Digital Breast Tomosynthesis
42
6/10/2011 Imaging in Medicine S809 | Eleni Pitri THE OPEN UNIVERS ITY A MODERN BREAST CANCER SCREENING AND DIAGNOSIS TOOL: DIGITAL BREAST TOMOSYNTHESIS
Transcript of Digital Breast Tomosynthesis

|
The Open University
A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
Table of Contents
1. Introduction 3
1.1 Scope and Topic Area 3
1.2 Project Aim and Objectives 3
1.2 Structure of the Report 4
2. Literature Review 5
2.1 Progress of Breast screening and diagnosis 5
2.2 Conventional X-ray Mammography 6 2.2.1 Conventional X-ray Mammography Principles 6
2.2.2 Disadvantages of Conventional Mammography 7
2.3 Digital Breast Tomosynthesis (DBT) 8 2.3.1 The Development of Tomosynthesis92.3.2 Basic Technologic Principles of DBT 10 2.3.3 DBT Technical Considerations12 2.3.4 Detector Requirements 14 2.3.5 Radiation Dose 16
3. DBT Clinical Trials – Comparison with Conventional Mammography 16
3.1 The Potential Advantages of DBT in clinical Practice 16
3.2 DBT clinical Trials 17
4. Discussion 23
5. Conclusion 25
References 26
1. Introduction:
Page 2 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
1.1 Scope and Topic Area
Breast cancer is the most frequent type of cancer and the second leading cancer type for
estimated deaths among the women in U.S.A.1. It is proved that screening and early detection of
breast cancer may contribute to the successful treatment of the disease. At the moment, X-ray
mammography, Analog or Full Field Digital Mammography (FFDM) are used in routine clinical
practice for screening and have contributed to the reduction of breast cancer mortality.
Since the implementation of the flat-panel digital detectors, a new valuable tool is available for
screening and diagnosing breast cancer, that is, Digital Breast Tomosynthesis (DBT). Despite the
other competing technologies such as Ultrasonography, contrast enhanced MRI and Breast CT,
Digital Breast Tomosynthesis is more likely to replace conventional mammography as it may be
considered as an improvement of the current FFDM.
1.2 Project Aim and Objectives
The aim of this project is to understand DBT technology and critically analyze the advantages
and limitations of the technique. In particular the effort will be focused on comparing
conventional X-ray Mammography with the literature results of DBT clinical case studies.
The project objectives can be summed up as follows:
Review of the progress in breast screening and diagnosis
Familiarization with Tomosynthesis imaging technique
Review of the existing literature on DBT
Page 3 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
Analysis of the results of clinical case studies
Comparison of DBT with conventional X-ray Mammography
Interpretation of the results obtained
1.3 Structure of the report
Chapter 2: Literature Review
This chapter presents the major aspects of theoretical background related to X-ray
Mammography and Breast Tomosynthesis
Chapter 3: DBT Clinical Trials – A comparison with Conventional Mammography
At this point the clinical case studies reported in literature are analyzed and compared.
Chapter 4: Discussion
The results obtained by the literature review are summarized and issues that arise from the
potential use of DBT into clinical practice are discussed.
Chapter 5: Conclusions
2 Literature Review
Page 4 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
2.1 Progress of Breast Screening and Diagnosis
Ever since early attempts to use X-rays took place, for the diagnosis of breast cancer, a great
progress has been made in the area. In 1913, the first mammograms were taken by Albert
Salomon at mastectomies and few years later Mammography was used in-vivo2. In 2000 the first
FFDM system gained the first approval by the U.S Food and Drug Administration (FDA) and,
since then, Analog Mammography has been replacing. In the last decade, a new X-ray tool for
breast screening and diagnosis has been developed, that of DBT. In addition to X-ray
investigating techniques, other modalities such as MRI and Ultrasound have been added to the
breast cancer diagnosis methods. Nowadays, apart from the techniques showing anatomical
changes, investigating tools based on functional changes have been introduced.
Figure 1: A schematic diagram showing the progress of breast screening and diagnosis. Where CR = Computed Radiography, MRI = Magnetic Resonance Imaging, CE-DSM = Dual-Energy Contrast-enhanced Digital Subtraction Mammography and CE-DBT = Dual-Energy Contrast-enhanced Digital Breast Tomosynthesis
2.2 Conventional X-ray Mammography
Page 5 of 28
Analog Mammography
CR- Mammmography
FFDM
Anatomic Changes
DBT Ultrasound Elastography
Physio-pathological Changes
Contrast enhanced MRI
CE-DSM
CE-DBT
Cellular Metabolic Changes

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
2.2.1 Conventional X-ray Mammography Principles:
X-ray mammography is proved to be an efficient technique for screening and diagnosing breast
cancer at an early stage. Currently both Analog and FFDM Mammography systems are used in
clinical practice. However, in the last decade most of the analog systems with screen-film
cassettes have been replaced.
Image creation in conventional mammography is based on X-ray attenuation. The mammograms
must image the contrast between similar soft tissues (e.g. fat, blood vessel and soft tissues with
different density), thus, low kV is required to maximize photoelectric effect and make tissues
differences distinguishable.
Figure 2: In conventional Mammography the X-ray tube, the compressed breast and the detector are stationary, while one image is obtained from one projection3.
During the scan, the breast is compressed between the compression paddle and the stationary
breast support. The compression evens out the breast thickness and achieves better visualization
Page 6 of 28
Detector
BreastCompression paddle
X-rays

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
of tissues and abnormalities, less radiation dose to the patient and reduction of scattering.
Furthermore, compression is used to prevent patient motion that causes image blurring. The
views most frequently used in conventional screening mammography are craniocaudal (CC) and
mediolateral oblique (MLO), whereas in diagnostic cases other views are also used4.
2.2.2 Disadvantages of Conventional Mammography:
Although conventional Mammography is an efficient modality which provides reasonably high
sensitivity, high resolution and low patient dose, a disadvantage may be traced in terms of
receiving a 2D imaging of a 3D object. The attenuated beam which arrives on the flat-panel
detector (or the screen film cassette in case of analog system) is proportional to the total
attenuation of all the structures between the X-ray tube and the detector (Figure 3). This causes
an overlap between structures leading to potential loss of information, sensitivity and specificity.
This limitation of conventional Mammography complicates the interpretation of mammograms;
it further deteriorates the detection of breast cancer and renders the localization of abnormalities
difficult. The consequence is that, in cases of questionable findings, even where findings prove
benign, further examinations are needed in order to investigate them and this may cause
additional anxiety to patients let alone additional costs.
Page 7 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
Figure 3: In conventional mammography overlapping structures may lead in loss of information (hidden objects of interest), this effect is eliminated in the 3D Breast Tomosynthesis. (Image captured from Smith et al3)
2.3 Digital Breast Tomosynthesis
Digital Breast Tomosynthesis (DBT) is a new tool which is expected to address these key
limitations of mammography and has the potential efficacy to replace conventional
mammography. DBT is similar to X-ray mammography. It is also based on X-ray attenuation,
but, instead of 2D images, it reconstructs a number of planar projections providing 3D
information. The DBT device is, in most cases, based on the existing digital mammography
system; patient positioning during image acquisition is very similar to conventional digital
mammography, but the required image reconstruction differs.
DBT is a type of limited angle CT with low radiation dose to the patient, similar to that of
mammography. Comparably to 2D mammograms, the reconstructed breast images produced by
DBT reduce potential false diagnosis due to structure overlapping and increases cancer
localization and delineation of borders.
Page 8 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
2.3.1 The development of Tomosynthesis:
Tomosynthesis is not a newly invented technique. The conception of the technique goes back to
1930s when Ziedes des Plantes introduced the theory of limited angle tomography only its
implementation was not possible5. Digital detectors made the implementation of Tomosynthesis
feasible and in 1972 Grant made up the term “Tomosynthesis”. At this early stage the limitations
of digital detectors obstruct trials from taking place for the clinical use of the technique. From
late 1980s to late 1990s Tomosynthesis was almost abandoned due to the development of spiral
CT which seemed to dominate over all 3D X-ray imaging.
Until flat-panel detectors were introduced in late 1990s, clinical applications were not feasible.
Full-filled flat panel detectors are characterized by low noise, high frame rate and high detective
quantum efficiency (DQE) which are required for a reasonable acquisition time of several (low
dose) projections used in Tomosynthesis systems.
Over the last years Tomosynthesis clinical applications have increased and improved. The
applications which gather most interest are Breast Tomosynthesis and pulmonary nodule
imaging. The interest in Breast Tomosynthesis has been further growing after the U.S. FDA
approved the first Breast Tomosynthesis System in February 2011.
Page 9 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
2.3.2 Basic technologic principles of Digital Breast Tomosynthesis
As mentioned before, the DBT device in almost all commercial systems is combined with the
existing digital mammography system. Similarly to conventional mammography the breast is
compressed between the compression paddle and the stationary breast support which contains the
digital detector. The integrated systems can take a conventional mammogram and a
Tomosynthesis set of slices at the same compression.
Figure 4: Schematic representation of DBT operation principles6.
There are more than one motion geometries of the tube and the detector for Tomosynthesis
image acquisition5. In current DBT systems, the partial isocentric motion is used (Shown in
Figure 5). The X-ray tube moves in an arc about the compressed breast during the exposures
while the detector is fixed, and a number of projections are obtained. This type of geometry is
preferable because it may more easily be integrated into the current Digital Mammography
Systems.
Page 10 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
Figure 5: Schematic representation of partial isocentric motion (captured from Dobbins et al5)
During image acquisition there are two methods of moving the tube. The first one is the step-
and-shoot method that the tube completely stops and ‘shoots’ at each position. The second is the
continuous exposure method where the tube moves continuously and the exposures are low dose
short pulses. Both methods are not without advantages and disadvantages; yet currently the
second method is preferred due to the faster scan times it provides.
The projection data obtained by the scan are reconstructed into a series of high resolution images
aligned in parallel to the breast platform, perpendicular to the X-ray beam. Because of the
limited scan angle there is less resolution in the axis of X-ray beam and higher resolution in the
perpendicular plane. The number of images is proportional to the breast thickness and the
distance between them. The most frequent spacing is 1mm. The set of images are transferred and
read at a common workstation where the radiologist can interpret the reconstructed images.
Page 11 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
2.3.3 DBT Technical Considerations
As mentioned above DBT reconstructs images which provide 3D information but, as a result of
the limited scan angle, the depth or out-of-plane resolution is low. This limitation of DBT
produces out-of-plane artifacts such as the streak artifact of Figure 67. This type of artifact is
prominent in visualization of calcifications with DBT. As shown in Figure 6, it does not only
degrade the image quality of the focus plane but reduces the visualization in neighboring slices
as well. This artifact can be reduced by increasing the scan angle and therefore increasing the
depth resolution.
Figure 6: A calcification is seen in four different slices due to an out-of-plane artifact and therefore
reduces the visualization in these slices: (a) in focus plane; showing the in-plane black artifact below and
above the high contrast calcification, (b) 6 mm from the focus plane, (c) 10 mm from the focus plane and
(d) 17 mm from the focus plane. The tube motion is parallel to the streak artifact from top to bottom.
(Image captured from Tingberg et al7)
Page 12 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
The optimal scan angle of the tube must be estimated according to a number of factors; the
appropriate depth resolution is only one of them. Another factor to be taken into consideration is
the scan time. Wider scan angle demands longer scan time, which increases the probability of
motion artifacts. Given that the detector is fixed, the field of view is also influenced by wide scan
angles and may lead to missing tissues. Furthermore, wide scan angles produce thicker effective
breast that induces noise and scattering. Other issues negatively affected by wide angle range are
the in-plane and detector resolution.
The number of projection is another technical issue for DBT. The optimal number of projection
is also depended on several parameters such as:
The scan angle: serves to avoid reconstruction artifacts. A number of projections per
degree-scan-angle is required –referred as projection sampling.
Scan time must be kept as short as possible thus can become a limiting factor for the
number of projections considering the limited frame rate of detectors.
Large numbers of projections may induce electronic noise.
In current systems the number of projections varies from 11 to 49 and the scan angle of the tube
from 150 to 5008. Each manufacturer has used different methods and reconstruction algorithms to
develop a DBT system, thus different optimal scan angle and number of projections are received.
Table 1 gives the scan angle of the DBT systems provided by four manufacturers; each of them
uses a different method.
Page 13 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
Figure 7: DBT systems by four different manufacturers. (A) Siemens – Mammomat Inspiration9 (B) GE Breast Tomosynthesis10 (C) Hologic- Selenia Dimensions11 (D) Giotto - IMS12
Table 1: Differences among commercially available DBT systems
Manufacturer Name Total scan angle
Projections Detector
Siemens MAMMOMAT Inspiration
500 25 a-Se
GE GE Breast Tomosynthesis
250 9 CsI
Hologic* Selenia Dimensions 150 15 a-Se
Giotto IMS 400
(non uniform distribution)
11 a-Se
*Hologic: Selenia Dimensions is the first commercially available system that gained the FDA approval in February 2011.
Page 14 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
2.3.4 Detector Requirements:
One of the most essential parts of the DBT system is the full-field flat-paned detector. Due to the
low dose of the exposures, high detective quantum efficiency (DQE) and low noise are required.
Because of the numerous projections high frame rate is also essential. The detectors used in most
of the current DBT systems are selenium-based but cesium iodide (CsI) crystals based on
amorphous silicon are also suitable. Selenium has the highest DQE at the low energies of
mammography, more than 95% X-ray absorption. This allows imaging at radiation doses as low
as those used in DBT.
2.3.5 Radiation Dose
The radiation dose to the patient is a critical consideration for Mammography system
manufacturers and regulators. Radiation dose to the patient and image quality are related and
must be used in an optimum way.
The current DBT systems are within the Mammography Quality Standards Act (MQSA)13 limits
which are set at 3 mGy per exposure. The limits concern the Mean Glandular Dose (MGD) at a
phantom of a standard breast for a single CC view. The MGD of a single view DBT
examination, as they are calculated in early clinical studies, is equal or slightly higher than that
of a single view FFDM. As Teerstra et al14 and Good et al15 have reported in their studies, the
MGD of DBT system is almost equal to that of FFDM; the first has reported 1.74 mGy and the
latter 2 mGy.
Page 15 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
3 DBT Clinical Trials – Comparison with Conventional Mammography
3.1 The potential advantages of DBT in clinical practice
DBT is a new tool developed to contribute to the detection and diagnosis of breast lesions,
especially in women with dense breast tissue. The set of reconstructed images from different
angle projections allows visualization of thin breast sections and provides more detailed
information for breast structures (normal tissues and abnormalities). Theoretically, DBT has
superior sensitivity compared to 2D X-ray Mammography. DBT is expected to provide improved
detection of lesions, even to allow detection of small cancers not visualized by conventional
mammography. DBT has the capability to provide more information on the margins of a mass
and characterize the abnormalities more accurately. Thus, the specificity of the technique is
increased while the false-positive recalls are reduced.
The numerous potential benefits of DBT clinical use must be proved and evaluated in large
randomized clinical trials. The sensitivity and specificity of the technique, in the different types
of breast abnormalities, should also be evaluated during clinical trials.
Page 16 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
3.2 DBT clinical trials
Recent DBT clinical trials aim to give an early evaluation of the DBT technique. The findings
from these studies have generally shown a superiority of DBT in the detection and border
determination of masses. In the detection of calcification there are several opinions and the
physicians’ preferred technique is still questionable. The main problem with calcifications
detection is that calcifications are dispersed in space; therefore 1mm thick DBT slice may
include only a small number of calcifications, making the calcification cluster less perceptible.
These early studies have concluded that DBT cannot provide 100% sensitivity and specificity.
However, most of them have agreed that it can provide improved sensitivity and specificity.
Finally, all of the studies have shown that DBT demands considerably longer reading times by
the physician. This major limitation of DBT over conventional mammography is expected to be
balanced. First because of the reduction of diagnostic examinations resulting out of an
improvement in recall rates. Second because of the familiarization of physicians with the new
technique that is expected to reduce the interpretation times.
One of the first clinical studies was that of Poplack et al16; the aim of whose project was the
comparison between diagnostic DBT and film-screen mammography in a group of 98 women
recalled to be examined after a digital screening mammogram. The results have shown that the
DBT image quality was equal (51 subjects) or superior (37 subjects) to screen-film
mammography in 89% of the cases. A percentage of 11% was assessed to be inferior to screen-
film mammography, calcifications were reported at 73% of these cases. Masses showed better
image quality on DBT in a considerable higher amount of cases (68%) or equal quality in 26% of
Page 17 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
them. Among the conclusions of the project was that DBT with FFDM in screening has the
potential to reduce the recall rate and the reduction was estimated to 40%.
Figure 8: Left breast of 84-year old woman16. (A)Focal compression view: irregular mass is shown by arrows (B)Single slice of DBT: Irregular shaped mass with its margins is shown by arrows and central fat by circle (C)Arrows show infiltrating lobular carcinoma with central fat deposition
Another early clinical study was that of Good et al15; 9 physicians evaluated the image quality of
30 cases for three different modes: FFDM, 11 projections acquired for DBT before the
reconstruction and the reconstructed DBT slices. The results are similar to those of Poplack et al;
they have shown that the reconstructed DBT images were significantly better in 23% of cases,
somewhat better in 44% of cases, comparable in 31% of cases and inferior in only 1.9% of cases.
Good et al also estimated the readout times of DBT (2.7 min per examination) and FFDM (1.6
min per examination) and verified that the read out times were longer in the case of DBT
examinations.
Page 18 of 28
Analog Mammography DBT Photomicrograph

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
Gur et al17, using 8 experienced radiologists and 125 cases (35 with verified findings of cancer
and 90 with no findings) assessed the image quality of four different display conditions: FFDM
alone, 11 low dose projections, reconstructed DBT images and combined FFDM with DBT. The
investigators found that the sensitivity of DBT alone was similar to that of the combination of
DBT with FFDM (93%) and the sensitivity of FFDM alone was non-significantly reduced
(88%). The specificity of combined DBT with FFDM was the greatest (0.72) compared to DBT
alone (0.64) and FFDM alone (0.60). Gur et al have concluded that the combination of DBT with
FFDM would have led to 30% reduction of recall rate for cancer free examinations compared to
FFDM alone; slightly lower than that of Poplack et al. Using of DBT alone would have
diminished the recall rate by 10%. The time to view and rate images was also evaluated for each
mode; as it is seen in Table 2 the longest mean time was for the combined mode. The results for
FFDM and DBT are slightly lower than those estimated by Good et al, though the difference
between the two modes is still almost the same.
Table 2: Mean Time for all readers and examinations to view and rate images from each imaging display mode. Data taken by Gur et al17.
Mode Mean Time per Examination (min)
Standard Deviation
FFDM alone 1.22 1.15
Frame 1.38 0.99
DBT 2.05 1.46
Combined FFDM and DBT
2.39 1.65
Page 19 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
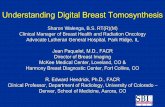
Rafferty et al18 were the first to produce a large multi-centre trial to compare and analyze the
results of FFDM alone and FFDM with combinations of CC and MLO views of DBT. They used
the Receiver Operating Curve (ROC) method to analyze data from 310 subjects and 15 readers.
As it is shown in Figure 9 there is significant improvement in ROC performance in both fatty
and dense breasts when the combination of FFDM with DBT views was used. It is also notable
that the ROC performance of combined FFDM with DBT in dense breasts is superior to FFDM
alone, not only in fatty dense breasts but also in fatty breasts. These results support the opinion
that DBT would improve the detection of breast lesions in women with dense breast tissue.
However, the best performance is still for fatty breasts. The investigators have shown a reduction
in recall rates for cancer free cases of 43% in fatty breasts and 34% in dense breasts when using
combined FFDM with DBT compared to FFDM alone. Estimations close to those stated by Gur
et al and Poplack et al.
Figure 9: ROC curves of FFDM alone and combination of FFDM and DBT for fatty and dense breasts. It is shown that the combination of the two modalities is better than FFDM alone both for dense and fatty breasts.
Page 20 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
Teerstra et al14 compared the diagnostic images from FFDM and DBT of 513 cases. As opposed,
to the majority of clinical trials, this study has concluded that DBT is as good as FFDM and is
not superior in detection of breast cancer. Estimations for sensitivity showed that the two modes
had almost the same sensitivity (92.9%). The specificity of FFDM (86.1%) was slightly better
than DBT (84.4%). It is also important to note that this study found DBT to be as good as FFDM
in detection of malignant calcification (all clusters were detected by using both techniques)
which is also to be contrasted with the results of the majority of studies.
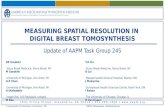
Helvie et al, as it is presented in a recent paper6, assessed the DBT capabilities in delineation of
masses margins (all cases were scheduled for biopsy.) The comparison of DBT with
conventional Mammography showed that DBT was better in determination of the perimeter of
masses: 77% of the perimeter of a mass could be visualized by DBT and only 53% by FFDM.
Figure 10: Invasive ductal cancer 6 : The cancer of this case is only apparent in the CC view of conventional mammography. On the other hand DBT (1mm thick slice) provides information not only for the cancer but also for the margins at both views.
Page 21 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
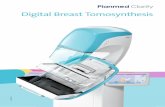
Helvie et al assessed the Maximum Intensity Projection (MIP) images of DBT in the detection of
microcalcifications. MIP images are 1 or 2 cm thick slices specially reconstructed from DBT
examinations in order to overcome the problem of calcifications dispersion in several DBT slices
(Figure 11). The investigators have shown that calcification clusters were visible by DBT MIP
images in 100% of cases, based on conventional mammography results. It is worth noting that
the visualization of calcification was slightly less when 1 mm thick DBT slices were examined
(96% for benign and 97% for malignant cases).
Figure 11: Ductal carcinoma in situ is shown by arrows as a microcalcification cluster6. (A) CC view of FFDM (B) 11 mm thick MIP image of DBT. The MIP image of a DBT examination shows the calcifications as good as FFDM.
Page 22 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
4 Discussion
The positive early results from clinical trials justify the positive reactions for DBT by the
majority of radiologists. However, prior to further induction of DBT in clinical practice the
considerations and questions arising from DBT use must be investigated. Not only the
superiority but also the cost-effectiveness and the utility of the technique must be proved during
large randomized clinical trials.
What seems to be important is to first determine the best use of DBT into routine clinical
practice. It is expected to be very useful at both diagnostic and screening level, but it is still
questionable whether it is feasible to be used in both cases. The early studies have shown that
due to its improved visualization of overlying structures and improved delineation of masses
margins, DBT has an important role to play in diagnostic applications. Also DBT has the
capability to more accurately determine the type of abnormalities. The use of DBT in screening
is more complicated. DBT has a major disadvantage compared to conventional mammography; it
demands significantly longer interpretation times by the physician. This disadvantage must be
overcome by the benefits of DBT in screening. In order to conclude about the utility of DBT in
screening; it is important to accurately evaluate the recall rates – biopsy rates and the specificity
of DBT in large-scale clinical trials. The high specificity of DBT may be proved enough to
improve current diagnostic procedures and patients may go directly for biopsy after a DBT
screening.
Another important consideration arising from DBT clinical use is the number of views which
need to be acquired. So far it has not been clarified whether DBT should be performed in both
CC and MLO view or in only one of the two. It is not even clarified whether it should be used
Page 23 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
alone or as an adjunctive to FFDM. The majority of studies have shown a weakness of DBT in
the detection of calcifications in favor of the opinion that a static view should also be taken
(FFDM view or an analogous MIP image). The results from the large multi-centre study of
Rafferty et al, were also in consonance with this opinion. They have shown that one DBT view
adjunctive to FFDM can provide higher sensitivity and specificity than FFDM alone.
The efficient use of DBT will require substantial training, by the physician. The non-familiarity
of physicians with DBT images induces the risk of an initial increase in recall rates due to
normal tissues that look different and suspicious. In addition physicians familiarity with DBT is
essential not only for interpreting the DBT examinations but also for minimizing the
interpretation times.
Page 24 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
Conclusion
DBT is an outstanding new development for screening and diagnosing of breast cancer. The
initial results from early clinical studies are in favor of the new technique, especially in the case
of masses. The evaluation of calcifications is still questionable and needs further investigation.
So far it has not been clarified whether DBT should be used alone or as an adjunctive to FFDM
However, the early results reveal that DBT alone or as an adjunctive will significantly contribute
in the improvement of current breast cancer screening and early diagnosis by decreasing recall
rates and false positive biopsies. It is essential to confirm these early results with large
randomized clinical trials.
An important advantage of DBT, over other competing technologies, is that its basic technology
is X-ray mammography. It can be integrated in the existing installed systems; it uses the existing
familiar digital radiologic equipment and seems to be easily accepted by patients and health care
professionals.
All these factors create a positive prospective that DBT may overcome the barriers, which it
currently faces, and finally will become a cost-effective, low dose imaging modality in the field
of mammography.
Page 25 of 28

A modern breast cancer screening and diagnosis tool: DIGITAL BREAST TOMOSYNTHESIS
Imaging in Medicine S809
Eleni Pitri
References
Page 26 of 28

1 American Cancer Society (2011) Cancer Facts and Figures 2011 [online],
http://www.cancer.org/Research/CancerFactsFigures/CancerFactsFigures/cancer-facts-figures-2011,
(assessed July 2011).
2 Gold, R.H., Basset, L.W. and Widoff, B.E. (1990) ‘Highlights from the History of Mammography’,
Radiographics, vol. 10, p.p. 1111-1131.
3 Smith, A. (2011) Design Considerations in Optimizing a Breast Tomosynthesis System [online],
http://www.hologic.com/data/Design_Considerations_Optimizing_Breast_Tomo.pdf (assessed July 2011).
4 Radiology Info (2011) Mammography [online], http://www.radiologyinfo.org/en/info.cfm?pg=mammo
(assessed Augast 2011)
5 Dobbins III, J.T. and Godfrey, D.J. (2003) ‘Digital X-ray Tomosynthesis: Current state of the art and
clinical potential’, Physics in Medicine and Biology, vol. 48, pp. R65-R106.
6 Helvie, M.A. (2010) ‘Digital Mammography Imaging: Breast Tomosynthesis and advanced application’,
Radiologic Clinics of North America, vol. 48, no. 5, pp. 917-929.
7 Tingberg, A. (2010) ‘X-Ray Tomosynthesis: A review of its use for breast and chest imaging’, Radiation
Protection Dosimetry, vol. 139, no. 1-3, p.p. 100-107.
8 Dobbins III, J.T. (2009) ‘Tomosynthesis imaging: At a translational crossroads’ Medical Physics, vol. 36,
no. 6, pp/ 1956-1967.
9 Siemens (2009) 3D Tomosynthesis with MAMMOMAT Inspiration [online],
http://www.medical.siemens.com/siemens/en_GLOBAL/gg_sps_FBAs/files/Mammo_Brochures/
WS_MAMMOMAT_Inspiration_Tomo_DRUCK_engl_0907.pdf (Assessed July 2011)
10 GE Healthcare (2011) GE Breast Tomosynthesis
11Smith, A. (2011) Fundamentals of Breast Tomosynthesis System [online],
http://www.hologic.com/data/WP-00007_Tomo_08-08.pdf (assessed July 2011)
12 Giotto(2010) The new Dimensions in Digital Mammography [online],
http://www.imsitaly.com/downloads/GiottoBrochure.pdf (Assessed July 2011)

13 U.S. Food and Drug Administration (FDA) (2009) Mammography Quality Standards Act Regulations
[online], http://www.fda.gov/Radiation-EmittingProducts/MammographyQualityStandardsActandProgram/
Regulations/ucm110906.htm#s90012 (assessed Augast 2011).
14 Teerstra, H. J., Loo, C. E., van den Bosh, M. A. A. J, van Tinteren, H., Rutgers, E.J.T., Muller, S.H. and
Gilhuijs K.G.A. (2010) ‘Breast Tomosynthesis in clinical practice: initial results’, European Radiology, vol.
20, pp. 16-24.
15 Good, W. F., Abrams, G. S., Catullo, V. J., Chough, D. M., Canott, M. A., Hakim, C. M. and Gur, D
(2008) ‘Digital breast tomosynthesis: A pilot observer Study’, American Journal of Roentgenology, vol. 190,
p.p. 865–869.
16 Poplack, S.P., Tosteson, T.D., Kogel, C.A. and Nagy, H.M. (2007) ‘Digital Breast Tomosynthesis: Initial
Experience in 98 Women with Abnormal Digital Screening Mammography’, American Journal of
Roentgenology, vol. 189, p.p. 616-623.
17 Gur, D., Abrams, G. S., Chough, D.M., Gannot, M.A., Hakim, C.M., Rerrin, R.L., Rathfon, G.Y., Sumkin,
J.H., Zuley, M.L. and Bandos, A.I. (2009) ‘Digital breast Tomosynthesis: observer performance study’,
American Journal of Roentgenology, vol. 193, p.p. 586-591.
18 Rafferty, E.A., Smith, A.P. and Niklason, L.T. [Radiologic Society of North America 95th Scientific
Assembly and Annual Meeting] (2009) Assessing radiologist performance in dense versus fatty breasts
using combined full-field digital mammography and breast Tomosynthesis compared to full-field digital
mammography alone [online], http://rsna2009.rsna.org/search/event_display.cfm?em_id=8016152 (Assessed
Augast 2011).