Differential diagnosis of abdominal pain · Inguinal és femoral hernia „1. Invaginate loose...
60
Differential diagnosis of abdominal pain Lakatos Péter László
Transcript of Differential diagnosis of abdominal pain · Inguinal és femoral hernia „1. Invaginate loose...

Differentialdiagnosis of
abdominal pain
Lakatos Péter László

The acute abdominal pain
Precise anamnesis
Physical examination
are prognosticated to the cause of the pain

The acute abdominal pain Anamnesis
Sudden pain Perforation
Mesenteric infarction
Aortic aneurysm rupture
The onset is determinated
Progressio Gastroenteritis has constant pain Appendicitis has rising pain
Colic has decrease-increase-dedrease-increase pain
The extended pain is rarely life threatening

Az acut hasi fájdalomAnamnézis
A hirtelen fájdalom okai Perforáció
Mesenteriális infarctus
Aorta aneurisma ruptura
A beteg szinte percre meg tudja mondani a kezdetet.
Progresszió A gastroenteritis állandó
Az appendicitis fokozódó
A kólika csökken – nő –csökken – nő
Tartama A hetek óta tartó fájdalom
ritkán életet veszélyeztető
A: spontaneously pass away f.g. gastroenteritis
B: colic (intestinal, kidney, gall bladder)
C: progressive: appendicitis, diverticulitis

The acute abdominal pain Anamnesis
Sudden pain Perforation
Mesenteric infarction
Aortic aneurysm rupture
The onset is determinated
Progressio Gastroenteritis has constant pain Appendicitis has rising pain
Colic has decrease-increase-dedrease-increase pain
The extended pain is rarely life threatening

The acute abdominal pain Anamnesis
Location
The pain is not always fit
to the organ

The acute abdominal pain Anamnesis
Location
Appendicitis
Early periumbilical pain
Later right iliac fossa
pain

The acute abdominal pain Anamnesis
Location
Cholecystitis
Right upper quadrant

The acute abdominal pain Anamnesis
Location
Pancreatitis
Epigastric
Back

The acute abdominal pain Anamnesis
Location
Diverticulitis
Left-side lower
abdomen

The acute abdominal pain Anamnesis
Location
Peptic ulcer perforation
epigastric pain

The acute abdominal pain Anamnesis
Location
Ileus
Periumbilical pain

The acute abdominal pain Anamnesis
Location
Mesenteric
ischaemia/infarction
Periumbilical pain

The acute abdominal pain Anamnesis
Location
Abdominal aneurysm
rupture
Abdominal-back pain

The acute abdominal pain Anamnesis
Location
Gastroenteritis
Periumbilical

The acute abdominal pain Anamnesis
Location
Pelvic inflammation
Lower abdomen

The acute abdominal pain Anamnesis
Location
Extrauterine gravidity
Lower abdomen

The acute abdominal pain Anamnesis
Intensity of the pain
Difficult to measure

The acute abdominal pain Anamnesis
Location
Appendicitis
Early periumbilical pain
Later right iliac fossa
pain
Intensity
++

The acute abdominal pain Anamnesis
Location
Cholecystitis
Right upper quadrant
Intensity
++

The acute abdominal pain Anamnesis
Location
Pancreatitis
Epigastric
Back
Intensity
++ - +++

The acute abdominal pain Anamnesis
Location
Diverticulitis
Left-side lower
abdomen
Intensity
+ - ++

The acute abdominal pain Anamnesis
Location
Peptic ulcer perforation
epigastric pain
Intensity
+++

The acute abdominal pain Anamnesis
Location
Ileus
Periumbilical pain
Intensity
++

X-ray findings of ileus

The acute abdominal pain Anamnesis
Location
Mesenteric
ischaemia/infarction
Periumbilical pain
Intensity
+++

The acute abdominal pain Anamnesis
Location
Abdominal aneurysm
rupture
Abdominal-back pain
Intensity
+++

The acute abdominal pain Anamnesis
Location
Gastroenteritis
Periumbilical
Intensity
+ - ++

The acute abdominal pain Anamnesis
Location
Pelvic inflammation
Lower abdomen
Intensity
++

The acute abdominal pain Anamnesis
Location
Extrauterine gravidity
Lower abdomen
Intensity
++



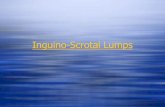
Inguinal és femoral hernia
„1. Invaginate loose scrotal skin with your index
finger. 2. Follow the spermatic cord upward to
above the inquinal ligament, and find the opening
of the external inquinal ring. 3. If possible, gently
follow the inguinal canal laterally. 4. Ask the
patient to strain down or cough. 5. Note any
palpable herniating mass as it touches your finger.
Palpate the anterior thigh in the region of the
femoral canal…..
If the findings suggest a hernia, try to reduce it by
sustained pressure with your finger. If the mass is
tender or the patient reports nausea and vomiting,
you have to finish this maneuver.
Incarcerated hernia: when its contents can not be
returned to the abdominal cavity.
Strangulated hernia:when the blood supply is
compromised (tenderness, nausea, vomiting)”
Lateral inquinal, indirect
Medial inquinal, direct
Femoral Bates B: A guide to physical examination. Fifth edition.


The acute abdominal pain Anamnesis
The characteristic of the pain
Connections
Relating to mealtimes
Decrease – duodenal ulcer
Increase- gastric ulcer, gall bladder, pancreas
Relating to defecation - colon
Relating to urination stimulus - nephrolith
Relating to position
Peritonitis- immobile
Nephrolith- restless, look for the less painfull position

The acute abdominal pain Anamnesis
The relation of the pain with other symptoms Fever
Shivering
Nausea
Vomiting
Night sweats
Loss og weight
Myalgia
Arhalgia
Icterus
Meteorism
Dysuria
Obstipation
Diarrhoea

The acute abdominal pain Anamnesis
Pain and
Previous diseases
Family anamnesis

The acute abdominal pain Physical examination
Examination of the anamnesis
Verify
Exclude

The acute abdominal pain Physical examination
Examination of the anamnesis
Verify
Exclude
The anamnesis and the physical examination
can be atypical in elder patients, gravidity,
diabetes, immundefections and ascites

The acute abdominal pain Physical examination
The patient position
movement
expression
general imperssion

The acute abdominal pain Physical examination
Vital signs
Other organs examination

The acute abdominal pain Physical examination
Abdomen
Tenderness
Abdominal resistance
Defense
Percussion
Auscultation
Rectal digital examination
Gynecologic examination

The acute abdominal pain Laboratory examination
Blood test
Electrolyte
BUN, creatinine
Blood glucose
Astrup
Liver function
Amylase
Urine
Pregnancy test

The acute abdominal pain X-ray
Free abdominal air
Air-fluid levels
Ultrasound
CT

The acute abdominal pain X-ray
Free abdominal air
Air-fluid levels

The acute abdominal pain Other diagnostics
Peritoneal lavage
Laparoscopy
Explorative
laparotomy

The definition of acute abdomen
Life-threatening condition due to acute onset abdominal disease with typical symptoms and physical findings, which reqiures: Prompt surgical intervention
Acute appendicitis
Acute peritonitis
Acute intestinal obstruction
Acute mesenteric vascular insufficiency
Rupture of the spleen, extrauterin gravidity, dissection of aortic aneurysm
Emergent admission to a monitored bed or intensive care unit Acute pancreatitis
Acute cholecystitis
Purpura abdominalis

Physical findings in acute abdomen syndrome
Abdominal pain The medication can influence. In case of shock the pain
might be diminished
Vomiting Mostly in cases of obstruction of intestine
Involuntary muscular rigidity Inflammation(irritation) of parietal peritoneum
Distension As a consequence of mechanic or paralytic ileus
Shock Hypotension, sweating, pallor, tachycardy. In case of
shock sometimes bradycardy because of the vagal (oarasympathic) activation

The chronic abdominal pain
„Organ disease”
Chronic pancreatitis
Abdominal neoplasia
Inflammatory bowel
disease
Mesenteric ischemia
Pelvic inflammatory
disease
Endometriosis
„Functional disease”
Irritable bowel syndrome
Non ulcer dyspepsia
Gall bladder – pain
(dyskinesia)

The chronic abdominal pain
Location
Connection (mealtime, defecation, position, daytime, nervousness)?
Other symptoms?
General status
Physical examination
Precise examiantions (laboratory, radiology, „ex juvantibus”)

The chronic abdominal pain Chronic pancreatitis
After eating
Belt-like pain
Severe status
Steatorrhea

The chronic abdominal pain Abdominal neoplasia
The pain slowly comes in to the life of the
patient
The location of the pain is depends on the
location of the tumor
Progressive

The chronic abdominal pain Inflammatory bowel disease
The pain and the defecation is in a nexus
(tenesmus !)
The localisation of the pain nearly depends
on the location
The pain is caused by the activity of the
disease

The chronic abdominal painMesenteric ischemia
In a typical cause after maeltime
(abdominal angina)
Sometimes auscultated
In a chronic case effect malabsorption
Progressive

The chronic abdominal pain Pelvic inflammatory disease
Lower abdominal pain on either side
Gynecological exam (rectalis) confirm
Common inflammatory symptoms

The chronic abdominal pain Endometriosis
Lower abdominal pain
Symptoms often worsen with the
menstrual cycle

The chronic abdominal painIrritable bowel syndrome
Everything is around the stool
After mealtime immediate defecation
No symptoms during the night
Normal gender status
Other gastrointestinal signs
Other psychology signs

The chronic abdominal painNon ulcer dyspepsia
Upper abdominal pain or dyscomfort
A lot of types – few regularity in the
symptoms
There is no „alarm” sign in the definition

The chronic abdominal painGall bladder – pain (dyskinesia)
After mealtime
Pain under the right ribs
Usually with other symptoms (nausea,
meteorism)
Long lasting compalint – mainly females
„Negative” bile examiantions

Summary-differencial diagnostics of abdominal pain
ANAMNESIS (since when-how-associated to?)
Location of the abdominal pain. Rebound
tenderness
Auscultation of bowel movement
Free air in the abdomen – percussion of liver span
Hernial orifices should always carefully examined
for the presence of a mass
Appropriate imaging and laboratoy investigations
Rectal digital examination