DISEASE MONITORING Dr Mahiran Mustafa Chairman of CPG Development Committee
22
DISEASE MONITORING Dr Mahiran Mustafa Chairman of CPG Development Committee
-
Upload
summer-kerr -
Category
Documents
-
view
24 -
download
0
description
DISEASE MONITORING Dr Mahiran Mustafa Chairman of CPG Development Committee. CONTENTS. Brief review on different phases in dengue infection Issues at different phases Clinical monitoring for each phase Laboratory monitoring for each phase. INTRODUCTION. - PowerPoint PPT Presentation
Transcript of DISEASE MONITORING Dr Mahiran Mustafa Chairman of CPG Development Committee

DISEASE MONITORING
Dr Mahiran MustafaChairman of CPG
Development Committee

CONTENTS
• Brief review on different phases in dengue infection
• Issues at different phases
• Clinical monitoring for each phase
• Laboratory monitoring for each phase

INTRODUCTION
• Monitoring dengue cases require the understanding that dengue infection is a systemic and dynamic disease.
• Its clinical, haematological and serological profiles changing from day to day and accelerate by the hour during the critical phase, particularly in those with plasma leakage
• Failure in recognising and interpreting the clinical and
laboratory manifestations can lead to delay in appropriate management thus cause intractable shock and death
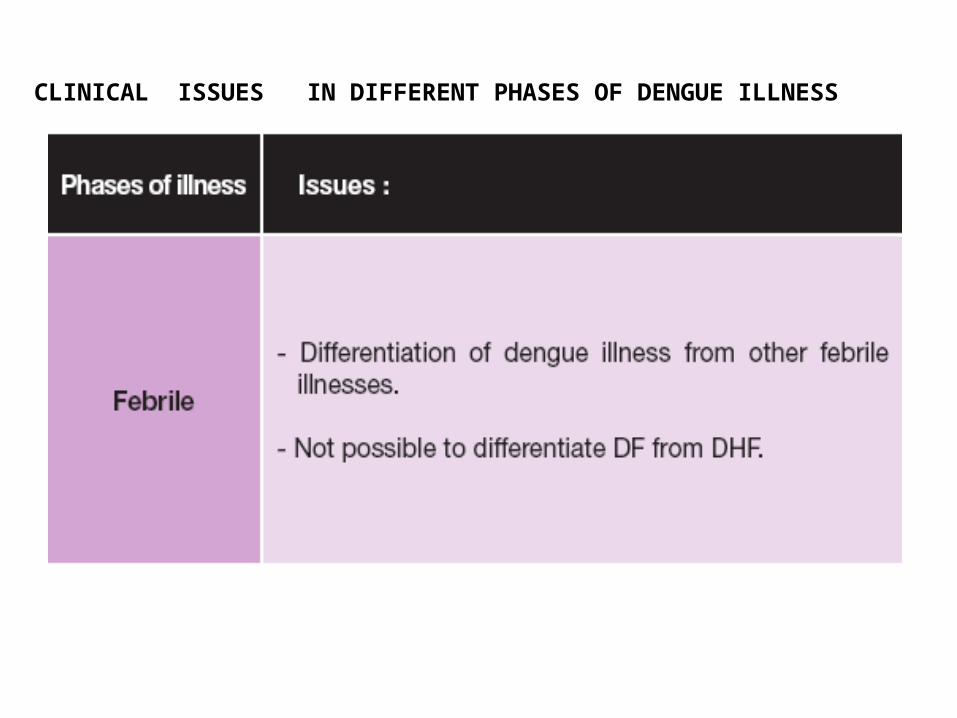
CLINICAL ISSUES IN DIFFERENT PHASES OF DENGUE ILLNESS


OUTPATIENT MONITORING
Symptoms:1. Warning signals 2. Bleeding manifestations3. Inability to tolerate oral
fluids4. Reduced urine output5. Seizure
Signs:1. Dehydration2. Shock 3. Bleeding4. Any organ failure
Laboratory:1. HCT
2. Hb
3. Platelet

DISEASE MONITORING CARD
DENGUE DISEASE PROGRESSION CARDPatient’s name: ________________________________I/C No. : _______________________________Date of onset of fever : __________________________
Date Temp °C BP PR PCV/HCT
WBC Platelet Attending Clinic/ phone no.
Next Appointment

CLINICAL ISSUES IN DIFFERENT PHASES OF DENGUE ILLNESS

• Clinical deterioration often occurs during the critical phase because of marked plasma leakage
Evidence of plasma leakage includes: raised HCT haemodynamic instability fluid accumulation in extravascular space

• Vascular permeability leads to leakage
• Haemoconcentration
• Hypovolaemia leads to reflex tachycardia and vasoconstriction
• Inadequate perfusion of the tissue leads to increased anaerobic glycolysis and resultant lactic acidosis
• Shock that leads to DIC and bleeding
Pathophysiology

WARNING SIGNALS
• Vomiting
• Abdominal pain
• Restlessness or altered mental state
• Mucosal Bleed
• Sudden change of temperature to subnormal
• Raising HCT with rapid drop in platelet


CLINICAL ISSUES IN DIFFERENT PHASES OF DENGUE ILLNESS

SEVERE MANIFESTATIONS
• Acute abdomen
• Hepatitis and hepatic failure
• CNS manifestations
• Carditis or cardiomyopathy

Pathophysiological changes from normal circulation to compensated and decompensated shock
Normal Circulation Compensated shock Decompensated / Hypotensive shock
Clear consciousness Clear consciousness Change of mental state – restless, combative or lethargy
Brisk capillary refill time (<2 sec)
Prolonged capillary refill time (>2 sec)
Mottled skin, very prolonged capillary refill time
Warm and pink extremities Cool extremities Cold, clammy extremities
Good volume peripheral pulses
Weak & thready peripheral pulses
Feeble or absent peripheral pulses
Normal heart rate for age Tachycardia Severe tachycardia with bradycardia in late shock
Normal blood pressure for age Normal systolic pressure with raised diastolic pressure Postural hypotension
Hypotension/ unrecordable BP
Normal pulse pressure for age
Narrowing pulse pressure Narrowed pulse pressure (<20 mmHg)
Normal respiratory rate for age
Tachypnoea Metabolic acidosis/ hyperpnoea



Fluid Guidelines

Fluid Therapy: Non Shock
Recommendation • Encourage adequate oral fluid intake. (Grade C)• IV fluid is indicated in patients who are vomiting
or unable to tolerate oral fluids. (Grade C)• IV fluid is also indicated in patients with
increasing HCT (indicating on-going plasma leakage) despite increased oral intake. (Grade C)
• Crystalloid is the fluid of choice for non shock patients. (Grade C)

Indications for referral to Intensive
• Recurrent or persistent shock
• Requirement of respiratory support (non-invasive and invasive ventilation)
• Significant bleeding
• Encephalopathy or encephalitis

DISCHARGE CRITERIA
• Afebrile for 48 hours• Improved general condition• Improved appetite• Stable haematocrit• Rising platelet count • No dyspnoea or respiratory distress from pleural
effusion or ascites• Resolved bleeding episodes• Resolution/recovery of organ dysfunction

Summary:Principles of disease monitoring
1.Dengue is a systemic and dynamic disease. Therefore disease monitoring is governed by different phases of the disease.
2. The critical phase (plasma leakage) may last for 24-48 hours. Monitoring needs to be intensified and frequent adjustments in the fluid regime may be required.
3. Recognition of onset of reabsorption phase is also important because intravenous fluid regime needs to be progressively reduced/ discontinued