Do you feel lucky? Real Risk of Ectasia High Risk LASIK ... · Belin/Ambrosio Enhanced Ectasia...
17
Slide 1 High Risk LASIK Patients Do you feel lucky? Derek N. Cunningham, OD, FAAO Slide 2 Traditional Risk Assessment • Randelman Scale – What’s the point • Topography (unilateral keratoconics?) • Residual stromal bed (only measured in very few cases, mostly calculated) • Age? • Preoperative corneal thickness • Preoperative spherical equivalent Slide 3 Real Risk of Ectasia Slide 4 Slide 5 Professor H. Burkhard Dick Dr. Michael C Knorz Dr. Colman Kraff Dr. Marguerite McDonald Dr. Stephen Slade Dr. John A. Vukich Dr. Steve Schallhorn Professor Jan Venter Dr. Mitchell C Brown Dr. Stephen Coleman Dr. Joseph Colin Dr. Steven J. Dell Slide 6 Enormous Dataset Statistical Significance… • 109,924 consecutive LVC Treatments (60,071 Patients) from April 1st, 2010 to June 30th, 2011. • Follow-up availability as follows: 1 Week 79,695 (72.5%) – 1 Month 78,266 (71.2%) – 3 Month 54,083 (49.2%) – 6 Month 21,655 (19.7%) • Preoperative Refractive Stratification as follows: – Low/Mod Myopia 85,905 (78.2%) – High Myopia 5,365 (4.9%) – Low/Mod Hyperopia 12,675 (11.5%) – High Hyperopia 2,159 (2.0%) – Mixed Astigmatism 3,820 (3.5%)
Transcript of Do you feel lucky? Real Risk of Ectasia High Risk LASIK ... · Belin/Ambrosio Enhanced Ectasia...
Slide 1 High Risk LASIK Patients
Do you feel lucky?
Derek N. Cunningham, OD, FAAO
Slide 2 Traditional Risk Assessment
• Randelman Scale
– What’s the point
• Topography (unilateral keratoconics?)
• Residual stromal bed (only measured in very few cases, mostly calculated)
• Age?
• Preoperative corneal thickness
• Preoperative spherical equivalent
Slide 3 Real Risk of Ectasia
Slide 4
Slide 5
Professor H. Burkhard DickDr. Michael C KnorzDr. Colman KraffDr. Marguerite McDonaldDr. Stephen SladeDr. John A. Vukich
Dr. Steve SchallhornProfessor Jan VenterDr. Mitchell C BrownDr. Stephen ColemanDr. Joseph ColinDr. Steven J. Dell
Slide 6 Enormous Dataset
Statistical Significance…
• 109,924 consecutive LVC Treatments (60,071 Patients) from April 1st, 2010 to June 30th, 2011.
• Follow-up availability as follows: 1 Week 79,695 (72.5%) – 1 Month 78,266 (71.2%) – 3 Month 54,083 (49.2%) – 6 Month 21,655 (19.7%)
• Preoperative Refractive Stratification as follows:– Low/Mod Myopia 85,905 (78.2%) – High Myopia 5,365 (4.9%) – Low/Mod Hyperopia 12,675 (11.5%) – High Hyperopia 2,159 (2.0%) – Mixed Astigmatism 3,820 (3.5%)
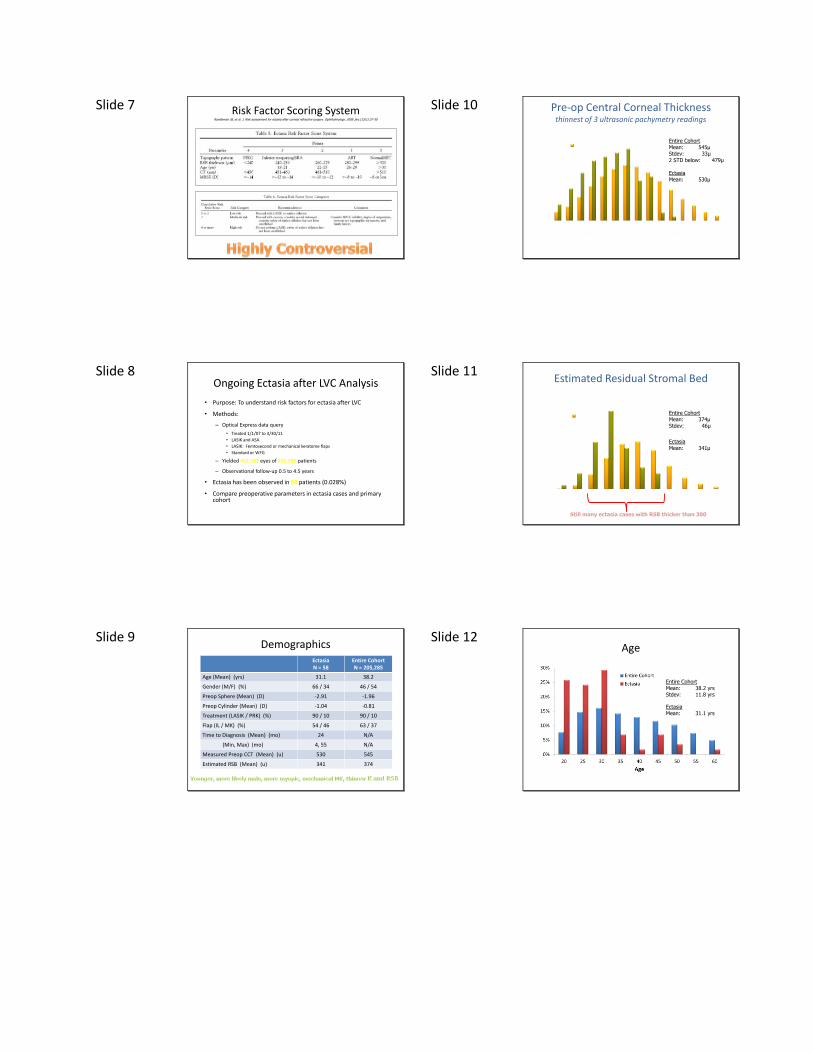
Slide 7 Risk Factor Scoring SystemRandleman JB, et al. J. Risk assessment for ectasia after corneal refractive surgery. Ophthalmology. 2008 Jan;115(1):37-50
Slide 8 Ongoing Ectasia after LVC Analysis
• Purpose: To understand risk factors for ectasia after LVC
• Methods:
– Optical Express data query
• Treated 1/1/07 to 4/30/11
• LASIK and ASA
• LASIK: Femtosecond or mechanical keratome flaps
• Standard or WFG
– Yielded 402,583 eyes of 205,285 patients
– Observational follow-up 0.5 to 4.5 years
• Ectasia has been observed in 58 patients (0.028%)
• Compare preoperative parameters in ectasia cases and primary cohort
Slide 9 Demographics
EctasiaN = 58
Entire CohortN = 205,285
Age (Mean) (yrs) 31.1 38.2
Gender (M/F) (%) 66 / 34 46 / 54
Preop Sphere (Mean) (D) -2.91 -1.96
Preop Cylinder (Mean) (D) -1.04 -0.81
Treatment (LASIK / PRK) (%) 90 / 10 90 / 10
Flap (IL / MK) (%) 54 / 46 63 / 37
Time to Diagnosis (Mean) (mo) 24 N/A
(Min, Max) (mo) 4, 55 N/A
Measured Preop CCT (Mean) (u) 530 545
Estimated RSB (Mean) (u) 341 374
Slide 10 Pre-op Central Corneal Thickness thinnest of 3 ultrasonic pachymetry readings
Entire CohortMean: 545µStdev: 33µ2 STD below: 479µ
EctasiaMean: 530µ
Slide 11 Estimated Residual Stromal Bed
Entire CohortMean: 374µStdev: 46µ
EctasiaMean: 341µ
Still many ectasia cases with RSB thicker than 300
Slide 12 Age
Entire CohortMean: 38.2 yrsStdev: 11.8 yrs
EctasiaMean: 31.1 yrs
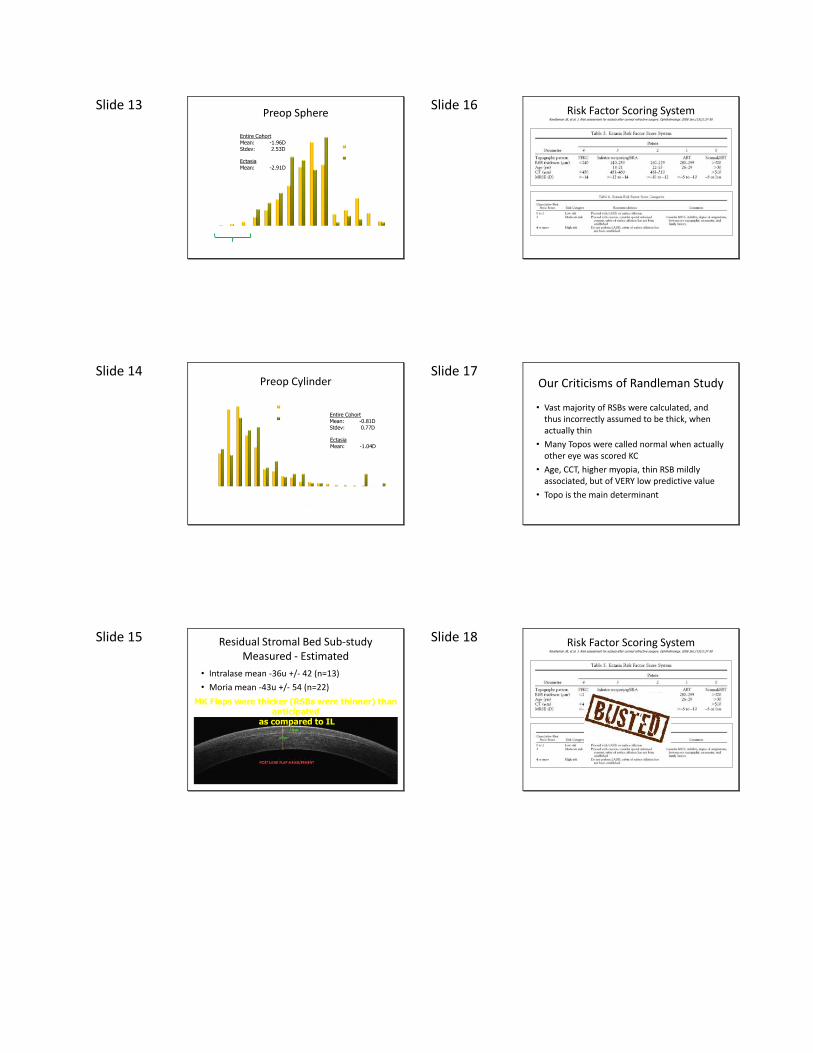
Slide 13 Preop Sphere
Entire CohortMean: -1.96DStdev: 2.53D
EctasiaMean: -2.91D
Slide 14 Preop Cylinder
Entire CohortMean: -0.81DStdev: 0.77D
EctasiaMean: -1.04D
Slide 15 Residual Stromal Bed Sub-studyMeasured - Estimated
• Intralase mean -36u +/- 42 (n=13)
• Moria mean -43u +/- 54 (n=22)
MK Flaps were thicker (RSBs were thinner) than anticipated
as compared to IL
Slide 16 Risk Factor Scoring SystemRandleman JB, et al. J. Risk assessment for ectasia after corneal refractive surgery. Ophthalmology. 2008 Jan;115(1):37-50
Slide 17 Our Criticisms of Randleman Study
• Vast majority of RSBs were calculated, and thus incorrectly assumed to be thick, when actually thin
• Many Topos were called normal when actually other eye was scored KC
• Age, CCT, higher myopia, thin RSB mildly associated, but of VERY low predictive value
• Topo is the main determinant
Slide 18 Risk Factor Scoring SystemRandleman JB, et al. J. Risk assessment for ectasia after corneal refractive surgery. Ophthalmology. 2008 Jan;115(1):37-50
Slide 19 Ocular asymmetry
• Relative scales
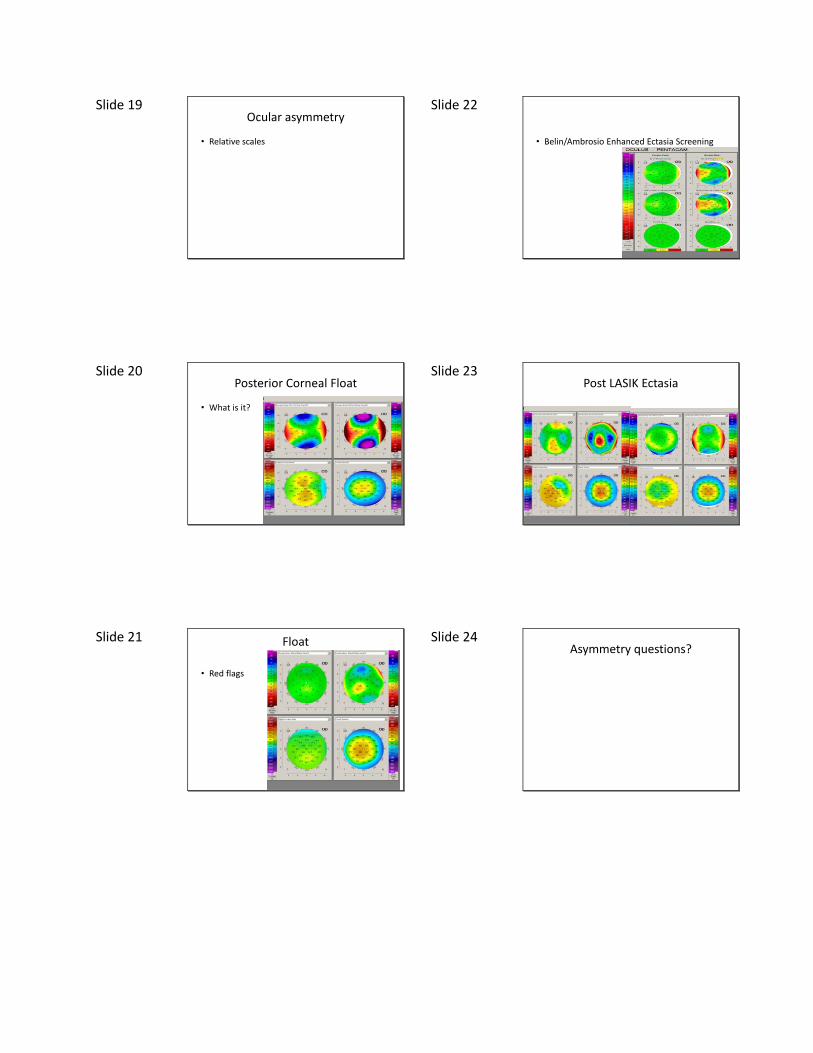
Slide 20 Posterior Corneal Float
• What is it?
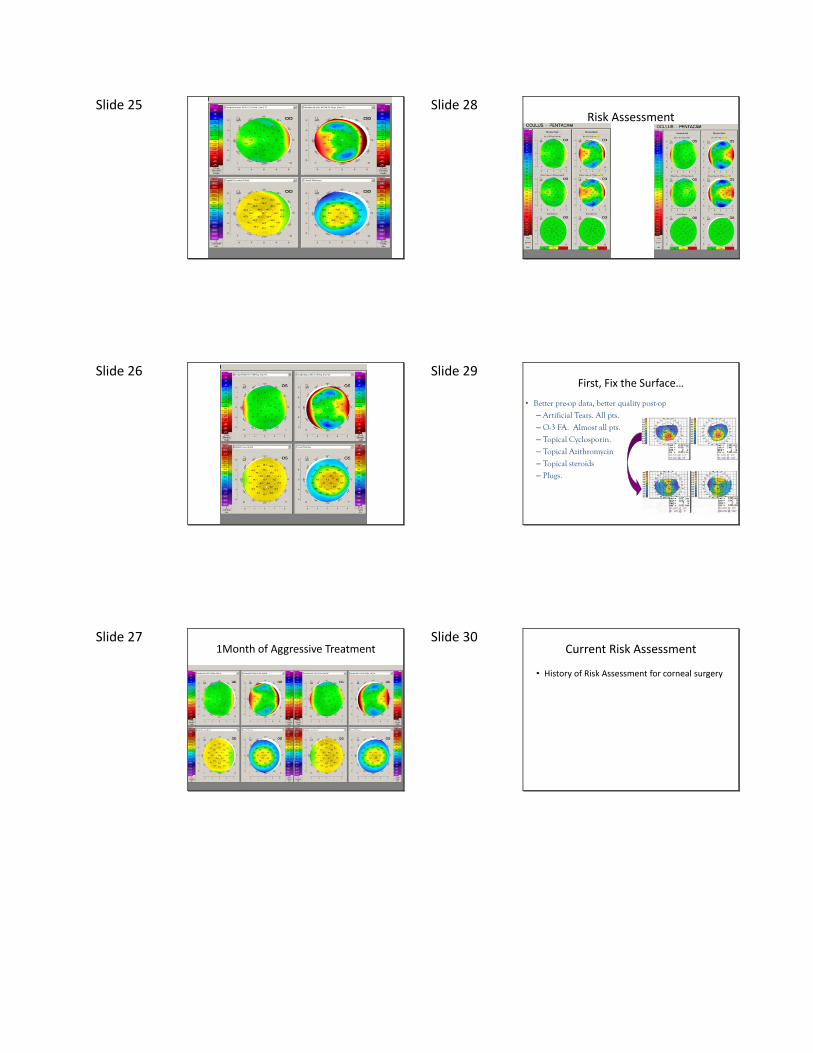
Slide 21 Float
• Red flags
Slide 22
• Belin/Ambrosio Enhanced Ectasia Screening
Slide 23 Post LASIK Ectasia
Slide 24 Asymmetry questions?
Slide 25
Slide 26
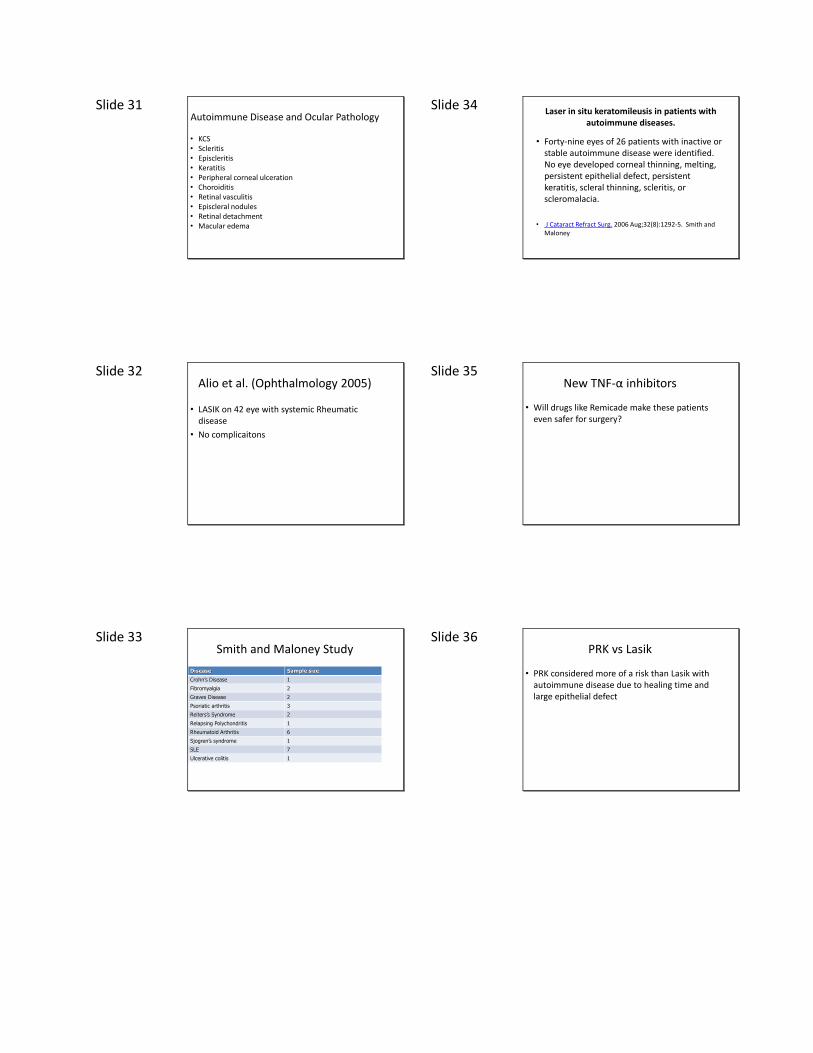
Slide 27 1Month of Aggressive Treatment
Slide 28 Risk Assessment
Slide 29 First, Fix the Surface…
• Better pre-op data, better quality post-op
– Artificial Tears. All pts.
– O-3 FA. Almost all pts.
– Topical Cyclosporin.
– Topical Azithromycin
– Topical steroids
– Plugs.
Slide 30 Current Risk Assessment
• History of Risk Assessment for corneal surgery
Slide 31 Autoimmune Disease and Ocular Pathology
• KCS• Scleritis• Episcleritis• Keratitis• Peripheral corneal ulceration• Choroiditis• Retinal vasculitis• Episcleral nodules• Retinal detachment• Macular edema
Slide 32 Alio et al. (Ophthalmology 2005)
• LASIK on 42 eye with systemic Rheumatic disease
• No complicaitons
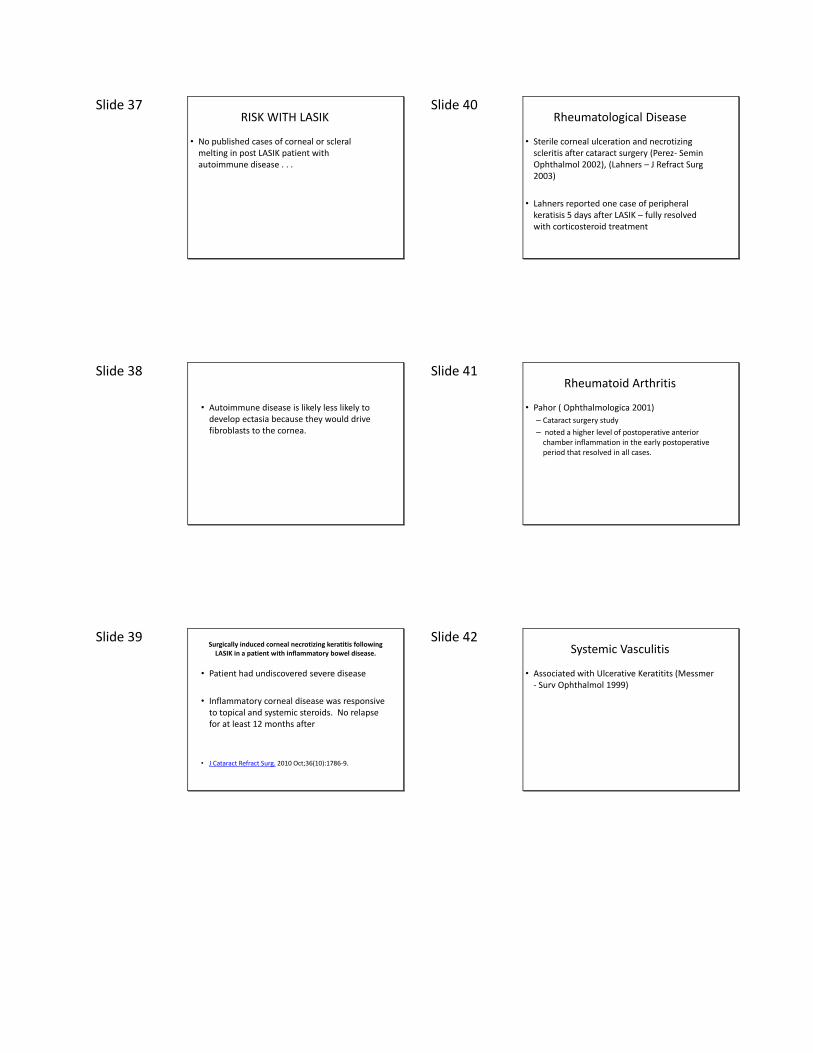
Slide 33 Smith and Maloney Study
Disease Sample size
Crohn’s Disease 1
Fibromyalgia 2
Graves Disease 2
Psoriatic arthritis 3
Reiters’s Syndrome 2
Relapsing Polychondritis 1
Rheumatoid Arthritis 6
Sjogren’s syndrome 1
SLE 7
Ulcerative colitis 1
Slide 34 Laser in situ keratomileusis in patients with
autoimmune diseases.
• Forty-nine eyes of 26 patients with inactive or stable autoimmune disease were identified. No eye developed corneal thinning, melting, persistent epithelial defect, persistent keratitis, scleral thinning, scleritis, or scleromalacia.
• J Cataract Refract Surg. 2006 Aug;32(8):1292-5. Smith and Maloney
Slide 35 New TNF-α inhibitors
• Will drugs like Remicade make these patients even safer for surgery?
Slide 36 PRK vs Lasik
• PRK considered more of a risk than Lasik with autoimmune disease due to healing time and large epithelial defect
Slide 37 RISK WITH LASIK
• No published cases of corneal or scleralmelting in post LASIK patient with autoimmune disease . . .
Slide 38
• Autoimmune disease is likely less likely to develop ectasia because they would drive fibroblasts to the cornea.
Slide 39 Surgically induced corneal necrotizing keratitis following
LASIK in a patient with inflammatory bowel disease.
• Patient had undiscovered severe disease
• Inflammatory corneal disease was responsive to topical and systemic steroids. No relapse for at least 12 months after
• J Cataract Refract Surg. 2010 Oct;36(10):1786-9.
Slide 40 Rheumatological Disease
• Sterile corneal ulceration and necrotizing scleritis after cataract surgery (Perez- Semin Ophthalmol 2002), (Lahners – J Refract Surg 2003)
• Lahners reported one case of peripheral keratisis 5 days after LASIK – fully resolved with corticosteroid treatment
Slide 41 Rheumatoid Arthritis
• Pahor ( Ophthalmologica 2001)
– Cataract surgery study
– noted a higher level of postoperative anterior chamber inflammation in the early postoperative period that resolved in all cases.
Slide 42 Systemic Vasculitis
• Associated with Ulcerative Keratitits (Messmer - Surv Ophthalmol 1999)
Slide 43 Autoimmune Disease With Strong Association to Corneal Melting
• Wegener’s Granulomatosis
• Relapsing polychondritis
• Polyarteritis nodosa
Slide 44 Autoimmune Disease With a Loose Association to Corneal Melting
• SLE
• Crohn’s disease
• Ulcerative colitis
Slide 45 Autoimmune Disease With No Associated Corneal Melting
• Hashimoto’s disease
• Reiter’s syndrome
• Fibromyalgia
Slide 46 Autoimmune disease indirectly linked to corneal ulceration
• Graves – lagophthalmos and exposure can cause problems
• Scleroderma – lagophthalmos or severe malnutrition
Slide 47 Liability
• LASIK may not be clinically contraindicated in patients with autoimmune disease, but the FDA labels it as such.
Slide 48 Post-op Treatment
• Any post-op complication should be treated aggressively (like epithelial ingrowth)
Slide 49 Cobo-Soriano (Ophthalmology 2006)
DX # 0f eyes
Rheumatiod Arthiritis 29
SLE 31
Spondylitis 2
Psoriasis 91
Crohn’s Disease/UC 67
Keloids 18
Diabetes Mellitus 44
Immunosuppressicve therapy 56
Slide 50 Recurrent Uveitis
• Patients at high risk of developing recurrent flares of acute anterior uveitis, such as those with spondyloarthropathies should be carefully considered
• A patient developed acute DLK three years after LASIK while he was having an recurrent acute anterior uveitis attack (Diaz-Valle – J Refract Surg 2009)– Treated with good results
Slide 51
Slide 52 Diabetes and Eye Disease
• Diabetic Keratopathy
– SPK
– Recurrent corneal erosions
– Neurotrophic keratopaty
– Tear dysfunction
– Endothelial dysfunction
• Increased risk of infection
Slide 53 Diabetes and LASIK
• Shown to be safe if patient is well controlled
Slide 54 Nerve Regeneration
• Topical cyclosporine significantly improved corneal sensitivity at 3 months post LASIK (Peyman – J Refract Surg 2008)
• Suggests that Restasis may enhance nerve regeneration
Slide 55 New Study on Nerve Regeneration
• Allergan Post Lasik study
Slide 56 Risk Lasik vs Contact lens wearMcGee – J Cataract Refract Surg 2009
• Risk to eye health and permanent vision loss
• RGPs are still safer than LASIK
• Daily wear lenses are equally safe to LASIK (ONLY IF THE PATIENT IS 100% COMPLIENT)
• Extended wear carries more patient risk than LASIK
Slide 57 Diabetes
• Stability Issues
• Protective against ectasia?
Slide 58 Herpes
• Simplex vs Zoster
Slide 59 Laser in situ keratomileusis in patients with a
history of ocular herpes.
• Laser in situ keratomileusis was safe in patients with a history of ocular herpes
• inactive for 1 year before surgery
• perioperative systemic antiviral prophylaxis
• J Cataract Refract Surg. 2007 Nov;33(11):1855-9.
Slide 60 Herpes
• Dormancy
Slide 61 Hx of Keloid Scarring
Slide 62 Systemic Meds
• General precautions
• Obtaining clearance
Slide 63 Steroids
Slide 64 Immunosuppressants
Slide 65 Accutane
• Lack published reports of complications with LASIK.
• Don’t test it.
• Accutane = severe dry eye (temporary)• Decrease photoreceptor turnover (night blindness)
• LASIK = possible dry eye (femto probably not)
Slide 66 Imitrex and LASIK
• Triptans and the incidence of epithelial defects during laser in situ keratomileusis.
• There is no correlation between the use of sumatriptan for relief of migraine headaches and the generation of epithelial defects during LASIK. There appears to be no reason to stop triptans before proceeding with LASIK.
• J Refract Surg. 2005 Jan-Feb;21(1):72-6.
Slide 67 Patient Populations
• Be careful of generalizing patients
Slide 68 Pregnancy
• Decreased Corneal sensitivity
• Increased corneal thickness and curvature
Slide 69 Amblyopes
Slide 70 Monocular Patients
Slide 71 Ocular Surface DX
• Liability vs Results
Slide 72 Blepharitis
Slide 73 Dry Eye
• Severity Scale
Slide 74
Slide 75
Slide 76 Dry Eye
• How dry is too dry?
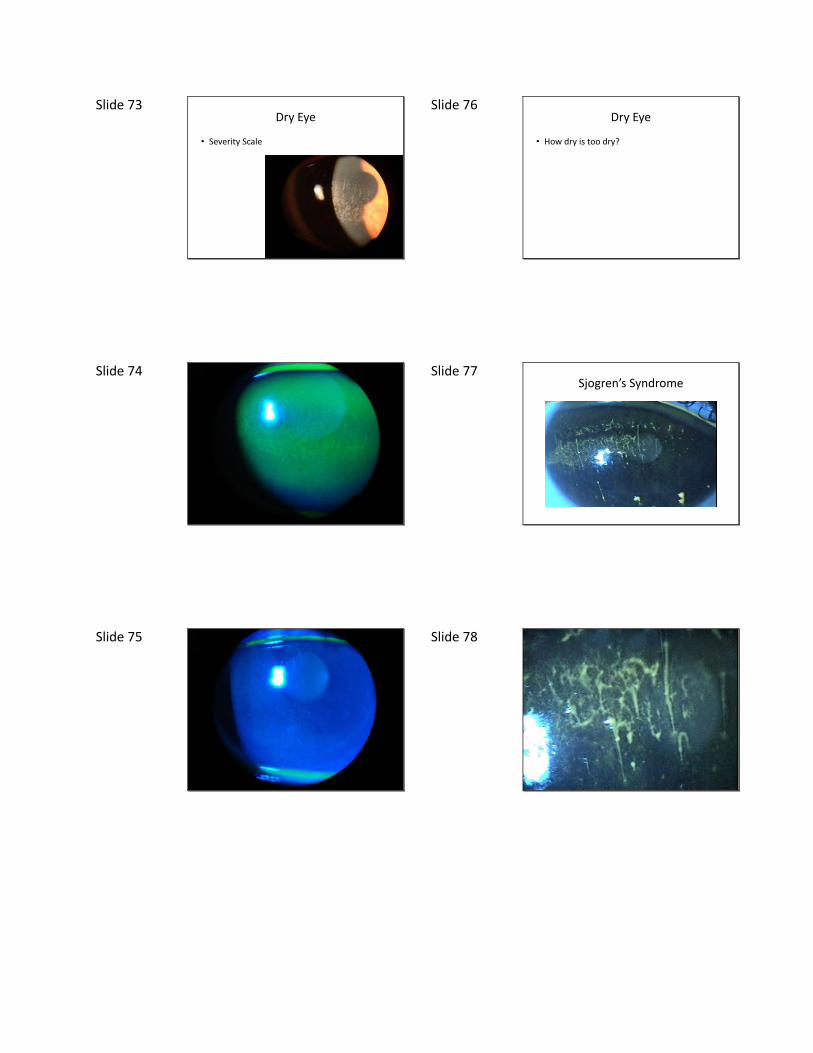
Slide 77 Sjogren’s Syndrome
Slide 78
Slide 79 Allergy
• Atopic disease has been historically linked to DLK, haze and myopic regression after PRK (Yang – AmJ Ophthalmol 1998)
Slide 80 Comorbidities and Flap Stability
• Does ocular surface disease decrease flap stability
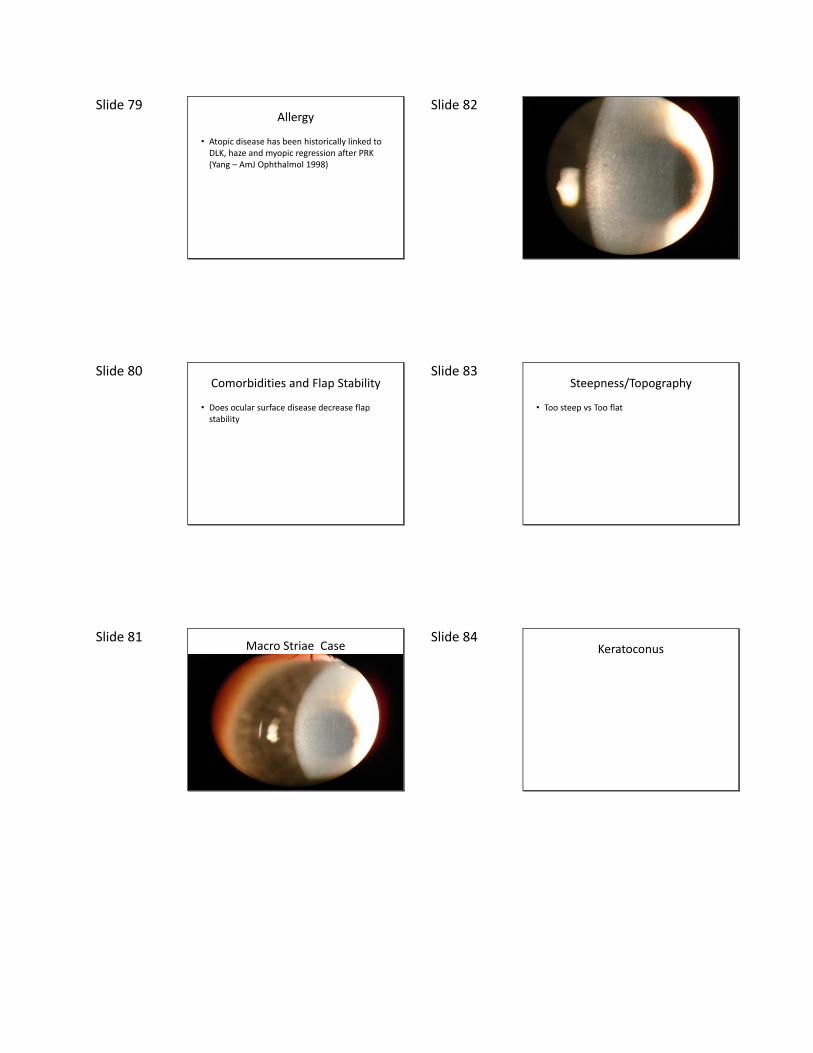
Slide 81 Macro Striae Case
Slide 82
Slide 83 Steepness/Topography
• Too steep vs Too flat
Slide 84 Keratoconus
Slide 85 Keratoconus
• LASIK with Riboflavin
Slide 86 Forme Fruste KK
• Do We Dare?
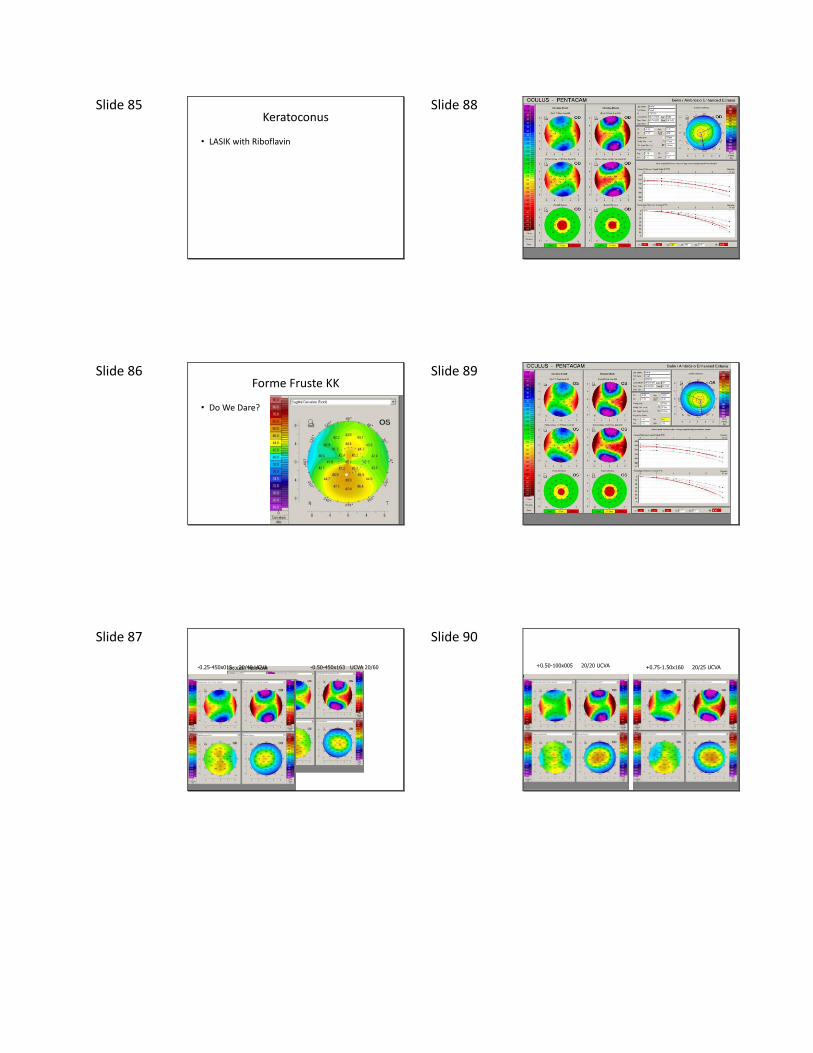
Slide 87
-0.25-450x015 20/40 UCVA -0.50-450x163 UCVA 20/60
Slide 88
Slide 89
Slide 90
+0.50-100x005 20/20 UCVA +0.75-1.50x160 20/25 UCVA
Slide 91
Slide 92
Slide 93 Recurrent Corneal Erosions
• Are they ever stable?
• How bad can they get?
Slide 94 Recurrent Corneal Erosions
• Perisurgical prophylaxis
Slide 95 Previous RK
• LASIK vs Surface Ablation
Slide 96