
Dr. Vohra Duodenum Shortest (25cm) part of the small intestine. Joins the stomach to the jejunum....
26
-
Upload
kenzie-mason -
Category
Documents
-
view
219 -
download
4
Transcript of Dr. Vohra Duodenum Shortest (25cm) part of the small intestine. Joins the stomach to the jejunum....


Dr. Vohra
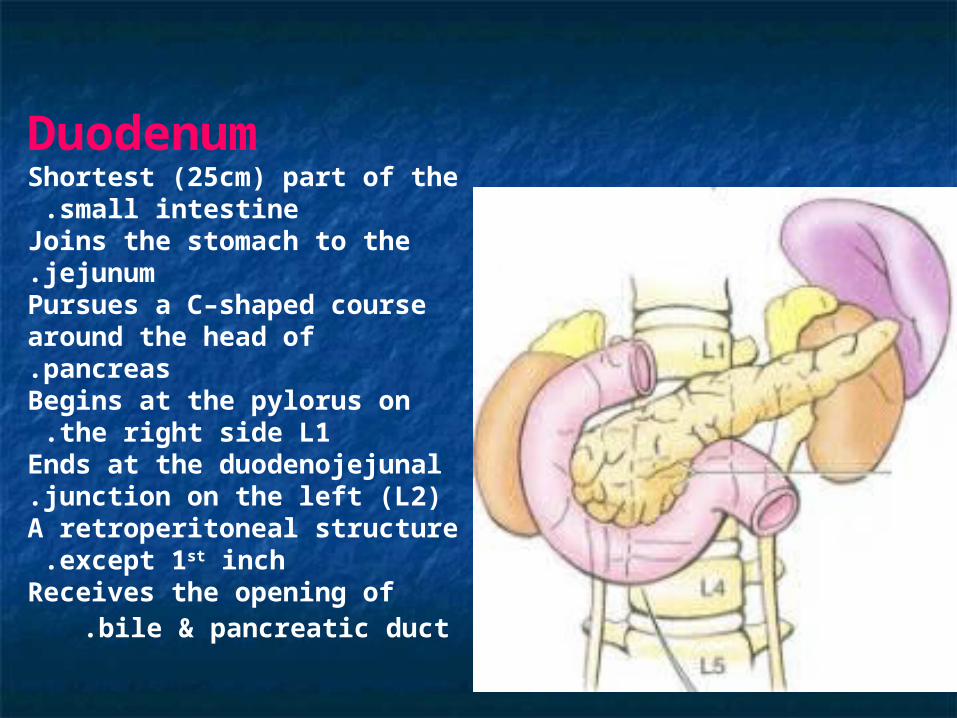
DuodenumShortest (25cm) part of the small intestine .
Joins the stomach to the jejunum.Pursues a C–shaped course around the head of pancreas.Begins at the pylorus on the right side L1 .
Ends at the duodenojejunal junction on the left (L2).A retroperitoneal structure except 1st inch .
Receives the opening of bile & pancreatic duct.
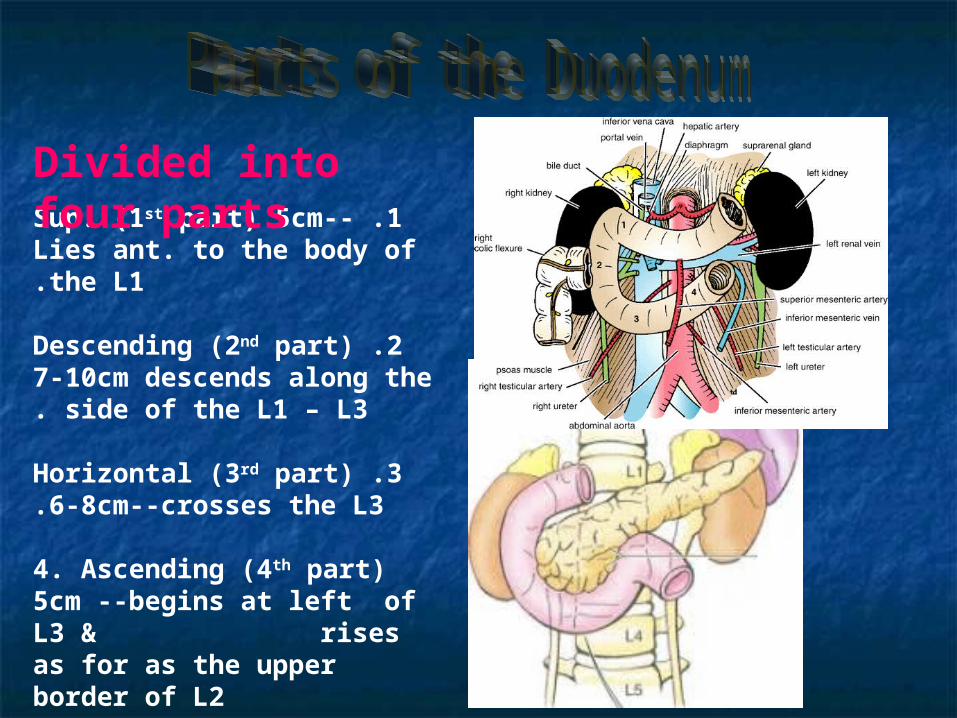
1 .Sup. (1st part) 5cm--Lies ant. to the body of the L1.
2 .Descending (2nd part) 7-10cm descends along the side of the L1 – L3.
3 .Horizontal (3rd part) 6-8cm--crosses the L3.
4. Ascending (4th part) 5cm --begins at left of L3 & rises as for as the upper border of L2
Divided into four parts
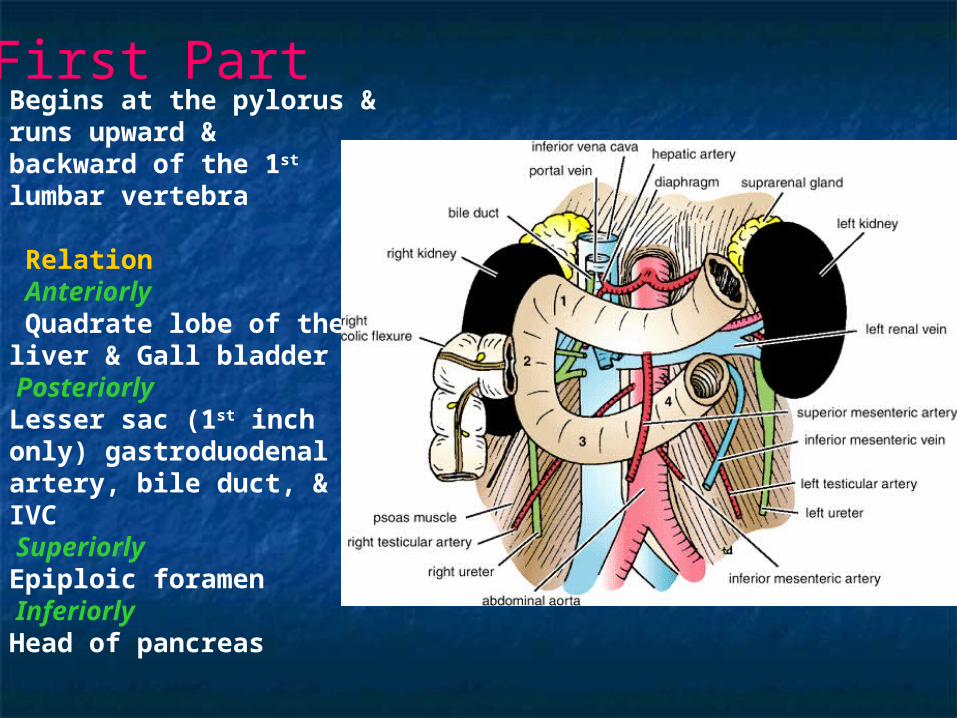
Begins at the pylorus & runs upward & backward of the 1st lumbar vertebra
Relation Anteriorly Quadrate lobe of the liver & Gall bladderPosteriorly Lesser sac (1st inch only) gastroduodenal artery, bile duct, & IVCSuperiorly Epiploic foramenInferiorly Head of pancreas
First Part
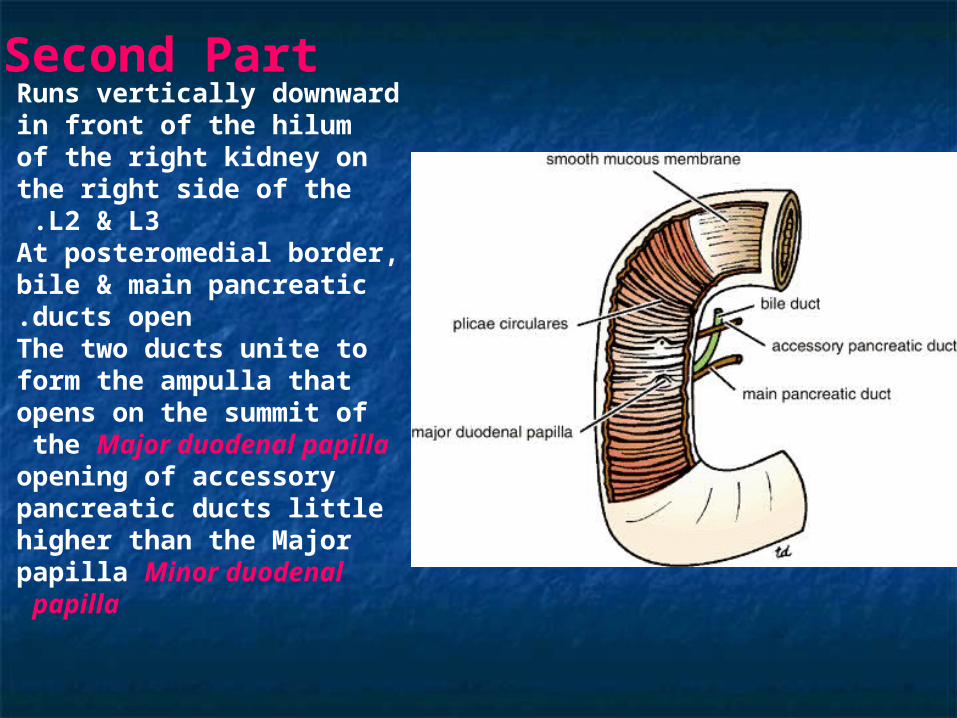
Runs vertically downward in front of the hilum of the right kidney on the right side of the L2 & L3 .At posteromedial border, bile & main pancreatic ducts open.The two ducts unite to form the ampulla that opens on the summit of the Major duodenal papilla opening of accessory pancreatic ducts little higher than the Major papilla Minor duodenal papilla
Second Part
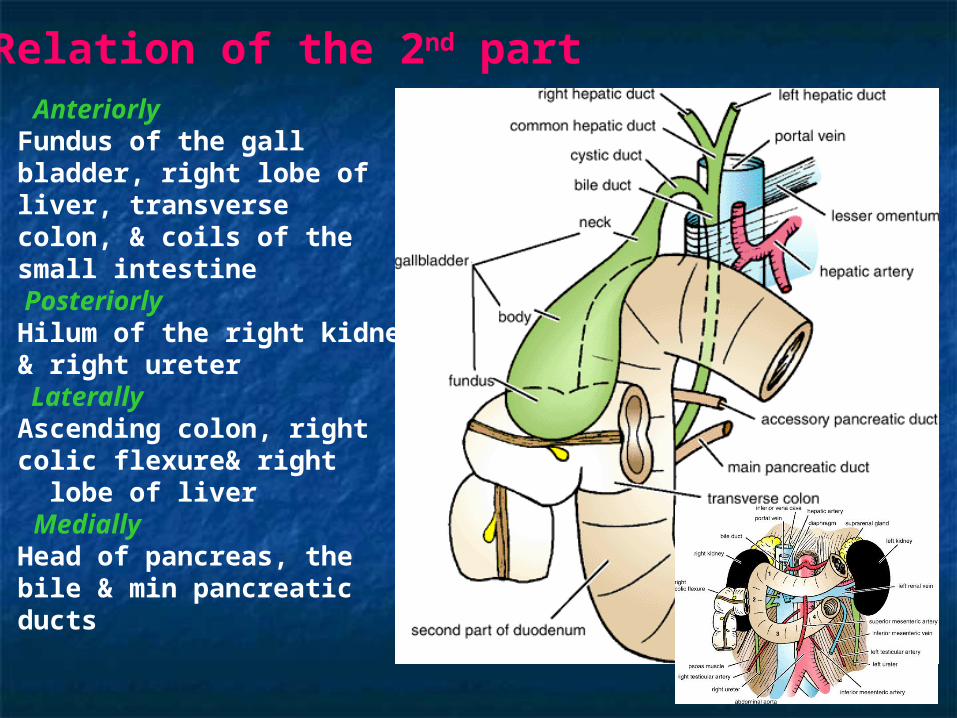
Anteriorly Fundus of the gall bladder, right lobe of liver, transverse colon, & coils of the small intestinePosteriorly Hilum of the right kidney & right ureterLaterally
Ascending colon, right colic flexure& right lobe of liver Medially Head of pancreas, the bile & min pancreatic ducts
Relation of the 2nd part
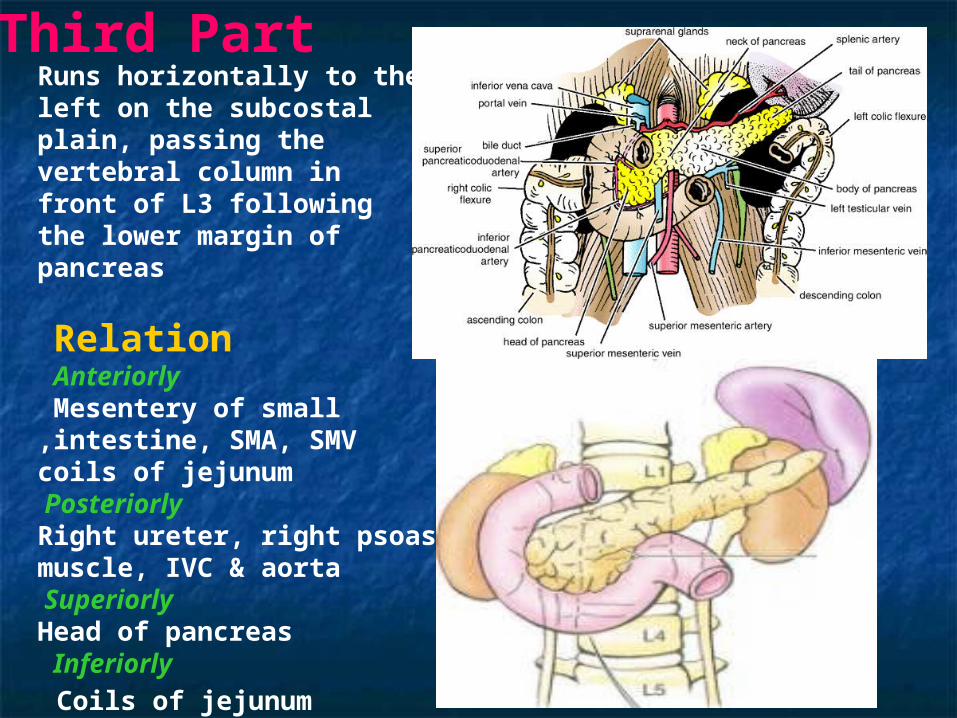
Runs horizontally to the left on the subcostal plain, passing the vertebral column in front of L3 following the lower margin of pancreas
Relation Anteriorly Mesentery of small intestine, SMA, SMV,coils of jejunumPosteriorly Right ureter, right psoas muscle, IVC & aortaSuperiorly Head of pancreasInferiorly
Coils of jejunum
Third Part
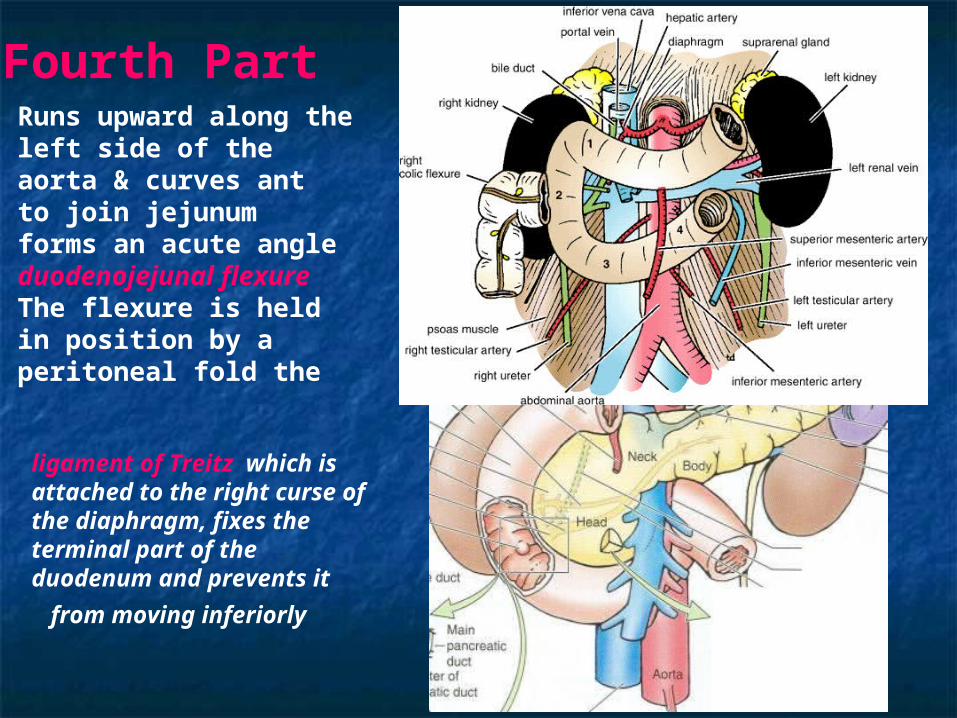
Runs upward along the left side of the aorta & curves ant to join jejunum forms an acute angle duodenojejunal flexure The flexure is held in position by a peritoneal fold the
ligament of Treitz which is attached to the right curse of the diaphragm, fixes the terminal part of the duodenum and prevents it from moving
inferiorly
Fourth Part
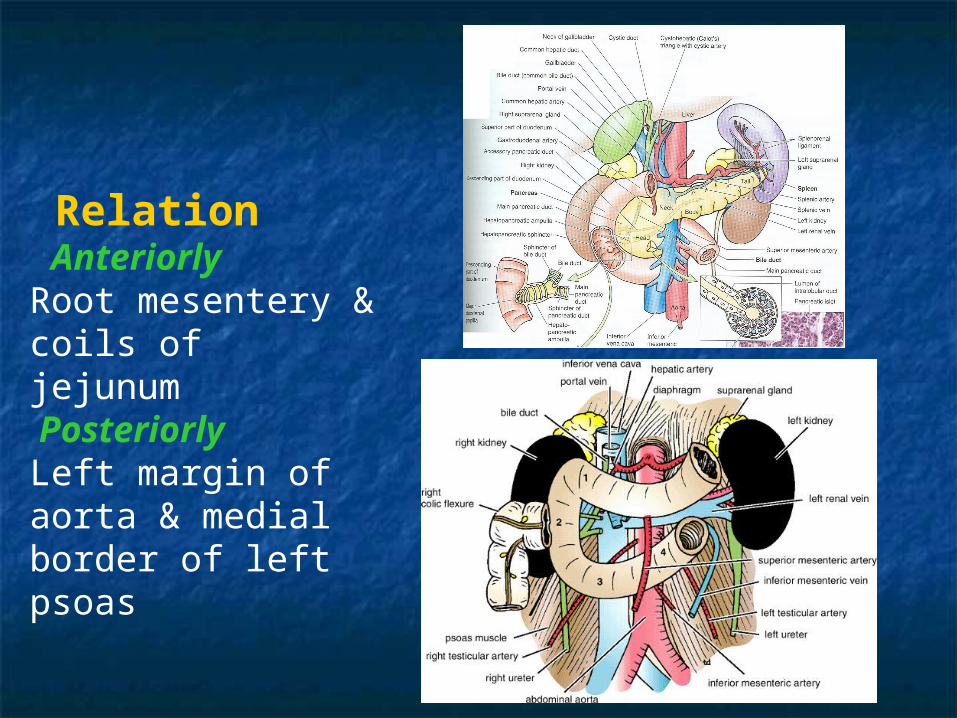
Relation Anteriorly Root mesentery & coils of jejunumPosteriorly Left margin of aorta & medial border of left psoas
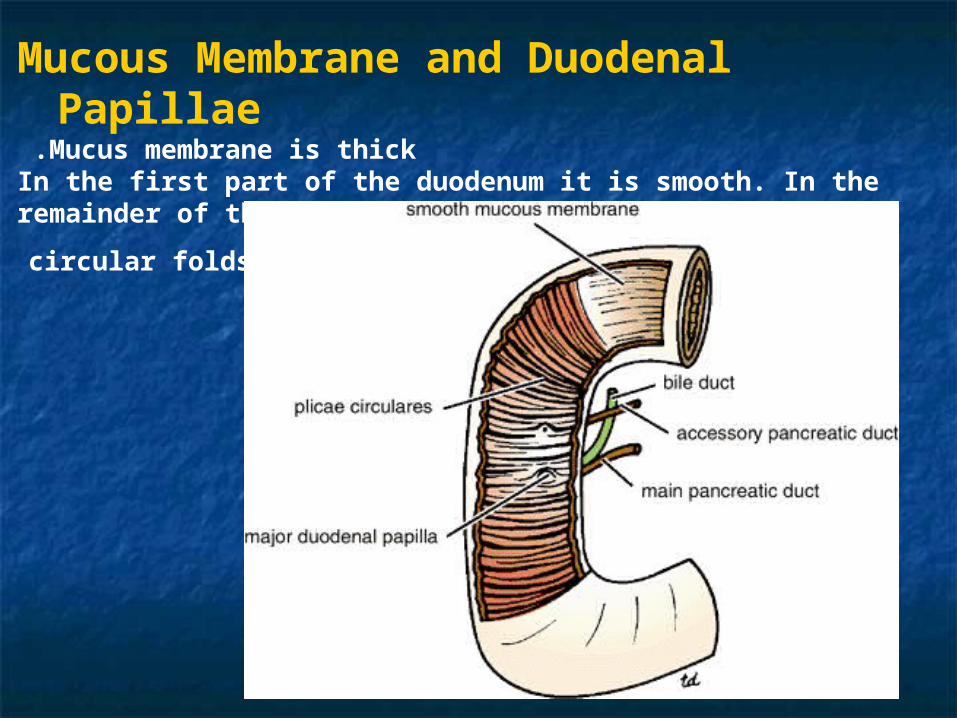
Mucous Membrane and Duodenal Papillae Mucus membrane is thick.
In the first part of the duodenum it is smooth. In the remainder of the duodenum it is thrown into numerous
circular folds called the plicae circularis
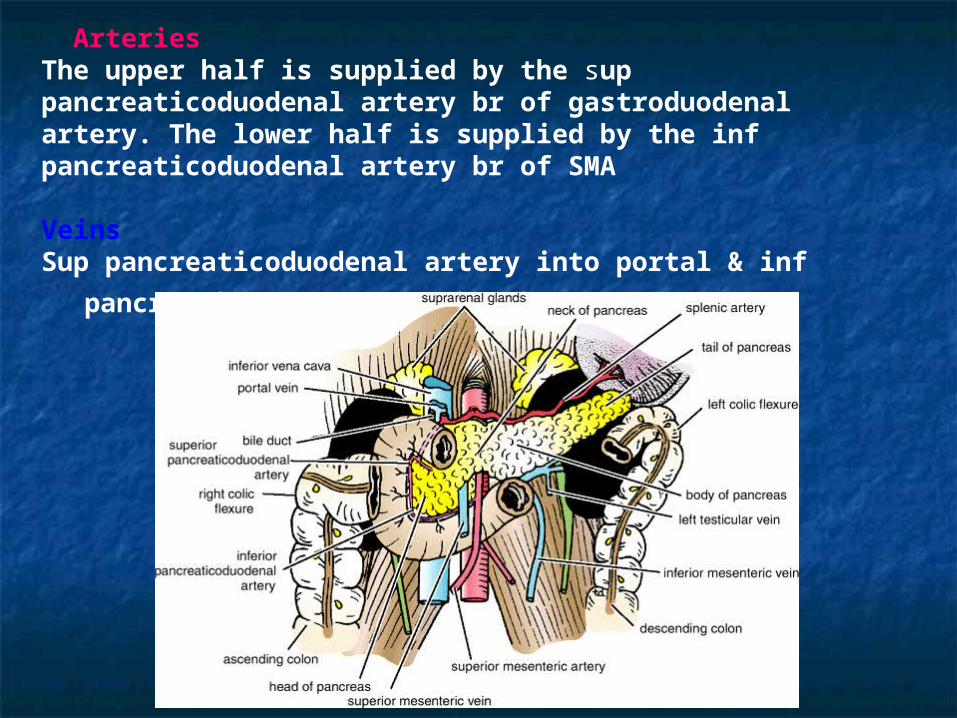
Arteries The upper half is supplied by the sup pancreaticoduodenal artery br of gastroduodenal artery. The lower half is supplied by the inf pancreaticoduodenal artery br of SMA
VeinsSup pancreaticoduodenal artery into portal & inf
pancreaticoduodenal drains into SMA
Nerve Supply Sympathetic & parasympathetic (vagus)
nerves from celiac & superior mesenteric plexuses
Clinical Notes Trauma to the duodenumIn severe injury to ant abdominal wall, the 3rd part
May be severely crushed against the L3
Duodenal UlcerAn ant ulcer of the 1st inch of 1st part may perforate into greater sac and the fluid my go to the right iliac fossa. In this case the differential diagnoses b/w a perforated duodenal ulcer & perforated appendix may be difficult
Duodenal Recesses Close to the duodenojejunal junction, there may be four small pocketlike pouches of peritoneum called the superior duodenal, inferior duodenal, paraduodenal and
retroduodenal recesses
Important Duodenal RelationGallstone may ulcerate the duodenum


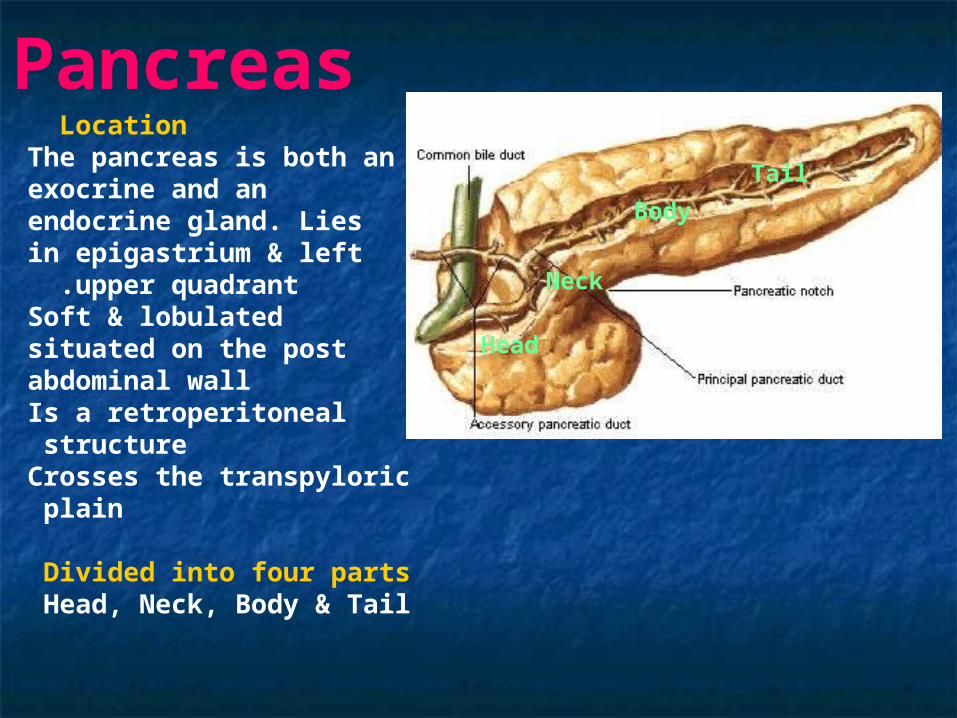
Location The pancreas is both an exocrine and an endocrine gland. Lies in epigastrium & left
upper quadrant .Soft & lobulated situated on the post abdominal wallIs a retroperitoneal structure Crosses the transpyloric plain
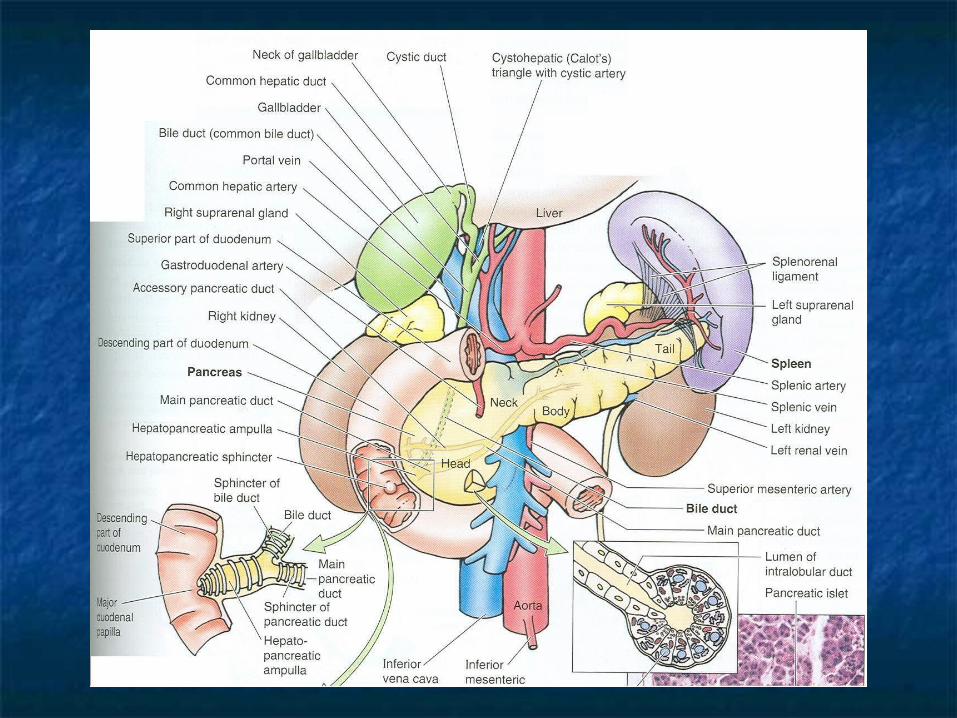
Divided into four parts Head, Neck, Body & Tail
PancreasTail
Head
Neck
Body
Pancreas Head of the pancreas Is disc shaped lies within the concavity of duodenum A part from head extends to the left behind the SMA is called UNCINATE PROCESS
Neck of the pancreas Constricted portion of pancreas connects head to the body
Body of the pancreasRuns upward & to the left across the midline
Tail of the pancreasPasses forward in the splenicorenal ligament & comes in
contact with the hilum of the spleen
Tail
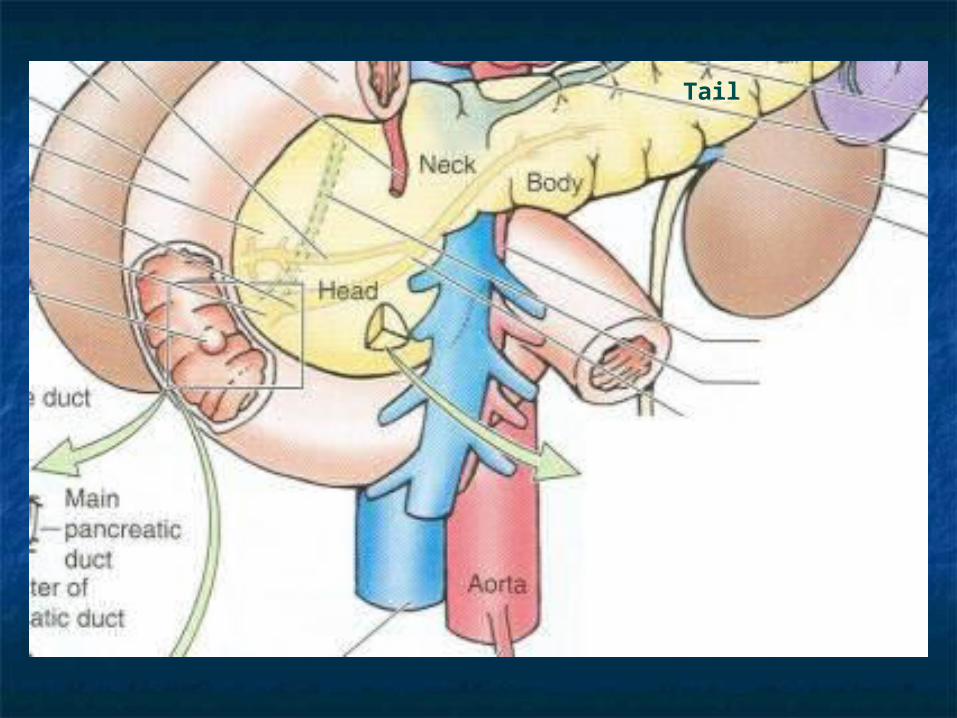
Relation of the pancreasAnteriorly from right to left Transverse colon, transverse mesocolon, lesser sac & stomachPosteriorly from right to leftBile duct, portal & splenic veins, IVF, aorta, origin of SMA, left psoas muscle, left suprarenal gland, left kidney, & hilum of the spleen
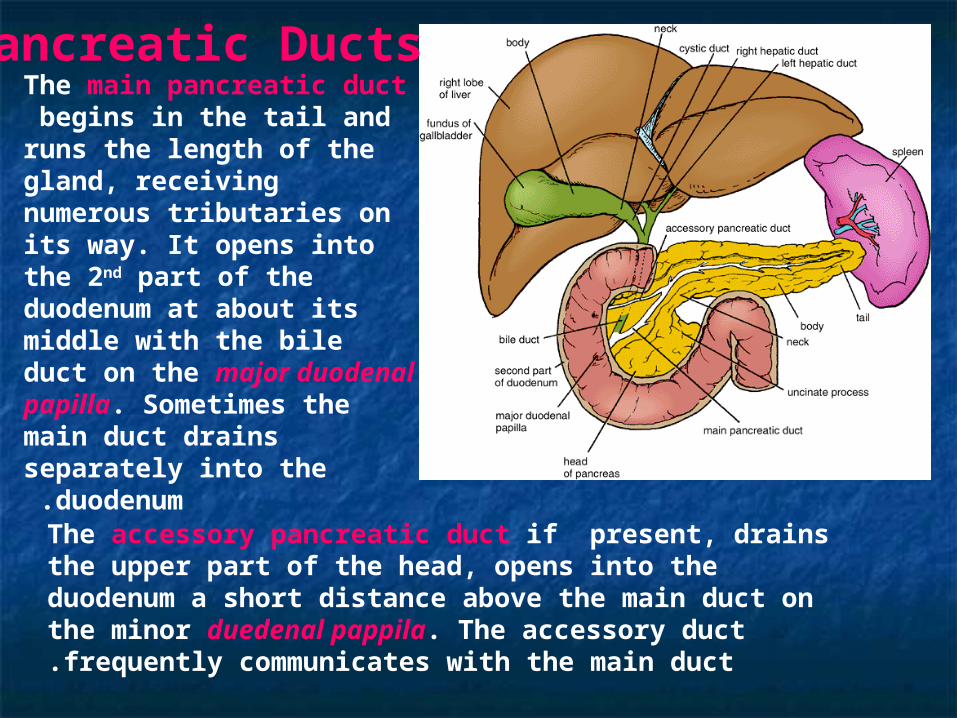
The main pancreatic duct begins in the tail and runs the length of the gland, receiving numerous tributaries on its way. It opens into the 2nd part of the duodenum at about its middle with the bile duct on the major duodenal papilla. Sometimes the main duct drains separately into the duodenum .
Pancreatic Ducts
The accessory pancreatic duct if present, drains the upper part of the head, opens into the duodenum a short distance above the main duct on the minor duedenal pappila. The accessory duct frequently communicates with the main duct.
Blood SupplyArteriesThe splenic and the superior and inferior pancreaticoduodenal arteries supply the pancreas.
VeinsThe corresponding veins drain into the portal system.
Lymph DrainageLymph nodes are situated along the arteries that supply the gland. The efferent vessels ultimately drain into the celiac and superior mesenteric lymph nodes.
Nerve SupplySympathetic and parasympathetic (vagal) nerve fibers supply the area.
Diagnosis of Pancreatic Disease
The deep location of the pancreas sometimes gives rise to problem of diagnosis for the following reasons
Pain from the pancreas is commonly referred to the back.Because the pancreas lies behind the stomach and transverse colon, disease of the gland can be confused with that of the stomach or transverse colon.Inflammation of the pancreas can spread to the peritoneum forming the posterior wall of the lesser sac. This in turn can lead to adhesions and the closing off of the lesser sac to form a pseudocyst.
















![Vohra Instructor Manual All Chapter File[1]](https://static.fdocuments.net/doc/165x107/55cf9c57550346d033a97fcf/vohra-instructor-manual-all-chapter-file1.jpg)


