Dr Vincent Connolly Clinical Director ECIST
15
The (R)evolution of Ambulatory Emergency Care Dr Vincent Connolly Clinical Director ECIST
Transcript of Dr Vincent Connolly Clinical Director ECIST

The (R)evolution of Ambulatory Emergency Care Dr Vincent Connolly Clinical Director ECIST

Vincent Connolly
Because its complex!
Why is emergency care so challenging?

95% of the increase in short stay admissions
• Urinary disorders • Gastroenteritis / colitis • Tonsillitis • Cellulitis • Pneumonia (unspecified) • GORD • Convulsions • Abscesses, carbuncles

Value Equation
Patient experience X Patient Outcomes
Cost

Doing things differently

Anatomy
Physiology
Psychology
(R)evolution starts here

Patient Selection is the key step

Default to Day Surgery
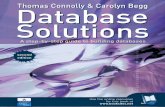
Suitability for day surgery Pathway
Clearly suitable
Unsure
Clearly unsuitable
Day surgery Home if ok
Inpatient care ? Home if ok
Inpatient care Hospital stay
20–30%
5–20%
40–65%

Models of AEC – 4Ps
• Passive – receive referrals
• Pathway driven – restricted to particular agreed pathways
• Pull – senior clinician takes calls for emergency referrals
• Process driven – all patients considered for AEC

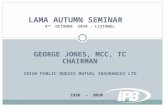
Example of an AEC process model
ED
Ambulatory Emergency Care Centre
Acute Assessment Unit Wards
GPs
999
Walk Ins
Home and/or clinic
Home Clinic
Overarching principle; Treat all emergency patients as ambulatory until proven otherwise
Specialty admissions
Clinically unstable
Clinical conversation

4 simple questions
• Is this patient clinically stable?
• Is the patient functionally capable of being managed in the AEC Unit?
• Would this patient have been admitted to hospital before AEC existed?
• Could the patient’s needs be better met by another service?

Why is good practice not adopted?
• Culture & Beliefs • Weak system enablers • Leadership and management capacity &
capability • Staffing constraints • Estates constraints • Financial constraints

The (R)evolution of suspected PE management

(R)evolution Outcomes
• It dies out and things go back to “normal”
• It stabilises
• It takes over and becomes the norm

If I cant dance I don’t want to be part of your revolution.
Emma Goldman