PJ, Jalava KM. Itraconazole drastically increasesplasma concentrations of lovastatin and lovastatic acid. Clin PharmacolTher 1996;60:54-61.
105. Neuvonen PJ, Kantola T, Kivisto KT. Simvastatin but notpravastatin is very susceptible to interaction with the CYP3A4inhibitor itraconazole. Clin Pharmacol Ther 1998;63:332-41.
106. Mazzu AL, Lasseter KC, Shamblen EC, Agarwal V, Lettieri J,Sundaresen P. Itraconazole alters the pharmacokinetics of atorvastatinto a greater extent than either cerivastatin or pravastatin. Clin Phar-macol Ther 2000;68:391-400.
107. Bennett JC, Moreland LW. Musculoskeletal and connectivetissue disease. In: Cecil RL, Andreoli TE, eds. Cecil essentials ofmedicine. 4th ed. Philadelphia: Saunders; 1997:921-7.
108. Shaukat A, Benekli M, Vladutiu GD, Slack JL, Wetzler M, BaerMR. Simvastatin-fluconazole causing rhabdomyolysis. Ann Pharma-cother 2003;37:1032-5.
109. Liedholm H, Nordin G. Erythromycin-felodipine interaction.DICP 1991;25:1007-8.
110. Neuvonen PJ, Suhonen R. Itraconazole interacts with felodipine.J Am Acad Dermatol 1995;33:134-5.
111. Tailor SA, Gupta AK, Walker SE, Shear NH. Peripheral edemadue to nifedipine-itraconazole interaction: a case report. Arch Dermatol1996;132:350-2.
112. Jensen CW, Flechner SM, Van Buren CT, et al. Exacerbation ofcyclosporine toxicity by concomitant administration of erythromycin.Transplantation 1987;43:263-70.
113. Spicer ST, Liddle C, Chapman JR, et al. The mechanism ofcyclosporine toxicity induced by clarithromycin. Br J Clin Pharmacol1997;43:194-6.
114. Lampen A, Christians U, Guengerich FP, et al. Metabolism ofthe immunosuppressant tacrolimus in the small intestine: cytochromeP450, drug interactions, and interindividual variability. Drug MetabDispos 1995;23:1315-24.
115. Gomez DY, Wacher VJ, Tomlanovich SJ, Hebert MF, Benet LZ.The effects of ketoconazole on the intestinal metabolism and bioavail-ability of cyclosporine. Clin Pharmacol Ther 1995;58:15-9.
116. Floren LC, Bekersky I, Benet LZ, et al. Tacrolimus oral bioavail-ability doubles with coadministration of ketoconazole. Clin Pharmacol
Ther 1997;62:41-9.117. Soltero L, Carbajal H, Rodriguez-Montalvo C, Valdes A. Coad-
ministration of tacrolimus and ketoconazole in renal transplant recipi-ents: cost analysis and review of metabolic effects. Transplant Proc2003;35:1319-21.
118. Vasquez E, Pollak R, Benedetti E. Clotrimazole increasestacrolimus blood levels: a drug interaction in kidney transplantpatients. Clin Transplant. 2001;15:95-9.
119. Bussey HI, Knodel LC, Boyle DA. Warfarin-erythromycin inter-action. Arch Intern Med 1985;145:1736-7.
120. Hassell D, Utt JK. Suspected interaction: warfarin and ery-thromycin. South Med J 1985;78:1015-6.
121. Bachmann K, Schwartz JI, Forney R Jr, Frogameni A, JaureguiLE. The effect of erythromycin on the disposition kinetics of warfarin.Pharmacology 1984;28:171-6.
122. Recker MW, Kier KL. Potential interaction between clar-ithromycin and warfarin. Ann Pharmacother 1997;31:996-8.
123. Oberg KC. Delayed elevation of international normalized ratiowith concurrent clarithromycin and warfarin therapy. Pharma-cotherapy 1998;18:386-91.
124. Black DJ, Kunze KL, Wienkers LC, et al. Warfarin-fluconazole,part II: a metabolically based drug interaction: in vivo studies. DrugMetab Dispos 1996;24:422-8.
125. Berrettini WH. A case of erythromycin-induced carbamazepinetoxicity. J Clin Psychiatry 1986;47:147.
126. Albani F, Riva R, Baruzzi A. Clarithromycin-carbamazepineinteraction: a case report. Epilepsia 1993;34:161-2.
127. O’Connor NK, Fris J. Clarithromycin-carbamazepine interactionin a clinical setting. J Am Board Fam Pract 1994;7:489-92.
128. Wong YY Ludden TM, Bell RD. Effect of erythromycin on carba-mazepine kinetics. Clin Pharmacol Ther 1983;33:460-4.
129. Miles MV, Tennison MB. Erythromycin effects on multiple-dosecarbamazepine kinetics. Ther Drug Monit 1989;11:47-52.
130. Spina E, Arena D, Scordo MG, Fazio A, Pisani F, Perucca E. Ele-vation of plasma carbamazepine concentrations by ketoconazole inpatients with epilepsy. Ther Drug Monit 1997;19:535-8.
131. Nair DR, Morris HH. Potential fluconazole-induced carba-mazepine toxicity. Ann Pharmacother 1999;33:790-2.
132. Finch CK, Green CA, Self TH. Fluconazole-carbamazepine inter-action. South Med J 2002;95:1099-100.
133. Tenenbein M. Theophylline toxicity due to drug interaction. JEmerg Med 1989;7:249-51.
134. Paulsen O, Hoglund P, Nilsson LG, Bengtsson HI. The interac-tion of erythromycin with theophylline. Eur J Clin Pharmacol1987;32:493-8.
135. Wiggins J, Arbab O, Ayres JG, Skinner C. Elevated serum theo-phylline concentration following cessation of erythromycin treatment.Eur J Respir Dis 1986;68:298-300.
136. Richards W, Church JA, Brent DK. Theophylline-associatedseizures in children. Ann Allergy 1985;54:276-9.
137. Iliopoulou A, Aldhous ME, Johnston A, Turner P. Pharmacoki-netic interaction between theophylline and erythromycin. Br J ClinPharmacol 1982;14:495-9.
138. Tjia JF, Colbert J, Back DJ. Theophylline metabolism in humanliver microsomes: inhibition studies. J Pharmacol Exp Ther1996;276:912-7.
139. Fleischmann J. Topical and systemic antifungal and antiviralagents. In: Newman MG, van Winkelhoff AJ, eds. Antibiotic andantimicrobial use in dental practice. 2nd ed. Chicago: Quintessence;2001:69-88.
Copyright ©2004 American Dental Association. All rights reserved.
on March 20, 2010
jada.ada.orgD
ownloaded from