Diseases of gall bladder. Drawing of the normal embryologic development of the gallbladder and bile...
42
Diseases of gall bladder
-
Upload
sharleen-hubbard -
Category
Documents
-
view
223 -
download
2
Transcript of Diseases of gall bladder. Drawing of the normal embryologic development of the gallbladder and bile...

Diseases of gall bladder

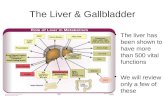
Drawing of the normal embryologic development of the gallbladder and bile ducts illustrates the foregut (A), the cranial end of the hepatic diverticulum, which represents pars hepatica (B) and the
cystic diverticulum (C). The ventral (D) and dorsal (E) pancreas are also demonstrated.

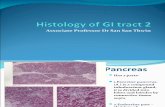
Normal gallbladder histology. The undulating mucosal epithelium overlies a delicate lamina and only one smooth muscle layer.
No muscularis mucosae .No submucosa.

Normal physiology
• Bile excretion is normally 500-1000 ml/day• Bile is concentrated 5-10x via active absorption of electrolytes accompanied
by passive movement of water• CCK causes gallbladder contraction and release of stored bile 50ml into gut• Bile is critical for intestinal absorption of dietary fat, but NOT the gallbladder.• Bile is 2/3 bile salts, bicarbonate rich, has 3% organic solutes.
• Bile salts: cholates, chenodeoxycholates, deoxycholates, lithocholates, are highly effective detergents, solubilize water-insoluble lecithin secreted by the liver
• Lecithin (phosphatidylcholine): hydrophobic, non-aqueous;
• 95% of secreted bile salts is reabsorbed in ileum and returned to liver via portal blood, called enterohepatic circulation of bile salts.
• Cholesterol is eliminated by loss of 0.5 g of bile salts per day

Congenital Anomalies
• Congenitally absent/Agenesis
• Duplication
• Aberrant location (partial or complete embedding in liver substance)
• Foulded fundus creating phrygian cap
• Hypoplastic narrowing of biliary channels

Abnormal positionLeft sided (with or without situs inversus), intrahepatic (5%), retroperitoneal, suprahepatic; also
within falciform ligament, lesser sac or abdominal wall. Agenesis (absence)Usually no cystic duct eitherAssociated with choledocholithiasis, duodenal atresia and other congenital anomaliesNo clinical significance CystsMay begin as pseudodiverticula (Rokitansky-Aschoff sinuses) with progressive occlusion of
communication with gallbladder DiverticulaSolitary, 6 mm to 8 cmRarely are congenital anomalies with all 3 layers of gallbladder wallUsually pseudodiverticula (Rokitansky-Aschoff sinuses) with incomplete muscular wall; due to
cholelithiasis or cholecystitis HeterotopiaAlso called ectopia or choristomaNormal tissue in abnormal locationUsually incidentalIncludes liver; gastric ,pancreatic heterotopia with acinar tissue, rarely islets, that may cause
acute pancreatitis in gallbladder

Gastric Hetrotropia

Pancreatic hetrotropia

Hourglass gallbladderDivided by central constrictionVariant of transverse septate gallbladderUsually acquired, due to septum of inflamed fibrous tissue or adenomyomatous
hyperplasia HypoplasiaAssociated with extrahepatic biliary atresiaMicro gallbladderDefined as less than 2-3 cm long, 0.5 -1.5 cm wideAssociated with idiopathic neonatal hepatitis, alpha-1-antitrypsin disease, cystic
fibrosisMultiseptate gallbladderCongenital or acquired3-10 communicating compartments lined by columnar epitheliumStones often present in adults .Phrygian capInversion of distal fundus into body, to which it may become adherentEither anatomic variant or acquired abnormalityPresent in 5% of cholecystograms. Wandering gallbladderLong mesentery or no firm attachment to liverAt risk for torsion.

Figure 18-48 Phrygian cap of the gallbladder; the fundus is folded inward.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 27 February 2006 12:33 PM)
© 2005 Elsevier

Cholelithiasis
• Upto 20% of adult population
• Majority is symptom free
• 90% cholesterol stones
• 10% pigment stones (bilirubin & calcium)

Cholesterol gallstones.

Pigment gallstones.

Gallstonesprevalence & risk factors
• Cholesterol stones1. European & Americans2. Advancing age3. Estrogen , oral contraceptives & pregnancy4. Obesity & metabolic Syn5. Rapid weight reduction6. Gallbladder stasis ;neurogenic or hormonal7. D19H is
1. ABCG5 & ABG2 gene variant ( ATP-binding cassette transporters).
8. Inborn disorder of bile acid metabolism9. Hyperlipidemia

Pathogenesis of cholesterol stones
Only 10% are pure (at least 90% cholesterol), the remainder are mixtures with at least 60% cholesterol by weight
1. initially bile supersaturation with cholesterol occurs,
2. Cholesterol monohydrate precipitates when no longer soluble in bile; (initial crystallization),
3. Accelerated cholesterol nucleation in the bile4. then stone growth facilitated by bile stasis
hypomotility of GB 5. & mucin hypersecretion

four contributing factors for cholelithiasis:
1. supersaturation,2. cholesterol crystal nucleation, 3. gallbladder hypomotility,4. and accretion within the gallbladder mucous
layer.

Gallstonesprevalence & risk factors
• Pigment stones– Asian >Westerners - rural>urban– Chronic haemolytic syndromes– Biliary infection– G.I. disorder;
• ileal disease (crohn),• ileal resection or bypass, • cystic fibrosis with pancreatic insuffiency

Pathogenesis of pigment stones• Composed of calcium salts of unconjugated bilirubin.• Black stones associated with (increased unconjugated bilirubin in
bile) Composed of calcium bilirubinate, calcium salts & mucin glycoprotein
• older age,• chronic hemolysis, • cirrhosis, • sclerosing cholangitis • severe ileal dysfunction or bypass
• Brown (not black) stones associated with infected bile (usually E. coli).
• Microbial glucuronidase hydrolysis bilirubin glucuronide, • Ascaris lumbricoides or schistosoma liver fluke

Cholecystitis
• Acute cholecystitis– Calculus– Acalculus
• Chronic cholecystitis– AIDS-related,– emphysematous, – eosinophilic, – follicular, – gangrenous, – granulomatous, – malakoplakia, – porcelain gallbladder, – xanthogranulomatous

Acute cholecystitismorphology
• GB usually enlarged & tense• Discolored by subserosal hemorrhage• GB wall thickened, edematous & hyperemic.• Serosa covered by fibrin or suppurative coagulative
exudative.• Calculous cholecystitis shows obstructing stone in neck
of gall bladder or cystic duct.• Empyema GB lumen contains pure pus.• Gangrenous cholecystitis GB transformed into necrotic
green-black organ.• Emphysematous cholecystitis clostridia & choliforms.

Acute cholecystitisclinical features
• Acute Calculous cholecystitis– Right upper quardrant or epigastric pain.– Fever,anorexia,tachycardia,sweating,N/V– Leukocytosis ↑ ALP ,↑ S.bilirubin– Presentation can be severe sudden or mild
which may resolve spontaneously without medical intervention
• Acute Acalculous cholecystitis ↑ insidious but ↑ γ perforation.

I-Acute Calculus Cholecystitis • 90% of cases due to gallstones• 50% have bacterial infection • 50% of those with jaundice have coexisting choledocholithiasis• Due to chemical irritation inflammation of obstructed GB.• Mucosal phospholipase hydrolyzes luminal lecithin to toxic
lysolecithin• Protective glycoprotein layer is disrupted exposing mucosal
epithelium to detergent action of bile salts• PG released within the wall of distended GB → mural & mucosal
inflammation.• GB dysmotility→ distention & ↑ intraluminal pressure ↓ blood flow to
mucosa• Frequent in DM with gallstones

Acute calculous cholecystitis; the stone was not photographed.

II-Acute Acalculus Cholecystitis Risk factors
• 10% of cases• Sepsis with hypotension & multisystem organ failure.• Immunosuppression• Major trauma & burn• Diabetes mellitis• Infections eg salmonella typhi.• Systemic vasculitis• Severe atherosclerotic ischemia• May be associated with infection by CMV, cryptosporidia or
microsporidia in AIDS patients• 10-50% mortality• Cocaine related acute cholecystitis

II-Acute Acalculus Cholecystitispathogenesis
• 10% of acute cholecystitis• Due to ischemia, systemic vasculitis ,severe
atherosclerosis.• Cystic artery is end artery with no collateral
circulation• Inflammation & edema of the wall compromising
blood flow• GB stasis• Accumulation of biliary sludge (cholesterol
microcrystal).• Cystic duct obstruction by mucus & viscous bile.

Chronic cholecystitis• Most cholecystectomies are performed for intermittent obstruction of
gallbladder neck / cystic duct by gallstones, causing biliary colic• 95% are associated with cholelithiasis• 75% women, ages 40+• 1/3 E.coli & enterococci• Rokitansky Aschoff sinuses
• Procelain gallbladder - dystrophic calcifications• Xanthogranulomatous – thickened• Hydrops / mucocele
– Distended gallbladder containing clear and watery (hydrops) or mucoid secretions (mucocele), instead of bile
– Adult cases almost always due to impacted stones in ampulla or cystic duct.

Chronic cholecystitis with cholesterol stones. The gallbladder wall is thickened and gray-white, owing to fibrosis and inflammation. The mucosa is effaced. Multiple faceted cholesterol
gallstones are present within the lumen. The exterior of the specimen is black as a result of India ink application.

Complication of cholecystitis
• Bactrial superinfection with cholangitis or sepsis
• GB perforation with local abscess
• GB rupture with peritonitis
• Biliary fistula – intestinal fistula
• Procelain GB ↑ cancer

Extra hepatic Bile ducts
• Choledocholithiasis - stones within bile ducts • Asian ↑ γ primary which are pigmented stones &
associated with BT infections.– Complications
• Obstuctive jaundice• Pancreatitis• Cholangitis• Hepatic abscess• Sec biliary cirrhosis• Acute calculous cholecystitis• Ascending cholangitis

Biliary Atresia
• 1:1200 live births
• Within first 3 months of life
• 20% Fetal form due to aberrant intrauterine development associated with– malrotation of Ab.viscera ,interrupted
IVC ,polysplenia & Cong HD.
• Perinatal form = destruction of normal BT. Sec to Viral infection & autoimmunity.

Biliary AtresiaMorphology
• Present with neonatal cholestasis• Intrahepatic bile ducts inflammation &
destruction ,bile duct proliferation ,PT edema & fibrosis, parenchymal cholestasis
• Cirrhosis develops within 3 to 6 months of birth.
• Type I common ducts• Type II hepatic bile ducts• Type III 90% at or above the porta hepatis

Figure 18-54 Biliary atresia, schematized to show the pattern of biliary tract injury.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 27 February 2006 12:33 PM)
© 2005 Elsevier

Choledochal cyst
• Congenital dilation of CBD• Often > 10 yrs age• Present with biliary colic• 20 % symptomatic in adulthood.• Caroli disease along with cystic dilatation
of intrahepatic BT• Complications
– Stone formation, stenosis, pancreatitis, hepatic biliary obs , carcinoma

Secondary sclerosing cholangitis
• Much more common than primary sclerosing cholangitis
• Causes: biliary obstruction (choledocholithiasis, post-operative, chronic pancreatitis, choledochal cyst, extrahepatic biliary atresia),
• infection (immunodeficiency states), toxins, ischemia, malignancy, other (chronic graft vs. host disease, sarcoidosis, Langerhans cell histiocytosis, systemic mastocytosis)
• Associated with hepatic lobar atrophy, bacterial infection
• Micro: fibrosis, inflammation, ulceration, foreign body granulomas• DD: bile duct carcinoma (no lobular pattern of peribiliary glands, no
concentric fibrosis around peribiliary glands, infiltrating glands, perineural invasion, often marked cytologic atypia)

Primary sclerosing cholangitis
• Chronic cholestatic disorder of unknown origin (possibly autoimmune) involving entire biliary tract from ampulla of Vater to small intrahepatic bile ducts or gallbladder
• Much less common than secondary sclerosing cholangitis• Rule of 70’s: 70% men, 70% have chronic inflammatory bowel disease
(particularly ulcerative colitis which is usually detected first; only 4% with ulcerative colitis have primary sclerosing cholangitis, which is unaffected by colectomy), 70% younger than age 45
• Also associated with chronic pancreatitis (15-25%), Riedel’s thyroiditis, retroperitoneal and mediastinal fibrosis, orbital pseudotumor, Sjogren’s syndrome, angioimmunoblastic lymphadenopathy
• Symptoms: fatigue, pruritis, jaundice• Complications: biliary cirrhosis and liver failure in all cases with median
survival 9-12 years; cholangiocarcinoma (10-43%), colon carcinoma• End stage disease is associated with hyperplasia of glands of extrahepatic
bile ducts, with low incidence of dysplasia and adenocarcinoma,

Carcinoma of extrahepatic bile ducts
• 90-95% of extrahepatic bile duct malignancies are adenocarcinomas (bile duct carcinoma, cholangiocarcinoma)
• Present in 0.5% of autopsies

Tumors of GB
• Benign– Adenoma
• Tubular• Papillary• Tubulopapillary
– Inflammatory Polyp– Adenomyosis,– cholesterol polyp,– granular cell tumor,– hyperplastic/metaplastic polyp,– inflammatory polyp,– villous papilloma

Tumors of GB
• Malignant – gallbladder carcinoma – carcinoma in situ – clear cell carcinoid, – Ewings/PNET – gastrointestinal stromal tumor, – large cell neuroendocrine carcinoma, – malignant fibrous histiocytoma, – metastases to gallbladder, – mucinous tumor– sarcomatoid carcinoma – small cell carcinoma– squamous cell carcinoma

Carcinoma of GB• Common in women 7th decade of life• Gallstone risk factor 0.5% after 20 years• Infiltrating pattern is more common appear as thickening of GB
wall , or perforation & fistula formation to adjacent viscera.• Exophytic pattern grows into the lumen as cauliflower mass.• Fundus & neck of GB commonest site• Adenocarcinomas• Adenosquamous CA • Carcinoid or carcinosarcoma• Papillary tumors have better prognosis• Peritonium, GIT & lung common site of metastasis

Figure 18-55 Gallbladder adenocarcinoma. A, The opened gallbladder contains a large, exophytic tumor that virtually fills the lumen. B, Malignant glandular structures are present within a densely fibrotic gallbladder wall.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 27 February 2006 12:33 PM)
© 2005 Elsevier

Figure 18-55 Gallbladder adenocarcinoma. A, The opened gallbladder contains a large, exophytic tumor that virtually fills the lumen. B, Malignant glandular structures are present within a densely fibrotic gallbladder wall.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 27 February 2006 12:33 PM)
© 2005 Elsevier

TNM staging for Carcinoma of gallbladder and cystic duct
• Primary tumor (T) - carcinoma of gallbladder and cystic duct• TX: Primary tumor cannot be assessed• T0: No evidence of primary tumor• Tis: Carcinoma in situ• T1: Tumor invades lamina propria or muscular layer• T1a: Tumor invades lamina propria• T1b: Tumor invades muscular layer• T2: Tumor invades perimuscular connective tissue; no extension beyond serosa or into liver• T3: Tumor perforates the serosa (visceral peritoneum) or directly invades the liver or one other
adjacent organ or structure, such as the stomach, duodenum, colon, pancreas, omentum or extrahepatic bile ducts
• T4: Tumor invades main portal vein or hepatic artery or invades two or more extrahepatic organs or structures
• Regional lymph nodes (N) - carcinoma of gallbladder and cystic duct• NX: Regional lymph nodes cannot be assessed• N0: No regional lymph node metastasis• N1: Metastasis to nodes along the cystic duct, common bile duct, hepatic artery or portal vein• N2: Metastases to periaortic, pericaval, superior mesenteric artery or celiac artery lymph nodes
• Distant metastasis (M) - carcinoma of gallbladder and cystic duct• M0: No distant metastasis• M1: Distant metastasis








![Ciliated foregut cyst in the triangle of Calot: the first ... · choledochal cyst or gallbladder duplication should also be considered [10]. To our knowledge, this is the first description](https://static.fdocuments.net/doc/165x107/5fa33b0766d4b8106c1097d5/ciliated-foregut-cyst-in-the-triangle-of-calot-the-first-choledochal-cyst-or.jpg)