Digestive Diseases Introduction to Human Diseases Chapter 10.
39
Digestive Diseases Introduction to Human Diseases Chapter 10
-
Upload
sydni-collins -
Category
Documents
-
view
215 -
download
0
Transcript of Digestive Diseases Introduction to Human Diseases Chapter 10.

Digestive Diseases
Introduction to Human Diseases
Chapter 10

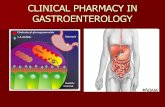
Gastrointestinal System Anatomy
OropharynxEsophagusStomachSmall intestineLarge intestineRectumOther digestive organs: liver, gall bladder, pancreas

Stomatitis
Inflammation of the oral mucosaEtiology: Herpetic stomatitis (cold sores, HSV 1) Aphthous stomatitis (canker sores) Temporary immunosuppression involve in both
S/S: painful blisters or ulcersTreatment: topical anesthetics & rinses, antiviral meds for herpes (1 day of meds)

Gastroesophageal Reflux Disease(GERD)
Backup (reflux) of gastric & duodenal contents (food & acid) past the incompetent lower esophageal sphincter into the esophagusMore GERD in people over 40 YOAStats: 7% of US population have daily heartburn 20-40% with heartburn have GERD

GERD
Usually involves the following: Functional/mechanical problem with LES Certain foods, meds, hormones
Coffee, etoh, b-or Ca channel blockers, nitrates, progesterone
Obesity (contributing factor)

GERD
S/S: Heartburn, regurgitation, dysphagia, cough, chest pain,
wheezing
Treatment: Antacids, H2 blockers, PPI, prokinetic agents 80% GERD is controlled with meds, 20% need surgery
Other issues: 50% GERD get esophagitis 8-15% GERD have Barrett’s esophagus (stricture)

Gastritis
Acute or chronic inflammation & erosion of the gastric mucosaEtiology: idiopathic frequently, may be due to foods, meds, alcohol, caffeineS/S: epigastric pain, nausea & vomiting, belching, full feeling in epigastriumTreatment: avoidance of irritants, H2 blockers or antacids

Gastroenteritis
Inflammation of the stomach & small intestine Some types: traveler’s diarrhea, food poisoning
Etiology: commonly infectious (viral, bacterial, protozoal, parasitic), also meds and toxinsDiagnosis: history, stool culture for bacteria or stool exam for parasitesTreatment: varies with etiology Meds for parasitic, helminthic, protozoal Antiemetics, sometimes antidiarrheals Avoids of fatty or dairy foods, increased fluid intake

Hiatal Hernia
Protrusion of part of the stomach through the diaphragmatic opening into the thoraxTypes: Sliding (most common) GE jct + stomach slide upwards
into thorax Paraesophageal (rolling) GE jct remains fixed
More common in: women, obesity, trauma,older age Etiology: unknown Suspected: high intra-abdominal pressure or weakness of
gastroesophageal junction, trauma

Hiatal Hernia (HH)
S/S: 50% asymptomatic Heartburn, chest pain, dysphagia, reflux
Diagnosis: CXR, endoscopy
Treatment: Diet, meds for reflux, change in activities,
surgery

Peptic Ulcers
Well-defined lesion (ulcers) in the mucosa of the lower esophagus, stomach, pylorus, or duodenumEtiology: Gastric acid hypersecretion conditions, Helicobacter
pylori infection, mucosal damage from aspirin, NSAID’s, alcohol, tobacco
More common in: Middle-aged and older males, smokers, alcohol and
NSAID users, Type A blood type (gastric) and type O blood type (duodenal)

Peptic Ulcers
S/S: heartburn, epigastric pain, nausea, vomiting, GI bleeding, symptoms within/about 2 hours post-prandial
Diagnosis: endoscopy
Treatment: H. pylori: antibiotics, bismuth Same as reflux, also possible endoscopic
surgery (cautery) or routine surgical resection

Infantile Colic
Paroxysmal abdominal pain or crampingFirst 3 months of lifeEtiology: Excessive fermentation & gas production, overeating,
air swallowing, rapid feeding, inadequate burping
S/S: crying, drawing up legsDiagnostics: Rule of Three’s (1st 3 months of life, crying 3 hrs/day, 3 days/week, at least 3 weeks.)Treatment: calming child, feeding techniques, etc.

Lower GI Tract Diseases
Celiac Disease/ Gluten Induced EnteropathyMalabsorption due to immunologic reaction to part of gluten (wheat), gluten intolerance, and mucosal damage to intestineInherited, female to male = 2 to 1S/S: abdominal distention, diarrhea (large, greasy, grey-yellow), poor absorption of B12 & folate, weight loss,

Celiac Disease
Testing: small intestinal biopsy (villi destruction) and improvement on gluten-free diet
Treatment: Dietary avoidance of wheat products,
supplements if needed of folate, etc.

Irritable Bowel Syndrome
GI symptom complex with no known organic cause: Alternating constipation & diarrhea Some change in colon motility
A diagnosis of exclusionMost frequent GI disorder in USEtiology: unknownDisorder of adults

IBS
Treatment: Variable, avoidance of foods or other factors
that provoke episodes No single successful treatment

Crohn’s Disease/ Regional Enteritis
Chronic inflammatory disease of unknown etiology that primarily involves the ileum Transmural thickening of bowel wall Patchy or segmental areas of this Thickening of wall, narrowing of lumen
S/S: abdominal pain, diarrhea, anorexia & weight loss, anal or other fissures, fistulas

Crohn’s Disease
Diagnosis Colonoscopy & biopsy
Treatment: Immunosuppressives, anti-inflammatories,
surgery (colectomy, ileostomy)

Ulcerative Colitis
Inflammation & ulceration of the colon, beginning in rectum or sigmoid and extending proximallyOnly mucosa is involvedUniform involvement of the area, no segments or patches of healthy tissueEtiology, diagnostic test, treatment: like Crohn’s Disease

Diverticular Disease
Diverticulosis Outpouching of colonic mucosa that bulge
through wall into peritoneum
Diverticulitis Infection of diverticuli
Etiology: obstruction of diverticuli by matter (particulate material in stool, fecalith, etc) and subsequent infection

Diverticular Disease
S/S LLQ pain, fever, nausea, diarrhea
Diagnostics Blood tests nondiagnostic, CT scan
Treatment Dietary changes (high fiber), antibiotics for
flare-up, surgery if needed

Acute Appendicitis
Inflammation & infection of appendix, often due to obstruction by fecalith
S/S: RLQ pain (McBurney’s Point), anorexia, low-grade fever, nausea, possible peritonitis if rupture occurs
Treatment: appendectomy

Hemorrhoids
Dilated, tortuous veins of anus or rectum Internal or external
S/S: itching, bleeding, pain
Etiology: high intraabdominal pressure conditions
Treatment: antiinflammatories, hemorrhoidectomy

Abdominal Hernias
Protrusion of an internal organ through an abnormal opening in the abdominal wall Umbilical (ventral), femoral, or inguinal (most
common type)
Etiology: congenital or acquired weakness in part of abdominal wall Lifting, pregnancy, obesity = predispositions
S/S: visible or palpable bulge is most common, sometimes pain, nausea, vomiting

Hernias
Incarcerated vs. strangulated hernia
Treatment: Surgery (herniorraphy)

Colorectal Cancer
Adenocarcinoma almost alwaysDisease of adults (over 40 YOA)Risk factors: High meat, low fiber diets, IBS, polyposis
S/S: often asymptomatic, occult lower GI bleeding, change in bowel habitsDiagnosis: sigmoidoscopy or colonoscopy and biopsy, routine screening after age 50

Colorectal Cancer
Treatment: Surgery if early Chemotherapy/radiation if mets

Diarrhea
Frequent passage of feces, often increased in volume and fluidity
Is this itself a disease?
Sign or symptom?
Etiology: numerous
Testing: stool cultures, examination for WBC, RBC, parasites, etc

Helminths
Worms living as parasites in human GI tract
Types: Roundworms
Ingestion of larvae deposited by dogs/cats Usually children ingest dirt
Pinworms Egg deposition around anus Nocturnal pruritis

Pancreatitis
Inflammation of pancreas Autodigestion due to leaking pancreatic
digestive enzymes
Acute or chronicMild or life-threateningEtiology: associated with alcoholism, biliary disease, trauma, severe hyperlipidemias

Pancreatitis
S/S: Upper abdominal pain, vomiting
Diagnosis: blood tests helpful
Treatment: IV hydration, treatment of vomiting, no oral foods (GI rest)

Biliary Diseases
Cholelithiasis Gallstones, mostly cholesterol in US Mostly middle-ages or older females May are asymptomatic
Cholecystitis Inflammation of GB wall Often occurs due to obstruction of cystic duct
by gallstone

Biliary Diseases
S/S: Severe RUQ pain, often spasmic, nausea,
vomiting, intolerance of fatty foods
Diagnosis: ultrasound, blood tests
Treatment: If mild: dietary avoidance If severe: laparoscopic cholecystectomy

Cirrhosis
Chronic, irreversible degenerative liver disease, like scarring with regrowth of abnormal liver cells
Due to repeated trauma of many etiologies: Toxins, infections, metabolic, circulatory
Liver failure (hepatic insufficiency) often occurs

Cirrhosis
Etiologies: Alcoholic is most common etiology Also biliary diseases, hemochromotosis,
idiopathic
S/S: jaundice, firm, enlarged palpable liver, weight loss, pruritis, increased bleeding,ascites, edema of legs and abd wall, esophageal varices

Hepatitis
Acute viral etiology is most common Hepatitis A: infectious hepatitis Hepatitis B: via human secretions or feces Hepatitis C: less common, often becomes
chronic, quiescent for decades Hepatitis D: delta hepatitis Hepatitis E: rare in US, feces-contaminated
water Hepatitis G: blood-borne illness

Hepatitis
Diagnosis: blood testing for antibodies and antigens, liver function tests
S/S: RUQ pain, nausea, fatigue, jaundice, loss of appetite, fever
Treatment: Usually supportive, immunoglobulin

Pancreatic Cancer
Usually adenocarcinoma
Often head of the pancreas
Geriatric disease (60-70 YOA)
Remains asymptomatic until late Great majority of patients have advanced
disease at time of diagnosis