Diabetes and pregnancy Great Expectations! Sister Lesley Mowat Dr Shirley Copland.
22
Diabetes and pregnancy Great Expectations! Sister Lesley Mowat Dr Shirley Copland
-
Upload
linette-reeves -
Category
Documents
-
view
223 -
download
1
Transcript of Diabetes and pregnancy Great Expectations! Sister Lesley Mowat Dr Shirley Copland.

Diabetes and pregnancy
Great Expectations!
Sister Lesley Mowat
Dr Shirley Copland

Pregnancy -the ideal outcome
• As normal a pregnancy as possible
• Healthy mother and baby
• Aiming to reduce the rates of miscarriage, congenital anomaly and perinatal mortality to the same levels as the background population

Topics
• Prepregnancy planning
• Care during pregnancy
• Gestational diabetes

Pre-pregnancy planning
• All patients with type 1, type 2 or secondary diabetes who are in the child bearing years should be made aware of the importance of planning for any pregnancy
• Discuss during routine review along with contraception issues

Pre-pregnancy planning
• Key message is that excellent glycaemic control prior to conception and during pregnancy results in the optimal outcome for mother and baby
• Self management of diabetes and issues of hypoglycaemia need to be discussed e.g. insulin adjustment, glucose targets, driving, teach use of hypostop/glucogon to partner

Pre-pregnancy planning
• Diabetes complications need to be recognised and managed optimally
• Review medications NB Ace inhibitors are teratogenic
• Rubella status to be checked
• Commence folic acid 5mg
• Review other health issues, menstrual status and gynaecological factors

Pre-pregnancy planning
• SIGN guidelines strongly recommend that pre-pregnancy care is provided by a mutli-disciplinary specialist team
• Advise early attendance at specialist clinic for pre-pregnancy advice i.e. Combined Diabetes/Obstetric Clinic, AMH (weekly Tues pm)

Why need to plan?
• Pregnancy in Type 1 diabetes is a high risk state for both the mother and the foetus
• Increased risks of diabetes complications
• Increased risk of obstetric complications
• Increased foetal and neonatal hazards

Why need to plan?
• Patients with type 2 diabetes are also at increased risk of obstetric complications and their babies are equally at risk of malformation and neonatal problems
• Type 2 diabetes increasing in young women
• Tight glycaemic control prior to and during pregnancy is essential and insulin therapy likely to be required

Maternal risks with Type 1 diabetes
• Severe hypoglycaemia with loss of hypoglycaemic awareness (30%)
• Ketoacidosis can develop more rapidly
• Worsening of pre-existing retinopathy - laser treatment can be required
• Worsening of pre-existing renal dysfunction and hypertension

Obstetric risks in diabetes
• Increased rates of miscarriage
• Higher incidence of pre-eclampsia
• Obstructed labour and polyhydramnios now less common
• High caesarean section rates (71%)

Foetal and neonatal risks
• Congenital malformation rates remain greater than the background population e.g. cardiac defects, sacral agenesis
• Late intrauterine deaths and increased foetal distress - aim to deliver between 38-40 weeks
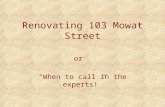
• Macrosomia(most >50th centile, many 95th)
• Neonatal hypoglycaemia is common

G E S T A T IO N ( W E E K S )
4 24 03 83 63 43 23 0
W t .( K g )
6
5
4
3
2
1
9 0
5 0

Aims prior to conception
• Blood glucose levels between 4 - 7 mmols
• HbA1c target of 7.0% or less
• Avoiding disabling hypoglycaemia
• ?How

Patient commitment
• Home glucose monitoring 4 -6 times daily (or more!)
• Multiple injection insulin regime i.e. basal bolus regime with self adjustment
• Address lifestyle issues and review diet
• Clinic visits 6-8 weekly and telephone support

Pregnant at last!
• Patients should attend combined obstetric /diabetes ante-natal clinc as soon as pregnancy is confirmed
• May need admission for stabilisation of control early or at any time during the pregnancy - open door policy in Ashgrove Ward, AMH
• Routine 2- 4 weekly review schedule followed but seen as often as required

Pregnancy
• Patients strive for near normal glycaemia throughout the pregnancy i.e. blood sugar 4-7 mmols
• Self titration of the insulin dose is essential
• Insulin doses at least double by the end of pregnancy
• Encouraged to check for ketones if bs greater the 10 mmols and seek immediate advice if present (risk of foetal death)

Delivery
• Ideally vaginal delivery between 38 and 40 weeks gestation
• Neonatal intensive care facilities required
• During labour iv insulin/10 % dextrose regime used to maintain euglycamia
• High ceasarean section rate
• Post delivery insulin doses return to pre- pregnancy level in type 1 patients. Type 2 often diet alone initially if breast feeding

Gestational Diabetes
• Carbohydrate intolerance of variable severity with onset or first recognition during pregnancy
• Usually seen in the third trimester and glycaemic control returns to normal immediately after pregnancy
• May be the first presentation of type 1 or type 2 diabetes

Gestational Diabetes
• Screening - by a random venous glucose if glycosuria ++ is detected and routinely at 28 weeks gestation
• If greater than 5.5 mmols/l two hours or more after food or greater than 7.0 mmols/l within two hours of eating then requires further investigation by a 75g OGTT

Gestational diabetes
• Diagnosis confirmed if fasting bs is greater than 5.5 mmols/l or two hour OGTT level greater than 9 mmols/l
• Associated with macrosomia and treatment by diet and/or insulin may cause a modest reduction in birth weight
• Initial management is dietary - if blood glucose remains elevated and if evidence of macrosomia then insulin treatment started

Gestational diabetes
• Marker for increased risk of future diabetes
• OGTT arranged 6 months post partum, majority are normal at that stage
• Up to 50% may go on to develop later diabetes mainly type 2
• Should be advised on lifestyle and weight reduction to reduce risk
• Protocol for follow up in primary care