Digital Breast tomosynthesis - gov.uk · 2015-07-02 · Digital breast tomosynthesis (DBT) is a...
40
DIGITAL BREAST TOMOSYNTHESIS NHSBSP Publication No 69 September 2010
Transcript of Digital Breast tomosynthesis - gov.uk · 2015-07-02 · Digital breast tomosynthesis (DBT) is a...

Digital Breast tomosynthesis
NHSBSP Publication No 69 September 2010

Authors
Members of the Digital Breast Tomosynthesis Working Party
Professor Fiona J gilbert Aberdeen Biomedical Imaging Centre, University of Aberdeen (Chair)
Professor Kenneth C young National Coordinating Centre for the Physics of Mammography, Guildford
Dr susan m astley Imaging Sciences, University of Manchester
ms Patsy Whelehan Centre for Oncology and Molecular Medicine, University of Dundee
Dr maureen g C gillan Aberdeen Biomedical Imaging Centre, University of Aberdeen
Published byNHS Cancer Screening Programmes Fulwood House Old Fulwood Road Sheffield S10 3TH
Tel: 0114 271 1060 Fax: 0114 271 1089
Email: [email protected] Website: www.cancerscreening.nhs.uk
© NHS Cancer Screening Programmes 2010
The contents of this document may be copied for use by staff working in the public sector but may not be copied for any other purpose without prior permission from NHS Cancer Screening Programmes.
The document is available in PDF format on the NHS Cancer Screening Programmes website.
ISBN 978-1-84463-071-4
Typeset by Prepress Projects Ltd, Perth (www.prepress-projects.co.uk) Printed by Bell & Bain, Glasgow

NHSBSP September 2010
Digital Breast Tomosynthesis | iii
CONTENTS
ACKNOWLEDGEMENTS iv
1. INTRODUCTION 1
1.1 Overview of tomosynthesis 11.2 Digital Breast Tomosynthesis Working Party 21.3 Methodology 3
2. TECHNICAL ASPECTS OF TOMOSYNTHESIS 4
2.1 General principles 42.2 Technical features of current digital breast tomosynthesis systems 42.3 Reconstruction of DBT images 72.4 Tomosynthesis image display 82.5 Workstation requirements for DBT 8
3. ISSUES FOR THE NHS BREAST SCREENING PROGRAMME 9
3.1 Context 93.2 Equipment 93.3 PACS 93.4 Resource and practical issues 103.5 Technical and clinical evaluation of DBT equipment for use in the NHSBSP 113.6 Technical quality control and radiation dose monitoring 113.7 Training 113.8 Research required 123.9 Summary of recommendations 12
APPENDIX 1: Digital breast tomosynthesis system questionnaire 13
APPENDIX 2: Responses to questionnaire: comparison of DBT systems 16
APPENDIX 3: Bibliography of publications from manufacturers of digital breast tomosynthesis systems 29
APPENDIX 4: Manufacturers’ contact details 33
REFERENCES 34

NHSBSP September 2010
iv | Digital Breast Tomosynthesis
ACKNOWLEDGEMENTSThe authors would like to acknowledge the support of Sarah Sellars, Assistant Director, NHS Breast Screening Programme, and of the following companies who sent and presented information on the development of their tomosynthesis systems: Dexela, GE, Hologic, Sectra, Siemens and XCounter.
Figures 1 and 2 are based on data first published in 2003 in Digital x-ray tomosynthesis: current state of the art and clinical potential by James T Dobbins III and Devon J Godfrey.1 They appear with the kind permission of Professor Dobbins and IOP Publishing Limited.

NHSBSP September 2010
Digital Breast Tomosynthesis | 1
1. INTRODUCTION
1.1 Overview of tomosynthesis
In standard two dimensional (2D) film or full field digital mammography (FFDM), overlapping dense fibroglandular tissue within the breast can reduce the visibility of malignant abnormalities or simulate the appearance of an abnormality. This can lead to unnecessary recalls, biopsies and psychological stress for the women concerned. In addition mammography is known to be less sensitive in women with dense breasts, who are at higher risk of developing breast cancer.2 This is of particular concern for the NHS as it extends the screening programme to women aged 47–49, as these pre- or perimenopausal women have a higher proportion of dense breast tissue.3,4 It is also potentially problematic for women aged 40–49 whose family history places them at moderate or high risk of the disease and for whom annual mammography is therefore recommended.5
Digital breast tomosynthesis (DBT) is a newly developed form of three dimensional (3D) imaging with the potential to improve the accuracy of mammography by reducing tissue overlap. This overlap, which is sometimes known as anatomical noise, degrades image quality in standard 2D projection imaging. The fundamental principles of tomographic imaging were established in the 1930s. However it was several decades before any practical clinical applications were reported, with the development of flat panel digital display detectors, rapid computer processing and advances in reconstruction and post-processing algorithms.1 In DBT, multiple projection images of the breast are acquired from different angulations of the x-ray tube.6 The images are then processed using algebraic reconstruction algorithms to produce tomographic sections through the breast. These sections can be viewed on a soft copy workstation, either as slices or sequentially in a dynamic video mode. By minimising the superimposition of overlying breast tissue, DBT has the potential to differentiate malignant features more definitively from non-malignant ones.
The superiority of DBT to standard 2D projection mammography was first demonstrated using phantoms and mastectomy specimens.7–10 Later studies with prototype systems indicate that the image quality of DBT is highly dependent on system geometry and the selection of optimal image acquisition, reconstruction and display parameters.6,11–13
1.1.1 Lesion visibility
It has been noted that masses and architectural distortions are more clearly visible with DBT than with film–screen mammography and that lesions can be more accurately classified.14–20 One study reported equal or better visualisation of microcalcifications using DBT,21 although other studies suggest that resolution is less sharp than with conventional mammography.17,18,22 This lower resolution may result partly from system geometry, the reconstruction of images after processing22,23 and the need to combine image slices into thicker slabs for optimal visualisation of microcalcification clusters. It has been suggested that a standard-view digital mammogram should be acquired along with two-view DBT for optimal assessment of microcalcifications.6,24,25 The development of computer aided detection (CAD) algorithms for DBT may also facilitate lesion detection and image interpretation.6,26–28

NHSBSP September 2010
2 | Digital Breast Tomosynthesis
1.1.2 Cancer detection and recall rate
A blinded reader study of 60 mixed cases reported no significant change in cancer detection rate when using DBT but noted that the false positive recall rate was 83% lower than when using FFDM.29 A blinded assessment of 100 cases reported a 40% improvement in sensitivity and 20% reduction in recall rate with DBT when compared with mammography.30 A 43% reduction in recall rate (from 7.5% to 4.3%) was observed by an American screening population study involving 1957 women.31 A retrospective multireader performance study with 125 cases, including 35 cancer cases, reported a 30% reduction in false positive recall rate using a combination of DBT and FFDM when compared with FFDM alone.32 Using DBT alone or in combination with FFDM produced no significant improvement in sensitivity, however.32 Teertstra et al33 reached a similar conclusion regarding sensitivity in their blinded assessment of images from 513 women with abnormal screening mammography or clinical symptoms.
1.1.3 Number of DBT views
It was initially suggested that DBT image acquisition be restricted to the mediolateral oblique (MLO) view.34 However a later study by the same research group reported that 65% of lesions were judged equally visible on both MLO and craniocaudal (CC) views while 35% were more visible, or only visible, on one or the other.35 Using a different DBT system a retrospective, non-blinded consensus study of 36 patients with subtle lesions reported better visibility with one-view DBT than with either one- or two-view FFDM.18 One of the largest screening studies to date reported a 42% reduction in recall rate when using one-view DBT rather than conventional mammography, although the study had insufficient cancer cases to establish any differences in sensitivity.36 In a study of 200 suspicious breast lesions, Gennaro et al37 demonstrated that the sensitivity, specificity and lesion conspicuity of one-view DBT were comparable with those of two-view FFDM.
1.1.4 Reader performance
Multireader studies have reported improved receiver operating characteristic (ROC) performance using the combination of DBT and FFDM rather than FFDM alone; inter-reader variability has also been found to decrease, even among radiologists with differing levels of experience.38–42 The need for substantial reader training has nevertheless been highlighted.32,43,44
1.2 Digital Breast Tomosynthesis Working Party
1.2.1 Remit
The Digital Breast Tomosynthesis Working Party was set up to examine the current status of DBT technology, to advise on whether this technology should be considered for use in the NHS Breast Screening Programme (NHSBSP) and, if so, to identify areas where more detailed research is needed to assess DBT’s clinical utility.

NHSBSP September 2010
Digital Breast Tomosynthesis | 3
1.2.2 Composition
The multidisciplinary working party included
• a radiologist from the NHSBSP with extensive experience in breast imaging research and health technology evaluation
• an experienced breast screening radiographer with particular expertise in digital mammography and DBT
• the NHSBSP’s lead medical physicist with expertise in the evaluation and quality assurance of equipment, including digital mammography and DBT systems
• an imaging scientist with special interests in breast image analysis• a research fellow with experience in health technology evaluation.
1.3 Methodology
The working party met on two occasions. At the first meeting the aims of the group were established and companies involved in the production of DBT equipment were identified. It was agreed that representatives of these companies would be invited to give presentations and be interviewed using a structured questionnaire (Appendix 1). DBT equipment companies were identified through personal contact and through international radiology meetings (among them the European Congress of Radiology, Symposium Mammographicum, the International Workshops on Digital Mammography and the Radiological Society of North America). The structured questionnaire was drafted, circulated and agreed by members of the working party before distribution to the companies’ representatives.These were then invited to attend the second meeting of the working party in London, allowing its members where necessary to clarify information supplied in the questionnaire. Companies unable to send a representative to the meeting participated by teleconference. Information derived from the questionnaires and interviews is summarised in Appendix 2. The companies which participated are listed in Appendix 3. A table summarising the technical data for their equipment was sent out in March 2010, allowing each company to check and, where necessary, update the information to reflect new developments.

NHSBSP September 2010
4 | Digital Breast Tomosynthesis
2. TECHNICAL ASPECTS OF TOMOSYNTHESIS
2.1 General principles
In conventional geometric tomography, a plane of interest is established by moving the detector (originally a film–screen cassette) and the x-ray tube in opposite directions. This establishes a plane of interest (or a plane of focus). The contribution of structures in all other planes is blurred in the resulting tomographic image. Features within the plane of focus appear relatively sharp. The great disadvantage of this approach is that there is only a single plane of focus for each exposure and geometric configuration. In tomosynthesis an arbitrary number of planes may be retrospectively reconstructed from a single sequence of projection images. Typically a series of projection images is obtained while the x-ray tube moves in a circular or linear motion. However the motion of the x-ray tube could be more complex and the imaging detector could be stationary or moving. After the acquisition sequence is complete the projection images are combined by shifting and adding these together to bring a specific plane into focus. Different planes can be brought into focus by varying the amount of shifting. The advantages of tomosynthesis over conventional projection imaging are
• depth localisation• improved conspicuity, owing to the removal of the clutter caused by overlying tissue structures• improved contrast of local structure by limiting the dynamic range to a single plane.
Practical tomosynthesis differs from computed tomography (CT) in that projections are obtained over only a limited range of angles; it is thus often described as ‘limited angle tomography’. In CT, projections are obtained through either 180° or 360° rotations of x-ray tubes and detectors. This allows a complete sampling of the tissues to be imaged and the reconstitution of a complete 3D dataset; by this means slices can be reconstructed in any direction. The main disadvantage of CT imaging of the breast is the higher radiation dose involved in conventional system designs. At the moment, dedicated breast CT systems remain a subject of research and none is yet commercially available.
2.2 Technical features of current digital breast tomosynthesis systems
This section discusses in more detail the current features of digital breast tomosynthesis systems. It examines how these systems differ from conventional projection breast imaging and, in particular, how designs differ between the various manufacturers.
A number of key design features distinguish the different DBT systems. The most important of these are the mechanism for collecting data, the detector, the way in which images are acquired, and the software used to reconstruct and display the images. These are all interrelated and each is currently the subject of active research.
2.2.1 Detector and tube technology
The development of DBT was held back for many years by the lack of suitable x-ray imaging detectors. The main requirements for a suitable detector are

NHSBSP September 2010
Digital Breast Tomosynthesis | 5
• a large imaging area• rapid readout• high detective quantum efficiency (DQE).
The introduction of flat panel detectors into breast imaging systems meets all of these requirements. Digital mammography systems are now available with an imaging field of up to 24 × 30 cm. The whole projection image can be read out in a fraction of a second, enabling a series of projection images to be taken in a few seconds. Current detectors can achieve a DQE of 50% at low spatial frequencies (< 1 cycle per mm) at the doses normally used in projection mammography. However it has been a particular challenge for digital mammography to maintain a high DQE at the dose levels used for DBT projections, which are 10–15 times lower than those used in conventional projection imaging. This challenge has been met by minimising the presence of electronic noise in the images.
One way to lower the relative noise in the projection images used in DBT is to employ higher energy x-ray spectra, a development also seen in conventional digital mammography systems. Manufacturers have thus introduced x-ray tubes with either a rhodium (Rh) or a tungsten (W) target, rather than the molybdenum (Mo) targets normally used in film–screen imaging. Accompanying this change in target materials has been the introduction of filter materials other than the conventional molybdenum. Rhodium filters are in widespread use, with thicknesses ranging from 25 to 50 µm. The advantage of using a higher energy spectrum is that the x-rays are more penetrating; this leads to a lower breast dose while a greater photon flux reaches the imaging detector, thereby reducing the relative amount of quantum noise in the image. The disadvantage is that a lower radiographic contrast is generated by the structures of interest in the breast. On balance, however, adopting these spectra leads to an improvement in the ratio of contrast to noise. This trend has continued with the development of DBT systems with even higher energy spectra that use a tungsten/aluminium (W/Al) or tungsten/silver (W/Ag) target–filter combination.
2.2.2 Image acquisition parameters
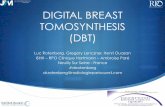
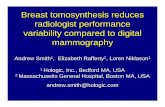
GeometryThe geometrical configuration used in DBT varies considerably between manufacturers. A distinction can be made between systems that use a completely isocentric motion and those that use a partial isocentric motion. In the first (Figure 1) the x-ray tube and detector rotate about the same axis. In the second (Figure 2) the detector remains stationary.
Tomography angleThe range of angles over which projection images are acquired is called the tomography angle. On most systems the tomography angle can be varied. The approach adopted by the different manufacturers can be classed as a narrow or wide angle. The Hologic and Sectra systems use narrow tomography angles of 15º and 11º respectively. The Hologic system is capable of being operated at a tomography angle of up to 30º. The GE and XCounter systems operate at slightly wider angles of 25º and 26º respectively, while Siemens favours a very wide tomography angle of 50º. The advantages and disadvantages of using narrow or wide tomography angles remain a matter for research and debate. However it is claimed that a wide angle provides better depth resolution while a narrow one enhances in-plane resolution.

NHSBSP September 2010
6 | Digital Breast Tomosynthesis
Figure 1 Complete isocentric motion, in which both the x-ray tube and image receptor rotate about a common axis.
Figure 2 Partial isocentric motion, in which the detector is stationary.
R76 Topical Review
(a)
(c)
(b)
Figure 5. Tomosynthesis geometries using isocentric motion. (a) Complete isocentric motion, inwhich both the x-ray tube and image receptor rotate about a common axis. (b) Partial isocentricmotion, in which the detector stays in one plane (or is stationary) and the x-ray tube rotates aboutsome point of rotation. (c) Partial isocentric motion of Niklason et al, in which the detector isstationary. (Figure adapted from figure A1 in Niklason et al (1997).)
and shifted data to account for magnification differences as the tube and detector rotate. Theselatter two steps may be summarized in the following equation from Kolitsi et al:
r =(
h − ad sin α
b cos α − a
)(1 − a
b cos α
)(15)
where r is the location in a fictitious plane containing QrPr of an object projected at location hin the horizontal plane. This fictitious plane containing QrPr has the property that the lengthof the line segment QrPr does not change length as a function of α. Therefore, a series of
R76 Topical Review
(a)
(c)
(b)
Figure 5. Tomosynthesis geometries using isocentric motion. (a) Complete isocentric motion, inwhich both the x-ray tube and image receptor rotate about a common axis. (b) Partial isocentricmotion, in which the detector stays in one plane (or is stationary) and the x-ray tube rotates aboutsome point of rotation. (c) Partial isocentric motion of Niklason et al, in which the detector isstationary. (Figure adapted from figure A1 in Niklason et al (1997).)
and shifted data to account for magnification differences as the tube and detector rotate. Theselatter two steps may be summarized in the following equation from Kolitsi et al:
r =(
h − ad sin α
b cos α − a
)(1 − a
b cos α
)(15)
where r is the location in a fictitious plane containing QrPr of an object projected at location hin the horizontal plane. This fictitious plane containing QrPr has the property that the lengthof the line segment QrPr does not change length as a function of α. Therefore, a series of
DoseManufacturers typically aim to perform a tomographic acquisition that results in a radiation dose comparable with the dose used in projection breast imaging. A detailed procedure is being prepared for publication that will extend the current UK, EU and International Atomic Energy Authority breast dosimetry protocols to include DBT systems.45 An earlier paper by the same authors extends the existing protocols to include the type of spectra used in modern 2D and 3D systems.46
Number of projectionsThe number of DBT projections is influenced by various factors, including the scan time, electronic noise and the tomography angle. In the clinical trials for the Hologic system, for example, 15 projections were used with a 15º tomography angle. The Siemens system uses 25 projections with a 50º tomography angle. Each projection will typically contribute approximately the same dose.

NHSBSP September 2010
Digital Breast Tomosynthesis | 7
In general, sufficient projections are needed to ensure adequate angular sampling. A number of simulation studies have been conducted to compute the optimal numbers of projections for specific systems.12,13
2.3 Reconstruction of DBT images
Reconstruction algorithms aim to produce images in which the low contrast objects are conspicuous, fine detail is visible and there are few artefacts. Clearly a balance has to be struck between dose, number of views and image quality.
The imaged volume is constructed from a sequence of between 9 and 48 projection mammograms acquired over a limited range of angles (between –25º and +25º, depending on the manufacturer). From the reconstructed volume a series of images can be displayed to show tissue at different depths in the breast. This overcomes the limitation of overlapping breast tissue in standard 2D projection mammograms. It also improves the conspicuity of lesions, as they can be displayed in images that include less background clutter than in a standard mammogram, which in turn allows for improved contrast.
The mathematical basis for the reconstruction of projection images was provided in 1917 by Radon,47 who showed how to reconstruct a single 2D slice from a set of one-dimensional projections. This enabled the development of computed tomography, which would become an important clinical tool from the late 1970s. In 1932 Ziedses des Plantes,48 working on a new technique that he called planigraphy, developed a method for reconstructing an arbitrary number of planes from a set of projection images. The first practical application of this came much later49 but early systems were hampered by the use of film (one per projection) and by the crude optical mechanisms for viewing the data. It was not until high quality projection images could be recorded digitally that tomosynthesis became a viable clinical technique.7
Once projection data have been obtained they must be pre-processed prior to reconstruction, for example with a logarithmic transformation.1 This allows pixel values to be related to tissue attenuation.
Many reconstruction algorithms are based on filtered backprojection, in which the signal at a detector is smeared back into the image space along a line in the direction of the attenuating tissue that gave rise to the signal.50 Projections are filtered in advance of this to reduce artefacts and the blurring inherent in the method. Owing to the limited number of angles at which images are acquired in DBT, the frequency space corresponding to the object being imaged is filled unevenly. A number of adaptations have been developed to compensate for the resulting artefacts in the reconstructed images.51–53 Filtered backprojection is more rapid than iterative methods and variants of it are used in both the Hologic and the Siemens systems.
Iterative methods have also been applied in the reconstruction of DBT images, however.8,54,55 In these, estimates of error are used successively to improve the reconstruction. The XCounter, Sectra and Dexela systems apply iterative methods. Simultaneous algebraic reconstruction has also been applied to DBT.56 This method conceives the image being reconstructed as an array of unknown values that can be found by solving a set of algebraic equations in terms of the projection data and by iterating this process until a solution is identified. A variant of this method is used in the GE system.

NHSBSP September 2010
8 | Digital Breast Tomosynthesis
2.4 Tomosynthesis image display
The reconstructed slices produced by commercial DBT systems are 0.5–3 mm thick. Images are viewed as a stack and the reader scrolls through them as if moving through the breast, with features moving in and out of focus.
The optimal thickness of tissue in which to identify breast abnormalities may occasionally be thicker than typical slice thickness; to address this overlapping slabs can be formed, each comprising several slices. These slabs are typically a few millimetres thick and, again, are viewed as if scrolling through the breast with features moving in and out of focus. A single slab encompassing the thickness of the breast thus resembles a conventional projection mammogram. If the slab thickness selected is insufficient and a single cluster of microcalcifications appears in several slabs the relationship between the particles will not be apparent when these slabs are viewed individually. The contrast of individual particles may nevertheless be greater than in a conventional mammogram and individual particles will move in and out of focus as the viewer scrolls through the slabs. The use of CAD for microcalcifications may overcome this limitation, although it is not yet clear how best to display prompts when viewing images in this way.
2.5 Workstation requirements for DBT
A supplement to the Digital Imaging and Communications in Medicine (DICOM) standard (Supplement 125) on how DBT images should be stored and displayed has only recently been published.57 As a result it may not be possible to display images produced by one manufacturer’s system on another’s workstation, although this should change in time. Workstations used for DBT also place additional demands on computer memory and power. This is particularly true if the workstation is used to perform the reconstruction as well as to display the images.

NHSBSP September 2010
Digital Breast Tomosynthesis | 9
3. ISSUES FOR THE NHS BREAST SCREENING PROGRAMME
3.1 Context
The new DBT technology is advancing even as the NHSBSP continues to work through the challenges of implementing 2D FFDM. It is expected that FFDM and Picture Archiving and Communications System (PACS) will be embedded by the time evidence-based conclusions are possible on the clinical utility of DBT in the NHSBSP. As a result the transition to DBT, if it happens, will not represent a great technological leap. The resource implications are nevertheless likely to be considerable.
3.2 Equipment
In April 2010 approximately one-third of NHSBSP centres had at least one FFDM unit. However most of the units are unable to undertake DBT. Were DBT to become a standard modality within the NHSBSP, these units would thus have to be replaced before end of life; alternatively the change in practice would have to be deferred until they reached end of life. FFDM units are expensive but DBT units are still more expensive and likely to remain so. Even for FFDM units amenable to a simple upgrade (eg software only) such upgrades involve considerable costs. Any evidence-based conclusion that DBT has a place in the NHSBSP on clinical grounds would need to include a rigorous assessment of cost-effectiveness.
3.3 PACS
DBT has significant implications for PACS, a system encompassing image viewing, image transfer, and short- and long-term archiving solutions. Reporting workstations that are suitable for 2D FFDM are not necessarily suitable for reporting DBT. Current DBT images do not comply with the new supplement 125 to the DICOM standard; however it is hoped that compliance will be achieved by existing and future manufacturers as new DBT equipment enters the market. In the meantime non-compliance with the DICOM supplement does not preclude image storage in PACS, although this would have to be explored with individual manufacturers.
In addition to the DICOM conformance issues, there are significant costs to upgrading existing workstations for DBT and centres currently choosing reporting workstations for FFDM will want to select the most futureproof versions available within their cost constraints.
DBT is a modality that generates large files for each examination and this makes particular demands on the imaging IT network infrastructure. Sufficient bandwidth is needed in both cabling and switching to ensure that image transfer speeds do not fall to unacceptable levels as a result of the increased traffic. Expert IT advice would be required in Trusts to address this.
Image transfer management hardware and software (such as shuttles and servers) are part of PACS solutions and the specification for these, too, must be robust enough to cope with the image volumes and traffic involved in the NHSBSP. The detailed requirements will depend on whether DBT is adopted as a screening tool or exclusively for diagnostic assessment.

NHSBSP September 2010
10 | Digital Breast Tomosynthesis
Although image storage is probably the simplest element of PACS it can be managed in various ways. Most local PACS will have short-term storage provision. If this provision is not expanded, however, the length of time for which images are stored will diminish as image volumes increase. Several options for long-term storage are under consideration: some Trusts have made their own on-site long-term storage arrangements; there are also various regional initiatives being developed in and outside of the Connecting for Health framework; and there is the potential for national long-term storage arrangements. In each case the image volumes associated with any additional work would need to be calculated, costed and catered for. The question also arises of when, or whether, raw data should be stored and NHSBSP centres might find national guidance on this helpful. Storing raw data is probably of greatest benefit for research and for the development and evaluation of new software products. These include CAD algorithms and quantitative breast density estimation software.
3.4 Resource and practical issues
3.4.1 Variables afecting examination times
Examination times for the first DBT system to become commercially available in the UK* do not appear to be significantly different from 2D FFDM, although independent quantitative data to support this impression are as yet unavailable. One key factor governing examination times comes into play if both 2D and 3D images are needed; it is the ability of the equipment to perform both examinations in a single compression episode. As the comparison table at Appendix 2 shows, this is not a universal design feature in DBT. The speed with which the system allows the grid between 2D and 3D imaging to be removed and replaced is another factor affecting the examination time as is the number of projection images acquired. It may take radiographers longer to check 3D image quality than to check 2D images as all projection images must be scrolled or cined through in order to detect motion blur. Movement perpendicular to the chest wall between projection images indicates movement of the subject during the exposure sequence. Movement parallel to the chest wall is caused by the projection variation. Acquisition workstation and gantry designs for DBT are not expected to differ significantly from FFDM, and nor is their installation. Here too, however, information is limited.
3.4.2 Variables affecting reporting times
Reporting times are significantly longer for DBT than 2D examinations because the quantity of information to be processed by the observer is much greater. The number of reconstructed slices to be viewed will depend on the slice thickness and the breast thickness. Even with efficient scrolling and cine options, however, the time taken to view all the reconstructed images is likely to be considerably greater than in a 2D examination. There is presently insufficient evidence to quantify reporting times for either diagnostic or screening use of DBT.
CAD is not currently available for DBT but is in development. It is expected to be particularly useful for microcalcifications and may limit reporting time increases if it enables observers to concentrate their searches on soft-tissue abnormalities.
*A second DBT system has now become commercially available in the UK, although it has not yet undergone formal clinical evaluation.

NHSBSP September 2010
Digital Breast Tomosynthesis | 11
3.5 Technical and clinical evaluation of DBT equipment for use in the NHSBSP
New designs for FFDM systems currently undergo technical evaluation by the National Coordinating Centre for Physics in Mammography (NCCPM). Once methodologies are developed for testing DBT systems, the tests will need to be applied to each such system as it comes on the market. Ideally, technical evaluations should be published soon after the release of equipment new to the UK.
Clinical user evaluation methodologies should be devised that minimise as far as is practicable the workload for evaluation centres and the time taken to produce reports. More efficient than the current user evaluation system would be a detailed NHSBSP specification that sets out the necessary clinical and practical features and performance criteria. Each manufacturer would be expected to match their product against this specification and provide evidence that the performance criteria are met. This might require some UK clinical user evidence, for which installations in approved centres would continue to be needed. It is particularly important to assess the ergonomic implications of new equipment designs. All of these findings could be collated into a single web-based document which would be updated when a new system came on the market.
3.6 Technical quality control and radiation dose monitoring
Suitable test protocols for commissioning, routine testing by physicists, and routine testing by radiographers would all need to be developed for DBT. Radiographer testing has been particularly challenging in the case of standard FFDM because manufacturers’ recommendations and methodologies vary and UK physicists’ preferences add a further dimension. Ideally manufacturers should liaise with UK mammography physicists at an early stage to agree suitable test protocols for DBT; NCCPM is currently working with most of the major manufacturers on the testing of their DBT systems as part of the OPTIMAM research project.
A robust but practical methodology for calculating radiation dose to the breast is urgently needed for DBT, and one is currently in development (see section 2.2).
3.7 Training
The process of training radiographers to use DBT is not expected to be radically different from applications training on any new equipment. DBT is more complex than standard FFDM, however, and the time needed to complete the training is thus likely to be longer. The training provided by equipment suppliers tends to increase with the number of systems purchased; centres installing DBT should therefore satisfy themselves in advance that sufficient training is available and that any linguistic and other difficulties associated with a lack of UK-based trainers can be kept to a minimum.
One supplier has worked with field experts to devise a sophisticated two-day DBT reporting training course, although the conditions for evaluating its effectiveness (or that of any other user training) are not yet in place. A two-day training course represents a significant time investment for a busy radiologist or film reader; options for shorter courses and online training should therefore be explored that support the achievement of competence in DBT interpretation. System suppliers and UK Breast Screening Training Centres could work together on developing and evaluating these training courses.

NHSBSP September 2010
12 | Digital Breast Tomosynthesis
3.8 Research required
Further clinical research is needed as studies published to date have yielded conflicting results. DBT needs to be compared with current standard imaging practice across key performance indicators such as sensitivity and specificity in screening and accuracy in diagnostic assessment.58 If it is found that DBT performance is at least as effective as FFDM then one of the primary aims of the research should be to be establish whether DBT could or should be used as a standalone imaging modality and whether one- or two-view DBT would be needed. This would help to determine if DBT should be used as a screening tool or if it should be restricted to the diagnostic setting. It is possible that DBT would prove more useful in women with dense breasts or in younger women; this too needs to be established. Effective comparison between DBT and standard FFDM is aided by systems that can undertake both acquisitions in a single compression, thus avoiding the confounding effects of small differences in positioning. Further work is needed to determine the optimal configuration and to develop specific phantoms and performance standards for DBT. This would form the basis for a formal comparison of commercially available systems that differ in key design features such as projection angle range, number of projections and reconstruction algorithms. Preliminary work towards these objectives has been reported as part of an EU-funded initiative (www.highrex.eu) and forms part of the OPTIMAM research project.59
Only when a robust body of clinical research data is available will it be possible to conclude whether and where DBT fits in UK clinical practice. Many questions of a more detailed nature also remain. Some practical issues require investigation, such as the method for displaying and reviewing DBT images and its impact on reporting times. Acceptability to women should also be investigated in light of compression and examination times which are longer than with standard FFDM.
A UK DBT research strategy is needed, developed by the NHSBSP in consultation with the Royal College of Radiologists Breast Group and other key stakeholders, to ensure that these key questions are answered as soon as possible.
3.9 Summary of recommendations
1. Manufacturers should be encouraged to make images produced compliant with the new DICOM standard for DBT (Supplement 125).
2. Manufacturers should be encouraged to develop systems able to perform DBT projection image acquisitions in the same compression episode as 2D acquisition.
3. Technical and clinical evaluation of new systems, technical quality control and dose calculation methodology development should be completed as soon as possible.
4. When making FFDM purchasing decisions, breast imaging centres might want to consider futureproofing in readiness for possible DBT implementation.
5. Robust cost-effectiveness evaluation should be undertaken, either after or (preferably) in parallel with clinical research demonstrating the utility of DBT.
6. UK Breast Screening Training Centres and DBT suppliers should collaborate in the production and rigorous evaluation of training courses for DBT reporting.
7. A comprehensive UK research strategy needs to be developed.

NHSBSP September 2010
Digital Breast Tomosynthesis | 13
APPENDIX 1: DIGITAL BREAST TOMOSYNTHESIS SYSTEM QUESTIONNAIRE
The purpose of this questionnaire is to obtain information on the technical and clinical performance of commercial DBT systems to enable us to determine whether any system(s) are appropriate or likely to be appropriate in the near future for a clinical trial in the UK NHSBSP.
Please answer the questions and include any comments in the spaces provided. Indicate which information (if any) that you want to be kept confidential. Any additional information you wish to be considered by the committee should be included as an Appendix.
Company name
Company representative
1. Has the system been submitted for FDA (or equivalent) approval?
If so, estimated target date for approval?
2. Is the system commercially available?
If not, estimated target date?
3. If commercially available, number and location of systems installed worldwide
4. Is the system CE marked?
If not, estimated target date?
5. Is NCCPM evaluation completed?
If not, estimated target date?
6. Can existing 2D systems be upgraded to incorporate the DBT package?
If so, please state which 2D model(s) can be upgraded.
7. Anode/filter material
8. Detector type
9. Detector element size
10. DBT projection exposure mode

NHSBSP September 2010
14 | Digital Breast Tomosynthesis
11. Plate size
12. (a) Actual pixel size
(b) Pixel size in reconstructed image
13. Minimum reconstruction slice thickness
14. Optimal slice thickness
15. Slab thickness
16. Recommended viewing protocol
17. Time from beginning of first projection exposure to end of last exposure
18. Rotation angle of system (degrees)
19. Range of gantry angles over which DBT can be acquired (degrees)
20. Projection exposure angles (give each angle)
21. Number of exposures
22. Exposure (mAs) at each angle
23. How are exposures controlled?
24. Phantom studies: radiation dose and phantom thickness
25. Breast studies: radiation dose and breast thickness for a single MLO view
26. Mean glandular breast radiation dose
27. Image processing time (reconstruction and display)
28. Breast compression (compared with standard 2D)
29. How is compression controlled?
30. Maximum compressed breast thickness for DBT imaging
31. Reconstruction algorithms
32. Is the DBT system able to acquire a 2D mammogram in the same compression?
33. Recommended DBT views
34. Image size (MB) per 2D view (raw and processed data)

NHSBSP September 2010
Digital Breast Tomosynthesis | 15
35. Image size (MB)
(a) Raw projection images total
(b) Processed projection images total
(c) Full reconstructed dataset
(d) Overall total
36. Can the same workstation be used for DBT and 2D?
37. Workstation storage capacity (GB and number of cases)
38. Format used for image storage
39. Can images be displayed on a PACS workstation?
40. Is CAD available for masses, calcifications or both?
41. Are CAD marks displayed in DBT slices or in 2D image?
42. What is the DBT system sensitivity/specificity for detection of soft tissue masses? (Give reference)
43. What is the DBT system sensitivity/specificity for detection of microcalcifications? (Give reference)
44. What would be your predicted reduction in recall rate compared with 2D? (Give reference)
45. Estimated reading time per case for DBT? (Give reference)

NHSBSP September 2010
16 | Digital Breast Tomosynthesis
APPENDIX 2: RESPONSES TO QUESTIONNAIRE: COMPARISON OF DBT SYSTEMS

NHSBSP September 2010
Digital Breast Tomosynthesis | 17
Dex
ela
ho
log
icg
es
ectr
as
iem
ens
XC
oun
ter
1. H
as th
e sy
stem
be
en s
ubm
itted
for
FDA
(or
equi
vale
nt)
appr
oval
?If
so, e
stim
ated
targ
et
date
for
appr
oval
?
Con
fiden
tial
Sel
enia
Dim
ensi
ons
2D is
so
ftw
are
upgr
adea
ble
to
3D o
pera
tion
and
has
FDA
ap
prov
al.
Sel
enia
Dim
ensi
ons
3D s
yste
m h
as b
een
subm
itted
to F
DA
Con
fiden
tial
Cur
rent
ly n
o pl
ans
to s
ubm
it fo
r FD
A
appr
oval
Est
imat
ed 2
011
No
2. Is
the
syst
em
com
mer
cial
ly
avai
labl
e?If
not,
estim
ated
ta
rget
dat
e?
Con
fiden
tial
Yes,
out
side
US
AN
ot c
omm
erci
ally
av
aila
ble
No.
Aw
aitin
g re
sults
of o
ngoi
ng
clin
ical
tria
ls
befo
re d
ecid
ing
on c
omm
erci
al
avai
labi
lity
Yes,
out
side
US
A.
Ava
ilabl
e fo
r ne
w
syst
ems
and
as a
n up
grad
e to
Mam
mom
at
Insp
iratio
n FF
DM
sy
stem
No.
Uni
t is
only
a
prot
otyp
e sy
stem
3. If
com
mer
cial
ly
avai
labl
e, n
umbe
r an
d lo
catio
n of
sys
tem
s in
stal
led
wor
ldw
ide?
Con
fiden
tial
A s
igni
fican
t num
ber
of
com
mer
cial
sys
tem
s co
verin
g al
l maj
or
Eur
opea
n co
untr
ies,
Sou
th
Am
eric
a, M
iddl
e E
ast,
Afr
ica
and
Asi
a-P
acifi
c.
Larg
e nu
mbe
r of
rese
arch
un
its in
stal
led
in U
SA
Not
com
mer
cial
ly
avai
labl
eN
/AFi
rst c
omm
erci
al
syst
ems
curr
ently
be
ing
inst
alle
d.
Thre
e te
st s
ites
with
rese
arch
pr
otot
ype
(Mal
mö,
N
ew Y
ork
and
Nor
th C
arol
ina)
.M
ore
than
20
inst
alla
tions
w
orld
wid
e
N/A
4. Is
the
syst
em C
E
mar
ked?
If no
t, es
timat
ed
targ
et d
ate?
Con
fiden
tial
Yes
Con
fiden
tial
No.
Aw
aitin
g re
sults
of
clin
ical
tria
ls b
efor
e se
ttin
g a
targ
et
date
Yes
N/A

NHSBSP September 2010
18 | Digital Breast Tomosynthesis
Dex
ela
ho
log
icg
es
ectr
as
iem
ens
XC
oun
ter
5. Is
NC
CP
M
eval
uatio
n co
mpl
eted
?If
not,
estim
ated
ta
rget
dat
e?
Con
fiden
tial
Dim
ensi
ons
2D te
chni
cal
eval
uatio
n co
mpl
eted
, re
port
aw
aite
d.U
ser
eval
uatio
n on
D
imen
sion
s 2D
for
scre
enin
g un
der
way
, sh
ould
repo
rt e
arly
201
0
Con
fiden
tial
No
plan
s fo
r ev
alua
tion
until
de
cisi
on m
ade
on
com
mer
cial
isat
ion.
Test
ing
by E
UR
EF
grou
p ha
s be
en
perf
orm
ed a
s pa
rt
of H
ighR
eX E
U
proj
ect
Mam
mom
at
Insp
iratio
n 2D
te
chni
cal a
nd
clin
ical
eva
luat
ion
repo
rts
in p
ress
No
6. C
an e
xist
ing
2D
syst
ems
be u
pgra
ded
to in
corp
orat
e th
e D
BT
pack
age?
If so
, ple
ase
stat
e w
hich
2D
mod
el(s
) ca
n be
upg
rade
d
Con
fiden
tial
Sel
enia
Dim
ensi
ons
2D
can
be u
pgra
ded
to D
BT
capa
bilit
y by
lice
nce
key.
Sel
enia
Dig
ital S
yste
ms
can
be fo
rklif
t upg
rade
d to
S
elen
ia D
imen
sion
s w
hen
appr
opria
te
Sen
ogra
phe
Ess
entia
l will
be
the
plat
form
fo
r D
BT
whe
n co
mm
erci
ally
av
aila
ble
2D S
ectr
a M
icro
Dos
e L3
0 w
ill
be u
pgra
deab
le
Yes,
Mam
mom
at
Insp
iratio
nN
o, th
is is
a
dedi
cate
d D
BT
devi
ce
7. A
node
/filte
r m
ater
ials
W a
node
/Rh
filte
rW
ano
de. T
hree
filte
rs
avai
labl
e: R
h an
d A
g fo
r 2D
, Al f
or 3
D
Ano
des:
Mo
and
Rh
Filte
rs: M
o an
d R
h
W/A
lM
o/M
o, M
o/R
h, W
/R
h (2
D)
W/R
h (3
D)
W/A
l
8. D
etec
tor
type
CM
OS
act
ive
pixe
l sen
sor
dete
ctor
a-S
e de
tect
or m
ater
ial o
n a-
Si T
FT a
rray
CsI
Spe
ctra
l pho
ton
coun
ting,
cr
ysta
lline
Si
Sol
id-s
tate
de
tect
or o
f a-S
eP
hoto
n co
untin
g ga
seou
s lin
e de
tect
or
9. D
etec
tor
elem
ent
size
74.8
µm
70 µ
m ×
70
µm10
0 µm
× 1
00 µ
mLi
ne d
etec
tors
50
µm
85 µ
m60
µm
10. D
BT
proj
ectio
n ex
posu
re m
ode
Pul
sed
acqu
isiti
ons
in
cont
inuo
us s
wee
p at
va
riabl
e ve
loci
ty
Pul
sed
acqu
isiti
ons
in
cont
inuo
us s
wee
pS
tep
and
shoo
tC
ontin
uous
Con
tinuo
usC
ontin
uous
11. P
late
siz
e29
× 2
3 cm
24 c
m ×
29
cm24
cm
× 3
1 cm
24 c
m ×
26
cm24
cm
× 3
0 cm
Mul
tislit
det
ecto
r, sp
read
ove
r 24
cm
× 3
0 cm

NHSBSP September 2010
Digital Breast Tomosynthesis | 19
Dex
ela
ho
log
icg
es
ectr
as
iem
ens
XC
oun
ter
12. (
a) A
ctua
l pix
el
size
(b) P
ixel
siz
e in
re
cons
truc
ted
imag
e
(a) 7
4.8
µm(b
) 74.
8 µm
× 7
4.8
µm
× 1
mm
(a) 7
0 µm
in 2
D, 1
40 µ
m in
3D
(pro
ject
ions
)(b
) 88
µm a
ppro
x. fo
r 18
× 2
4 cm
fiel
d of
vie
w.
108
µm a
ppro
x. fo
r 24
× 2
9 cm
fiel
d of
vie
w.
Mat
ched
to d
ispl
ayed
pix
el
size
for
the
2D im
age
whe
n it
is d
ispl
ayed
to fi
t to
scre
en o
n a
5 M
P m
onito
r
(a) 1
00 µ
m ×
100
µm
(b) 1
00 µ
m ×
100
µm
(a) 5
0 µm
(b) T
o be
de
term
ined
(a) 8
5 µm
(b) 8
5–10
0 µm
(v
aria
ble)
(a) 6
0 µm
(b) 6
0 µm
13. M
inim
um
reco
nstr
uctio
n sl
ice
thic
knes
s
0.5
mm
1 m
mC
onfid
entia
l1
mm
1 m
m1
mm
14. O
ptim
al s
lice
thic
knes
s1
mm
1 m
mC
onfid
entia
lC
urre
nt d
efau
lt is
sam
e as
slic
e th
ickn
ess
(3 m
m)
1 m
mN
ot c
linic
ally
ev
alua
ted
15. S
lab
thic
knes
sU
ser
confi
gura
ble
1–99
mm
sel
ecta
ble
on th
e S
ecur
View
DX
Wor
ksta
tion
Con
fiden
tial
Def
ault
is s
ame
as s
lice
thic
knes
s (3
mm
)
3, 5
, 7 m
mU
ser
confi
gura
ble
from
2 m
m to
full
brea
st th
ickn
ess
16. R
ecom
men
ded
view
ing
prot
ocol
Dep
ends
whe
ther
DB
T pr
iors
and
/or
FFD
M p
riors
ar
e av
aila
ble.
Han
ging
pr
otoc
ol c
an in
tegr
ate
FFD
M, t
omo,
MR
I and
US
View
ing
prot
ocol
defi
ned
by u
ser.
Use
r ca
n re
ad, i
n an
y or
der,
3D im
ages
from
an
y vi
ew, c
orre
spon
ding
2D
imag
es if
ava
ilabl
e an
d pr
iors
. 3D
imag
es
can
be s
crol
led
man
ually
or
aut
omat
ical
ly p
laye
d in
cin
e m
ode.
2D
and
3D
im
ages
acq
uire
d un
der
one
com
pres
sion
are
co
-reg
iste
red
for
view
ing
Con
fiden
tial
Rec
onst
ruct
ed 2
D
imag
e pu
t in
first
la
yer
follo
wed
by
full
stac
k.R
econ
stru
cted
2D
imag
e m
ay
also
be
used
fo
r co
mpa
rison
w
ith a
ny p
riors
. O
ther
wis
e pr
otoc
ols
follo
w
2D a
nd c
an b
e ad
just
ed b
ased
on
pref
eren
ce
Con
figur
able
at
syn
go
Mam
moR
epor
t w
ith T
omoV
iew
er
Not
inve
stig
ated

NHSBSP September 2010
20 | Digital Breast Tomosynthesis
Dex
ela
ho
log
icg
es
ectr
as
iem
ens
XC
oun
ter
17. T
ime
from
be
ginn
ing
of fi
rst
proj
ectio
n ex
posu
re
to e
nd o
f las
t ex
posu
re
2–4
s<
4 s
Con
fiden
tial
3–10
s (e
xpos
ure
time
typi
cally
< 2
s)
< 2
5 s
18 s
18. R
otat
ion
angl
e of
sy
stem
(deg
rees
)30
0 (+
150/
–150
)+
195
to –
155
+16
5 to
–18
5–1
00/+
180
± 1
80±
100
19. R
ange
of g
antr
y an
gles
ove
r w
hich
D
BT
can
be a
cqui
red
(deg
rees
)
Full
rang
e, a
s ab
ove
Full
rang
e, a
s ab
ove
25 Det
ecto
r an
gle
for
tom
o: +
20 to
+90
(R
MLO
) or
–20
to
–90
(LM
LO)
Full
rang
e, a
s ab
ove
± 9
0±
100
20. P
roje
ctio
n ex
posu
re a
ngle
s (g
ive
each
ang
le, d
egre
es)
–20,
–15
, –11
, –7,
–4,
–2,
–1
, 0.5
, 0, 0
.5, 1
, 2, 4
, 7,
11, 1
5, 2
0
Cur
rent
com
mer
cial
co
nfigu
ratio
n ha
s 15
eq
ually
spa
ced
proj
ectio
ns(–
7.50
, –6.
43, –
5.36
, –4.
29,
–3.2
1, –
2.14
, –1.
07, 0
.00,
1.
07, 2
.14,
3.2
1, 4
.29,
5.
36, 6
.43,
7.5
0)
Con
fiden
tial
21 p
roje
ctio
ns0,
0.5
5, 1
.1, 1
.65,
2.
2, 2
.75,
3.3
, 3.8
5,
4.4,
4.9
5, 5
.5,
6.05
, 6.6
, 7.1
5, 7
.7,
8.25
, 8.8
, 9.3
5, 9
.9,
10.4
5, 1
1
± 2
5, e
very
sec
ond
degr
ee48
ang
les
spre
ad
equa
lly o
ver
±13
21. N
umbe
r of
ex
posu
res
1715
exp
osur
es o
ver
a 15
° an
gula
r ra
nge.
The
se
wer
e de
term
ined
thro
ugh
a st
udy
to b
e op
timal
pa
ram
eter
s fo
r sc
reen
ing
use.
Diff
eren
t num
ber
of
expo
sure
s an
d an
gula
r ra
nges
are
pos
sibl
e fo
r cl
inic
al s
tudi
es
950
000
exp
osur
es
for
a fu
ll im
age
owin
g to
co
ntin
uous
read
out
of 2
1 de
tect
or li
nes
25C
ontin
uous
line
ar
scan
ning
. Ang
les
defin
ed b
y po
sitio
n of
line
det
ecto
rs
22. E
xpos
ure
(mA
s) a
t ea
ch a
ngle
Varia
ble
5.88
mA
s fo
r 48
mm
co
mpr
esse
d br
east
at
28 k
V
Varia
ble.
Tot
al e
xpos
ure
is s
ubdi
vide
d in
to e
qual
ex
posu
res
at e
ach
angl
e
Varia
ble
0.03
mA
s pe
r pr
ojec
tion
Uni
form
: tot
al
mA
s/25
App
rox.
1 m
As/
angl
e

NHSBSP September 2010
Digital Breast Tomosynthesis | 21
Dex
ela
ho
log
icg
es
ectr
as
iem
ens
XC
oun
ter
23. H
ow a
re
expo
sure
s co
ntro
lled?
Aut
omat
ic e
xpos
ure
cont
rol
Use
r se
lect
able
. AE
C
mod
es: A
uto
Filte
r, A
uto
kV, A
uto
Tim
e.A
lso
poss
ible
to u
se
Man
ual m
ode.
The
AE
C
mod
e al
low
s fo
r au
to-
sens
or s
elec
tion
or m
anua
l se
lect
ion
of s
enso
r re
gion
(a
nd p
ossi
bilit
ies)
Aut
omat
ic
expo
sure
con
trol
. M
anua
l kV
and
m
As
sele
ctio
n w
ill
also
be
poss
ible
Aut
omat
ic.
Adj
usts
out
put
dyna
mic
ally
bas
ed
on m
easu
red
CN
R
in th
e im
age
Aut
omat
ickV
sel
ecte
d ba
sed
on th
ickn
ess,
mA
s ba
sed
on p
re-p
ulse
Pre
sele
ctio
n ba
sed
on b
reas
t thi
ckne
ss
and
com
posi
tion
24. P
hant
om s
tudi
es:
radi
atio
n do
se a
nd
phan
tom
thic
knes
s
A s
tudy
of r
adia
tion
dose
ha
s be
en u
nder
take
n in
col
labo
ratio
n w
ith
the
Med
ical
Phy
sics
D
epar
tmen
t at R
oyal
M
arsd
en u
sing
Mon
te
Car
lo m
odel
ling.
Thi
s ha
s be
en v
alid
ated
usi
ng
phan
tom
s.Fo
r st
udy
at U
VA M
ark
Will
iam
s (A
ssoc
iate
P
rofe
ssor
of R
adio
logy
, B
iom
edic
al E
ngin
eerin
g,
and
Phy
sics
, UVA
) ch
oose
s th
e m
As
so th
at,
give
n th
e be
am s
pect
rum
ap
prop
riate
for
that
bre
ast
type
, the
MG
D is
equ
al to
or
less
than
the
aggr
egat
e M
GD
of a
n ac
tual
two-
view
FFD
M. T
his
is d
one
usin
g lo
ok-u
p ta
bles
Rad
iatio
n do
se le
vel i
n bo
th 2
D a
nd 3
D im
agin
g ca
n be
set
by
serv
ice
engi
neer
via
sel
ectio
n of
dos
e ta
bles
, allo
win
g im
agin
g w
ith a
ran
ge
of d
ose/
imag
e qu
ality
op
timiz
atio
ns d
epen
ding
on
use
r pr
efer
ence
.D
efau
lt 2D
imag
ing
dose
is
1.2
mG
y w
hen
imag
ing
the
AC
R p
hant
om (e
quiv
alen
t to
4.2
cm
50/
50 b
reas
t).
Def
ault
3D im
agin
g do
se
is 1
.45
mG
y fo
r sa
me
phan
tom
Con
fiden
tial
0.68
mG
y fo
r C
DM
AM
pha
ntom
, 6
cm P
MM
A
equi
vale
nt
1–2
mG
y fo
r 5
cm
brea
st e
quiv
alen
t P
MM
A p
hant
om,
acco
rdin
g to
cus
tom
er
pref
eren
ce
Typi
cal 1
.4 m
Gy
AG
D fo
r 45
mm

NHSBSP September 2010
22 | Digital Breast Tomosynthesis
Dex
ela
ho
log
icg
es
ectr
as
iem
ens
XC
oun
ter
25. B
reas
t stu
dies
: ra
diat
ion
dose
and
br
east
thic
knes
s fo
r a
sing
le M
LO v
iew
1.26
mG
y fo
r 4.
8 cm
bre
ast
1.41
mG
y fo
r 4–
4.5
cm
brea
stS
ame
dose
as
FFD
M s
cree
ning
.E
xact
val
ues
vers
us b
reas
t th
ickn
ess
are
confi
dent
ial
0.68
mG
y fo
r st
anda
rd b
reas
t. D
ose
leve
ls w
ill b
e ad
just
ed, b
ased
on
resu
lts fr
om c
linic
al
stud
ies
1–2
mG
y fo
r a
5 cm
br
east
, acc
ordi
ng
to c
usto
mer
pr
efer
ence
1.2
mG
y fo
r 4.
0 cm
, 2
mG
y fo
r 7.
0 cm
26. M
ean
glan
dula
r br
east
rad
iatio
n do
se1.
26 m
Gy
Ave
rage
for
1900
im
ages
was
2.3
mG
y fo
r co
mpr
esse
d br
east
th
ickn
ess
of 6
.1 c
m
± 1
.4 c
m.
Con
fiden
tial
From
firs
t 100
pa
tient
s: 0
.68
mG
y pe
r vi
ew, d
ose
leve
ls n
ot fi
nalis
ed
See
abo
veTy
pica
l 1.2
mG
y fo
r 4.
0 cm
, 2 m
Gy
for
7.0
cm
27. I
mag
e pr
oces
sing
tim
e (re
cons
truc
tion
and
disp
lay)
2 m
in3–
4 s
Con
fiden
tial
< 1
5 s
in
com
mer
cial
pr
oduc
t
< 1
min
15 m
in in
pro
toty
pe
28. B
reas
t co
mpr
essi
on
(com
pare
d w
ith
stan
dard
2D
)
Sam
e as
2D
Con
figur
able
. Clin
ical
tria
l us
ed s
ame
com
pres
sion
as
2D
Sam
e as
2D
Sam
e as
2D
Pilo
t stu
dy
plan
ned
to a
sses
s ho
w re
duct
ion
in c
ompr
essi
on
affe
cts
dose
and
im
age
qual
ity
Sam
e as
2D
, co
nfigu
rabl
eLe
ss th
an 2
D,
typi
cally
bel
ow
100
N
29. H
ow is
co
mpr
essi
on
cont
rolle
d?
Mot
oris
edM
anua
lly u
sing
foot
sw
itch,
gan
try
butt
ons
or
man
ual k
nob
Mot
oris
edM
otor
ised
Opt
imis
ed
com
pres
sion
fe
atur
e (O
pcom
p)
Mot
oris
ed u
sing
fo
ot p
edal
30. M
axim
um
com
pres
sed
brea
st
thic
knes
s fo
r D
BT
imag
ing
8 cm
15.5
cm
Con
fiden
tial
10 c
m fo
r pr
otot
ype
8 cm
9 cm
31. R
econ
stru
ctio
n al
gorit
hms
Itera
tive
reco
nstr
uctio
nFi
ltere
d ba
ckpr
ojec
tion
Sim
ulta
neou
s al
gebr
aic
reco
nstr
uctio
n te
chni
ques
Itera
tive
reco
nstr
uctio
n ba
sed
on th
e La
nge–
Fess
ler
algo
rithm
Ana
lytic
, filte
red
back
proj
ectio
nIte
rativ
e re
cons
truc
tion

NHSBSP September 2010
Digital Breast Tomosynthesis | 23
Dex
ela
ho
log
icg
es
ectr
as
iem
ens
XC
oun
ter
32. I
s th
e D
BT
syst
em
able
to a
cqui
re a
2D
m
amm
ogra
m in
the
sam
e co
mpr
essi
on?
Yes
Yes.
In c
ombi
ned
3D/2
D
prot
ocol
, sys
tem
acq
uire
s 3D
imag
e, re
turn
s to
0
degr
ees,
repl
aces
ant
i-sc
atte
r gr
id, a
cqui
res
a 2D
im
age.
Use
of t
he c
ombo
mod
e (2
D +
3D
) can
be
part
of
the
acqu
isiti
on w
orkfl
ow
prot
ocol
Con
fiden
tial
A re
cons
truc
ted
2D
proj
ectio
n im
age
can
be g
ener
ated
fr
om th
e sa
me
data
set a
s 3D
sl
ices
. Qua
lity
of
reco
nstr
ucte
d 2D
im
age
has
to b
e ve
rified
in c
linic
al
tria
l
Yes
No
33. R
ecom
men
ded
DB
T vi
ews
MLO
(MLO
and
CC
als
o su
ppor
ted)
MLO
and
CC
for
scre
enin
g us
e.A
dditi
onal
imag
es fo
r di
agno
stic
use
can
be
acqu
ired
in a
ny a
ngle
or
with
any
pad
dle
norm
ally
us
ed fo
r di
agno
stic
pu
rpos
es. M
agni
ficat
ion
is
not u
sed
for
DB
T
MLO
, no
need
id
entifi
ed fo
r ot
her
view
s
Aw
aitin
g re
sults
fr
om c
linic
al tr
ials
co
mpa
ring
two-
view
pro
ject
ion
mam
mog
raph
y w
ith C
C a
nd M
LO
view
DB
T as
wel
l as
MLO
onl
y D
BT
Cus
tom
er
pref
eren
ceM
LO
34. I
mag
e si
ze (M
B)
per
2D v
iew
(raw
and
pr
oces
sed
data
)
Raw
23
MB
Pro
cess
ed 2
3 M
BC
ombi
ned
46 M
B23
MB
per
imag
e us
ing
CM
OS
det
ecto
r
16 M
B (1
8 ×
24
cm)
26 M
B (2
4 ×
30
cm)
Unc
ompr
esse
d si
ze is
sa
me
raw
or
proc
esse
d.
How
ever
thes
e co
mpr
ess
diffe
rent
ly in
PA
CS
. P
roce
ssed
file
s co
mpr
ess
abou
t 3.5
:1, r
aw fi
les
abou
t 2:1
8 M
B (1
9 ×
23
cm)
14 M
B (2
4 ×
30
cm)
50 M
B r
aw a
nd
proc
esse
d20
MB
/vie
w40
MB
for
24 ×
30
cm r
aw a
nd
proc
esse
d

NHSBSP September 2010
24 | Digital Breast Tomosynthesis
Dex
ela
ho
log
icg
es
ectr
as
iem
ens
XC
oun
ter
35. I
mag
e si
ze (M
B)
per
view
1. R
aw p
roje
ctio
n im
ages
tota
l2.
Pro
cess
ed
proj
ectio
n im
ages
to
tal
3. F
ull r
econ
stru
cted
da
tase
t4.
Ove
rall
tota
l
For
23 ×
29
cm:
1. 4
142.
414
3. 1
265
for
55 m
m b
reas
t4.
209
3
For
18 ×
24
cm:
1. 3
02.
8 (N
B: p
roce
ssed
pr
ojec
tion
imag
es a
re n
ot
stor
ed in
divi
dual
ly b
ut a
re
com
pres
sed
as a
DIC
OM
se
cond
ary
capt
ure
obje
ct
and
cann
ot b
e fu
rthe
r co
mpr
esse
d by
the
PAC
S.)
3. 4
0 fo
r 55
mm
bre
ast
4. 3
12 (c
anno
t be
furt
her
com
pres
sed
by th
e PA
CS
)Fo
r 24
× 3
0 cm
:1.
39
2. 1
23.
46
for
55 m
m b
reas
t4.
388
For
19 ×
23
cm1.
72
2. 7
23.
app
rox.
500
for
45 m
m b
reas
t4.
Ove
rall
tota
l is
not t
he s
um o
f all
prev
ious
item
s as
no
t all
the
data
m
ay b
e sa
ved
or s
tore
d. G
E
prod
uct s
olut
ion
is
confi
dent
ial.
For
24 ×
31
cm1.
126
2. 1
263.
app
rox
800
for
45 m
m b
reas
t with
1
mm
slic
e sp
acin
g4.
Ove
rall
tota
l is
not t
he s
um o
f all
prev
ious
item
s as
no
t all
the
data
m
ay b
e sa
ved
or s
tore
d. G
E
prod
uct s
olut
ion
is
confi
dent
ial.
For
24 ×
26
cm1.
Up
to 8
00,
depe
ndin
g on
th
ickn
ess
2. U
p to
400
3. A
ppro
x. 1
50 M
B
typi
cal
4. 1
350
for
appr
ox.
60 m
m b
reas
t
For
24 ×
30
cm:
1. 5
002.
500
3. 5
00 (d
epen
ding
on
bre
ast s
ize:
1
slic
e =
max
. 10
MB
)4.
150
0 fo
r 50
mm
br
east
For
24 ×
30
cm:
1. 4
02.
< 4
03.
< 9
80 fo
r 45
mm
ob
ject
4. <
480
0

NHSBSP September 2010
Digital Breast Tomosynthesis | 25
Dex
ela
ho
log
icg
es
ectr
as
iem
ens
XC
oun
ter
36. C
an th
e sa
me
wor
ksta
tion
be u
sed
for
DB
T an
d 2D
?
Yes
Yes.
Wor
ksta
tion
is a
n ex
tens
ion
of H
olog
ic
Sec
urVi
ew w
orks
tatio
n.2D
imag
es c
an b
e re
view
ed a
s w
ith th
e S
elen
ia s
yste
m. 3
D im
age,
or
co-
regi
ster
ed 2
D/3
D
imag
es c
an b
e di
spla
yed.
S
yste
m s
uppo
rts
stan
dard
w
orks
tatio
n to
ols
for
both
2D
and
3D
. Spe
cific
3D
to
ols
incl
ude
met
hods
to
scr
oll t
hrou
gh th
e 3D
da
tase
t, ci
ne m
ode
for
auto
mat
ic s
crol
ling,
hei
ght
mea
surin
g to
ols,
2D
/3D
ov
erla
p, c
ine
scro
lling
in
mul
tiple
win
dow
s
Yes
Yes.
The
m
ulti-
mod
ality
w
orks
tatio
n al
low
s th
e ra
diol
ogis
t to
wor
k w
ith a
nd
com
pare
any
cas
e fr
om o
ne s
ingl
e w
orks
tatio
n
Yes
Yes
37. W
orks
tatio
n st
orag
e ca
paci
ty (G
B
and
num
ber
of c
ases
)
2 TB
. Upg
rade
able
as
requ
ired
1 TB
. Sto
res
appr
oxim
atel
y 45
00 c
ombi
ned
2D/3
D
imag
es
Con
fiden
tial
Con
figur
able
1 TB
New
PC
for
DB
T(In
tel Q
uad
Cor
e W
3520
, 2.6
6 G
Hz,
6
GB
RA
M,
1000
GB
)
3000
GB
, ap
prox
imat
ely
2000
cas
es
38. F
orm
at u
sed
for
imag
e st
orag
eD
ICO
M2D
: MG
3D: M
G S
econ
dary
C
aptu
re (S
C) a
nd in
201
0 w
ill s
uppo
rt D
ICO
M T
omo
IOD
(see
bel
ow)
DIC
OM
MG
en
hanc
ed
(3D
obj
ect f
or
Mam
mog
raph
y –
supp
lem
ent 1
25)
DIC
OM
DIC
OM
MG
for
proj
ectio
nsD
ICO
M C
T fo
r sl
ices
DIC
OM

NHSBSP September 2010
26 | Digital Breast Tomosynthesis
Dex
ela
ho
log
icg
es
ectr
as
iem
ens
XC
oun
ter
39. C
an im
ages
be
disp
laye
d on
a P
AC
S
wor
ksta
tion?
Yes
Cur
rent
ly, H
olog
ic
supp
orts
MG
sec
onda
ry
capt
ure
form
at w
hich
ca
n be
dis
play
ed o
nly
on
a H
olog
ic w
orks
tatio
n.
Exp
ect t
o re
leas
e su
ppor
t fo
r th
e D
ICO
M S
OP
cla
ss
for
mul
tifra
me
DB
T ‘B
reas
t To
mos
ynth
esis
Imag
e S
tora
ge’ f
or m
odal
ity M
G
by s
umm
er 2
010.
Whe
n th
e PA
CS
wor
ksta
tion
also
sup
port
s th
is, i
t will
be
pos
sibl
e to
dis
play
im
ages
on
PAC
S. U
ntil
then
, ind
ivid
ual s
lices
and
an
nota
tions
can
be
save
d as
sec
onda
ry c
aptu
re
and
disp
laye
d on
PA
CS
w
orks
tatio
ns. S
tand
ard
2D
MG
imag
es c
an c
urre
ntly
be
dis
play
ed o
n PA
CS
w
orks
tatio
ns
Yes
Yes
Yes
Dep
ends
on
PAC
S
wor
ksta
tion.
Im
ages
> 2
GB
are
a
prob
lem
for
som
e w
orks
tatio
ns
40. I
s C
AD
ava
ilabl
e fo
r m
asse
s,
calc
ifica
tions
or
both
?
Not
for
DB
TIf
a 2D
imag
e is
take
n as
pa
rt o
f DB
T ac
quis
ition
, C
AD
can
be
calc
ulat
ed
from
the
2D im
ages
. 3D
C
AD
exp
ecte
d to
be
rele
ased
in 2
010
Yes
No.
Wor
k on
goin
g fo
r m
icro
calc
ifica
tions
Not
yet
for
DB
TN
o
41. A
re C
AD
mar
ks
disp
laye
d in
DB
T sl
ices
or
in 2
D im
age?
2D im
ages
onl
yC
AD
mar
ks, c
alcu
late
d fr
om th
e 2D
imag
es, c
an
be p
lace
d on
eith
er o
r bo
th o
f the
2D
and
3D
im
age
sets
. Whe
n 3D
CA
D
is re
leas
ed m
arks
will
be
disp
laya
ble
on th
e D
BT
slic
es
2D im
ages
N/A
Will
be
in s
lices
an
d on
2D
imag
esN
/A

NHSBSP September 2010
Digital Breast Tomosynthesis | 27
Dex
ela
ho
log
icg
es
ectr
as
iem
ens
XC
oun
ter
39. C
an im
ages
be
disp
laye
d on
a P
AC
S
wor
ksta
tion?
Yes
Cur
rent
ly, H
olog
ic
supp
orts
MG
sec
onda
ry
capt
ure
form
at w
hich
ca
n be
dis
play
ed o
nly
on
a H
olog
ic w
orks
tatio
n.
Exp
ect t
o re
leas
e su
ppor
t fo
r th
e D
ICO
M S
OP
cla
ss
for
mul
tifra
me
DB
T ‘B
reas
t To
mos
ynth
esis
Imag
e S
tora
ge’ f
or m
odal
ity M
G
by s
umm
er 2
010.
Whe
n th
e PA
CS
wor
ksta
tion
also
sup
port
s th
is, i
t will
be
pos
sibl
e to
dis
play
im
ages
on
PAC
S. U
ntil
then
, ind
ivid
ual s
lices
and
an
nota
tions
can
be
save
d as
sec
onda
ry c
aptu
re
and
disp
laye
d on
PA
CS
w
orks
tatio
ns. S
tand
ard
2D
MG
imag
es c
an c
urre
ntly
be
dis
play
ed o
n PA
CS
w
orks
tatio
ns
Yes
Yes
Yes
Dep
ends
on
PAC
S
wor
ksta
tion.
Im
ages
> 2
GB
are
a
prob
lem
for
som
e w
orks
tatio
ns
40. I
s C
AD
ava
ilabl
e fo
r m
asse
s,
calc
ifica
tions
or
both
?
Not
for
DB
TIf
a 2D
imag
e is
take
n as
pa
rt o
f DB
T ac
quis
ition
, C
AD
can
be
calc
ulat
ed
from
the
2D im
ages
. 3D
C
AD
exp
ecte
d to
be
rele
ased
in 2
010
Yes
No.
Wor
k on
goin
g fo
r m
icro
calc
ifica
tions
Not
yet
for
DB
TN
o
41. A
re C
AD
mar
ks
disp
laye
d in
DB
T sl
ices
or
in 2
D im
age?
2D im
ages
onl
yC
AD
mar
ks, c
alcu
late
d fr
om th
e 2D
imag
es, c
an
be p
lace
d on
eith
er o
r bo
th o
f the
2D
and
3D
im
age
sets
. Whe
n 3D
CA
D
is re
leas
ed m
arks
will
be
disp
laya
ble
on th
e D
BT
slic
es
2D im
ages
N/A
Will
be
in s
lices
an
d on
2D
imag
esN
/A
Dex
ela
ho
log
icg
es
ectr
as
iem
ens
XC
oun
ter
42. W
hat i
s th
e D
BT
syst
em s
ensi
tivity
/sp
ecifi
city
for
dete
ctio
n of
sof
t tis
sue
mas
ses?
Unk
now
nS
ensi
tivity
and
spe
cific
ity
can
be c
alcu
late
d an
d as
sum
es th
at a
forc
ed
BIR
AD
S s
core
of 4
or
5 is
con
side
red
posi
tive
and
a sc
ore
of 1
, 2 o
r 3
is c
onsi
dere
d ne
gativ
e.
(In a
forc
ed B
IRA
DS
sc
ore
0 is
not
allo
wed
.) S
ensi
tivity
and
spe
cific
ity
have
not
bee
n re
port
ed
sepa
rate
ly fo
r m
asse
s an
d m
icro
calc
ifica
tions
. Fo
r th
e co
mbi
ned
coho
rt,
com
pris
ing
appr
oxim
atel
y 50
% o
f eac
h, u
sing
2D
pl
us D
BT
vers
us 2
D a
lone
, se
nsiti
vity
impr
oved
by
10.7
% a
nd s
peci
ficity
in
crea
sed
by 5
.1%
.60
Are
as u
nder
the
RO
C
curv
e (A
z) h
ave
been
re
port
ed s
epar
atel
y fo
r ca
lcifi
catio
n an
d no
n-ca
lcifi
catio
n ca
ses.
For
ca
lcifi
catio
n ca
ses,
the
Az
incr
ease
d by
0.0
4 us
ing
2D p
lus
DB
T ve
rsus
2D
al
one
(P-v
alue
0.0
73).
For
non-
calc
ifica
tion
case
s,
the
Az
incr
ease
d by
0.1
0 us
ing
2D p
lus
DB
T ve
rsus
2D
alo
ne (P
-val
ue 0
.000
8)61
To b
e co
nfirm
ed in
ongo
ing
clin
ical
tr
ials
Aw
aitin
g th
e re
sults
of
clin
ical
tria
lsS
ee li
tera
ture
.D
epen
ds o
n st
udy
popu
latio
n
Not
yet
eva
luat
ed

NHSBSP September 2010
28 | Digital Breast Tomosynthesis
Dex
ela
ho
log
icg
es
ectr
as
iem
ens
XC
oun
ter
43. W
hat i
s th
e D
BT
syst
em
sens
itivi
ty/s
peci
ficity
fo
r de
tect
ion
of
mic
roca
lcifi
catio
ns?
Unk
now
nS
ee a
bove
Aw
aitin
g re
sults
of
clin
ical
tria
lsA
wai
ting
resu
lts o
f cl
inic
al tr
ials
See
lite
ratu
re.
Dep
ends
on
stud
y po
pula
tion
Not
yet
eva
luat
ed
44. W
hat w
ould
be
you
r pr
edic
ted
redu
ctio
n in
reca
ll ra
te c
ompa
red
with
2D
?
Unk
now
n. E
stim
ate
20–3
0% re
duct
ion,
ba
sed
on e
xper
ienc
e of
D
Kop
ans
at M
GH
with
the
GE
sys
tem
Mea
n re
duct
ion
in re
call
rate
of 4
2.6%
for
norm
al
case
s w
as o
bser
ved
60
D K
opan
s sh
owed
41
% re
duct
ion
in
reca
ll ra
te61
Aw
aitin
g re
sults
of
clin
ical
tria
lsS
ee li
tera
ture
.D
epen
ds o
n st
udy
popu
latio
n
Not
yet
eva
luat
ed
45. E
stim
ated
read
ing
time
per
case
for
DB
T?
41.6
s62
Diffi
cult
to g
ive
accu
rate
es
timat
es b
ecau
se
mos
t exp
erie
nce
is w
ith
read
er s
tudi
es a
nd n
ot
repr
esen
tativ
e of
clin
ical
re
adin
g tim
es (a
s re
ader
s ar
e no
t exp
erie
nced
with
D
BT
read
ing
and/
or a
re
perf
orm
ing
mul
tiple
ste
ps
in re
cord
ing
data
, and
ca
ses
are
mor
e co
mpl
ex
than
scr
eeni
ng c
ases
). D
Kop
ans
estim
ated
40
s b
ut p
roba
bly
an
unde
rest
imat
e; P
hilp
otts
es
timat
es 2
D re
view
tim
e to
be
60 s
and
DB
T re
view
tim
e to
be
twic
e th
at.64
3D
CA
D is
exp
ecte
d to
im
prov
e re
adin
g tim
e by
sp
eedi
ng u
p th
e de
tect
ion
of m
icro
calc
ifica
tions
(w
hich
are
tim
e-co
nsum
ing
to s
earc
h fo
r on
mul
tiple
to
mos
ynth
esis
slic
es)
Est
imat
ed <
1 m
in
for
aver
age
brea
stA
wai
ting
the
resu
lts
of c
linic
al tr
ials
Dep
ends
on
expe
rienc
eN
ot y
et e
valu
ated

NHSBSP September 2010
Digital Breast Tomosynthesis | 29
APPENDIX 3: BIBLIOGRAPHY OF PUBLICATIONS FROM MANUFACTURERS OF DIGITAL BREAST TOMOSYNTHESIS SYSTEMS
Dexela
Williams MB, Judy PG, Mitali J et al. Tomographic dual modality breast scanner. In: Krupinski EA ed. Proceedings of the 9th International Workshop on Digital Mammography, 2008. Berlin: Springer-Verlag, 2008, 5116: 99–107.
Wu T, Stewart A, Stanton M et al. Tomographic mammography using a limited number of low-dose cone-beam projection images. Med Phys, 2003, 30(3): 365–380.
GE
Buls N, Mommaerts L, Wathion I et al. Development of multi-spectrum and multi-geometry computational model for x-ray breast imaging. Oral presentation to RSNA, 2009, Chicago, Illinois, USA.
Chan HP, Wei J, Zhang Y et al. Digital breast tomosynthesis (DBT) mammography: effect of number of projection views on computerized mass detection using 2D and 3D approaches. Oral presentation to RSNA, 2009, Chicago, Illinois, USA.
Gennaro G. Inter-reader variability: tomosynthesis versus digital mammography. Oral presentation to RSNA, 2008, Chicago, Illinois, USA.
Gennaro G, Baldan E, Bezzon E. Clinical performance of digital breast tomosynthesis versus full-field digital mammography: preliminary results. In: Krupinski EA ed. Proceedings of the 9th International Workshop on Digital Mammography, 2008. Berlin: Springer-Verlag, 2008, 5116: 477–482.
Gennaro G, Toledano A, Baldan E et al. Clinical performance of digital breast tomosynthesis compared to digital mammography: blinded multireader study. Oral presentation to European Congress of Radiology, 2009, Vienna, Austria.
Gennaro G, Toledano A, di Maggio C et al. Digital breast tomosynthesis versus digital mammography: a clinical performance study. Eur Radiol, 2010, 20(7): 1545–1553.
Gennaro G, Dromain C, Balleyguier CS et al. Digital breast tomosynthesis vs digital mammography: analysis of discordant cancer cases. Oral presentation to ECR, 2010, Vienna, Austria.
Helvie M. Characterization of benign and malignant breast masses by digital breast tomosynthesis mammography. Oral presentation to RSNA, 2008, Chicago, Illinois, USA.

NHSBSP September 2010
30 | Digital Breast Tomosynthesis
Helvie M. Research digital tomosynthesis mammography: detection of T1 invasive breast carcinomas not diagnosed by conventional breast imaging or physical exam. Oral presentation to RSNA, 2008, Chicago, Illinois, USA.
Helvie M, Hadjiiski L, Zhang Y et al. Digital breast tomosynthesis mammography: initial assessment of non-palpable microcalcifications. Oral presentation to RSNA, 2008, Chicago, Illinois, USA.
Helvie M, Chan H-P, Hadjiiski L et al. Digital breast tomosynthesis mammography: successful assessment of benign and malignant microcalcifications. Oral presentation to RSNA, 2009, Chicago, Illinois, USA.
Klausz R, Souchay H. Digital tomosynthesis: finite thickness slices or tomographic planes? Oral presentation to RSNA, 2009, Chicago, Illinois, USA.
Kontos D, Ikejimba L, Bakic PR et al. Digital breast tomosynthesis parenchymal texture analysis for breast cancer estimation: results from a screening trial. Oral presentation to RSNA, 2009, Chicago, Illinois, USA.
Kopans D. Calcification in digital breast tomosynthesis (DBT). Oral presentation to RSNA, 2008, Chicago, Illinois, USA.
Kopans D, Moore R. Digital breast tomosynthesis (DBT): NCI 3000 Women Trial. Oral presentation to RSNA, 2009, Chicago, Illinois, USA.
Malhaire C, Thibault F, Dromain C et al. Digital breast tomosynthesis: approaching mammographic challenges. Oral presentation to RSNA, 2009, Chicago, Illinois, USA.
Moore R, Kopans D. Initial callback rates for conventional and digital breast tomosynthesis mammography: comparison in the screening setting. Oral presentation to RSNA, 2007, Chicago, Illinois, USA.
Raeymaeckers S, Buls N, Souchay H et al. Image quality phantom for digital breast tomosynthesis. Oral presentation to RSNA, 2009, Chicago, Illinois, USA.
Rouault S, Muller S, Iordache R et al. Designing an anthropomorphic breast phantom for breast tomosynthesis. Eur Radiol, 2009, 19: 533–586.
Roubidoux M, Rahnama-Moghadam S, Hadjiiski L et al. Digital tomosynthesis mammography compared to clinical mammogram spot views. Oral presentation to RSNA, 2009, Chicago, Illinois, USA.
Souchay H, Klausz R. Out-of-plane propagation of texture as a function of acquisition parameters in digital breast tomosynthesis. Oral presentation to Tomosynthesis Imaging Symposium, 2009, Duke University, Durham, North Carolina, USA.
Souchay H, Hersemeule G, Hendrick ER. Image quality performance evaluation of digital breast tomosynthesis on GE Senographe Essential system. Oral presentation to ECR, 2010, Vienna, Austria.
Thibault F, Dromain C, Breucq C et al. Digital breast tomosynthesis (DBT): a multi-reader clinical performance study. Oral presentation to ECR, 2010, Vienna, Austria.

NHSBSP September 2010
Digital Breast Tomosynthesis | 31
Williams MB, Judy PG, More MJ et al. The impact of anisotropic sampling on the MTF of reconstruction in limited aperture tomosynthesis. In: Samei E, Hsieh J eds. Physics of Medical Imaging 2009, Proceedings of SPIE, Lake Buena Vista, Florida, USA, 2009, 7258: 72581P–72581P-7.
Hologic
Good WF, Abrams GS, Catullo VJ et al. Digital breast tomosynthesis: a pilot observer study. AJR, 2008, 190: 865–869.
Gur D, Abrams GS, Chough DM et al. Digital breast tomosynthesis: observer performance study. AJR, 2009, 193(2): 586–591.
Michell M, Wasan RK, Whelehan P et al. Digital breast tomosynthesis: a comparison of the accuracy of digital breast tomosynthesis, two-dimensional digital mammography and two-dimensional screening mammography (film–screen). Breast Cancer Res 2009, 11(Suppl 2): O1.
Niklason L. Comparison of FFDM with breast tomosynthesis to FFDM alone: performance in fatty and dense breasts. Oral presentation to Tomosynthesis Imaging Symposium, 2009, Duke University, Durham, North Carolina, USA.
Niklason L. Inter-reader variability for the decision to recall and BIRADS characterization: comparing breast tomosynthesis plus FFDM to FFDM alone. Oral presentation to Tomosynthesis Imaging Symposium, 2009, Duke University, Durham, North Carolina, USA.
Poplack SP, Tosteson TD, Kogel CA, Nagy HM. Digital breast tomosynthesis: initial experience in 98 women with abnormal digital screening mammography. AJR, 2007, 189(3): 616–623.
Rafferty EA. Inter-reader variability: comparing breast tomosynthesis combined with FFDM to FFDM alone. Oral presentation to ECR Satellite Symposium, 2009, Vienna, Austria.
Rafferty EA. Multicenter, retrospective study: comparing breast tomosynthesis combined with FFDM to FFDM alone. Oral presentation to ECR Satellite Symposium, 2009, Vienna, Austria.
Rafferty EA, Niklason L, Jameson LA. Breast tomosynthesis: one view or two? Oral presentation to RSNA, 2006, Chicago, Illinois, USA.
Rafferty EA, Niklason L, Halpern E et al. Assessing radiologist performance using combined full-field digital mammography and breast tomosynthesis versus full-field digital mammography alone: results of a multi-center, multi-reader trial. Oral presentation to RSNA, 2007, Chicago, Illinois, USA.
Rafferty E, Smith A, Niklason L. Assessing radiologist performance in dense versus fatty breasts using combined full-field digital mammography and breast tomosynthesis compared to full-field digital mammography alone. Oral presentation to RSNA, 2009, Chicago, Illinois, USA.
Smith AP, Rafferty EA, Niklason L. Clinical performance of breast tomosynthesis as a function of radiologist experience level. In: Krupinski EA ed. Proceedings of the 9th International Workshop on Digital Mammography, 2008. Berlin: Springer-Verlag, 2008, 61–66.
Smith AP, Rafferty EA, Niklason L. Breast tomosynthesis reduces radiologist performance variability compared to digital mammography. Oral presentation to ECR 2009, Vienna, Austria.

NHSBSP September 2010
32 | Digital Breast Tomosynthesis
Teertstra HJ, Loo CE, van den Bosch MA et al. Breast tomosynthesis in clinical practice: initial results. Eur Radiol, 2010, 20(1): 16–24.
Sectra
None.
Siemens
Andersson I, Ikeda DM, Zackrisson S et al. Breast tomosynthesis and digital mammography: a comparison of breast cancer visibility and BIRADS classification in a population of cancers with subtle mammographic findings. Eur Radiol, 2008, 18: 2817–2825.
Lo JY, Baker JA, Orman J et al. Breast tomosynthesis initial clinical experience with 100 human subjects. Oral presentation to RSNA, 2006, Chicago, Illinois, USA.
Svahn T, Andersson I, Chakraborty D et al. The diagnostic accuracy of breast tomosynthesis vs digital mammography: a free-response observer performance study. Oral presentation to RSNA, 2009, Chicago, Illinois, USA.
XCounter
Carton AK, Ullberg C. Optimization of a dual-energy contrast-enhanced technique for a photon counting digital breast tomosynthesis system. In: Krupinski EA ed. Proceedings of the 9th International Workshop on Digital Mammography, 2008. Berlin: Springer-Verlag, 2008: 116–123.
Maidment ADA, Ullberg C. Clinical evaluation of a photon-counting tomosynthesis mammography system. In: Astley SM, Brady M, Rose C, Zwiggelaar R eds. Proceedings of the 8th International Workshop on Digital Mammography, 2006. Berlin: Springer-Verlag, 2006, 4046: 144–151.
Maidment ADA, Albert M, Thunberg S et al. Evaluation of a photon-counting breast tomosynthesis imaging system. In: Flynn MJ ed. SPIE International Symposium on Medical Imaging, 2005. San Diego: SPIE, 5745: 572–582.
Maidment ADA, Ullberg C, Lindman K et al. Evaluation of a photon-counting breast tomosynthesis imaging system. In: Flynn MJ ed. SPIE International Symposium on Medical Imaging, 2006. San Diego: SPIE, 6142: 61420B.

NHSBSP September 2010
Digital Breast Tomosynthesis | 33
APPENDIX 4
Manufacturers’ contact details
Dexela
Dexela Ltd Wenlock Business Centre 50–52 Wharf Road London N1 7EU
Tel: +44 (0)207 148 3107 Fax: +44 (0)207 148 3107 Web: www.dexela.com
Hologic
Hologic UK Ltd Unit 2, Link 10 Napier Way Crawley, West Sussex, RH10 9RA
Tel: +44 (0)129 352 2080 Fax: +44 (0)129 352 8010 Web: www.hologic.com
GE
GE Healthcare (UK) Pollards Wood Nightingales Lane Chalfont St Giles Bucks HP8 4SP
Tel: +44 (0)1494 545200 Web: www.gehealthcare.com
Sectra
Sectra Ltd Baird House Seebeck Place Knowlhill Milton Keynes MK5 8FR
Tel: +44 (0)1908 673107 Fax: +44 (0)1908 242904 Web: www.sectra.com
Siemens
Siemens Healthcare (UK) Newton House Sir William Siemens Square Frimley Camberley Surrey GU16 8QD
Tel: 0845 600 1966 Web: www.medical.siemens.com
XCounter
XCounter AB Svärdvägen 11 S-182 33 Danderyd Sweden
Tel: +46 8 622 23 00 Fax: +46 8 622 23 12 Web: www.xcounter.se

NHSBSP September 2010
34 | Digital Breast Tomosynthesis
REFERENCES1. Dobbins JT III, Godfrey DJ. Digital x-ray tomosynthesis: current state of the art and clinical potential. Phys Med Biol,
2003, 48(19): R65–106.2. Boyd NF, Guo H, Martin LJ et al. Mammographic density and the risk and detection of breast cancer. N Engl J
Med, 2007, 356(3): 227–236.3. Fletcher SW, Elmore JG. Clinical practice: mammographic screening for breast cancer. N Engl J Med, 2003,
348(17): 1672–1680.4. Kolb TM, Lichy J, Newhouse JH. Comparison of the performance of screening mammography, physical
examination, and breast US and evaluation of factors that influence them: an analysis of 27,825 patient evaluations. Radiology, 2002, 225(1): 165–175.
5. National Collaborating Centre for Primary Care. Familial Breast Cancer: the Classification and Care of Women at Risk of Familial Breast Cancer in Primary, Secondary and Tertiary Care (Partial Update of CG41). National Institute for Health and Clinical Excellence, 2006.
6. Dobbins JT. Tomosynthesis imaging: at a translational crossroads. Med Phys, 2009, 36(6): 1956–1967.7. Niklason LT, Christian BT, Niklason LE et al. Digital tomosynthesis in breast imaging. Radiology, 1997, 205(2):
399–406.8. Suryanarayanan S, Karellas A, Vedantham S et al. Comparison of tomosynthesis methods used with digital
mammography, Acad Radiol, 2000, 7(12): 1085–1097.9. Wu T, Stewart A, Stanton M et al. Tomographic mammography using a limited number of low-dose cone-beam
projection images. Med Phys, 2003, 30(3): 365–380.10. Sechopoulos I, Ghetti C. Optimization of the acquisition geometry in digital tomosynthesis of the breast. Med Phys,
2009, 36(4): 1199–1207.11. Smith A. Full-field breast tomosynthesis. Radiol Manage, 2005, 27(5): 25–31.12. Chan H, Wei J, Zhang Y et al. Digital breast tomosynthesis DBT mammography: effect of number of projection
views on computerised mass detection using 2D and 3D approaches. Oral presentation to RSNA, 2008, Chicago, Illinois, USA.
13. Mertelmeier T, Ludwig J, Zhao B, Zhao W. Optimization of tomosynthesis acquisition parameters: angular range and number of projections. In: Krupinski EA ed. Proceedings of the 9th International Workshop on Digital Mammography, 2008. Berlin: Springer-Verlag, 2008, 5116: 220–227.
14. Rafferty EA, Georgian-Smith D, Kopans DB, et al. Comparison of full-field digital tomosynthesis with two view conventional film screen mammography in the prediction of lesion malignancy. Oral presentation to RSNA, 2002, Chicago, Illinois, USA.
15. Rafferty EA, Kopans DB, Georgian-Smith D, et al. Comparison of full-field digital tomosynthesis and conventional two view screen film mammography in lesion detection and assessment of lesion conspicuity. Oral presentation to RSNA, 2003, Chicago, Illinois, USA.
16. Helvie M, Roubidoux MA, Hadjiiski L et al. Tomosynthesis mammography versus conventional mammography: comparison of breast masses detection and characterisation. Oral presentation to RSNA, 2007, Chicago, Illinois, USA.
17. Poplack SP, Tosteson TD, Kogel CA, Nagy HM. Digital breast tomosynthesis: initial experience in 98 women with abnormal digital screening mammography. Am J Roentgenol, 2007, 189(3): 616–623.
18. Andersson I, Ikeda DM, Zackrisson S et al. Breast tomosynthesis and digital mammography: a comparison of breast cancer visibility and BIRADS classification in a population of cancers with subtle mammographic findings. Eur Radiol, 2008, 18(12): 2817–2825.
19. Tingberg A, Andersson I, Ikeda DM et al. BIRADS Classification of breast tomosynthesis compared to mammography and ultrasonography. In: Krupinski EA ed. Proceedings of the 9th International Workshop on Digital Mammography, 2008. Berlin: Springer-Verlag, 2008, 5116: 67–73.
20. Fornvik DBR, Zackrisson S, Timberg P et al. Breast tomosynthesis: assessment of breast cancer size compared with digital mammography and ultrasonography. Oral presentation to ECR, 2009, Vienna, Austria.
21. Kopans DB, Moore R, Gavenonis S. Calcification in digital breast tomosynthesis. Oral presentation to RSNA, 2008, Chicago, Illinois, USA.
22. Lau BA, Reiser IS, Nishikawa RM. Microcalcification detectability in tomosynthesis. In: Hsieh J, Samei E eds. Medical Imaging 2008: Physics of Medical Imaging. Proceedings of the SPIE. San Diego: SPIE, 2008, 6913: 69134L–69134L-7.
23. Sidky EY, Pan X, Reiser IS et al. Enhanced imaging of microcalcifications in digital breast tomosynthesis through improved image-reconstruction algorithms. Med Phys, 2009, 36(11): 4920–4932.

NHSBSP September 2010
Digital Breast Tomosynthesis | 35
24. Nishikawa RM, Reiser I, Seifi P et al. A new approach to digital breast tomosynthesis for breast cancer screening. In: Hsieh J, Flynn MJ eds. Medical Imaging 2007: Physics of Medical Imaging. Proceedings of the SPIE. San Diego: SPIE, 2008, 6510: 65103C.1–65103C.8.
25. Das M, Gifford HC, O’Connor M, Glick SJ. Evaluation of a variable dose acquisition technique for microcalcification and mass detection in digital breast tomosynthesis. Med Phys, 2009, 36(6): 1976–1984.
26. Reiser I. Automated detection of microcalcification clusters for digital breast tomosynthesis using projection data only: a preliminary study. Med Phys, 2008, 35(4): 1486–1493.
27. Reiser I, Nishikawa RM, Giger ML et al. Computerized mass detection for digital breast tomosynthesis directly from the projection images. Med Phys, 2006, 33(2): 482–491.
28. Chan H-P, Wei J, Zhang Y et al. Computer-aided detection of masses in digital tomosynthesis mammography: comparison of three approaches. Med Phys, 2008, 35(9): 4087–4095.
29. Rafferty EA, Kopans DB, Georgian-Smith D et al. Evaluation of call-back rate for screening mammography using full-field digital tomosynthesis versus conventional film screen mammography. Oral presentation to ARRS, 2003, San Diego, California, USA.
30. Lo J, Baker J, Orman J et al. Breast tomosynthesis: initial clinical experience with 100 human subjects. Oral presentation to RSNA, 2006, Chicago, Illinois, USA.
31. Moore R, Kopans DB, Rafferty EA et al. Initial callback rates for conventional and digital breast tomosynthesis mammography in the screening setting. Oral presentation to RSNA, 2007, Chicago, Illinois, USA.
32. Gur D, Abrams GS, Chough DM et al. Digital breast tomosynthesis: observer performance study. Am J Roentgenol, 2009, 193(2): 586–591.
33. Teertstra HJ, Loo CE, van den Bosch MA, van Tinteren H, Rutgers EJ, Muller SH et al. Breast tomosynthesis in clinical practice: initial results. Eur Radiol, 2010, 20(1): 16–24.
34. Rafferty EA, Kopans DB, Wu T, Moore RH. Breast tomosynthesis: will a single view do? Oral presentation to RSNA, 2004, Chicago, Illinois, USA.
35. Rafferty EA, Niklason LE, Jameson-Meehan L. Breast tomosynthesis: one view or two? Oral presentation to RSNA, 2006, Chicago, Illinois, USA.
36. Kopans D, Moore R. Digital breast tomosynthesis (DBT) NCI 3000 women trial. Oral presentation to RSNA, 2008, Chicago, Illinois, USA.
37. Gennaro G, Toledano A, di Maggio C et al. Digital breast tomosynthesis versus digital mammography: a clinical performance study. Eur Radiol, 2010, 20(7): 1545–1553.
38. Rafferty EA, Niklason L, Halpern E et al. Assessing radiologist performance using combined full-field digital mammography and breast tomosynthesis versus full-field digital mammography alone: results of a multi-centre, multi-reader trial. Oral presentation to RSNA, 2007, Chicago, Illinois, USA.
39. Smith AP, Rafferty EA, Niklason L. Clinical performance of breast tomosynthesis as a function of radiologist experience level. In: Krupinski EA ed. Proceedings of the 9th International Workshop on Digital Mammography, 2008. Berlin/Heidleberg, Germany, Springer-Verlag, 2008, 5116: 61–66.
40. Gennaro G, Toledano A, Baldan E et al. Inter-reader variability: tomosynthesis versus digital mammography. Oral presentation to RSNA, 2008, Chicago, Illinois, USA.
41. Smith AP, Rafferty EA, Niklason L. Breast tomosynthesis reduces radiologist performance variability compared to digital mammography. Oral presentation to ECR 2009, Vienna, Austria.
42. Rafferty, EA. Inter-reader variability: comparing breast tomosynthesis combined with FFDM to FFDM alone. Oral presentation to ECR Satellite Symposium, 2009, Vienna, Austria.
43. Gur D. Tomosynthesis: potential clinical role in breast imaging. Am J Roentgenol, 2007, 189(3): 614–615.44. Good WF, Abrams GS, Catullo VJ et al. Digital breast tomosynthesis: a pilot observer study. Am J Roentgenol,
2008, 190(4): 865–869.45. Dance DR, Young KC, van Engen RE. Estimation of mean glandular breast dose for digital tomosynthesis: factors
for use with the UK, European and IAEA breast dosimetry protocols (in preparation).46. Dance DR, Young KC, van Engen RE. Further factors for the estimation of mean glandular dose using the United
Kingdom, European and IAEA breast dosimetry protocols. Phys Med Biol, 2009, 54(14): 4361–4372.47. Radon J. Über die Bestimmung von Funktionen durch ihre Integralwerte längs gewisser Mannigfaltigkeiten.
Berichte über die Verhandlungen der Sächsischen Akademie der Wissenschaft, Leipzig, Math-Phys, 1917, 69: 262–77
48. Ziedses des Plantes BG. Eine neue Methode zur Differenzierung in der Roentgenographie (Planigraphie). Acta Radiol, 1932, 13: 182–192
49. Garrison JB, Grant DG, Guier WH, Johns RJ. Three dimensional roentgenography. Am J Roentgenol, 1969, 105: 903–908.

NHSBSP September 2010
36 | Digital Breast Tomosynthesis
50. Lauritsch G, Harer WH. A theoretical framework for filtered backprojection in tomosynthesis. In: Hanson K ed. Medical Imaging 1998. Physics of Medical Imaging. Proceedings of the SPIE. San Diego: SPIE, 1998, 3338: 1127–1137.
51. Orman J, Mertelmeier T, Haerer W. Adaptation of image quality using various filter setups in the filtered backprojection approach for digital breast tomosynthesis. In: Astley SM, Brady M, Rose C, Zwiggelaar R eds. Proceedings of the 8th International Workshop on Digital Mammography, 2006. Berlin: Springer-Verlag, 2006, 4046: 175–182.
52. Ludwig J, Mertelmeier T, Kunze H, Harer W. A novel approach for filtered backprojection in tomosynthesis based on filter kernels determined by iterative reconstruction techniques. In: Krupinski EA ed. Proceedings of the 9th International Workshop on Digital Mammography, 2008. Berlin: Springer-Verlag, 2008, 5116: 612–620.
53. Wu T, Moore RH, Kopans DB. Voting strategy for artifact reduction in digital breast tomosynthesis. Med Phys, 2006, 33: 2461–2471.
54. Wu T, Stewart A, Stanton M et al. Tomographic mammography using a limited number of low-dose cone-beam projection images. Med Phys, 2003, 30(3): 365–380.
55. Wu T, Moore RH, Rafferty EA et al. A comparison of reconstruction algorithms for breast tomosynthesis. Med Phys, 2004, 31(9): 2636–2647.
56. Van de Sompel D, Brady M. Systematic performance analysis of SART as applied to digital breast tomosynthesis, In: Krupinski EA ed. Proceedings of the 9th International Workshop on Digital Mammography, 2008. Berlin: Springer-Verlag, 2008, 5116: 561–569.
57. The DICOM Standard. Available via Digital Imaging and Communications in Medicine (DICOM) site at http://medical.nema.org/. Accessed 16.06.2010.
58. Mundy L, Hiller JE. Breast Tomosynthesis: A Breast Cancer Screening Tool. Prioritising Summary, vol 21. Canberra: Australia and New Zealand Horizon Scanning Network, 2008.
59. Van Engen R, Bouwman R, van der Burght R et al. Image quality measurements in breast tomosynthesis. In: Krupinski EA ed. Proceedings of the 9th International Workshop on Digital Mammography 2008. Berlin: Springer-Verlag, 2008, 5116: 696–702.
60. Rafferty EA. Multicenter, retrospective study: comparing breast tomosynthesis combined with FFDM to FFDM alone. Oral presentation to ECR Satellite Symposium, 2009, Vienna, Austria.
61. Kopans D, Moore R. Digital breast tomosynthesis (DBT) NCI 3000 women trial. Oral presentation to RSNA, 2009, Chicago, Illinois, USA.
62. Moore R, Levy A, Stewart A, Kopans D. Reading behaviour for screening digital breast tomosynthesis (DBT) compared to conventional 2D mammography (CM). Oral presentation to RSNA, 2006, Chicago, Illinois, USA.
63. Fratt L. Mammography’s next step: the dawning of breast tomosynthesis. Health Imaging & IT, June 2008. Available at http://www.healthimaging.com/index.php?option=com_articles& view=article&id=1106. Accessed 16.06.2010.