DEVELOPMENTAL DYSPLASIA of THE NEONATAL HIP JOINT, Dr TRẦN NGÂN CHÂU
Upload
sai-prasanth-g-tCategory
view
68download
4
BY : G T SAI PRASANTHMODERATOR: DR VENKATDASS K
02-01-2015
GANGA HOSPITAL
DEVELOPMENTAL DYSPLASIA OF THE HIP


The early pioneers in DDH

What is DDH ?How does it occur ?Why does it occur ?When does it occur ?What are the various presentations of DDH ?How to identify DDH in children ?What are the various management principles
of treating DDH ?

Dysplastic hip:Increased obliquity and loss of concavityof the acetabular roofExcessive lateral inclination of the roofWidening of the teardropIntact Shenton’s line
Subluxated hip:Widened tear drop femoral head distanceBreak in Shenton’s lineFemoral head not in full contactReduced centre-edge angle
Dislocated hip :The femoral head is not in contact with acetabulum at all.

What is DDH ?
The AAP defines it as a condition in which the femoral head has an abnormal relationship to the acetabulum.
It is a spectrum of disorders of abnormal hip development.
Can present in varied forms at different ages.
Can present as a dislocation, subluxation, dysplasia of the acetabulum or as a component of other syndromes
(Teratologic dislocation of the hip)

Why does DDH occur ? ( Etiology )
Predisposing factors for development of DDH include : Ligamentous laxity Breech position (esp. the frank breech ) Postnatal positioning of the child Primary acetabular dysplasia (unlikely) Racial predilection

Ligamentous laxity as described by Wynn - Davies
The maternal Relaxin hormones cross the placenta and induce ligamentous laxity, female child more affected.
Newborns with DDH have a higher ratio of Collagen III to Collagen I.
DDH is found in families with laxity as a trait.

Prenatal positioning is stronglyassociated with DDH
16% of infants with DDH are born in breech postion
Frank breech with flexion at hip & knees in complete extensionare most predisposed to develop DDH.The pull of hamstrings can predispose to the dislocation.
OligohydramniosIntrauterine CrowdingInvolvement of left hip more than rightFirst born child

Postnatal positioning in cradle boards be predisposing factor, while abducting them can be protective.
Whites and Native Americans have a higher incidence
Association of DDH with other conditions like : Metatarsus adductus Torticollis Hyperthyroidism in pregnancy

How does DDH occur ? (Pathophysiology)
The affected hip
spontaneously
slides out.
subluxatable hip
Posterosuperior rim of acetabulum loses its sharp margin, becomes flat & thickened.
The capsule becomes loose and more elastic.The ligamentum teres elongates.

Neolimbus of Ortolani
Produces the *clunk* Dislocatable hip
Hip out of acetabulum
Hips that are dislocated have20 Barriers to Reduction :
Thickened pulvinarElongated ligamentum teresThe inferior capsule hour glass
Dislocated hip

Iliopsoas attaching to the lesser trochanter narrows the openingacting like a * Chinese Finger trap*.
Chronic long standing dislocated hips have acetabular muscular and femoral head changes.
The acetabulum becomes excessively anteverted, the roof becomes convex, medial wall thickensThe femoral head becomes oval and medially flat.High riding dislocationThe muscles become short and contribute to the upward pull

How does DDH present ? (Clinical features)
In a Neonate : Ortolani or Barlows Sign Ultrasonographic features
Hip examination in a neonate : Relaxed child (well fed, calm, mothers lap, quiet
room) Experienced examiner * Feel* of the hip movements – a delicate event Examine one hip at a time Very light touch Spending adequate time with the patient

Barlow’s sign
Attempt to dislocate / subluxate the femoral head from the acetabulum Hip is ADDUCTED, a gentle push applied to slide the hip POSTERIOR
Thumb medially, apply a postero- lateral force
Hip felt to slide out of acetabulum POSITIVE
Once the force stopped, the hip slides back

Ortolani’s sign
Reverse of Barlow’s test. Attempt to reduce a dislocated hip
Thigh held b/w thumb and index finger
With the other fingers gently liftthe GT and simultaneously abductthe hip
Positive result – Femoral head slips into the socket with a palapable CLUNK
Repeat both the tests to be sureof the findings

In an Infant : The signs of DDH in the infant depends on
whether the hip is reducible or non reducible. Limitation of abduction Galeazzi’s sign Looking for the number of thigh folds
Affected hip

Klisic’s test for B/L dislocation
B/L hip dislocation in a child can be confusing due to the symmetry in findings.Symmetry on abductionKnees at the same levelKLISIC’S test to differentiate :
Index finger on ASISMiddle finger on G TImaginary line drawn should pointto umbilicus
Dislocated hip the G T comes more proximally shifting the line below the umbilicus

In a Walking child : Trendelenberg test positive Galeazzi’s sign positive Exgg lumbar lordosis in B/L cases Waddling gait Limited abduction in dislocated hips Excessive rotations

How to identify DDH ? (Radiology findings)
Various radiographic techniques used : Ultrasonography Arthrography X rays Magnetic resonance Imaging

The role of Ultrasonography in DDH
Shows the soft anatomy& relationship of femoral headwith acetabulum.
Pioneered by GRAF
Articular cartilage little echoCapsule, muscles moderate echoFibrocartilagenous labrumstrong echo
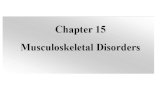
Lateral imaging technique
Examination at 6 weeks of age found to be most sensitive

BASELINE
ACETABULARROOFLINE
INCLINATIONLINE
The intersection of the baseline and the acetabular roofline forms the ALPHA angle
The intersection of the baseline with the inclination lineforms the BETA angle
As the alpha angle decreases the acetabular wall becomes more shallow.
Lesser the alpha angle and greater the beta angle - subluxated femoral head
GRAF CLASSIFICATION:Graf I – normalGraf II – immature/ somewhat abnormal Graf III – subluxatedGraf IV – dislocated hips

Advantages and disadvantages of using Ultrasonography to diagnose unstable hips Advantages :• A very sensitive indicator of infant hip abnormality as compared to radiography.• Picks up cases that are clinically silent and will dislocate in future• Can be performed on all within 2-3 minutes
Disadvantages :• It is too oversensitive and results in overtreatment of hips that would otherwise develop normally• In infants younger than 3 months old, the Graf method is unreliable as the reference points are indistinct.• Some ultrasonographically normal hips also may dislocate.
CONSENSUS :USG is a valuable adjunct to clinical exmn and radiography and must be used judiciously.

The role of X rays
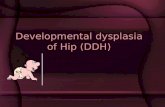
Features of an Unossified pelvis:
• Upper femur is not ossified.• Most of the acetabulum is cartilagenous in the form of Triradiate Cartilage• Hilgenreiner’s Line : A line through the triradiate cartilages• Perkins line : A line perpendicular to the first, at the lateral margin of the bony acetabulum.• Shenton’s Line • In a normal hip, the medial beak of femoral metaphysis lies in lower inner quadrant.

Measurements of Acetabular Index: Angle formed by junction of HG line with a line drawn
from the acetabular surface. Newborns : Avg 27.5 0 , 6 months 23.5 0, 2 yrs 20 0
Older child the center-edge angle is used . Junction of Perkin’s line with a line from the centre of
femoral head to lateral margin of acetabulum.6-13 yrs : >19 0 normal, >14 yrs : 25 0(SEVERINS
Classification)

Acetabular teardrop :• Appears normally b/w 6-24 months in normal hip and later in dislocated hip.• Teardrop in a dislocated/subluxated hip is wider and loses its convexity
Acetabular Index of Depth :Depth of the centre Width of the opening
>38% is normal
Femoral head extrusion IndexFalse profile view : For evaluating the anterior acetabular dysplasia

The role of Arthrography & MRI
Severin pioneered the description of the arthrographic anatomy of the hip joint.
Patient under GA, median subadductor approach used. Insert the needle 2 cm distal to origin to the adductor
longus, direct the needle medially towards the opposite Sternoclavicular joint.
A small amount of contrast injected. If in the joint the contrast shouldflow freely around the femoral head.Xray films should be taken in all directions of joint movement

• The free margin of acetabular labrum is seen as a ‘ Sharp thorn’ overlying the femoral head. • In dislocated position of the femoral head, the capsule is enlarged over the femoral head& ‘hourglass’ constriction seen.
USE OF MRI:
• Excellent anatomical view of the infant hip.• The downsides being the cost and the need for sedation in infants.• MRI classification of Kishiwagi for DDH hips :• Group I : Sharp acetabular rim, reducible with Harness• Group II : Rounder acetabular rim, may be reduced with Harness• Group III : Inverted acetabular rim, not reducible

How to treat this patient ??
Depending on the age of the patient at the time of diagnosis and treatment : Treatment of the neonate Treatment of the young child ( 1 – 6 months
old ) Treatment of the child ( 6 months to 2 yrs
old) Treatment of an older child (> 2 yrs old )

Treatment of the Neonate
PAVLIK HARNESS is the preferred treatment Indications :
Positive Ortolani’s Sign Positive Barlow’s sign USG abnormal at birth Repeat at 6 weeks If found abnormal Harness
How to put a Pavlik’s Harness ?Chest strap just below the nipple lineFeet placed in the stirrups & hips placed in 120 0 of
flexionPosterior strap to be applied loose, let the abduction
occur with gravityNever force abduction by the straps

• Hyperflexion of the hips produces femoral nerve palsy due to compression
• Hyperflexion can also cause femoral head to dislocate inferiorly.
• Inadequate flexion will fail to reduce the hip
• Forceful abduction can cause avascular necrosis of femoral head due to compression.
• Educate the parents regarding the care of the baby with Harness.
• Repeat clinical exmn and USG at the end of 6 weeks of treatment • If clinical exmn is negative and USG shows a well
reduced hip, then discontinue the harness and follow clinically
• If the hip remains dislocated, discontinue the harness, examine the hip under anesthesia & arthrography to ascertain the cause.

Treatment of the Young Child (1-6 months)
PAVLIK HARNESS The first choice of treatment for dislocated/subluxated
hips Maintain flexion more than 90 0
Examine the child weekly with clinico-USG exmn & after 3-4 weeks;
If reduction obtained, continue the Harness for 6 more weeks.
If reduction not obtained, discontinue Harness and try for other treatment methods.
A P radiograph of the hip and look for a notch above the acetabulum. The presence of this notch is a good sign & it indicates good acteabular development.

Problems and complications of Pavlik Harness
• Failure of reduction of the hip joint, especially the high dislocations
• Avascular necrosis of the joint :• Hospital treated children have higher chances than
those treated at home
• High dislocations treated with Harness.• Forceful abduction and reduction
• Femoral nerve palsy
• Pavlik Harness Disease: • Prolonged positioning of the hip in flexion and
abduction potentiated dysplasia
• Flattening of posterolateral acetabulum• Discontinue Harness after 3-4 weeks if reduction not
achieved.• Factors leading to Harness failure : • > 7 weeks at presentation, b/l hip dislocation, absent
Ortolani’s sign.

Treatment of the child ( 6 months to 2 years old)
Either the child presents first time with a dislocated hip or he/she were initially treated with splintage which failed.
Goals of the treatment : Obtain and maintain reduction without AVN.
Methods of treatment: Closed reduction +/- Traction Open reduction +/- Traction

Use of Traction for reduction
• The need for traction as a prerequisite for reduction has been a controversial area.• The need for traction has been challenged by the fact that hips can reduced safely without preliminary traction.• Different application methods of traction exist :
Bryant’s traction position(hip at 900 flexion )
Traditional traction position (hip at 300flexion)

CLOSED REDUCTION
• Done under GA / deep sedation• It is a seemingly simple procedure but, the proper performance and interpretation needs experience.
• The method of closed reduction :
Flex the hip beyond 90 0
Gradually abduct the limb while gently lifting the greater trochanter
After palpable reduction is felt, move the hip to determine its ROM
The Hip is moved in all planes till the point of redislocation
Compare the reduced ROM with the maximum ROM

From this construct a * SAFE ZONE *, the range of movements during which the hip remains in the
acetabulum.
A wide safe zone indicates a stable hip
A wide abduction or the need for 10-15 0 of internal rotation to maintain reduction, indicates an unstable hip
Obtain an Arthrogram at the time of reduction to evaluate the depth & stability of reduction.
The width of the medial dye pool on an AP radiograph indicates the likely stability.
Good reduction – narrow rim of contrastFair reduction – 5-6 mm of dye poolPoor reduction - > 6 mm dye pool

• A stable hip has wide SAFE ZONE and gets dislocated only at the periphery of movements
• An unstable hip redislocates easily and has a narrow safe zone. • Open reduction must be performed for cases where closed reduction is not able to hold the hip in reduction.
• Casting can be done for stable hips for 6 weeks and the acetabular development is good, femur becomes well seated.

HIP SPICA CAST
The Hip Spica cast should maintain more than 900 flexion, 30-400 abduction, around 10-150 internal rotation.
The most experienced must hold the position of immobilization.
Extreme abduction/ internal rotation can cause AVN. After cast, take an intraop X ray/ CT to see the
reduction. MRI can also be performed as it gives additional
information about the femoral head vascularity. After 6 weeks remove the spica, Exmn Under
Anaesthesia is performed. Put the hip through moderate range of movements
and look for the stability

Repeat the AP X ray and look for reduction. Reapply the cast if the reduction is good.
After 6 weeks the second cast is also removed and the child examined again.
A third cast may or may not be applied for 6 weeks/ abduction splint may be used.


OPEN REDUCTION
• The primary indication for open reduction is failure to obtain a stable hip with closed reduction.
• Open reduction of the hip is done either through :• Medial approaches• Anterior approach
• The medial approach has the advantages of minimal dissection & viewing the obstructions to reduction directly.
• The disadvantages include a limited view of the hip joint and damage to MFCA.
• The anterior approach provides good exposure and Capsulorrhaphy can be done.

Medial Approach to open reduction
Not a surgery for the inexperienced surgeon as the chances of causing AVN to the femoral head are high.
Recommended for children 1 year or younger.The MFCA vessels cross the operative field and have to
be retracted to safety.Transect the iliopsoas+/- adductor longus , incise the
medial hip capsule and reach the joint.Removal of thickened & constricted medial capsule +
removal of ligamentum teres allows reduction.Take a radiograph to assess the reduction.Post operatively, place the child in a below knee hip
spica cast.Convert it to above knee spica after 6 weeks if reduction
maintained.


Anterior Approach to open reduction
Has stood the test of time.Pros being a wider exposure of the hip joint as
compared to the medial, good cosmesis (using the bikini incision), ability to perform capsulorrhaphy but difficult to expose the depths of acetabulum.
In cases of high dislocation of femoral head, the technique can be challenging as the muscles are constricted.
Take a radiograph after the joint has been reduced. If reduction is too tight do a femoral shortening and capsulorraphy if the capsule is too lax.
Apply a hip spica cast after reduction with a bar in between.
Take a radiograph after 6 weeks and reapply the cast.


• Treatment of the Older child ( 2 yrs and older ):
• Problems faced in the older child :• Femoral head is usually in a more proximal position• Hip muscles are severely contracted
• Femoral shortening is needed & higher the dislocation more is the shortening needed.
• Primary acetabular reorientation osteotomy may be needed.
• Children between 2-3 yrs of age, pelvic osteotomy is needed if the acetabular coverage is not adequate.
• Children who are older than 3 yrs at reduction usually need an acetabular procedure.

A potential complication of combining acetabular procedure with femoral shortening is ‘Posterior dislocation of hip’
Occurs usually during the derotation.

Age based guidelines for the treatment of DDH
Neonate - Place the patient in Pavlik harness for 6 weeks1 to 6 months – Place the patient in a Pavlik harness for 6
weeks after the hip reduces6 to 18 months – Treat he patient with taction & closed
reduction. Closed reduction successful – hip spica for 3 months
Closed reduction unsuccessful – Open reduction medial approach(<12months), anterolateral approach (>12 months)
18-24 months – Treat the patient with a trial of closed reduction or open reduction ( anterolateral approach)
24 months- 6yrs – Primary open reduction ( AL approach) + femoral shortening ,+/- Salters Osteotomy

Complications and Pitfalls of the available treatment
Avascular necrosis of femoral head Inadequate reduction and redislocationResidual acetabular dysplasia

Avascular necrosis of femoral head
Excessive pressure application to the femoral head : Immobilization in extreme abduction or internal
rotation Contraction of the muscles crossing the hip Increases the pressure on the femoral head &
occludes the vascularity Diagnosed when the femoral head fails to ossify or
grow even after 1 year of reduction. Widened femoral neck, bone density changes. Measurements in a normal femur:
L = 2 x R Tip of GT slightly below the centre of head Auriculotrochanteric distance = 10-25 mm.

Classification systems:

• In B-O type I AVN, changes are limited to femoral head, & the metaphyses isn’t involved. Irregular ossification of the head.
• In B-O type II AVN, the lateral metaphysis sustains injury -- leadingto an early closure of the lateral epiphysis – VALGUS deformity.
• In B-O type III AVN, the entire metaphysis is affected – premature closure of the physis -- extremely short femoral neck.
• In B-O type IV AVN, growth disturbance of the medial growth plate -- VARUS deformity.
• With B-O types II,III,IV there is relative overgrowth of GT &reversal of auriculotrochanteric distance leading to abductor limp.
• Abductor limp : shortening of femoral neck (decreases the lever arm) , lengthening of GT causing decreased abductor action.

Interventions to treat AVN affected hips :
Trochanteric Epiphysiodesis can prevent overgrowth of GT, best for children around 5 yrs, presence of ossific nucleus of GT
Trochanteric advancement can be performed in the presence of an abductor limp due to GT overgrowth. Lateral transfer is better & usually done at 8 yrs of age.
Intertrochanteric Double Osteotomy performed when the trochanter is markedly overgrown & abutting the pelvis. Double osteotomy of the femoral neck is done. Technically very challenging.
Lateral Closing Wedge Valgus Osteotomy with Trochanteric Advancement usually used for coxa vara with trochanteric overgrowth.

Inadequate Reduction & Redislocation
Most common complication of managing DDH patients is failure to obtain and maintain the reduction.
Failure to recognize a dislocated hip after a closed reduction warrantes a poor outcome.
A redislocation after an open reduction is a difficult situation.
The tissues around the hip are very much constricted and scarred.
Closed reduction/ repeat open reduction of a failed open reduction can be performed.

Residual Acetabular Dysplasia
Post – reduction the actebulum remodells in response to the pressure exerted by the reduced femoral head.
If this process is incomplete, certain parts of acetabulum remain dysplastic.
The development of the “sourcil” or eyebrow indicates proper acetabular development.
Indicators of improper acetabular development: Widening of joint more than 6% up-sloping sourcil

Late presenting Acetabular Dysplasia
The patients may present with hip complaints late in adolescence.
Aching pain, pain in the groin region (hip jt) or lateral hip pain (abductor fatigue).
Presence of limp, positive Trendelenberg test and Trendelenberg sign.
Labral tears and degeneration due to deficient acetabular coverage pain is provocated by Impingement test (flexion,internal rotation and adduction)
AP radiograph, false profile view, abduction internal rotation view & Gad enhanced MRI arthrogram may be used.
Gd-MR-arthrogram demonstrates labral pathology.

Abduction-internal rotation view shows concentric reduction of hip
False profile view : for assessing the anterior acetabular coverage
AP radiograph to differentiate between subluxation, dislocation and dysplasia.

Treatment strategy for late presenting acetabular dysplasias
Take a supine X ray of the hip in abduction + internal rotation
Assess whether hip can be concentrically reduced
Yes No
Perform redirectional Salvage procedure performed
procedures that reorient Femoral head is not covered by
acetabulum & increase the preexisting articular cartilage
femoral head coverage

Reconstructive procedures for Dysplasia

Pemberton’s Osteotomy
aka pericapsular osteotomy of the iliumRedirects the inclination of the acetabular roof by an
osteotomy of the ilium superior to the acetabulum followed by levering the roof inferiorly
The triradiate cartilage acts as a hinge on which the acetabular roof is rotated anteriorly & laterally
Recommended for dysplastic hips b/w 1 yr to 12 yrs in the presetting of concentric reduction of femoral head
Advantage over Innominate osteotomy is that : Internal fixation not always required No need of implant removal Greater degree of correction can be achieved

Pemberton’s Osteotomy

Salter Innominate Osteotomy
Salter observed that on extending these hips there is a deficient cover anteriorly and on adducting superior deficiency
Salter’s osteotomy of the innominate bone – redirection of the acetabulum for better anterior and superior coverage
Prerequisites for success : Femoral head opposite the acetabulum No contractures of iliopsoas & adductor Concentric reduction of femoral head in the
acetabulum Congrous joint Good range of hip movements

Salter Innominate Osteotomy

Dega Osteotomy
Dega’s Osteotomy allows allows the surgeon to increase acetabular coverage anteriorly, centrally, or posteriorly.
The osteotomy starts above the acetabulum and proceeds into the triradiate cartilage behind and beneath the acetabulum.
The acetabular fragment is then pried downward and held in place with bone wedges.
The placement of the wedges determines the area of acetabular coverage that is improved.
If wedges are placed posteriorly, posterior acetabular coverage is augmented, as is often necessary in neuromuscular-related hip dislocations.


Ganz osteotomy
Triplanar periacetabular osteotomy.Adolescents and adults who require correction of
congruency and containment of the femoral headProximal femoral osteotomy can be combined when
femoral degenerative changes are present. This helps to achieve uninvolved wt bearing surfaces
Advantages : Only one approach Large amount of correction can be performed Correction in all planes can be performed Acetabular blood supply preserved Posterior column of pelvis remains intact, immediate
weight bearing can be started

Chiari Osteotomy
Chiari Osteotomy is performed when concentric reduction of hip is impossible.
It is an Osteotomy that augments the acetabulum.A controlled fracture through the ilium – medial
displacement of the acetabular fragment & the intact hip capsule
Improves the superolateral femoral coverage It is a salvage procedure & places the femoral head under
a surface of cancellous bone with capacity for regeneration
Indications : coxa magna after AVN/Perthes disease congenital subluxations 4-6 yrs of age, untreated DDH
> 4 yrs Dysplastic hips with osteoarthritis Paralytic dislocations caused by muscle weakness

Teratologic dislocation of the hip
Also known as Antenatal Dislocation of the hipFixed dislocation at birth, with restriction of ROMMost of these children have an associated syndrome/
MSK abnormalityArthrogryposis, myelomeningocoele, chromosomal
abnormalities, diastrophic dwarfism, lumbosacral agenesis.
The treatment of these hips depends on the nervous system functioning, prognosis of ambulation post reduction, muscle power in lower extremities etc.
Closed reduction is usually unsuccessful Open reduction when the child is around 6 months old.Medial/ anteromedial approach to the hip is preferred
choice of tretament.

Bibliography
Tachdjian’s Pediatric Orthopaedics 4th edition Tachdjian’s Pediatric Orthopaedics 5th edition Who’s Who of OrthopaedicsCampell’s Orthopaedics 12th ed Internet

Thank you