Disruptive Communication Among the Interdisciplinary Team ...
100
Pittsburg State University Pittsburg State University Pittsburg State University Digital Commons Pittsburg State University Digital Commons Doctor of Nursing Practice Irene Ransom Bradley School of Nursing Spring 2021 Disruptive Communication Among the Interdisciplinary Team: Disruptive Communication Among the Interdisciplinary Team: Gaining Insight and Providing Nurse Education Gaining Insight and Providing Nurse Education Kristen Marie Anderson Pittsburg State University, [email protected] Follow this and additional works at: https://digitalcommons.pittstate.edu/dnp Part of the Adult and Continuing Education Commons, Educational Assessment, Evaluation, and Research Commons, Health Communication Commons, Interprofessional Education Commons, Nursing Administration Commons, and the Other Nursing Commons Recommended Citation Recommended Citation Anderson, Kristen Marie, "Disruptive Communication Among the Interdisciplinary Team: Gaining Insight and Providing Nurse Education" (2021). Doctor of Nursing Practice. 45. https://digitalcommons.pittstate.edu/dnp/45 This Scholarly Project is brought to you for free and open access by the Irene Ransom Bradley School of Nursing at Pittsburg State University Digital Commons. It has been accepted for inclusion in Doctor of Nursing Practice by an authorized administrator of Pittsburg State University Digital Commons. For more information, please contact [email protected].
Transcript of Disruptive Communication Among the Interdisciplinary Team ...

Pittsburg State University Pittsburg State University
Pittsburg State University Digital Commons Pittsburg State University Digital Commons
Doctor of Nursing Practice Irene Ransom Bradley School of Nursing
Spring 2021
Disruptive Communication Among the Interdisciplinary Team: Disruptive Communication Among the Interdisciplinary Team:
Gaining Insight and Providing Nurse Education Gaining Insight and Providing Nurse Education
Kristen Marie Anderson Pittsburg State University, [email protected]
Follow this and additional works at: https://digitalcommons.pittstate.edu/dnp
Part of the Adult and Continuing Education Commons, Educational Assessment, Evaluation, and
Research Commons, Health Communication Commons, Interprofessional Education Commons, Nursing
Administration Commons, and the Other Nursing Commons
Recommended Citation Recommended Citation Anderson, Kristen Marie, "Disruptive Communication Among the Interdisciplinary Team: Gaining Insight and Providing Nurse Education" (2021). Doctor of Nursing Practice. 45. https://digitalcommons.pittstate.edu/dnp/45
This Scholarly Project is brought to you for free and open access by the Irene Ransom Bradley School of Nursing at Pittsburg State University Digital Commons. It has been accepted for inclusion in Doctor of Nursing Practice by an authorized administrator of Pittsburg State University Digital Commons. For more information, please contact [email protected].

DISRUPTIVE COMMUNICATION AMONG THE INTERDISCIPLINARY TEAM:
GAINING INSIGHT AND PROVIDING NURSE EDUCATION
A Scholarly Project Submitted to the Graduate School
in Partial Fulfillment of the Requirements
for the Degree of
Doctor of Nursing Practice
Kristen Marie Anderson
Pittsburg State University
Pittsburg, Kansas
May 2021

ii
ACKNOWLEDGEMENTS
I would like to thank Dr. Kristi Frisbee for her support, guidance, and patience. I would
also like to thank Dr. Amanda Alonzo, Dr. Alicia Mason Collins, and Dr. Amy Hite for
their valuable insight and recommendations to improve this research project. I truly
appreciate the two participating hospitals and all of the nurses for agreeing to contribute
to the study. Finally, I would like to thank my family for their unconditional love and
support throughout my graduate education.

iii
DISRUPTIVE COMMUNICATION AMONG THE INTERDISCIPLINARY TEAM:
GAINING INSIGHT AND PROVIDING NURSE EDUCATION
An Abstract of the Scholarly Project by
Kristen Anderson, BSN, RN
The purpose of this study is to identify what types of disruptive behavior nurses
are experiencing, discuss outcomes of disruptive behavior, and educate healthcare
providers and administrators of disruptive communication. Understanding the
consequences of disruptive communication can help educators articulate the need for
training in conflict management and therapeutic communication methods. It can also aid
healthcare providers to be more conscious of their behavior in the professional setting.
Seven research questions related to communication were developed and analyzed in this
study. The author developed a pre-education survey that included demographics,
multiple-choice questions, and open-ended questions to assess the nurses' knowledge and
feelings regarding disruptive communication in a mixed-method, cross-sectional design
to evaluate knowledge and hear the voice of the participant. The post-education
questionnaire included multiple-choice questions, assessing the nurses' feelings toward
addressing disruptive behavior. Statistical analysis was utilized to calculate the
frequency, percent, and mean of quantitative data. This study contributes to nursing
knowledge, supporting the need for positive communication techniques, revealing
adverse outcomes from disruptive communication, and discussing the need for continuing
education. Effective communication can contribute to the capstone of healthcare: patient
safety and high-quality care. Therefore, continuing education, institutional policy, and

iv
legislative policy need to be implemented to improve communication among the
interdisciplinary team.

v
TABLE OF CONTENTS
CHAPTER………………………………………….......……………………………PAGE
I. INTRODUCTION………………………………..……………………………………..1
Introduction…………………………………..……………………………………1
Description of the Clinical Problem/Issue…………..…………………………….2
Significance………………………………………...………………………...……3
Specific Aims/Purpose…………………………….......…………….....………….4
Theoretical Framework………………………...….......………….………….....…4
Communication Accommodation Theory………………………………...5
Social Exchange Theory…….…………………………………………….5
Orchestra Theory………………………………………………………….6
Project Questions……………………………………….......……………..….…...7
Definition of Key Terms……………………………….......………………..…….7
Logic Model………………………………………………...……………..………8
Summary…………………………………………….......…………………..…….9
II. REVIEW OF THE LITERATURE……………………………...……………………11
Literature Synthesis………………………………..…………….....……………12
Qualities Related to Poor Communication Methods……......………..………….13
Communication Differences………………………......……………...….13
Disruptive Behaviors and Hierarchies……………......………………….14
Satisfaction of the Interdisciplinary Team………………......…………………...16
Physician Satisfaction………………………………….…….....………..16
Nurse Satisfaction…………………………......…………………………17
Patient and Family Satisfaction……………….....………………….…...18
Methods to Improve Communication....................................................................19
Frequent Physician-Nurse Interactions......................................................19
Education...............................................................................................................20
SBAR.....................................................................................................................21
Face-To-Face Communincation.................................................................21
Poor Communication and Patient Outcomes.........................................................22
Summary................................................................................................................22
III. METHODOLOGY......................................................................................................25
Project Design........................................................................................................25
Project Site and Population....................................................................................27
Ethical Considerations/Protection of Human Subjects..........................................28
Instruments.............................................................................................................29
Content Validity.....................................................................................................31
Analytical Methods................................................................................................31
Procedure...............................................................................................................31

vi
Budget....................................................................................................................33
Strengths and Weaknesses of the Project...............................................................33
Summary................................................................................................................34
IV. EVALUATION RESULTS.........................................................................................35
Purpose...................................................................................................................35
Sample....................................................................................................................36
Description of Key Terms/Variables.....................................................................39
Analysis of Project Questions................................................................................39
Knowledge Gain....................................................................................................46
Additional Statistical Analysis...............................................................................47
Summary................................................................................................................50
V. DISCUSSION...............................................................................................................52
Relationship of Outcomes to Research..................................................................52
Observations..........................................................................................................56
Evaluation of Theoretical Framework...................................................................56
Evaluation of the Logic Model..............................................................................59
Limitations.............................................................................................................60
Implications for Future Projects/Research.............................................................62
Implications for Practice/Health Policy/Education................................................62
Conclusion.............................................................................................................63
REFERENCES..................................................................................................................65
APPENDICES...................................................................................................................70

vii
LIST OF TABLES
TABLE………………………………………………………………………………PAGE
Table 1. Total Years of Experience...................................................................................37
Table 2. Current Unit……………………….....................................................................38
Table 3. Current Shift........................................................................................................38
Table 4. Types of Disruptive Behavior..............................................................................40
Table 5. How Often Disruptive Behavior is Witnessed.....................................................41
Table 6. A Patient was Placed in a Dangerous Situation due to Disruptive
Communication…………………………………………………………………………..42
Table 7. A Patient Experienced Harm due to Disruptive
Communication…………………………………………………………………..…........42
Table 8. Level of Satisfaction……………........................................................................44
Table 9. Perception of Disruptive Behavior’s Effect on Job Satisfaction.........................44
Table 10. Confidence Level Before Educational Offering................................................45
Table 11. Confidence Level After Educational Offering...................................................46
Table 12. Education Needs to be Included in Continuing Education Responses..............49

viii
LIST OF FIGURES
FIGURE……………………………………………………………………………...PAGE
Figure 1. Logic Model for the Research Project .................................................................8
Figure 2. Project Design……………………………………............................................27
Figure 3. Confidence Levels Before Educational Offering...............................................48
Figure 4. Confidence Levels After Educational Offering..................................................49

1
CHAPTER I
Introduction
While working on a cardiology floor in the Midwest for over three years, this
author discovered a universal indignation among the floor nurses; spited by various nurse
practitioners and doctors. When asked to recount their experiences with nurse
practitioners and doctors, nurses described instances of getting yelled at, being talked
down to, hung up on, and even completely ignored. One nurse stated:
One night, I had a patient who fell at 0300. Naturally, I called the on-call
physician expecting to obtain an order for a CT of the head. After he picked up, I
stated, ‘hello, Dr. C. I have your patient, Mr. Smith in room 209. I wanted to
inform you that he fell out of bed and hit his head.’ and then I heard the click of
him hanging up on me. I didn’t know what to do, and there wasn’t a nurse
practitioner on call. So, I just wrote a note and moved on.
Another nurse shared her experience:
I had a [arterial] cut-down where the patient’s groin site started bleeding. There
isn’t a protocol except to hold pressure. It took a while to get a call back from the
cardiothoracic surgeon, so I just held pressure until he answered his page. When
we finally got a hold of him, he started screaming at me; accusing me of ruining
his graft. At the time, I was scheduled to transfer from Cardiology to the ICU

2
within the next couple of weeks. After that experience, the surgeon told my
supervisor that I was not to transfer to the ICU or ever take cardiothoracic surgery
patients again. If he would have answered his page sooner or written specific
orders to not hold direct pressure on the graft, the situation could have gone
better.
Dozens of similar stories were shared among the unit. Recently, there has been
push-back from nurses across the unit who are searching for ways to alert administrators
of the presence of a hostile work environment. After speaking with her floor supervisor,
this author decided that a research project could benefit the hospital by providing
information on disruptive communication, how often disruptive communication occurs,
what types of disruptive communication are present, and what outcomes come from
disruptive communication.
Description of the Clinical Problem/Issue
According to the literature, communication errors are the leading cause of
inadvertent patient harm. Healthcare providers need to be aware of communication
errors, for communication errors are a daily occurrence that can be prevented. Leonard et
al. (2004) report:
Analysis of 2455 sentinel events reported to the Joint Commission for Hospital
Accreditation revealed that the primary root cause in over 70% [of inadvertent
patient harm] was communication failure. Reflecting the seriousness of these
occurrences, approximately 75% of these patients died. (p.86)
This statement reflects the seriousness of the issue, validating the potential harm that
disruptive communication can cause patients.

3
Kimes et al. (2015) stated, “The focus on a culture of safety within health care
emphasizes the need to limit any controllable negative influence on patient safety”
(p.225). Therefore, healthcare as a whole needs to do better when confronting issues such
as disruptive communication. It is unacceptable for nurse administrators to tell nurses,
“that’s just the way things are” as nurses try to confront the issue when it is the patients
who are ultimately being harmed.
Although some changes have been made to improve communication in
healthcare, more needs to be done to advocate for nurses. Many facilities hold policies
that discourage, or even prohibit disruptive behavior (Rosenstein & O’Daniel, 2008;
Kimes et al., 2015). However, doctors are often viewed as a precious resource to hospital
administrators because of their extensive knowledge and expertise, the revenue they
generate, and the general scarcity of doctors. Thus, their inappropriate behavior often
goes ignored. On the other hand, nurses are also valuable resources, and the country is
experiencing a national shortage of them. If nurses feel as if their voices are not being
heard, it could lead to issues with recruitment and retention (Robeznieks, 2015; Kimes et
al., 2015, p. 223). Therefore, doctors, nurse practitioners, and hospital administrators
need to be aware of the consequences of their actions and the risks they are taking by
ignoring the disruptive behavior.
Significance
Disruptive communication has a significant influence on nurse satisfaction,
turnover rates, and patient safety. Rosenstein & O’Daniel (2005) address satisfaction and
patient safety by gaining nurse perspectives. Nurses reported, “Employee stress as a
result of physician yelling resulted in decreased patient safety” (p. 25). Another nurse

4
stated, “Most nurses are afraid to call Dr. X when they need to, and frequently won’t call.
Their patient’s medical safety is always in jeopardy because of this” (Rosenstein &
O’Daniel, 2005, p. 25). Patient safety is the pinnacle of nursing. Therefore, if patient
safety is repeatedly jeopardized, nurses may become dissatisfied with their work. Kimes,
Davis, & Medlock (2015) found that “ineffective collaboration” caused nurses to feel
“belittled, angry, and disrespected.” Due to the increased stress, anxiety, anger, and
frustration that is caused by disruptive communication, it is stressed throughout the
research that disruptive communication needs to be corrected; for it is believed to affect
nurse retention rates.
Specific Aims/Purpose
The purpose of this study is to identify what types of disruptive behavior nurses
are experiencing, discuss outcomes of disruptive behavior, and educate healthcare
providers and administrators of disruptive communication. Understanding the
consequences of disruptive communication can assist educators in articulating the need
for training in conflict management and therapeutic communication methods. It can also
aid healthcare providers to be more conscious of their behavior in the professional
setting. This author hopes this will lead to increased job satisfaction for nurses, higher
nurse retention rates, and better patient outcomes.
Theoretical Framework
Communication Accommodation Theory
The Communication Accommodation Theory (CAT) is an Interaction-Centered
Theory, meaning the theory focuses on the interaction itself, or how participants utilize
verbal and non-verbal behavior to facilitate the conversation (Baylund et al., 2012).

5
Baylund et al. (2012) describe CAT as, “the ways individuals modify their
communicative behavior as a result of their communication with each other” (p.265).
CAT allows individuals to “predict and explain” verbal and non-verbal cues that
providers make to “maintain or decrease social distance” in communicating (Baylund et
al., 2012, p.265). The two main concepts of CAT are divergence and convergence.
Baylund et al. (2012) explain that a person may use divergence to indicate differences in
communication styles (p.265). Convergence allows a person to match another’s
communication style usually indicating a positive connection. CAT acknowledges that
providers may accommodate one another by considering the other participant’s needs and
the power dynamic within the relationship. Baylund et al. (2012) explain, “Those
traditionally perceived as having greater power tend to be accommodated more than those
with less power” (p.265). CAT has been limited to healthcare communication studies,
focusing on “intergroup conflict among multi-specialty doctors” (Baylund et al., 2012,
p.266). CAT can be utilized to determine how nurses and doctors perceive conversations
through body-posturing, tone of voice, non-verbal cues, rate of speech, eye contact, and
so on. The disadvantage of using this theory is it is mostly applicable to face-to-face
communication. Doctors and nurses often communicate over the phone, so this theory
would not be applicable for a study focusing on phone communication.
Social Exchange Theory
Another theory that can be applied to the study is the Social Exchange Theory
(SET). SET interactions are interdependent, based on the idea that the exchange of social
and material resources is the basis of human interaction (Cropanzano & Mitchell, 2005,
p.874). According to Cropanzano and Mitchell (2005), SET emphasizes that

6
“interdependent transactions have the potential to generate high-quality relationships,
although as we shall see this only will occur under certain circumstances” (p.874). Xerri
(2012) describes SET as, “the social interactions tend to be mutually dependent and
contingent upon the actions of another person” (p.4). SET contains the theory of
reciprocity, based on the assumption that if one completes one good deed for another, a
good deed will be returned, possibly at a later time (Xerri, 2012, p.4). Often, when nurses
and doctors communicate, each party expects that they will gain something from the
conversation, whether it is information, a medication, approval, respect, etc. When a
doctor or nurse receives positive input from the opposite source, they are more likely to
provide positive output in the future to the same source.
The Orchestra Theory
The Schutzian Lifeworld Phenomenological Orchestra Study performed by
Valerie Malhotra (1981) provides an interesting and appropriate theoretical model for the
project. The orchestra study describes how each member of an orchestra provides their
own knowledge, experience, and talents to contribute to the orchestra as a whole.
Malhotra (1981) states, “Each player must not only be conscious of his or her own part,
but also of the parts of other musicians” (p.105). This is also true of healthcare workers.
Each provider must understand the role of other team members to successfully carry out
orders and provide exceptional care. Malhotra (1981) also explains that musicians may
only hear certain parts being played, “but do not hear the entire musical piece while they
are playing (Lancaster et al., 2015, p.276). Therefore, they must use quality verbal and
non-verbal communication to understand each member is doing his or her part to
contribute to the same goal. Like an orchestra, healthcare workers have different roles to

7
play, but collaborate to “create a cohesive final performance” (Lancaster et al., 2015,
p.276).
Project (Practice) Question(s)/Hypotheses
1. What type of disruptive behavior are nurses experiencing?
2. How frequently do nurses experience disruptive behavior?
3. What outcomes do nurse’s perceive result from disruptive behavior?
4. Do nurses perceive there is a relationship between communication and job
satisfaction?
5. Is there a relationship between the frequency of disruptive behavior and the
nurse’s perception of the relationship between communication and job
satisfaction?
6. How confident do nurses feel addressing disruptive behavior before an
educational intervention?
7. How confident do nurses feel addressing disruptive behavior after an educational
intervention?
Definition of Key Terms/Variables
Disruptive communication: frequently used term to describe poor communication
methods and behaviors. Belittling, yelling, sexual harassment, verbal outbursts, physical
threats, degrading, and ignoring behaviors have all been identified as disruptive behavior
(Higgins & MacIntosh, 2010; Rosenstein, 2009; Rosenstein & O’Daniel, 2008; Kimes et
al., 2015, p.223)
Communication: “process by which information is exchanged between
individuals through a common system of symbols, signs, or behavior; personal rapport;

8
information communicated: information transmitted or conveyed; a verbal or written
message” (Merriam- Webster, n.d.). Leonard et al. (2004) describe communication in
healthcare as intricate and highly important (p.85). McCaffrey et al. (2010) state “skilled
communication focuses on critical communication proficiencies, including self-
awareness, inquiry and dialogue, conflict management, negotiation, advocacy, and
listening” (p.173). The concept and definition of communication seem simple. Why do
healthcare providers struggle with effective communication?
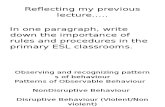
Figure 1
Logic Model for the Research Project
Disruptive communication is displayed under “problem” in the Logic Model,
leading to “negative outcomes,” including adverse patient outcomes and hostile work
environments. Hostile work environments can lead to decreased job satisfaction, which
can result in low nurse retention rates. Adverse patient outcomes can lead to decreased
patient safety, also resulting in low nurse retention rates. Providing an intervention
Goals Outcomes Intervention Problem
Disruptive
Communication
Hostile Work
Environment
Low retention
Adverse Patient
Outcomes
Decreased Job
Dissatisfaction
Decreased
Patient Safety
Nursing Insight
And
Education
Motivation
for Change
Respect
&
Understanding
Active
Listening
Effective, Clear
Communication

9
including nursing insight and education may lead to positive outcomes. These positive
outcomes, or “goals,” include motivation for change, respect and understanding, active
listening, and effective, clear communication.
Summary of the Chapter
Disruptive communication is a universal issue in healthcare. However, it is often
disregarded by unenforced policies, general disrespect, simply ignoring the issue, and a
lack of education. Hospitals around the world have fallen victim to disruptive
communication. In some cases, nurses attempted to inform their supervisors and
administrators of the growing issue. In result, many were told “that’s just how it is”.
Research has shown that this can cause a decrease in job satisfaction and work ethic
(Rosenstein et al, 2005; Manojlovich, 2005). Communication not only affects nurse
attitudes but can also affect patient safety. For example, Kimes et al. (2015) found,
“nurses reported they often avoided subsequent interaction with doctors and were less
likely to communicate effectively with them in future situations…one nurse reported she
would ‘exhaust all means possible’ before contacting a physician” (p.226). Therefore,
healthcare leaders should enforce zero-tolerance policies for disruptive communication
within the healthcare setting while continuing to educate their staff on the importance of
positive communication.
The purpose of the study is to identify what types of disruptive behavior nurses
are experiencing, discuss outcomes of disruptive behavior, and inform healthcare
providers and administrators of disruptive communication. Using the Communication
Accommodation Theory, Social Exchange Theory, and Orchestra Theory, this author will

10
incorporate and identify communication techniques and teamwork methods within the
project. Seven project questions were developed.
Through this project, nursing insight and education to nursing staff using
Orchestra Theory, SET, communication techniques, and conflict management to promote
a motivation for change, active listening, respect/understanding, and effective, clear
communication will be provided. Many unnecessary errors, poor outcomes, and
dissatisfaction can be prevented if healthcare providers respected one-another, and work
as worked as a team.

11
CHAPTER II
Review of the Literature
Communication is an underrated and vital skill that all healthcare providers are
expected to master. However, there have been reports of dissatisfaction,
misinterpretation, medication errors, and mortalities due to poor communication. The
literature does not put it lightly; “communication failures are the leading causes of
inadvertent patient harm” (Leonard et al., 2004, p.85). The authors within the literature
agree that when nurses, doctors, and nurse practitioners refuse to communicate in a
healthy manner, it is ultimately the patient who suffers.
According to the literature, communication errors are the leading cause of
inadvertent patient harm. Nurses and doctors need to be aware of communication
errors, for communication errors are a daily occurrence that can be prevented.
The Joint Commission for Hospital Accreditation reviewed 2455 sentinel events
and found that over 70% of the cases resulted from communication failure among
the interdisciplinary team (Leonard et al., 2004). Although some changes have
been made to improve communication in healthcare, Zwarenstein et al. (2013)
explain:
Many problems of coordination and communication may arise from lack
of a common cross-team understanding of the care priorities for a specific

12
patient at a specific time and the resulting failure of individual team
members to align their activities to those priorities, rather than s imple
miscommunication. (p.494)
This evidence provides insight into what is known about interprofessional
communication in reference to the research literature. Common themes identified in the
literature include patient outcomes, nurse and physician satisfaction, theories, and
improvement strategies regarding interprofessional communication. This review will
assess common variables linked to poor communication and will identify missing links in
the literature.
Literature Synthesis
A search of CINAHL, Summon, Google Scholar, Medline, and PubMed
was conducted using the terms nurse, communication, physician, satisfaction,
patient outcomes, interdisciplinary team, dissatisfaction, disruptive,
inappropriate, and theory. Results included a great deal of discussion on several
topics including communication differences, disruptive behavior, communication
techniques, nursing theories, patient outcomes, and satisfaction levels. Poor
communication techniques were often linked to patient harm and undesirable
outcomes. A total of 20 articles and one guideline were utilized for research.
Interdisciplinary communication is the key concept reviewed in this synthesis.
Qualities related to poor communication methods, interdisciplinary satisfaction,
patient satisfaction, and communication techniques were reviewed to identify
contributing factors and important concepts.
Qualities Related to Poor Communication Methods

13
Qualities such as communication differences and hierarchies can cause
gaps in communication between nurses and doctors. Differences in
communication methods may lead to misunderstanding and confusion between
the two parties. Hierarchies may cause a disconnect between those who should be
working together as a team. These qualities should be addressed with training
and leadership to help people understand each other, encourage voice, and
healthily coordinate care.
Communication Differences
Several issues contributing to communication gaps have been identified
by the literature. The literature reviewed suggests that nurses and doctors are
taught to communicate differently. In nursing school, nurses are taught to look at
the ‘big picture’ and be very broad in their explanations , whereas doctors are
taught to get straight to the problem and be concise. Nurses typically rely on care
plans, goal sheets, and patient meetings to communicate issues, while doctors
utilize short discussions focusing on medical issues (McCaffrey et al., 2010,
p.173). McCaffrey et al. (2010) conducted a study surveying 462 nurses and 78
doctors, finding communication differences between the two disciplines. The
nurses stated in their surveys that they felt that the communication styles utilized
at work were ineffective, especially between doctors and nurses (McCaffrey et
al., 2010, p. 173). Doctors reported they preferred to spend little time on
communication, and they expect nurses to anticipate the doctor’s needs and take
orders correctly (McCaffrey et al., 2010). McCaffrey et al. (2010) state, “Doctors
did not identify information obtained from nurses as particularly useful or

14
important, and often described it as bothersome” (p.173). The difference between
the two communication techniques sparked frustration and impatience among
nurses and Doctors. McCaffrey et al. (2010) discuss that the importance of
communication is not emphasized within nursing schools, medical schools, and
the workplace. They recommend development of a common language that is
agreed upon, then distributed throughout the healthcare system to allow a good
relationship between the two professions.
Disruptive Behaviors and Hierarchies
Hierarchies can lead to disruptive behavior by causing a divide between
the interdisciplinary team. In healthcare, doctors are viewed as the highest-
ranking member of the interdisciplinary team. Disruptive behavior from doctors
has been identified and described in a variety of ways, including verbal
outbursts, physical threats, degrading or insulting comments, ignoring behaviors,
and sexual harassment (Higgins & MacIntosh, 2010; Rosenstein, 2009;
Rosenstein & O’Daniel, 2008; Kimeset al. 2015). According to Robinson et al.
(2010), “the well-entrenched hierarchical authority structure and sexism (even
though women make up over one-third of the physician workforce) complicate
nurse-physician communication” (p.206). Although many hospitals have adopted
a “zero tolerance policy” regarding disruptive behavior, few have followed
through with the policy, resulting in little improvement (Rosenstein & O’Daniel,
2008; Kimes et al., 2015, p. 223). Doctors are considered a “precious resource”,
making health care organizations more likely to tolerate inappropriate behavior
displayed by doctors (Kimes et al., 2015, p.227). Dixon-Woods et al. (2019)

15
discuss the hierarchy’s “untouchables,” or doctors who hold a significant amount
of power and influence. Dixon-Woods et al. (2019, p.580) explain that the poor
behavior of untouchables is derived from their revenue generation or
professional position. They are often seen as unapproachable and can be difficult
to discipline, leading to an environment of fear and hostility .
Kimes et al. (2015) found within their study that disruptive behavior was a
frequent experience when 12 out of 15 (75%) participants reported disruptive
behavior within a surgical department (p.225). In a study conducted by Robinson
et al. (2010), a nurse vocalized, “he said in the presence of the patient, ‘it is
amazing on this floor; the nurses don’t know what they are doing’” (p.212).
Nurses reported feeling that they annoyed Doctors when they contacted them for
clarification of orders (Kimes et al., 2015, p.226).
Ineffective collaboration impacts nurses’ confidence and emotional state,
often leading them to avoiding interaction with doctors in future situations
(Kimes et al. 2015, p.226). As Kimes et al. (2015) discusses, “one participant
reported disruptive physician behavior often ‘intimidates nurses into not
questioning because they want to keep the peace’” (p.225). This behavior is
dangerous both for patients and for nurses who will be less willing to notify
doctors of any indication of a problem in fear of being reprimanded. It is the
nurse’s responsibility to advocate for his or her patient. If nurses are
uncomfortable communicating with doctors, there is likely to be an error or
mishap (Kimes et al., 2015, p.225). Although researchers disagree upon how
much negative influence disruptive behavior has on patient outcomes, Kimes et

16
al. (2015) suitably states that the focus should be on limiting “any controllable
negative influence on patient safety” (p.225).
Satisfaction of the Interdisciplinary Team
Communication is highly associated with job satisfaction. Doctors and
nurses are expected to communicate with each other to obtain the ‘big picture’ of
a patient’s situation. However, nurses and doctors are both guilty of letting
information “slip through the cracks” through poor communication. Burroughs
and Bartholomew (2014) indicate that communication failures result in
distancing measures. For instance, nurses can withhold information, be
unavailable for updates, or refuse to communicate with doctors. Doctors can
display unavailability, use an irritated tone of voice while speaking to a nurse, or
display body language to “nonverbally portray that it is unnecessary to converse
with a nurse” (Burroughs & Bartholomew, 2014, p.60). After collaborating
toward better communication skills, nurses and doctors, alike have responded
positively toward new communication practices.
Physician Satisfaction
Physician responses provided helpful perspective in the literature. Doctors
expressed appreciation for clarity and precision, collaborative problem solving,
maintenance of mutual respect, an authentic understanding of one’s professional
role, and a calm and supportive demeanor under stress (Robinson et al., 2010,
p.209-211). The most popular response expressed by participants in the study
that Robinson et al. (2010) conducted was, “the need for straightforward
unambiguous communication” (p.210). Doctors and nurses need to communicate

17
their needs clearly and effectively to fully understand each other. If either party
“beats around the bush” to spare feelings, the language may be misinterpreted,
possibly resulting in an undesirable outcome. One of the doctors shared his
experience in Robinson et al.’s (2010) study, describing an outcome of a
conversation with a resident about a patient’s discharge (p.210). The resident
responded, “…yeah, yeah, yeah. The patient is going home. Fine” (Robinson et
al., 2010, p.210). When the doctor followed up the next day, it turned out the
patient never went home and the nurse did not know anything about the
discharge (Robinson et al., 2010). The patient was not harmed in the situation,
but a financial burden was forced upon them by staying an unnecessary night.
Nurse Satisfaction
A physician’s actions and communication styles often play a role in
nurse’s job satisfaction (Coeling & Cukr, 2000; Manohlovich, 2005, p. 367). If
disruptive communication is tolerated, it can be devastating; nurses are
considered a scarce resource as a result of the nursing shortage and disruptive
communication can cause nurses to leave a workplace (Kimes et al., 2015, p.
227). Throughout the literature, after the implementation of communication
techniques, nurses reported higher satisfaction ratings. Although most of the
articles reported an increase in nurse satisfaction ratings, Robinson et al. (2010)
explained in detail what contributed to contentment. “Establishment of a
relationship was seen as almost a precursor to communication” (213), stated
Robinson et al. (2010), “…participants had to feel comfortable with each other in
order to communicate effectively”. Nurses feel that when they can establish a

18
trusting relationship with a physician, they are more likely to express concerns
and participate in collaboration.
Nurses also appreciate teamwork and feel that it is beneficial when team
members come together to solve problems (Robinson et al., 2010, p.213). It is
frustrating for nurses when Doctors do not understand or respect the nursing
profession or their scope of practice (Robinson et al., 2010, p.213). Robinson et
al. (2010) explains, “it would be difficult for communication to be perceived as
respectful if it was not based on an authentic understanding of what one brings to
the situation” (p.214). They suggest implementing interprofessional education
for nurses and doctors to develop a true understanding of each other.
Patient and Family Satisfaction
The literature suggests that communication directly affects patient
outcomes and satisfaction. Patients benefit when both professions (doctors and
nurses) seek each other out for “routine and complex decision -making”
(Robinson et al., 2010, p.210). When Doctors and nurses do not collaborate,
patients and family members may experience confusion, dissatisfaction, delays,
and re-admissions (Zwarenstein et al. (2013). Riskin et al. (2017) affirms,
“rudeness can debilitate intervention acuity, thus resulting in poorer medical
treatment and…potentially catastrophic clinical outcomes” (p.8). In Robinson et
al.’s (2010) study, patient care was improved when nurses and Doctors could rely
on each other (p.211).
Khan et al. (2015) performed a study that surveyed pediatric patient’s
parents. From the study, Khan et al. (2015) gained information on the

19
relationship between communication and patient/family satisfaction. “On
multivariable analyses, parents’ ratings of their direct communications with
doctors and nurses, and their observations of teamwork and communication
between doctors and nurses, were significant predictors of top-box overall
experience” (p.6). The research indicates that improving communication
(especially on night shift) can significantly improve a patient or family member’s
hospital experience. Khan et al. (2015) suggests that further research needs to be
conducted, specifically regarding night shift, teamwork, and communication
(p.8).
Methods to Improve Communication
Methods of communication need to be observed to try to mend broken
relationships among nurses and Doctors. Linking factors in the work
environment and nurse communication can provide insight into how to improve
nurses’ perceptions of communication with Doctors (Manojlovich & DeCicco,
2007, p.541).Common methods include frequent physician-nurse interactions,
education, and the use of SBAR.
Frequent Physician-Nurse Interactions
There were many recurring themes throughout the literature involving
different techniques to improve communication. Frequent physician-nurse
interactions through rounding together and specific floor assignments for doctors
proved to be beneficial for nurse and physician satisfaction, as well as patient
outcomes (Gordon et al., 2011). Important factors for communication include

20
clarity, precision, collaboration, mutual respect , and an understanding of
professional roles (Robinson et al., 2010).
Education
Nurses and Doctors need to be reminded of the importance of
communication and how it can benefit their practice. McCaffrey et al. (2010)
suggests nurses and Doctors need to be informed of the importance of
communication and how collaboration can contribute to positive patient
outcomes (p.174). McCaffrey et al. (2010) also propose that cultural differences
and body language need to be discussed when teaching communication (p.175).
Body language accounts for 67% of actual messages received by the listener
(Dixon et al., 2006; McCaffrey et al., 2010). Role-playing is a great teaching
strategy that can be used to teach participants how to interpret and display
appropriate body language (McCaffrey et al., 2010). Scenarios and practice
simulations could be used to advance listening skills , improve expressing clear
messages, gain an appreciation of the significance of body language, and learn
how to use negotiation and conflict resolution (McCaffrey et al., 2010).
Educating nurses and doctors of each other’s roles may also improve
communication through understanding and mutual respect. Education plays an
important role in effective and safe communication. It is highly encouraged that
medical schools, nursing schools, residency programs, and hospitals implement
education resources to improve communication methods. Leonard et al. (2004)
agree, “To date, we are seeing that teaching and embedding a few basic tools and

21
behaviours can provide tremendous clinical benefits. We have seen improved
cultural measures—attitudes surrounding teamwork and safety climate” (p.90).
SBAR
SBAR is an effective tool used throughout healthcare to create a
standardized and predictable communication method. SBAR stands for situation
(what is going on with the patient), background (what is the clinical background
or context), assessment (state findings and what one thinks the problem is), and
recommendation (clearly state what one is expecting to gain from the
conversation) (Leonard et al., 2004). This method allows nurses to “briefly and
concisely” relay information to doctors (Leonard, et al., 2004, p.86).
Surprisingly, Leonard et al. (2004) was the only source in the reviewed literature
that mentioned SBAR and how it can improve communication between nurses
and doctors.
Face-To-Face Communication
A recurring theme throughout the literature was the importance of face -to-
face interaction. Both-doctors and nurses expressed an appreciation for the
opportunity to build relationships and trust amongst each other (Gordon et al.,
2011; Lancaster et al., 2015). Gordon et al. (2011) express, “Increasing face-to-
face communication between nurses and doctors could potentially improve
timeliness of action, accuracy of performance, and understanding, openness, and
collaboration among caregivers” (p.427). Gordon et al. (2011) explain that face-
to-face interaction allows for an exchange for nonverbal cues and allows nurses

22
and Doctors to identify each other, contributing to, “an atmosphere supporting
openness and collaboration” (p.47).
Poor Communication and Patient Outcomes
Poor communication has been linked to adverse patient outcomes in prior
research. In a prospective cohort study performed by Khan et al. (2010) poor
“physician-nurse interactions are associated with patient mortality and
readmissions. Teamwork has been correlated with patient outcomes and quality
care” (p.7). Several articles had the similar message, “communication failures
are the leading cause of inadvertent patient harm” (Leonard et al., 2004, p.85).
Improving communication is an underrated yet imperative skill that all
healthcare workers need to develop on. A participant in Lancaster et al.’s (2015)
study perfectly explained why communication is so important:
Communication is essential in any field. In medicine, it is particularly
important because you delegate work on behalf of the patient. You have to
be clear on your assessments and management plan, and this has to be laid
out very carefully to the patient, your colleagues, to nursing staff, and
aides who are participating in care. (p.280)
Nurses and Doctors need to acknowledge this, for if communication fails, it is
ultimately the patient who loses.
Summary
Numerous studies have been developed to understand what is causing
miscommunication, to learn how to improve communication among the
interdisciplinary team, and to link poor communication methods to patient harm.

23
The literature thoroughly discussed the importance of utilizing proper
communication to ameliorate job satisfaction between doctors and nurses,
improve patient and family satisfaction with care, and to validate the need for the
use of appropriate communication techniques. Descriptive research also
identified the effects of effective and ineffective communication. Effective
communication derives from clear and concise language, mutual respect, an
understanding of professional roles, positive body language, pleasant tone -of-
voice, and professionalism. With the use of positive communication, nurses and
doctors are more likely to collaborate with one-another, respect each other, and
form healthy relationships. Patients and family members are likely to pick up on
the relationships among their care team, emphasizing the importance of healthy
communication.
It is indicated that further research needs to be developed concerning
specifically what errors are being as a result of miscommunication, and what
forms of disruptive communication are being seen. A fair amount of research has
been developed on the benefits of effective communication in the work
environment, but it would be interesting to validate how often disruptive
communication is reported in the workplace, and how destructive it can be . There
have been proven ties between face-to-face communication and positive
outcomes. Therefore, methods of increasing face-to-face interaction between
healthcare providers must be explored further. Gaining perceptions of those
within the interdisciplinary team can be utilized for educational purposes,
providing insight into issues within the workplace. Bringing up the importance of

24
communication and acknowledging disruptive behavior can push healthcare
providers and hospital administrators to strive for a heal thy work environment,
leading to positive outcomes.
The results of this literature review supported the author’s belief that new
communication techniques need to be implemented in nursing school and
medical school curriculum. Each member of the interdisciplinary team needs to
be aware of communication styles and techniques to improve the quality and
safety of patient care. Healthcare providers who can communicate effectively
create better patient outcomes, a perception of professionalism, mutual respect ,
all which leads to an increase in job satisfaction.

25
CHAPTER III
Methodology
Communication is a vital skill that every healthcare professional should possess.
When healthcare professionals communicate effectively, care is delivered safely and
efficiently. However, when communication is disruptive, healthcare professionals have
reported dissatisfaction, misinterpretation, medication errors, and mortalities as a result of
disruptive communication. The purpose of this project is to identify the type and level of
disruptive communication at select Midwestern healthcare facilities in order to develop a
program to teach nurses how to manage disruptive behavior. This chapter will discuss the
designs of the scholarly project by outlining the sampling process, describing the
demographics, and examining the instrument to be used as well as potential statistical
analysis methods.
Project Design
A mixed-method descriptive research design was utilized to measure
communication methods, outcomes, and satisfaction among nurses. It was used to
determine if discussing communication methods and techniques through an educational
offering will improve nurses’ level of confidence in managing disruptive behavior. The
information from this study will help educators and leaders prepare nurses, nurse

26
practitioners, and doctors by educating and training them on the importance of effective
communication and advocacy.
The project utilized a one-group pre-test/post-test design focused on nurses’
confidence level in managing disruptive behavior. The chosen method of data collection
was selected to yield information comparing the difference between pre-test and post-test
scores after receiving education over disruptive communication and communication
techniques. The pre-test asked participants about disruptive communication in the
workplace the participants have personally experienced and assessed their confidence
level of managing disruptive communication. The post-test was available to the nurses
immediately after finishing the educational offering. Understanding what types of
disruptive communication nurses are experiencing and incorporating communication
techniques into nursing education could potentially allow hospitals, clinics, and schools
to adopt these methods, encouraging nurses to properly advocate for their patients and
work constructively within the interdisciplinary team. A diagram detailing the project
design can be found below.

27
Figure 2
Project Design
Project Site and Population
The surveys prepared by this author and agreed upon by the Doctor of Nursing
Practice Scholarly Project Committee were administered to two different regional
hospitals. A convenience sampling of registered nurses was used and was determined by
the number of participants at each location. A PowerPoint presentation utilizing
communication methods collected from scholarly peer-reviewed journal articles and
nursing textbooks was be prepared by this author. It was given live online through Webex
communication software at Hospital A, while the pre- and post-tests were distributed in
the break room. The same PowerPoint presentation was sent via Health Stream to
participants along with links to the pre- and post-test at Hospital B. All participants who
viewed the educational offering received the pre-test and post-test. The inclusion criterion
for the study will require that participants hold a valid RN license and work within the
hospital setting. Participants must also be at least eighteen years of age and speak English
Research Development
• Pre-Test
• Post-Test
• Educational Offering
• Participant Recruitment
Educational Offering
• Pre-Test
• Post-Test
Compilation of Test Scores
•Descriptive Statistics
Dissemination of Data
• Scholarly Project
• Journal Submission

28
as their primary language. The study did not include vulnerable subjects including
mentally disabled individuals, children, or prisoners. It did not discriminate against
specific populations due to race, religion, or ethnicity. All surveys were answered
confidentially, and confidentiality was maintained during the data coding process.
Participants were ensured that they will not experience harassment or discomfort during
the research study. There were minimal risks associated with the pre-test and post-test.
The responses of the subjects remain confidential to prevent any risk of criminal or civil
liability or to cause damage to their financial standing, employability, or reputation.
Participation in the educational opportunity was voluntary; no monetary
compensation was provided. Individuals were invited to participate in the study and
educational offering via email. Consent was obtained on online consent forms and
provided before initiating the pre-test. After providing informed consent, participant data
was obtained through the participant’s completion of the surveys. The data was analyzed
using descriptive statistics. To guarantee confidentiality, the collected information did not
contain any participant identifiers and were anonymously provided using both Health
Stream software and traditional handouts. Additionally, data from completed online
questionnaires was coded by Health Stream and submitted online to the researcher only.
Ethical Considerations/Protection of Human Subjects
As stated above, participation in the study was solely voluntary. Due to the nature
of the study, which involves a pre-test and post-test regarding sensitive information,
unique experiences, and perceptions, the primary ethical concern was the potential
identification of participants due to the survey response answers. Therefore, anonymity is
imperative. Information was recorded and stored without any identifiers to maintain

29
obscurity. False information, such as the fabrication of events provided by participants
was also concerning, potentially leading to the contamination of data. Finally, validity
and reliability of a developed instrument can alter the data’s statistical significance. This
author will uphold the three basic principles of human subject protection: respect for
persons, beneficence, and justice. IRB approval was obtained by this author before
contacting participants and collecting data.
Instruments
The study utilized two formats to deliver surveys to obtain data—a pre-test survey
and a post-test survey. One hospital’s surveys were administered through an online
format using Health Stream software. The other hospital completed the surveys
anonymously with pen and paper. Both survey formats were the same, containing
demographic data including age, gender, years of practice, and area of practice. They
included open-ended, closed-ended, and Likert-scale questions. The pre-test included
questions regarding the nurses’ personal experience with disruptive communication,
including narratives, and patient outcomes. While both surveys assessed nurses’
confidence level in managing disruptive behaviors, the post-survey did not include
questions regarding personal experience; instead, it focused on the educational outcomes.
The quantitative data obtained from the surveys were analyzed using descriptive
statistics.
A survey tool was developed for the study because a specific instrument for the
study could not be found. However, the instrument was based on a previous study
conducted by Rosenstein & O’ Daniel (2005). In their study, perceptions of disruptive
behavior among the interdisciplinary team were thoroughly assessed, addressing

30
outcomes, job satisfaction, and nurse retention. The study included nurse practitioners,
doctors, and nurses. Using the Rosenstein & O’ Daniel (2005) survey as a model,
modifications were made, and a new expanded survey was created for this research study.
The first several questions in the pre- and post-test addressed the participant’s
demographics. In the pre-test, the next set of questions addressed the “occurrence of
disruptive behavior among nurses and doctors, the influence of gender, psychological and
clinical variables and clinical outcomes, and respondent’s comments” (Rosenstein & O’
Daniel, 2005). The final group of questions in the pre-test and most of the post-test
addressed the nurse’s confidence in managing disruptive behavior. Both surveys included
open-ended, closed-ended, and five-point Likert-scale questions. The study focused on
the following research questions:
1. What type of disruptive behavior are nurses experiencing?
2. How frequently do nurses experience disruptive behavior?
3. What outcomes do nurses perceive result from disruptive behavior?
4. Do nurses perceive there is a relationship between communication and job
satisfaction?
5. Is there a relationship between the frequency of disruptive behavior and the
nurse’s perception of the relationship between communication and job
satisfaction?
6. What is the nurse’s level of confidence in managing disruptive behavior before an
educational offering?
7. What is the nurse’s level of confidence in managing disruptive behavior after an
educational offering?

31
Content Validity
The survey instrument was developed by the researcher; therefore, instrument
validity needed to be determined. To determine content validity, the survey instrument
was reviewed by a board of Pittsburg State University Irene Ransom Bradley School of
Nursing faculty members. Faculty members were provided the survey, and provided
feedback utilizing their previous experience within the field of nursing. Changes were
made based on feedback.
Analytical Methods
Descriptive statistics were used to describe demographic data, such as the number
of participants, gender, age, and confidence. Correlational statistical analysis was
performed on frequency of disruptive behavior and nurse job satisfaction.
Procedure
The proposal defense took place by March 30th, 2020 with the project committee
consisting of two Pittsburg State University Irene Ransom Bradley School of Nursing
faculty members and one Pittsburg State University Department of Communications
faculty member. Upon proposal approval, the proposal was sent to Irene Ransom Bradley
School of Nursing and Pittsburg State University’s IRB committee for approval. The IRB
form, Research Involving Human Subjects, was completed by the author and approved by
Pittsburg State University in early January 2021. The educational offering took place
January of 2021. A voice-over PowerPoint presentation was used at one hospital and live
online presentation was given at the other. Before the presentation, participants at both
hospitals were asked to complete a pre-test with questions regarding demographics,
experience with and perceptions of disruptive behavior, and confidence levels in

32
managing disruptive behavior. After finishing the educational offering, the participants
completed a post-test, focusing on demographics and confidence levels in managing
disruptive behavior. Surveys at Hospital A were available for nurses to pick up and fill
out anonymously in the break room. Participants were instructed to fill out the
questionnaire, and leave it face-down in a drop box. The researcher collected the
submissions every Friday for two weeks. Although the traditional route of gathering data
is not as secure as advanced online sources, it still allowed anonymity. Hospital B posted
the pre-questionnaire on Health Stream for the nurses to complete. The data was
disseminated, statistically analyzed, and the findings were reported.
The research project consisted of a pre-test, educational offering, and post-test to
assess experiences of disruptive behaviors, outcomes from disruptive behaviors, nurse
satisfaction levels, and confidence-levels while addressing disruptive behaviors. Consent
was obtained from participants by giving them with the pre-test through Hospital A, and
before taking the online pre-test at Hospital B. The pre-test was developed and
administered anonymously in the breakroom and using Health Stream, an education
software available online. Health Stream allowed for convenient online delivery of the
assessment tools to participants and allowed them to complete the assessment on their
own time. Data obtained by the researcher did not contain any participant identifiers,
allowing for the protection of participants. The pre- and post-test were left in the
breakroom by the researcher and was available to nursing staff in the emergency, med-
surg, and surgery departments at Hospital A. The pre- and post-test was available on
Health Stream for obstetrics, surgical, med-surg, emergency department, and the
intensive care unit at Hospital B. The data was reviewed and analyzed by the researcher

33
using descriptive statistical analysis. After completion of the pre-test, participants were
invited to participate in the educational offering.
The educational offering was available to all departments at both hospitals,
offered to both—participants, and non-participants. It was provided through a PowerPoint
presentation available through Health Stream at Hospital B. At Hospital A, a live
presentation with the same PowerPoint was provided online through a communication
service called Webex. Therefore, participants at both hospitals could engage in the
research study at home or at the hospital with access to wi-fi and to a computer. Both
participating facilities had multiple computers and educational centers available to their
nursing staff. A review of evidence-based communication techniques and confidence-
building strategies was provided within the PowerPoint. A post-test was provided
immediately following the educational offering. Like the pre-test, the post-test was
available in the break room at Hospital A and on Health Stream for Hospital B. The data
from the survey was analyzed using descriptive statistics.
Budget
There was no cost incurred for the creation and distribution of the surveys. The
student utilized resources from the Pittsburg State University Irene Ransom Bradley
School of Nursing as indicated.
Strengths and Weaknesses of the Project
Strengths of the project include the pre-test acting as a control, comparing the
sample’s pre- and post-test scores to determine if the participants feel more confident in
their communication methods. Weaknesses of the study include human error and false
information that may be provided by participants, affecting the validity of the research.

34
Nurses are the only portion of the interdisciplinary team who are invited to provide
insight on disruptive behavior. This is concerning because disruptive behavior is
experienced across the spectrum of healthcare providers.
Summary
A descriptive mixed-methods research design was used in this scholarly project
through convenience sampling from two small hospitals in the Midwest. Descriptive
statistics was evaluated upon review of the research. A review of data analysis was used
to determine whether registered nurses feel more confident in managing disruptive
behavior after learning and reviewing communication techniques. It also assessed what
types of disruptive behaviors nurses are experiencing, what outcomes are manifested
from disruptive behavior, and how it affects job satisfaction among nurses. Evaluation of
the research outcomes occurred, utilizing a one group pre-test-post-test method.

35
CHAPTER IV
Evaluation Results
Purpose
The purpose of this study was to identify what types of disruptive behavior nurses are
experiencing, discuss outcomes of disruptive behavior, and educate healthcare providers
and administrators about disruptive communication. Data was collected with the goal of
assessing disruptive behaviors, disruptive behavior’s relationship to job satisfaction, and
nurse confidence levels in managing disruptive behavior. Seven questions were
developed to guide the project:
1. What type of disruptive behavior are nurses experiencing?
2. How frequently do nurses experience disruptive behavior?
3. What outcomes do nurses perceive result from disruptive behavior?
4. Do nurses perceive there is a relationship between communication and job
satisfaction?
5. Is there a relationship between the frequency of disruptive behavior and the
nurse’s perception of the relationship between communication and job
satisfaction?
6. What is the nurse’s level of confidence in managing disruptive behavior before an
educational offering?

36
7. What is the nurse’s level of confidence in managing disruptive behavior after an
educational offering?
We can determine if nurses could benefit from communication education to understand
better communication styles and how to confront disruptive behavior through data
analysis. In this chapter, there will be a discussion of the population studied and analysis
of data collected in relation to the project’s purpose.
Sample
Two questionnaires and an educational offering were provided at two rural
hospitals in the Midwest. Nurses from the Medical-Surgical, Emergency, and Surgical
Departments were invited to participate at both hospitals. Hospital B had the addition of
Obstetrics and Intensive Care nurses. A convenience sampling of registered nurses was
utilized and determined by the number of participants at each location. Once approval
was granted through Hospital A, Hospital B, and Pittsburg State University, data was
collected within two weeks in the month of February of 2021. Only registered nurses
were asked to participate in the research study. The study did not include vulnerable
subjects including mentally disabled individuals, children, or prisoners. It did not
discriminate against specific populations due to race, religion, or ethnicity. At Hospital A,
ten nurses participated in the pre-education questionnaire, while only five nurses
participated in the post-education questionnaire. Hospital B had 41 participants in the
pre-and post-education questionnaire. A total of 51 nurses participated in the pre-
questionnaire, and 46 nurses contributed to the post-education questionnaire. In both the
pre-and post-questionnaires, only two males participated in the study. The majority of the
nurses in both studies had greater than 15 years of experience, worked days, and worked

37
on the Medical-Surgical unit, as portrayed in Tables 1-3 below. Descriptive statistics
were used to calculate frequencies and percentages.
Table 1.
Total Years of Experience
Pre-Questionnaire Post-Questionnaire
Year Frequency
(N=51)
Percent (%) Frequency
(N=47)
Percent (%)
0-1 Year 3 5.9 2 4.3
2-5 Years 2 3.9 1 2.1
5-10 Years 16 31.4 13 27.7
10-15 Years 5 9.8 6 12.8
Greater than 15
Years
25 49 24 51.1
Missing
1
2.1
Total
51
100
47
100
Table 2.
Current Unit
Pre-Questionnaire Post-Questionnaire
Frequency
(N=51)
Percent (%) Frequency
(N=47)
Percent (%)

38
Medical/Surgical/General 22 43.1 17 36.2
Intensive Care 1 2 1 2.1
Outpatient Clinic 5 9.8 5 10.6
Emergency Department 5 9.8 5 10.6
Obstetrics 4 7.8 4 8.5
Surgery 14 27.5 14 29.8
Missing
1
2.1
Total 51 100 47 100
Table 3.
Current Shift
Pre-Questionnaire Post-Questionnaire
Frequency
(N=51)
Percent (%) Frequency
(N=47)
Percent (%)
Days 40 78.4 37 78.7
Evenings 1 2 1 2.1
Nights 10 19.6 8 17
Missing 1 2.1
Total 51 100 47 100
Description of Key Terms/Variables

39
Four key variables were evaluated throughout the project. Disruptive behavior is
an independent variable that could lead to adverse outcomes. Therefore, the goal was to
measure outcomes (if any) nurses perceive or experience and how often they experience
these outcomes. Job satisfaction, outcomes, and confidence levels are all dependent
variables that stem from disruptive behavior. Therefore, it is essential to measure all these
variables thoroughly and evaluate if there is a relationship between the independent and
dependent variables.
Analysis of Project Questions
This project was performed to answer seven questions. Therefore, to ensure
thoroughness, each question will be answered individually.
The first question asks, “What type of disruptive behavior are nurses
experiencing?” Participants were given five specific statements and asked to state if they
were true or false. These statements included, “A nurse practitioner or doctor has hung up
the telephone on me”, “A nurse practitioner or doctor has yelled at me”, “A nurse
practitioner or doctor has belittled me”, “A nurse practitioner or doctor has cursed at me”,
and “A nurse practitioner or doctor has asked me not to call back about a patient situation
I found concerning”. A total of 51 (N=51) participants responded. Descriptive statistics
calculating frequency, percent, and mean were used for the table below (Table 4). The
majority of the nurses responded “True” to experiencing “Hung up on phone” (51%),
“Yelled” (72.5%), and “Belittled” (68.6%). The majority of nurses answered “False” to
“Cursed At” (58.8%) and “Asked Not to Call Back” (76.5%).
Table 4
Types of Disruptive Behavior

40
Frequency (N=51) Percent (%) Mean
Hung up Phone
True 26 51
1.49
False 25 49
Total 51 100
Yelled
True 37 72.5
1.27
False 14 27.5
Total 51 100
Belittled
True 35 68.6
1.31
False 16 61.4
Total 51 100
Cursed At
True 21 41.2
1.59
False 30 58.8
Total 51 100
Asked Not to Call
Back
True 12 23.5
1.76
False 39 76.5
Total 51 100
Question two examined, “how frequently do nurses experience disruptive
behavior?” To answer this question, this author asked the participants, “about how often
do you witness disruptive behavior in the workplace?” To answer this question, data was
derived utilizing descriptive statistics. Results stated that 2% of the subjects witnessed
disruptive behavior daily, 25.5% weekly, 17.6% monthly, 3.9% annually, and 51% stated

41
almost never (Table 5). The mean was calculated as 3.76, meaning an average rating of
“monthly” Descriptive statistics were utilized to calculate frequency, percent, and mean.
Table 5.
How Often Disruptive Behavior is Witnessed
Frequency (N=51) Percent (%)
Daily 1 2
Weekly 13 25.5
Monthly 9 17.6
Annually 2 3.9
Almost Never 26 51
Total 51 100
The third research question inquires, “What outcomes do nurses perceive result
from disruptive behavior?” Nurses were asked to answer true or false to two quantitative
questions measuring outcomes. The first question regarding outcomes states, “A patient
was placed in a dangerous situation due to disruptive communication. (i.e. yelling,
belittling, hanging up the phone, etc.). Of the respondents, 23.5% stated “true” while
76.5% answered “false” (Table 6). The second question included, “I have witnessed a
patient experience harm due to disruptive communication. (i.e. yelling, belittling, hanging
up the phone, etc.). A total of 21.6% of the respondents indicated “true” while 78.4% said
“false” (Table 7). Descriptive statistics were used to calculate frequency, percent, and
mean.
Table 6.

42
A Patient was Placed in a Dangerous Situation due to Disruptive Communication
Frequency (N=51) Percent (%)
True 12 23.5
False 39 76.5
Total 51 100
Note. The mean is 1.76.
Table 7.
A Patient Experienced Harm due to Disruptive Communication
Frequency (N=51) Percent (%)
True 11 21.6
False 40 78.4
Total 51 100
Note. The mean is 7.6.
The participants were immediately asked a qualitative follow-up question to
analyze a specific outcome that the nurse had experienced. They were asked, “Please
explain how the patient was harmed or placed in a dangerous situation resulting from
disruptive communication.” Ten nurses from Hospital B and four nurses from Hospital A
answered this question (N=14). Two participants explained that two patients “Had to be
taken back to surgery.” and that it “Could have been avoided.” Five responses stated the
physician dismissed their concerns. Responses included, “Refused to listen to RN, [the
patient] coded.” “Made me feel like I was seeing something that wasn’t there; had me
second-guessing my skills as a nurse and made me fearful to call them back.” “The
doctor told me that they were too busy to deal with this and this was not real, and they

43
had real sick people to attend to.” “Provider on call at night but gave minimal medication
because the patient was not his.” Three respondents stated that doctors had yelled at staff,
describing “Physician was cursing and yelling in frustration during a YAG procedure…
patient verbalized feeling belittled and said, ‘he was cussing at me.’ There could have
been injury to the eye with the laser”-“when a surgeon starts yelling during a surgery I fill
it puts the patient at risk due to loss of control and focus from the Dr.” One respondent
stated, “I have witnessed nurses afraid to call about concerns because they had been
belittled by a physician before.” One respondent said, “[patients] left in small town
hospitals. ICU [patients] admitted creating hardships for inappropriate admits”. One
nurse stated, “Would rather not say.” Another respondent stated, “I have not witnessed
[a] patient in this situation.” One participant stated, “I have witnessed nurses afraid to call
about concerns because they had been belittled by a physician before.”
The fourth research question asked, “Do nurses perceive there is a relationship
between communication and job satisfaction?” Participants were asked to rate
“Communication between caregivers affects job satisfaction” on a Likert Scale to assess
the level of job satisfaction. The majority of the respondents (96.1%) stated “agree,”
while the rest of the respondents (3.9%) stated “somewhat agree” (Table 8). Descriptive
statistics were utilized to calculate frequency, percent, and mean.
Table 8.
Level of Satisfaction
Frequency (N=51) Percent (%)
Agree 49 96.1
Somewhat Agree 2 3.9

44
Neutral 0 0
Somewhat Disagree 0 0
Disagree 0 0
Total 51 100
Note: The mean is 1.04
The fifth research question inquires, “Is there a relationship between the
frequency of disruptive behavior and the nurse’s perception of the relationship between
disruptive behavior and job satisfaction?” A one-way ANOVA was conducted to
compare how often nurses witness disruptive behavior and the nurse’s perception of
communication’s effect on job satisfaction. There was a significant effect of the
frequency of disruptive behavior on the nurse’s perception of communication’s effect on
job satisfaction [F(46, 4) = 1.558, p = 0.202]. Due to the limited number of cases, the
author could not conduct a post hoc test. The results from the one-way ANOVA test are
displayed below.
Table 9.
Perception of Disruptive Behavior’s Effect on Job Satisfaction
Sum of
Squares
df Mean
Square
F Sig.
Between
Groups
0.229 4 0.057 1.558 0.202
Within
Groups
1.692 46 0.37
Total 1.922 50

45
The sixth question asks, “What is the nurse’s level of confidence in managing
disruptive behavior before an educational offering?” To answer this research question,
participants were asked to rate their confidence levels utilizing a Likert Scale. Descriptive
statistics calculating frequency, percent and mean were used to determine the results
(Table 9). The majority of the respondents (39.2%) replied “Somewhat Confident”, while
27.5% chose “Confident”, 19.6% “Neutral”, 11.8% “Somewhat Unsure”, and 2%
“Unsure” (N=51).
Table 10.
Confidence Level Before Educational Offering
Frequency (N=51) Percent (%)
Confident 14 27.5
Somewhat Confident 20 39.2
Neutral 10 19.6
Somewhat Unsure 6 11.8
Unsure 1 2
Total 51 100
Note: The mean is 2.22.
The final question asks, “What is the nurse’s level of confidence in managing
disruptive behavior after an educational offering?” In the post-questionnaire, participants
were asked, again, “What would you rate your confidence level in addressing disruptive
behavior?” Again, participants utilized a Likert Scale to rate their confidence levels.
Descriptive statistics were utilized to calculate frequency, percentage, and mean (N=47).

46
Of the respondents, 34.8% rated their confidence levels “confident”, 39.1% “Somewhat
Confident”, 17.4% “Neutral”, and 8.7% Somewhat Unsure”. None of the respondents
stated “unsure”. Results are displayed in the table below (Table 10).
Table 11.
Confidence Level After Educational Offering
Frequency (N=47) Valid Percentage (%)
Confident 16 34.8
Somewhat Confident 18 39.1
Neutral 8 17.4
Somewhat Unsure 4 8.7
Unsure 0 0
Total 46 100
Missing 1
Note: The mean is 2.00
Knowledge Gain
This study utilized a Mixed-Method design to assess nurse’s insight, experience,
and confidence levels pertaining to disruptive communication. Quantitative data reflected
findings related to how often disruptive behavior is witnessed, what type of disruptive
behaviors are exhibited, if satisfaction levels are affected by disruptive behavior, and how
confident nurses are confronting disruptive behaviors. Qualitative data provided personal
insight from the participants’ experience regarding how disruptive communication can
lead to negative outcomes.
Additional Statistical Analyses

47
After answering the seven research questions, additional statistical analyses were
performed to support the statistical evidence and report stimulating findings for further
research. A paired samples test was performed to compare the pre-and post-questionnaire
findings regarding nurse’s confidence levels when addressing disruptive behavior. The
results of the individual pre- and post-education questions regarding confidence levels
were displayed above. A paired test was used to determine if the confidence levels were
truly elevated after learning how to effectively confront disruptive behavior. According to
the paired t-test, the p-value is equal to 0.058, meaning that the findings were statistically
significant. Figure 1 displays confidence levels before the educational offering, while
Figure 2 shows an increase in confidence levels after the educational offering.

48
Figure 3
Confidence Levels before Educational Offering

49
Figure 4
Confidence Levels after Educational Offering
Another interesting finding within the research was the participants’ responses to
the question, “I feel that education regarding positive communication needs to be
included in continuing education for nurses, nurse practitioners, and Doctors.” in the pre-
and post-education questionnaires. Most of the respondents in the pre- (80.4%) and post-
(87%) questionnaire agreed with the statement. None of the participants responded,
“Somewhat Disagree” or “Disagree”. Descriptive statistics were utilized to calculate
mean, frequency, and percentage of the responses. See Table 11 for results.
Table 12.
Education Needs to be Included in Continuing Education Responses
Pre-Education Post-Education

50
Frequency
(N=51)
Percentage (%) Frequency
(N=46)
Percentage (%)
Agree
41 80.4 40 87
Somewhat Agree 9 17.6 5 10.9
Neutral
1 2 1 2.2
Somewhat
Disagree
0 0 0 0
Disagree
0 0 0 0
Total 51 100 46 100
Mean =1.22 Mean= 1.15
Summary
Results from the data analysis revealed findings in the study that were related to
the purpose of the research. The purpose of this study was to identify what types of
disruptive behavior nurses are experiencing, discuss outcomes of disruptive behavior, and
educate healthcare providers and administrators of disruptive communication. Two
questionnaires were utilized to gather quantitative and qualitative data before and after
and education offering.

51
When participants were asked what type of disruptive behavior they have
experienced within the workplace, the majority of nurses stated they were yelled at
(72.5%), belittled (68.6%), and hung up on (51%). When calculating the frequency of
disruptive behavior experienced, the bulk (51%) of the participants stated “almost never,”
followed by 25.5% of them reporting “weekly.” Although most of the subjects said they
had not witnessed a patient being placed in a dangerous situation or experienced harm
from disruptive communication, some chose to share their experiences when they
witnessed this. Harmful outcomes include patients returning to surgery, nurses
questioning their skills, and even patients coding. A total of 96.1% of participants agreed
that communication between caregivers affects job satisfaction. After receiving education
regarding disruptive communication and proper communication techniques, confidence
levels rose significantly.
The rationale for this research was to argue the need for additional education
regarding communication techniques within the workplace and practice/policy change to
support better communication styles. With this analysis of data, it can be concluded that
these changes are warranted. Further discussion about the implications of the data will
continue in Chapter V.

52
CHAPTER V
Discussion
The purpose of this study was to identify what types of disruptive behavior nurses
are experiencing, discuss outcomes of disruptive behavior, and educate healthcare
providers and administrators of disruptive communication. Understanding the
consequences of disruptive communication can help educators articulate the need for
training in conflict management and therapeutic communication methods. It can also aid
healthcare providers to be more conscious of their behavior in the professional setting.
The goal is that effective communication techniques will lead to increased job
satisfaction for nurses, higher nurse retention rates, and better patient outcomes.
Relationship of Outcomes to Research
Seven research questions were developed and tested for this scholarly project. The
first research question tested was, "what type of disruptive behavior are nurses
experiencing?" The pre-questionnaire used five specific questions utilizing a true-false
format of answers to collect data. These questions included:
• A nurse practitioner or doctor has hung up the telephone on me.
• A nurse practitioner or doctor has yelled at me.
• A nurse practitioner or doctor has belittled me.
• A nurse practitioner or doctor has cursed at me.

53
• A nurse practitioner or doctor has asked me not to call back about a patient
situation I found concerning.
The majority of the nurses responded "True" to experiencing "Hung up on phone"
(51%), "Yelled" (72.5%), and "Belittled" (68.6%). These results depict the forms of
disruptive behaviors nurses are experiencing. Researchers, educators, and policymakers
need to understand the behaviors are in order to focus on these issues when addressing
disruptive communication.
The second question evaluates how frequently nurses experience disruptive
behavior. The majority (51%) stated, "Almost Never," followed by 25.5% answering
"Weekly," 17.6% "Monthly," and 3.9% "Annually," and 2% "Daily." The frequency of
the behavior emphasizes how relevant the issue truly is. If most nurses responded "Daily"
versus "Almost Never," the problem would be ubiquitous and would need to be addressed
immediately. Remarkably, even though most nurses stated, "Almost Never," the second
most prevalent response was "Weekly," which is quite frequent, therefore, increasing the
relevance of the issue.
The third question was, "What outcomes do nurses perceive result from disruptive
behavior?" This question assesses if nurses have witnessed harmful situations and
outcomes and specifically asks nurses to share their experiences with the researcher.
Remarkably, 23.5% of respondents have seen a patient being placed in a dangerous
situation, and 21.6% witnessed actual harm to a patient. A total of 14 participants (27%)
shared their experiences. Of the experiences shared, most (five) were related to
doctors/nurse practitioners dismissing nurses' concerns. This led to a patient coding, a
nurse second-guessing his/her skills, and upset patient family members. Three

54
respondents shared instances where patients were in danger because the physician/NP
was yelling. Two participants described patients going back to surgery because of
disruptive behaviors. One respondent described patients being admitted and kept in rural
hospitals when they need a higher level of care. Another volunteer stated they have
witnessed other nurses display apprehension when calling doctors/nurse practitioners for
a patient concern. Knowing the frequency and type of negative outcomes fuels the need
for change, as well as education for healthcare providers. The main goal of healthcare is
safety and quality of care. If research proves a relationship between disruptive behavior
and a lack of patient safety, stakeholders such as policymakers, educators, and health
institutions will be more motivated for change.
The fourth question examines nurse’s perception of communication’s relationship
with job satisfaction. Participants were asked to rate "Communication between caregivers
affects job satisfaction" on a Likert Scale to assess the level of job satisfaction. The
majority of the respondents (96.1%) stated: "agree." Job satisfaction affects retention
rates. Nurses are already experiencing a shortage; therefore, low retention rates
exacerbate the issue. Thus, nursing leaders need to know what affects job satisfaction and
what they can do to improve it. This question shows how important proper
communication and behaviors are for retaining nurses.
The fifth question queries, "Is there a relationship between the frequency of
disruptive behavior and the nurse’s perception of the relationship between disruptive
behavior and job satisfaction?" A one-way ANOVA test was conducted to compare how
often nurses witness disruptive behavior and the nurse’s perception of communication’s
effect on job satisfaction. There was a significant effect of the frequency of disruptive

55
behavior on the nurse’s perception of communication’s effect on job satisfaction [F(46,
4) = 1.558, p = 0.202]. Due to the limited number of cases, the author could not conduct a
post hoc test. These results suggest that the frequency of disruptive communication can
influence the nurse’s perception of disruptive behavior’s effects on job satisfaction. For
example, if a nurse rarely experiences disruptive behavior within the workplace (such as
annually) they are more likely to believe that disruptive behavior does not affect job
satisfaction. Although frequency may influence perception, nursing leaders need to pay
attention and listen to their nurses when they report any dissatisfaction within the
workplace.
The sixth question asks, "What is the nurse's level of confidence in managing
disruptive behavior before an educational offering?" The majority (39.2%) of participants
responded, "Somewhat Confident." A total of 27.5% chose "Confident," 19.6%
"Neutral," 11.8% "Somewhat Unsure," and 2% stated "Unsure." This question allowed
this author to compare the pre-and post-questionnaire answers to evaluate the educational
offering's effectiveness. This, too, validates the need for continuing education regarding
effective communication.
The final question asks, "What is the nurse's level of confidence in managing
disruptive behavior after an educational offering?" Like the previous question, this
question assesses the effectiveness of the educational offering. Of the respondents, 34.8%
rated their confidence levels "confident," 39.1% "Somewhat Confident," 17.4%
"Neutral," and 8.7% Somewhat Unsure". None of the respondents stated, "Unsure."
Evidence showed that confidence levels raised after the educational offering, deeming the
curriculum as valid. For instance, data shows that the amount of nurses who marked

56
“confident” increased from 19.6% to 34.8% and the number of respondents who stated
“unsure” in the pre-questionnaire (2%) declined to 0% in the post-questionnaire.
Observations
The results from this study indicate the need for additional education regarding
communication and proper communication techniques. As stated before, patient safety
and quality of care are the essential components of healthcare. As found in the research,
disruptive behaviors hinder safety and quality of care. Therefore, the need for change is
validated, whether it is education, policy change, or institutional policies. An interesting
finding within the research was the participants' responses to the question, "I feel that
education regarding positive communication needs to be included in continuing education
for nurses, nurse practitioners, and Doctors." in the pre-and post-education
questionnaires. A total of 80% of respondents answered "agree" in the pre-questionnaire.
In comparison, the number of respondents rose to 87% in the post-questionnaire. This
indicates an agreeance among the participants that continual education needs to be
implemented.
Evaluation of Theoretical Framework
The theoretical framework, CAT was applied to the research project through
nurse education. CAT observes the human tendency to adjust their behavior to match
their interaction with others. The nurses were educated on the usage and effects of verbal
and non-verbal cues. Verbal cues include word choice and communication styles, such as
passive, passive-aggressive, aggressive, and assertive communication. Non-verbal cues
include the usage of space, body language, facial expression, gestures, eye contact, and
vocal expression. In the educational offering, they were encouraged to use assertive

57
communication while maintaining aware of their non-verbal cues to effectively and
respectively exchange information with a doctor or nurse practitioner.
SET is a social psychological perspective that explains that reciprocity and
behaviors are based on a cost-benefit analysis. For example, a doctor is more likely to
comply with a nurse’s request if the nurse communicates their needs in a polite,
respectful way. While verbal and non-verbal cues can help the nurses obtain what they
want/need from the nurse/doctor relationship, the education followed SET by
emphasizing the importance of following the SBAR format when discussing concerns
with a physician. Using SBAR helps health-care providers avoid long narrative
descriptions and ensures that facts are shared with the doctor or nurse practitioner. The
SBAR format also allows for the nurse to clearly state what they expect to gain
from the conversation. Utilizing concise language is important, for in a study
performed by McCaffrey et al. (2010), doctors reported they preferred to spend little
time on communication, and they expect nurses to anticipate the doctor’s needs
and take orders correctly.
The pre- and post-education questionnaires allowed for the evaluation of
utilizing CAT and SET as the framework for the educational offering. To
evaluate the nurses’ confidence level utilizing SBAR for SET, they were asked to
rate the statement, “I feel comfortable utilizing the Situation Background Assessment
Recommendation (SBAR) format when communicating with a nurse practitioner or
physician” on a Likert-Scale. The scores were consistent, with 78.4% stating “agree
in the pre-questionnaire, while 78.3% agree in the post-questionnaire. While
there is consistency in responses between the pre-and post-questionnaires, it is

58
remarkable that only 2% of the respondents replied “Unsure” in the pre-
questionnaire, none of them replied “Unsure” in the post -questionnaire. To
evaluate the curriculum based on CAT and SET, nurses were asked to rate,
“What would you rate your confidence level in addressing disruptive behavior”
on a Likert-Scale. A total of 27.5% of nurses responded “Confident” in the pre -
questionnaire, raising to 34.8% in the post-questionnaire. The rise in confidence levels
in using SBAR and addressing disruptive behaviors seen in the post-questionnaire
validates the efficacy of the curriculum based on CAT and SET.
The theoretical framework, "The Schutzian Lifeworld Phenomenological
Orchestra Study," performed by Valerie Malhotra (1981), was applied to this scholarly
project. This theory compares the healthcare team to an orchestra. It describes how each
member of an orchestra provides their knowledge, experience, and talents to contribute to
the orchestra as a whole. To fully function as an orchestra, musicians have to know their
roles and anticipate everyone else's in the orchestra. Like musicians in an orchestra, each
health team member must utilize quality verbal and non-verbal communication to
understand each member's contribution to the same goal. To provide the highest quality
of care, nurses and doctors must communicate effectively to achieve the desired outcome.
The pre-and post-education questionnaires assess relationships between disruptive
behavior and its effects on the interdisciplinary team, patient outcomes, and job
satisfaction levels. Therefore, it is evaluating if disruptive communication negatively
influences the effectiveness of the healthcare team. The questionnaire also provides
insight into nursing perceptions of physician behavior changes regarding understanding
the nurse's role by asking, "I feel that if doctors properly understand the nursing role, they

59
would respect nurses more." In both—the pre- (49%) and post-questionnaires (56.5%),
the majority of the respondents replied: "agree." This supports the theory's belief that
healthcare members need to understand each other's roles to function properly. Future
studies should be performed to verify that understanding each other's roles can improve
respect and communication to prove the theory.
Evaluation of the Logic Model
In the first chapter, a logic model was established to display the relationship
between disruptive communication, adverse outcomes, and nursing education
implementation. The logic model shows the transition from the need, development,
implementation, and desired education outcomes regarding communication. This
scholarly project closely followed the logic model. First, it analyzed the prevalence of
disruptive communication and what outcomes are produced through a pre-education
questionnaire. Education regarding disruptive communication and effective
communication was then provided through a PowerPoint presentation, utilizing
information gathered through the literature review. Afterward, the participants took a
post-education questionnaire, rating their beliefs about communication and confidence
levels when confronting disruptive communication. Since this study was not longitudinal,
it is challenging to assess motivation for change, respect and understanding, active
listening, and effective, clear communication. However, perceptions did change after the
educational offering was given. Perceived confidence levels when addressing disruptive
behavior rose after receiving the educational offering. The respondents also validated the
need for continuing education regarding communication techniques. Even with a time
limitation, the logic model proved useful and appropriate for this scholarly project.

60
Limitations
Time was a factor in data collection and analysis. The information was collected
and analyzed independently by this author. Additional time would allow the researcher to
re-evaluate the research subjects at least three months after the educational offering. This
would determine if values and beliefs are consistent after completing the questionnaires
and education. The collection of data lasted two weeks at Hospital B and four weeks at
Hospital A. If there had been more time for data collection, more nurses may have
participated in the research. Another weakness was the limited sample size—a total of 51
nurses for the pre-questionnaire and 46 nurses for the post-questionnaire. Finally, the
nurses who participated in the pre-questionnaire were the same ones who participated in
the post-questionnaire Hospital B, while it is unknown if the subjects were the same for
the Hospital A questionnaires. This is due to the format of how the research project was
distributed at each hospital. Hospital B utilized Health Stream, formatted in a quiz-like
fashion. The subjects were not allowed to proceed to the "next step" until they finished
the pre-requisites. Therefore, the results were consistent, with a total of 41 nurses
participating in both surveys. ACRH used a more traditional style of collecting research
data, utilizing a pen-and-paper format of questionnaires. This format led to the
discrepancy of sample sizes in the pre-and post-questionnaires. A total of ten nurses filled
out a pre-questionnaire, while only five filled out the post-questionnaire. Using a method
such as Health Stream at both hospitals can prevent inconsistencies and provide more
accurate results. The inconsistency of the number of participants from each hospital can
also be related to the number of nurses employed at each hospital. Hospital A has less
than 50 nurses on staff, while Hospital B employs at least 100 nurses. The difference in

61
nurse population between the two hospitals explains the variation between the number of
participants at each hospital. Performing the study at two hospitals with similar sizes of
nursing staff could prevent this discrepancy.
Another limitation found within the study was the majority of respondents work
day-shift. Different shifts may have different frequencies and occurrences with disruptive
behaviors. In the pre-questionnaire, 40 participants reported working day shift, while ten
work nights and one works evenings. The post-questionnaire also had mostly day shift
nurses (N=37), while eight nurses work nights and one works evening shifts. The
collected data determining years of experience may have also been skewed, because it
may be likely that day shift nurses have more experience. According to Ritonja et al.
(2019) “While the evidence is unclear regarding age and shift work tolerance, there is
biologic plausibility for poorer shift work tolerance at older age” (p. 204). Statistics
reflects this by showing that 49% (N=25) of respondents have over 15 years of
experience in the pre-questionnaire with 52.2% (N=41) in the post-questionnaire. The
respondents' average experience in both questionnaires is 10-15 years (M=4.07, M=3.92).
With the availability of more time and a larger sample, perhaps a comparison could be
conducted, determining the frequency of disruptive behavior and years of experience as a
nurse.
Implications for Future Projects/Research
Longitudinal studies, as well as larger sample sizes, would benefit future research
regarding disruptive communication. If the researcher utilizes multiple hospitals to gather
data, using the same format for data collection would be more consistent. It would be
interesting to use the data found from this scholarly project to teach nurse practitioners

62
and Doctors the outcomes of disruptive communication, emphasizing the importance of
effective communication. Further, it would be insightful to gain nurse practitioners' and
Doctors' perspectives regarding poor outcomes and if they experience disruptive
behaviors from other NPs, Doctors, or nurses.
Implications for Practice/Health Policy/Education
This study's results indicate the need to emphasize communication styles and
techniques in nursing and medical School curriculum. Communication techniques need to
be improved, and a common language must be agreed upon by all healthcare fields. A
total of 87% of participants agreed that continuing education concerning communication
techniques among healthcare professionals needs to be implemented. Boards and private
companies may support the dissemination of continuing education.
Policies concerning disruptive communication and bullying have been deliberated
among congress in the past. For instance, in 1983, the United States Supreme Court took
on the case, Connick v. Myers in which they ruled, "First Amendment protections are
available for workplace speech only if it covers matters of public concern and does not
interfere with the office operations that benefit the public" (Smith & Coel, 2018, p.97).
Smith & Coel (2018) elaborate:
Under Connick v. Myers, anti-bullying regulations could be First Amendment
violations only if (1) the alleged bullying speech is about a public concern and (2)
the speech is not disruptive to office responsibilities that require productive
collaboration to serve the public. (p.99)
This is concerning, for this protects the bullies while leaving the targeted victims and
whistleblowers vulnerable. To address this issue, Drs. David C. Yamada, Gary Namie

63
and Ruth Namie sought state support and law reform by "…persuasively arguing that
current employment law has created an invisible workforce that is subject to extreme
emotional abuse without legal redress" (Chu, 2014, p.353). Chu (2014) examines that
37% of American workers have been bullied at work (p.27). In 1970, The Occupational
Safety and Health Act (OSHA) was signed into law to assure healthy working conditions
and safety. However, OSHA does not cover workplace bullying. In 2007, Dr. Yamada
and his team submitted The Healthy Workplace Bill to the state of Connecticut Senate to
protect the victims of bullying, require the employer to provide compensation for the
victim and remove the bully from the work environment (Chu, 2014, p.366). Fortunately,
the bill was approved, which provided a step in the right direction toward a
comprehensive statute protecting employees. Research like this scholarly project can
validate the toxicity of bullying and disruptive behaviors, pushing for further policy
change at the federal and state government levels.
Conclusion
The purpose of this study was to identify what types of disruptive behavior nurses
are experiencing, discuss outcomes of disruptive behavior, and educate healthcare
providers and administrators of disruptive communication. In this study, nurses shared
their insight, experiences, and beliefs through quantitative and qualitative analysis. The
majority (87%) of participants agreed that continuing education concerning
communication techniques among healthcare professionals needs to be implemented. A
total of 96.1% of participants agreed that communication between caregivers affects job
satisfaction. Job satisfaction is an essential variable for nurse retention rates. Therefore,
this study suggests that if institutions want to improve their retention rates during a

64
nursing crisis, they need to consider policy changes and address disruptive
communication.
This study contributes to nursing knowledge, supporting the need for positive
communication techniques, revealing adverse outcomes from disruptive communication,
and discussing continuing education. This study supports the author's belief that new
communication techniques need to be implemented in nursing and physician education.
Each member of the interdisciplinary team needs to be aware of communication styles
and practices to improve patient care quality and safety.

65
References
Bylund, C. L., Peterson, E. B., & Cameron, K. A. (2012). A practitioner's guide to
interpersonal communication theory: An overview and exploration of selected
theories. Patient Education and Counseling, 87(3), 261-267.
10.1016/j.pec.2011.10.006
Burroughs, J., & Bartholomew, K. (2014). New ways for doctors and nurses to work
together. Physician Executive, 40(3), 60-64
https://search.ebscohost.com/login.aspx?direct=true&db=bsh&AN=96107060&sit
e=ehost-live&scope=site
Center, D. (2018). Knowing oneself: The first step to be an effective member of an
interprofessional team. The Journal of Continuing Education in Nursing, 49(9),
397-399. http://dx.doi.org.library.pittstate.edu/10.3928/00220124-20180813-04
Chu, S. (2014). The workplace bullying dilemma in Connecticut: Connecticut's response
to the Healthy Workplace Bill. Connecticut Public Interest Law Journal,
13(2), 351-386. https://cpilj.files.wordpress.com/2014/07/13-conn-pub-int-l-j-
351.pdf.
Cropanzano, R., & Mitchell, M. S. (2005). Social exchange theory: an interdisciplinary
review. Journal of Management, 31(6), 875-900. 10.1177/014920630527960
Dixon-Woods M, Campbell A, Martin G, et al. (2019). Improving employee voice about
transgressive or disruptive behavior: A case study. Academic Medicine, 94(4),
579-585. 10.1097/ACM.0000000000002447
Gordon, M. B., Melvin, P., Graham, D., Fifer, E., Chiang, V. W., Sectish, T. C., &
Landrigan, C. P. (2011). Unit-based care teams and the frequency and quality of

66
physician-nurse communications. Archives of Pediatrics & Adolescent Medicine,
165(5), 424-428. 10.1001/archpediatrics.2011.54
Hailu, F. B., Kassahun, C. W., & Kerie, M. W. (2016). Perceived nurse—physician
communication in patient care and associated factors in public hospitals of Jimma
Zone, South West Ethiopia: cross sectional study. Plos One, 11(9).
10.1371/journal.pone.0162264.
Khan, A., Rogers, J. E., Melvin, P., Furtak, S. L., Faboyede, M., Schuster, M. A., &
Landrigan, C. P. (2015). Physician and nurse nighttime communication and
parents’ hospital experience. Pediatrics, 136(5), 1-10. 10.1542/peds.2015-2391d
Kimes, A., Davis, L., Medlock, A., & Bishop, M. (2015). 'I'm not calling him!':
Disruptive physician behavior in the acute care setting. Medsurg Nursing: Official
Journal of the Academy of Medical-Surgical Nurses, 24(4), 223-227.
http://library.pittstate.edu:2048/login?url=https://library.pittstate.edu:4471/docvie
w/1705664103?accountid=13211
Kowalski, K. (2018). Creating interprofessional teams. The Journal of Continuing
Education in Nursing, 49(7), 297-298.
http://dx.doi.org.library.pittstate.edu/10.3928/00220124-20180613-04
Lancaster, G., Kolakowsky‐Hayner, S., Kovacich, J., & Greer‐Williams, N. (2015).
Interdisciplinary communication and collaboration among Doctors, nurses, and
unlicensed assistive personnel. Journal of Nursing Scholarship, 47(3), 275-284.
10.1111/jnu.12130
Leonard, M., Graham, S., & Bonacum, D. (2004). The human factor: the critical
importance of effective teamwork and communication in providing safe care.

67
Quality and Safety in Health Care, 13(Suppl1), I85-I90.
10.1136/qhc.13.suppl_1.i85
Manojlovich, M. (2005). Linking the practice environment to nurses' job satisfaction
through nurse‐physician communication. Journal of Nursing Scholarship, 37(4),
367-373. 10.1111/j.1547-5069.2005.00063.x
Manojlovich, M., & DeCicco, B. (2007). Healthy work environments, nurse-physician
communication, and patients' outcomes. American Journal of Critical Care: An
Official Publication, American Association of Critical-Care Nurses, 16(6), 536-
543.
https://link.gale.com/apps/doc/A171139133/AONE?u=psu_main&sid=AONE&xi
d=34a165ab
McCaffrey, R. G., Hayes, R., Stuart, W., Cassell, A., Farrell, C., Miller-Reyes, C., &
Donaldson, A. (2010). A program to improve communication and collaboration
between nurses and medical residents. The Journal of Continuing Education in
Nursing, 41(4), 172-178. 10.3928/00220124-20100326-04
Merriam-Webster. (2018). Communication. In Merriam-Webster.com dictionary.
Retrieved February 26, 2018, from https://www.merriam-
webster.com/dictionary/communication?src=search-dict-hed
Registered Nurses’ Association of Ontario (2012). Managing and mitigating conflict in
health-care teams. Toronto, Canada: Registered Nurses’ Association of Ontario.
Retrieved June 20, 2018, from http://rnao.ca/sites/rnao-ca/files/Managing-
conflict-healthcare-teams_hwe_bpg.pdf

68
Registered Nurses’ Association of Ontario (2012). Toolkit: Implementation of best
practice guidelines. Toronto, Canada: Registered Nurses’ Association of Ontario.
Retrieved June 21, 2018, from https://rnao.ca/sites/rnao-
ca/files/RNAO_ToolKit_2012_rev4_FA.pdf
Riskin, A., Erez, A., Foulk, T. A., Riskin-Geuz, K. S., Ziv, A., Sela, R., Pessach-
Gelblum, L., & Bamberger, P. A. (2017) (2017). Rudeness and medical team
performance. Pediatrics, 139(2), e20162305. 10.1542/peds.2016-2305
Ritonja, J., Aronson, K. J., Matthews, R. W., Boivin, D. B., & Kantermann, T. (2019).
Working Time Society consensus statements: Individual differences in shift work
tolerance and recommendations for research and practice. Industrial health, 57(2),
201–212. https://doi.org/10.2486/indhealth.SW-5
Robinson, F. P., Gorman, G., Slimmer, L. W., & Yudkowsky, R. (2010). Perceptions of
effective and ineffective nurse-physician communication in hospitals. Nursing
Forum, 45(3), 206-216. 10.1111/j.1744-6198.2010.00182.x
Rosenstein, A.H., O’Daniel, M. (2005). Disruptive behavior and clinical outcomes:
Perceptions of nurses and doctors. American Journal of Nursing. 2005. 105(1),
54-64. 10.1097/00000446-200501000-00025
Smith, F. L., & Coel, C. R. (2018). Workplace bullying policies, higher education and the
First Amendment: Building bridges not walls. First Amendment Studies, 52, 96-
111. Retrieved from https://doi.org/10.1080/21689725.2018.1495094.
Thomson, K., Outram, S., Gilligan, C., & Levett-Jones, T. (2015). Interprofessional
experiences of recent healthcare graduates: A social psychology perspective on
the barriers to effective communication, teamwork, and patient-centered

69
care. Journal of Interprofessional Care, 29(6), 634–640. https://doi-
org.library.pittstate.edu/10.3109/13561820.2015.1040873
Xerri, M. (2012). Workplace relationships and the innovative behaviour of nursing
employees: a social exchange perspective. Asia Pacific Journal of Human
Resources, 51(1), 103-123. 10.1111/j.1744-7941.2012.00031.x
Zwarenstein, M., Rice, K., Gotlib-Conn, L., Kenaszchuk, C., & Reeves, S. (2013).
Disengaged: a qualitative study of communication and collaboration between
Doctors and other professions on general internal medicine wards. BMC Health
Services Research, 13(1), 1-9. 10.1186/1472-6963-13-494

APPENDIX

71
APPENDIX A
Disruptive Communication Demographic Survey
The purpose of having this survey is to gather general demographics of the participants
in this research study. This helps the researcher have a clearer vision of the participant’s
outlook and experiences.
1. What is your gender?
a. Male
b. Female
c. Trans Man
d. Trans Woman
e. Gender Fluid
f. I do not wish to respond to this question.
2. How long have you practiced as a Registered Nurse?
a. 0-1 year
b. 2-5 years
c. 5-10 years
d. 10-15 years
e. Greater than 15 years
3. What unit do you work on in your current hospital?
a. Medical-Surgical/General Ward
b. Intensive Care Unit
c. Outpatient Clinic
d. Emergency Department

72
e. OB/Labor & Delivery
4. How long have you worked on your current unit?
a. 0-1 year
b. 2-5 years
c. 5-10 years
d. 10-15 years
e. Greater than 15 years
5. Do you currently work days, evenings, or nights?
a. Days
b. Evenings
c. Nights

73
APPENDIX B
Pre-Education Questionnaire
The purpose of this study is to determine if a relationship exists between disruptive
communication and poor outcomes. The information from this study will help educators
and leaders prepare nurses, nurse practitioners, and physicians by educating and
training them on the importance of effective communication and patient advocacy.
Confidentiality will be ensured by maintaining anonymity. The results from the survey
will be viewed by the surveyor. Results from the questionnaire will be used in an
educational opportunity. Names and identifying factors will not be shared within the
educational opportunity.
1. Communication between caregivers has an effect on job satisfaction.
a. Agree
b. Somewhat Agree
c. Neutral
d. Somewhat Disagree
e. Disagree
2. Communication between caregivers directly affects patient care.
a. Agree
b. Somewhat Agree
c. Neutral
d. Somewhat Disagree
e. Disagree

74
Please choose true or false for the following statements.
3. I have felt anxiety before approaching a nurse practitioner or physician for a face-
to-face interaction for fear of disruptive communication. (i.e. yelling, sarcasm,
belittling, etc.)
a. True
b. False
4. I have felt anxiety before calling a nurse practitioner or physician for fear of
disruptive communication.
a. True
b. False
5. A nurse practitioner or doctor has hung up the telephone on me.
a. True
b. False
6. I have hung up the telephone on a nurse practitioner or doctor.
a. True
b. False
7. A nurse practitioner or doctor has yelled at me.
a. True
b. False
8. I have yelled at a nurse practitioner or doctor.
a. True
b. False
9. A nurse practitioner or doctor has belittled me.

75
a. True
b. False
10. I have belittled a nurse practitioner or doctor.
a. True
b. False
11. A nurse practitioner or doctor has cursed at me.
a. True
b. False
12. I have cursed at a nurse practitioner or doctor.
a. True
b. False
13. A nurse practitioner or doctor has asked me not to call back about a patient
situation I found concerning.
a. True
b. False
14. A patient was placed in a dangerous situation due to disruptive communication.
(i.e. yelling, belittling, hanging up the phone, etc.)
a. True
b. False
15. I have witnessed a patient experience harm due to disruptive communication. (i.e.
yelling, belittling, hanging up the phone, etc.)
a. True
b. False

76
16. Please explain how the patient was harmed or placed in a dangerous situation
resulting from disruptive communication.
17. About how often do you witness disruptive behavior in the workplace?
a. Daily
b. Weekly
c. Monthly
d. Annually
e. Almost Never
18. Improvements need to be made regarding communication between nurses, nurse
practitioners, and doctors.
a. Agree
b. Somewhat Agree
c. Neutral
d. Somewhat Disagree
e. Disagree
19. Proper communication skills and zero-tolerance policies (such as consequences
for disruptive communication) should be enforced in the workplace, nursing
schools, and medical schools.
a. Agree
b. Somewhat Agree
c. Neutral
d. Somewhat Disagree
e. Disagree

77
20. I feel comfortable contacting a nurse practitioner or physician when needed.
a. Agree
b. Somewhat Agree
c. Neutral
d. Somewhat Disagree
e. Disagree
21. I feel comfortable utilizing the Situation Background Assessment
Recommendation (SBAR) format when communicating with a nurse practitioner
or physician.
a. Agree
b. Somewhat Agree
c. Neutral
d. Somewhat Disagree
e. Disagree
22. I feel that education regarding positive communication needs to be included in
continuing education for nurses, nurse practitioners, and physicians.
a. Agree
b. Somewhat Agree
c. Neutral
d. Somewhat Disagree
e. Disagree
23. I feel that if physicians properly understand the nursing role, they would respect
nurses more.

78
a. Agree
b. Somewhat Agree
c. Neutral
d. Somewhat Disagree
e. Disagree
24. What would you rate your confidence level in addressing disruptive behavior?
a. Confident
b. Somewhat Confident
c. Neutral
d. Somewhat Unsure
e. Unsure
25. If you have any comments or questions about the survey or experience, please
leave them here.
Thank you for participating in this study. For any questions or concerns, contact Kristen
Linn at (620)-228-3828 or at [email protected].

79
APPENDIX C
Post- Education Questionnaire
The purpose of this study is to determine if a relationship exists between disruptive
communication and poor outcomes. The information from this study will help educators
and leaders prepare nurses, nurse practitioners, and physicians by educating and
training them on the importance of effective communication and patient advocacy.
Confidentiality will be ensured by maintaining anonymity. The results from the survey
will be viewed by the surveyor. Results from the questionnaire will be used in an
educational opportunity. Names and identifying factors will not be shared within the
educational opportunity.
1. Improvements need to be made regarding communication between nurses, nurse
practitioners, and doctors.
a. Agree
b. Somewhat Agree
c. Neutral
d. Somewhat Disagree
e. Disagree
2. Proper communication skills and zero-tolerance policies (such as consequences
for disruptive communication) should be enforced in the workplace, nursing
schools, and medical schools.
a. Agree
b. Somewhat Agree

80
c. Neutral
d. Somewhat Disagree
e. Disagree
3. I feel comfortable contacting a nurse practitioner or physician when needed.
a. Agree
b. Somewhat Agree
c. Neutral
d. Somewhat Disagree
e. Disagree
4. I feel comfortable utilizing the Situation Background Assessment
Recommendation (SBAR) format when communicating with a nurse practitioner
or physician.
a. Agree
b. Somewhat Agree
c. Neutral
d. Somewhat Disagree
e. Disagree
5. I feel that education regarding positive communication needs to be included in
continuing education for nurses, nurse practitioners, and physicians.
a. Agree
b. Somewhat Agree
c. Neutral
d. Somewhat Disagree

81
e. Disagree
6. I feel that if physicians properly understand the nursing role, they will respect
nurses more.
a. Agree
b. Somewhat Agree
c. Neutral
d. Somewhat Disagree
e. Disagree
7. I am aware of the consequences of my actions and the risks I am taking by
ignoring disruptive behavior.
a. Agree
b. Somewhat Agree
c. Neutral
d. Somewhat Disagree
e. Disagree
8. Physicians, nurse practitioners, and administrators should be included in
education regarding communication techniques and avoiding disruptive behavior.
a. Agree
b. Somewhat Agree
c. Neutral
d. Somewhat Disagree
e. Disagree
f.

82
9. What would you rate your confidence level in addressing disruptive behavior?
a. Confident
b. Somewhat Confident
c. Neutral
d. Somewhat Unsure
e. Unsure
10. How likely are you to report events that involve disruptive behavior to your
supervisor?
a. Likely
b. Somewhat Likely
c. Neutral
d. Somewhat Unlikely
e. Unlikely

83
APPENDIX D
Informed Consent
Title of Research Disruptive Communication Among the Interdisciplinary Team:
Gaining Insight and Providing Nurse Education
Principle Investigator,
Affiliation and Contact Information Kristen Anderson, BSN, RN
Pittsburg State University
Irene Ransom Bradley School of Nursing
Email: [email protected]
Phone: 620-228-3828
Additional Investigators and Affiliations Kristi Frisbee, DNP, RN
Pittsburg State University
Irene Ransom Bradley School of Nursing
Amanda Alonzo, Ph.D.
Pittsburg State University
Irene Ransom Bradley School of Nursing
Alisha Mason-Collins, Ph.D.
Pittsburg State University
Institutional Contact Pittsburg State University
Irene Ransom Bradley School of Nursing
Phone: 620-235-4431
Introduction and Purpose of the Study
Communication is a vital skill that every healthcare professional should possess. When
healthcare professionals communicate effectively, care is delivered safely and
efficiently. However, when communication is disruptive, healthcare professionals have
reported dissatisfaction, misinterpretation, medication errors, and mortalities as a result
of disruptive communication. The purpose of this study is to validate the relationship
between disruptive communication and poor outcomes while teaching nurses
communication techniques and how to manage disruptive behavior.
Description of the Research
Participants will be asked to fill out a questionnaire, regarding their personal experience
with disruptive communication. Afterwards, they watch a PowerPoint presentation
discussing the harmfulness of disruptive communication and how it can be improved.
Afterwards, the participant will fill out a second questionnaire regarding the education.
Potential Risks and Discomforts
Risk for participation in this study include, but are not limited to emotional
stress/discomfort, loss of confidentiality, and embarrassment.
Potential Benefits
Potential benefits to the subjects include letting participants voices be heard and being
part of a research project. Findings from this research project may benefit subjects by

84
changing policies within their own hospitals once a problem is established. Benefits to
the field would be supportive research findings toward disruptive communication and
poor outcomes. It would add educational suggestions and findings to the field, as well.
Confidentiality
To maintain the highest level of confidentiality, the collected information will not
contain any participant identifier and will be anonymously collected by the researcher.
Any identifying material will be omitted from the statistics provided during the
educational project. Information will be recorded and stored without any identifiers to
maintain obscurity.
Compensation
No compensation will be offered to the subjects.
Voluntary Participation and Authorization
Your decision to participate in this study is complete voluntary. If you decide to not
participate in this study, it will not affect the care, services, or benefits to which you are
entitled
Withdrawal from the Study and/or Withdrawal of Authorization
If you decide to participate in this study, you may withdraw from your participation at
any time without penalty.
Cost/Reimbursements
There is no cost for participating in this study. Any medical expenses resulting from
participation in this study will not be reimbursed by the investigators.
I voluntarily agree to participate in this research program
□ Yes
□ No
Note: A copy of the consent will be kept by the Principal Investigator. The
participant may print a copy of the consent form if he/she/they wish.

85
APPENDIX E
Nurse Education

86

87

88

89

90

91