Dislokasi Hip 2
30
Anatomi
Transcript of Dislokasi Hip 2

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 1/30
Anatomi

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 2/30
ANATOMY
Femur connects toacetabulum by 5separated ligaments,such as:
Iliofemoral ligament Pubofemoral ligament
Ischiofemoral ligament
transverse acetabular
ligament
femoral head ligament
2

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 3/30
DF!N!T!ON " T!O#O$Y
%ip &oint dislocation is a situation 'here femoralhead locates out of the acetabulum
(auses
trauma )rom high pressure or energy, suchas traffic accident and fall )rom signi)icantaltitude
*

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 4/30
Posterior Dislocation
+-./ cases
Mostly because o) Tra))ic accident
0ressure is trasmitted by 2 'ays: During high deceleration, knee hit
dashboard and distribute the pressurethrough )emur to hips
!) the leg is e1tended and nee is loced,
the pressure can be distributed )romfloorboard through thigh and lo'er o)hip 3oint
4

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 5/30

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 6/30
type ! dislocation is a puredislocation 'ith at most aninsigni)icant posterior 'all
)ragmenttype !! dislocation isassociated 'ith a single largeposterior 'all )ragment
type !!! dislocation has acomminuted posterior 'all)racture
type !6 has an 7acetabular)loor8 9more than posterior
'all )racturetype 6 dislocation isassociated 'ith a )emoralhead )racture

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 7/30
$e3ala linis
%ip 3oint in a state o) flexion ,adduction , and endorotasi
The leg loo shorterFemur caput is palpabled in the
pel;is

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 8/30
<adiology 1amination
On anteroposterior 9A0photo, femoral headseems located out fromacetabulum and placed
above itObli=ue photo can be used
to measure )ragment
CT scan is the best 'ay toidenti)y acetabulum)racture and e;ery bone)ragments

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 9/30
MANA$MNT
Must do repotition immediately Closed reductioncan be done by a couple methods :>igelo', ?timson,dan Allis
!n type !! a)ter reposition, big )ragment is )i1ated 'ithscre' by surgery
!n type !!! usually per)orms close reduction and)ragments that trapped in acetabulum 'ill undergo
surgery Type !6 dan 6 reduction and surgery
.

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 10/30
?timson Methods
0atients in the proneposition , lo'er limb traumale)t hanging
0el;ic immobili@ed bypressing the sacrum
The le)t hand holds thedoctor anle and )le1ion .
<ight hand holding do'n the
area belo' the nee Bith the rocing motion and
rotation as 'ell as directpressure to do repositioning
C

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 11/30
>igelo' Methods
The patient in the supineposition on the )loor
Doing the opposite
traction in the regionanterior superior iliacspine and ilium
#egs )le1ed . or more
in the abdominal areaand carried out alongitudinal traction
CC

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 12/30
Allis Methods
The patient in the supineposition
Doing pel;ic immobili@ationFle1ion o) the nee at .and legs diaddusi light andmedial rotation
0er)orm ;ertical tractionand )emoral head isremo;ed )rom the posteriorpart o) the acetabulum
%ip and nee is e1tended 'ith caution
C2

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 13/30
A)ter open reduction, ne1t step is apply traction onthe leg
Traction is being maintained )or 3 weeks (ouple
days a)ter reduction, acti;e and passi;e mo;ement o)the hip 3oint can be done
!n the end o) third 'ee, patient is permitted to 'alusing the kruk
0atient is allo'ed to lean on himself at the end o) week 121! and is permitted to do normalactivity "1# months a)ter surgery
7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 14/30
OM0#!A?!
$schiadicus nerve in%ury
&ascular in%ury ?ometimes there is ruptur on thesuperior gluterus artery and bleeding may occur
Corpus femoris fracture!) it happens at the same time 'ith hip dislocation,
usually 'e missed the hip dislocation ?o that 'eha;e to do Eray e1amination )or e;ery )emoral body,
trochanter and hip )ractures

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 15/30
'vaskular (ecrosis
A;asular necrosis is seen on E-<ay as increasedopacity )emoral head, but this change cannot beidenti)ied at least )or 'ee, and sometimes more9until 2 years, depends on ho' )ast the bone is beingmanaged 'ell
)nreducted dislocation A)ter 'ees, untreated dilocation rarely can be reducted
'ith closed manipulation and need open reduction
*steoartritis
?econdary OA usually occurs and caused by 9Cdestroyed cartilago 'hen dislocated, 92 )ragmentremains on 3oint 9* )emoral head ischemic necrosis

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 16/30
'nterior Dislocation

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 17/30
Anterior dislocation
Anterior dislocation is most o)ten caused byhypere1tension pressure against the abducting leg
li)ting the )emoral head out o) the acetabulum
Gsually the lateral )emoral head remains in thee1ternal obturator muscle but can also be )ound
belo' 9 obturator dislocation or under the iliopsoasmuscle in relation to the superior pubic ramus9 dislocation pubis
CH

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 18/30
(lassi)ication anterior dislocation o) the hip 3oint according to psteinType I: Superior dislocations, including
pubic and subspinous IA No associated fractures
IB Associated fracture or impaction ofthe femoral head
IC Associated fracture of the acetabulum
Type II: Inferior dislocations, includingobturator, and perineal
IIA No associated fractures IIB Associated fracture or impaction of
the femoral head
IIC Associated fracture of the acetabulumC+

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 19/30
(#!N!(A# F!ND!N$
%ip 3oint in a positionesorotasi
1tension and abduction
There 'as no shorteningo) the limbs
Bhere the )emoral head
can be palpated easily in)ront o) the inguinal region
%ip 3oint di))icult to mo;e
C.
7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 20/30
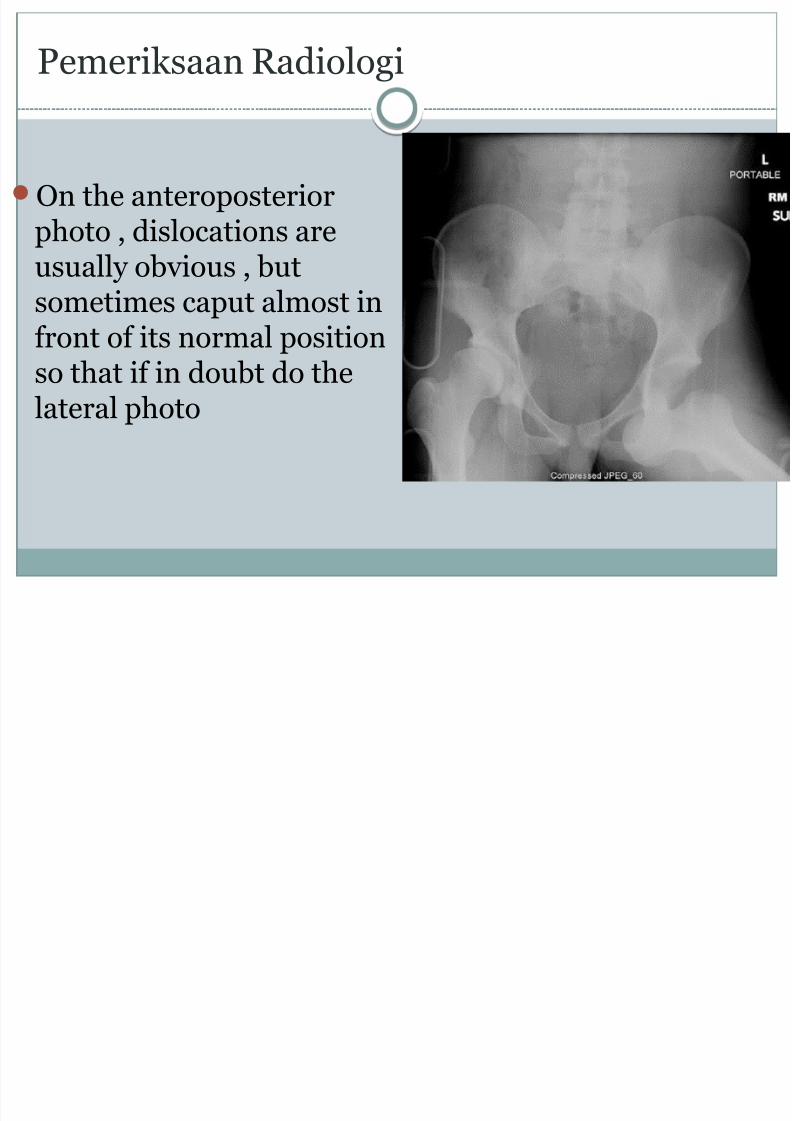
0emerisaan <adiologi
On the anteroposteriorphoto , dislocations are
usually ob;ious , butsometimes caput almost in)ront o) its normal positionso that i) in doubt do the
lateral photo

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 21/30
C+(-'. D$/.*C'$*(

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 22/30
Central Dislocation
The central dislocation is a fracture dislocation , 'hichis caput )emur is located on the medial acetabulumfracture
22

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 23/30
Mechanism O) !n3ury
These dislocations can occur i) someone falls fromheight, falling one hand , or blow on the
trochanter ma%or This punch can push caput)emoris and the acetabulum base to cause )racture o)the acetabulum and pel;is

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 24/30
(linical ?ymptoms
The position o) the pel;is seemed normal0ruises and abrasions lateral sectionThe mo;ement o) the hip 3oint is ;ery limited
24

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 25/30
0emerisaan <adiologi
On the anteroposterior photo , caput )emorisappears shifted to the medial and there isfractures of the acetabulum floor

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 26/30
The patient 'as placedin a supine position ,
then an assistant toper)orm a lateraltraction , 'hileoperators per)orm
longitudinal traction

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 27/30
T<ATMNT
?urgeons attracti;e 'ith strong thigh and then bring out the head o)the thigh mengaddusi , use hard pads as a )ulcrum
!) this method is successful, longitudinal traction is maintained
)or 4- 'ees 'ith E - ray inspection to ensure that the caput)emoris remain under 'eight-bearing part o) the acetabulum
!) manipulation fails , the combination o) longitudinal andlateral traction can reduce dislocation )or 2-* 'ees
On all o) these methods , the mo;ement needs to begin as soon as
possible Bhen traction is remo;ed , the patient is allo'ed to 'ae up 'ith
the support o) crutches 9+'ees

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 28/30
!ndication o) operation:
'cetabulum fracture 'ith shi)t o) I 2 mm in thedome o) the acetabulum
Posterior wall fracture 'ith I 5 / in;ol;emento) the 3oint articulation sur)ace on the posterior 'all
(linical instability in )le1i . degree
ragments stuck in the acetabulum a)ter closed
reduction
2+

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 29/30
(ompliaction
6isceral in3ury and se;ere shoc
?ti))ness o) 3oints , 'ith or 'ithout osteoarthritis
Necrosis avaskular

7/26/2019 Dislokasi Hip 2
http://slidepdf.com/reader/full/dislokasi-hip-2 30/30
0<O$NO?!?
The prognosis o) the hip 3oint
dislocation depending on :The damage other tissuesThe initial management o) dislocationThe se;erity o) the dislocation
*