Diagnostic Imaging of Hydrocephalus & Pneumocephalus
64
C.N.S. Hydrocephalus & Pneumocephalus
-
Upload
mohamed-zaitoun -
Category
Health & Medicine
-
view
742 -
download
0
Transcript of Diagnostic Imaging of Hydrocephalus & Pneumocephalus

C.N.S.Hydrocephalus & Pneumocephalus

Mohamed Zaitoun
Assistant Lecturer-Diagnostic Radiology Department , Zagazig University Hospitals
EgyptFINR (Fellowship of Interventional
Neuroradiology)[email protected]



Knowing as much as possible about your enemy precedes successful battle
and learning about the disease process precedes successful management

Hydrocephalusa) Ventricular Anatomyb) CSF Dynamicsc) Etiologyd) Classification

a) Ventricular Anatomy :-The ventricular system consists of two lateral
ventricles and midline third & fourth ventricles-The foramen of Monro connects the lateral ventricles
with the third ventricle-The cerebral aqueduct (of Sylvius) connects the third
ventricle with the fourth ventricle-The fourth ventricle continues inferiorly as the central
canal of the spinal cord, the fourth ventricle also drains into the subarachnoid space & basal cisterns via three foramina :
Paired foramina of Luschka (Luschka is Lateral) Single foramen of Magendie (Magendie is Medial)




1-Foramen of Monro

1-Cerebral aqueduct

Normal Sagittal T2 shows CSF flow-related signal void at the aqueduct of Sylvius (long black arrow) , foramen of Magendie (thick black arrow) and foramen magnum (white arrows)

b) CSF Dynamics :-CSF is produced by the choroid plexus, which is located
in specific locations throughout the ventricular system :
1-Body & temporal horns of each lateral ventricle2-Roof of third ventricle3-Roof of fourth ventricle-No choroid plexus in the cerebral aqueduct or occipital
or frontal horns of the lateral ventricles

-The ventricular volume is approximately 25 mL , the volume of the subarachnoid space is approximately 125 mL , for a total CSF volume of approximately 150 mL
-CSF production is 500 mL/day , which completely replenishes the total CSF volume 3-4 times per day
-CSF is absorbed primarily by the arachnoid granulations (leptomeningeal evaginations extending into the dural venous sinuses) & to a lesser extent by the lymphatic system & cerebral veins



T1 of the normal brain showing typical flow of CSF) , CSF is black , from the paired lateral ventricles (LV) , CSF passes through the paired interventricular foramina of Monro (yellow arrow) into the single midline third ventricle (TV) , CSF then flows down the single midline aqueduct of Sylvius (a channel shaped like a toothpick and slender in all diameters ; green arrow) into the single midline fourth ventricle (FV) , CSF leaves the ventricular system through the two lateral foramina of Luschka and the midline foramen of Magendie , here , CSF is shown exiting through the foramen of Magendie (blue arrow) and entering the cisterna magna (CM) , within the subarachnoid space (SAS) , CSF flows over the convexities of the brain and the folia of the cerebellum and around the brainstem (curved arrows) , from the CM , CSF also courses inferiorly to surround the spinal cord (orange arrow)

c) Etiology :-Large ventricles not always due to increased
CSF volume :1-Cerebral atrophic processes can lead to
relative enlargement of ventricles2-Ventricles may be congenitally large (probably
secondary to reduced white matter volume)

-Increased CSF volume may be due to :1-Overproduction (choroid plexus tumors , i.e.
papilloma & carcinoma)2-Obstruction of flow (non-communicating /
obstructive)3-Reduced CSF resorption (communicating non-
obstructive)

-Hydrocephalus more likely if :1-Commensurate (identical) enlargement of
temporal horns2-Ventricles disproportionately enlarged
compared to sulci3-Effacement of third ventricular recess4-Evidence of CSF transudation (periventricular)

d) Classification :(i) Non-Communicating Hydrocephalus(ii) Communicating Hydrocephalus

(i) Non-Communicating Hydrocephalus :a) Etiologyb) Radiographic Features

a) Etiology :1-Foramen of Monro Obstruction 2-Aqueduct Obstruction3-Fourth Ventricle Obstruction

1-Foramen of Monro Obstruction :a) 3rd Ventricle Tumors :1-Colloid Cyst2-Oligodendroglioma3-Central Neurocytoma4-Giant cell astrocytoma in tuberous sclerosis5-Ependymoma6-Meningioma (rare)b) Suprasellar Tumors



2-Aqueduct Obstruction :a) Congenital aqueduct stenosisb) Ventriculitisc) Intraventricular hemorrhaged) Tumors :-Mesencephalic (Mid Brain)-Pineal , posterior 3rd ventricular region-Tectal glioma


1-Midbrain , 2-Pons , 3-Medulla , 4-Cisterna magna , 5-4th ventricle , 6-Cerebellum , 7-Tentorium cerebelli , 8-Cerebral aqueduct (of Sylvius)

1-Interpeduncular cistern2-Cerebral aqueduct3-Hippocampus

3-Fourth Ventricle Obstruction :a) Congenital : Dandy-Walker (DW) malformationb) Intraventricular hemorrhagec) Infection (cysticercosis)d) Subependymomae) Exophytic brainstem gliomaf) Posterior fossa tumors: ependymoma ,
medulloblastoma , hemangioblastoma , metastasis , astrocytoma

1-Temporal lobe (Right side) , 2-Pons , 3-Fourth ventricle , 4-Cerebellar hemisphere

b) Radiographic Features :1-Disproportionate dilatation of ventricles up to
the point of obstruction2-Underlying abnormality causing the
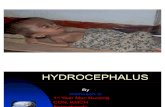
obstruction3-Ballooning of temporal horns (Mickey Mouse
ears) is a sensitive sign4-Effacement of sulci due to mass effect

Mickey mouse ears

5-Periventricular interstitial edema due to elevated intraventricular pressure and transependymal CSF flow T2 bright halo in noncompensated cases
6-Absence of normal flow void in aqueduct by MRI
7-Direct measurement of increased intracranial pressure via CSF puncture is sometimes performed for diagnostic purposes

(ii) Communicating Hydrocephalus :a) Etiologyb) Radiographic Featuresc) Normal Pressure Hydrocephalusd) Spontaneous Intracranial Hypotension

a) Etiology :-No obstruction to CSF flow but poor resorption
through arachnoid granulations secondary to :1-Post hemorrhagic (especially SAH)2-Bacterial Meningitis3-Malignant Meningitis4-Surgery5-Venous Thrombosis

b) Radiographic Features : (1-3 as non-communicating)
1-Ballooning of temporal horns2-Effacement of sulci (mass effect)3-Periventricular interstitial edema ( T2W bright
halo)4-Symmetrical dilatation of all ventricles5-The 4th ventricle is usually not very enlarged

c) Normal Pressure Hydrocephalus :1-Definition2-Radiographic Features

1-Definition :-Form of communicating hydrocephalus in
which there is no evidence of increased intracranial pressure
-Clinical triad : gait incoordination, dementia & urinary incontinence
-Clinical response to CSF tap is the gold standard for establishing the diagnosis

2-Radiographic Features :-No specific imaging findings-Dilated ventricles (frontal and temporal horns of the lateral
ventricles most affected)-Periventricular T2 bright halo-Prominent cerebral aqueduct flow void (classically referred
to hypointensity in the Sylvian aqueduct as a result of to-and-fro CSF flow , on T1 : CSF signal is replaced by signal that is lower than that of the contents of the lateral ventricles , on T2 : there is low signal instead of the expected high fluid signal)


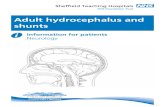
T2 FLAIR

T2 shows enlarged ventricles with normal volume of brain parenchyma , the frontal horns (solid arrow) and the posterior horns (open arrow) of the lateral ventricles are dilated , the third ventricle (arrowhead) is very wide , the hypointensity in the third ventricle signifies turbulent flow of cerebrospinal fluid

d) Spontaneous Intracranial Hypotension : (SIH)1-Incidence2-Radiographic Features

1-Incidence :-The syndrome of intracranial hypotension
results when CSF volume is lowered by leakage or by withdrawal of CSF in greater amounts than can be replenished by normal production
-Manifests as postural headache exacerbated by upright position

2-Radiographic Features :-Downward displacement of cerebellar tonsils and
midbrain (sagging) , (D.D. from Chiari I)-Flattening of pons against the dorsal clivus-Subdural collection-Diffuse brain swelling -Distention of major dural venous sinuses , the dural
sinuses enlarge as they compensate for the loss of intracranial CSF volume :
Venous distension sign >> the sign is positive when there is a convex inferior margin of the midportion of the dominant transverse sinus on a sagittal image , this is distinct from the normal appearance of this segment which usually has a concave or straight lower margin
-Diffuse dural enhancement seen in 100% of cases

T1 showing superiorly a hyperaemic and engorged pituitary gland (superior arrow) , the inferior arrow shows the abnormal inferior displacement of the cerebellar tonsils through the foramen magnum

T1 shows the sagging brain appearance with distortion of the anterior margin of the pons and medulla (black arrows) and decreased vertical dimension of the suprasellar cistern and sagging tuber cinereum (dashed arrow) , as well as the prominent pituitary gland (white arrow)

Sagittal T2 & T1+C show : sagging of the midbrain as well as cerebellar tonsils , enlarged dural sinuses and hypophysis

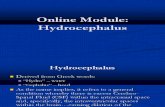
Subdural effusions

T1+C shows diffuse pachymeningeal (dural) enhancement (open arrows)

Axial T1+C showing increased dural enhancement and slightly increased subarachnoid space seen on coronal T2

T1+C shows marked enhancement of thickened pachymeninges (small arrows) and downward displacement of the cerebellar tonsils (large arrow)

(a) Normal inferior margin of the midportion of the dominant transverse sinus (concave or straight lower margin) , (b) Venous distension sign

T1 through the approximated middle third of the dominant transverse sinus shows convex inferior margin of the transverse sinus (curved arrow) that is the Venous Distension Sign indicative of IH

-Myelography is useful in identifying the location of CSF leak , ideally the lumbar puncture is performed on the CT table , 10 mls of myelographic contrast is slowly introduced into the thecal space , following removal of the needle the patient is asked to roll once and is immediately scanned , it is important to scan early as contrast will track a long way from the leak in a relatively short time

Pneumocephalus1-Trauma (compound fractures of vault , fractures
involving paranasal sinuses or mastoid air cells)2-Postoperative3-osteoma of paranasal sinus (especially ethmoid)
may erode through sinus wall4-Other sinus or skull base erosive tumors5-Empty sella (rare complication, development of
communication between sella & sphenoid sinus)