
Dr. A.R.Pintilie. 1.Cardiovascular Diseases 2.Urinary Tract Infections 3.Gastrointestinal Disorders...
59
Dr. A.R.Pintilie
-
Upload
sabrina-holt -
Category
Documents
-
view
214 -
download
0
Transcript of Dr. A.R.Pintilie. 1.Cardiovascular Diseases 2.Urinary Tract Infections 3.Gastrointestinal Disorders...

Dr. A.R.Pintilie

1.Cardiovascular Diseases 2.Urinary Tract Infections 3.Gastrointestinal Disorders 4.Diabetes 5.Infections 6.Neoplastic Diseases 7.Uterine fibromyomas

1.Cardiovascular Diseases – Cardiovascular disease is one of the most important nonobstetric cause of disability and death in pregnant women occurring in about 1% of all pregnant women.
The influence of pregnancy on cardiovascular diseases
-minors cv incidents: palpitation, dyspnea-majors cv incidents: pulmonary edema, cardiac
failure, rhythm disturbances, arterial embolism The risk for death is up to the folowing 3 groups
factors:Group nr.1 ( mortality 0-1%):- atrial or ventricular septal defect- patent ductus arteriosus- mitral stenosis (class I and II)

Group nr.2 (mortality 5-15%):- mitral stenosis (class III and IV)- aortic stenosis- aortic coarctation (without valvular
involvement)- Fallot tetralogy (uncorrected)- artificial valveGroup 3 (mortality 25-50%):- pulmonary hypertension- aortic coarctation with valvular involvement - Marfan's syndrome - Eisenmenger's syndrome

The lesions are classified according to the functional grading of the New York Heart Association as follows:
=> class I = patients with cardiac disease and no limitation of physical activity; these patients do not have symptoms of cardiac insufficiency nor anginal pain (uncompromised patients);
=> class II = slightly compromised: patients with cardiac disease and slight limitation of physical activity; they are free from symptoms while at rest, but ordinary activity is accompanied by undue fatigue, palpitation, dyspnea or anginal pain;

=> class III = markedly compromised: patients with cardiac disease and marked limitation of physical activity; less than ordinary activity causes discomfort in the form of excessive fatigue, palpitation, dyspnea or anginal pain;
=> class IV = severely compromised: patients with cardiac disease and inability to perform any physical activity without discomfort ; symptoms of cardiac insufficiency or of the anginal syndrome may develop even at rest and any activity increases them.

The influence of cardiovascular disease on pregnancy - increased incidence of spontaneous abortion , - increased incidence of prematurity and low-birth-
weight
With satisfactory surgical correction prior to pregnancy maternal risks are decreased dramatically and fetal environment is improved.
Operations to correct heart lesions are seldom necessary during pregnancy as it is indicated by the excellent results that can be obtained by medical treatment alone.

Delivery should be accomplished vaginally unless there are obstetrical indications for cesarean delivery. In spite of the physical effort inherent in labor and vaginal delivery, less morbidity and mortality are associated with it.
Induction of labor for heart disease alone is contraindicated
During labor, the patient should be kept in a semirecumbent position.
Prophylactic antibiotics are recomended in all cases of congenital or acquired heart disease to prevent subacute bacterial endocarditis in uncomplicated vaginal deliveries.

2.Urinary Tract Infections Asymptomatic bacteriuria Asymptomatic (covert) bacteriuria
refers to persistent actively multiplying bacteria within the urinary tract without symptoms. A clean-voided specimen containing more than 100,000 colonies/ml is considered evidence for infection.
Bacteriuria has been linked to an increased incidence of preterm births, pregnancy-induced hypertension and anemia.
A 10 to 14 day course of one of these agents (ampicillin, nitrofurantoin, cephalosporin) will effectively eradicate bacteriuria in about 70% of pregnant patients.

Cystitis and urethritis The principal symptoms are frequency,
dysuria and suprapubic pain and tenderness. Although cystitis is usually uncomplicated it is presumed that the upper urinary tract may become involved by ascending infection.
Bacterial cystitis responds readily to any of several regimens (Ampicillin 500mg every 6 hours, Nitrofurantoin lOOmg once a day, Sulfisoxazole lg, four times daily). Treatment should be continued for 10 days. Single-dose therapy (as described for asymptomatic bacteriuria) has been shown effective.

Acute pyelonephritis Acute upper urinary tract infections usually
develop late in the second trimester, early in the third or after delivery. Approximately two thirds occur in women who have asymptomatic bacteriuria.
The usual symptoms are : chills, fever, flank pain, dysuria, nausea and vomiting. The temperature may have high levels (40-41C). Palpation of the kidney area produces severe pain and there may be tenderness along the course of the ureter and over the bladder. The right kidney is most often involved, but the infection frequently occurs bilaterally.

The diagnosis is confirmed by examination of a catheterized specimen of urine which will contain many pus cells and bacteria (E. coli, Klebsiella, Enterobacter, Proteus). About 15% of women also have bacteriemia. The white blood cell count may be as high as 20,000 to 30,000.
Undelivered patients are best treated in the hospitalThe medication should be continued for at least 14 days. Antimicrobial resistance of E.coli to ampicillin has often been encountered. For these reasons, many prefer to give gentamicin or tobramycin along with ampicillin or a cephalosporin or extended spectrum penicillin.
Intravenous hydration to insure adequate urinary output is essential.

3.Gastrointestinal Disorders Appendicitis Acute appendicitis occurs with the same
frequency in pregnant as in nonpregnant women, but the diagnosis is more difficult and delay in treatment is hazardous. The difficulty in diagnosis and delay in operative intervention increase with gestational age, as does maternal and fetal mortality.
The enlarged uterus may obscure the appendix which tends to be displaced upward and laterally, containment of infection by the omentum becomes increasingly unlikely and appendiceal rupture causes generalized peritonitis.

Changes in position of the appendix as pregnancy advances

Effects on pregnancy outcome Abortion or premature labor may occur if
the infection involves the uterine serosa. Uterine contractions stimulated by the infection are frequently tetanic and predispose to fetal hypoxia and intrauterine fetal death.
Diagnosis Nausea and vomiting, epigastric pain and
pain localizing in the right side of the abdomen and tenderness anywhere from McBurney's point to the right flank- during the first trimester, the pain localizes in the right lower quadrant; at 6 months, the point of maximal thickness is above the iliac crest and at 8 months, it rises to the level of the right costal margin.

All these simptoms are suggestive but the diagnosis is reputed to be more difficult because the clinical picture tends to be masked by the symptoms and physical changes of pregnancy:
=> nausea, vomiting and abdominal discomfort of early pregnancy;
=> upward displacement of the appendix by the expanding uterus;
=> round ligament spasm, physiologic leukocytosis and elevated sedimentation rate.
If appendicitis is suspected, treatment is immediate surgical exploration. In most reports, the diagnosis is verified in about half of women who undergo surgical exploration.
Intravenous antimicrobial are given.If generalized peritonitis does not develop, then the prognosis is quite good.
Undiagnosed appendicitis often stimulates labor. In these cases , an acute surgical abdomen is encountered within a few postpartum hours.
When generalized peritonitis develops , cesarian delivery is indicated at the time of appendectomy.

Hepatitis A and pregnancy In developed countries the effects of HA on
pregnancy are not dramatic. However, at least in some underprivileged populations, both perinatal and maternal death are substantialy increased. Treatment consists of a well-balanced diet and diminished activity. Women with less severe illness may be managed as outpatients.
There is no evidence that HA virus is teratogenic. Risk of transmission to the fetus is negligible and to the newborn infant it is quite small. The risk of preterm birth appears to be increased.

Hepatitis B and pregnancy HB infection is a major cause of acute hepatitis
as well as its serious sequelae, namely chronic hepatitis, cirrhosis and hepatocellular carcinoma.
The course of HB infection in the mother does not seem to be altered by pregnancy.
The likelihood of preterm delivery is increased Transplacental viral transfer from the mother to
the fetus is rare. Instead, infection of the fetus or infant is by ingestion of infected material during delivery or exposure subsequent to birth. Some infected infants are asymptomatic but others develop fulminant disease and succomb. The majority (85%) become chronic carriers who can infect others.

Mothers with AgHBs and AgHBe are very likely to transmit the disease to their infants, whereas those who are negative for AgHBe but positive for AbHBe do not appear to transmit the infection.
Infection of the newborn whose mother chronically carries the virus can usually be prevented by the administration of HB immune globulin very soon after birth, followed promptly by HB vaccine.
For these reasons HB serological screening for all prenatal patients is recommended. If positive, and especially if e antigen is identified in the mother, the offspring should be given HB immune globulin and recombinant vaccine.

4.Diabetes
P. White classification (1978) was designed originally to prognosticate pregnancy outcome, because infant survival decreased with increasing severity of diabetes. The classification suggested by the American College of Obstetricians and Gynecologists (1986) relates the duration of diabetes to the severity of end- organ derangement, especially the eyes, kidneys, cardiovascular system.


Pregestational diabetes Diagnosis during pregnancy High plasma glucose levels, glucosuria and
ketoacidosis are elements of diagnosis. Women with only minimal metabolic derangement may be difficult to identify. In these cases diagnosis is based on:
=> strong familial history of diabetes; => large infants or unexplained fetal losses; => persistent glucosuria.

Effect of pregnancy on diabetes During pregnancy, control of diabetes is
usually made more difficult due to a variety of complications:
- nausea and vomiting may lead on the one hand to hypoglycemic shock
-infection during pregnancy commonly results in insulin resistance and ketoacidosis
-the exertion of labor may also result in troublesome hypoglicemia unless the amount of insulin given is reduced accordingly, or glucose is provided by intravenous infusion.
-after delivery, the need of exogenous insulin most often decreases .Hypoglycemic shock occurs more often in the immediate period following delivery than at any other time in pregnancy.

Effects of diabetes on pregnancy Maternal effects of diabetes include the
following : The likelihood of preeclampsia-eclampsia
is increased about four times. This incidence is increased even in the absence of demonstrated preexisting vascular or renal disease;
Some bacterial infections are more common in diabetic pregnancy;

Water balance is readily disturbed. Both fetal and maternal edema are common complications. Hydramnios occurs in 5 to 50% of diabetic mothers;
Excessive size of the infant (macrosomia) is so common a finding that unrecognized maternal diabetes should be suspected in patients who deliver babies weighing more than 4320g (9 pounds);
The rate of cesarean delivery is increased; Maternal mortality is increased because of the
complications of diabetes as well as an increased risk for hypertension, infection and operative delivery.

Fetal and neonatal effects : Stillbirth and neonatal death rates are
increased even with mild maternal diabetes. The risk of intrauterine fetal death rises sharply after the 36th week;
The incidence of preterm delivery in many cases induced because of hypertension, is increased two to three times.
Neonatal morbidity is common. Major congenital anomalies occur in 4% to 12%
of infants and include: anencephaly, spina bifida and hydrocephalus, cardiac anomalies (transposition of the great vessels, atrial and ventricular septal defects), situs inversus, renal anomalies. They occur primarily as a result of the influence of hyperglicemia on the developing embryo during the fifth to eighth week after conception.

Management during pregnancy The maternal glucose level should be kept
as close to normal as possible. The pregnancy should continue until the fetus is functionally mature, unless the intrauterine environment is deteriorating.
In general, glucosuria is a signal to evaluate carefully the plasma glucose levels.
A diet containing 25 to 30 cal/Kg of ideal body weight with a lower limit of 1,700 cal and a upper limit of 2,000 cal is prescribed (125g = 500 cal of protein, remainder of the calories equally divided between fat and carbohydrates).
Delivery Ideally, delivery of the overtly diabetic
woman should be accomplished near term.

Vaginal delivery is feasible if the diabetes is uncomplicated, the pelvis is normal, size of infant is not excessive and if the cervix is favorable for induction.
Cesarean section is indicated if: —> the disease is severe;
—> pregnancy complications exist; —> induction is unsuccessful; —> the progress in labor is poor; —> an excessive fetal size exist. Management of the newborn patient: => to prevent or reduce respiratory distress; => correction of acid-base abnormalities and
maintenance of optimal hydration, glucose levels and oxygenation are often critical matters;
=> treatment of hypocalcemia and hyperbilirubinemia.

Gestational diabetes Definition Gestational diabetes implies that this
disorder is induced by pregnancy, perhaps due to exaggerated physiological changes in glucose metabolism. At the Third International Workshop-Conference on Gestational Diabetes, held in Chicago in 1991, this disorder was defined as carbohydrate intolerance of variable severity with onset or first recognition during the current pregnancy.

Screening The American College of Obstetricians and
Gynecologists (1986) recommends screening only for women considered to be at risk:
-age over 30; -family history of diabetes; -a prior macrosomic, malformed or stillborn infant; -obesity, hypertension or glucosuria; -hydramnios and repeated abortions. The screen consists of a 50g oral glucose
load given without regard to the time of the last meal or the time of day. Venous plasma glucose is measured 1 hour later. A value greater than 140mg/dl is abnormal and dictates the performance of a standard glucose tolerance test.

Effects of diabetes on pregnancy => fetal anomalies are not increased; => class Al has not greater risk for fetal
death; => class A2 has been associated with
unexplained stillbirth similar to pregnancies complicated by overt diabetes (F.D.Johnstone et al, 1990);
=> higher incidence of macrosomic fetuses. Management Pregnant women without persistent
fasting hyperglicemia but with an abnormal oral glucose tolerance test (class Al) are treated typically by diet alone (that provide 30 to 35 kcal/ Kg of ideal body weight each day. Insulin should be added if the 2 hour blood glucose level cannot be kept within normal range prescribed diabetic diet

5.Infections
ACQUIRED IMMUNODEFICIENCY SYNDROME (AIDS)
The etiological agents of the immunodeficiency syndrome are human immunodeficiency viruses, HIV-1 and HIV-2, which are RNA retroviruses capable of inducing severe immunological dysfunction in T4 helper lymphocytes.
Pathogenesis The common denominator of AIDS is profound
immunosuppression, principally of cell-mediated immunity, which gives rise to a variety of opportunistic infections and neoplasms.

Clinical manifestations The incubation period is usually within days
to weeks. Acute illness is usually similar to other viral syndromes. After simptoms abates, the set-point of chronic viremia begins.
Screening Serological testing and counseling
should be offered to all pregnant women. Fetus-infant transmision Because trasplacental viral transfer is
thought to be the major mode of vertical transmission, at the present time there is no reason to think that cesarean delivery will decrease the incidence of peripartum transmission.

Schematic model of the natural history of HIV-1 infection

Management Counseling is mandatory for the HIV-positive
woman early in pregnancy, if possible. If she chooses to continue pregnancy, ongoing couseling for psychological support is important.
The American College of Obstetricians and Gynecologists recommends CD4 cell count determination during each trimester. If those are less 500/ml, consideration is given to Zidovudine therapy. This drug is well tolerated in pregnancy, without teratogenic effects when was given in early stages of gestation.
Those who perform or assist in vaginal or cesarean deliveries should wear gloves and gowns when handling the placenta or the infant until blood and amniotic fluid have been removed from the infant's skin .

TOXOPLASMOSIS Toxoplasma gondii is a protozoa which has a
complex life cycle . Toxoplasma infection results in the development of antibodies and cell-mediated immunity.
Clinical aspects Toxoplasmosis in pregnancy is often but not
invariably asymptomatic. When clinical findings are present, there is lymphadenopathy and malaise without fever. The posterior cervical nodes are most typically involved.More severe disease may involve the spleen, liver, myocardium, brain or lungs.
Up to 60% of acutely infected women transmit the organism to their offspring. There is no difference in the frequency of transmission of toxoplasmosis whether the mothers were symptomatic or not.

Effects on pregnancy The role of toxoplasmosis in the genesis of
human first-trimester abortions is minimal. The severely affected fetus may develop IUGR, nonimmune hydrops, hydrocephalus or microcephalus. Apparently normal neonates may develop problems later in life (neurologic and/or ophtalmologie sequelae).
Management The pregnant woman who has a positive
Toxoplasma titer on a TORCH screen must be counseled on the risk to the fetus. If the patient elects to continue her pregnancy, drug therapy should be initiated as soon as it is practical. Medical therapy has been estimated to reduce the risk of damage from infection by approximately 50%.

Spiramycin is an antibiotic that does not cross the placenta in significant amounts, reduces the risk of transmission to the fetus in the face of an acute maternal infection. It is recommended for use in acute maternal toxoplasmosis diagnosed before the third trimester. Treatment is continued throughout the remainder of pregnancy (500mg, six times daily, oral administration).
Pyrimethamine is an antimalarial drug, a folic acid antagonist, used to treat proven fetal infection. Folinic acid (calcium leucovorin) can be given with pyrimethamine to reduce its marrow toxicity. A recommended dose of pyrimethamine has been 50 to 100 mg orally (first day), followed by a maintenance dose of lmg/Kg every 3 to 4 days.
Sulfadiazine is also a folic acid antagonist (50 to 75mg/Kg of body weight, followed ty 50 to lOOmg/day in four divided doses).

SYPHILIS Antepartum syphilis can profoundly affect
pregnancy outcome by causing preterm labor, fetal death and neonatal infection. Fortunately is the most susceptible to therapy.
Fetal and neonatal infection Any stage of maternal syphilis may result in
fetal infection. Spirochetes readly cross the placenta but not so
often before 18 weeks of gestations. Diagnosis Maternal: VDRL,RPR,TP-PA. Fetal:... same in amniotic fluid and ultrasound. TreatmentPenicillin G 2.4 mil units with a second dose 1 week
after the first one


6.Neoplastic Diseases Breast carcinoma Breast cancer is the most common malignancy of
women of all age groups. Thus, it is not surprising that breast cancer is encountered with some frequency during pregnancy.
Effects of pregnancy on breast cancer A large number of breast cancers appear to be
estrogen or progesterone dependent. Theoretically at least, they should be more aggressive because of the hyperestrogenemia and hyperprogesteronemia that characterize normal pregnancy.
In reality, it appears that pregnancy does not exert much influence on the cause of mammary cancer, thus therapeutic abortion does not improve its prognosis.

Breast cancer

Although survival is stage-dependent, there may be serious delays in clinical assessment, because hormonally induced physiological breast changes tend to obscure breast masses and this is particularly evident during lactation when there is lobular hyperplasia and galactostasis.
Diagnosis and treatment The diagnostic approach in the pregnant woman with
a breast tumor is not different from that of a nonpregnant woman. Any suspicious breast mass found during pregnancy should prompt an aggressive plan to determine the cause, whether by mammography and fine-needle aspiration or by open biopsy. Magnetic resonance imaging and ultrasonography are reasonable alternatives .
Surgical treatment should not be delayed because of pregnancy- a modified radical mastectomy or a total mastectomy with axillary node dissection can be performed.

Radiotherapy is not recommended during pregnancy because abdominal scatter is considerable even with shielding.
Prophylactic oophorectomy during pregnancy is not indicated.
Patients who present with advanced breast carcinoma early in gestation frequently elect a termination of pregnancy. Termination of pregnancy facilitates the prompt administration of combination chemotherapy, which is indicated in premenopausal women. Later in pregnancy, systemic chemotherapy may be undertaken as the outcomes reported have generally been good in leukemic patients treated with agents similar to those employed for breast cancer.

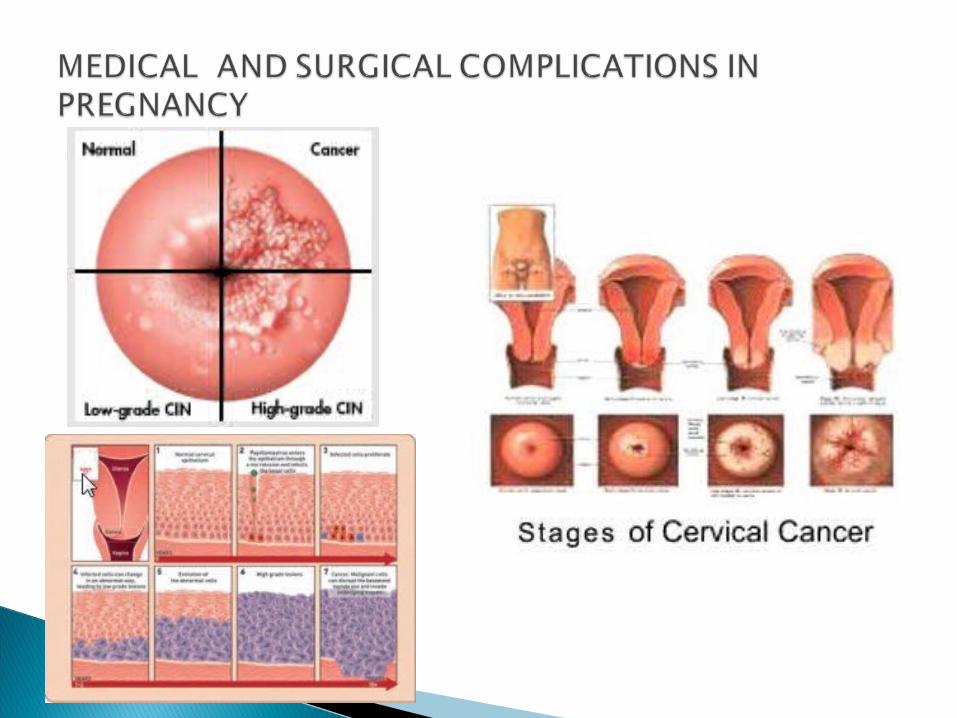
Cervical neoplasia It is the most common gynecologic malignancy
found in pregnant women. Intraepithelial neoplasia The effects of pregnancy and delivery on
premalignant and malignant epithelial cervical lesions are not understood completely and disagreement persists .
During pregnancy, endocervical curettage is omitted to avoid risks of hemorrhage and membrane rupture. Conization is avoided because of an increased incidence of hemorrhage, abortion and preterm labor. Other complications after a cone biopsy during pregnancy include infection, stenosis and laceration during delivery. Women with histologically confirmed intraepithelial neoplasia may be allowed to deliver vaginally and given definitive treatment after delivery.

Invasive carcinoma Pregnancy coexisting with invasive cervical
carcinoma complicates both staging and treatment. The survival rate for invasive carcinoma has not been profoundly different for pregnant and nonpregnant women within a given stage of disease. When frankly invasive carcinoma is identified, most favor delivery by the abdominal route.
Treatment Once the diagnosis has been established, patients
with carcinoma in situ and, in some instances, microinvasive disease, may be followed to term without further therapy. In patients continuing pregnancy, cytologic and colposcopic examinations should be performed periodically to rule out progression of the disease.

Definitive therapy, using cryosurgery or laser, may be accomplished in the postpartum period for patients with cervical intraepithelial neoplasia.
Invasive cancer demands relatively prompt therapy. In general, during the first half of pregnancy, immediate treatment is advised, whereas during the later half a reasonable option is to await fetal maturity.
Preferred treatment for patients with stage lb and early stage IIa invasive carcinoma is radical hysterectomy plus bilateral pelvic lymphadenectomy. Surgical treatment allows ovarian conservation and vaginal function and minimizes exposure at an early age to the adverse effects of radiation on the intestinal and urinary tracts.
Before 20 weeks, hysterectomy is usually performed with the fetus in utero.

Radiotherapy is given for more extensive cancer.
Cesarean section is the preferred method of delivery and it is performed prior to surgical treatment or radiation therapy when fetal pulmonary maturation is documented (pulmonary maturation may occur at 32 to 34 weeks gestation, particularly if corticosteroids have been administered).
Prognosis The overall prognosis for all stages of cervical
cancer dining pregnancy is probably similar to that for nonpregnant women

Ovarian tumors in pregnancy Ovarian neoplasms occur once in every 500 to 1,000
pregnancies. Their existence may be unsuspected before the prenatal examination, at which time the finding of an ovarian enlargement may present considerable diagnostic and therapeutic difficulties.
Diagnosis The ovary containing the corpus luteum may be
enlarged during the firsr trimester but on reexamination at 2 or 3 week intervals it becomes progressively smaller after the eighth to tenth week of pregnancy.
True ovarian neoplasms are usually larger than 5cm in diameter and do not decrease in size on repeated examinations.

Ovarian cancer

Discovery of an adnexal mass is much easier if the first prenatal pelvic examination is performed in the first trimester. As pregnancy advances, an ovarian cyst is displaced by the enlarged uterus. Sonography may be helpful.
Complications and management Torsion is the most common complication and
may lead to rupture. The symptoms are acute, with sudden onset of abdominal pain, vomiting and pyrexia. Pelvic examination will reveal a tender cystic mass and the distinction from tubal pregnancy may be possible.
Pressure symptoms may arise if the cyst becomes incarcerated in the pelvis or it is of very large size. These will include dysuria, pain, abdominal distension.
Suppuration is most likely in the puerperium as a result of trauma sustained during delivery.

There is an increased tendency to spontaneous abortion if the cyst is large. A cyst in the pelvis will obstruct labor, causing malpresentation or non-engagement of the head.
Immediate removal of the cyst is necessary, regardless of the stage of pregnancy if symptoms of torsion or hemorrhage arise or if rapid growth of the mass is detected.
Cesarean section and tumorectomy are preferable. Whereas in most advanced stages hysterectomy and
bilateral adnexectomy is indicated, in certain circumstances it can be justified to remove the tumor and await fetal maturity.
There does not appear to be an adverse influence of pregnancy on ovarian cancer. Because of the relatively young age of the pregnant population, there is a higher proportion of less-advanced tumors.
7.Uterine fibromyomas The coexistence of uterine fibromyomas and
pregnancy is relatively common. Small tumors are of little consequence unless their location is submucous, in which case the abortion rate is almost doubled.
Although tumors of any size may produce symptoms of pain or pressure, surgical intervention is rarely necessary during pregnancy.
Diagnosis The main problem in diagnosis is the recognition of
the existence of pregnancy in a fibroid uterus. This is particularly difficult when implantation bleeding or threatened abortion complicates the early course. A pregnancy test or sonography are useful.

Uterine fibroma and pregnancy

Complications and management Degenerative changes are likely to occur during
pregnancy, the hemorrhagic variety (red degeneration) being the most common. Pain, local tenderness and slight elevation of temperature are the usual symptoms.
Myomectomy is rarely necessary and is frequently followed by abortion if the uterine wall is incised. An exception is a pedunculated subserous tumor, which may twist and become necrotic as the uterus enlarges and rises out of the pelvis. If torsion occurs, laparotomy is imperative before gangrenous changes and peritonitis develop. This type of tumor can be usually removed without invading the myometrium.

The major complications resulting from fibroids arise during labor and delivery:
=> obstruction of the birth canal; => an increased incidence of dysfunctional labor; => fetal malpositions; => faulty placental separation: => hemorrhage following delivery. Tumors blocking the inlet may make cesarean
section necessary. Those situated low in the anterior wall are usually
pulled up out of the pelvis as the lower uterine segment lengthens. If the tumor is placed posteriorly in the hollow of the sacrum, elevation may be prevented by the promontory of the sacrum.

Vaginal examination should be performed early in labor before deciding on the route of delivery. If the birth canal is not obstructed and the fetal position does not preclude vaginal delivery, a trial of labor should be given.
Occasionally, the presence of fibroids alters uterine contractility and induces dysfunctional labor or hemorrhage following delivery.
If cesarean section is necessary because of pelvic obstruction or abnormal labor, hysterectomy may or may not be indicated, but generally myomectomy should not be done because of hemorrhage.
The blood supply to uterine myomas may be reduced suddenly, during the puerperium. Laparotomy is indicated if symptoms of degeneration develop and persist during the stage of uterine involution.


















